 Taja Francis
Taja Francis Helen Baker-Henningham
Helen Baker-Henningham- 1Caribbean Institute for Health Research, University of the West Indies, Kingston, Jamaica
- 2School of Psychology, Bangor University, Bangor, United Kingdom
This paper describes the development of the Irie Homes Toolbox, a violence prevention program targeting parents of children aged two to six years. The intervention was designed to complement an existing, teacher-training, violence prevention program, the Irie Classroom Toolbox, thus promoting an integrated approach across home and school settings. The Irie Homes Toolbox was developed through a four-stage process by integrating data from theory, formative research, and practice to ensure the intervention is acceptable, feasible, relevant, and effective in the context. The perspectives of Jamaican preschool teachers and parents of preschool children, who are the end users, were integrated into the design of the intervention throughout the development process. Stage one involved integrating theory and formative research to inform the initial intervention design. Stages two and three involved iterative cycles of design, implementation and evaluation of the intervention content, process of delivery, structure and materials. Stage four involved a further cycle of learning through a process evaluation conducted as part of a cluster-randomized controlled trial. Data from each of these four stages was used to inform the design and ongoing revisions of the toolbox with the aim of developing a low-cost, scalable and sustainable intervention for the Jamaican context. The resulting program is theory-informed and uses empirically derived content and behavior change principles operationalized for the context in which it will be delivered. The Irie Homes Toolbox is suitable for integration into the existing preschool provision in Jamaica, thus utilizing an existing service and existing staff and increasing the likelihood for wide-scale dissemination.
Introduction
Globally, violence against children exists in almost all countries with the violence often being committed by caregivers (1). This violence is mainly due to the use of harsh discipline practices. The use of psychologically aggressive (e.g., name-calling, yelling) and physically violent (e.g., slapping, beating with an object) discipline practices are considered violence against children or child maltreatment (2). The use of physical violence on children is a direct breach of their human rights and an increasing global concern (3). Approximately 300 million children aged two to four worldwide are disciplined violently by their parents on a regular basis (1). It is estimated that 80% of children globally are spanked or hit at home (4). The use of physical punishment has been shown to be associated with increased child externalizing behavior, antisocial behavior, internalizing problems, lower cognitive ability, and lower self-esteem (5). These associations may also persist into adulthood resulting in increased violent and/or criminal behavior, antisocial behavior, mental health problems, and perpetuation of violence against their own children or spouses (5–7).
Parenting interventions are a key strategy used to prevent violence against children (8). A meta-analysis of child maltreatment parenting programs reported reductions to child maltreatment with an effect size of 0.2 SD, and reported benefits to parents' positive parenting practices, attitude, and self-confidence (9). The majority of studies in the meta-analysis included children younger than five years and interventions were delivered individually (e.g., through home-visiting or in clinic-based sessions), through group parenting sessions or a combination of both. In addition to preventing violence against children, these programs may also prevent child conduct problems, including the development of aggressive behavior (8). This is achieved by educating parents about the importance of positive attention and training them in non-violent alternatives to physical discipline (10).
Jamaican parents regularly use verbal aggression and physical punishment to discipline their children (11). In a study on parenting practices in 24 developing countries, 84% of Jamaican caregivers reported using physical discipline on their children aged five and younger; this was the highest prevalence of all the countries (12). In 2016, Jamaica became one of the first pathfinder countries in the global partnership to end violence against children. Both non-governmental organizations and the government have joined forces to end violence against children (13). The pervasiveness of caregivers' use of violent discipline strategies combined with the push globally and nationally for strategies to end violence against children, show an urgent need for a parenting intervention targeting violence prevention that can be effectively disseminated at scale in the Jamaican setting. Previous qualitative work with parents of preschool children in Jamaica has shown that although parents report frequent use of corporal punishment with their young child, they believe it is undesirable and ineffective suggesting that they would be receptive to training in behavior management (14).
Integrating such programs into existing services would promote parent participation and program sustainability. The most common services accessed by parents of young children are the health and education sector. For example, a parenting program for parents of two to six year old children, implemented in child health clinics in Iran decreased dysfunctional parenting practices and child physical and emotional abuse (15) and a training program for parents of three to seven year old children in Liberia, delivered in school settings, reduced the frequency of harsh punishment, and increased positive parenting practices (16). In Jamaica, we have demonstrated in efficacy trials that integrating parenting interventions into the existing primary health service has the potential to improve child development (17, 18); however sustaining these interventions has proved difficult due to staff workload (19).
Jamaican preschools cater to children aged three to six years and over 98% of young Jamaican children attend preschool. Training Jamaican preschool teachers in appropriate discipline techniques has shown benefits to teachers' child behavior management practices (20). We have developed a teacher-training, violence prevention program, the Irie Classroom Toolbox, to prevent violence against children (21). The Irie Classroom Toolbox has been evaluated with preschool and grade one primary school teachers and has shown large reductions to teachers' use of violence against children (22, 23).
Developing a complementary parent-training program to be implemented in preschools is a logical next step and has the potential for near universal coverage. Integrating the Irie Homes Toolbox into the services offered to parents through community preschools maximizes on this training of preschool teachers as (1) teachers trained in the Irie Classroom Toolbox can deliver the intervention with the parents, and (2) it promotes an integrated approach across home and school settings. In addition, integrating training in violence prevention into early childhood educational services will promote a high quality caregiving environment for young children that is safe, secure, and nurturing, in addition to providing cognitive stimulation. Provision of integrated violence prevention and early childhood development interventions thus promote child development across multiple domains, address multiple risk factors, and help children develop to their full potential (24, 25). Early childhood is a critical period for children's development and optimal development provides the foundation for future physical and mental health (26). Integrated interventions thus have the potential to lead to population-level improvements in child health and well-being (27).
This paper describes the development of the Irie Homes Toolbox, a violence prevention parenting program for parents of children aged two to six years. The main aims of the Irie Homes Toolbox are: (1) to prevent violence against children by parents/caregivers of young children, (2) to promote positive parenting practices including positive discipline, and (3) to prevent the early development of antisocial behavior in young children. The Irie Homes Toolbox was developed as a complementary program to the Irie Classroom Toolbox to promote an integrated approach to child behavior management across home and school settings. It was developed to be integrated into the existing preschool network and to be suitable for implementation by preschool teachers. Preschool teachers have regular contact with parents and are ideally placed to engage parents in a parent-training program being conducted at school. “Irie” is a Jamaican word that describes feeling at peace and in harmony with oneself and with others.
Methods
The Irie Homes Toolbox was developed over fifteen months using the framework of the UK Medical Research Council Guidance on Developing and Evaluating Complex Interventions (28). The development process consisted of four stages (Figure 1). The first stage involved integrating theory, empirical evidence, and the perspectives of the end users to inform the initial design of the program; the second stage involved repeated piloting of individual sessions to develop a first draft of the intervention; the third stage was a full piloting phase in which the entire intervention was piloted in five different preschools with groups of six parents, and the fourth stage involved conducting a quantitative and qualitative process evaluation of the intervention as part of a cluster randomized controlled trial. Within and between each stage, ongoing revisions were made to the intervention content, mode of delivery, structure, and materials based parents' and preschool teachers' suggestions and on the observations and experiences documented throughout the process by the research team. These iterative cycles of design, implementation, and evaluation were conducted to promote the acceptability, feasibility, relevance, and effectiveness of the intervention with the target population. All activities in the four stages of the development process were conducted by the authors of the paper and a female research assistant with extensive experience working in Jamaican preschools. Ethical consent for the study was obtained from the University of the West Indies (ECP 144, 17/18) and from the School of Psychology, Bangor University (ref: 2018-16364). Signed, informed consent was obtained from all parents and teachers participating in the study.
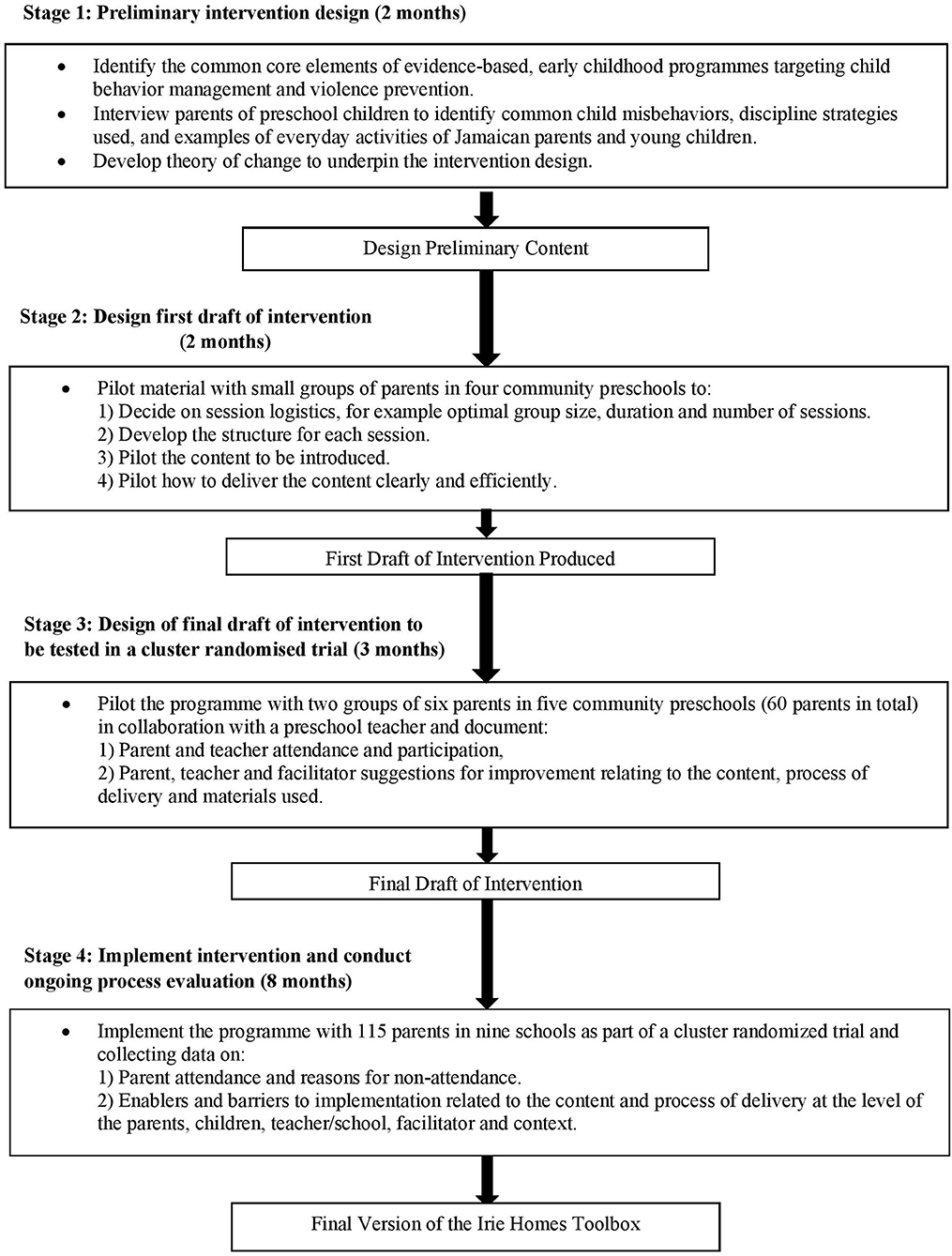
Figure 1. Stages in the development of the Irie Homes Toolbox.
