 Zeinab A. Kasemy1*
Zeinab A. Kasemy1* Eman E. Abd-Ellatif2
Eman E. Abd-Ellatif2 Asmaa A. Abdel Latif3
Asmaa A. Abdel Latif3 Nadia M. Bahgat4Hanaa Mohammad Abo Shereda5Safaa Ibrahim Shattla5Samira E. Aboalizm6Asmaa Hamed Abd Elhy6Abeer R. Allam7Ahmed N. Ramadan7Hemat Mostafa Amer8Naglaa Abdelmawgoud Ahmed8
Nadia M. Bahgat4Hanaa Mohammad Abo Shereda5Safaa Ibrahim Shattla5Samira E. Aboalizm6Asmaa Hamed Abd Elhy6Abeer R. Allam7Ahmed N. Ramadan7Hemat Mostafa Amer8Naglaa Abdelmawgoud Ahmed8 Abobakr A. AlJifri9Mervat M. El Dalatony3
Abobakr A. AlJifri9Mervat M. El Dalatony3- 1Department of Public Health and Community Medicine, Faculty of Medicine, Menoufia University, Shibin Al Kawm, Egypt
- 2Department of Public Health and Community Medicine, Faculty of Medicine, Mansoura University, Mansoura, Egypt
- 3Industrial Medicine and Occupational Health Division of Public Health and Community Medicine Department, Menoufia Faculty of Medicine, Shibin Al Kawm, Egypt
- 4Department of Anesthesiology and Intensive Care, Faculty of Medicine, Menoufia University, Shebeen El-Kom, Egypt
- 5Department of Psychiatric and Mental Health Nursing, Faculty of Nursing, Menoufia University, Shibin Al Kawm, Egypt
- 6Department of Medical Surgical Nursing, Faculty of Nursing, Menoufia University, Shibin Al Kawm, Egypt
- 7Department of Neuropsychiatry, Faculty of Medicine, Menoufia University, Shibin Al Kawm, Egypt
- 8Department of Family and Community Health Nursing, Faculty of Nursing, Menoufia University, Shibin Al Kawm, Egypt
- 9Department of Quality and Patient Safety in Healthcare, Private Hospital Riyadh, Jordan University of Science and Technology, Irbid, Jordan
Introduction: Work is a social double edged weapon activity that may have positive and negative effects on individual's quality of life and health.
Objectives: To estimate workaholism prevalence and to determine its effects on quality of life, mental health, and burnout among healthcare workers (HCWs).
Methods: Using a cross-sectional study, 1,080 Egyptian participants distributed as HCWs and non-HCWs were recruited. The study included 4 questionnaires to assess workaholism, quality of life (QoL), Psychological capital questionnaire (PCQ), and General health questionnaire (GHQ). Maslach Burnout Inventory (MBI) was applied to critical specialty HCWs in addition to pro-inflammatory markers including Il6, TNFα, and CoQ10.
Results: This study revealed that 24.4 and 24.8% of HCWs were workaholic and hardworking, respectively, in comparison to 5.9 and 28.1% among non-HCWs (P < 0.001). Somatic symptoms and anxiety/ insomnia domains of GHQ were higher among HCWs than non-HCWs (P < 0.001 and 0.002, respectively). QoL was significantly lower among HCWs than non-HCWs (P < 0.001). Workaholism was reported among 43.2% of HCWs with critical specialty (P < 0.001). Components of PCQ components were significantly higher among HCWs with critical specialty than non-critical HCWs while QoL showed the reverse (P < 0.05). Working excessively was a predictor to burnout [Emotional exhaustion (β = –0.23) and depersonalization (β = −0.25)] and TNFα (β = 0.41). Emotional exhaustion was a predictor to Il6 (β = 0.66), TNFα (β = 0.73), and CoQ10 (β = −0.78).
Conclusion: There is a significant association between workaholism and psychologically poor-health and poor quality of life among HCWs. Critical specialty healthcare workers showed association between workaholism, burnout and pro-inflammatory markers. Addressing of personal characteristics, supporting factors in the work environment and periodic examination of the healthcare workers and responding accordingly is required.
Introduction
Work is a social double edged weapon activity that may have positive and negative effects on individual's life and health (1). In the 1970s, it was the first time to introduce the term “Workaholism” describing a constant need to work which can harm health physically, mentally, psychologically and socially (2, 3). Andreassen et al. (4) defines workaholism (Work addiction) as becoming too anxious, strongly motivated by work, and spending huge efforts into your work leading to social, physical, psychological health impairment. Workaholism has a set of two characteristics occurring together: Working excessively (WE) (behavioral component) and working compulsively (WC) (cognitive component) (5).
In situations that require higher efforts to attain the expected level of performance, job demands might become stressors affecting the entire human life (6). Quality of life (QoL) is how a person perceives his place in life in a frame of culture affecting his objectives, expectations, standards and fears (7). QoL could be affected by many factors like the individual's physical and psychological status, personal beliefs, social relations, and its related prominent environmental features. Epidemiological studies highlighted the negative impacts of overworking on the risks of cardiovascular disorders, fatigue, stress, depression, anxiety, sleeping quality, alcoholism and smoking, mental health status, hypertension, musculoskeletal disorders, and health behaviors in addition to poor quality of life (8–11).
Healthcare providers of different ages are usually highly concerned with their jobs leading to workaholism (12). They are more susceptible to stress and burn-out which is physical, emotional, mental, and spiritual exhaustion as they are in charge of human lives (13, 14). Some researchers suppose that burnout syndrome is a variant of depression (15).
There is strong evidence that depression is accompanied by an increase of proinflammatory cytokines e.g., interleukin-1 (IL-1), IL-2, IL-6, tumor necrosis factor-α (TNFα), and acute phase proteins (16). Coenzyme Q10 (CoQ10) is an antioxidant that has anti-inflammatory effects and lower levels of CoQ10 have been associated with depression in patients (17). Much of the interest in inflammation and depression has been focused on cytokines, which mediate the innate immune response, including tumor necrosis factor alpha (TNF-α), and IL-6, which appears to be one of the most reliable peripheral biomarkers in major depression (18).
Developing an environment promoting resilience for HCWs limits negative, and elevates positive, outcomes of stress in healthcare settings. Optimism is needed for HCWs to see the world as a positive place, accepting and handling difficulties as a challenge not a barrier and as a consequence this will improve their functioning level, patients' satisfaction, and therapeutic outcome.
According to authors' knowledge, no published articles reported the percentage of workaholism among Egyptian healthcare workers. This work aimed to 1- Estimate workaholism prevalence and to determine its effects on quality of life and mental health among healthcare workers (HCWs) 2- Study the relation between workaholism and burnout and their association to pro-inflammatory markers including IL6, TNFα, and Coenzyme Q10 among critical specialty healthcare workers.
