 Zicheng Wang
Zicheng Wang Qiushi Wu
Qiushi Wu Juan Ming
Juan Ming- 1School of Public Management, Jinan University, Guangzhou, China
- 2School of Economics and Commerce, Guangdong University of Technology, Guangzhou, China
Background: Rural–urban migrants frequently suffer from overrepresented health risks but have poor access to public health services. In China, homeownership status may play a vital role in obtaining local welfare. However, the relationship between homeownership and utilization of public health services has remained largely unexplored. This study aims to address the direct linkage between homeownership and utilization of local public health services among rural migrants in China.
Methods: We applied the dataset from the 2017 National Migrants Population Dynamic Monitoring Survey (NMPDMS-2017) to explore the direct relationship between homeownership and the utilization of local public health services. Logit regression was conducted to discuss the associations and to explore the interaction effect.
Results: The logit estimations reveal that homeownership is positively related to the establishment of a health record and participation in health education. The interaction term of homeownership and household location and the interaction between homeownership and healthcare center location are related to the increased establishment of a health record. However, the interaction of homeownership and household location merely reveals significant correlations with the health education model.
Conclusion: Homeownership is positively associated with the utilization of local public health services among rural migrants in China. Furthermore, homeowners living in urban residential communities and within the vicinity of the healthcare center are more likely to access public health services than those living in other locations.
Background
China has experienced a massive internal migration since 1978. In 2018, approximately 288 million rural migrants were employed as industrial workers in destination cities. They have become an indispensable part of the urban labor force and an inalienable component of the urbanization of the country (1). However, the Hukou system in China divides the population into rural (agricultural Hukou) and urban (nonagricultural Hukou) parts. Agricultural Hukou are assigned to residents who were born in towns and villages; urban Hukou are usually for those who were born in cities. The migrants with agricultural Hukou can apply for urban Hukou when they meet certain criteria, including educational achievement, social insurance, vocational qualification certificate, etc. These criteria are so strict that few can obtain the access. Without a local non-agricultural Hukou, rural migrants are mostly excluded from sharing public benefits from the local governments as they have limited access to purchase a house and utilize the public health services. Moreover, their children do not qualify for local public education. Thus, the Hukou system still acts as a main constraint preventing rural migrants from migrating to urban cities for employment and reducing their access to local public services and permanent settlement (2, 3). In fact, their temporary status categorizes them as marginalized in destination cities (4, 5). They are often treated as cheap laborers who substitute for urban citizens in undertaking undesirable jobs, but they share no equal rights with the local citizens. Rural–urban migrants are frequently exposed to overrepresented health risks, including communicable diseases (e.g., tuberculosis and sexually transmitted diseases), non-communicable chronic diseases and risk factors, workplace injury and occupational health risks, and poor mental health and women's health (6). However, rural migrants are still regarded as outsiders in terms of access to the local welfare system (7), and urban public health care to them is limited (8, 9).
The serious health risks of rural migrants are among the most concerning issues in the process of new urbanization in China (10). The public healthcare system is almost universally accepted as an important factor that would enhance the health status of migrants (11). In 2009, the central government launched the Essential Public Health Services (EPHS) project to provide basic health services to all urban and rural dwellers (12, 13). This project consists of nine types of basic services, including the establishment of health records, health education, health services for children aged 0–36 months, maternal health services, elder health services, immunizations, infectious disease reporting and treatment, services for patients with type II diabetes, and services for patients with severe mental illness (14–17).
Unfortunately, rural migrants remain less likely to utilize basic public health services compared to local citizens (8, 16). Previous studies have discussed the determinants of public healthcare utilization from the supply and demand sides. Demographic and socioeconomic factors are the major determinants on the demand side (18, 19), while the prevalence of healthcare utilization is differentiated by gender, education attainment, employment status, migration duration, health status, and others (16, 18, 20–22). On the supply side geographical access (distance) is regarded as the main barrier to accessing healthcare services (15).
However, those studies offer no direct discussion on the relationship between homeownership and public healthcare utilization. Homeownership is widely perceived as the crucial milestone in the assimilation process, wherein owning a house represents the long-term commitment to settle down permanently and become a member of the local society (23, 24). Thus, homeownership may establish access to neighborhoods with improved physical and social conditions (25, 26) and, in turn, influence the utilization of local public health services. In the case of China, rural migrants often experience poor living conditions and have a low likelihood of becoming homeowners (27, 28). Homeownership has served as a precondition for attaining membership in major cities and the first step toward obtaining local welfare benefits, such as education, health care, and welfare provision (29, 30).
