 Colin Tomes
Colin Tomes Ben Schram2†
Ben Schram2†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 09 November 2020
Sec. Occupational Health and Safety
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.583336
Objectives: Heart Rate Variability has gained substantial interest in both clinical and athletic settings as a measurement tool for quantifying autonomic nervous system activity and psychophysiological stress. However, its uses in tactical work settings, such as military, police, and firefighting environments, remain controversial. Given the physical, mental, and emotional stress public safety personnel face both operationally and in training, heart rate variability measurement may be key in promoting their health, safety and operational effectiveness.
Methods: This study identified, critically appraised, and summarized primary studies investigating relationships between heart rate variability and outcomes of interest to tactical personnel. Key literature databases were searched, and quality assessment checklists were applied to analyze retained literature. The results of the screening and assessment processes, along with key data extracted from each study were summarized and tabulated. Research gaps were also identified to facilitate improvements to how tactical personnel and health or performance providers may best utilize heart rate variability to monitor or promote personnel health and performance, and thereby facilitate public safety.
Results: Twenty studies were included and were all of generally high quality. Cohort size, length of follow-up, measurement objectives, data acquisition, and data analysis all varied considerably across studies, precluding meta-analysis. However, study results correlating heart rate variability and relevant outcomes indicated that overall, heart rate variability is an effective indicator of key fitness and performance elements in the tactical work setting.
Conclusions: Heart rate variability can be an effective health and performance tool in tactical work environments. However, measurement methods must be carefully selected and applied. Further research is required to understand causal relationships. Specifically, larger cohort inclusion and the isolation and study of specific variables unique to public safety work and training may improve the effectiveness of heart rate variability measurement to provide meaningful information to end users and providers.
Heart rate is typically described as the number of beats of the heart per minute, however, the time between beats in a healthy heart is highly variable; the heart is under constantly varying regulation modulating its activity from the two complimentary branches of the autonomic nervous system (ANS): the sympathetic and parasympathetic nervous systems (1, 2). The autonomic nervous system is the efferent branch of the peripheral nervous system responsible for regulating most unconscious bodily activities; respiration, distribution of blood flow, digestion, pupillary response, waste excretion, arousal, and heart rate (1). The ANS is itself composed of two complimentary pathways that typically act antagonistically to maintain homeostasis. The sympathetic nervous system originates from the thoracic and upper lumbar vertebrae, and governs response that require immediate action, such as the “fight or flight” response to acute stress. The parasympathetic nervous system is characterized as a more slow-moving, dampening response, and governs actions that do not typically require immediate action (1).
With respect to the heart specifically, the sympathetic nervous system increases heart rate, which will decrease the variation in time between beats. This is accomplished not only through direct innervation, in which the muscle is stimulated to contract more quickly and more forcefully, but also through catecholamines secreted via the adrenal glands (1). The parasympathetic nervous system regulates the heart through the vagus nerve, slowing conduction of the sinoatrial node and contributing to respiratory sinus arrhythmia, the natural increase in heart during inspiration and decrease during expiration (3).
Disruption of the balance between sympathetic and parasympathetic influences on the cardiovascular system can lead to devastating health consequences (4, 5). These disruptions have been described as excess allostatic load (6). Allostatic loading occurs in situations of either energy insufficiency, in which energy demand exceeds supply, and focus must be diverted wholly to survival and the maintenance of a positive energy balance, or in situations with energy abundance, but social conflict or disruption (6). While the two types of allostatic load differ to some extent, both disrupt cardiovascular autonomic balance, and are associated with the development of chronic diseases, such as excessive inflammation, chronic pain, diabetes, asthma, fatigue, depression, and anxiety (5). Acute injuries, such as concussion, may also contribute to elevated allostatic load (7), and consequent disruptions to cardiac autonomic balance. Conversely, higher levels of physical fitness are associated with a more optimal cardiovascular autonomic balance (8).
HRV has been identified as a valid measurement of autonomic nervous system regulation and has both time and cost advantages over other methods, such as biomarker testing, while also being noninvasive. With recent technological developments, HRV data are now available and interpretable by coaches and individual athletes, not requiring specialist appointments to read or understand results (9). Correlations between HRV measurements and process or outcome measures are allowing for readily accessible insights to valuable health and fitness data (10, 11) and have been associated with the prediction of morbidity from the chronic and acute disorders mentioned above. Individuals at high risk for the development of ANS dysregulation or allostatic loading and consequent morbidity may therefore benefit from HRV monitoring. In the athletic performance setting, HRV data has been proven useful in improving the precision of energy expenditure estimates (12). More recently, HRV has been investigated as a means of quantifying fatigue and recovery levels, detecting overuse injuries, and calibrating training loads (11, 13, 14). Research continues to emerge linking HRV domains to human performance optimization efforts, which have themselves recently gained interest within the tactical community.
Tactical personnel, individuals who have sworn to protect and serve their communities (15), and who may place their own health and safety at risk in execution of those duties, are often faced with a multitude of unique challenges that often result in stresses to their autonomic nervous systems (16, 17), and may benefit from access to the fitness and health data HRV analyses can provide. For example, police officers and other first responders (firefighters, emergency medical responders) may be sedentary for the majority of their time on duty but could be called with little to no warning into situations of extreme danger and physiological stress (18). The ability to monitor physiological response during these events may help protect their health. Likewise, military personnel, while often prepared in advance for deployment, are exposed to high levels of physical, mental, and emotional stress for prolonged periods of time (19), and may thus also benefit from physiological data measurement and analysis. Furthermore, tactical personnel are also regularly subjected to operations in austere environments, dysregulated sleep and poor nutrition (20, 21). As a result of these occupational demands, literature has reported the risk of cardiovascular disease, especially in police officers, may be greater than that of the general population (22). Conversely, many tactical personnel perform at extraordinary levels of physical performance and may seek to optimize their training, avoid overtraining and maximize the balance between training and operational demands (23).
As a result, HRV applications developed in both clinical and athletic settings may be of interest to tactical organizations seeking an inexpensive and noninvasive means of monitoring the health and fitness of their personnel, both in training and in operations. However, the unique requirements of working as a tactical professional may dictate that functional inferences derived from HRV measurements originally developed in athletic or clinical populations may not always generalize to tactical populations (15). To date, no comprehensive, systematic reviews of the literature examining associations between occupational fitness, operator or trainee health, or occupational performance and heart rate variability analyses for tactical personnel have been conducted. Therefore, the aim of this systematic review was to identify primary studies examining relationships between HRV and relevant health and operational outcomes specifically in tactical personnel, critically appraise the methodological quality of the identified studies, and summarize the results to inform tactical professionals and those in the health and performance fields supporting tactical professionals.
Prior to conducting the initial search, this study was registered with PROSPERO (ID: 153293). The PRISMA guidelines for systematic reviews were followed and the outcome of each step can be found in Figure 1 (24). A rapid search using a set of predetermined keywords was conducted to determine relevant subject heading terms and develop a sample of salient articles to guide a detailed search strategy.