Stage One: Preliminary Intervention Design
Methods
In stage one, conducted in December 2017 and January 2018, we integrated evidence from theory, empirical research studies and the perspectives of Jamaican parents. The first step involved identifying the core components of evidence-based parenting programs related to both the content and methods of implementation (29). The focus was on programs targeting parents of children between two and eight years that aimed to improve positive and reduce negative parenting practices, reduce child maltreatment, and/or reduce child behavior problems. We included programs focussing on child maltreatment and on child externalizing behavior, as both types of program include training parents in appropriate discipline techniques. Programs reviewed included the Incredible Years Parenting Program (30), Triple-P Positive Parenting Program (31), Parent Management Training Oregon Model (PMTO) (32), Parent-Child Interaction Therapy (33), Parent Corps (34), and ACT Raising Safe Kids (35) from high-income countries and Sinovuyo (36), Parents Make a Difference (15), and Projecto Paceria (37) from low and middle-income countries (LMIC). We also examined reviews and meta-analyses of the common core components of parenting interventions to identify the components that lead to more effective parenting interventions to prevent and reduce children's externalizing behavior (38–40) and to prevent and treat parents' use of violence against children (41–43). As the parenting intervention is planned as a complementary program to the Irie Classroom Toolbox, we also identified components from the Irie Classroom Toolbox that would be applicable to parents. We created a working draft of possible content and behavior change techniques that would be used in the intervention from these three sources of information, [that is from: (1) the content and method of implementation used in evidence-based parenting programs, (2) qualitative and empirical reviews of common core components from interventions for externalizing behavior and to prevent violence against children, and (3) the core components from the Irie Classroom Toolbox]. To operationalise these core components for the Jamaican cultural context and to inform the design of the intervention materials, we conducted a series of rapid interviews with parents of preschool children to identify common child misbehaviours, discipline strategies used, and examples of everyday activities of Jamaican parents and young children. Through these interviews, we identified the language used by parents to describe children's positive and negative behaviors and words parents use to praise and to chastise children. This information was essential for designing the intervention so that it resonated with the intended particpants and was appropriate for the cultural and economic context. We approached four inner-city preschools to assist us with this initial development. We chose preschools that were located close to the university, were reasonably representative of inner-city preschools in terms of size, staffing, and facilities available, and with whom we had a good working relationship from previous studies. Parents of children attending the school were selected by convenience and a group of ten parents in each school were interviewed. Interviews were conducted on the school compound and lasted approximately fifteen min. A total of thirty-five mothers and five fathers participated in these interviews. The topic guide included: (1) questions about child behavior (e.g., “What are some things that your child does when they are giving trouble?” “What are the main problems you have with your child?”), (2) questions about parent behavior (e.g., “What are some things you say to your child when s/he misbehaves?” “Tell me some of the reasons you slap your child.” “What do you say to your child when s/he is being good?” What instructions do you have to repeat constantly to your child?”), and (3) questions about child activities (e.g., “What game does your child play and what toys does s/he play with?” “What does your child do after school?”). Finally, we developed a theory of change to underpin the intervention development. The theory of change for the Irie Homes Toolbox is similar to that for the Irie Classroom Toolbox and incorporates the COM-B system for understanding behavior which states that for a behavior to occur and be sustained, three factors are required: capability, motivation and opportunity (44). Behavior change techniques to promote these three factors are thus incorporated into the intervention.
Results
The common core components of evidence-based parenting interventions and the components of the Irie Classroom Toolbox relevant to parents are shown in Table 1. The core components that have been shown to be most effective in programs targeting child behavior problems vs. child maltreatment share some commonalities and there are also some differences. For programs targeting child externalizing behavior, building a positive parent-child relationship through nurturing, positive and sensitive interactions, the use of praise and positive reinforcement, emotional communication, and learning appropriate discipline methods such as time-out and consequences have been shown to be important components (38, 40). For programs targeting child maltreatment, learning non-violent discipline approaches, daily child-led play, and parental self-management skills have been shown to be most effective (41, 42). In terms of the process of delivering the content, the most effective programs are delivered in a non-stigmatizing way, focus on building parents' self-confidence and involve modeling, rehearsal and practice, supportive feedback, homework assignments, and problem-solving activities (38, 42, 43). These components were thus included in our initial intervention design. We also prioritized relevant content and process components from the Irie Classroom Toolbox as these components (1) have proven effectiveness in the Jamaican setting, and (2) are used by the preschool teachers who will ultimately deliver the intervention to parents. The content used most and most liked by teachers included paying attention to positive behavior, explicitly teaching the expected behavior, giving clear instructions, and interactive reading (21). The training methods most valued by teachers included rehearsal and practice, giving positive and supportive feedback, ensuring teachers recognized the benefits of the intervention to the children and to themselves, group support, provision of necessary materials to implement the intervention, and making sessions fun (21). Table 2 outlines how the parent interview responses were used in intervention development to ensure the program was acceptable, relevant, and feasible for the Jamaican cultural context. The responses were used in the design of role plays, practice activities, visual aids, and problem-solving activities. The theory of change is shown in Figure 2. The core intervention content is delivered using evidence-based behavior change techniques leading to increases in parents' skills, motivation and opportunity to use the strategies with their child. This leads to improved parental outcomes including increased positive parenting, reduced negative parenting, and reduced violence against children. The improvements in parental outcomes in turn lead to improved child behavior and school readiness skills. Using the information from the review of core components, parental interviews and theory of change, we developed an outline of the content and process delivery of the intervention for testing in stage two.
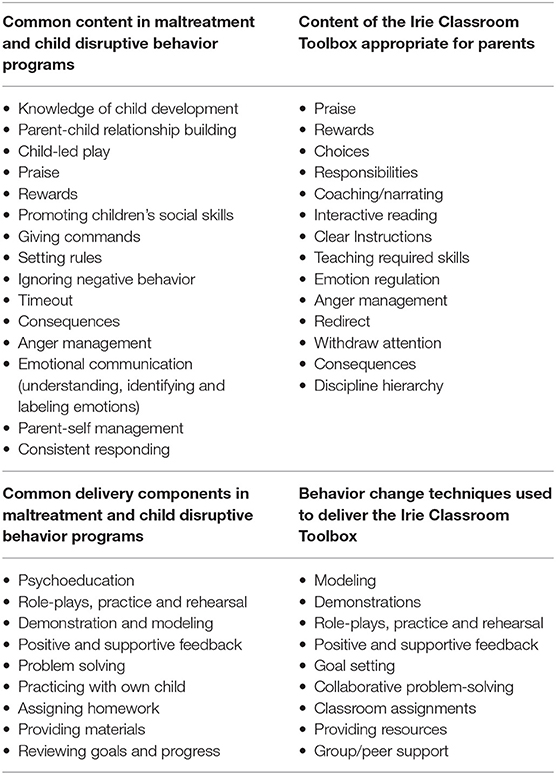
Table 1. Core content and behavior change techniques used in parenting interventions to prevent and/or treat child disruptive behavior and child maltreatment and in the Irie Classroom Toolbox.
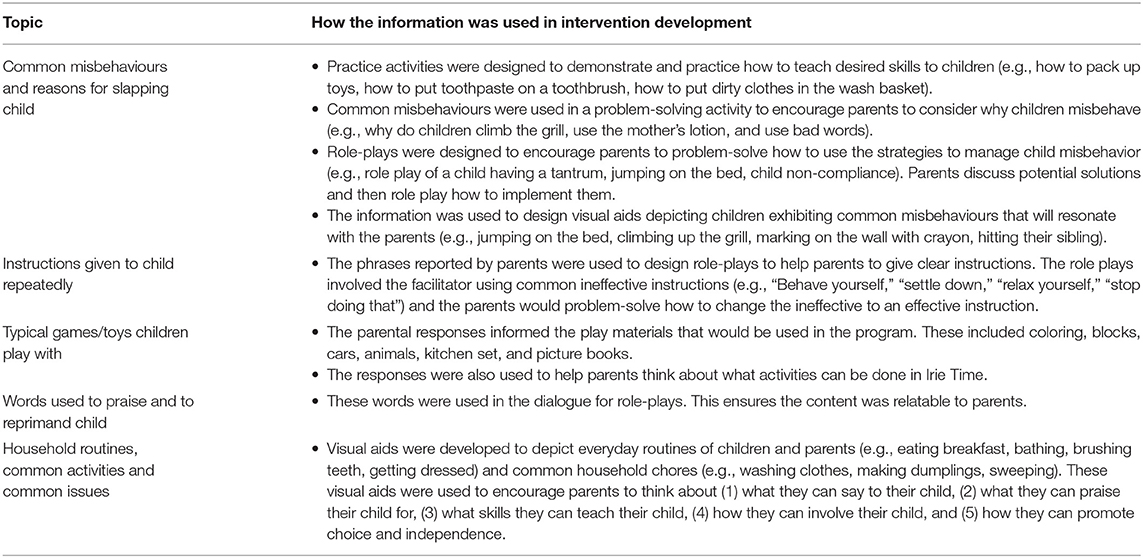
Table 2. How parents' interview responses were used in the development of the intervention.
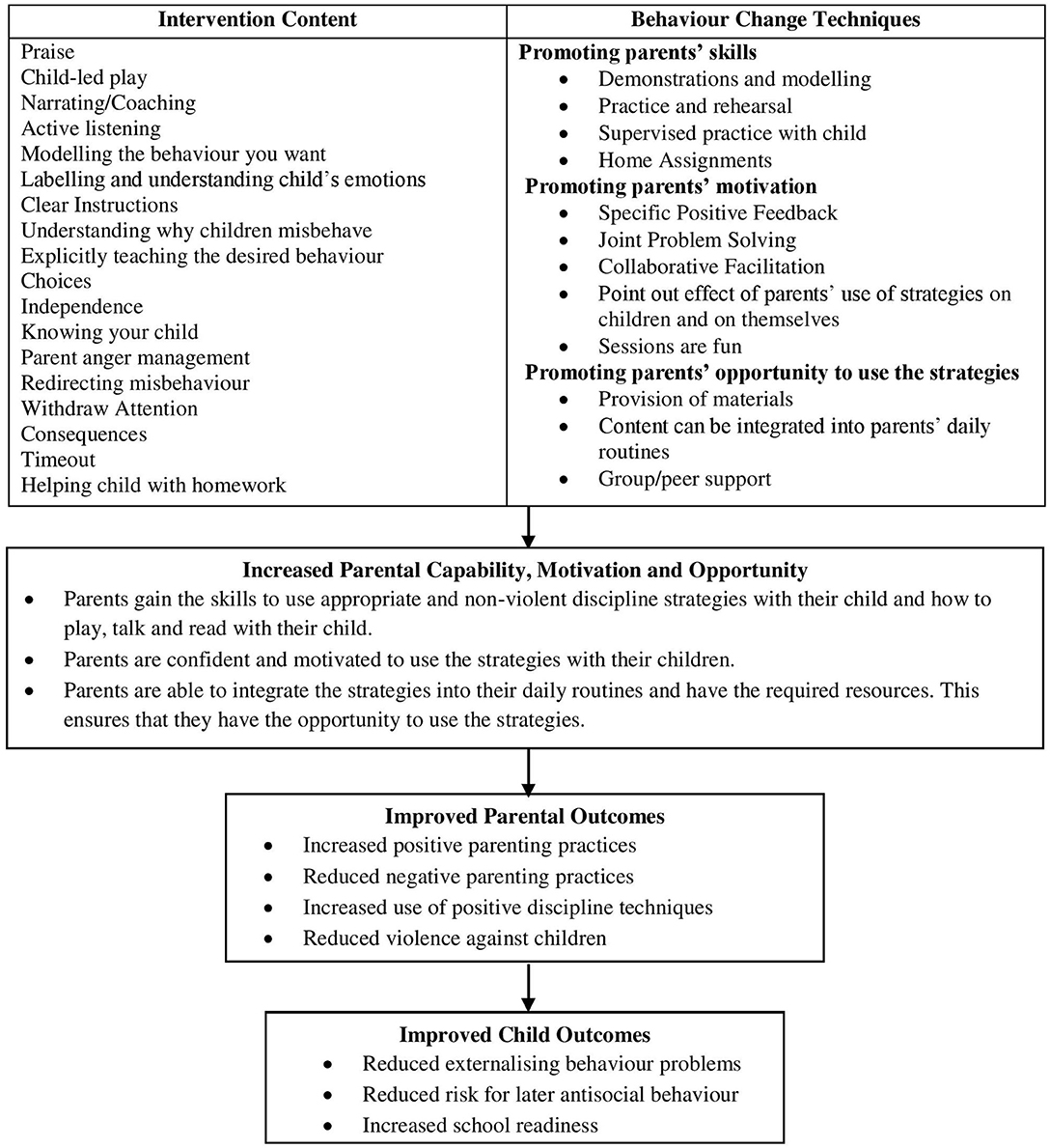
Figure 2. Theory of change.
Stage Two: Designing the First Draft of the Intervention
Methods
The aim of stage two was to undertake preliminary piloting of the intervention content and methods of implementation to produce a first draft of the intervention. The activities for stage two were conducted in February and March 2018. We continued to work within the same four community preschools that participated in stage one and convenience samples of five to twelve parents were invited to participate in sessions. The majority of participants were mothers although four fathers and one grandfather were included in the sample. Sessions were conducted at the beginning of the school day. Each individual session was piloted twice with different groups of parents, with ongoing revisions based on lessons learnt during each session. During these sessions one member of the team delivered the content while another team member made notes on: (1) parents' engagement, level of understanding, ability to use the strategies, and what content resonated within the group, (2) ideas for materials and visual aids that would help to promote parents' understanding and engagement, (3) session logistics including session structure, duration and optimal group size. Throughout the process of piloting the sessions, we used the following guidelines to inform our decision making and note taking:
• Be reflective: constantly think of ways to improve the acceptability, feasibility, relevance, and effectiveness of the program.
