
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 10 December 2020
Sec. Public Health Education and Promotion
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.563180
 Ming Guan1,2,3*
Ming Guan1,2,3*Background: The floating population in urban China is facing multiple barriers to access to comprehensive, affordable, and culturally effective public health services. However, little is known about the role of geodemographic factors. This study aimed to assess the associations between geodemographic factors and access to public health services among the Chinese floating population.
Methods: This study employed the data from the 2015 Migrant Dynamic Monitoring Survey data in China. Descriptive statistical analysis and principal component analysis were used to provide basic characteristics of the main variables. Multiple logistic models were used to analyze how province-level units, economic regions, and economic zones had significant associations with residential health records establishment, social medical insurance, and types and methods of health knowledge attainment in urban China. Using multiple indicator multiple cause models, the association between geodemographic factors and types and methods of health knowledge attainment was studied.
Results: The results indicated that there was regional unbalance in the case of residential health records. Regional differences were significantly associated with social medical insurance. Provincial differences were significantly associated with health knowledge attainment. There were regional differences in the methods of health knowledge attainment. In the most provincial units, geodemographic factors had significant associations with types and methods of health knowledge attainment.
Conclusions: This study confirmed empirical associations between geodemographic factors and access to public health services among Chinese floating population. The relevant suggestion was that provincial units with less-developed public health services should enhance their capabilities to equalize public health services.
• Health status was poor among floating population in China.
• Health records among floating population were geographically distributed unevenly in China.
• Social medical insurance among the floating population was geographically covered unevenly in China.
• Health knowledge among the floating population was geographically obtained unevenly in China.
• There is an urgent need to balance health service utilization for the floating population in China.
• Findings from this study have the potential to redesign health policy for the floating population in China.
Since entry into the new century, the Chinese floating population, especially the interprovincial floating population (1), increase year by year due to rapid economic growth. The floating population referred to the large and increasing number of migrants without local household registration status and had become a new demographic phenomenon in China. Most of these migrants move from the rural areas of the central and western parts of China to the eastern and coastal metropolitan areas in pursuit of a better life.
Recent evidence suggested that the floating population in China was characterized by stigma and discrimination (2), poor psychological and social health (3), poor sense of belonging (4), and high prevalence of induced abortion (5). It has previously been observed that they exhibited poor awareness of reproductive health (6) and lived in poor living environment (7). Although the prevalence of diabetes in the floating population was lower than that in the general population, the potential threat brought by the diabetes in floating population was imponderable due to the growing population number and the poor disease management (8). Despite low percentage of participation in moderate and vigorous activities (9), prevalent drinking behavior (10), and smoking behaviors (11) were high among them. Since access to public health services affected the medical treatment seeking behaviors of floating population (12–14), geodemographic factors could be speculated to have association with their health status.
Early research reported the uneven supply of public health services across migrant population groups and regions. For instance, the utilization of health services among young migrants (15) and old-aged migrants (16) were insufficient in comparison with the general population. It was impossible to cover internal migrants with lower socioeconomic status and across provinces by public health services (17). Even worse, there was an imbalance of basic public health service utilization between urban and suburban areas (18). Thus, the relationship between geodemographic factors and access to public health services possibly existed among the Chinese floating population.
This study aimed to assess equalization of basic public health services geographically. With an official publicly available survey data, the present study tried to investigate the associations between geodemographic factors and access to public health services among internal migrants in China. The statistical outcomes would reveal the targeted relationships.
This study used data from 2015 Migrant Dynamic Monitoring Survey. The survey adopted a stratified three-stage probability proportionate to size sampling, and the annual national data on migrants from each province in 2014 was considered the basic sampling frame. According to the random principle through the multistage clustering sampling method, the sample of the floating population was collected from 6 major industries in 170 counties and districts from 31 province-level units and Xinjiang Production and Construction Corps (XPCC). The subject of the survey was the inflow of persons aged 15 and above who lived in the place of inflow for more than 1 month and were not registered in the district (county, city). The sampling method of this data was based on the annual report data of floating population, all staff in 31 provinces (districts and municipalities) and XPCC in 2014. A total sample size of 206,000 was projected for the survey, involving a total of approximately 500,000 floating population family members. Here, only the part of the migrant population that began to move after 1978 was studied. Thus, in the total sample, persons were excluded due to marriages, residential mobility, seeking help from relatives and friends, accepting training, military service, and giving birth. And, the duration of population floating was constrained to 1978–2015.
Establishment of health records was reflected by the question: “Do you have established health records in your local community?” The response options were “no, I have never heard of this,” “no, but I have heard of this,” “I have established health records,” and “I don't know.” The “no” response was coded as 0, the “yes” response was coded as 1, and The “I don't know” response was coded as missing values.
Social medical insurance was reflected by the question: “Which type of social medical insurance were you covered by” The six choices were the following: new rural cooperative medical scheme (NRCMS), Cooperative medical insurance for urban and rural residents (CMIURR), urban resident based basic medical insurance (URBMI), urban employee-based basic medical insurance (UEBMI), and free medical treatment (FMT).
The methods of access to health knowledge were reflected by a multiple choice question: “How did you access health knowledge?” The eight choices were the following: lecture (1 = yes, 0 = no), books/magazine/CD (1 = yes, 0 = no), radio/TV programmes (1 = yes, 0 = no), face-to-face consultation (1 = yes, 0 = no), online medical consultation (1 = yes, 0 = no), community advocacy (1 = yes, 0 = no), bulletin board(1 = yes, 0 = no), SMS/WeChat (1 = yes, 0 = no). For convenience, the methods of access to health knowledge were abbreviated by knpatha, knpathb, knpathc, knpathd, knpathe, knpathf, knpathg, and knpathh, respectively.
The types of access to health knowledge were reflected by a multiple-choice question: “Did you access the below health knowledge in the destines in the last year?” The response options were occupational disease prevention (1 = yes, 0 = no), nutritional health knowledge (1 = yes, 0 = no), reproduction and contraception/eugenics (1 = yes, 0 = no), chronic disease prevention (1 = yes, 0 = no), smoking control (1 = yes, 0 = no), mental disorders (1 = yes, 0 = no), tuberculosis (1 = yes, 0 = no), STD/AIDS (1 = yes, 0 = no), and other infectious diseases(1 = yes, 0 = no). For convenience, the types of access to health knowledge were abbreviated by kntypea, kntypeb, kntypec, kntyped, kntypee, kntypef, kntypeg, kntypeh, and kntypei, respectively.
The coverage of public health services was reflected by establishment rate of health records (ERHR), social medical insurance ratio (SMIR), inaccess health knowledge ratio (IHKR), and methods of inaccess to health knowledge ratio (MIHKR). The ERHR (=persons with health records/total sample), SMIR (=persons with social medical insurance/ total sample), IHKR (=persons with inaccess to health knowledge/total sample), and MIHKR (=persons with inaccess methods of access to health knowledge/total sample) can be calculated with formulas.
First, a descriptive analysis was conducted to analyze socioeconomic factors by chi-square test. Frequency and percentage were employed to reflect categories' distribution in the socioeconomic variables. Second, the logistic regression was used to reflect geographic equality of public health services in the province-level units, economic regions, and economic zones. Thus, public health services like NRCMS (1 = yes, 0 = no), CMIURR (1 = yes, 0 = no), URBMI (1 = yes, 0 = no), UEBMI (1 = yes, 0 = no), and FMT (1 = yes, 0 = no) were outcome variables. And geographic variables were independent variables. When regressing economic regions, Pearl River Delta was referred. This was because Pearl River Delta attracted a number of the floating population under the increasing regional gaps and global economic bloom. From 2000 to 2010, the floating population mainly flowed into three economic regions and provincial capitals and cities in the eastern China. Third, the multiple indicator multiple cause (MIMIC) model was adopted to measure the associations between socio-economic factors and types of access to health knowledge and methods in a specific province-level unit. The socio-economic factors were age “(2015+9/12) minus (birth year+ birth month /12)”, gender (male = 1, female = 0), education (educated = 1, uneducated = 0), Hukou (household registration, rural = 1, other = 0), marital status (first married = 1, others = 0), income (unit: Chinese Yuan), and flowing direction (interprovince = 1, other = 0) were the main covariates. Principal component analysis (PCA) in conjunction with varimax rotation with Kaiser's criterion was performed to explore the structure of types and methods of access to health knowledge. The Kaiser–Meyer–Olkin (KMO>0.7, adequate) coefficient and Bartlett's test would be measured to reflect suitable to conduct PCA. The internal consistency would be assessed by Cronbach's alpha. In the confirmatory factor analysis, root mean square error of approximation (RMSEA: <0.05 close, < 0.08 good, <0.10 reasonable) was employed to measure goodness-of-fit of MIMIC models.
Regarding ethical acceptability, this study used secondary data from the 2015 Migrant Dynamic Monitoring Survey and was deemed excluded from IRB review. With respect to human rights, this study implemented to protect human subjects with the anonymous survey dataset.
Table 1 showed that most of the sample accepted middle school and above education. Regarding Hukou, more than 85% of the floating population had agricultural Hukou. Regarding marital status, 80% of them were first married, followed by 16% unmarried. More than half of them were interprovincial migrants. Number of males surpassed number of females. Regarding age, mean male age was somewhat higher than that of females. Most of the floating population were adult laborers who were younger than 60 years old and earned <10 thousand Chinese Yuan per month in the last year.
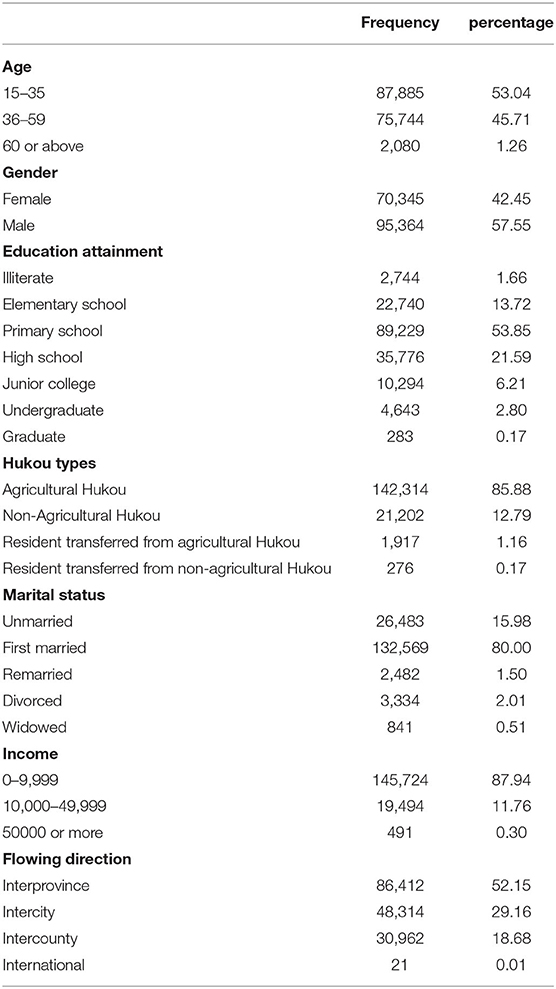
Table 1. Sample characteristics (total = 165,709).
The coverage rate of social medical insurance reached 93.66%. See Figure 1, provinces with establishment rate of floating population health records>40% were Inner Mongolia (40.238%), Heilongjiang (52.725%), Shandong (47.535%), Hubei (50.612%), Hunan (45.419%), Chongqing (40.756%), Qinghai (50.431%), and Ningxia (47.793%). Figure 2 showed provinces with uncoverage rates of social medical insurance>10% were Beijing (14%), Liaoning (13%), Jilin (12%), Heilongjiang (16%), Xinjiang (12%), XPCC (14%), Taiwan (20%), and Hongkong (17%). See Figure 3, provinces with unaccess to health knowledge>10% were Shanxi (10%), Anhui (11%), Jiangxi (12%), Hainan (14%), Guizhou (11%), Tibet (21%), and Shannxi (10%). Figure 4 showed province-level units with more than one knowledge access method were Beijing, Tianjin, Inner Mongolia, Shanghai, Qinghai, XPCC, and Taiwan.