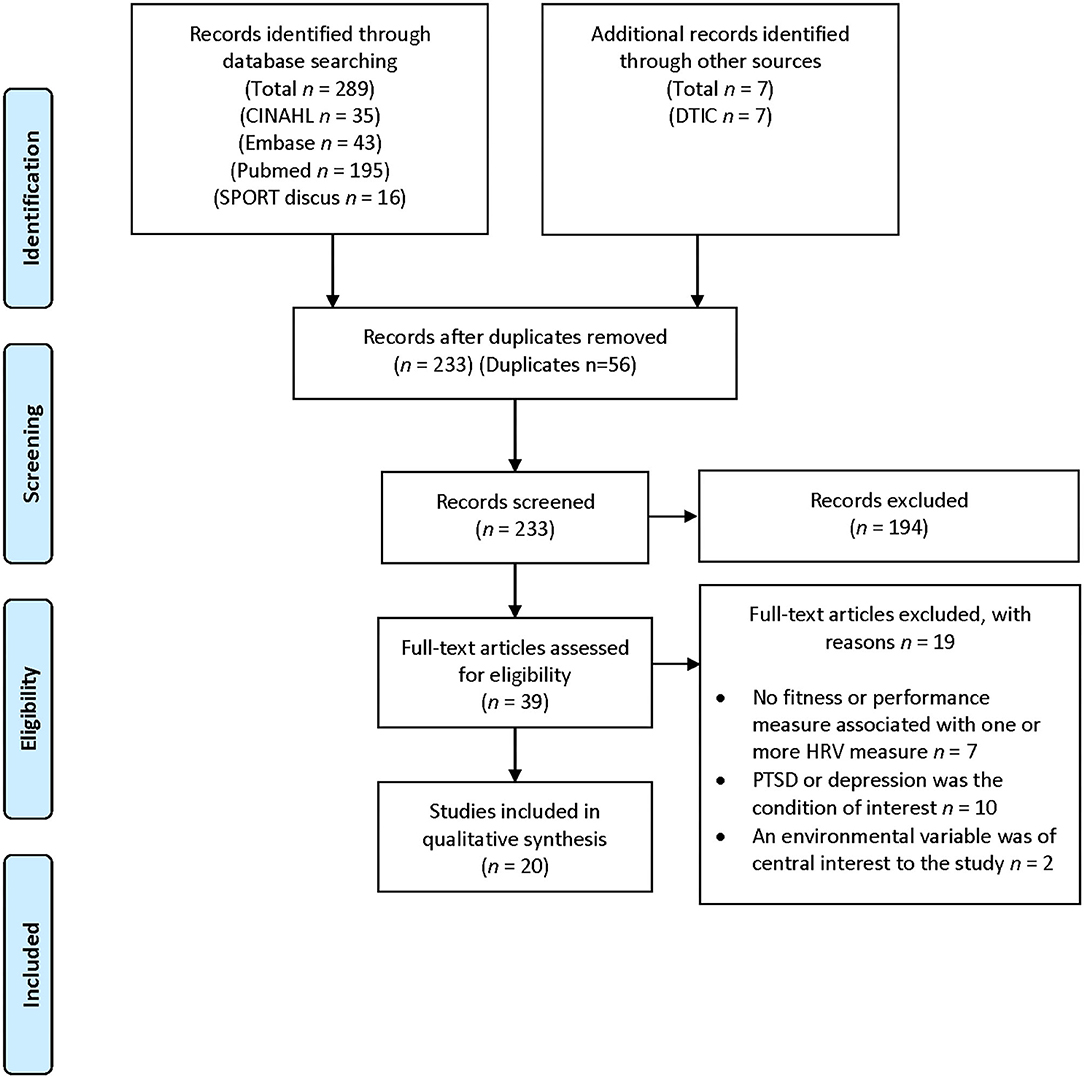
Figure 1. PRISMA flow diagram.
The PICO strategy developed to construct the organization and syntax of search terms was as follows: Patient(s); tactical personnel, and derivative, related, or more specific terms that would capture research conducted with public safety operators or trainees, Intervention; while no interventional studies were expected, given the observational nature of HRV analysis and the research aim, if studies compared HRV to another health or performance monitoring modality, results could be considered provided details of the HRV analysis were included. The control/comparison was not limited or specified; any comparison method could be included, provided the specific details of HRV monitoring were reported. For outcomes, a wide variety of health and occupational outcomes were considered, including physical fitness/injury, mental/emotional stress, or recovery, resilience or job performance.
Each database (Pubmed, CINAHL, Embase, and SportDiscus) was then sequentially searched by a single author (CT) using database heading terms, Boolean operators and available filters. A second author independently verified the search results (RO). The Defense Technical Information Center (DTIC) was also searched to capture gray literature not indexed in traditional academic databases. The DTIC was utilized as an expedient means of capturing information relevant to the research question and population of interest that was not peer-reviewed but was still likely to contribute to the aim of the study. The final search was executed and verified on 9 October 2019. Details of the finalized search strategy and initial results can be seen in Table 1. Duplicates were screened using EndNote software (Clarivate Analytics, Philadelphia, PA, USA), while additional duplicates were removed manually.
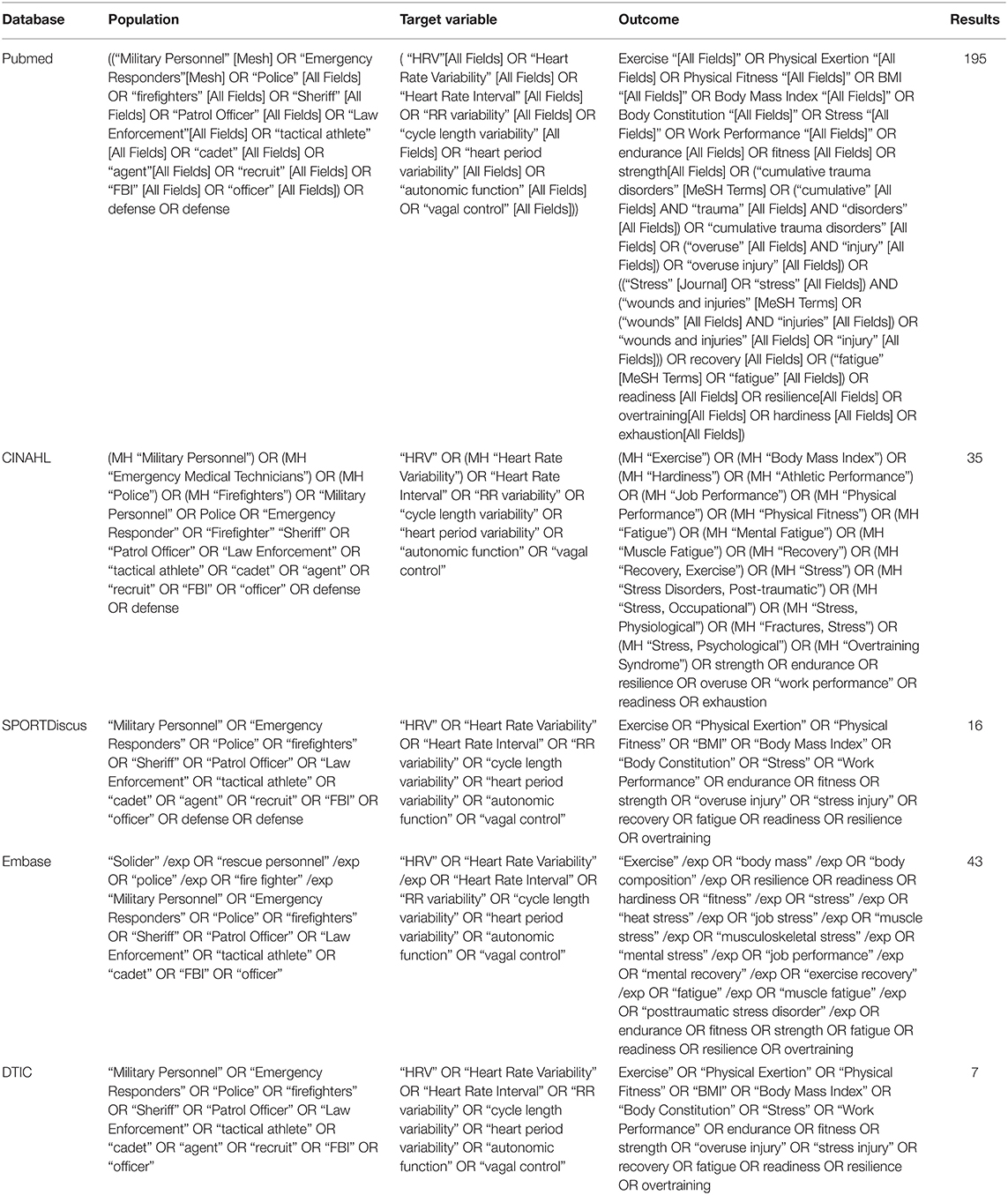
Table 1. Search strategy and initial results.