• Evaluate whether parents understand and are able to use the concepts introduced and plan how their knowledge and skills can be improved.
• If something does not work, or does not work well, problem solve in real-time. Try a different approach and document what happens.
• Pay close attention to the group vibe; if it's flat then something is wrong. Identify ways to maximize participation, fun, and interest.
• Pay attention to individuals in the group, ensure all are participating.
• Make note of scenarios that resonate with the group.
• Note parents' strengths and needs throughout the session.
• Note examples that parents give and use their comments and ideas to revise the content and delivery of the program.
After each session, the notes were discussed among the research team and decisions made to increase the acceptability, feasibility, relevance, and effectiveness of the intervention. These decisions were incorporated into the relevant session prior to piloting the session with a different group of parents.
Results
Tables 3, 4 show how we operationalized our key principles of acceptability, feasibility, relevance and effectiveness based on our observations and notes as we piloted the intervention. To promote acceptability, we aimed to: (1) ensure the intervention was fun and engaging, (2) acknowledge parents' current strengths, and (3) help parents see the benefits of the program. The key factors influencing feasibility were considered to be: (1) session logistics, (2) the equipment required to conduct the intervention, (3) whether parents could easily integrate the content into their daily lives, and (4) how to individualize the content to ensure participants' individual needs were met. To promote the relevance of the intervention, we ensured that the material resonated with the parents and met their needs. In addition, as this is a preschool-based program, we included content on how parents can support their child's homework. The acceptability, feasibility, and relevance of the intervention are all critical to its effectiveness. Additional factors considered under effectiveness were: (1) the optimal group size, (2) parent understanding and skill using the strategies, (3) parent motivation, (4) parents' reports on their use of the strategies at home, (5) parents' ability to generalize their use of the strategies, (6) ensuring the sessions are supportive, collaborative and non-critical, and (7) designing the session structure (Table 4).
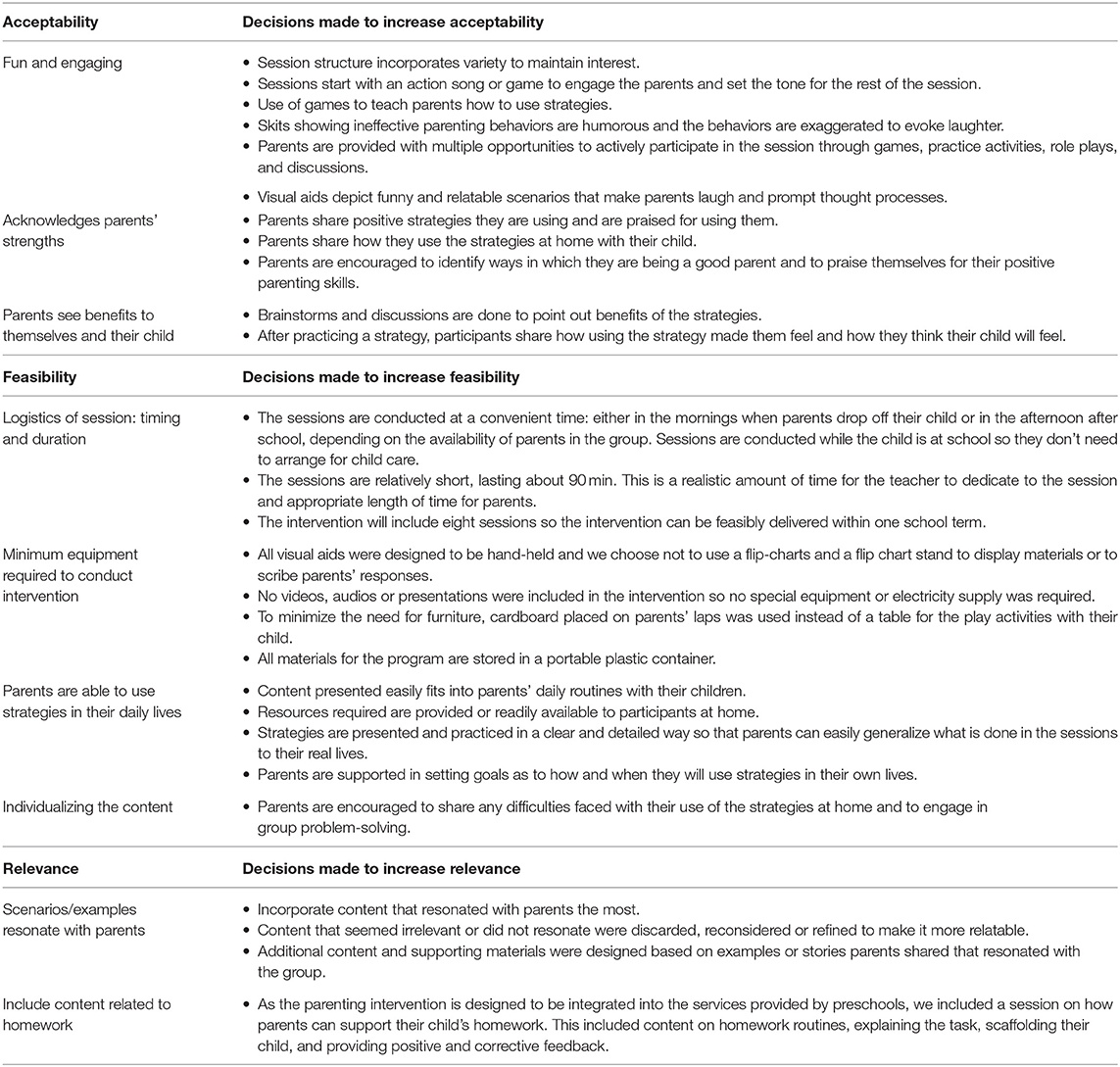
Table 3. Decisions made to improve the acceptability, feasibility, and relevance of the intervention.
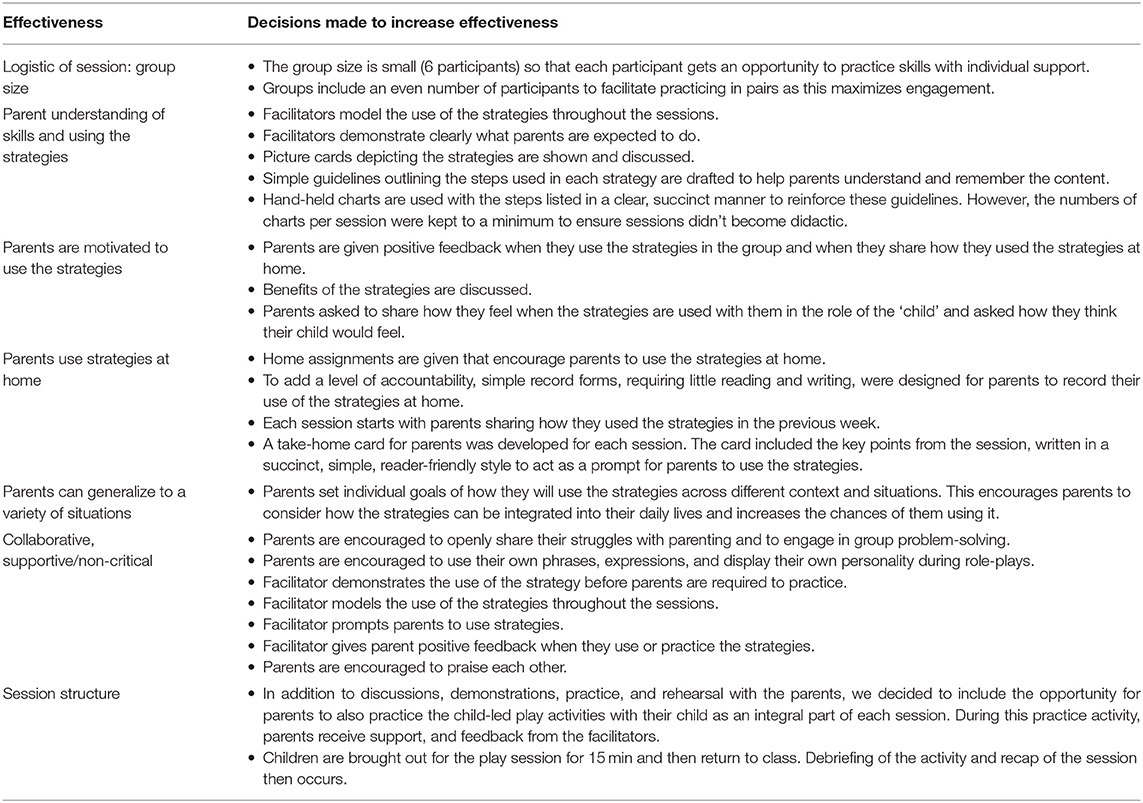
Table 4. Decisions made to improve the effectiveness of the intervention.
A core component of the intervention is to encourage parents to engage in daily child-led play or Irie Time. To ensure parents had the resources available to do this, we decided to include a toy or book in the materials given to parents after each session. We choose toys that facilitated free-play such as blocks, cars, animals and a pretend play set, rather than structured toys such as puzzles, and matching games. We also included three wordless picture books. Two of these books were adapted from the Reach Up and Learn parenting intervention, additional details, and extra pictures were added to make them more suitable for the older child age range targeted in this intervention (45). One book was designed specifically to reinforce content introduced through the program. This book encouraged parents to label children's emotions and included pictures of children expressing different emotions followed by a scenario in which a child may feel that way (for example, a sad face followed by a picture of a child looking sad because they dropped their ice-cream). During the session, we demonstrated the child-led play or book activity, encouraged the parents to practice, and then parents played or read with their child during the session with support from the facilitators. In this way, we capitalized on the fact that the sessions were being conducted at school as children could join the sessions for the play activity only. During the rest of the session, the children were in their classroom and no child-care was required.
By the end of stage two, we had developed an initial draft of the content and process of delivery of the intervention and designed the intervention materials (for example, picture cards, charts, take-home cards for parents, homework assignment record forms for parents, picture books) to be tested in stage three.
Stage 3: Design of the Final Draft of the Intervention
Methods
The first draft of the Irie Homes Toolbox produced through stage two activities consisted of eight 90-min sessions. The full program was then piloted in five new community preschools from April-June 2018. The ultimate goal is for the Irie Homes Toolbox to be delivered by preschool teachers who have been trained in the Irie Classroom Toolbox, hence it was important to include the perspectives of preschool teachers in the development of this parenting intervention. We invited preschools whose teachers had participated in the Irie Classroom Toolbox training to assist us (46). Harsh punishment is common in Jamaica preschools and the rationale for involving teachers who were already familiar with the Irie Classoom Toolbox was that these teachers had developed a good understanding of child behavior management strategies and had experienced the training methods used to help them to change their discipline practices. Six parent-child dyads were recruited from each school, giving a total sample size of thirty parents. The parents were selected based on interest and availability. When a parent dropped out of the program before the sessions began or after attending one session, an additional parent was recruited to participate in the training sessions. The participating parents' children were aged two to six years with a mean age of 3.5 years; 40% of the children were boys. There was one father and the remaining participants were mothers. The preschool principal allocated one teacher to assist the research team and the sessions were delivered in collaboration with a teacher from each school. This ensured that we could include the perspectives of preschool teachers in the intervention design and we could identify challenges associated with teacher participation. Two team members attended each session, one acting as a facilitator and one as a notetaker. After each session, the facilitators and the preschool teacher reflected on (1) parents' level of understanding of the content presented and acquisition of skills, (2) parents' degree of engagement and participation during the session, (3) parents' ability to generalize and apply the skills across multiple activities and contexts, and (4) examples of child and parent behaviors that resonated with the group. These notes were then used to refine the content, delivery, structure, and materials of the intervention with the aim of increasing its acceptability, feasibility, relevance, and effectiveness. These changes were made on an ongoing basis so the refinements could be implemented and piloted in an iterative and cyclical process of design, implementation, and evaluation. In stage three, we also piloted parent recruitment and engagement strategies and made notes on teachers' engagement in the sessions as co-facilitators.
Results
Table 5 outlines the refinements made to the content, delivery, materials and structure of the intervention based on the data collected from piloting during stage three. Refinements included: (1) adding content related to parents' personal needs, (2) adapting the training methods for content that parents found more difficult, (3) making changes to the session structure, (4) designing additional materials, (5) building more redundancy into the parenting sessions, and (6) providing additional guidelines for the co-facilitator. The data was used to develop the final draft of the Irie Homes Toolbox to be tested in a cluster randomized controlled trial. A summary of how the information from stages one to three was used to ensure the content and methods of implementation used in the Irie Homes Toolbox are acceptable, feasible, relevant, and effective in the context is shown in Figure 3.