Methods
Using a cross-sectional study, 1,080 participants distributed as HCWs and non-HCWs were recruited. Self-administered questionnaires were used by a team of trained personnel. The trained team members chose the non-crowding days of work and time of rest of HCWs to encourage them to share and to avoid any extra load on them. HCWS of four different hospitals were interviewed. HCWs included physicians and nurses with critical (departments of Surgery, Anesthesia and ICU) and non-critical specialties. For the non-HCWs group, the trained personnel directed their efforts to the administrative board in the involved hospitals of the HCWs and 3 governmental and 2 private sectors to gain wide sharing. The questionnaires were left to be filled in for HCWs and then collected later at an appropriate time while the non-HCWs the trained team collected the data immediately by an interviewer based questionnaire.
Exclusion Criteria
Any person refused to share or wanted to withdraw at any point of the research was excluded from the study.
Sample Size
As the frequency of workaholism among Egyptians healthcare workers (HCWs) was not studied before so the occurrence probability equaled to its non-occurrence (p =q = 0.5) and with acceptable limit of precision (D) of 0.03 value, the sample size was estimated to be 1,014 participants divided into 2 groups; HCWs and non-HCWs. To avoid drop out, the sample has increased to 1,126. About 1,126 questionnaires were delivered to both groups in equal numbers. HCWs responded to 540 questionnaires out of 563 ones with a response rate of 95.9%. Non-HCWs group responded to 544 questionnaires with a response rate of 96.6%. Four incomplete questionnaires were excluded leaving 540 ones.
Tools
The study included 4 questionnaires to assess workaholism, quality of life, Psychological capital components, and General health questionnaire:
I. The adapted version of the Dutch Workaholism Scale (DUWAS) (19): It contains 10 items of a 4-point scale with a range from 1–4 (Almost never to always); the questionnaire included two equally divided scales: working excessively (WE) and working compulsively (WC). The cutoff point was 2.5 in both scales. More than 2.5 in both scales (WE and WC) equaled workaholic. Above 2.5 (WE) and below 2.5 (WC) equaled hard worker. Below 2.5 (WE) and above 2.5 (WC) equaled compulsive worker. Less than 2.5 in both of (WE and WC) equaled relaxed worker were defined as (5, 20, 21).
II. World Health Organization Quality-of-Life Scale (WHOQOL-BREF) (22): a twenty six item revised version was used. It fits most of geographical, ethnic background, and cultural aspects. It consists of 4 categories; physical (R = 7–35), mental (R = 6–30), social(R = 3–15), and environmental (R = 8–40) well-being over the past 4 weeks. Low score means Low QOL. The range of reliability test in WHOQOL-BREF is 0.70–0.80.
III. Psychological capital Questionnare (PCQ-12): (Short form) of the Psychological Capital Questionnaire (PCQ-24). It includes four subscales titled self-efficacy (item numbers 1–4), hope (item numbers: 5–7), resilience (item numbers 8–10), and optimism (item numbers 11–12). A Likert 6 point scale ranging from 1: Strongly disagree, to 6: Strongly agree was used (23–25).
IV. General Health questionnaire (GHQ-28): Four subscales were used to measure the general health state: somatic symptoms, anxiety/insomnia, social dysfunction and symptoms of depression. To rate recent psychological state, a Likert 4 point scale ranging from (1: Not at all, to 4: Much more than usual) was used. Low score means good psychological status (26).
Healthcare Workers Who Were Working in Critical Specialty (Departments of Surgery, Anesthesia, and ICU) Were Studied Regarding
1. Burnout using the Maslach Burnout Inventory (MBI) which is a Likert scale questionnaire, the answer of each question ranged from never = 0 to everyday = 6. It contains 22 items divided into three subscales: emotional exhaustion (EE 9 items, R = 0–≥27) depersonalization (DP 5 items, R = 0–≥13) and personal accomplishment (PA 8 items, R = ≥ 37–0) (27).
2. Blood samples were collected after 8 h of fasting at the early morning. Blood samples were taken by sterile syringe from each participate. 3–4 cm venous blood collected in plan tube and centrifugated. Finally supernatants were removed and stored at −80 °C until determination via ELISA kits. These investigations were used for assessing biomarkers of depression including Interleukin 6 (IL-6) (ELISA KIT‘, Sino Gene Clon Biotech Co.,Ltd, Detection range 4.7 ng/L −800 ng/L), Tumor necrosis factor alpha, TNF-α (ELISA KIT‘, Sino Gene Clon Biotech Co.,Ltd, Detection range 15.6 ng/L −1,000 ng/L) and Coenzyme Q10 (CoQ10) (ELISA Kit, Sino Gene Clon Biotech Co.,Ltd, Detection range: 1.56 ng/ml −50 ng/ml).
Ethical Approval
Approval of the local institutional research board was obtained.
Statistical Analysis
SPSS version 22(SPSS Inc., Chicago, IL, USA) was used to analyze the data. Qualitative data were expressed as no and %, while quantitative data were expressed as mean ±SD. Test of normality was conducted. Non-paired t-test was used to compare between 2 means of normally distributed variables while ANOVA test was used to compare between means of more than 2 groups for normally distributed variables. For analysis of non-parametric data, Mann-Whitney was used between 2 groups while a Kruskal-Wallis test was employed to compare between more than 2 groups. Qualitative variables were analyzed by Chi-Squared (χ2). A Pearson correlation test was used to assess direction and strength of association between quantitative variables. Multiple regression analysis using pathway analysis was applied to detect the predictors between dependent and independent variables. Significance level was set at P < 0.05.
Results
Workaholism was reported in 24% of HCWs and while it was 17.9, 31.9, and 41.7% in Nonnis et al. (21), Schaufeli et al. (33), and Schaufeli et al. (5), respectively (P < 0.001) (Figure 1).