Review studies, conference proceedings and other literature that was not primary, not peer-reviewed, not available in English or had no available abstract was also rejected manually if not captured by search filters. Article titles clearly irrelevant to the topic (e.g., drug intervention studies, in vitro studies) were also removed. Articles reporting results from animal studies, a human population that did not include active or veteran tactical personnel, and studies using HRV as an intervention rather than a measurement (e.g., biofeedback device studies) were also screened out for the purposes of this review.
Developed inclusion criteria were applied to the remaining titles: tactical personnel or trainees (well or unwell), veterans, measurement of HRV, assessment of a health/fitness/occupational outcome, use of HRV analysis findings to predict, measure or monitor a state of disease, physical or occupational performance. All study design types were considered, provided that HRV analyses were reported in relation to another factor. Article relevance to the question was first screened by CT. An additional author verified inclusions and exclusions (RO). Disagreements were adjudicated by a third author, BS.
The Critical Appraisal Skills Programme (CASP) toolkit (Middle Way, Oxford, UK) (25) was selected for methodological assessment of the included studies. This assessment system has been used in previous systematic reviews and allows for fair and equitable assessment of a variety of study types (26). Three CASP checklists were ultimately necessary to evaluate the selected studies; the cohort study checklist, comprised of 13 total questions, the case-control checklist, comprised of 11 questions, and the randomized control trial checklist, also of comprised 11 questions. The randomized control trial checklist was the most suitable for quasi-experimental studies included in this review. The first two questions of each checklist screen for validity, and the following 9-11 questions guide reviewers through the assessment of study results, relevance of the results, methodology, and applicability. On the cohort study checklist, Question 7 simply asks for a summary of the results. This question was omitted, resulting in a final maximum score of 12. For each question that could be answered dichotomously, a publication was awarded with 1 point for answers of “yes” and 0 points for answers of “no” or “can't tell.” The case-control and randomized-control trial checklists required no modification beyond score quantification. For any questions which were not answered dichotomously within the checklist, an objective parameter was fit to the question. For example, on all checklists, there is a question pertaining to the precision of the results, phrased, “how precise were the results?” This question was awarded a “1” (yes) if exact measurements of significance, rather than inequalities, were reported. For other questions asking for treatment effect sizes, publications were awarded “1” point (yes) for including power or effect size analysis, and “0” points (no) if no determination was made as to the effect size. Disagreements in CASP scoring between authors were resolved by consensus. A referee (RO) was appointed prior to initiation of scoring. Screening and quality assessment were completed 2 February 2020.
The results of the search, screening, and selection processes are summarized in the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram (Figure 1). A total of 296 citations were captured in the finalized search, executed on 9 October 2019. At that time, all eligible results were downloaded, retained and screened in accordance with the screening methodology. A total of 56 duplicates were removed, leaving 233 titles. Of these, 194 were identified as irrelevant to the research question. From the remaining studies, the following exclusion criteria were developed: post-traumatic stress disorder (PTSD) or depression were the condition of interest (n = 10), an environmental condition was a key variable in the study (n = 2), HRV was measured, but not linked to a health and fitness or occupational outcome (n = 7). The remaining 20 publications were retained for this review. Further screening for quantitative review was considered, but ultimately not possible due to the heterogeneity of the included studies. The review was completed on 14 March 2020.
The mean CASP of the quasi-experimental studies was 9.67 ± 0.58 of 11 maximum points. The mean CASP of the case-control studies was 10.5 ± 0.7 of 11 maximum points, and the mean CASP of the cohort studies was 10.73 ± 0.78 of 12 maximum points.
Details of all relevant data retrieved from each included study can be found in Table 2. The Author(s), title, year, participants, demographics as available, anthropometrics as available, the performance metric(s) and key results, significant or not, as well as the final CASP score are included. The HRV analysis or analyses selected and their results are also included if succinct summarizations of the data were possible. Studies are organized first by design methodology, then alphabetically.
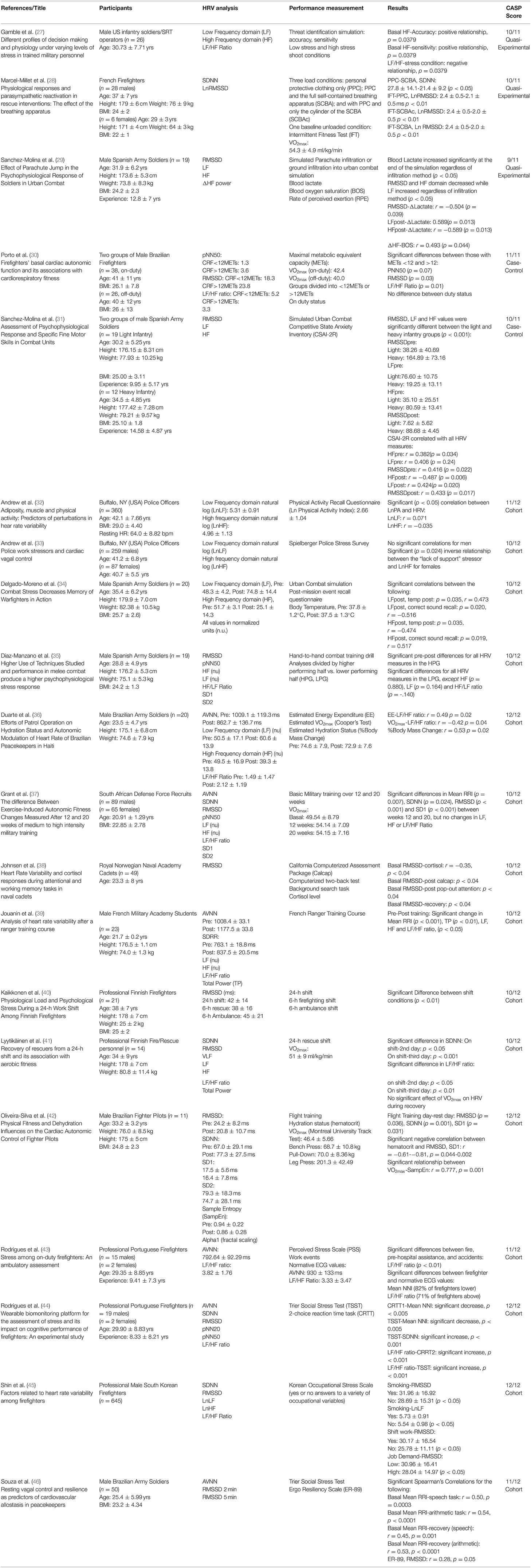
Table 2. Data extraction and summary of selected studies.