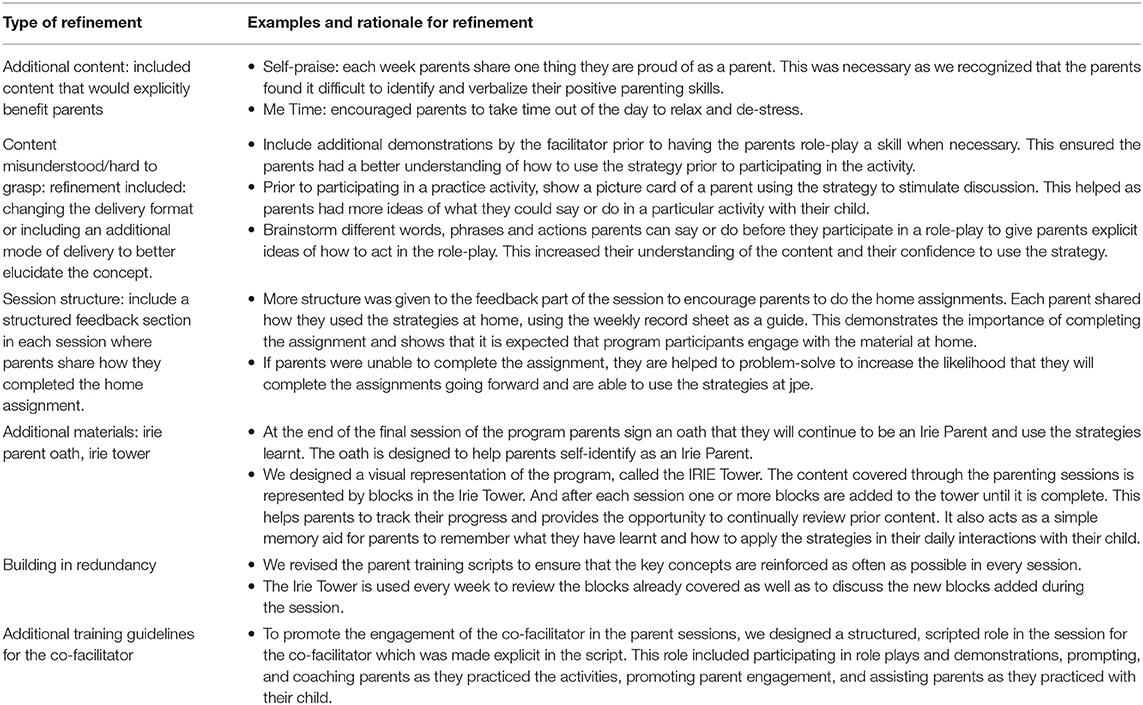
Table 5. Refinements made to the content, delivery, materials, and structure of the intervention in stage three.
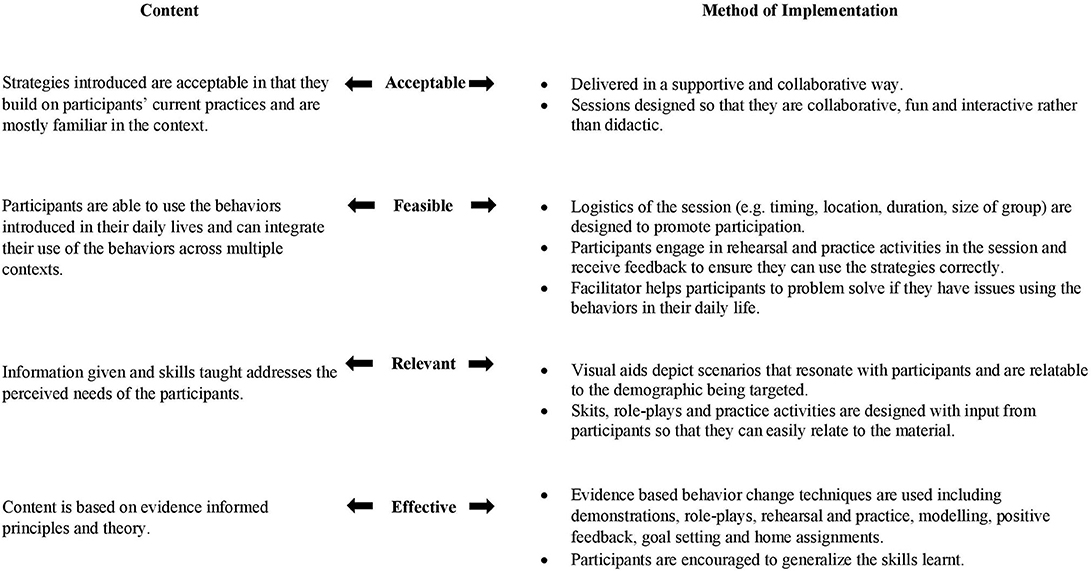
Figure 3. Acceptability, feasibility, relevance and effectiveness of a behavior change intervention.
The most effective recruitment strategies involved working through the teachers and/or school principal rather than the research team recruiting parents directly. Three of the parents recruited directly by the research team decided they no longer wanted to participate before the program commenced and four parents attended only the first session. These parents were replaced by parents recruited through their child's teacher and/or the school principal. The average attendance of the participating parents was 81% (range 50–100%). We also found that the collaborating teachers would rarely attend the entire session and would leave the sessions frequently to attend to other duties. To promote teacher engagement, we therefore included a structured and scripted co-facilitator role for the teacher in the revised intervention as shown in Table 5.
Stage 4: Implement Intervention and Conduct Ongoing Process Evaluation
Methods
The intervention was tested in a cluster-randomized trial in eighteen community preschools that had not participated in stages one to three. The parenting sessions were implemented during the period September 2018 to April 2019. Preschools were selected to participate in the trial based on the following criteria: (1) had participated in the Irie Classroom Toolbox training and had two or more Irie trained teachers still working at the school, (2) were interested in participating in the program, (3) had parents who consistently dropped children and/or picked up children from school rather than a driver, (4) had no other structured parenting program currently operating, and (5) the principal and all teachers in the school consented to participate in the study. Nine preschools were randomized to participate in the parenting intervention and an ongoing process evaluation was conducted. Parents were recruited at the school by the research team with the help of the teachers and principal. A minimum of six parents were recruited from each school in the Autumn term and an additional six recruited in the Spring term resulting in a minimum total of 12 parents per school. The inclusion criteria for parents were: (1) interested in participating in the program, (2) able to stay back for 90 min either in the morning after dropping off their child or in the afternoon when they came for pick-up one day a week, and (3) parent gave consent for him/herself and his/her child to participate in the study. The quantitative results from the trial will be reported separately. In this paper we are focusing on the process of developing the intervention. One hundred and fifteen parent-child dyads participated in the intervention. The children were aged two to six years old with a mean age of four years; 52.2 % of the sample were boys. Caregivers had mean age of 31 years, 104 (90.4%) were mothers, two (1.7%) were fathers, and nine (7.8%) were other relatives. Less than half the parents completed high school (46%) and 43% were in paid employment. The ultimate aim is for the preschool teachers to implement the intervention. However, in this small-scale efficacy trial we wanted to assess the effectiveness of the program when delivered consistently and with high fidelity; when the intervention is delivered by teachers the quality of implementation may be more variable. Hence, a member of the research team delivered the intervention. Each school principal allocated one preschool teacher to assist the research team by co-facilitating the parenting session. This ensured that we were able to continue integrating the perspectives of the preschool teachers, into the program design. Parenting sessions were held on the school compound (in the school yard or any available room), once a week for eight weeks and lasted 90 min.
The ongoing process evaluation included a quantitative and qualitative component. The quantitative component included recording parent and teacher attendance. For the qualitative component, after each session the facilitators (including the preschool teacher) discussed the session together and then the main facilitator completed a record form that documented enablers and barriers related to: (1) the content of the session (for example, what resonated with parents and what was more difficult), (2) the process of delivery (for example, techniques parents enjoyed the most and least), (3) the context in which the session was delivered (for example, logistics and environment), (4) the involvement of the children, (5) teachers' co-facilitation of the sessions, and (6) facilitators' skills in delivering the session. Notes were also made on individual parents' engagement, understanding, strengths, and needs. Facilitators noted their perceptions of which strategies were most acceptable, feasible, relevant, and effective and suggested solutions to any problems encountered in implementing the intervention. The information from the facilitator record forms was used to further refine the Irie Homes Toolbox.
In addition to the ongoing process evaluation, in-depth, individual, semi-structured interviews were conducted with a subsample of participating parents (n = 28) and with one teacher from each preschool who co-facilitated the sessions (n = 9). A section of the interview focussed on participants' perspectives of the main benefits of the program and is reported here. One or two parents from each school who had attended a minimum of four sessions were randomly selected for interview. Eighty three (79%) parents had attended four or more sessions and fourteen parents were randomly selected from participants in round one (Autumn term) and a further fourteen parents were randomly selected from participants in round two (Spring term). In-depth interviews with parents were conducted over two phases, within one month after the end of the sessions. Teacher interviews were conducted at the end of round two. Interviews were conducted in a quiet place in each preschool by a female research assistant who had not been involved in implementing the sessions. All interviews were recorded and transcribed. The analysis was conducted using the framework approach which is particularly appropriate for applied research with specific objectives (47). Codes were developed by HBH and a trained research assistant applied the codes to the data and developed the thematic charts. The coding was checked by TF and any discrepancies were discussed and resolved by TF and HBH.
Results
Parental attendance averaged 71.5% in round one (Autumn term) and 67.1% in round two (Spring term). 61.8% parents attended six or more sessions with 28.7% all eight sessions. We documented the reasons for parent non-attendance and 79% of the absences were rated as legitimate. Legitimate absences were absences that were deemed unavoidable such as: clinic/doctor visit, called in to work unexpectedly, child being sick, unchangeable appointments, and meeting at older children's school. Teachers co-facilitated a mean of 7.1 (SD 0.9) sessions in round one (the Autumn term) and 3.4 (SD 2.8) sessions in round two (the Spring term). In the Spring term, teachers had many competing activities and responsibilities and attendance was more challenging. In addition, teachers were confident that the facilitator would continue to conduct the sessions if they were absent and this also led to reduced attendance, especially in the face of competing activities.
Facilitators made notes of multiple instances that supported the fact that the intervention developed was acceptable, feasible, relevant, and effective to the participants. In terms of acceptability it was noted that parents would consistently laugh and have fun with the games, role-plays, and visual aids presented. Parents were eager and willing to participate in the different activities during the sessions and they would incorporate their own personality and flair to the activities further confirming their acceptability. The feasibility of the strategies was shown through the parents' reports on how they used the strategies at home in different situations. The relevance of the intervention was illustrated through the discussions in which parents shared instances of issues they were experiencing with their child and would provide examples of how the strategies helped them at home. Throughout the sessions, facilitators documented evidence of effectiveness including parents being able to use strategies with little to no prompting and becoming more confident and skilled in using the strategies as the weeks progressed.
Tables 6, 7 present the evidence from the qualitative interviews on parents' and teachers' perspectives of the benefits of the intervention. Both parents and teachers reported that parents had better emotional self-regulation skills, used less violence against their child(ren) and that parent-child relationships improved. Parents also reported being more confident and proud of their parenting skills, while teachers reported that parents used more praise with their child and showed more interest in school activities. Teachers reported similar benefits to themselves from co-facilitating the sessions, especially in terms of better emotional self-regulation, less violence against children (both in the classroom, and with their own children), and using the other strategies introduced through the program (e.g., praise, modeling, withdrawing attention, and redirecting children's attention) more frequently than previously at school and at home. Parents and teachers also reported similar benefits to children including children being more independent and displaying fewer behavior difficulties (for example, less aggression, and fewer tantrums). Parents also reported increased child compliance and an increase in their child's positive behavior and emotions. Teachers perceived children of participating parents to be more confident in school. Teachers also reported benefits to their relationships with parents and expressed more empathy with and understanding of parents and the difficulties they faced.