Figure 1. Province-level units ERHR>40%.

Figure 2. Province-level units with SMIR >10%.
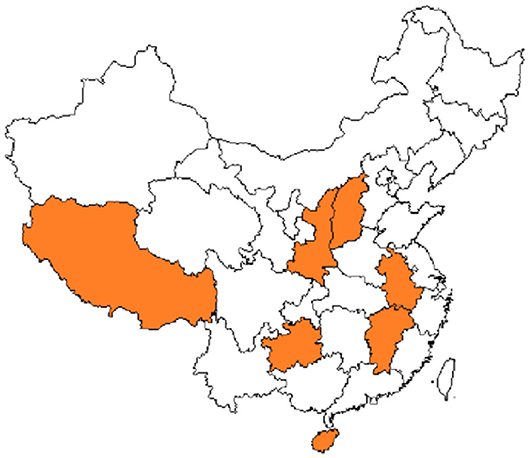
Figure 3. Province-level units with IHKR>10%.

Figure 4. Province-level units with MIHKR >1.
See Table 2. More than 30% of the floating population had established health records. The establishment rate of health records of males was higher than that of females. Regarding social medical insurance, there were significant gender difference in NRCMS (new rural cooperative medical scheme), CMIURR (cooperative medical insurance for urban and rural residents), URBMI (urban resident based basic medical insurance), and UEBMI (urban employee-based basic medical insurance). Simultaneously, the coverage rate of social security programs of males was higher than that of females. Regarding access to health knowledge, there were significant gender differences in kntypea (access to occupational disease prevention knowledge), kntypeb (access to nutritional health knowledge), kntypec (access to reproduction and contraception/eugenics knowledge), kntypee (access to smoking control knowledge), kntypef (access to mental disorders knowledge), kntypeh (access to STD/AIDS knowledge), and kntypei (access to other infectious diseases knowledge). Likewise, access to knowledge rate of male was higher than that of females. Regarding methods of access to health knowledge, there were significant gender difference in knpatha (access to health knowledge with lecture), knpathd (access to health knowledge with face-to-face consultation), knpathe (access to health knowledge with online medical consultation), knpathf (access to health knowledge with community advocacy), and knpathg (access to health knowledge with bulletin board). Similarly, methods of access to health knowledge of males were more than those of females.
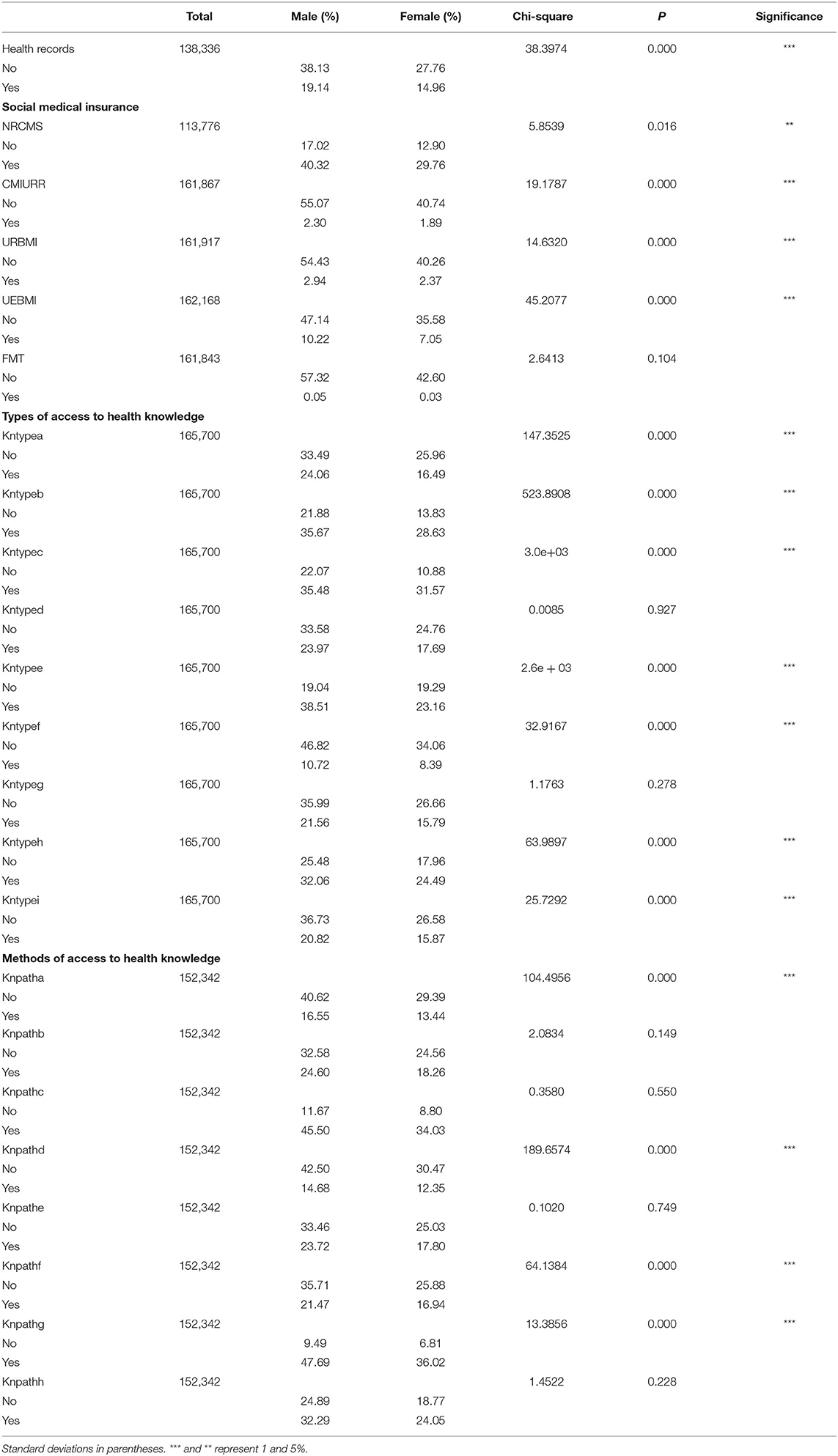
Table 2. Gender difference in the access to public health services.
See Table 3. Shanxi, Inner Mongolia, Hainan, Tibet, Gansu, and Xinjiang had significant associations with access to kntypea (access to occupational disease prevention knowledge). Hebei, Shanxi, Inner Mongolia, Anhui, Jiangxi, Henan, Guangdong, Guangxi, Hainan, Sichuan, Guizhou, Yunan, Tibet, Shannxi, Gansu, Qinghai, Ningxia, and Xinjiang had significant associations with kntypeb (access to nutritional health knowledge). Fujian, Shandong, Hubei, Hunan, Guangdong, Guangxi, Chongqing, Yunan, Tibet, Ningxia, and Xinjiang had significant associations with kntypec (access to reproduction and contraception/eugenics knowledge). Hebei, Shanxi, Hainan, Tibet, and XPCC had significant associations with kntyped (access to chronic disease prevention knowledge). Tibet had significant associations with kntypee (access to smoking control knowledge). Shanghai, Fujian, Hubei, Hunan, Guangdong, Guangxi, Chongqing, Sichuan, and Beijing had significant associations with kntypef (access to mental disorders knowledge). Hebei, Hunan, Chongqing, Sichuan, Guizhou, Yunan, Tibet, Gansu, Qinghai, Ningxia, Xinjiang, XPCC, and Beijing had significant associations with kntypeg (access to tuberculosis knowledge). Fujian, Jiangxi, Henan, Hubei, Hunan, Guangdong, Guangxi, Hainan, Chongqing, Sichuan, Guizhou, Yunan, Tibet, Gansu, Qinghai, Xinjiang, and XPCC had significant associations with kntypeh (access to STD/AIDS knowledge). Shanghai, Fujian, Henan, Hubei, Hunan, Guangdong, Guangxi, Chongqing, Sichuan, Guizhou, Yunan, Gansu, Qinghai, Ningxia, Xinjiang, XPCC, and Beijing had significant associations with kntypei (access to other infectious diseases knowledge). But, Tianjin, Liaoning, Jilin, Heilongjiang, Jiangsu, and Zhejiang had no significant associations with kntypea (access to occupational disease prevention knowledge), kntypeb (access to nutritional health knowledge), kntypec (access to reproduction and contraception/eugenics knowledge), kntyped (access to chronic disease prevention knowledge), kntypee (access to smoking control knowledge), kntypef (access to mental disorders knowledge), kntypeg (access to tuberculosis knowledge), kntypeh (access to STD/AIDS knowledge), and kntypei (access to other infectious diseases knowledge). Thus, the access imbalance of health knowledge types was reflected by the associations between province-level units and types of access to health knowledge.
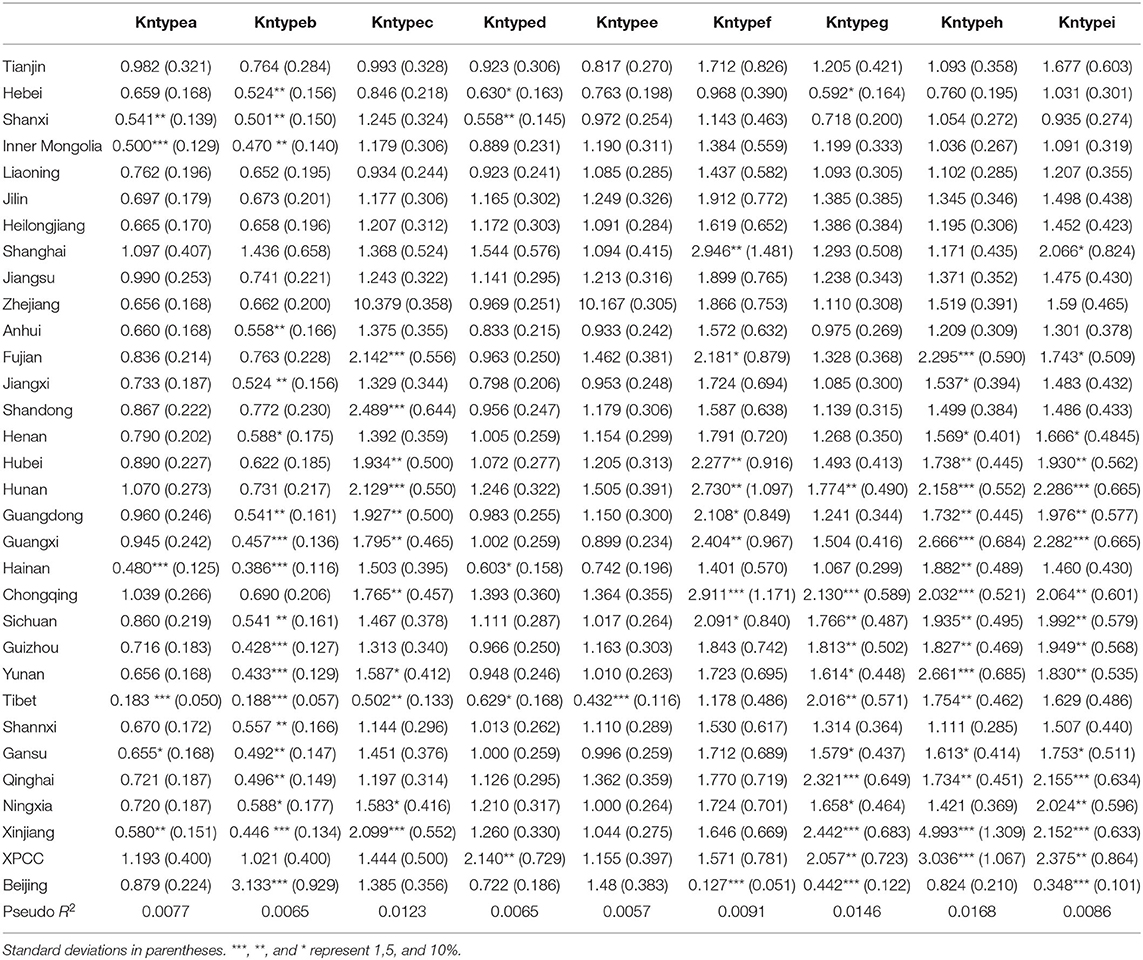
Table 3. Associations between province-level units and types of access to health knowledge (sample = 165,649).