Three study design methodologies were utilized in the selected studies. Quasi-experimental studies (27–29) and case-control studies (30, 31) represented a total of four included studies. All other studies were of a cohort design. The follow-up period for the cohort studies varied from single instances of data collection activity, such as administration of a questionnaire and a single ECG trace, to as long as 20 weeks of follow-up in one study (37).
Selected publications included males only in 11 studies, both males and females in seven studies and the gender distribution was not reported in three studies. Seven tactical subpopulations were represented; general law enforcement officers (32, 33), Army (27, 29, 31, 34–36, 46), Defense Force trainees (37), Naval cadets (38), Army Ranger trainees (39) firefighters/rescue personnel (28, 30, 40, 41, 43, 45), and Air Force fighter pilots (42). Specifically, the Army personnel were members of either the US, Brazilian or Spanish militaries. For the Fire/Rescue personnel, members were serving in French, Brazilian, Finnish, Portuguese, or South Korean communities. A total of nine countries were represented: USA (27, 32, 33), Spain (29, 31, 34, 35), Brazil (30, 36, 42, 46), South Africa (37), Norway (38), France (28, 39), Finland (40, 41), Portugal (43, 44), and South Korea (45).
Analytical methods vary widely in their mathematical approach and provide different information on different autonomic processes. Table 3 describes the HRV analysis methods discussed in this review and provides an expansion of each acronym, a brief explanation of the measurement, and its clinical implications.
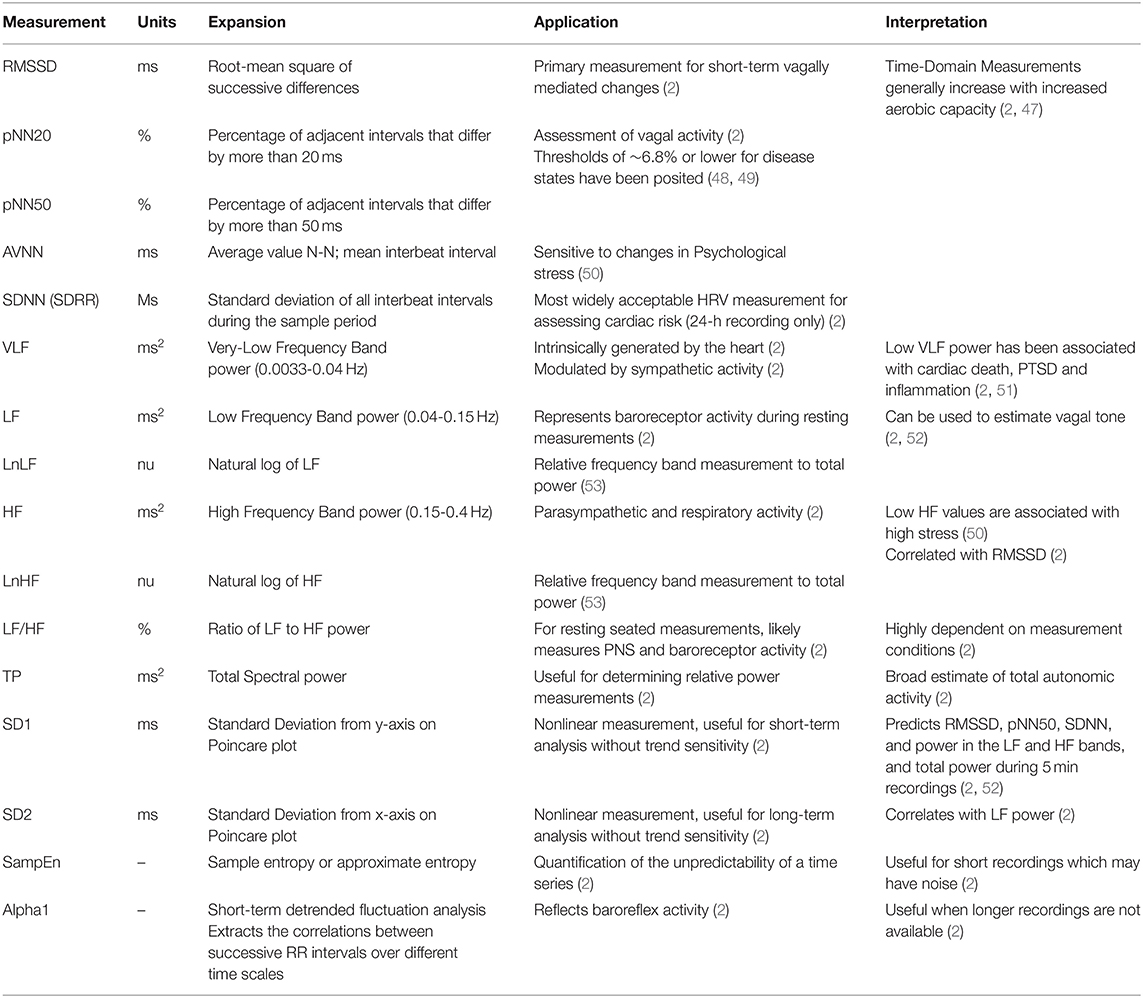
Table 3. Expansion and definition of HRV measurement acronyms.
The low-frequency band (LF) and high frequency band (HF) spectral power were the most popular analytical methods, with 18 studies documenting these HRV characteristics. Other spectral analyses included LF/HF ratio (27, 30, 36, 37, 39, 41, 44, 45, 54), total power (TP) (39), and the very-low frequency band (VLF) (41). The nonlinear analyses included alpha1 (α1), a measure of signal self-similarity (42), sample entropy (SampEn) (42), SD1, and SD2 (35, 37, 42).
The root-mean square of successive differences (RMSSD) was the most popular time-domain analysis, with 11 studies documenting this HRV characteristic. Other time-domain analyses included pNN20 (54), pNN50 (30, 35, 37, 54), mean interbeat interval, or AVNN (36, 37, 39, 43, 46, 54), or SDNN/SDRR (28, 37, 39, 41, 42, 45, 54).
A total of four studies examined the relationship between one or more HRV metrics and aerobic fitness (VO2max) (30, 36, 41, 42). Three of the four were cohort study designs (36, 41, 42), and one was quasi-experimental (30). Three (30, 42), including the experimental study (36), found significant relationships between one or more HRV values and aerobic fitness, and one did not (41). The study finding no significant relationship examined only the LF/HF ratio and SDNN HRV indices. Of the studies reporting significant relationships, LF/HF ratio (36, 41), sample entropy, PNN50, and RMSSD were examined. The pooled mean VO2max across all four studies was 45.4 ± 6.2 ml/kg/min, with the lowest VO2max in the cohort of off-duty male Brazilian firefighters (40.0 ml/kg/min) (30) and the highest in the cohort of male Brazilian peacekeepers (52.9 ml/kg/min) (36).
Two studies (32, 42) examined fitness variables that were not estimates of aerobic capacity. One recorded one-rep maximum strength measurements from Brazilian fighter pilots (bench press, pull-down and leg press) and found no significant relationships between HRV indices measured on a rest day or on a flight training day and those strength tests. The other study (32) found a significant correlation between self-reported physical activity levels and the LF and HF signal strengths.