To address this gap, the current study employs a unique national survey in China to further explore the direct linkage between homeownership and public health services utilization. Three issues are addressed. First, is there a positive association between homeownership and the utilization of local public health services? Second, does any interaction effect exist between homeownership and the location of household/healthcare center access to public health services? Third, does homeownership effect vary in terms of employment status, migration duration, and migration patterns?
This study contributes to the literature in two distinct ways. First, it addresses concurrently the demand- and supply-side barriers to local health service utilization and emphasizes the direct role of homeownership. Second, it is the first study to explore the direct relationship between homeownership and local public health service utilization within China.
Materials and Methods
Data Sources
We used data from the 2017 National Migrants Population Dynamic Monitoring Survey (NMPDMS-2017) conducted by the National Health and Family Planning Commission of China. NMPDMS-2017 is an open-access and nationally representative cross-sectional survey of internal migrants aged 15–69 years. These migrants lack the local Hukou, and they have lived in local cities for more than 1 month. The survey is conducted in 32 provincial units, which cover all 31 provinces and the Xinjiang Production and Construction Corps (XPCC) of China, 348 cities, and 8,450 communities or villages. The distribution of households surveyed across provincial units ranges from 2,000 to 10,000, including seven sampling units that consist of 2,000, 4,000, 5,000, 6,000, 7,000, 8,000, and 10,000 households. A total of 2,000 households are selected from the least populous unit (i.e., XPCC), and 10,000 households are selected from the largest units, such as Zhejiang and Guangdong provinces.
Sample populations are drawn using the stratified multistage random sampling method with the probability proportional to size (PPS) approach. City units in a province were divided into two tiers. One tier was the mandatory cities, including the provincial capitals and specific major cities. The second tier was all other cities (the city list is available from the https://chinaldrk.org.cn/wjw/#/home). Implicit stratification was implemented in city units according to the population size of the counties and the townships. The primary sampling units were townships, which were drawn from the city units using PPS. The village or neighborhood committee was derived from the townships. The two-phase sampling was applied to draw 20 household samples from targeted village or neighborhood committee. The respondent was the final sampling units, which were obtained using systematic sampling. If more than one individual was sampled in a household, the resample should be carried out until only one qualified migrant was sampled. When it is impossible to access the targeted sample, the NMPDMS team would replace this respondent with another one of the same gender, similar age, and similar residence duration.
Approximately 169,000 households were sampled, according to the definition of migrants. After eliminating missing variable data, we obtained 132,555 valid household samples.
Variables and Measures
The dependent variable is the utilization of local public health services. This variable is specified as the establishment of a health record and access to health education, which are two popular forms of essential public health services. These two outcomes are binary variables. The former was defined in accord with the question “whether you have establish a local health record”; the latter was derived from the item “which public education you have achieved from the local community in the last year.” In particular, the establishment of health record is coded 1 if the respondent is enrolled in the local health information record system and 0 otherwise. The survey incorporates all five main items of health education, including education in chronic disease prevention, mental health, infectious diseases, reproductive health, and occupational diseases. The dummy of health education attendance is equal to 1 if rural migrants attended at least one of the five items, while rural migrants who failed to attend any of the five items were set to 0.
The focal variable is homeownership derived from the question “What kind of house you actually live in in the urban destination?” Only the respondent had access to answer this question in the survey, which represents the homeownership status of the whole family. Homeownership is coded as 1 if the household owns a commodity house and 0 if they live in self-built housing, social rental, affordable housing, employer-provided dormitories, and other informal housing.
Kiwanuka et al. (31) and Jacobs et al. (32) chose control variables concurrently according to the demand- and supply-side barriers. On the demand side, demographic characteristics (gender, age, and marital status), health status (whether an individual suffers from chronic disease), and the intention of permanent settlement are incorporated1. Household location (urban residential community vs. village) and healthcare center location (whether the commuting time to the nearest healthcare center is <15 min) are included as supply-side factors.
Estimation Strategy
All analyses are conducted using Stata 15.0. Pearson chi-square and ANOVA tests are applied for univariate analysis. The logit regression model is used to explore the direct linkage between homeownership and the utilization of local public health services. The interaction and heterogeneous effects are also discussed through logit regressions.
Results
Baseline Characteristics
Table 1 presents the descriptive statistics of the dependent variables and controls. More than a quarter (26.09%) of rural migrants have registered health records, and 60.85% have participated in health education. Rural migrants have a low likelihood of becoming homeowners, given that only 17.32% of them own a house in local cities.