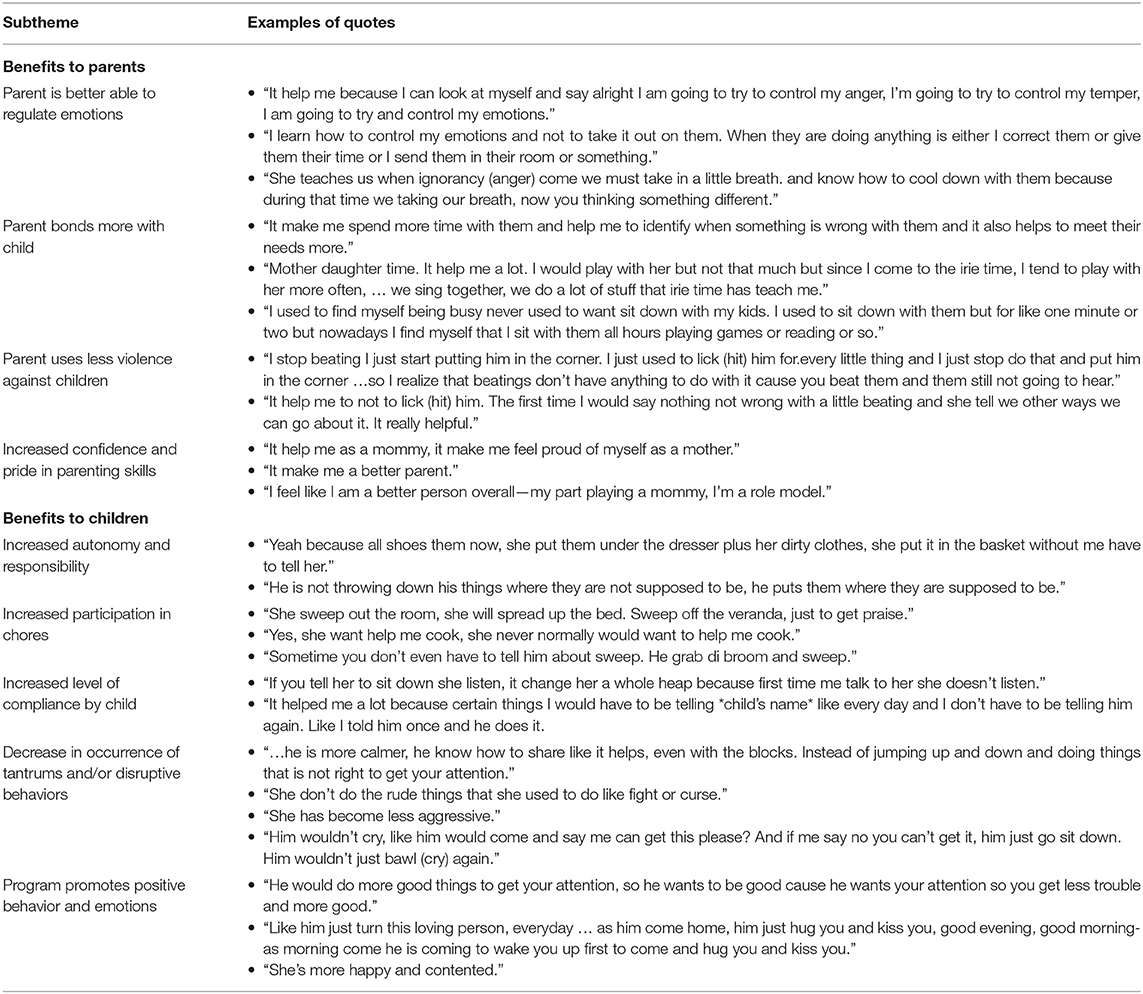
Table 6. Parents' perceptions of the benefits of the Irie Homes Toolbox.
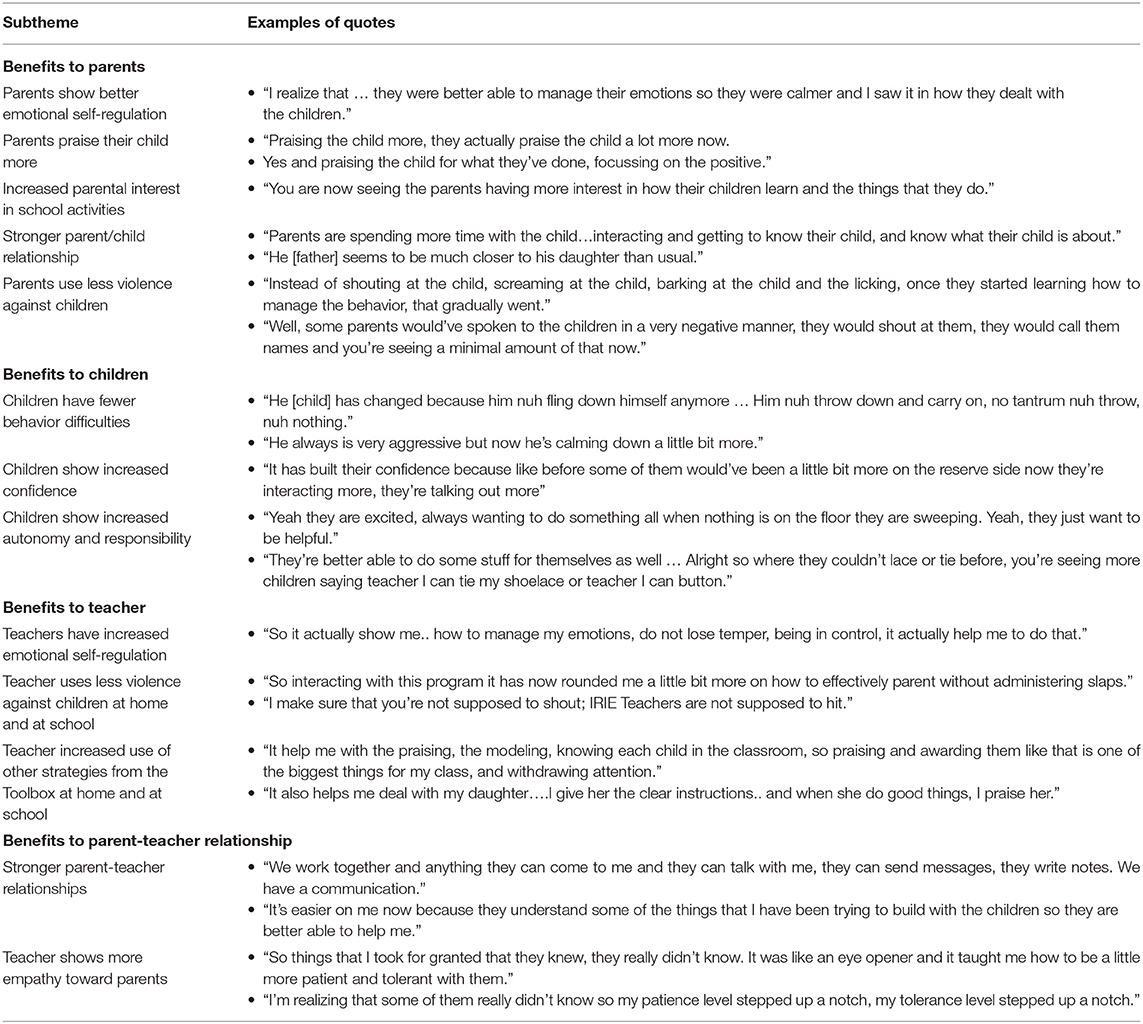
Table 7. Teachers' perceptions of the benefits of the Irie Homes Toolbox.
Table 8 shows the barriers faced in implementing the sessions with the changes made to address these barriers. This data was used to further refine the Irie Homes Toolbox to produce the final version of the program.
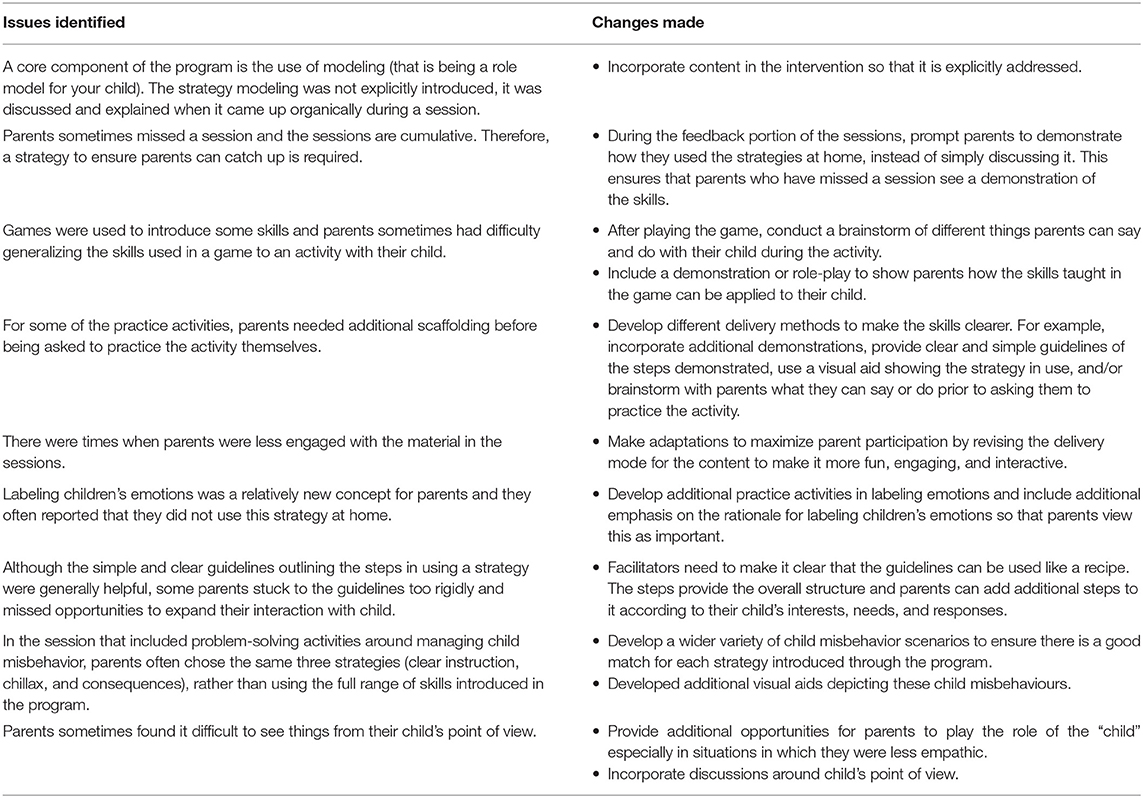
Table 8. Areas of the intervention requiring revision as extracted from the process evaluation tool and changes made in stage four.
Description of the Irie Homes Toolbox
The intervention developed through the four stages of this study is a violence prevention program for parents of children aged two to six years called the Irie Homes Toolbox. The main goals of the program are to prevent and/or reduce parents' use of violence against children, increase positive parent-child interaction, and prevent and/or reduce child externalizing behavior problems. The Irie Homes Toolbox is a group-based parenting program consisting of eight sessions, each lasting 90 min, delivered once a week for eight weeks. Each of these eight sessions follows a set structure that includes (1) a game or song, (2) feedback from the previous week including a discussion of the home assignment, (3) introduction of a new topic consisting of discussions, role plays, demonstrations, rehearsal, and practice, (4) introduction of a child-led play or picture book reading activity with demonstration, rehearsal, and practice, (5) practicing the child-led play or book activity with their child with supportive feedback, and (6) review, goal setting, and allocating homework assignment. The toolbox consists of content divided into five modules (1) promoting positive behavior, (2) preventing misbehavior, (3) understanding emotions, (4) managing misbehavior, and (5) supporting homework (Table 9). In each session, parents are encouraged to spend daily Irie Time with their child which involves spending quality time with their child and following their child's lead while playing with toys and/or looking at picture books (Table 9). The content covered through the eight sessions of the program is represented in the Irie Tower (Figure 4). The Irie Tower has the blocks representing the positive parenting strategies at the base of the tower as these form the foundation of the program. As the sessions progress, parents are encouraged to use the blocks near the bottom of the tower every day and to only use the blocks at the top when absolutely necessary. Materials used in the Irie Homes Toolbox include materials for facilitators and materials for parents (see Figure 5 for examples of these materials). Materials for facilitators include: (1) a fully scripted training manual including the training scripts for the eight sessions, (2) visual aids (including pictures of parents and children engaged in everyday activities and routines, pictures of parents using the strategies introduced in the program, and pictures of children engaged in common misbehaviors), (3) hand-held charts with key points from the session, and (4) the Irie Tower. Materials for parents include: (1) a take-home card for each session summarizing the content introduced, (2) a homework assignment record for each session, (3) selected toys and picture books for parents to use during Irie Time and (4) an Irie Parent Oath that parents sign on completion of the program (Figure 6).