Regarding types of access to health knowledge, after orthogonal rotation method for Caesar normalization after three iterations, PCA showed 2 factors (eigenvalues >1.0) were L1 (eigenvalue = 3.535) and L2 (eigenvalue = 1.023) had commutative contribution rate 50.65%. Cronbach's alphas of the two factors (L1: kntypea, kntyped, kntypef, kntypeg, kntypei; L2: kntypeb, kntypec, kntypee, kntypeh) were 0.7750 and 0.6159, respectively. This showed the factor analysis was highly acceptable.
See Figures 5–34. Except Beijing, Tianjin, and Shanghai, RMSEA values in total sample (RMSEA = 0.086), Hebei (RMSEA = 0.087), Shanxi (RMSEA = 0.081), Inner Mongolia (RMSEA = 0.090), Liaoning (RMSEA = 0.087), Jilin (RMSEA = 0.088), Heilongjiang (RMSEA = 0.082), Jiangsu (RMSEA = 0.089), Zhejiang (RMSEA = 0.083), Anhui (RMSEA = 0.089), Fujian (RMSEA = 0.085), Jiangxi (RMSEA = 0.084), Shandong (RMSEA = 0.083), Henan (RMSEA = 0.086), Hubei (RMSEA = 0.086), Hunan (RMSEA = 0.085), Guangdong (RMSEA = 0.090), Guangxi (RMSEA = 0.094), Hainan (RMSEA = 0.096), Chongqing (RMSEA = 0.091), Sichuan (RMSEA = 0.088), Guizhou (RMSEA = 0.096), Yunan (RMSEA = 0.097), Tibet (RMSEA = 0.096), Shannxi (RMSEA = 0.089), Gansu (RMSEA = 0.087), Qinghai (RMSEA = 0.091), Ningxia (RMSEA = 0.095), Xinjiang (RMSEA = 0.090), and XPCC (RMSEA =0.086) were <0.1. Thus, provincial differences were reflected by the associations between geodemographic factors and types of access to health knowledge.
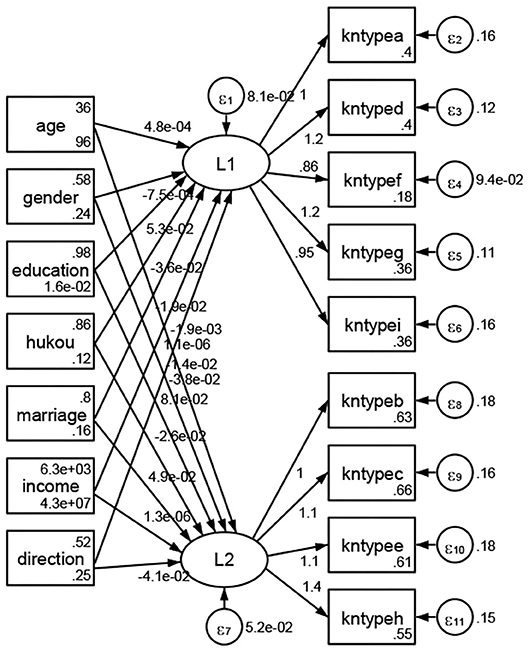
Figure 5. Total sample.

Figure 6. Hebei.
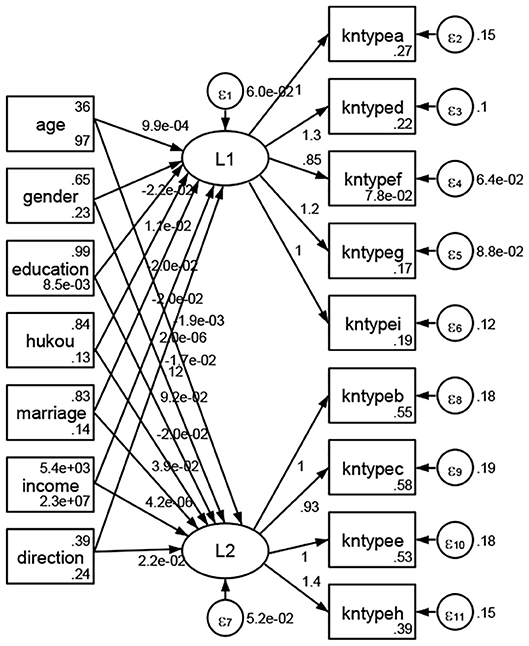
Figure 7. Shanxi.
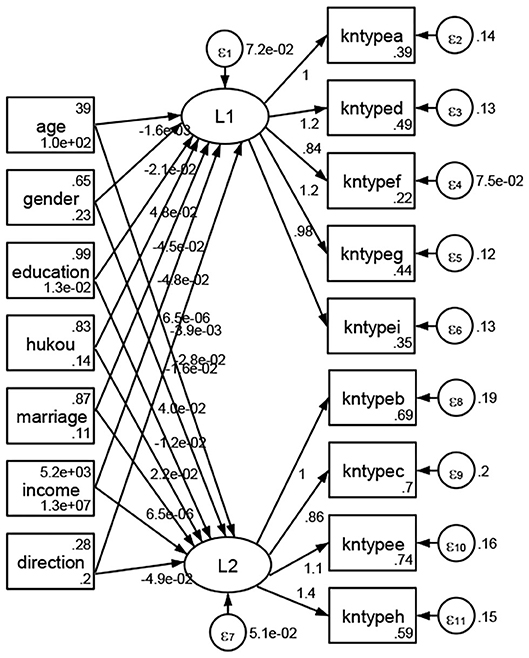
Figure 8. Inner Mongolia.
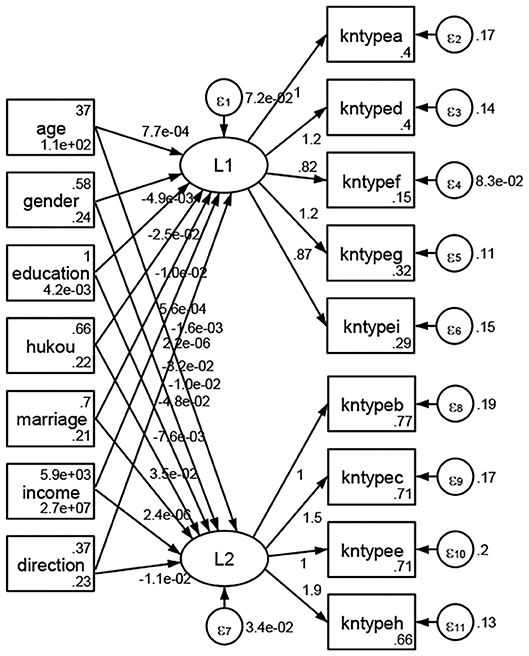
Figure 9. Liaoning.
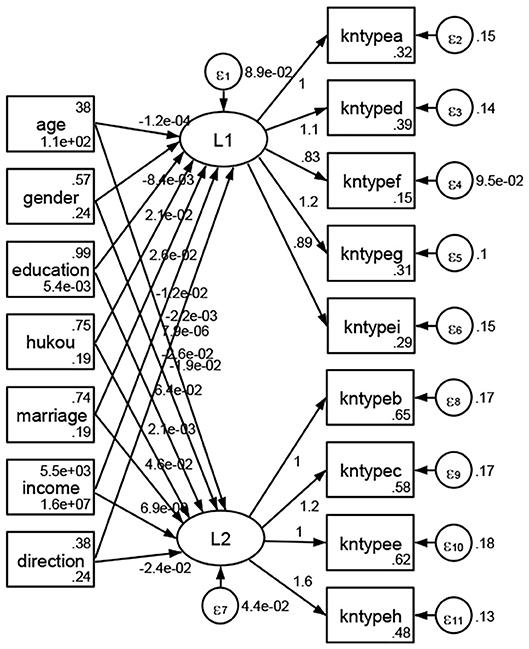
Figure 10. Jilin.
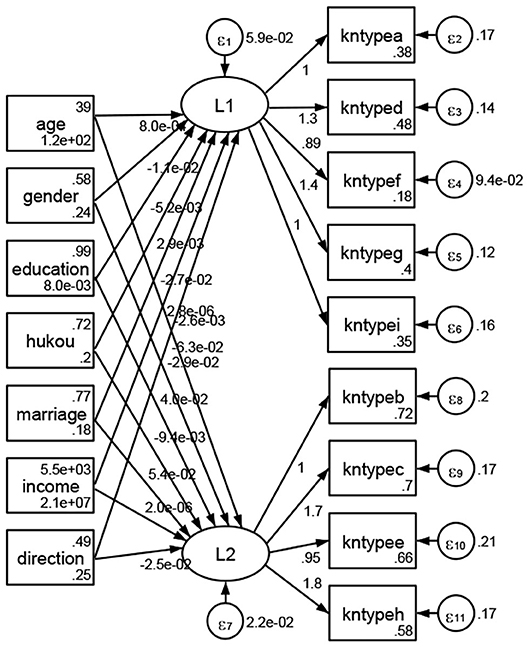
Figure 11. Heilongjiang.
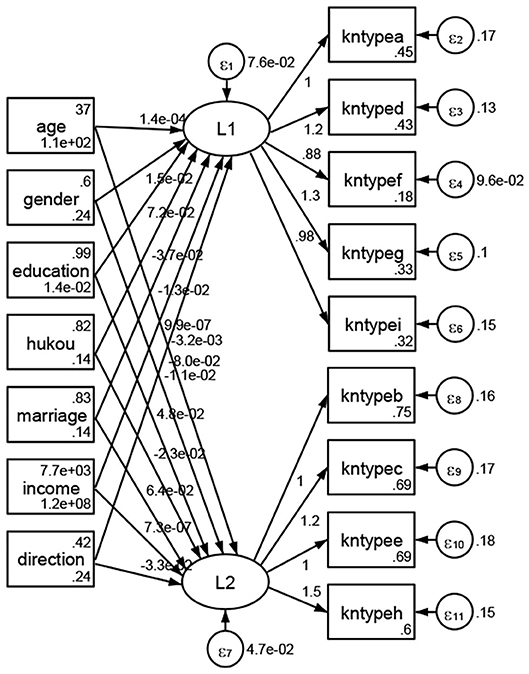
Figure 12. Jiangsu.
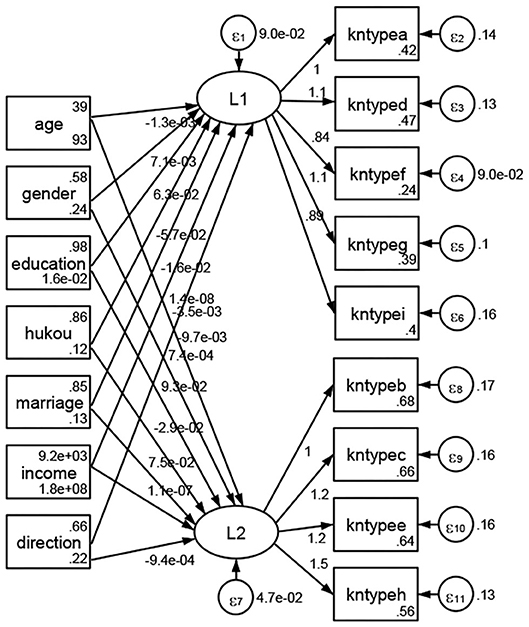
Figure 13. Zhejiang.