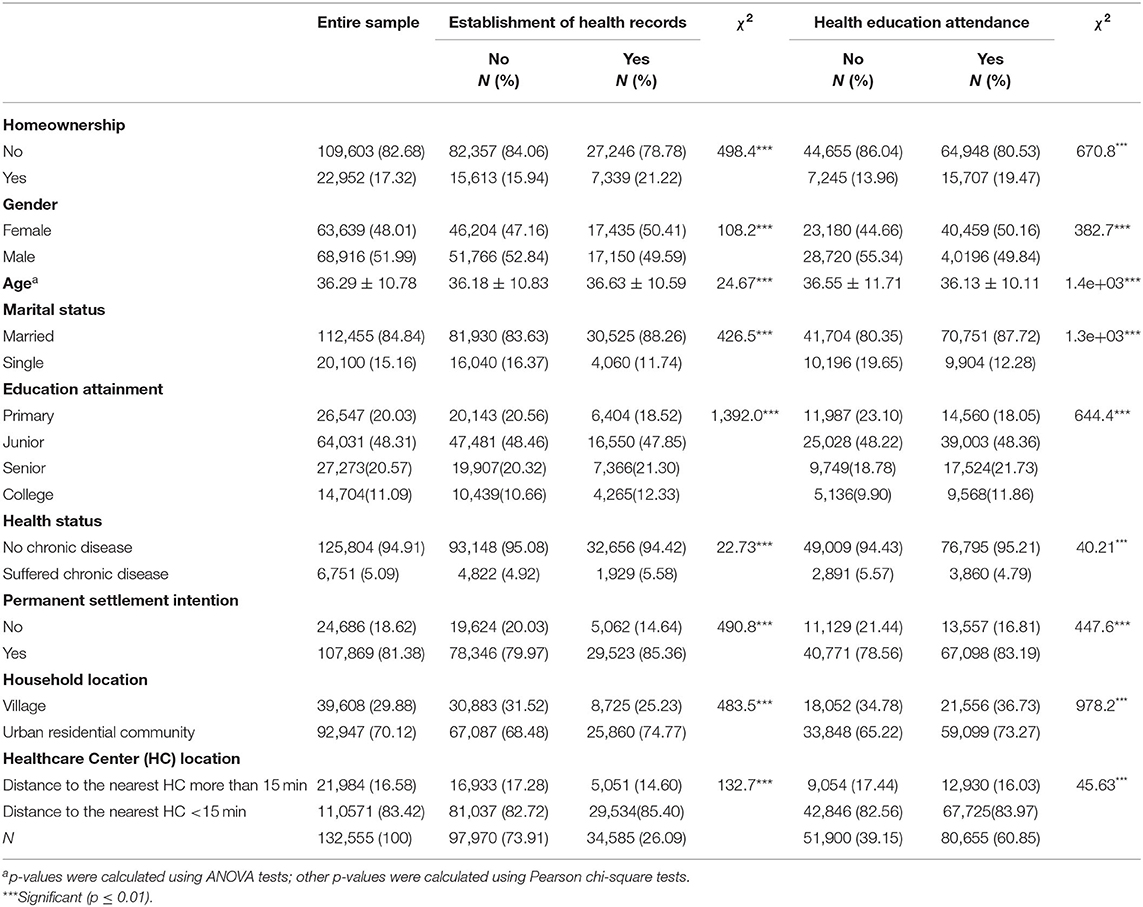
Table 1. Univariate analysis.
Of 132,555 respondents, 68,916 (51.99%) are males, 84.84% are married, and the average age is about 36 years old. Approximately one-fifth of rural migrants have no educational attainment beyond primarily school. The majority have completed the 9-year compulsory education. Approximately 5.09% of rural migrants report that they suffered from chronic disease in the previous year, and 81.38% of them intend to settle permanently. With respect to household and healthcare center locations, a mere 29.88% of rural migrants live in the village, and 83.42% spend <15 min commuting to the nearest healthcare center.
Univariate Analysis
The chi-square and ANOVA tests in Table 1 also indicate that the homeownership is more prevalent among rural migrants with health records than that of their counterparts (21.22 vs. 15.94%). Similarly, the homeownership rate among health education participants is also higher than that among non-participants (19.47 vs. 13.96%). Health record establishment and health education access have fewer male than female attendees (health record establishment: 49.59 vs. 50.41%; health education access: 49.84 vs. 50.16%) and more married than unmarried participants (health record establishment: 88.26 vs. 11.74%; health education access: 87.72 vs. 12.28%). The migrants who can access local public health services are more educated than those who lack such access. In terms of educational attainment, the majority completed senior middle school (health record establishment: 21.30 vs. 20.32%; health education access: 21.73 vs. 18.78%) and college (health record establishment: 12.33 vs. 10.66%; health education access: 11.86 vs. 9.90%). The beneficiaries of public health services typically tend to settle permanently (health record establishment: 85.36 vs. 79.97%; health education access: 83.19 vs. 78.56%). Moreover, the participants in public health services are more likely to live in the urban residential community than in villages (health record establishment: 74.77 vs. 68.48%; health education access: 73.27 vs. 65.22%) and can travel to the nearest healthcare center in <15 min (health record establishment: 85.40 vs. 82.72%; health education access: 83.97 vs. 82.56%).