Six studies utilized a simulated combat scenario for participant testing (27, 29, 31, 34, 35) or observed an actual tactical engagement (36). Of these studies, all found significant pre-event to post-event changes in HRV. Specifically, one study (35) comparing differences between high-performing and lower-performing soldiers in hand-to-hand combat training drills found significant time-domain differences (RMSSD, PNN50, SD1, SD2) between groups, but no differences in spectral-domain analyses. In the other studies, spectral analyses correlated with weapon accuracy and threat discrimination sensitivity (27), estimated energy expenditure, and hydration status as measured by percentage of body weight change of the course of the observation period (36). One study in this category compared a light infantry unit to a heavy unit in a simulated ground combat scenario (31). The light infantry unit, acclimated to such events and training, showed significantly different spectral responses when compared against the heavy infantry unit.
Three studies included a measurement of cognitive performance (34, 38, 43). Of these three, one found significant correlations between sound recall and the LF domain following a combat simulation (see section above) (34). One found significant relationships between greater basal RMSSD and two computerized cognitive stress tests, as well as during recovery from those tasks (38). The last study found a significant decrease in AVNN at the start of a two-choice critical reaction time task and a significant change in LF/HF ratio following the task (43).
Three studies (33, 45, 46) measured occupational stress directly through surveys or through a tactically relevant evaluation tool. Andrew et al. (55) found an inverse correlation between lnLF and the “lack of support” stressor; meaning that greater lack of support correlated with less vagal control as measured by LF power. Shin (45), in a sample of 645 professional South Korean firefighters, found significantly reduced RMSSD values in those that reported smoking, reported “high” vs. “low” job demand, and those that reported shift work. Significantly higher lnLF values were also reported in smokers. Souza et al. (46) measured trait resilience in a cohort of Brazilian Army soldiers using the ER-89 scale and found a correlation between trait resilience and RMSSD.
Three studies assessed cohorts of fire and rescue personnel working 24-h shifts (40, 41, 43). Kaikkonen et al. (40) found a significant difference in RMSSD between the 6-h firefighting and 6-h ambulance phases of professional Finnish firefighters' shifts, with the rescue phase of the shift resulting in a decrease of RMSSD. Lyytikäinen et al. (41), previously mentioned above, examined HRV changes during the recovery days following a 24-h shift. They found significant differences in the SDNN and LF/HF ratio from days 2 to 3 of recovery. Rodrigues et al. (44) found significant differences in LF/HF ratio during a variety of fire and rescue tasks. Specifically, the LF/HF ratio increased most during response to accidents. They also compared their mean N-N interval data to normative healthy adult data and found the rescue personnel lower AVNN values for rescuers, as well as higher LF/HF values.
Two studies (37, 39) followed participants through a period of tactical training. One (39) measured differences in AVNN, TP, LF, HF, and LF/HF ratio between the start and end of French Ranger training. They found significant changes in all measured values. Grant et al. (37) assessed the differences in aerobic capacity and HRV values at one 12 and 20 weeks during South African Defense Force initial entry training. They found that while the mean AVNN, SDNN, and RMSSD continued to improve between 12 and 20 weeks, the LF/HF ratio was not significantly different over the same time period (37).
The aim of this review was to identify primary studies examining relationships between HRV and relevant health, fitness and operational outcomes in tactical personnel, critically appraise the methodological quality of the identified studies, and summarize the results. The quality of the 20 included studies was generally high and included a variety of observational and quasi-experimental designs over a wide range of follow-up periods. While observational research was necessary for the aims of most studies, and variations in study designs and research questions covered a variety of topic in which single instance recordings were appropriate, few of the studies included in this review were longitudinal, and larger, more comprehensive datasets describing the HRV characteristics of tactical personnel in a variety occupational fields and settings would be beneficial. Further, the CASP checklists do not account for sample sizes, which were generally small, with a few notable exceptions, so while the methodology of the included studies may have been sound, caution must be taken when interpreting the results. Qualitatively, however, the studies included in this review generally agreed, and did indicate that HRV is an effective tool for measuring psychophysiological stress across professional environments and often correlates effectively with a wide variety of outcomes of interest. The included studies indicate that HRV measurements can be effectively applied across a wide variety of tactical settings.
Of the four studies investigating the relationships between HRV measures and aerobic fitness, only one found no significant association, and the mean VO2max of 51 ml/kg/min was higher than all but one of the other studies. This could suggest a ceiling effect, indicating that aerobic fitness above a certain capacity within a certain profession lends no additional benefits to recovery, but all considered studies used an indirect, estimated method to determine VO2max. Additionally, a variety of HRV analysis methods were used, and while frequency domain values did not trend significantly with physical fitness in all studies, the study by Oliveira-Silva et al. examining the cohort with the highest aerobic capacity did find a significant relationship when examining sample entropy (42), suggesting that non-linear methods may be the most suitable method for these study designs.
Further research in this area might focus on directly measuring aerobic capacity of the cohort, and conducting similar research investigating VO2max, HRV and recovery in different tactical professionals. Larger sample sizes may also clarify these emerging relationships. So far, only one study has examined any measurements of strength, and no measures of power have been linked to HRV indices. While no significant associations were found in a cohort of fighter pilots, it may be possible that fitness within the strength and power domains contributes to individual perception and response to stress, as well as recovery from stressful exposures in other tactical settings.
All six studies measuring HRV during simulated or actual combat situations found significant changes. While not unexpected, these results nonetheless provide a foundation on which organizations can begin to consider implementing additional psychophysiological monitoring of personnel to assist in training and deployment decisions. While these studies achieved high levels of external validity, by exposing personnel to rigorously designed and realistic simulations, questions remain as to which factors within these scenarios most significantly affected the HRV indices of operators, and therefore, which components require further validation or incorporation into regular training. For example, it is possible that load carriage, a common task for tactical personnel, may influence chest biomechanics and perceived stress, independently altering HRV. Previous research has indeed demonstrated that even experienced tactical personnel report increased exertion when carrying a load, even if physiological measures, such as estimated energy expenditure, do not significantly change (56). Spectral and time domain analyses of HRV may be able to quantify and explain these anomalies. Furthermore, while one study has conducted a threat identification scenario, live firearms were not used, and further research into the specific effect of live firearms operation on HRV may be necessary, and may provide additional information on underlying mechanisms that contribute to the effectiveness of deliberate HRV modulation as an intervention for improving tactical decision making (57). For field measurements and analyses of HRV in these scenarios and similar scenarios, selecting more robust analyses, such as nonlinear and fractal-scaling methods may again be the most suitable.
Making decisions under pressure and other cognitive work is critical to the success of many tactical operations, and a key skill for ensuring operator and public safety. While the studies examining cognitive stress and HRV values are limited to only three, which represented the military and firefighting professions, the results are promising. The value for organizations may come primarily from the ability of HRV to discriminate and quantify the severity of responses to cognitive demands without relying solely on subjective feedback. The results from one study in particular by Delgado-Moreno et al., which assessed recall capability and spectral HRV analysis (34), may demonstrate that personnel who adapt to stressful stimuli struggle less with higher-order tasks. This type of analysis and its integration into training, especially in law enforcement, may be beneficial for improving decision-making training and promoting improved public safety.