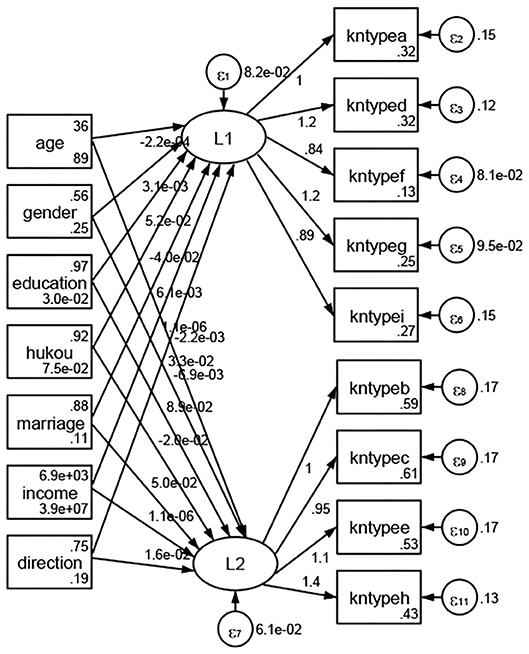
Figure 14. Anhui.
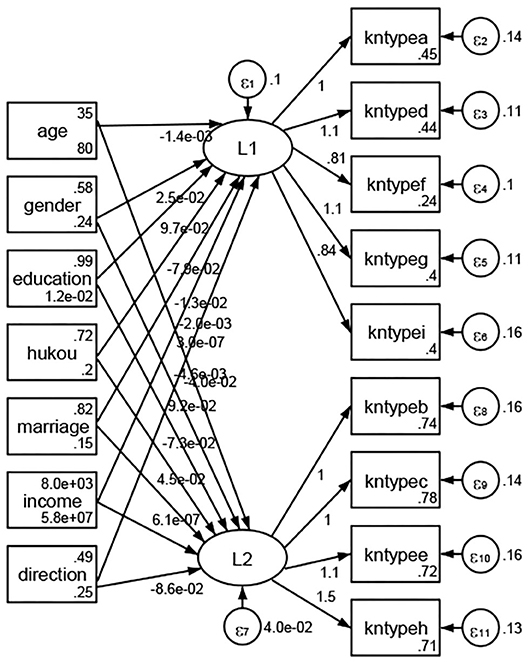
Figure 15. Fujian.
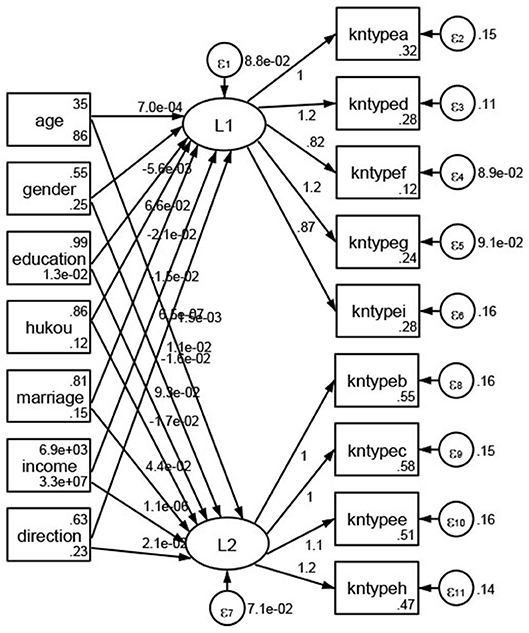
Figure 16. Jiangxi.
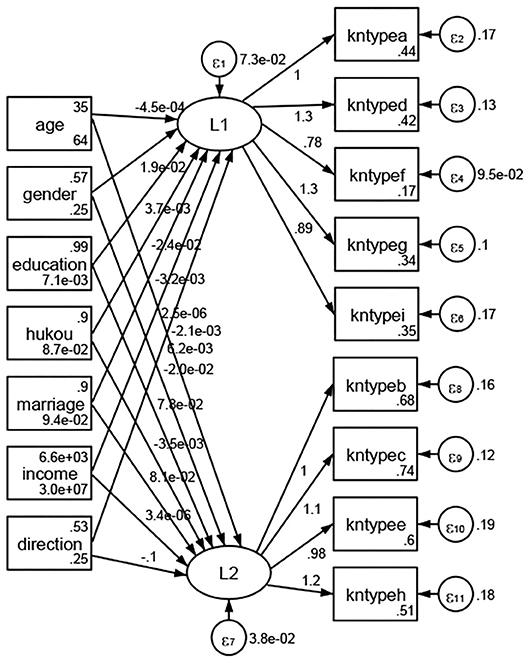
Figure 17. Shandong.
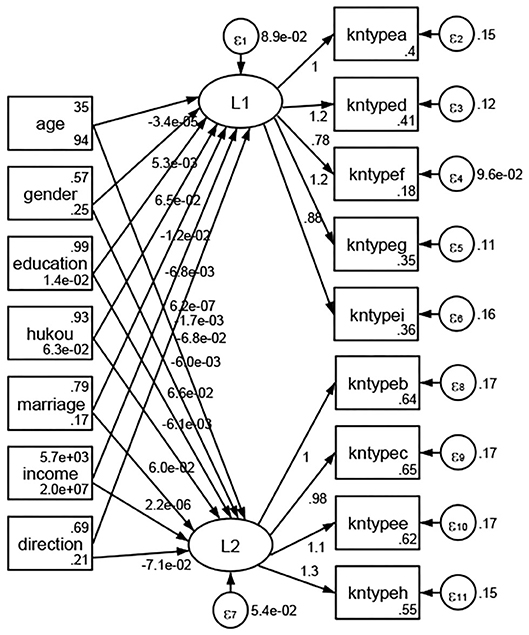
Figure 18. Henan.

Figure 19. Hubei.
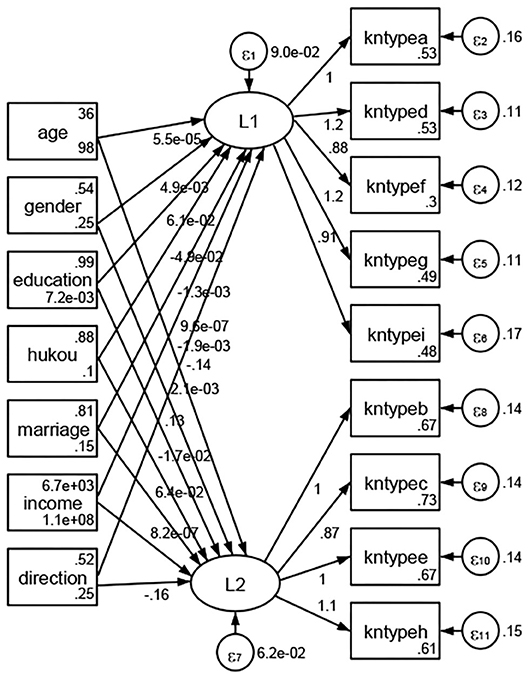
Figure 20. Hunan.
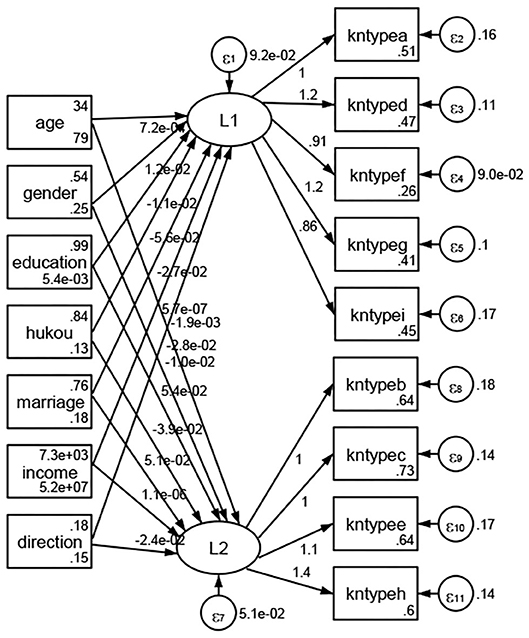
Figure 21. Guangdong.
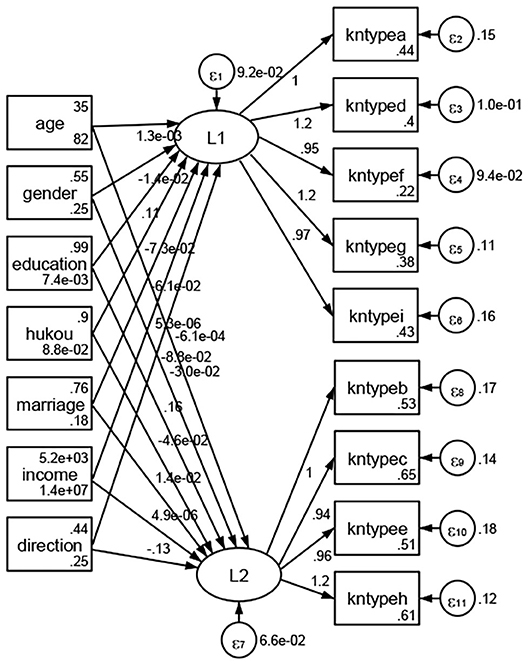
Figure 22. Guangxi.

Figure 23. Hainan.
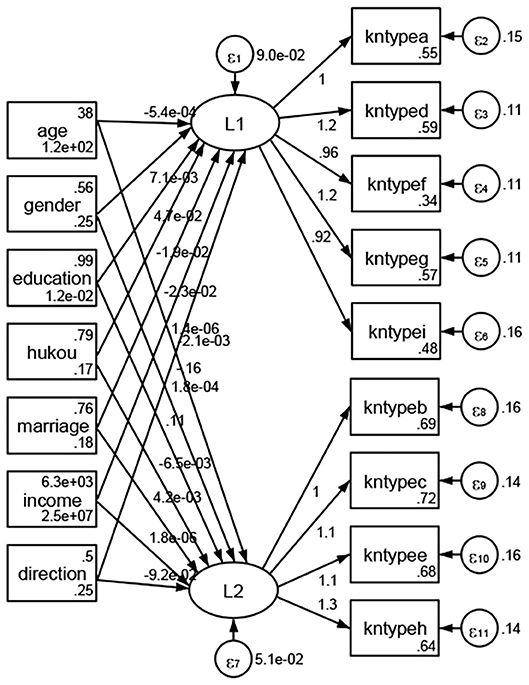
Figure 24. Chongqing.

Figure 25. Sichuan.
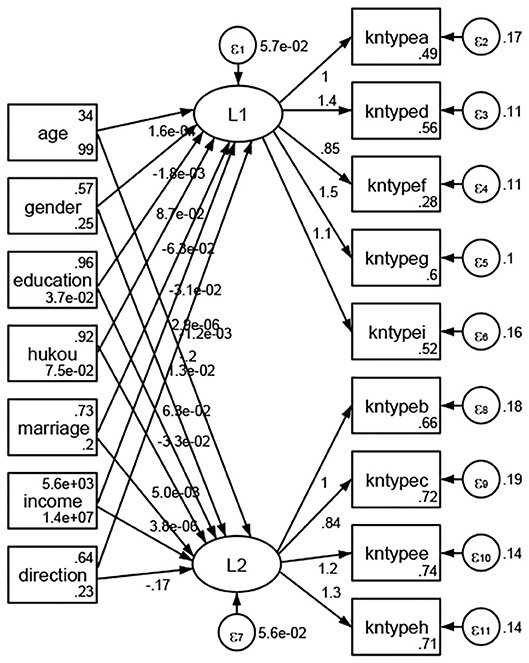
Figure 26. Guizhou.