Multivariate Logit Analysis
Logit regression was applied to identify the association between homeownership and the utilization of local public health services. Subsequently, odd ratios and 95% CI were calculated.
In the health record model (Table 2), logit estimations reveal that homeownership, gender, age, marital status, educational attainment, health status, permanent settlement intention, household location, and healthcare center location are related to the increasing prevalence of health record establishment. In the health education model, participation in health education is positively associated with homeownership, gender, marital status, educational attainment, permanent settlement intention, household location, and healthcare center location. However, age and health status are related to reduced access to health education.
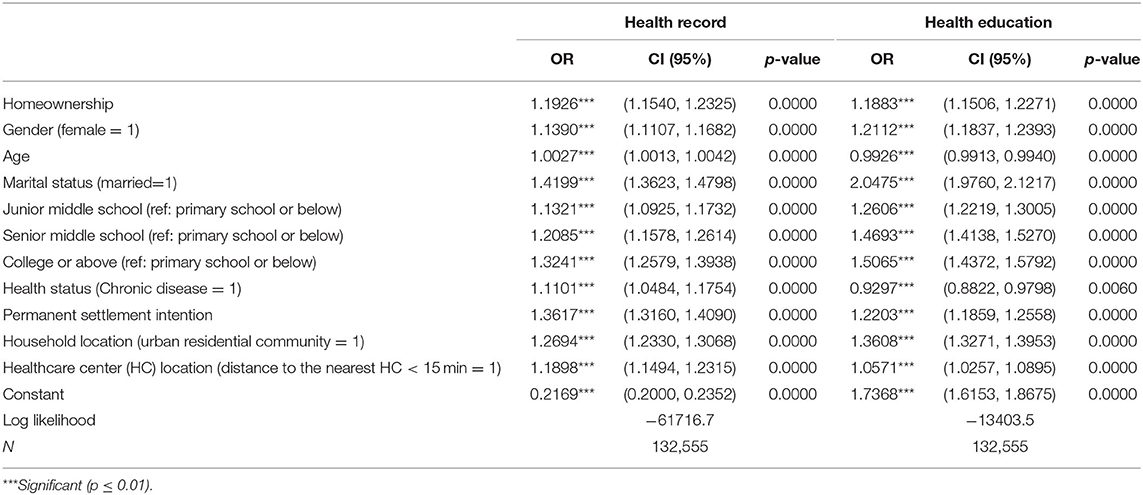
Table 2. Association between Homeownership and Utilization of Local Public Health Services.
Interaction Effect Analysis
The relationship between homeownership and utilization of local public services may depend on the location of the household and the healthcare center. To address this issue, the interaction term of homeownership and household location, and the interaction term of homeownership and healthcare center location are incorporated into the regressions. Table 3 indicates that the interaction term of homeownership and household location and the interaction between homeownership and healthcare center location are related to the increased establishment of health records. However, only the interaction term of homeownership and household location is significantly associated with the increased attendance of health education.
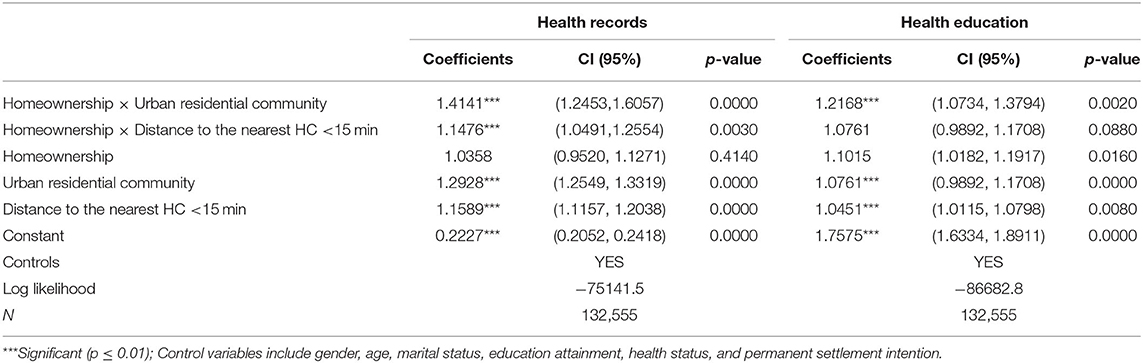
Table 3. Interaction effect of geographical accessibility and homeownership.