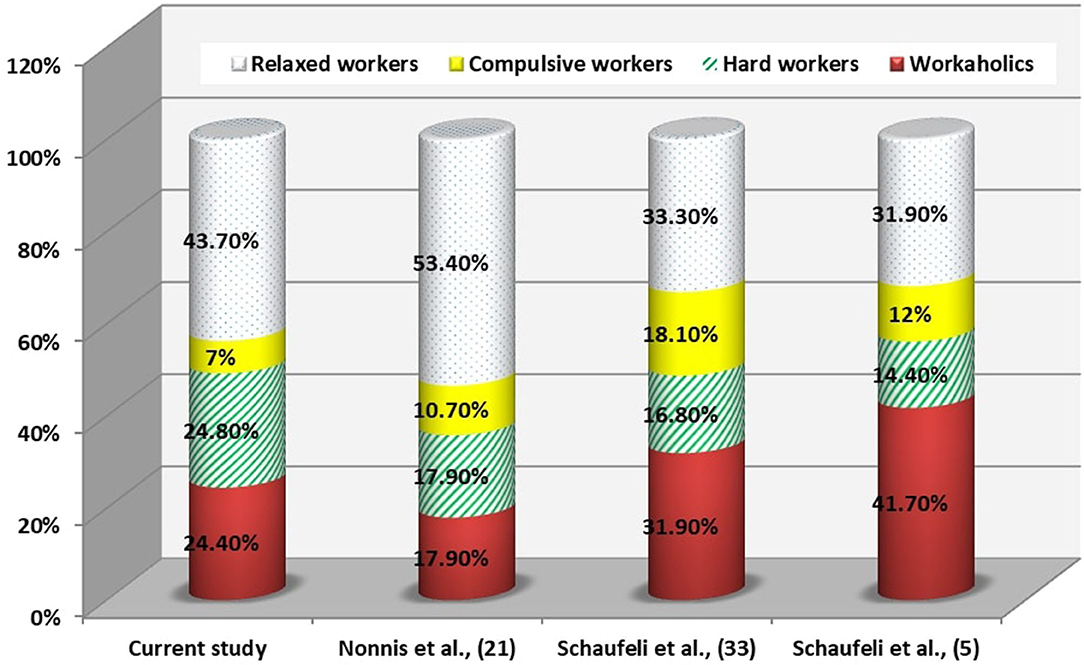
Figure 1. Comparison of the profiles of the current study with other research in health care.
Correlation analysis between scores of the entire studied group working excessively or compulsively revealed that there was a positive correlation with GHQ and PCQ items while there was a negative correlation with the quality of life (P < 0.05). Working excessively and compulsively were not predictors to GHQ but strong predictors to quality of life and PCQ components (Figures 2–4).

Figure 2. Path diagram of the model used for the whole group of subjects for work addiction scores and GHQ (n = 1,080) (Multiple regression analysis using pathway analysis was applied). *significant.
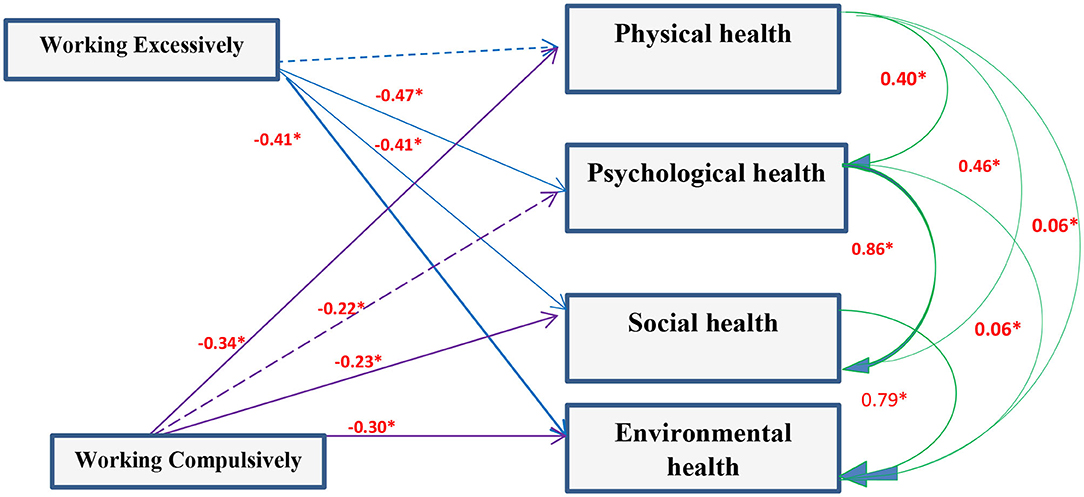
Figure 3. Path diagram of the model used for the whole group of subjects for work addiction scores and Quality of life (n = 1,080) (Multiple regression analysis using pathway analysis was applied). *significant.
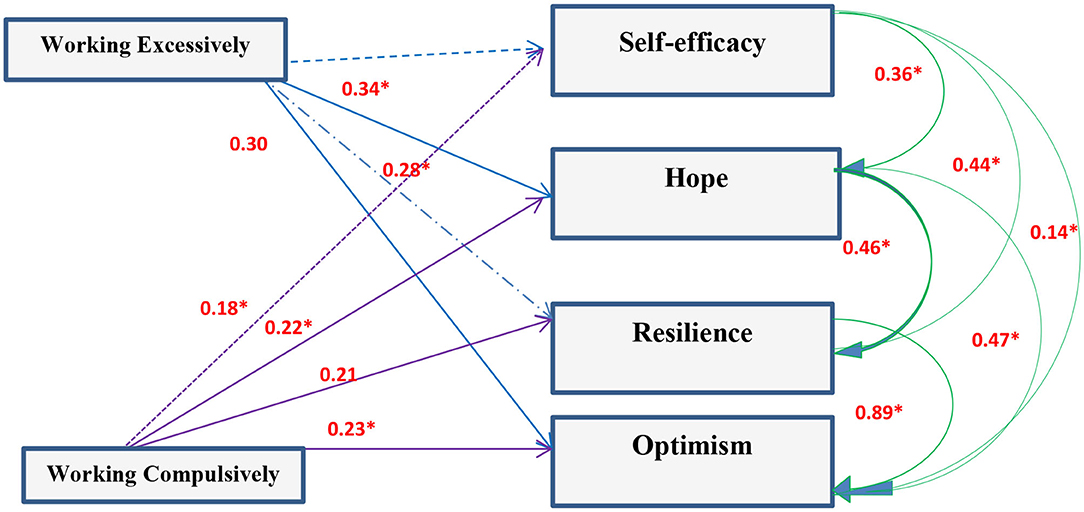
Figure 4. Path diagram of the model used for the whole group of subjects for work addiction scores and Psychological capital components (n = 1,080) (Multiple regression analysis using pathway analysis was applied). *significant.
Working excessively was a predictor to burnout (emotional exhaustion (β = −0.23, CI 95%: 0.03–1.60) and depersonalization (β = −0.25, CI 95%: 0.05–0.94) and TNFα (β = 0.41, CT 95%: 8.73–26.84). Emotional exhaustion was a predictor to Il6 (β = 0.66, CI 95%: 4.25–8.08), TNFα (β = 0.73, CI 95%: 6.64–11.36), and CoQ10 [β = −0.78, CI 95%: −0.55–(−0.35)] (Figure 5).