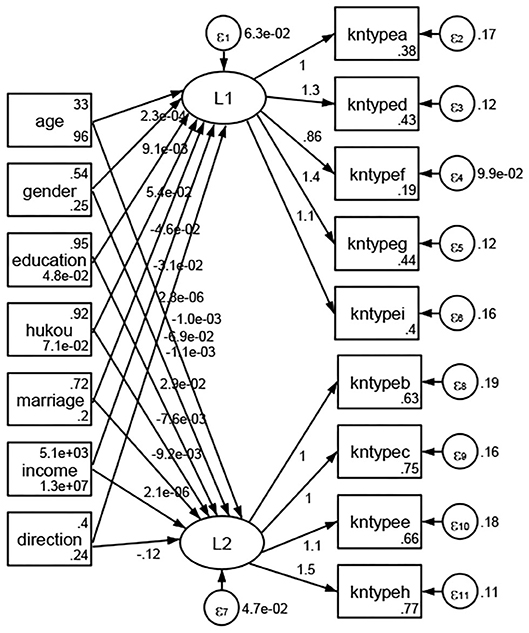
Figure 27. Yunan.

Figure 28. Tibet.
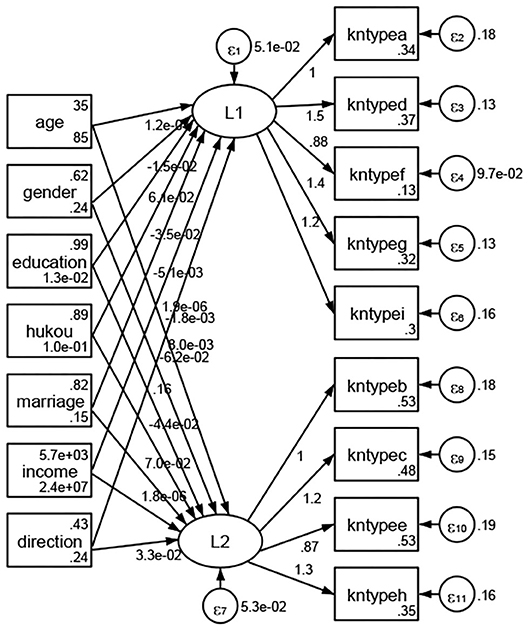
Figure 29. Shannxi.
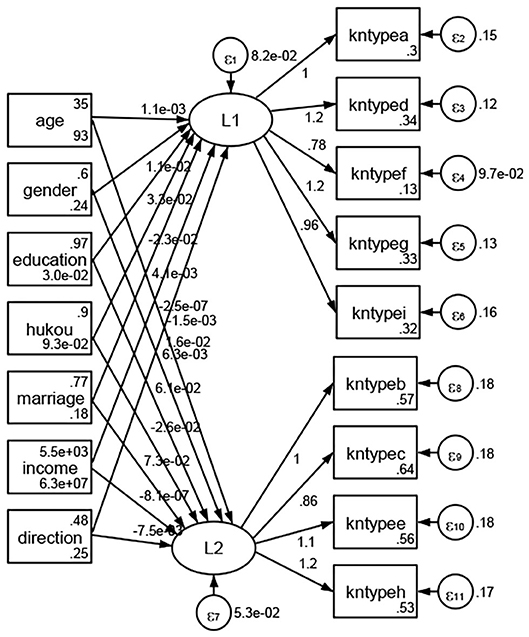
Figure 30. Gansu.
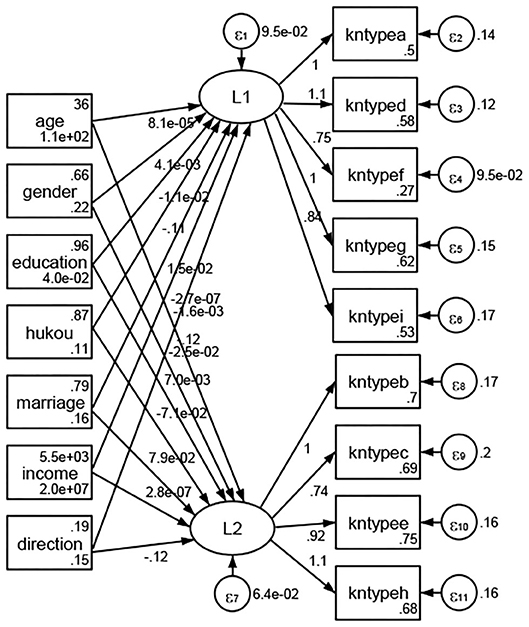
Figure 31. Qinghai.
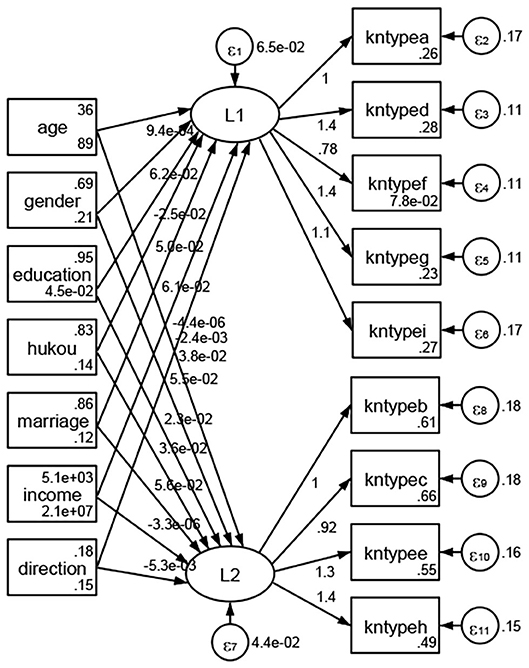
Figure 32. Ningxia.
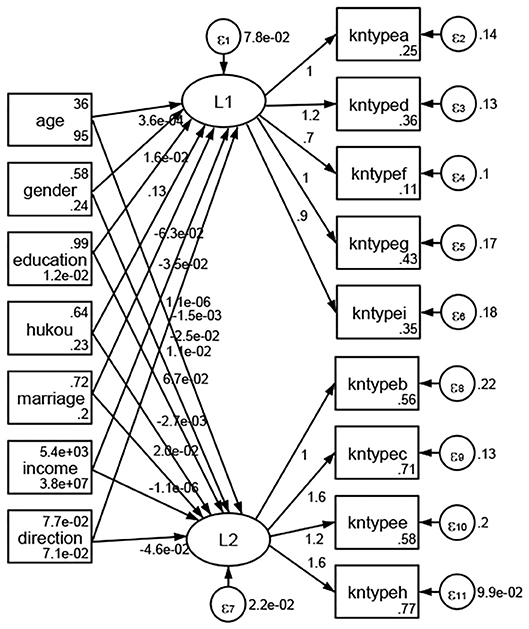
Figure 33. Xinjiang.
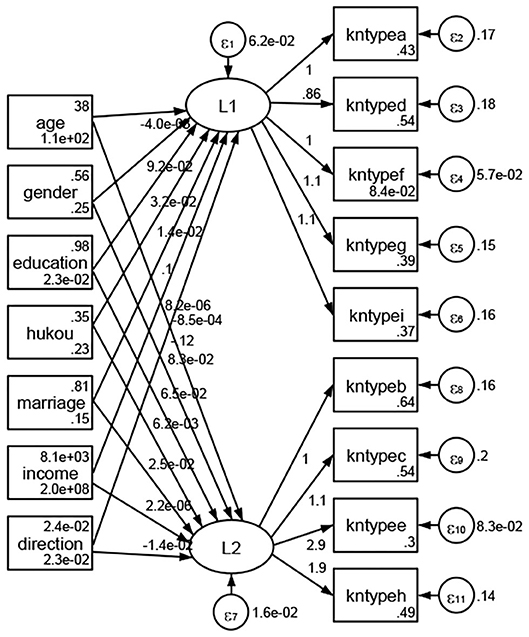
Figure 34. XPCC.
Regarding methods of access to health knowledge, after using the orthogonal rotation method for Caesar normalization for three iterations, PCA showed two factors (eigenvalues >1.0) were L1 (eigenvalue = 2.012) and L2 (eigenvalue = 1.516) had a commutative contribution rate of 44.10%. Cronbach's alphas of the two factors (L1: knpathb, knpathc, knpathe, knpathf, knpathg, knpathh; L2: knpatha, knpathd) were 0.5015 and 0.5499, respectively. This showed the factor analysis was moderately acceptable.
Except Beijing, Tianjin, Shanxi,Inner Mongolia, Liaoning, Jilin, Heilongjiang, Shanghai, Guangdong, Hainan, Guizhou, Yunan, Gansu, Qinghai, Xinjiang, and XPCC, Figures 35–50 showed RMSEA values in total sample (RMSEA = 0.060), Hebei (RMSEA = 0.070), Jiangsu (RMSEA = 0.063), Fujian (RMSEA = 0.060), Jiangxi (RMSEA = 0.060), Henan (RMSEA = 0.060), Hubei (RMSEA 0 = 0.063), Hunan (RMSEA = 0.062), Guangxi (RMSEA = 0.075), Chongqing (RMSEA = 0.066), Sichuan (RMSEA = 0.061), Tibet (RMSEA = 0.078), Shannxi (RMSEA = 0.055), Gansu (RMSEA = 0.060), Ningxia (RMSEA = 0.070), and XPCC (RMSEA = 0.095) were <0.1. Thus, provincial imbalance was reflected by the associations between geodemographic factors and methods of access to health knowledge.
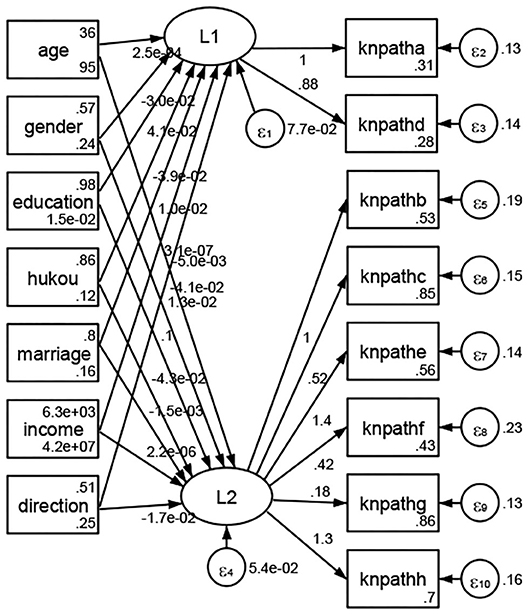
Figure 35. Total sample.
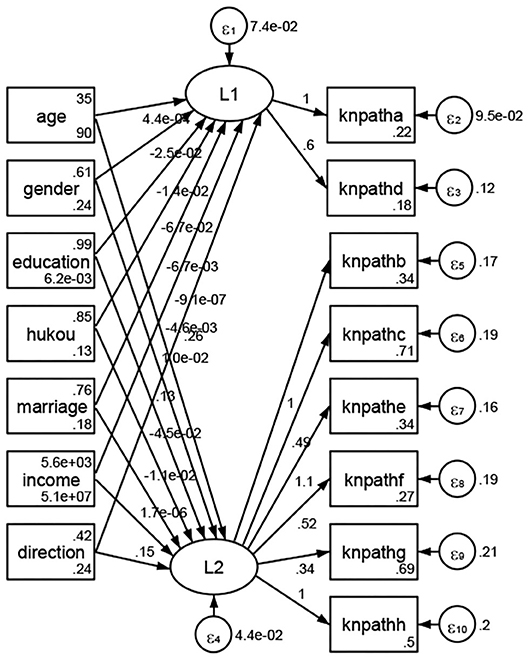
Figure 36. Hebei.