Heterogeneous Effect
The utilization of public health services may vary depending on socioeconomic status. To address the different traits, we divide the entire sample into several subgroups in terms of employment status, migration duration, and migration patterns. Regarding employment status, we categorize the sample as employed and unemployed groups. We also propose two migrant groups to determine migration duration, namely, short- (<5 years) and long-term (>5 years) durations. Migration pattern is dichotomized into interprovincial migration and intra-provincial migration.
Logit regression was employed to estimate the heterogeneous effects. The results from Table 4 show that associations between employment status and migration patterns are considerably similar in the health record and health education models. Homeownership is associated with increased local public health service utilization between the employed and unemployed subgroups. Certain positive correlations between homeownership and utilization of local public health services are drawn between interprovincial and intra-provincial groups. In terms of migration duration, significant relationships between long-term and short-term migrants and the prevalence of health record establishment are found. However, a significant association is found only between the short-term group and the health education model.
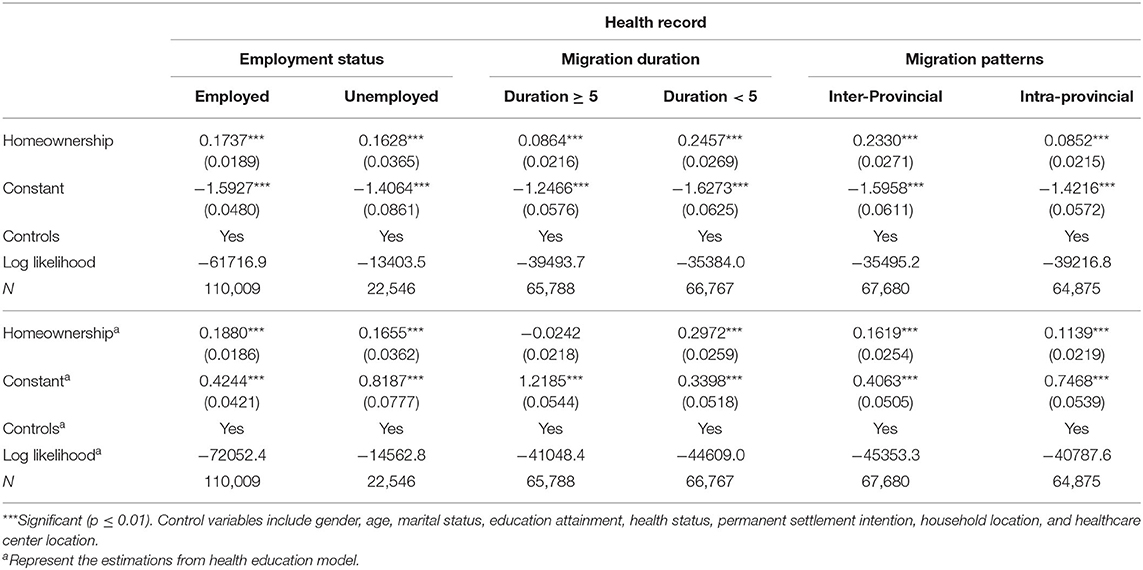
Table 4. Heterogeneous effect across employment status, migration duration, and migration patterns.
Discussion
Homeownership is positively associated with the utilization of local public health services among rural migrants. The potential mechanism may be described as follows. First, homeownership represents considerable socioeconomic success in the destination (24), and homeowners may share rising social status (33), thereby enhancing their likelihood of gaining access to local public health services. Second, owning a house in the destinations would encourage social integration among rural migrants (34), who may be encouraged to build greater neighborhood cohesion and social capital compared to renters (35). Homeownership, which symbolizes long-term residential stability, could maintain social ties and decrease stress, which may induce utilization of the essential public health services in the urban destinations (22, 36).
The control variables are also expected to show influence (Table 2). Males are less likely to utilize public health services than females, which is consistent with previous studies suggesting that females are more sensitive to health problems than males (20, 37). Regarding socioeconomic factors, high educational attainment is associated with a high prevalence of health record establishment and health education participation. These findings are consistent with previous evidence that the level of education is associated with the utilization of public health services (21, 38).