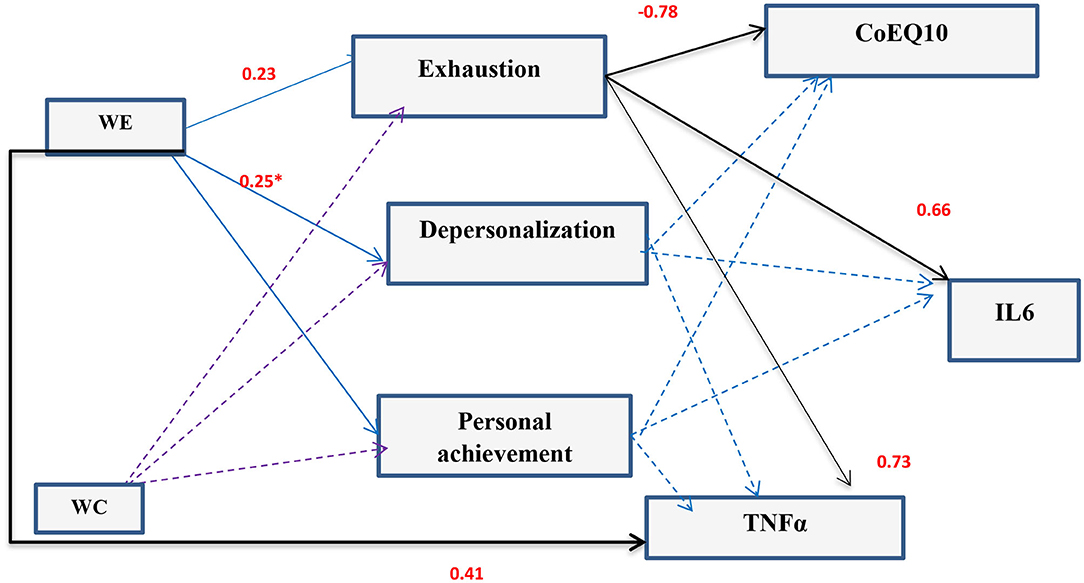
Figure 5. Path diagram of the model used for the whole critical specialty HCWs group for work addiction scores and burnout and pro-inflammatory markers (n = 81) (Multiple regression analysis using pathway analysis was applied). *significant.
Working >48 h/week was highly prevalent among HCWs (54.1%) in comparison to non-HCWs (36.3%) and about 73.3% HCWs don't take a weekend. The study revealed that 24.4% of HCWs were workaholic and 24.8% were hardworking in comparison to 5.9 and 28.1%, respectively, among non-HCWs (P < 0.001). GHQ results were higher among HCWs than among non-HCWs especially the somatic symptoms and anxiety/ insomnia (P < 0.001 and 0.002, respectively). HCWs had significantly lower quality of life than non-HCWs (P < 0.001) but there was no significant difference regarding PCQ components (P > 0.05). The comparison between physicians and nurses revealed that 86.8% of physicians don't take a weekend in comparison to nurses (23.5%). While 2.8% of the physician were relaxed workers, 64.9% of the nurses were relaxed workers (P < 0.001). GHQ results were higher and that of QOL were lower among physician than nurses (P < 0.001). Regarding PCQ components, all of them were significantly higher among physicians than nurses (P < 0.001). When studying the specialty of HCWS, it was found that critical specialty had significantly higher working hours and no weekends in comparison to non-critical specialty. Also QOL was significantly lower while PCQ components were significantly higher among HCWs with critical specialty (Table 1).
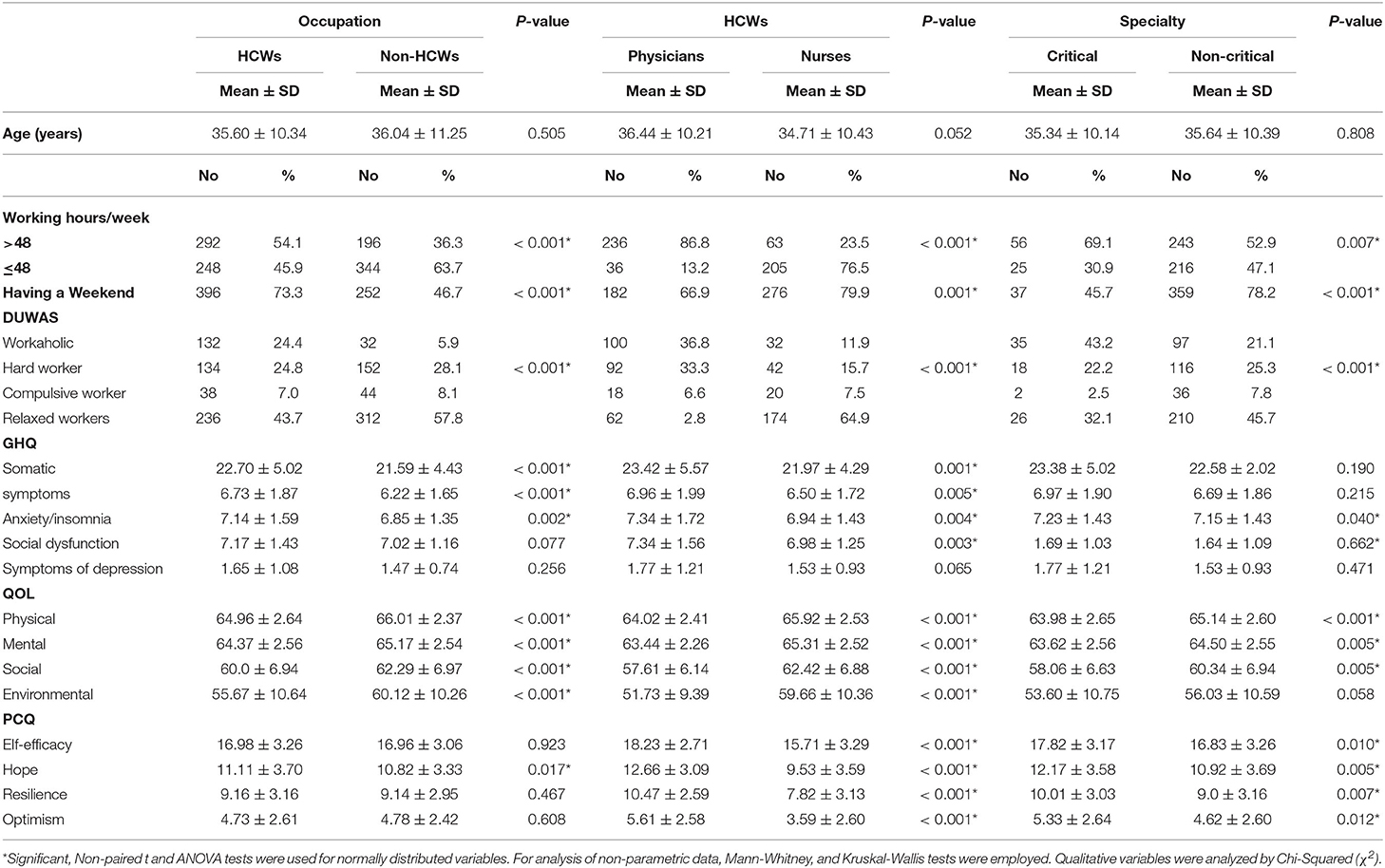
Table 1. Distribution of Dutch Workaholism Scale (DUWAS), General health questionnaire (GHQ), Quality of life (QOL), and Psychological capital components (PCQ) regarding occupation.