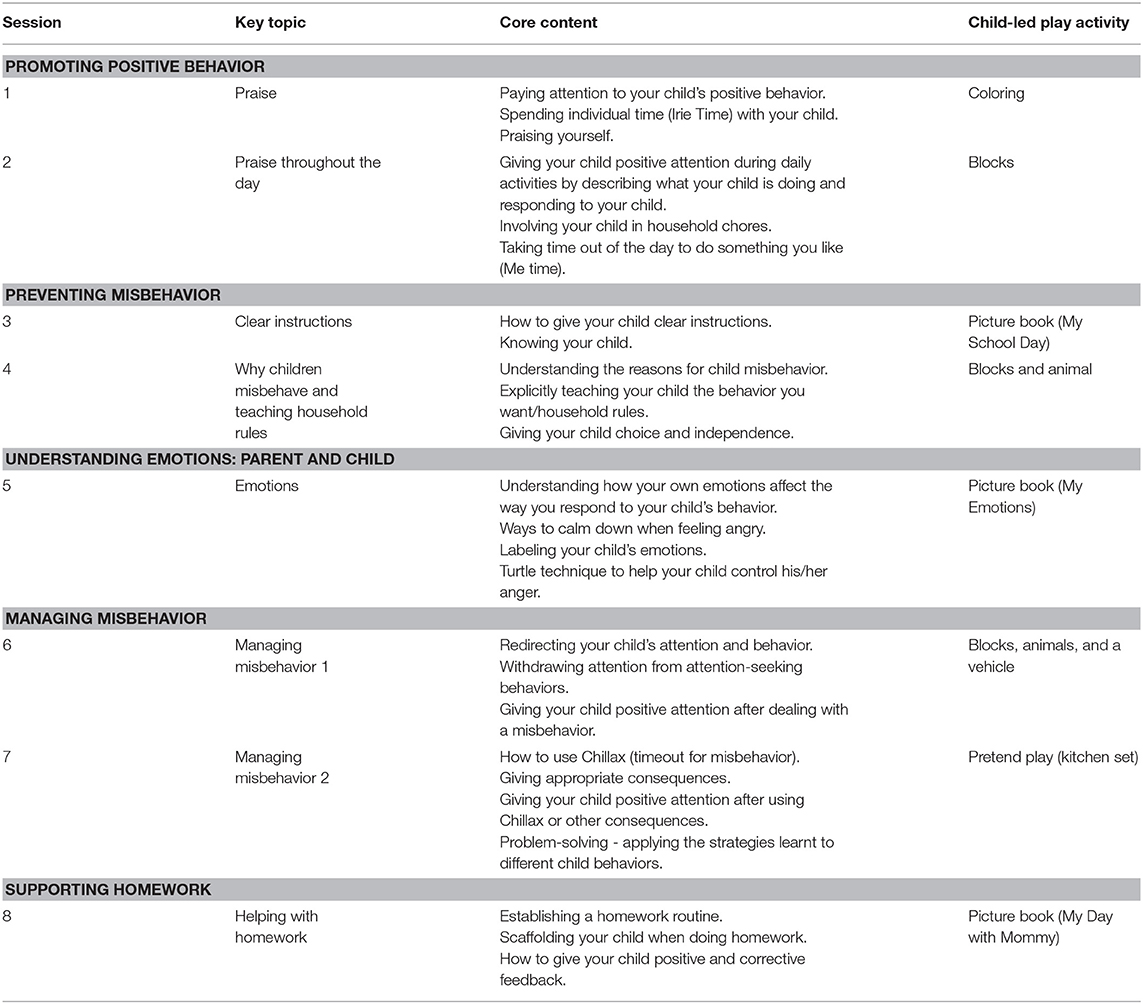
Table 9. Session content of the Irie Homes Toolbox.
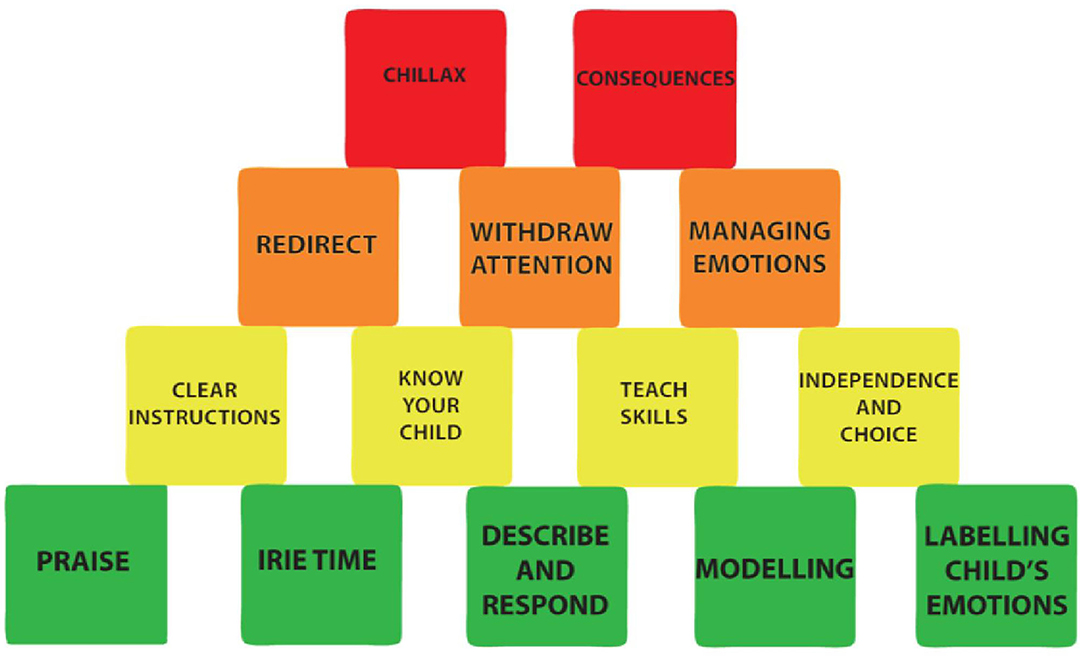
Figure 4. The Irie Tower: pictorial representation of the strategies introduced in the Irie Homes Toolbox. The base of the tower (green blocks) are strategies to promote positive behavior and to build a positive parent-child relationship. The yellow blocks are strategies to prevent child misbehavior. The orange and red blocks are strategies to manage child misbehavior. Parents are encouraged to use the strategies in the two bottom rows liberally and the strategies in the top rows more sparingly.
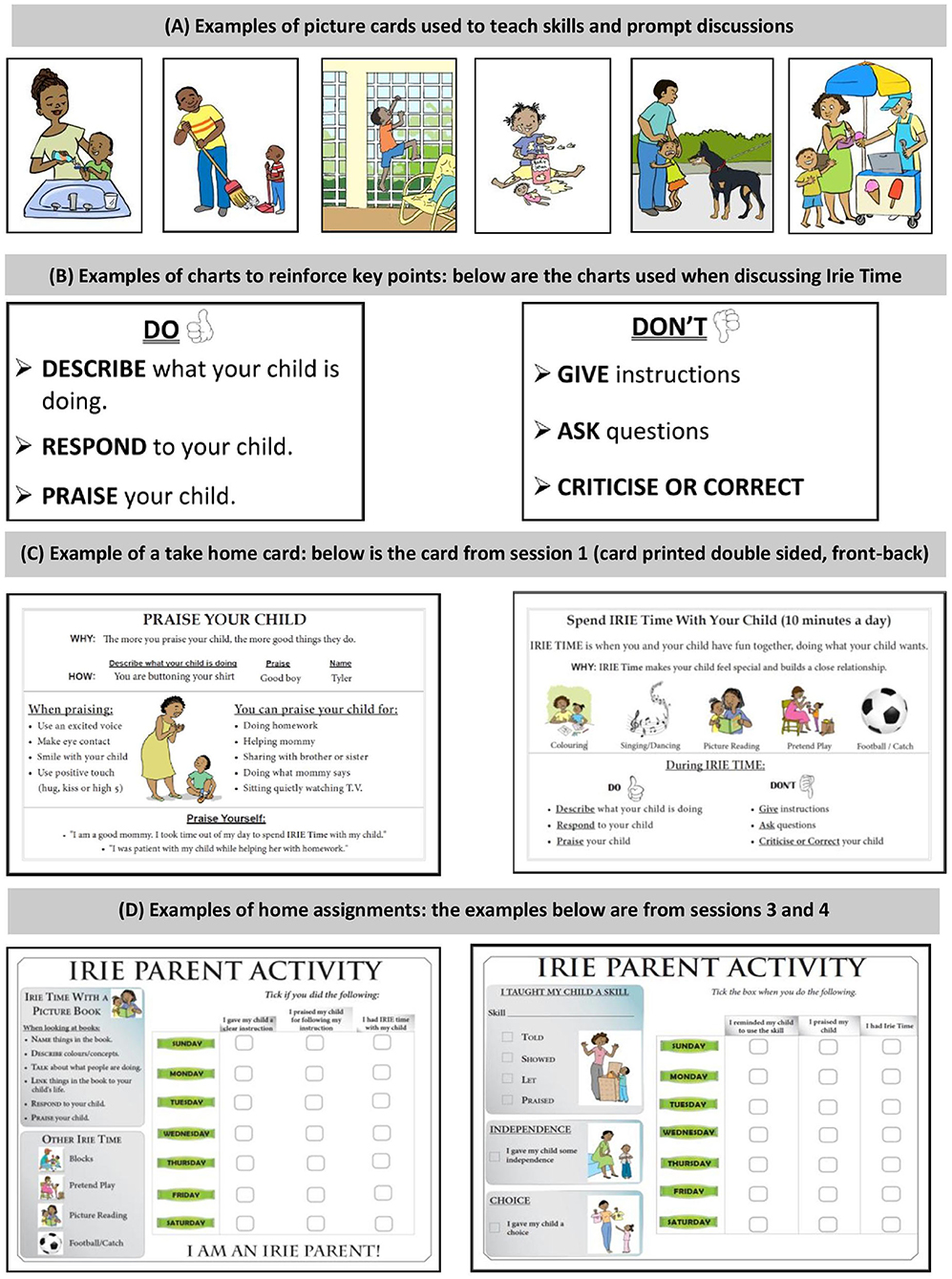
Figure 5. Examples of resources used in the Irie Homes Toolbox.
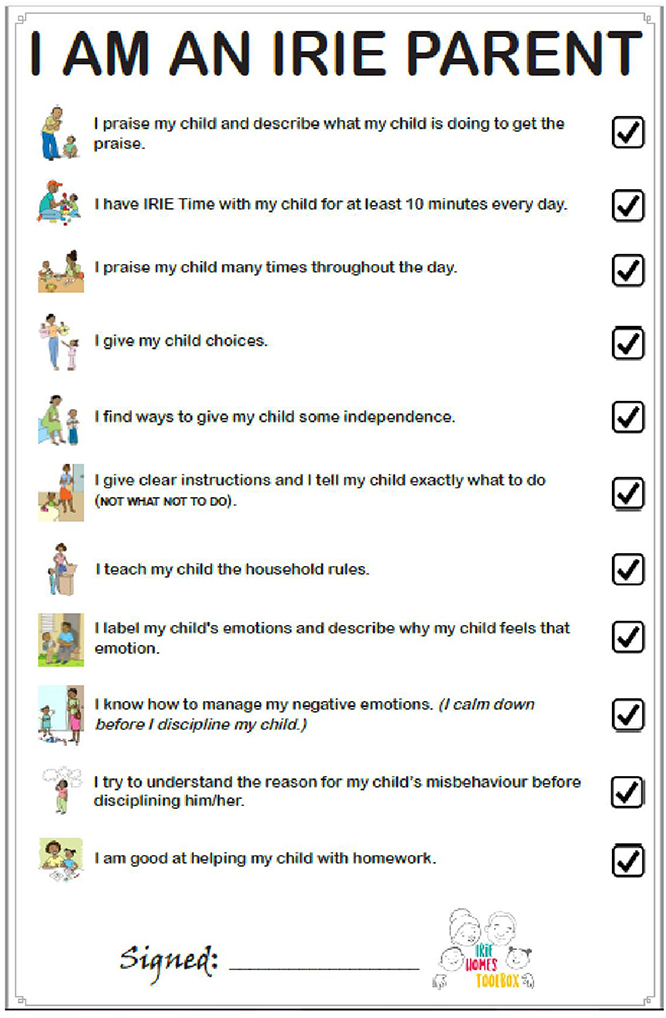
Figure 6. The Irie parent oath.