The results also reveal that migrants who suffered from chronic disease are more likely to utilize public health services than those who do not. This finding is in line with previous findings that individuals with poor health status are more likely to seek additional health services than those who are healthy (15, 20, 39). Furthermore, permanent settlement intention is related to the increased utilization of public health services, indicating that the expectation of social integration in the urban destination would encourage the seeking of public health services. This conclusion is consistent with Jing et al., demonstrating that social integration is positively related to establishment of the health records among elderly migrants in China (22).
Apart from the demand-side factors, the supply-side factors such as the availability of and convenient access to public healthcare are also regarded as important determinants (32). Migrants who live in the urban residential community and spend a short time traveling to a healthcare center are more likely to establish health records and participate in public health education than those who live in villages and spend a long time traveling to a health center. These findings are consistent with the argument that geographical accessibility is important to local public health service utilization (15, 31).
Homeowners generally reside in neighborhoods with affluent public services. The interaction effect regressions also demonstrate that homeowners living in urban residential communities are more likely to utilize public health services than those living in villages. Similarly, rural migrants who own a house within the vicinity of the healthcare center tend to access public health services. Therefore, homeownership substantially influences those with geographical access to health services, and homeowners in high-quality residential neighborhoods may exhibit high levels of social integration and numerous opportunities to utilize local public health services.
Conclusion
Main Findings
Rural migrants remain at a disadvantage for utilizing basic public health services. Homeownership status may play a vital role in attaining local welfare. This study confirms that homeownership is positively related to the utilization of local public health services among rural migrants in China. Moreover, homeowners living in urban residential communities and within the vicinity of the healthcare center are in an advantageous position to access public health services.
Limitations
This study explores the direct relationship between homeownership and the utilization of local public health services among rural migrants. Our research has two limitations. First, the NMPDMS-2017 reported only limited information about the Essential Public Health Services (EPHS). Therefore, this study discusses only two common forms of EPHS; additional items, including public health services for children and elders, immunizations, infectious disease protection, and services for patients with type II diabetes, should be incorporated in future studies. Second, the study addresses the demand- and supply-side barriers concurrently but only discusses the geographic accessibility due to data limitation. Other factors, such as availability, affordability, and acceptability of local public health services, should be further explored in future studies.
Implications
Homeownership is positively related to the utilization of public health services. Therefore, policymakers should pay increased attention to the housing attainment and improvement of living conditions of rural migrants. Providing habitable and affordable housing to rural migrants is an urgent issue for the local governments of these urban destinations. Thus, expanding the provision of public rental housing should be considered a major policy direction.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: The NMPDMS are open and available dataset from the Migrant Population Service Center of National Health Commission, the People's Republic of China (PRC). NMPDMS are however available from the Migrant Population Service Center of National Health commission upon reasonable research request. NMPDMS can be requested from the website of Migrant Population Service Center: https://chinaldrk.org.cn/wjw/#/home. Requests to access these datasets should be directed to https://chinaldrk.org.cn/wjw/#/home.
Author Contributions
ZW took leadership and responsibility for the research activity planning and made substantial contributions to the conception and design of the program. QW worked on the statistical analysis of the data. JM drafted the concept of the paper and participated in finalizing the manuscript. All authors read and approved the final manuscript.
Funding
This article was funded by the National Social Science Fund of China (grant no. 17BJY044&18ZDA081) and the Fundamental Research Funds for the Central Universities (grant no. 19JNQM16).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This manuscript has been released as a pre-print at Research Square: ZW, JM, and Jiachun Liu. Effect of homeownership on the utilization of local public health services among rural migrants in China: A nationwide cross-sectional study, 18 March 2020, PREPRINT (Version 1) available at Research Square [+https://doi.org/10.21203/rs.3.rs-17907/v1+].
Footnote
1. ^There are three potential reasons why we cannot incorporate household income into the model. First, according to the analytical framework from Jacobs et al. (32) and Kiwanuka et al. (31), household income is not viewed as the vital factor in accessing health services. Second, previous evidence from housing studies has demonstrated that household income was a significant factor affecting affordability to homeownership, which may result in multicolinearity. Third, the odd ratio of household income is closer to 1, adding it into the estimation, which indicates that income was unimportant for public health services utilization.