The young age groups showed more working hours than old age ones (P < 0.001). Workaholism and working hard were reported among 20.7% among young ages in comparison to 8% among old one (P < 0.001). Results of GHQ and PCQ components were significantly higher among young ages than old ones while QOL showed the reverse (P < 0.001). Males are working more hours than females. Males were workaholic (17.7%) in comparison to 11.9% among females. Results of GHQ and PCQ components were higher among males than females while QOL showed the reverse (Table 2).
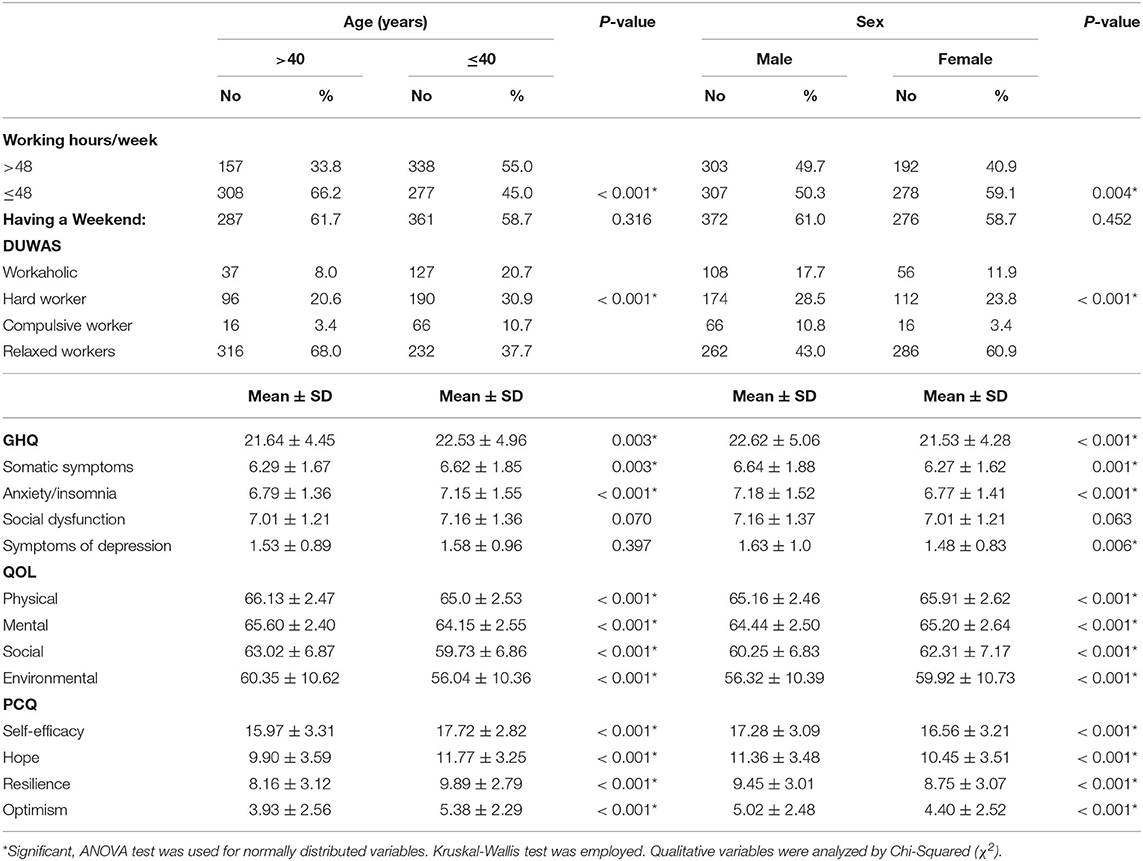
Table 2. Distribution of Distribution of Dutch Workaholism Scale (DUWAS), General health questionnaire (GHQ), Quality of life (QOL), and Psychological capital questionnaire (PCQ) regarding age and sex of the studied group.
Discussion
Workaholism seems to be challenge functioning as a resource and a demand for healthcare workers (HCWs) (28). The potential to energize workers makes workaholism able to create pleasure in work, hence more job satisfaction with positive emotional effects (29). A health impairment psychological process and feeling of emotional exhaustion among HCWs may be achieved at higher levels of workaholism causing a so-called “loss spiral” and hence job dissatisfaction (29–32).
Prevalence of Workaholosm
In the current study, workaholism among HCWs represented 24%. It is lower than that of Schaufeli et al. (33) and Schaufeli et al. (5) In the Netherlands and Japan which was 41.7 and 31.9%, respectively. Hu et al. (34) explained this variation by the tendency of employees in the Western cultures to be more work engaged than their peers in the Eastern cultures. But the current results were higher than that of Nonnis et al. (21) in Italy which was 17.9%. There are many factors could affect workaholism as gender, personality, cultural values within the countries but regardless of cultures, workaholism is injurious to the employees' well-being. Work addiction could be explained by the compulsive need to achieve status and success or to escape emotional stress. Hard work and diligence are known as desirable traits among physicians. It is common among people described as perfectionists who are at risk of the belief that the best is never good enough and this is concerning as HCWs' well-being is essential to ensure high quality healthcare services (35). Prevalence of workaholism among non-HCWs was 5.9% in the current results which is lower than a study carried out in Norway (4). The prevalence rates of workaholism ranging from 0.3 to 46.6% depending of the cut-off employed. In the present study an endorsement of at least 2.5 as the cut-off was used, and is in line with the authors' previous suggestion (20, 21).
Relation Between Workaholism, Mental Health, and Quality of Life
Analysis of the correlation between scores of the entire studied group and working excessively or compulsively showed that there was positive correlation with GHQ and Psychological capital items while there was negative correlation with quality of life. There is an association between workaholism and ill-health whether psychologically or physically (5, 36). Working compulsively has a cognitive pattern making individuals work hard leading to physical or mental exhaustion (29, 37). Hard work and diligence are known as desirable traits among physicians. Developing an environment promoting resilience for HCWs limits negative, and elevates positive, outcomes of stress in healthcare settings. Optimism is needed for HCWs to see the world as a positive place, accepting and handling difficulties as a challenge not a barrier and as a consequence this will improve their functioning level, patients' satisfaction, and therapeutic outcome. So working hard is associated with strong hope, resilience, and optimism (38–40).
The present findings reported that working excessively is more likely to be associated with psychophysical exhaustion and this agrees with Delgado et al. (35) and Andreassen et al. (41). Physical, mental, social, and environmental domains of quality of life were significantly different between HCWs and non-HCWs and also between physicians and nurses. Workaholism is associated with better health through active coping, and with poor health through emotional discharge.