Discussion
The development of the Irie Homes Toolbox was guided by theory, evidence, and practice. Through a series of four stages, the intervention content, materials, structure, and process of delivery was tested through an iterative and cyclical process of design, implementation and evaluation with the aim of producing a parenting intervention that was acceptable, feasible, relevant, and effective in the context. The resulting intervention: (1) is theory-informed and incorporates evidence-based content and evidence-based behavior change principles, (2) was developed with participation of Jamaican parents and teachers who are the end users, and (3) was designed to be low-cost and integrated into the existing preschool network thus promoting wider dissemination and sustainability. Evidence from stage four showed that parent attendance and retention in the intervention was good indicating that the intervention was acceptable to parents. Parents and teachers reported benefits to parenting and child behaviors that were targeted through the intervention. Specifically, this included: (1) parents using less violence against children and spending more time building a positive relationship with their child, and (2) children displaying more positive behaviors and fewer behavior difficulties at home and at school. These perceived benefits indicate that parents understood and were willing and able to use the strategies taught through the program, providing evidence for feasibility, relevance, and the perceived effectiveness of the intervention. Parents reported greater confidence in their parenting skills which is likely due to the positive, supportive, and non-critical nature of the program in combination with the changes that they perceived in their own and their children's behavior. The advantages of integrating the intervention into the preschool network were evident as teachers reported benefits to their relationship with the parents and to parents' interest and engagement in school activities. There was also evidence that teachers' involvement in delivering the Irie Homes Toolbox reinforced and enhanced their previous training in the Irie Classroom Toolbox as they reported increased use of appropriate child behavior management strategies in the classroom, in addition to with their own child(ren). The fact that teachers reported benefits to their own personal and professional life is promising as interventions are most likely to be sustained when there are clear benefits to the persons delivering an intervention, in addition to the intended beneficiaries (48). In previous qualitative research with Jamaican preschool teachers, we found no evidence of teachers showing empathy with parents and it was encouraging that in this study, teachers also reported an increased understanding of parents and the difficulties they faced (14). Empirical evidence of effectiveness will be reported separately with the results from the impact evaluation.
There are three broad categories in the literature for the development of behavior change interventions that involve: (1) transporting an existing evidence-based program for use in a new cultural and/or economic context [for example, (49)], (2) developing an intervention specific for the context [for example, (21, 36)], and/or (3) learning while growing which involves continually improving an existing intervention [for example, (50)]. For the development of the Irie Homes Toolbox, we developed a context-specific intervention while also learning while growing through iterative cycles of design, implementation, and evaluation with the results being used to continually improve the intervention. In developing an intervention specifically for the context, we transported and adapted evidence-based principles, rather than transporting an evidence-based program. This approach has several advantages. Firstly, the resultant intervention will be specific to the needs and context of the target group (51) and may lead to a more efficient intervention. For example, in a previous study of training Jamaican preschool teachers in child behavior management, we found that making substantial adaptations and additions to an evidence-based program (in this case the Incredible Years Teacher Training Program) led to a more efficient intervention, requiring less support, and supervision for participants, than when using a minimally adapted version (20). Secondly, there is a growing call for programs to be made freely available globally (52) and this is especially important in low and middle-income countries where the upfront and ongoing costs associated with many packaged programs are prohibitively high. Thirdly, there may also be challenges related to workforce capacity due to the need for highly skilled professionals to deliver some of these existing programs (53). The Irie Homes Toolbox was designed to be integrated into the existing preschool network and to be delivered by preschool teachers, many of whom are paraprofessionals. Fourthly, an intervention that has been developed in the context with participation from local stakeholders is likely to be more acceptable to participants, practitioners, and policy-makers. These factors suggest that transporting evidence-based principles and operationalising those principles for the setting may lead to an intervention that is more scalable and sustainable for that particular context (21).
The Irie Homes Toolbox incorporates the use of evidence-based behavior principles with a particular emphasis on behavior change principles that have been shown to be most valued by Jamaican preschool teachers in a complementary teacher-traning program. These behavior change principles include rehearsal and practice, positive feedback, group support, provision of materials, and ensuring sessions are fun and interactive (21). These methods are used extensively in the implementation of the Irie Homes Toolbox. The use of complementary content and methods of implementation across both the teacher and parent-training programs has several advantages including (1) promoting consistent use of strategies with children across home and school settings, and (2) making it easier for teachers to understand, adopt and implement the program with parents as it mirrors training that they have received. In addition, these interactive and practical training methodologies have been reported to be a key characteristic of effective early childhood parenting programs in LMIC in previous studies (49, 54–56).
The development and/or adaptation of interventions for use in LMICs often entail formative research (14, 57–60). Lachman et al. (36) developed a parenting program to address child maltreatment in South Africa by combining formative research with a theory driven approach that included identifying empirically-derived core components from the literature. To develop the Irie Homes Toolbox, we integrated data from three sources: (1) theory: including behavior change theory, the common core components of parenting programs and the core components used in the complementary teacher-training program, The Irie Classroom Toolbox, (2) formative research: seeking the perspectives of parents and teachers of preschool children, and (3) practice: repeatedly testing and revising the intervention under development with representatives from the beneficiary group. The intense piloting undertaken in this study as part of the intervention design provides the opportunity to pre-test every aspect of the intervention (content, process of delivery, structure, materials, recruitment, and engagement strategies) prior to wider-scale implementation to maximize the likelihood that it will be acceptable, feasible, relevant, and effective in the context. Enablers and barriers to the intervention's effectiveness were documented on an ongoing basis to ensure the intervention can be implemented in the real-world setting. In addition, the intervention was refined iteratively and collaboratively with the end users; incorporating the perspectives of the end users from the initial stages of design onwards increases the acceptability, feasibility, and relevance of the resultant intervention (61). During these learning cycles, we were able to identify problems, implement and evaluate possible solutions, and then implement the learning cycle again with the revised materials. These learning cycles continued until piloting of later drafts of the intervention resulted in little to no changes (29).
Following this development process, we now have an intervention that can be tested in a larger scale effectiveness trial. In the next phase of implementation, the program will be implemented by preschool teachers and supervised by government supervisors from the Early Childhood Commission. There will be a continued need for ongoing learning cycles to identify the strengths and needs of preschool teachers and government supervisors to implement the program and to identify the optimal levels of training and support to ensure the intervention maintains its effectiveness at scale. From a public health stand point, scaling up effective programs is critical to achieving population-level benefits in terms of reduced violence against children and reduced child externalizing behavior problems (62). However, few parenting interventions have been implemented successfully at scale, especially in LMIC, and paying attention to the scalability and effectiveness of an intervention from the design stage onwards is essential to wide-scale dissemination of effective programs. There were several decisions made in the development of the Irie Homes Toolbox to promote future scaling. Firstly, the Irie Homes Toolbox was designed as a complementary program to the Irie Classroom Toolbox. Preschool teachers who have been trained in the Irie Classroom Toolbox, and who are utilizing the strategies taught on a daily basis with children in their class, will deliver the Irie Homes Toolbox to groups of parents within their school. The Irie Classroom Toolbox is currently being disseminated nationally in Jamaica by the Early Childhood Commission, thus providing a strong foundation for the implementation of this intervention. Secondly, the Irie Homes Toolbox was designed to be relatively low cost, requiring few materials, or equipment. We choose not to rely on technology (e.g., video vignettes, audiotapes, presentations requiring a computer, or projector) and designed the sessions so that minimal resources were required. For example, all visual aids are hand-held so no flip-chart stand is required, and we used large pieces of cardboard placed on parents' laps to conduct child play activities rather than use a table. All materials required to implement the intervention are stored in a large, portable, plastic tub. Hence the sessions can be delivered across various locations within the school compound. Thirdly, throughout the development of the Irie Homes Toolbox, we continually revised and refined the intervention content, process of delivery, structure, and materials to promote its acceptability, feasibility, relevance, and effectiveness in the Jamaican early childhood education context. Although the intervention was developed specifically for the Jamaican context, the content, process of delivery, and materials of the program could be adapted to other LMICs. The Irie Homes Toolbox will be made available through a Creative Commons License to the global community.
The methods used in the development of the Irie Homes Toolbox are relevant for use in developing or adapting other educational and public health programs. We recommend an approach that integrates formative research, theory, empirically derived content and behavior change principles, with extensive piloting in the context. Throughout this process, ongoing attention should be given to ensuring the content, process of delivery, and materials used in the intervention meet the four key principles of acceptability, feasibility, relevance, and effectiveness. Figure 3 provides an overview of the key considerations involved in meeting these principles. Furthermore, it is important to engage the end users from the outset and to maintain their engagement throughout the development process. In addition, early consideration needs to be given to how, where, and by whom the intervention will be delivered as that will influence the design of the intervention. For an intervention to be suitable for use at scale, it is likely that it will need to be designed for use by an existing service, existing staff, and using low-cost materials. These factors have a strong effect on all four of the key principles of acceptability, relevance, feasibility, and effectiveness. Conducting a rigorous piloting and feasibility study of a new or adapted intervention prior to implementing an efficacy or effectiveness trial will ensure that the intervention fits the context, will assist in identifying the enablers and barriers to implementation thus maximizing the likelihood of success of the trial and the subsequent uptake of the intervention if is proven effective.
Data Availability Statement
The datasets generated for this article are not readily available because the data is mostly formative data and is not suitable for sharing as it is difficult to anonymise. Requests about datasets should be directed toaC5oZW5uaW5naGFtQGJhbmdvci5hYy51aw==.
Ethics Statement
The studies involving human participants were reviewed and approved by University of the West Indies, Ethics Committee and School of Psychology, Bangor University Ethics Committee. Written informed consent to participate in the study was provided by participating parents and teachers.
Author Contributions
HB-H and TF contributed to the conceptualization of the study, funding acquisition, project administration, investigation, data curation, data analysis, writing the original draft, and reviewing and editing the manuscript.
Funding
The development, implementation, and evaluation of the Irie Homes Toolbox was funded by Grand Challenges Canada (Saving Brains, seed grant) (Grant No. R-SB-POC-1707-08326).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the principals, teachers, parents, and children who participated in this study.
References
1. UNICEF. A Familiar Face: Violence in the Lives of Children and Adolescents. New York, NY: UNICEF (2017).
2. Straus MA, Hamby SL, Finkelhor D, Moore D, Runyan D. Identification of child maltreatment with the parent-child conflict tactics scales: development and psychometric data for a national sample of American parents. Child Abuse Negl. (1998) 22:249–70. doi: 10.1016/s0145-2134(97)00174-9
3. Wirtz AL, Alvarez C, Guedes AC, Brumana L, Modvar C, Glass N. Violence against children in Latin America and Caribbean countries: a comprehensive review of national health sector efforts in prevention and response. BMC Public Health. (2016) 16:1006. doi: 10.1186/s12889-016-3562-3
4. UNICEF. Hidden in Plain Sight: A Statistical Analysis of Violence against Children. New York, NY: UNICEF (2014). 200p.
5. Gershoff ET. Corporal punishment by parents and associated child behaviors and experiences: a meta-analytic and theoretical review. Psychol Bul. (2002) 128:539–79. doi: 10.1037/0033-2909.128.4.539
6. Ferguson CJ. Spanking, corporal punishment and negative long-term outcomes: a meta-analytic review of longitudinal studies. Clin Psychol Rev. (2013) 33:196–208. doi: 10.1016/j.cpr.2012.11.002
7. Gershoff ET, Grogan-Kaylor A. Spanking and child outcomes: old controversies and new meta-analyses. J Fam Psychol. (2016) 30:453–69. doi: 10.1037/fam0000191
8. Hillis S, Mercy J, Amobi A, Kress H. Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics. (2016) 137:e20154079. doi: 10.1542/peds.2015-4079
9. Chen M, Chan KL. Effects of parenting programs on child maltreatment prevention. Trauma Violence Abuse. (2015) 17:88–104. doi: 10.1177/1524838014566718
10. Mejia A, Haslam D, Sanders MR, Penman N. Protecting children in low- and middle-income countries from abuse and neglect: critical challenges for successful implementation of parenting programmes. Eur J Dev Res. (2017) 29:1038–52. doi: 10.1057/s41287-017-0105-4
11. Samms-Vaughan M, Lambert M. The impact of polyvictimisation on children in LMICs: the case of Jamaica. Psychol Health Med. (2017) 22:67–80. doi: 10.1080/13548506.2016.1274411
12. Lansford JE, Deater-Deckard K. Childrearing discipline and violence in developing countries. Child Dev. (2012) 83:62–75. doi: 10.1111/j.1467-8624.2011.01676.x
13. Jamaica. End Violence. (2019). Available online at: https://www.end-violence.org/impact/countries/jamaica (accessed October 20, 2019).