References
1. Wang Z, Guo M, Ming J. Effect of hometown housing investment on the homeownership of rural migrants in urban destinations: evidence from China. Cities. (2020) 105:102619. doi: 10.1016/j.cities.2020.102619
2. Yang X. Temporary migration and the spread of STDs/HIV in China: is there a link? Int Migrat Rev. (2004) 3:212–35. doi: 10.1111/j.1747-7379.2004.tb00194.x
3. Sun M, Fan CC. China's permanent and temporary migrants: differentials and changes, 1990–2000. Profes Geographer. (2011) 63:92–112. doi: 10.1080/00330124.2010.533562
4. Hesketh T, Jun YX, Lu L, Mei WH. Health status and access to health care of migrant workers in China. Public Health Rep. (2008) 123:189–97. doi: 10.1177/003335490812300211
5. Keung Wong DF, Li CY, Song HX. Rural migrant workers in urban China: living a marginalised life. Int J Soc Welfare. (2007) 16:32–40. doi: 10.1111/j.1468-2397.2007.00475.x
6. Mou J, Griffiths SM, Fong H, Dawes MG. Health of China's rural–urban migrants and their families: a review of literature from 2000 to 2012. Br Med Bullet. (2013) 106:19–43. doi: 10.1093/bmb/ldt016
7. Zhang X, Yu B, He T, Wang P. Status and determinants of health services utilization among elderly migrants in China. Global Health Res Policy. (2018) 3:8. doi: 10.1186/s41256-018-0064-0
8. Wei X, Pearson S, Zhang Z, Qin J, Gerein N, Walley J. Comparing knowledge and use of health services of migrants from rural and urban areas in Kunming City, China. J Biosoc Sci. (2010) 42:743–56. doi: 10.1017/S0021932010000313
9. Hong Y, Li X, Stanton B, Lin D, Fang X, Rong M, et al. Too costly to be ill: health care access and health seeking behaviors among rural-to-urban migrants in China. World Health Popul. (2006) 8:22–34. doi: 10.12927/whp.2006.18280
10. Gong P, Liang S, Carlton EJ, Jiang Q, Wu J, Wang L, et al. Urbanisation and health in China. Lancet. (2012) 379:843–52. doi: 10.1016/S0140-6736(11)61878-3
11. Wang L, Wang Z, Ma Q, Fang G, Yang J. The development and reform of public health in China from 1949 to 2019. Global Health. (2019) 15:45–55. doi: 10.1186/s12992-019-0486-6
12. Yin, D. A model to estimate the cost of the National Essential Public Health Services Package in Beijing, China. BMC Health Serv Res. (2015) 1:1–7. doi: 10.1186/s12913-015-0902-4
13. Burns LR, Liu GG. (editors.). China's Healthcare System and Reform. Cambridge: Cambridge University Press (2017). doi: 10.1017/9781316691113
14. Yang L, Sun L, Wen L, Zhang H, Li C, Hanson K, et al. Financing strategies to improve essential public health equalization and its effects in China. Int J Equity Health. (2016) 1:1–12. doi: 10.1186/s12939-016-0482-x
15. Tian M, Wang H, Tong XT. Essential public health services' accessibility and its determinants among adults with chronic diseases in China. PLoS ONE. (2015) 10:e0125262. doi: 10.1371/journal.pone.0125262
16. Qian Y, Ge D, Zhang L, Sun L, Li J, Zhou C. Does Hukou origin affect establishment of health records in migrant inflow communities? A nation-wide empirical study in China. BMC Health Serv Res. (2018) 18:704. doi: 10.1186/s12913-018-3519-6
17. Zhang D, Pan X, Li S, Liang D, Hou Z, Li Y, et al. Impact of the national essential public health services policy on hypertension control in China. Am J Hyperten. (2018) 31:115–23. doi: 10.1093/ajh/hpx139
18. Zhang J, Lin S, Liang D, Qian Y, Zhang D, Hou Z. Public health services utilization and its determinants among internal migrants in China: evidence from a nationally representative survey. Int J Environ Res Public Health. (2017) 14:1002. doi: 10.3390/ijerph14091002
19. Marshall KJ, Urrutia-Rojas X, Mas FS, Coggin C. Health status and access to health care of documented and undocumented immigrant Latino women. Health Care Women Int. (2005) 26:916–36. doi: 10.1080/07399330500301846
20. Lu L, Zeng J, Zeng Z. What limits the utilization of health services among China labor force? Analysis of inequalities in demographic, socio-economic and health status. Int J Equity Health. (2017) 16:30. doi: 10.1186/s12939-017-0523-0
21. Gong Y, Yin X, Wang Y, Li Y, Qin G, Liu L, et al. Social determinants of community health services utilization among the users in China: a 4-year cross-sectional study. PLoS ONE. (2014) 9:e98095. doi: 10.1371/journal.pone.0098095