The present association between workaholism and psychological ill health agrees with many studies (20, 42–45). There were great similarities between participants working excessively and compulsively regarding psychological distress, psychosomatic symptoms, job stress and impaired well-being (20, 46–48). On the base of above/below dichotomy Buelens and Poelmans (28), compared 8 groups of workers regarding work involvement, drive, and work enjoyment (3 workaholism dimensions). Work addicts had high scores in work involvement and drive, and low scores on enjoyment in addition to unfavorable scores on work-to-family conflict, work conflict, satisfaction with family and colleagues, and stress and health complaints in comparison with relaxed workers. Schaufeli et al. (33) found that engaged peers of workaholic managers were more satisfied with their jobs and less psychologically distressed. Dissimilarities between excessive and compulsive workers lie in perfectionism sought by the compulsive working group (49). Porter (50) explained poor social relationships at work by anger and frustration characterizing perfectionist workaholics and this could explain the relatively low positive correlation with PCQ among the working compulsively group in contrast to the working excessively one.
The current results revealed that across several occupations there is an association between workaholism and psychological health. In the same context, positive correlations were found between workaholism, and work overload and number of working hours (20, 47). Critical specialty seems to suffer from workaholism and its associated low QOL and high PCQ components. Especially when enjoying their work, participants experiencing great professional demands, may find difficulty in setting limits for themselves. So to reduce this risk and ensure maintain of a good work-life balance, managers should build supportive environment to all employees (51, 52).
Workaholics tend to have long working hours interfering with family and personal lives. HCWs suffer mental demands (large quantities of information with complicated decisions), organizational demands (working in a complex organizational environment), and emotional demands (dealing with suffering patients and their families). In addition, some demographic variables like gender and age may facilitate or deter workaholism. According to the present study findings, males are more workholics than females. This agrees with Burke and Koksal [48], and could be demonstrated by tendency of males to work longer hours (53). The reverse was found by Buelens and Poelmans (28) while Porter (50) failed to find a difference. In the present study, workaholism correlated with younger age group and this could be explained by the wise up experienced at old ages besides adjustment the work pattern due to being committed (e.g., having a family). This agrees with Andreassen et al. (54) and Taris et al. (55).
Relation Between Workaholism and Burnout and Inflammatory Markers
The present results showed that working excessively was a predictor to burnout (Emotional exhaustion and depersonalization) and this agrees with Nonnis et al. (2). It seems that workaholics over time are more vulnerable to quit working to a higher degree than non-workaholics. On studying burnout among HCWs with critical specialty, the results revealed that burnout is a strong predictor to pro-inflammatory cytokines TNF-α, IL6, and CoQ10. This agrees with some studies (16, 56, 57). Through their action on the brain, they cause behavioral symptoms of sickness like fatigue, sleepiness, loss of appetite and decreased libido (57). On the other hand, the enzymatic antioxidants level (co-enzyme Q10) decreased in depressed patients (58, 59). Recently researches prove that lower CoQ10 plays a role in the pathophysiology of depression. It is suggested that depressed patients may benefit from CoQ10 supplementation (58).
Strengths and Limitations
The present study was conducted in Egypt, thus the findings cannot necessary be generalized to workers from other countries. The work did not focus on the type of work whether organizationally employed or self-employed giving some limits on the possible covariates that may be associated with work addiction. The study was a cross-sectional one, so no conclusions can be drawn in terms of cause-and-effect relationships between study variables. Furthermore, all data were based on self-report and there is no gold standard for assessment of workaholism so this is a point of debate (60). Despite these limitations, there are points of strength. The work is (to the best of the authors' knowledge) the first to assess workaholism in a representative sample of workers in Egypt. The study included questionnaires and laboratory investigations to assess the association between work addiction and mental health in addition to burnout. As noted, the response rate (96.60%) is so acceptable. The study included 1,080 participants which provides high statistical power and consequently decreases the probability of Type 2 errors (61).
Conclusion
There is a significant association between workaholism and psychologically poor-health and poor quality of life among HCWs. Critical specialty healthcare workers showed association between workaholism, burnout, and pro-inflammatory markers. Addressing of personal characteristics, supporting factors in the work environment and periodic examination of the healthcare workers and responding accordingly is required.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional research board at Menoufia Faculty of Medicine, Egypt. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. ZK had the role of getting the idea, performing statistical analysis, writing the methodology and results sections, final revision, and publishing. ME had the role of writing the manuscript (Introduction) and conducting revision. EA-E, AAb, NB, HAb, SS, SA, AHA, ARA, HAm, NA, and AR collected data and share in writing (Methods: choice of tools and Discussion) and revision of the manuscript. AAl conducted the revision and editing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Special thanks to Dr. Heba K. Allam, Assistant Professor of Occupational Health and Industrial Medicine at Menoufia faculty of medicine, as she was the first one to tell us about workaholism term. Many thanks to all participants who agreed to give us some of their precious time. Also many thanks to students at faculty of medicine in Menoufia University, who volunteered in the process of data collection.
References
1. Tabeleão VP, Tomasi E, Neves SF. Qualidade de vida e esgotamento profissional entre docentes da rede pública de Ensino Médio e Fundamental no Sul do Brasil. Cad Saude Publica. (2011) 27:2401–8. doi: 10.1590/S0102-311X2011001200011
2. Nonnis M, Massidda D, Cuccu S, Cortese CG. The impact of workaholism on nurses' burnout and disillusion. Open Psychol J. (2018) 11:77–88. doi: 10.2174/1874350101811010077
3. Bartczak M, Ogińska-Bulik N. Workaholism and mental health among polish academic workers. Int J Occup Saf Ergonom. (2012) 18:3–13. doi: 10.1080/10803548.2012.11076910
4. Andreassen CS, Griffiths MD, Hetland J, Kravina L, Jensen F, Pallesen S. The prevalence of workaholism: a survey study in a nationally representative sample of Norwegian employees. PLoS ONE. (2014) 9:e102446. doi: 10.1371/journal.pone.0102446
5. Schaufeli WB, Shimazu A, Taris TW. Being driven to work excessively hard: the evaluation of a two-factor measure of workaholism in the Netherlands and Japan. Cross Cult Res. (2009) 43:320–48. doi: 10.1177/1069397109337239
6. Hakanen JJ, Bakker AB, Schaufeli WB. Burnout and work engagement among teachers. J School Psychol. (2006) 43:495–513. doi: 10.1016/j.jsp.2005.11.001
7. WHO: (WHOQOL Group 1994). Measuring Quality of Life. Available online at: https://www.who.int/healthinfo/survey/whoqolqualityoflife/en/index1.html (accessed April 18, 2020).