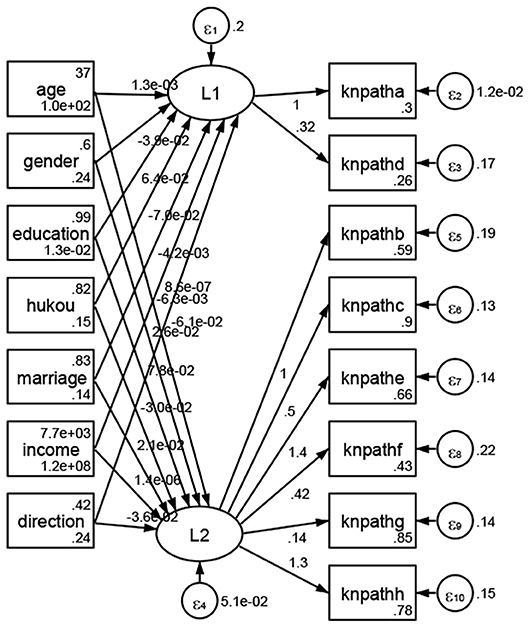
Figure 37. Jiangsu.

Figure 38. Fujian.
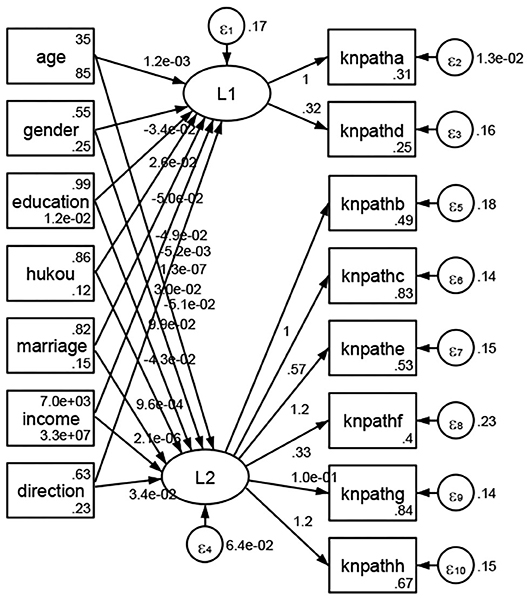
Figure 39. Jiangxi.
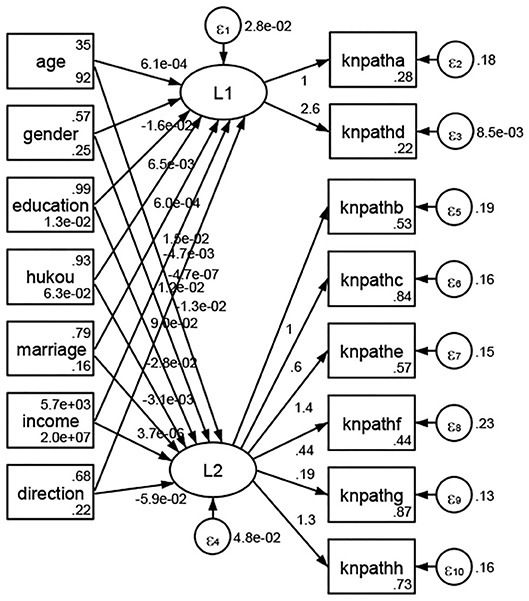
Figure 40. Henan.
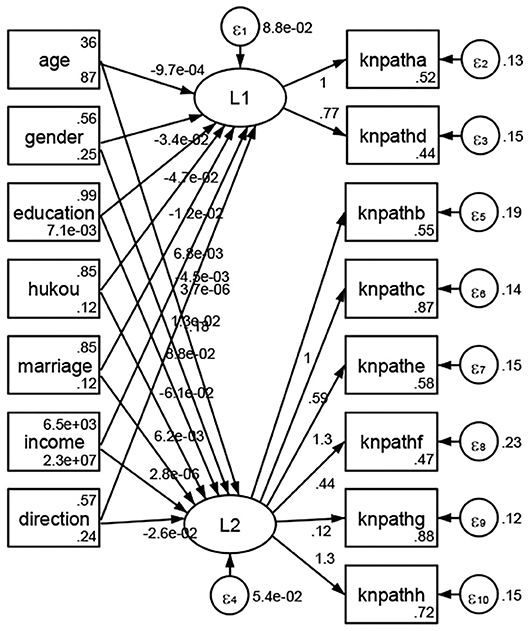
Figure 41. Hubei.
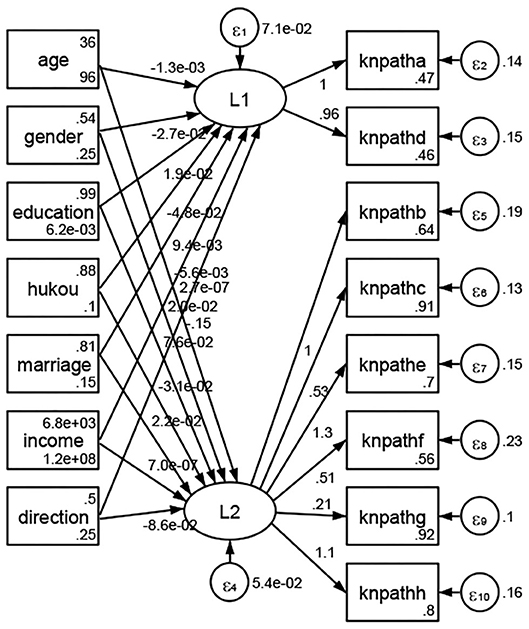
Figure 42. Hunan.
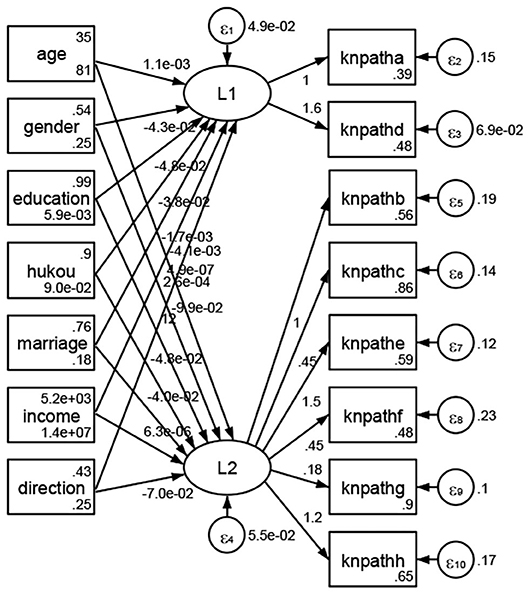
Figure 43. Guangxi.
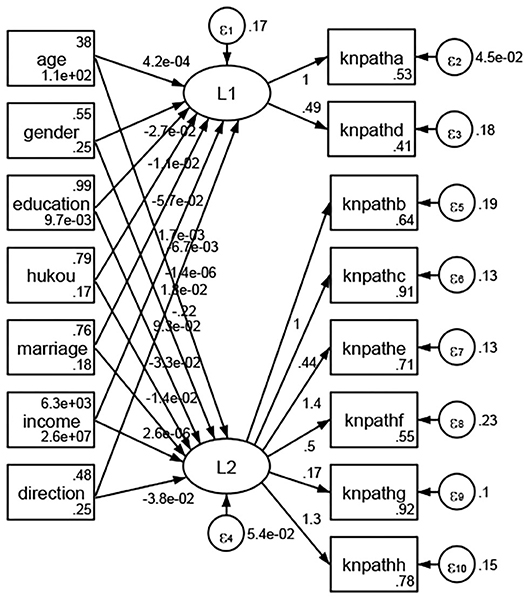
Figure 44. Chongqing.
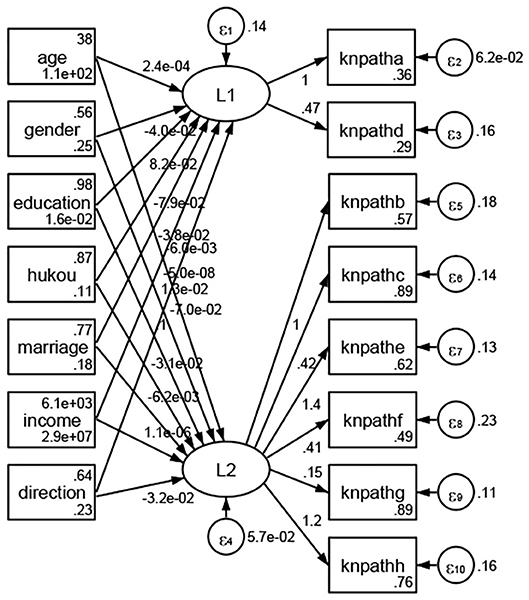
Figure 45. Sichuan.
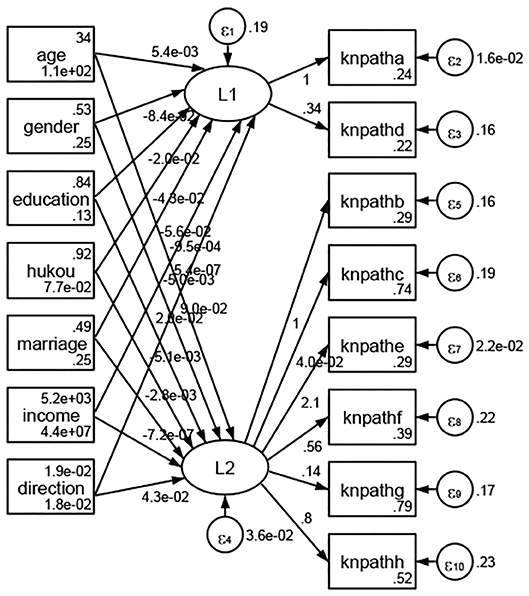
Figure 46. Tibet.
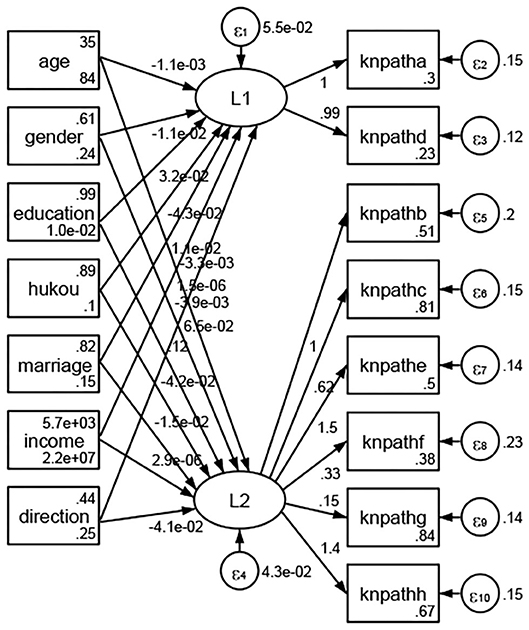
Figure 47. Shannxi.
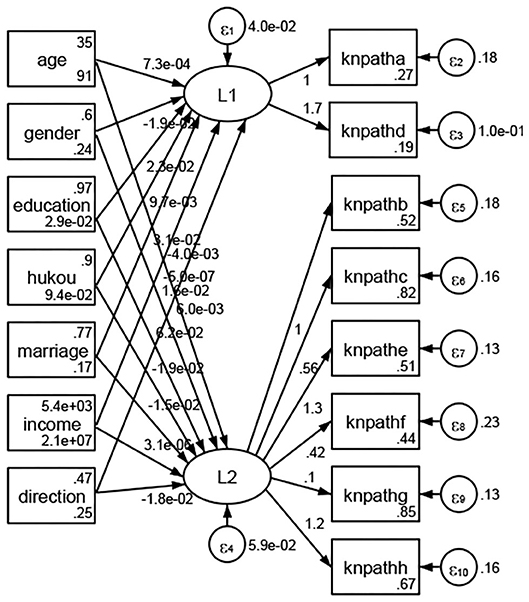
Figure 48. Gansu.