14. Baker-Henningham H. Transporting evidence-based interventions across cultures: using focus groups with teachers and parents of pre-school children to inform the implementation of the incredible years teacher training programme in Jamaica. Child Care Health Dev. (2011) 37:649–61. doi: 10.1111/j.1365-2214.2011.01208.x
15. Oveisi S, Ardabili HE, Dadds MR, Majdzadeh R, Mohammadkhani P, Rad JA, et al. Primary prevention of parent-child conflict and abuse in Iranian mothers: a randomized-controlled trial. Child Abuse Negl. (2010) 34:206–13. doi: 10.1016/j.chiabu.2009.05.008
16. Puffer ES, Green EP, Chase RM, Sim AL, Zayzay J, Friis E, et al. Parents make the difference: a randomized-controlled trial of a parenting intervention in Liberia. Glob Mental Health. (2015) 2:e15. doi: 10.1017/gmh.2015.12
17. Powell C, Baker-Henningham H, Walker S, Gernay J, Grantham-McGregor S. Feasibility of integrating early stimulation into primary care for undernourished Jamaican children: cluster randomised controlled trial. BMJ. (2004) 329:89. doi: 10.1136/bmj.38132.503472.7c
18. Chang SM, Grantham-McGregor S, Powell CA, Vera-Hernandez M, Lopez-Boo F, Baker-Henningham H, et al. Integrating a parenting intervention with routine primary health care: a cluster randomized trial. Pediatrics. (2015) 136:272–80. doi: 10.1542/peds.2015-0119d
19. Walker SP, Baker-Henningham H, Chang SM, Powell CA, Lopez-Boo F, Grantham-Mcgregor S. Implementation of parenting interventions through health services in Jamaica. Vulnerable Child Youth Stud. (2017) 13:127–41. doi: 10.1080/17450128.2017.1395100
20. Baker-Henningham H, Walker S. Effect of transporting an evidence-based, violence prevention intervention to Jamaican preschools on teacher and class-wide child behaviour: a cluster randomised trial. Glob Mental Health. (2018) 5:e7. doi: 10.1017/gmh.2017.29
21. Baker-Henningham H. The irie classroom toolbox: developing a violence prevention, preschool teacher training program using evidence, theory, and practice. Ann NY Acad Sci. (2018) 1419:179–200. doi: 10.1111/nyas.13713
22. Baker-Henningham H, Bowers M, Francis T, Vera-Hernandez M, Walker SP. The Irie Classroom Toolbox: a cluster randomised trial of a universal violence prevention programme in Jamaican preschools. Lancet Glob Health. (Submitted).
23. Baker-Henningham H, Scott Y, Bowers M, Francis T. Evaluation of a violence-prevention programme with Jamaican primary school teachers: a cluster randomised trial. Int J Environ Res Public Health. (2019) 16:2797. doi: 10.3390/ijerph16152797
24. Lannen P, Ziswiler M. Potential and perils of the early years: the need to integrate violence prevention and early child development (ECD+). Aggress Violent Behav. (2014) 19:25–628. doi: 10.1016/j.avb.2014.09.014
25. Phyfer J, Wakefield L. Calling for a comprehensive approach: violence prevention and early childhood development. S Afr Crime Q. (2016) 51:23–9. doi: 10.17159/2413-3108/2015/v0i51a769
26. Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu C, et al. Early childhood development coming of age: science through the life course. Lancet. (2017) 389:77–90. doi: 10.1016/s0140-6736(16)31389-7
27. Tomlinson M, Jordans M, MacMillan H, Betancourt T, Hunt X, Mikton C. Research priority setting for integrated early child development and violence prevention (ECD+) in low and middle income countries: an expert opinion exercise. Child Abuse Negl. (2017) 72:131–9. doi: 10.1016/j.chiabu.2017.07.021
28. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:a1655 doi: 10.1136/bmj.a1655
29. O'Cathain A, Croot L, Duncan E, Rousseau N, Sworn K, Yardley L, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open. (2019) 9:e029954. doi: 10.1136/bmjopen-2019-029954
30. Webster-Stratton C. The incredible years: parents, teachers, and children training series. Resid Treat Child Youth. (2001) 18:31–45. doi: 10.1300/j007v18n03_04
31. Sanders MR. Triple P-positive parenting program: towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clin Child Fam Psychol Rev. (1999) 2:71–90. doi: 10.1023/a:1021843613840
32. Forgatch MS, Patterson GR. Parent management training—oregon model: an intervention for antisocial behavior in children and adolescents. In: Weisz JR, Kazdin AE, editors. Evidence-Based Psychotherapies for Children and Adolescents. New York, NY: The Guilford Press (2010). p. 159–77.
33. Eyberg S. Parent-child interaction therapy: integration of traditional and behavioural concerns. Child Fam Behav Ther. (1998) 10:33–46. doi: 10.1300/j019v10n01_04
34. Brotman LM, Dawson-McClure S, Calzada EJ, Huang KY, Kamboukos D, Palamar JJ, et al. Cluster (school) RCT of parentcorps: impact on kindergarten academic achievement. Pediatrics. (2013) 131:e1521–9. doi: 10.1542/peds.2012-2632
35. Silva J. Parents Raising Safe Kids: ACT 8-Week Program for Parents. Washington, DC: American Psychological Association (2007).
36. Lachman JM, Sherr LT, Cluver L, Ward CL, Hutchings J, Gardner F. Integrating evidence and context to develop a parenting program for low-income families in South Africa. J Child Fam Stud. (2016) 25:2337–52. doi: 10.1007/s10826-016-0389-6
37. Santini PM, Williams LCA. A randomized controlled trial of an intervention program to Brazilian mothers who use corporal punishment. Child Abuse Negl. (2017) 71:80–91. doi: 10.1016/j.chiabu.2017.04.019
38. Kaminski JW, Valle LA, Filene JH, Boyle CL. A meta-analytic review of components associated with parent training program effectiveness. J Abnorm Child Psychol. (2008) 36:567–589. doi: 10.1007/s10802-007-9201-9
39. Garland AF, Hawley KM, Brookman-Frazee L, Hurlburt MS. Identifying common elements of evidence-based psychosocial treatments for children's disruptive behavior problems. J Am Acad Child Adolesc Psychiatry. (2008) 47:505–14. doi: 10.1097/chi.0b013e31816765c2
40. Leijten P, Gardner F, Melendez-Torres GJ, van Aar J, Hutchings J, Schulz S, et al. Meta-analyses: key parenting program components for disruptive child behavior. J Am Academy Child Adolesc Psychiatry. (2019) 58:180–90. doi: 10.1016/j.jaac.2018.07.900
41. Melendez-Torres GJ, Leijten P, Gardner F. What are the optimal combinations of parenting intervention components to reduce physical child abuse recurrence? reanalysis of a systematic review using qualitative comparative analysis. Child Abus Rev. (2019) 28:181–97. doi: 10.1002/car.2561
42. Temcheff CE, Letarte MJ, Boutin S, Marcil K. Common components of evidence-based parenting programs for preventing maltreatment of school-age children. Child Abuse Negl. (2018) 80:226–37. doi: 10.1016/j.chiabu.2018.02.004
43. van der Put CE, Assink M, Gubbels J, Boekhout van Solinge NF. Identifying effective components of child maltreatment interventions: a meta-analysis. Clin Child Fam Psychol Rev. (2017) 21:171–202. doi: 10.1007/s1056-017-0250-5
44. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:1. doi: 10.1186/1748-5908-6-42
45. Walker SP, Chang SM, Smith JA, Baker-Henningham H, the Reach Up Team. The reach up early childhood parenting program: origins, content and implementation. Zero To Three. (2018) 38:37–43. Available online at: https://www.bluetoad.com/publication/?i=483158&article_id=3040796&view=articleBrowser
46. Baker-Henningham H, Vera-Hernández M, Alderman H, Walker S. Irie classroom toolbox: a study protocol for a cluster-randomised trial of a universal violence prevention programme in Jamaican preschools. BMJ Open. (2016) 6:e012166. doi: 10.1136/bmjopen-2016-012166
47. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Huberman M, Miles H, editor. The Qualitative Researcher's Companion. London: Sage Publications (2002). p. 305–29.
48. Baker-Henningham H. The role of early childhood education programmes in the promotion of child and adolescent mental health in low- and middle-income countries. Int J Epidemiol. (2014) 43:407–33. doi: 10.1093/ije/dyt226
49. Smith JA, Baker-Henningham H, Brentani A, Mugweni R, Walker SP. Implementation of reach up early childhood parenting program: acceptability, appropriateness, and feasibility in Brazil and Zimbabwe. Ann NY Acad Sci. (2018) 1419:120–40. doi: 10.1111/nyas.13678
50. Nores M, Figueras-Daniel A, Lopez MA, Bernal R. Implementing aeioTU: quality improvement alongside an efficacy study-learning while growing. Ann NY Acad Sci. (2018) 1419:201–17. doi: 10.1111/nyas.13662
51. Leijten P, Melendez-Torres GJ, Knerr W, Gardner F. Transported versus homegrown parenting interventions for reducing disruptive child behavior: a multilevel meta-regression study. J Am Acad Child Adolesc Psychiatry. (2016) 55:610–7. doi: 10.1016/j.jaac.2016.05.003
52. Michie S, Fixsen D, Grimshaw JM, Eccles MP. Specifying and reporting complex behaviour change interventions: the need for a scientific method. Implement Sci. (2009) 4:40 doi: 10.1186/1748-5908-4-40
53. Mikton C. Two challenges to importing evidence-based child maltreatment prevention programs developed in high-income countries to low- and middle-income countries: Generalizability and affordability. In: Dubowitz H, editor. World Perspectives on Child Abuse. Aurora, CO: International Society for the Prevention of Child Abuse and Neglect (2012). p. 97.
54. Yousafzai AK, Aboud F. Review of implementation processes for integrated nutrition and psychosocial stimulation interventions. Ann NY Acad Sci. (2014) 1308:33–45. doi: 10.1111/nyas.12313
55. Yousafzai AK, Rasheed MA, Siyal S. Integration of parenting and nutrition interventions in a community health program in Pakistan: an implementation evaluation. Ann NY Acad Sci. (2018) 1419:160–78. doi: 10.1111/nyas.13649
56. Singla DR, Kumbakumba E. The development and implementation of a theory-informed, integrated mother-child intervention in rural Uganda. Soc Sci Med. (2015) 147:242–51. doi: 10.1016/j.socscimed.2015.10.069
57. Mejia A, Calam R, Sanders MR. Examining delivery preferences and cultural relevance of an evidence-based parenting program in a low-resource setting of central America: approaching parents as consumers. J Child Fam Stud. (2014) 24:1004–15. doi: 10.1007/s10826-014-9911-x
58. Alampay LP, Lachman JM, Landoy BV, Madrid BJ, Ward CL, Hutchings J, et al. Preventing child maltreatment in low-and middle-income countries: parenting for lifelong health in the Philippines. In: Verma S, Petersen, editors. Developmental Science and Sustainable Development Goals for Children and Youth. Springer, Cham: Social Indicators Research Series (2018). p. 277–92.
59. Sensoy Bahar O, Byansi W, Kivumbi A, Namatovu P, Kiyingi J, Ssewamala FM, et al. From “4Rs 2Ss” to “Amaka Amasanyufu” (Happy Families): adapting a US based evidence based intervention to the Uganda context. Family Process. (2020). doi: 10.1111/famp.12525
60. Baker-Henningham H, Walker S. A qualitative study of teacher's perceptions of an intervention to prevent conduct problems in Jamaican pre-schools. Child Care Health Dev. (2009) 35:632–42. doi: 10.1111/j.1365-2214.2009.00996.x
61. Croot L, O'Cathain A, Sworn K, Yardley L, Turner K, Duncan E, et al. Developing interventions to improve health: a systematic mapping review of international practice between 2015 and 2016. Pilot Feasibility Stud. (2019) 5:127. doi: 10.1186/s40814-019-0512-8
Keywords: violence prevention, parent training, intervention development, early childhood, behavior change, low-and middle-income country
Citation: Francis T and Baker-Henningham H (2020) Design and Implementation of the Irie Homes Toolbox: A Violence Prevention, Early Childhood, Parenting Program. Front. Public Health 8:582961. doi: 10.3389/fpubh.2020.582961
Received: 13 July 2020; Accepted: 06 October 2020;
Published: 16 November 2020.
Edited by:
Jane Fisher, Monash University, AustraliaReviewed by:
Stacie Craft DeFreitas, University of Houston–Downtown, United StatesJoshua Jeong, Harvard University, United States
Copyright © 2020 Francis and Baker-Henningham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helen Baker-Henningham, aC5oZW5uaW5naGFtQGJhbmdvci5hYy51aw==