8. Teles MA, Barbosa MR, Vargas AM, Gomes VE, Ferreira EF, Martins AM, et al. Psychosocial work conditions and quality of life among primary health care employees: a cross sectional study. Health Qual Life Outcomes. (2014) 12:72. doi: 10.1186/1477-7525-12-72
9. Wong K, Chan AHS, Ngan SC. The effect of long working hours and overtime on occupational health: a meta-analysis of evidence from 1998 to 2018. Int J Environ Res Public Health. (2019) 16:2102. doi: 10.3390/ijerph16122102
10. Nieuwenhuijsen K, Bruinvels D, Frings-Dresen M. Psychosocial work environmental and stress-related disorders: a systematic review. Occup Med. (2010) 60:277–86. doi: 10.1093/occmed/kqq081
11. Rios KA, Barbosa DA, Belasco AGS. Avaliação de qualidade de vida e depressão de técnicos e auxiliares de enfermagem. Rev Lat Am Enfermagem. (2010) 18:123–30. doi: 10.1590/S0104-11692010000300017
12. Koinis A, Giannou V, Drantaki V, Angelaina S, Stratou E, Saridi M. The impact of healthcare workers job environment on their mental-emotional health. coping strategies: the case of a local general hospital. Health Psychol Res. (2015) 3:1984. doi: 10.4081/hpr.2015.1984
13. Dordoni P, Kraus-Hoogeveen S, Beatrice IJM, Heijden VD, Peters P, Setti I, et al. Live to work or work to live? An age-moderated mediation model on the simultaneous mechanisms prompted by workaholism among healthcare professionals. Front Psychol. (2019) 10:868. doi: 10.3389/fpsyg.2019.00868
14. Rushton CH, Batcheller J, Schroeder K, Donohue P. Burnout and resilience among nurses practicing in high-intensity settings. Am J Crit Care. (2015) 24:412–20. doi: 10.4037/ajcc2015291
15. Iacovides A, Fountoulakis K, Kaprinis S, Kaprinis G. The relationship between job stress, burnout and clinical depression. J Affect Disord. (2003) 75:209–21. doi: 10.1016/S0165-0327(02)00101-5
16. Raedler TJ. Inflammatory mechanisms in major depressive disorder. Curr Opin Psychiatry. (2011) 24:519–25. doi: 10.1097/YCO.0b013e32834b9db6
17. Maes M, Mihaylova I, Kubera M, Uytterhoeven M, Vrydags N, Bosmans E. Lower plasma Coenzyme Q10 in depression: a marker for treatment resistance and chronic fatigue in depression and a risk factor to cardiovascular disorder in that illness. Neuroendocrinol Lett. (2009) 30:462–9.
18. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. (2009) 65:732–41. doi: 10.1016/j.biopsych.2008.11.029
19. Balducci C, Avanzi L, Consiglio C, Fraccaroli F, Schaufeli WB. A cross-national study on the psychometric quality of the Italian version of the Dutch work addiction scale (Duwas). Eur J Psychol Assess. (2017) 33:422–8 doi: 10.1027/1015-5759/a000300
20. Schaufeli WB, Taris TW, Bakker AB. It takes two to Tango: workaholism is working excessively and working compulsively. In: Burke RJ, Cooper CL, editors. The Long Work Hours Culture: Causes, Consequences and Choices. Bingley: Emerald Group Publishing Limited (2008). p. 203–25.
21. Nonnis M, Cuccu S, Cortese CG, Massidda D. The Italian version of the Dutch workaholism scale (DUWAS): a study on a group of nurses. Appl Psychol Bull. (2017) 278:47–57.
22. Yao G, Chung CW, Yu CF, Wang JD. Development and verification of validity and reliability of the WHOQOL-BREF Taiwan version. J Formos Med Assoc. (2002) 101:342–51. Available online at: http://www.fma.org.tw/jfma/PDF/2002-101/Issue%2005/A6.pdf
23. Kamei HH, Ferreira MC, Valentini F, Peres MF, Kamei PT, Damásio BF. Psychological capital questionnaire - short version (PCQ-12): evidence of validity of the Brazilian version. (2018). doi: 10.1590/1413-82712018230202
24. Luthans F, Youssef CM, Avolio BJ. Psychological Capital: Developing the Human Competitive Edge. Oxford: Oxford University Press (2007). doi: 10.1093/acprof:oso/9780195187526.001.0001
25. Ferreira MC, Chinelato RSC, David LM, Novaes WP, Silva JTM, Leonardo MGL. Validação convergente da Escala de Capital Psicológico Positivo. In: VI Congresso Brasileiro de Avaliação Psicológica. Maceió: Anais do VI Congresso Brasileiro de Avaliação Psicológica; IBAP (2013). Available online at: https://www.scielo.br/scielo.php?pid=S1413-82712018000200203&script=sci_arttext&tlng=en
26. Goldberg DP, Hillier VF. A scaled version of the general health questionnaire. Psychol Med. (1979) 9:139–45. doi: 10.1017/S0033291700021644
27. Maslach C, Jackson SE, Leiter MP. MBI: Maslach burnout inventory: CPP, Incorporated (1996). Available online at: https://www.scielo.br/scielo.php?pid=S1413-82712018000200203&script=sci_arttext&tlng=en
28. Buelens M, Poelmans SAY. Enriching the Spence and Robbins' typology of workaholism: demographic, motivational and organizational correlates. J Organ Change Manag. (2004) 17:440–58. doi: 10.1108/09534810410554470
29. Del Líbano M, Llorens S, Salanova M, Schaufeli WB. About the dark and bright sides of self-efficacy: workaholism and work engagement. Span J Psychol. (2012) 15:688–701. doi: 10.5209/rev_SJOP.2012.v15.n2.38883
30. Caesens G, Stinglhamber F, Luypaert G. The impact of work engagement and workaholism on well-being: the role of work-related social support. Career Dev. Int. (2014) 19:813–35. doi: 10.1108/CDI-09-2013-0114
31. Clark MA, Michel JS, Zhdanova L, Pui SY, Baltes BB. All work and no play? A meta-analytic examination of the correlates and outcomes of workaholism. J Manage. (2016) 42:1836–73. doi: 10.1177/0149206314522301
32. Hobfoll SE. Conservation of resources: a new attempt at conceptualizing stress. Am Psychol. (1989) 44:513–24. doi: 10.1037/0003-066X.44.3.513
33. Schaufeli WB, Taris TW, Van Rhenen W. Workaholism, burnout and engagement: three of a kind or three different kinds of employee well-being? Appl Psychol. (2008) 57:173–203. doi: 10.1111/j.1464-0597.2007.00285.x
34. Hu Q, Schaufeli W, Taris TW, Hessen DJ, Hakanen J, Salanova M, et al. East is east and west is west and never the twain shall meet. Work Engagement and workaholism across Eastern and Western cultures. Procedia. (2014) 1:6–24. Available online at: http://dspace.library.uu.nl/handle/1874/305458
35. Delgado C, Upton D, Ranse K, Furness T, Foster K. Nurses' resilience and the emotional labour of nursing work: an integrative review of empirical literature. Int J Nurs Stud. (2017) 70:71–88. doi: 10.1016/j.ijnurstu.2017.02.008
36. Taris TW, Schaufeli WB, Shimazu A. The push and pull of work: the differences between workaholism and work engagement. In: Bakker AB, Leiter MP, editors. Work Engagement: A Handbook of Essential Theory and Research. New York, NY: Psychology Press (2010). p. 39–53.