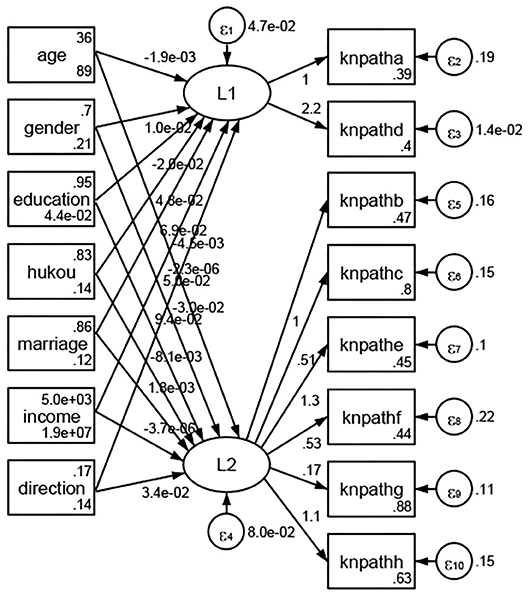
Figure 49. Ningxia.
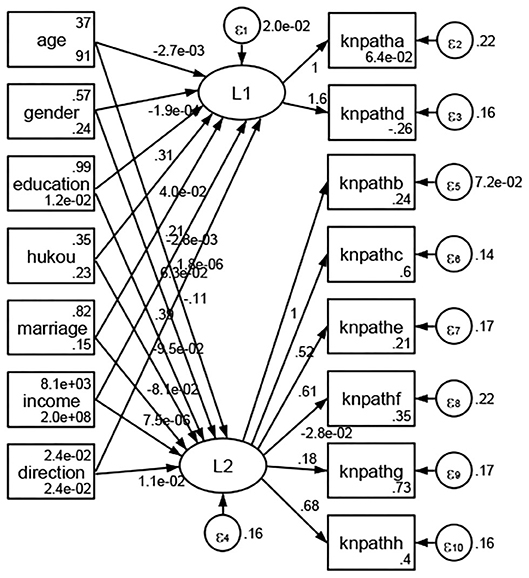
Figure 50. XPCC.
See Table 4. Regarding health records, the coefficients of Yangtze River Delta, Bohai Rim, and other region decreased in order. Thus, the zone imbalance of health records was reflected by the association between economic zones and health records.
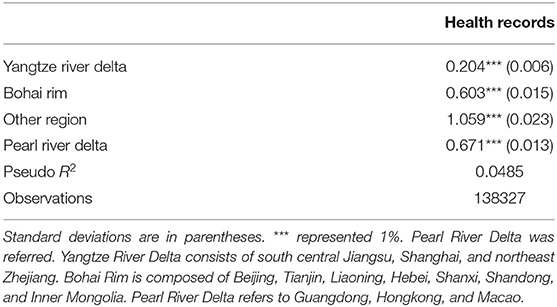
Table 4. Association between economic zones and health records.
See Table 5. Regarding NRCMS (new rural cooperative medical scheme), the coefficients of central China, western China, and Northeast China decreased in order. Regarding CMIURR (cooperative medical insurance for urban and rural residents), the coefficients of central China, western China, and northeast China decreased in order. Regarding URBMI (urban resident based basic medical insurance), the coefficients of central China, western China, and northeast China decreased in order. Regarding UEBMI (urban employee-based basic medical insurance), the coefficients of central China, western China, and northeast China decreased in order. Regarding FMT (free medical treatment), the coefficients of central China, northeast China, and eastern China decreased in order. Thus, regional differences were reflected by the associations between economic regions and social medical insurance.
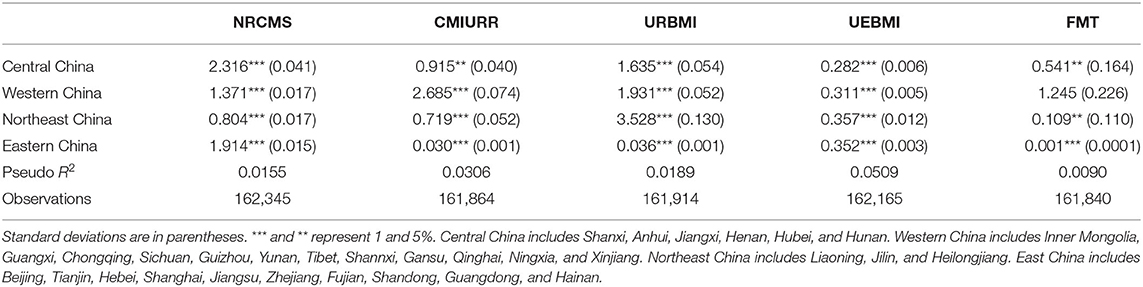
Table 5. Regional differences in the social medical insurance coverage.
This study reflected that the majority of the sample was educated and married with interprovince and intercity migration. Their establishment proportion of health records was low. Regarding social medical insurance, NRCMS (new rural cooperative medical scheme) coverage rate was the highest in the insurance system. Regarding types of access to health knowledge, kntypeb (nutritional health knowledge), kntypec (reproduction and contraception/eugenics knowledge), kntypee (smoking control knowledge), and kntypeh (STD/AIDS knowledge) accounted for more than half of the sample. Regarding methods of access to health knowledge, more than half of the sample utilized knpathc (radio/TV programmes), knpathg (bulletin board), and knpathh (SMS/WeChat) to access health knowledge. There were provincial, economic zones, and regional differences in the public health services for the floating population. There were geographic difference and provincial difference in the associations between geodemographic factors and public health services. Thus, there were geographical imbalances for the floating population to access comprehensive, affordable, and effective health care services.
The findings in this study were in accord with early studies which reported that public health services were not sufficient among Chinese floating population. For example, current research indicated that the comprehensive behavior intervention (19) was necessary to strengthen due to high prevalent rate of pulmonary tuberculosis (20), high risk factors for congenital heart defect (21), and obese (22) among the floating population. A substantial research provided potential and possible explanations for the necessary improvement of medical services in the floating population. For instance, a review indicated that the major hypertension problem of floating population was caused by their unhealthy lifestyle (drinking) and deficient disease management (23). With low household healthcare expenditure (24) and health insurance coverage (25), most of them lacked health knowledge (26), reproductive health knowledge and skills (27), and HIV-related sexual knowledge (28). Simultaneously, there existed a certain percentage of self-treatment behavior for rural floating populations when they felt uncomfortable or sick (29). Hence, public health services should be improved for the floating population.
The key point is that inadequate funds explained the reasons for the uneven distribution of essential public health services. Although implementation of the health reform since 2009 received a commendation from several scholars (30), another study indicated that the average investment of 3.97 USD per capita in the National Essential Public Health Services Package issued in 2009 was lower than the amount needed to meet its running costs among common residents (31). Another study explained that the reason for inequality in public health services, and the inefficiency of the fiscal transfer payment system, was Chinese local officials' fanatical pursuit of local economic growth in the vast majority of provinces (32). A study concluded that outsourced institutions provided by the primary medical institutions performed worse than public institutions led by the Chinese government in terms of efficiency and quality (33). In fact, despite developed cities such as Zhuhai, a cross-sectional study found government funds for basic public health services could not compensate for the actual costs under the constraints of a limited budget (34).
Other factors with minor importance also were documented in the early research. Early studies reported that market-oriented financing reforms of public health services (35), clear and detailed protocols (36), structural social capital (37), household registration (38), satisfaction with the attitude of primary health care workers (39), and social integration (40) were responsible for an increased utilization of local public health services among domestic migrants in China.
The strengths of this study were to focus on the relationship between geodemographic factors and access to public health services. To my best knowledge, this was the first study to report the associations between geodemographic factors and access to public health services among the Chinese floating population. The current study used multistage clustering random sampling method and large sample size, which increases the generalizability of the findings.
There were two limitations. First, cross-sectional data cannot reflect dynamic relationships. The cross-sectional design limited the ability to get more valuable conclusions related to causality. Second, samples of Beijing, Tianjin, Shanghai, Hongkong, Macao, and Taiwan were less than 100. Compared to large sample of the other provincial-level units, the statistical results in the provincial-level units with small samples lacked significance. Especially, significant associations of geodemographic factors with types of access to health knowledge and methods of access to health knowledge could be confirmed in part of the provincial-level units (provincial-level units with significant outcomes/total provincial-level units: 30/35 and 16/35).
The main findings of this study were regional imbalance in the case of establishment rate of health records, social medical insurance ratio, access to health knowledge ratio, and methods of access to health knowledge ratio. Regional differences were associated with social medical insurance and the methods of health knowledge attainment. The findings of this study were a good angle from which to recommend the national plans and policies related to the floating population.
For the purpose of boosting the health and well-being of the Chinese floating population, public health services for migrant populations should be improved. With respect to policy improvement and its future directions in China's floating population, this study indicated biased investment should be provided to public health services in unprivileged regions, areas neglected by policy, and economically undeveloped areas. Additional compensatory investment should be introduced to ensure public health services to remain adequately funded. The local governments of provincial-level units should launch targeted policies such as health knowledge education for the floating population. In order to promote the equalization of essential public health services, social organizations and community should undertake the responsibility in social support for the internal migrants. Meanwhile, comprehensive measures to improve capacity of primary health care sectors must be emphasized. Practically, recommendations to enable migrants to obtain basic public health services include abolishing the separation of local and migrant household registration, increasing local government's fiscal capacity, and improving multi-sector cooperation with health information systems.
In conclusion, access to public health services is low and varied widely across provincial-level units. Significant associations between geodemographic factors and access to public health services among Chinese floating population were confirmed in part of the country. Due to its unintended consequences, geographic imbalance of public health services should be paid attention by local policy-designers. Particularly, the targeted improvement of the effectiveness of health management needs an increase of local funds.
Publicly available datasets were analyzed for this study. These can be found here: The survey dataset used in this study could be obtained on the website: http://www.chinaldrk.org.cn/wjw/#/home.
MG is head of the International Issues Center and Family Issues Center at Xuchang University. He is interested in health care service, health change, and quality of life of migrants and elders in modern China.
MG designed the study, performed the statistical analysis, and completed the original version.
This project was funded by the Study on the Influence Mechanism of Human Social Factors on the Health of Floating Population (in Chinese: 人文社会因素对流动人口健康影响机制研究 ; Project number: 2021-ZDJH-0342) from 2021 general projects of Humanities and Social Sciences in the Henan Provincial Higher Education (in Chinese: 2021年度河南省高校人文社会科学研究一般项目), Multi-dimensional Evaluation of Health Service System of Floating Population in Henan Province (in Chinese: 河南省流动人口健康服务体系多维度评价研究; Project number: 2020BSH014) from 2020 Planning of Philosophy and Social Sciences in Henan Province (in Chinese: 2020年河南省哲学社会科学规划年度项目), and Research on the improvement of population mobility-driven health service system (in Chinese: 人口流动驱动的卫生服务体系改进; Project number: 2020ZD019) from 2020 Key Research Projects of Xuchang University (in Chinese:2020年许昌学院重点研究项目). This project was also funded by Construction study and practice of ideological and political teaching in the course of China Geography (in Chinese: 《中国地理》课程; Project number: 407) from Research and Practice Project of Higher Education & Pedagogy Reform in Henan Province in 2019 (in Chinese: 2019年度河南省高等教育教学改革研究与实践项目).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author of this paper would like to acknowledge the very helpful comments of two reviewers on the original submission.