The study by Shin et al. (45) was the largest cohort studied by a considerable margin, with a total of 645 participants. The Korean Occupational Stress Scale, while a subjective tool, is a widely utilized measurement of occupational stress and was used as the primary instrument (58). They found that the organization system and occupational climate were correlated with lnHF changes. Time-domain changes were also found in firefighters that reported high job stress. This agrees with another large cohort of manual laborers in Korea and suggests that organizational structures and employee support can have significant changes in the allostatic load of personnel (59). Although the study by Shin et al. did not account for physical activity outside the workplace, the study by Kang et al. did, and determined that social support was an independent risk factor for adverse HRV changes. Therefore, it cannot be assumed that improvements in physical conditioning will be able to fully counteract the potential negative effects of job stress induced by organizational, job support or occupational climate concerns. As such, tactical organizations may benefit from monitoring not only external occupational stressors and hazards but may potentially benefit from assessing the effects of internal organizational and support impacts. Further research accounting for physical conditioning in tactical personnel, and enhanced qualitative methods assessing occupational organization, support, and climate may clarify some of the unique causal relationships between organization-induced occupational stress and allostatic load in tactical operations.
Likewise, in the study by Andrew considering police work stressors and cardiac autonomic balance, a significant association between a lack of organizational support and frequency-domain changes in HRV was found, but for female officers only (33). The authors concluded that chronic insufficient organizational support may lead to a loss of the cardioprotective effect females typically experience as a result of greater vagal control compared to men. Their results were consistent with another study that found relationships between organizational occupational stress and metabolic disorder in women, but not men (60). Given that females will typically form a minority within a tactical organization, specific regard to their occupational support may be especially necessary to support their health and effectiveness. One solution Andrew and his colleagues offer is for police organizations to provide for support coping opportunities, a method of stress coping more typically adopted by females. Further research may investigate the effect of occupational organization, support methods and climate with specific regard to female operators or trainees to determine optimal strategies for maximizing their performance.
While shift work is endemic to many tactical organizations, the studies in this review represented exclusively fire and rescue personnel, and the results indicated that the autonomic impacts of shift work in tactical personnel may manifest differently than in other populations. For example, two separate studies in two very different geographical locations (Finland and Portugal), both found that fire and rescue personnel who were assigned to rescue duties, which included motor vehicle accident response, experienced significantly greater HRV changes than when they worked regular fire suppression duties (40, 43). Research in healthcare workers found limited differences between physicians and nurses who worked rotating shifts and those who worked day shifts only (61), indicating that research considering longer-term HRV measurements, such as the VLF component of the frequency-domain and the nonlinear SD2, may require careful interpretation in tactical settings.
Other work in this area to aimed at using HRV indices to measure physiological strain, which may then be used when determining work/rest cycles and other scheduling concerns. Time-domain analyses were the most common across these studies, but spectral analyses were also represented and were significant. While no significant associations were found between VO2max and shift recovery (discussed above), it should be noted that the autonomic effects of shift work lasted up to three days (41). Given that males may be more susceptible to adverse HRV changes induced by circadian rhythm disruptions (62), and that males comprise the majority of most tactical organizations, the effects of shift work on autonomic regulation should be investigated further in a wide variety of tactical operations to develop stronger evidence to guide policy decisions. Further studies or reanalysis efforts may also aim to apply novel indices, such as sample entropy or other signal-self similarity assessments to strengthen the relationships between HRV measurement, physiological strain and operator deployment decisions. Given the differences in HRV responses to different duties even within a single unit, other populations that rely on rotating shifts, such as law enforcement and military organizations should also be considered separately to determine the unique influences present between professions and how to proceed with long-term HRV measurement interpretations.
Two studies followed trainees through a period of accession training, one a Ranger training course in France, and the other basic military training in South Africa. Both found that tactical training results in HRV changes across both time and spectral domains, and one was specifically using HRV to assess for the presence of overtraining syndrome (OTS) between the 12th and 20th week of training (37), as OTS is known to contribute to injury risk (63). A link between HRV and chronic musculoskeletal injury has been proposed in endurance athletes (13), and if proven effective, tactical organizations may be able to screen and triage trainees before clinical symptoms develop, reducing the burden of injury during training. One recent study in Crossfit™ athletes found significant associations when investigating the relationships between workload and HRV in the time domain (64). Given the similarities between Crossfit™ and tactical conditioning activities (14), this association may prove especially valuable for tactical training programs and warrants further investigation in larger cohorts of tactical personnel. As previously stated, more robust HRV analytical methods may also be beneficial for inclusion in further studies.
The measurement and application of HRV indices to monitor psychological, physiological and more specifically, autonomic stress, encountered by the tactical operator continues to be developed and has made significant strides over the past decade in terms of utilization by a wide range of organizations, comparison to normative populations and quantification of the stress of tactical work. While strong evidence is still emerging, based on the quality and general agreement of studies included in this review, HRV monitoring appears to provide valuable insight into the psychophysiological responses of tactical personnel during occupationally relevant activities and recovery from those activities. However, substantial further research is still necessary. Specifically, the recruitment of larger cohorts and the collection of normative data specific to healthy tactical personnel should enhance result interpretation. Additionally, further isolation and analysis of specific variables relevant to the end user, such as the independent effects of load carriage, may help determine causal relationships, strengthen the reliability of applications and ultimately provide personnel with an additional tool to maximize health and performance. Finally, HRV may prove to be highly effective for mitigation of chronic musculoskeletal injury in tactical operators and trainees as a screening tool, but such associations require further exploration, in terms of both cohort selection and recruitment and HRV analysis method(s).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
CT and RO: conceptualization, methodology, and writing—original draft preparation. CT: software, formal analysis, investigation, writing—review and editing, and supervision. RO and BS: resources, data curation, visualization, project administration, and validation. All authors have read, reviewed, and approved the current manuscript for submission.
This research was funded in part through a Ph.D. scholarship provided for the lead author. No other funding or grant from any agency in the public, commercial or not-for-profit sectors was provided or obtained.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank the editorial and review personnel for their efforts, and all first responders protecting our communities throughout the world.