37. Schaufeli WB, Bakker AB, Van Dierendonck D. Prins JT. Workaholism among medical residents: it is the combination of working excessively and compulsively that counts. Int J Stress Manag. (2008) 16:249–72. doi: 10.1037/a0017537
38. Vetter MH, Vetter MK, Fowler J. Resilience, hope and flourishing are inversely associated with burnout among members of the Society for Gynecologic Oncology. Gynecol Oncol Rep. (2018) 25:52–5. doi: 10.1016/j.gore.2018.06.002
39. Ata EE, Yilmaz EB, Bayrak NG. Resilience, occupational satisfaction, burnout and compassion fatigue in Turkish intensive care nurses. Kontakt. (2020) 22:152–8. doi: 10.32725/kont.2020.028
40. Boldor N, Bar-Dayan Y, Rosenbloom T, Shemer J, Bar-Dayan Y. Optimism of health care workers during a disaster: a review of the literature. Emerg Health Threats J. (2012) 5:7270. doi: 10.3402/ehtj.v5i0.7270
41. Andreassen CS, Ursin H, Eriksen HR. The relationship between strong motivation to work, “workaholism”, and health. Psychol Health. (2007) 22:615–29. doi: 10.1080/14768320600941814
42. Taris TW, Schaufeli WB, Verhoeven LC. Workaholism in the Netherlands: measurement and implications for job strain and work-non-work conflict. Appl Psychol. (2005) 54:37–60. doi: 10.1111/j.1464-0597.2005.00195.x
43. Shimazu A, Schaufeli WB, Taris TW. How does workaholism affect worker health and performance? The mediating role of coping. Int J Behav Med. (2010) 17:154–60. doi: 10.1007/s12529-010-9077-x
44. Burke RJ. Workaholism in organizations: psychological and physical well-being consequences. Stress Med. (2000) 16:11–6. doi: 10.1002/(SICI)1099-1700(200001)16:1<11::AID-SMI825>3.0.CO;2-U
45. Kubota K, Shimazu A, Kawakami N, Takahashi M, Nakata A, et al. Association between workaholism and sleep problems among hospital nurses. Ind Health. (2010) 48:864–71. doi: 10.2486/indhealth.MS1139
46. Burken RJ. It's not how hard you work but how you work hard: Evaluating workaholism components. Int J Stress Manag. (1999) 6:225–40. doi: 10.1023/A:1021936220220
47. Schaufeli WB, Bakker AB, Burke RJ, Van Dierendonck D. Handleiding van de Utrechtse Burnout Schaal (UBOS) [Manual for the Utrecht Burnout Scale]. Lisse: Swets Test Services (2000).
48. Burke RJ, Koksal H. Workaholism among a sample of Turkish managers and professionals: an exploratory study. Psychol Rep. (2002) 91:60–8. doi: 10.2466/pr0.2002.91.1.60
49. Mudrack PE. Understanding workaholism: the case of behavioral tendencies. In: Burke R, editor. Work Hours and Work Addiction. Northampton, MA: Elgar (2006). p. 108–28.
50. Porter G. Workaholic tendencies and the high potential for stress among co-workers. Int J Stress Manag. (2001) 8:147–64. doi: 10.1023/A:1009581330960
51. Schaufeli WB, Bakker AB, van der Heijden FMMA, Prins JT. Workaholism, burnout and well-being among junior doctors: the mediating role of role conflict. Work Stress. (2009) 23:155–72. doi: 10.1080/02678370902834021
52. Emeny R, Lacruz ME, Baumert J, Zierer A, von Eisenhart Rothe A, Autenrieth C, et al. Job strain associated CRP is mediated by leisure time physical activity: results from the MONICA/KORA study. Brain Behav Immun. (2012) 26:1077–84. doi: 10.1016/j.bbi.2012.07.004
53. Harpaz I, Snir R. Workaholism: its definition and nature. Hum Relat. (2003) 56:291–319. doi: 10.1177/0018726703056003613
54. Andreassen CS, Hetland J, Pallesen S. The relationship between workaholism, basic needs satisfaction at work and personality. Eur J Pers. (2010) 24:3–17. doi: 10.1002/per.737
55. Taris TW, Van Beek I, Schaufeli WB. Demographic and occupational correlates of workaholism. Psychol Rep. (2012) 110:547–54. doi: 10.2466/03.09.17.PR0.110.2.547-554
56. Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK., et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. (2010) 67:446–57. doi: 10.1016/j.biopsych.2009.09.033
57. Young JJ, Bruno D, Pomara N. A review of the (2010) relationship between proinflammatory cytokines and major depressive disorder. J Affect Disord. (2014) 169:15–20. doi: 10.1016/j.jad.2014.07.032
58. Anderson G, Berk M, Dean O, Moylan S, Maes M. Role of immune-inflammatory and oxidative and nitrosative stress pathways in the etiology of depression: therapeutic implications. CNS Drugs. (2014) 28:1–10. doi: 10.1007/s40263-013-0119-1
59. Maes M, Mihaylova I, Kubera M, Uytterhoeven M, Vrydags N, Bosmans E. Lower plasma Coenzyme Q 10 in depression: a marker for treatment resistance and chronic fatigue in depression and a risk factor to cardiovascular disorder in that illness. Neuroendocrinol Lett. (2009) 30:462–9.
60. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
Keywords: burnout, healthcare workers, mental health, pro-inflammatory markers, quality of life, workaholism, work addiction
Citation: Kasemy ZA, Abd-Ellatif EE, Abdel Latif AA, Bahgat NM, Shereda HMA, Shattla SI, Aboalizm SE, Abd Elhy AH, Allam AR, Ramadan AN, Amer HM, Ahmed NA, AlJifri AA and El Dalatony MM (2020) Prevalence of Workaholism Among Egyptian Healthcare Workers With Assessment of Its Relation to Quality of Life, Mental Health and Burnout. Front. Public Health 8:581373. doi: 10.3389/fpubh.2020.581373
Received: 13 July 2020; Accepted: 23 October 2020;
Published: 26 November 2020.
Edited by:
William Edson Aaronson, Temple University, United StatesReviewed by:
Zhengxue Qiao, Harbin Medical University, ChinaSasho Stoleski, Saints Cyril and Methodius University of Skopje, North Macedonia
Copyright © 2020 Kasemy, Abd-Ellatif, Abdel Latif, Bahgat, Shereda, Shattla, Aboalizm, Abd Elhy, Allam, Ramadan, Amer, Ahmed, AlJifri and El Dalatony. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zeinab A. Kasemy, emVpbmFia2FzZW15QGdtYWlsLmNvbQ==; emVpbmFiLmthc2VteUBtZWQubWVub2ZpYS5lZHUuZWc=