XPCC, Xinjiang Production and Construction Corps; NRCMS, new rural cooperative medical scheme; CMIURR, Cooperative medical insurance for urban and rural residents; URBMI, urban resident based basic medical insurance; UEBMI, urban employee-based basic medical insurance; FMT, free medical treatment; knpatha, access to health knowledge with lecture; knpathb, access to health knowledge with books/magazine/CD; knpathc, access to health knowledge with radio/TV programmes; knpathd, access to health knowledge with face-to-face consultation; knpathe, access to health knowledge with online medical consultation; knpathf, access to health knowledge with community advocacy; knpathg, access to health knowledge with bulletin board; knpathh, access to health knowledge with SMS/WeChat; kntypea, access to occupational disease prevention knowledge; kntypeb, access to nutritional health knowledge; kntypec, access to reproduction and contraception/eugenics knowledge; kntyped, access to chronic disease prevention knowledge; kntypee, access to smoking control knowledge; kntypef, access to mental disorders knowledge; kntypeg, access to tuberculosis knowledge; kntypeh, access to STD/AIDS knowledge; kntypei, access to other infectious diseases knowledge; ERHR, establishment rate of health records; SMIR, social medical insurance ratio; IHKR, inaccess health knowledge ratio; MIHKR, methods of inaccess to health knowledge ratio; ERHR, persons with health records/total sample; SMIR, persons with social medical insurance/ total sample; IHKR, persons with inaccess to health knowledge/ total sample; MIHKR, persons with inaccess methods of access to health knowledge/ total sample; MIMIC, Multiple indicator multiple cause model; PCA, Principal component analysis; KMO, Kaiser-Meyer-Olkin; RMSEA, root mean square error of approximation; IRB, Institutional Review Board.
1. Liang Z, Li Z, Ma Z. Changing patterns of the floating population in China during 2000-2010. Popul Dev Rev. (2014) 40:695–716. doi: 10.1111/j.1728-4457.2014.00007.x
2. Wang JW, Cui ZT, Cui HW, Wei CN, Harada K, Minamoto K, et al. Quality of life associated with perceived stigma and discrimination among the floating population in Shanghai, China: a qualitative study. Health Promot Int. (2010) 25:394–402. doi: 10.1093/heapro/daq039
3. Duan JJ, Wang D, Nie J. Analysis of self-rated health status of the floating population in a district of Guangzhou. Nan Fang Yi Ke Da Xue Xue Bao. (2008) 28:998–1000.
4. Yan QL, Yang Y, Gao YY, Hou RF, Zhang X, Dai MX, et al. Mental health status and its influencing factors in the floating population in Chengdu. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. (2019) 41:729–36. doi: 10.3881/j.issn.1000-503X.11196
5. Wang X, Wu J, Li Y, Zhou Y, Li Y, Zhao R, et al. Changes in the prevalence of induced abortion in the floating population in major cities of China 2007-2014. Int J Environ Res Public Health. (2019) 16:E3305. doi: 10.3390/ijerph16183305
6. Zhou Y, Wang T, Fu J, Chen M, Meng Y, Luo Y. Access to reproductive health services among the female floating population of childbearing age: a cross-sectional study in Changsha, China. BMC Health Serv Res. (2019) 19:540. doi: 10.1186/s12913-019-4334-4
7. Guo W, Tan Y, Yin X, Sun Z. Impact of PM2.5 on second birth intentions of China's floating population in a low fertility context. Int J Environ Res Public Health. (2019) 16:E4293. doi: 10.3390/ijerph16214293
8. Han K, Yao J, Yin X, Zhao M, Sun Q. Review on the prevalence of diabetes and risk factors and situation of disease management in floating population in China. Glob Health Res Policy. (2017) 2:33. doi: 10.1186/s41256-017-0053-8
9. Zhao Y, Zhang M, Wang L, Li Y, Deng Q, Huang Z, et al. Physical activities and sedentary behavior among the Chinese floating population aged 18-59 in 2012. Zhonghua Liu Xing Bing Xue Za Zhi. (2014) 35:1208–11.
10. Li Y, Zhang M, Jiang Y, Deng Q, Zhao Y, Huang Z, et al. Drinking behaviors and patterns among floating population aged 18-59 years old in China, (2012). Zhonghua Liu Xing Bing Xue Za Zhi. (2014) 35:1186–91.
11. Huang Z, Wang L, Zhang M, Deng Q, Wang Z, Zhao Y, et al. Smoking behavior among the Chinese employed floating population aged 18-59 in 2012. Zhonghua Liu Xing Bing Xue Za Zhi. (2014) 35:1192–7.
12. Meng Y, Han J, Qin S. The impact of health insurance policy on the health of the senior floating population-evidence from China. Int J Environ Res Public Health. (2018) 15:E2159. doi: 10.3390/ijerph15102159
13. Cai X, Yang F, Bian Y. Gap analysis on hospitalized health service utilization in floating population covered by different medical insurances — case study from Jiangsu Province, China. Int J Equity Health. (2019) 18:84. doi: 10.1186/s12939-019-0992-4
14. Guan YQ, Zhang M, Zhang X, Zhao ZP, Huang ZJ, Li C, et al. Medical treatment seeking behaviors and its influencing factors in employed floating population in China. Zhonghua Liu Xing Bing Xue Za Zhi. (2019) 40:301–8. doi: 10.3760/cma.j.issn.0254-6450.2019.03.009
15. Yuan YF, Ji Y, Jiang Y, Zeng QQ, Chang C. [Analysis of utilization of public health services and associated factors among young migrants aged 15 to 24]. Beijing Da Xue Xue Bao Yi Xue Ban. (2012) 44:602–6.
16. Tang S, Long C, Wang R, Liu Q, Feng D, Feng Z. Improving the utilization of essential public health services by Chinese elderly migrants: strategies and policy implication. J Glob Health. (2020) 10:010807. doi: 10.7189/jogh.10.010807
17. Zhang J, Lin S, Liang D, Qian Y, Zhang D, Hou Z. Public health services utilization and its determinants among internal migrants in China: evidence from a nationally representative survey. Int J Environ Res Public Health. (2017) 14:1002. doi: 10.3390/ijerph14091002
18. Guo L, Bao Y, Li S, Ma J, Sun W. Quality analysis and policy recommendations on the utilization of community basic public health services in urban and suburban Shanghai from 2009 to 2014. Environ Sci Pollut Res Int. (2018) 25:28206–15. doi: 10.1007/s11356-018-2811-7
19. Chen ZH, Zhang M, Li YC, Huang ZJ, Wang LM. Co-prevalence of chronic disease risk factors and influencing factors in floating population in China. Zhonghua Liu Xing Bing Xue Za Zhi. (2017) 38:1226–30. doi: 10.3760/cma.j.issn.0254-6450.2017.09.017
20. Li X, Zhang H, Jiang S, Wang J, Liu X, Li W, et al. Active pulmonary tuberculosis case detection and treatment among floating population in China: an effective pilot. J Immigr Minor Health. (2010). 12:811–5. doi: 10.1007/s10903-010-9336-6
21. Ou YQ, Nie ZQ, Liu XQ, Mai JZ, Wu Y, Gao XM, et al. Study on the differences of risk factors regarding congenital heart defects between floating population and permanent residents in Guangdong. Zhonghua Liu Xing Bing Xue Za Zhi. (2013) 34:701–5.
22. Zhang R, Zhe W, Liao P, Zhang Y, Liu L, Ni M, et al. (2018). [Prevalence of central obesity among floating population employment in 5 surveillance sites of Xinjiang Uygur Autonomous Region 2012]. Wei Sheng Yan Jiu. (2018) 47:395–8.
23. Su L, Sun L, Xu L. Review on the prevalence, risk factors and disease management of hypertension among floating population in China during 1990-2016. Glob Health Res Policy. (2018) 3:24. doi: 10.1186/s41256-018-0076-9
24. Lu XP, Wu M. Determinants of household healthcare expenditure of rural floating population in Beijing: a Tobit model approach. Beijing Da Xue Xue Bao Yi Xue Ban. (2010) 42:565–9.
25. Zhao Y, Kang B, Liu Y, Li Y, Shi G, Shen T, et al. Health insurance coverage and its impact on medical cost: observations from the floating population in China. PLoS ONE. (2014) 9:e111555. doi: 10.1371/journal.pone.0111555
26. Wang JW, Cui ZT, Ding N, Zhang CG, Usagawa T, Berry HL, et al. A qualitative study of smoking behavior among the floating population in Shanghai, China. BMC Public Health. (2014) 14:1138. doi: 10.1186/1471-2458-14-1138
27. Liu H, Wang Q, Lu Z, Liu J. Reproductive health service use and social determinants among the floating population: a quantitative comparative study in Guangzhou city. BMC Health Serv Res. (2014) 14:502. doi: 10.1186/s12913-014-0502-8
28. Chen LX, Liang H, Yang XB. Meta-analysis on the effects of health education towards HIV/AIDS high-risk behavior, knowledge, and related attitude among floating population in China. Zhonghua Liu Xing Bing Xue Za Zhi. (2012) 33:99–105.
29. Zhang L, Wu M. Analysis on status and determinants of self-treatment of rural floating population in Beijing. Beijing Da Xue Xue Bao Yi Xue Ban. (2015) 47:455–8.
30. Niu H, Tian M, Ma A, Wang C, Zhang L. Differences and determinants in access to essential public health services in China: a case study with hypertension people and under-sixes as target population. Chin Med J. (2014) 127:1626–32.
31. Yin D, Wong ST, Chen W, Xin Q, Wang L, Cui M, et al. A model to estimate the cost of the National essential public health services package in Beijing, China. BMC Health Serv Res. (2015) 15:222. doi: 10.1186/s12913-015-0902-4
32. Chen T, Wang Y, Luo X, Rao Y, Hua L. Inter-provincial inequality of public health services in China: the perspective of local officials' behavior. Int J Equity Health. (2018) 17:108. doi: 10.1186/s12939-018-0839-4
33. Yuan H, Li H, Hou Z. Is it worth outsourcing essential public health services in China?-Evidence from Beilin district of Xi'an. Int J Health Plann Manage. (2020) 35:1486–502. doi: 10.1002/hpm.3051
34. Wang Z, Ao Q, Luo Y, Wang Q, Lu Z, Liu J. Estimating the costs of the national basic public health services in Zhuhai, China, through activity-based costing: a cross-sectional study. BMJ Open. (2019) 9:e024831. doi: 10.1136/bmjopen-2018-024831
35. Liu X, Mills A. Financing reforms of public health services in China: lessons for other nations. Soc Sci Med. (2002) 54:1691–8. doi: 10.1016/S0277-9536(01)00337-9
36. Zhao Y, Cui S, Yang J, Wang W, Guo A, Liu Y, et al. Basic public health services delivered in an urban community: a qualitative study. Public Health. (2011) 125:37–45. doi: 10.1016/j.puhe.2010.09.003
37. Hou Z, Lin S, Zhang D. Social capital, neighbourhood characteristics and utilisation of local public health services among domestic migrants in China: a cross-sectional study. BMJ Open. (2017) 7:e014224. doi: 10.1136/bmjopen-2016-014224
38. Meng X. Does a different household registration affect migrants' access to basic public health services in China? Int J Environ Res Public Health. (2019) 16:4615. doi: 10.3390/ijerph16234615
39. Liu J, Mao Y. Rural resident experience on national basic public health services: a cross-sectional survey in 10 Western provinces of China. Healthcare. (2019) 7:160. doi: 10.3390/healthcare7040160
Keywords: floating population, geographical differences, health knowledge, health records, social medical insurance
Citation: Guan M (2020) Associations Between Geodemographic Factors and Access to Public Health Services Among Chinese Floating Population. Front. Public Health 8:563180. doi: 10.3389/fpubh.2020.563180
Received: 18 May 2020; Accepted: 09 November 2020;
Published: 10 December 2020.
Edited by:
Sunjoo Kang, Yonsei University, South KoreaReviewed by:
Hye-Kyung Oh, Daegu University, South KoreaCopyright © 2020 Guan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Guan, Z21pbmcwNjA0QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.