1. Saper CB. The central autonomic nervous system: conscious visceral perception and autonomic pattern generation. Ann Rev Neurosci. (2002) 25:433–69. doi: 10.1146/annurev.neuro.25.032502.111311
2. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. (2017) 5:258. doi: 10.3389/fpubh.2017.00258
3. Grossman P, Taylor EW. Toward understanding respiratory sinus arrhythmia: relations to cardiac vagal tone, evolution and biobehavioral functions. Biol Psychol. (2007) 74:263–85. doi: 10.1016/j.biopsycho.2005.11.014
4. Mancia G, Bousquet P, Elghozi JL, Esler M, Grassi G, Julius S, et al. The sympathetic nervous system and the metabolic syndrome. J Hypert. (2007) 25:909–20. doi: 10.1097/HJH.0b013e328048d004
5. Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol. (2010) 141:122–31. doi: 10.1016/j.ijcard.2009.09.543
6. McEwen BS, Wingfield JC. The concept of allostasis in biology and biomedicine. Horm Behav. (2003) 43:2–15. doi: 10.1016/S0018-506X(02)00024-7
7. Conder RL, Conder AA. Heart rate variability interventions for concussion and rehabilitation. Front Psychol. (2014) 5:890. doi: 10.3389/fpsyg.2014.00890
8. Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. (2003) 33:889–919. doi: 10.2165/00007256-200333120-00003
9. Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. (2014) 44:139–47. doi: 10.1007/s40279-014-0253-z
10. Bigger JT, Fleiss JL, Rolnitzky LM, Steinman RC. The ability of several short-term measures of rR variability to predict mortality after myocardial infarction. Circulation. (1993) 88:927–34. doi: 10.1161/01.CIR.88.3.927
11. Bellenger CR, Fuller JT, Thomson RL, Davison K, Robertson EY, Buckley JD. Monitoring athletic training status through autonomic heart rate regulation: a Systematic review and meta-Analysis. Sports Med. (2016) 46:1461–86. doi: 10.1007/s40279-016-0484-2
12. Smolander J, Juuti T, Kinnunen M-L, Laine K, Louhevaara V, Männikkö K, et al. A new heart rate variability-based method for the estimation of oxygen consumption without individual laboratory calibration: application example on postal workers. Appl Ergon. (2008) 39:325–31. doi: 10.1016/j.apergo.2007.09.001
13. Gisselman AS, Baxter GD, Wright A, Hegedus E, Tumilty S. Musculoskeletal overuse injuries and heart rate variability: is there a link? Med Hypotheses. (2016) 87:1–7. doi: 10.1016/j.mehy.2015.12.003
14. Haddock CK, Poston WSC, Heinrich KM, Jahnke SA, Jitnarin N. The benefits of high-Intensity functional training fitness programs for military personnel. Military medicine. (2016) 181:e1508–e14. doi: 10.7205/MILMED-D-15-00503
15. Scofield DE, Kardouni JR. The tactical athlete: a Product of 21st century strength and conditioning. Strength Cond J. (2015) 37:2–7. doi: 10.1519/SSC.0000000000000149
16. Orr R, Pope R, Peterson S, Hinton B, Stierli M. Leg power as an indicator of risk of injury or illness in police recruits. Int J Environ Res Public Health. (2016) 13:237. doi: 10.3390/ijerph13020237
17. Zefferino R, L'Abbate N, Facciorusso A, Potenza A, Lasalvia M, Nuzzaco A, et al. [Assessment of heart rate variability (HRV) as a stress index in an emergency team of urban police]. G Ital Med Lav Ergon. (2003) 25 Suppl(3):167–9.
18. Ramey SL, Perkhounkova Y, Hein M, Bohr NL, Anderson AA. Testing a resilience training program in police recruits: a Pilot study. Biol Res Nurs. (2017) 19:440–9. doi: 10.1177/1099800417699879
19. Kline A, Falca-Dodson M, Sussner B, Ciccone DS, Chandler H, Callahan L, et al. Effects of repeated deployment to iraq and afghanistan on the health of new jersey army national guard troops: implications for military readiness. Am J Public Health. (2010) 100:276–83. doi: 10.2105/AJPH.2009.162925
20. Seelig AD, Jacobson IG, Smith B, Hooper TI, Boyko EJ, Gackstetter GD, et al. Sleep patterns before, during, and after deployment to iraq and afghanistan. Sleep. (2010) 33:1615–22. doi: 10.1093/sleep/33.12.1615
21. Yang J, Farioli A, Korre M, Kales SN. Dietary preferences and nutritional information needs among career firefighters in the United States. Glob Adv Health Med. (2015) 4:16–23. doi: 10.7453/gahmj.2015.050
22. Zimmerman FH. Cardiovascular disease and risk factors in law enforcement personnel: a comprehensive review. Cardiol Rev. (2012) 20:159–66. doi: 10.1097/CRD.0b013e318248d631
23. Schwartz MD. SMART (Sports Medicine and Rehabilitation Team) Centers: An Empirical Analysis. Pendleton CA: Naval Hospital Camp (2007). doi: 10.21236/ADA477206
24. Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
25. Critical Appraisal Skills Programme. CASP Checklists. (2019). Available online at: casp-uk.net/casp-tools-checklists/
26. Kanavaki AM, Rushton A, Klocke R, Abhishek A, Duda JL. Barriers and facilitators to physical activity in people with hip or knee osteoarthritis: protocol for a systematic review of qualitative evidence. BMJ Open. (2016) 6:e012049. doi: 10.1136/bmjopen-2016-012049
27. Gamble KR, Vettel JM, Patton DJ, Eddy MD, Caroline Davis F, Garcia JO, et al. Different profiles of decision making and physiology under varying levels of stress in trained military personnel. Int J Psychophysiol. (2018) 131:73–80. doi: 10.1016/j.ijpsycho.2018.03.017
28. Marcel-Millet P, Ravier G, Grospretre S, Gimenez P, Freidig S, Groslambert A. Physiological responses and parasympathetic reactivation in rescue interventions: the effect of the breathing apparatus. Scand J of Med Sci Sports. (2018) 28:2710–22. doi: 10.1111/sms.13291
29. Sanchez-Molina J, Robles-Perez JJ, Clemente-Suarez VJ. Effect of parachute jump in the psychophysiological response of soldiers in urban combat. J Med Syst. (2017) 41:99. doi: 10.1007/s10916-017-0749-9
30. Porto LGG, Schmidt ACB, de Souza JM, Nogueira RM, Fontana KE, Molina GE, et al. Firefighters' basal cardiac autonomic function and its associations with cardiorespiratory fitness. Work. (2019) 62:485–95. doi: 10.3233/WOR-192883
31. Sanchez-Molina J, Robles-Perez JJ, Clemente-Suarez VJ. Assessment of psychophysiological response and specific fine motor skills in combat units. J Med Syst. (2018) 42:67. doi: 10.1007/s10916-018-0922-9
32. Andrew ME, Shengqiao L, Wactawski-Wende J, Dorn JP, Mnatsakanova A, Charles LE, et al. Adiposity, muscle, and physical activity: predictors of perturbations in heart rate variability. Am J Hum Biol. (2013) 25:370–7. doi: 10.1002/ajhb.22379
33. Andrew ME, Violanti JM, Gu JK, Fekedulegn D, Li S, Hartley TA, et al. Police work stressors and cardiac vagal control. Am J Hum Biol. (2017) 29. doi: 10.1002/ajhb.22996
34. Delgado-Moreno R, Robles-Pérez J, Clemente-Suárez V. Combat stress decreases memory of warfighters in action. J Med Syst. (2017) 41:1–7. doi: 10.1007/s10916-017-0772-x
35. Diaz-Manzano M, Fuentes JP, Fernandez-Lucas J, Aznar-Lain S, Clemente-Suárez VJ. Higher use of techniques studied and performance in melee combat produce a higher psychophysiological stress response. Stress Health. (2018) 34:622–8. doi: 10.1002/smi.2829
36. Duarte AFA, Morgado JJM. Effects of patrol operation on hydration status and autonomic modulation of heart rate of brazilian peacekeepers in haiti. J Strength Cond Res. (2015) 2015:S82-S7. doi: 10.1519/JSC.0000000000001065
37. Grant CC, Mongwe L, Janse van Rensburg DC, Fletcher L, Wood PS, Terblanche E, et al. The difference between exercise-Induced autonomic and fitness changes measured after 12 and 20 weeks of medium-to-High intensity military training. J Strength Cond Res. (2016) 30:2453–9. doi: 10.1519/JSC.0b013e3182a1fe46
38. Johnsen BH, Hansen AL, Murison R, Eid J, Thayer JF. Heart rate variability and cortisol responses during attentional and working memory tasks in naval cadets. Int Marit Health. (2012) 63:181–7.