22. Jing Z, Wang Y, Ding L, Tang X, Feng Y, Zhou C. Effect of social integration on the establishment of health records among elderly migrants in China: a nationwide cross-sectional study. BMJ Open. (2019) 9:e034255. doi: 10.1136/bmjopen-2019-034255
23. Alba RD, Logan JR. Assimilation and stratification in the homeownership patterns of racial and ethnic groups. Int Migrat Rev. (1992) 26:1314–41. doi: 10.1177/019791839202600411
24. Amuedo-Dorantes C, Mundra K. Immigrant homeownership and immigration status: evidence from Spain. Rev Int Econ. (2013) 21:204–18. doi: 10.1111/roie.12031
25. Bramley G, Karley NK. Homeownership, poverty and educational achievement: school effects as neighbourhood effects. Housing Stud. (2007) 22:693–721. doi: 10.1080/02673030701474644
26. Holupka S, Newman SJ. The effects of homeownership on children's outcomes: real effects or self-selection?. Real Estate Econ. (2012) 40:566–602. doi: 10.1111/j.1540-6229.2012.00330.x
27. Tang S, Feng J, Li M. Housing tenure choices of rural migrants in urban destinations: a case study of Jiangsu Province, China. Housing Stud. (2017) 32:361–78. doi: 10.1080/02673037.2016.1210096
28. Fang Y, Zhang Z. Migrant household homeownership outcomes in large Chinese cities-the sustained impact of hukou. Euras Geography Econ. (2016) 57:203–27. doi: 10.1080/15387216.2016.1228075
29. Gan X, Zuo J, Ye K, Chang R, Li D, Zillante G. Are migrant workers satisfied with public rental housing?A study in Chongqing, China. Habitat Int. (2016) 56:96e102. doi: 10.1016/j.habitatint.2016.05.003
30. Gan X, Zuo J, Chang R, Li D, Zillante G. Exploring the determinants of migrant workers' housing tenure choice towards public rental housing: a case study in Chongqing, China. Habitat Int. (2016) 58:118–26. doi: 10.1016/j.habitatint.2016.10.007
31. Kiwanuka SN, Ekirapa EK, Peterson S, Okui O, Rahman MH, Peters D, et al. Access to and utilisation of health services for the poor in Uganda: a systematic review of available evidence. Trans R Soc Trop Med Hygiene. (2008) 102:1067–74. doi: 10.1016/j.trstmh.2008.04.023
32. Jacobs B, Ir P, Bigdeli M, Annear PL, Van Damme W. Addressing access barriers to health services: an analytical framework for selecting appropriate interventions in low-income Asian countries. Health Policy Plann. (2012) 27:288–300. doi: 10.1093/heapol/czr038
33. DeSilva S, Elmelech Y. Housing inequality in the United States: Explaining the white-minority disparities in homeownership. Housing Studies. (2012) 27:1–26. doi: 10.1080/02673037.2012.628641
34. Cui C, Geertman S, Hooimeijer P. Access to homeownership in urban China: a comparison between skilled migrants and skilled locals in Nanjing. Cities. (2016) 50:188–96. doi: 10.1016/j.cities.2015.10.008
35. Rohe WM, Lindblad M. Reexamining the Social Benefits of Homeownership After the Housing Crisis. Boston, MA: Joint Center for Housing Studies of Harvard University (2013).
36. Lim S, Stella SY, De La Cruz NL, Trinh-Shevrin C. Defining ethnic enclave and its associations with self-reported health outcomes among Asian American adults in New York City. J Immigrant Minority Health. (2017) 19:138–46. doi: 10.1007/s10903-015-0334-6
37. Jankovic J, Simic S, Marinkovic J. Inequalities that hurt: demographic, socioeconomic and health status inequalities in the utilization of health services in Serbia[J]. Europ J Public Health. (2010) 20:389–96. doi: 10.1093/eurpub/ckp189
38. Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health. (2005) 27:49–54. doi: 10.1093/pubmed/fdh207
Keywords: homeownership, utilization of local public health services, establishment of health record, attendance of health education, demand-side determinants, supply-side barriers
Citation: Wang Z, Wu Q and Ming J (2020) The Relationship Between Homeownership and the Utilization of Local Public Health Services Among Rural Migrants in China: A Nationwide Cross-Sectional Study. Front. Public Health 8:589038. doi: 10.3389/fpubh.2020.589038
Received: 30 July 2020; Accepted: 29 October 2020;
Published: 07 December 2020.
Edited by:
Mihajlo (Michael) Jakovljevic, Hosei University, JapanReviewed by:
Jacek Klich, Kraków University of Economics, PolandMilena Santric Milicevic, University of Belgrade, Serbia
Copyright © 2020 Wang, Wu and Ming. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Ming, mingjuan520888@gdut.edu.cn
†Present address: Juan Ming, School of Economics and Commerce, Guangdong University of Technology, Guangzhou, China