39. Jouanin J, Dussault C, Pérès M, Satabin P, Piérard C, Guézennec CY, et al. Analysis of heart rate variability after a ranger training course. Mil Med. (2004) 169:583–7. doi: 10.7205/MILMED.169.8.583
40. Kaikkonen P, Lindholm H, Lusa S. Physiological load and psychological stress during a 24-hour work shift among finnish firefighters. J Occup Environ Med. (2017) 59:41–6. doi: 10.1097/JOM.0000000000000912
41. LyytikÄInen K, Toivonen L, Hynynen ESA, Lindholm H, KyrÖLÄInen H, Lyytikäinen K, et al. Recovery of rescuers from a 24-h shift and its association with aerobic fitness. Int J Occup Med Environ Health. (2017) 30:433–44. doi: 10.13075/ijomeh.1896.00720
42. Oliveira-Silva I, Boullosa DA. Physical fitness, and dehydration influences on the cardiac autonomic control of fighter pilots. Aerosp Med Hum Perform. (2015) 86:875–80. doi: 10.3357/AMHP.4296.2015
43. Rodrigues S, Paiva JS, Dias D, Cunha JPS. Stress among on-duty firefighters: an ambulatory assessment study. PeerJ. (2018) 2018:12. doi: 10.7717/peerj.5967
44. Rodrigues S, Paiva JS, Dias D, Pimentel G, Kaiseler M, Cunha JPS. Wearable biomonitoring platform for the assessment of stress and its impact on cognitive performance of firefighters: an experimental study. Clin Pract Epidemiol Mental Health. (2018) 14:250–62. doi: 10.2174/1745017901814010250
45. Shin JH, Lee JY, Yang SH, Lee MY, Chung IS. Factors related to heart rate variability among firefighters. Ann Occup Environ Med. (2016) 28:6. doi: 10.1186/s40557-016-0111-6
46. Souza GG, Magalhaes LN, Cruz TA, Mendonca-De-Souza AC, Duarte AF, Fischer NL, et al. Resting vagal control and resilience as predictors of cardiovascular allostasis in peacekeepers. Stress. (2013) 16:377–83. doi: 10.3109/10253890.2013.767326
47. Singh N, Moneghetti KJ, Christle JW, Hadley D, Froelicher V, Plews D. Heart rate variability: an old metric with new meaning in the era of using mhealth technologies for health and exercise training guidance. Part two: prognosis and training. Arrhyth Electrophysiol Rev. (2018) 7:247. doi: 10.15420/aer.2018.30.2
48. Chakko S, Mulingtapang RF, Huikuri HV, Kessler KM, Materson BJ, Myerburg RJ. Alterations in heart rate variability and its circadian rhythm in hypertensive patients with left ventricular hypertrophy free of coronary artery disease. Am Heart J. (1993) 126:1364–72. doi: 10.1016/0002-8703(93)90535-H
49. Mietus JE, Peng CK, Henry I, Goldsmith RL, Goldberger AL. The pNNx files: re-examining a widely used heart rate variability measure. Heart. (2002) 88:378–80. doi: 10.1136/heart.88.4.378
50. Montano N, Porta A, Cogliati C, Costantino G, Tobaldini E, Casali KR, et al. Heart rate variability explored in the frequency domain: a tool to investigate the link between heart and behavior. Neurosci Biobehav Rev. (2009) 33:71–80. doi: 10.1016/j.neubiorev.2008.07.006
51. Shah AJ, Lampert R, Goldberg J, Veledar E, Bremner JD, Vaccarino V. Posttraumatic stress disorder and impaired autonomic modulation in male twins. Biol Psychiatry. (2013) 73:1103–10. doi: 10.1016/j.biopsych.2013.01.019
52. Voss A, Schroeder R, Heitmann A, Peters A, Perz S. Short-term heart rate variability-influence of gender and age in healthy subjects. PLoS ONE. (2015) 10:e118308. doi: 10.1371/journal.pone.0118308
53. Kuusela T. Methodological aspects of heart rate variability analysis. Heart rate variability (HRV) signal analysis. Clin Applic. (2013) 2013:9–42. doi: 10.1201/b12756-4
54. Rodrigues S, Dias D, Paiva JS, Cunha JPS. Psychophysiological stress assessment among on-duty firefighters. Conf Proc IEEE Eng Med Biol Soc. (2018) 2018:4335–8. doi: 10.1109/EMBC.2018.8513250
55. Andrew M, Miller D, Gu J, Li S, Charles L, Violanti J, et al. Exposure to police work stressors and dysregulation of the stress response system: the buffalo cardio-metabolic occupational police stress study. Epidemiology. (2012) 23:S202. doi: 10.1097/01.ede.0000416802.85566.d3
56. Tomes C, Orr RM, Pope R. The impact of body armor on physical performance of law enforcement personnel: a systematic review. Ann Occup Environ Med. (2017) 29:14. doi: 10.1186/s40557-017-0169-9
57. Andersen JP, Di Nota PM, Beston B, Boychuk EC, Gustafsberg H, Poplawski S, et al. Reducing lethal force errors by modulating police physiology. J Occup Environ Med. (2018) 60:867–74. doi: 10.1097/JOM.0000000000001401
58. Chang SJ, Koh SB, Kang D, Kim SA, Kang MG, Lee CG, et al. Developing an occupational stress scale for korean employees. Korean J Occup Environ Med. (2005) 17:297–317. doi: 10.35371/kjoem.2005.17.4.297
59. Kang D, Kim Y, Kim J, Hwang Y, Cho B, Hong T, et al. Effects of high occupational physical activity, aging, and exercise on heart rate variability among male workers. Ann Occup Environ Med. (2015) 27:22. doi: 10.1186/s40557-015-0073-0
60. Hartley TA, Burchfiel CM, Fekedulegn D, Andrew ME, Knox SS, Violanti JM. Associations between police officer stress and the metabolic syndrome. Int J Emerg Mental Health. (2011) 13:243. doi: 10.1155/2012/861219
61. Lecca LI, Setzu D, Del Rio A, Campagna M, Cocco P, Meloni M. Indexes of cardiac autonomic profile detected with short term holter ECG in health care shift workers: a cross sectional study. La Medicina del Lavoro. (2019) 110:437–45. doi: 10.23749/mdl.v110i6.8048
62. Hulsegge G, Gupta N, Proper KI, van Lobenstein N, IJzelenberg W, Hallman DM, et al. Shift work is associated with reduced heart rate variability among men but not women. Int J Cardiol. (2018) 258:109–14. doi: 10.1016/j.ijcard.2018.01.089
63. Andersen KA, Grimshaw PN, Kelso RM, Bentley DJ. Musculoskeletal lower limb injury risk in army populations. Sports Med. (2016) 2:22. doi: 10.1186/s40798-016-0046-z
Keywords: injury prevention and reduction, occupational stress and mental-physical health, physiological monitoring data, military, police, firefighting, first responder, occupational fitness
Citation: Tomes C, Schram B and Orr R (2020) Relationships Between Heart Rate Variability, Occupational Performance, and Fitness for Tactical Personnel: A Systematic Review. Front. Public Health 8:583336. doi: 10.3389/fpubh.2020.583336
Received: 14 July 2020; Accepted: 12 October 2020;
Published: 09 November 2020.
Edited by:
Paolo Melillo, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Nicola Mucci, University of Florence, ItalyCopyright © 2020 Tomes, Schram and Orr. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Colin Tomes, Y29saW4udG9tZXNAc3R1ZGVudC5ib25kLmVkdS5hdQ==
†ORCID: Ben Schram orcid.org/0000-0002-1865-0488
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.