
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 04 September 2020
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.00443
This article is part of the Research Topic Tuberculosis and Non- Tuberculous Mycobacteria Infections: Control, Diagnosis and Treatment View all 18 articles
 Frédéric Méchaï1*
Frédéric Méchaï1* Hugues Cordel1
Hugues Cordel1 Lorenzo Guglielmetti2,3
Lorenzo Guglielmetti2,3 Alexandra Aubry2,3
Alexandra Aubry2,3 Mateja Jankovic4
Mateja Jankovic4 Miguel Viveiros5
Miguel Viveiros5 Miguel Santin6
Miguel Santin6 Delia Goletti7
Delia Goletti7 Emmanuelle Cambau2,8 on behalf of the ESGMYC group†
Emmanuelle Cambau2,8 on behalf of the ESGMYC group†Objectives: To evaluate and compare practices regarding the diagnosis, isolation measures, and treatment of tuberculosis (TB) in high-income countries and mainly in Europe.
Materials and Methods: A survey was conducted from November 2018 to April 2019 within the European Society of Clinical Microbiology and Infectious Diseases Study Group for Mycobacterial Infections (ESGMYC). The practices observed were compared to the main international guidelines.
Results: Among 136 ESGMYC members, 64 (17 countries) responded to the questionnaire. In their practice, two (20.7%) or three sputum samples (79.3%) were collected for the diagnosis of pulmonary TB, alternatively induced sputum (n = 37, 67.2%), bronchoscopy (34, 58.6%), and gastric aspirates (15, 25.9%). Nucleic acid amplification tests (NAATs) were performed by 41 (64%) respondents whatever the smear result and by 47 (73%) in case of smear-positive specimens. NAAT and adenosine deaminase measurement were used for extrapulmonary TB diagnosis in 83.6 and 40.4% of cases, respectively. For isolation duration, 21 respondents (42.9%) were keeping isolation until smear negativity. An initial treatment without ethambutol was offered by 14% (n = 9) of respondents. Corticosteroid therapy, cerebrospinal fluid opening pressure testing, and repeated lumbar puncture were carried out for central nervous system TB by 79.6, 51.9, and 46.3% of the respondents, respectively. For patients with human immunodeficiency virus–TB coinfection, the preferred antiretroviral therapy included dolutegravir 50 mg twice a day (56.8%). Comparing with the recommendations of the main guidelines, the practices are not totally consistent.
Conclusion: This study shows heterogeneous practices, particularly for diagnosis, and isolation, although rapid molecular testing is implemented in most centers. More standardization might be needed.
In 2017, 10 million people were diagnosed with tuberculosis (TB) in the world (1, 2). Although the European region accounted for only 3% of all cases (3), TB remains a common infection. Despite a rate of latent TB estimated at 23% of the world population, there are very large disparities in incidence between continents and countries with an incidence of fewer than 10 per 10,000 inhabitants in Western Europe to more than 500 per 100,000 for countries such as South Africa, the Philippines, and Mozambique (2). The overall objective of the World Health Organization (WHO) by 2035 (The End TB strategy) is to reduce the number of deaths from TB by 95% (compared to 2015) and to reduce the incidence rate of TB by 90% to fewer than 10 per 100,000 people. In 2016, 58,994 cases of TB were reported in 30 European Union/European Economic Area (EU/EEA) countries (2). The decreasing notification rates observed in most countries are reassuring, but annual rates of decline are still insufficient to achieve the WHO target of TB elimination by 2050 in European low-incidence countries. Multidrug-resistant (MDR) TB was reported for 3.7% of 36,071 cases with drug susceptibility testing results and continues to be the highest (more than 10%) in the three Baltic countries. Extensively drug-resistant (XDR) TB was reported for 20.1% of 984 MDR TB cases tested for second-line drug susceptibility (4). Data on human immunodeficiency virus (HIV) coinfection remained widely incomplete in Europe. Of all TB cases with known HIV status, 4.5% were coinfected with the virus (5).
An evaluation of TB case management in the EU/EEA countries, with special focus on MDR and XDR-TB, was conducted in 2010, using a standardized survey tool in five European centers. Deviations from international standards of TB care were observed in the following areas: surveillance (no information available on patient outcomes); infection control (lack of respiratory isolation rooms/procedures and negative-pressure ventilation rooms); clinical management of TB, MDR-TB, and HIV coinfection (inadequate bacteriological diagnosis, regimen selection, and treatment duration); laboratory support; and diagnostic/treatment algorithms (6).
A response to this need of harmonization has already been initiated through the development of European Union Standards for TB Care (ESTC) in 2012 with an update in 2017. They identified key standards for the diagnosis, management, prevention, and control of TB, MDR-TB, and XDR-TB. These standards aim to support health care workers in optimizing TB case management and thus at contributing to improved TB control in the EU/EEA (7–11). In fact, after the implementation of these standards, the knowledge of appropriate TB case management in high-income countries and in particular the different European countries is scarce. The main aim of this study was therefore to verify the current good homogeneity of practices of the different actors involved in the fight against TB and to compare them with the main national or international recommendations.
A survey was conducted from November 2018 to April 2019 among members of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Mycobacterial Infections (ESGMYC), an offshoot of the ESCMID. The questionnaire was initially sent out on November 8, 2018, with subsequent reminders, the last being sent on March 15, 2019. The online questions comprised 63 items and focused on three topics: (1) diagnosis of TB, (2) isolation and prevention of TB transmission, and (3) TB treatment (summarized in Table 1). Descriptive statistics were used to analyze the results of the survey. The data were analyzed using STATA 10.0 (StataCorp LP, College Station, TX, USA). Paris-Seine-Saint-Denis University Hospitals Committee review waived the requirement for ethical approval for this study because of absence of interventional research on the human person, in accordance with the national legislation and the institutional requirements.
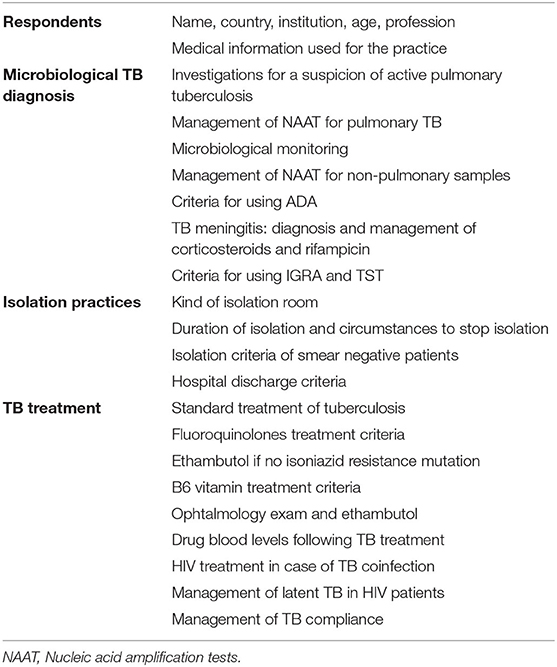
Table 1. Summary of the questionnaire.
In a second step, in order to understand the differences in the management of TB in high-income countries, we compared the participants' responses to the main principles of TB management according to the following international recommendations: Infectious Disease Society of America/Centers for Disease Control/American Thoracic Society (IDSA/CDC/ATS) guidelines (12, 13), National Institute for Health and Care Excellence (NICE) guidelines (14), ERS/ECDC (European Respiratory Society/European Centers for Disease Control) guidelines (11), WHO (15), and the recommendations of the French Hospital Hygiene Society (16). These are summarized in Tables 2–4 for comparing the proposals of each academic society.
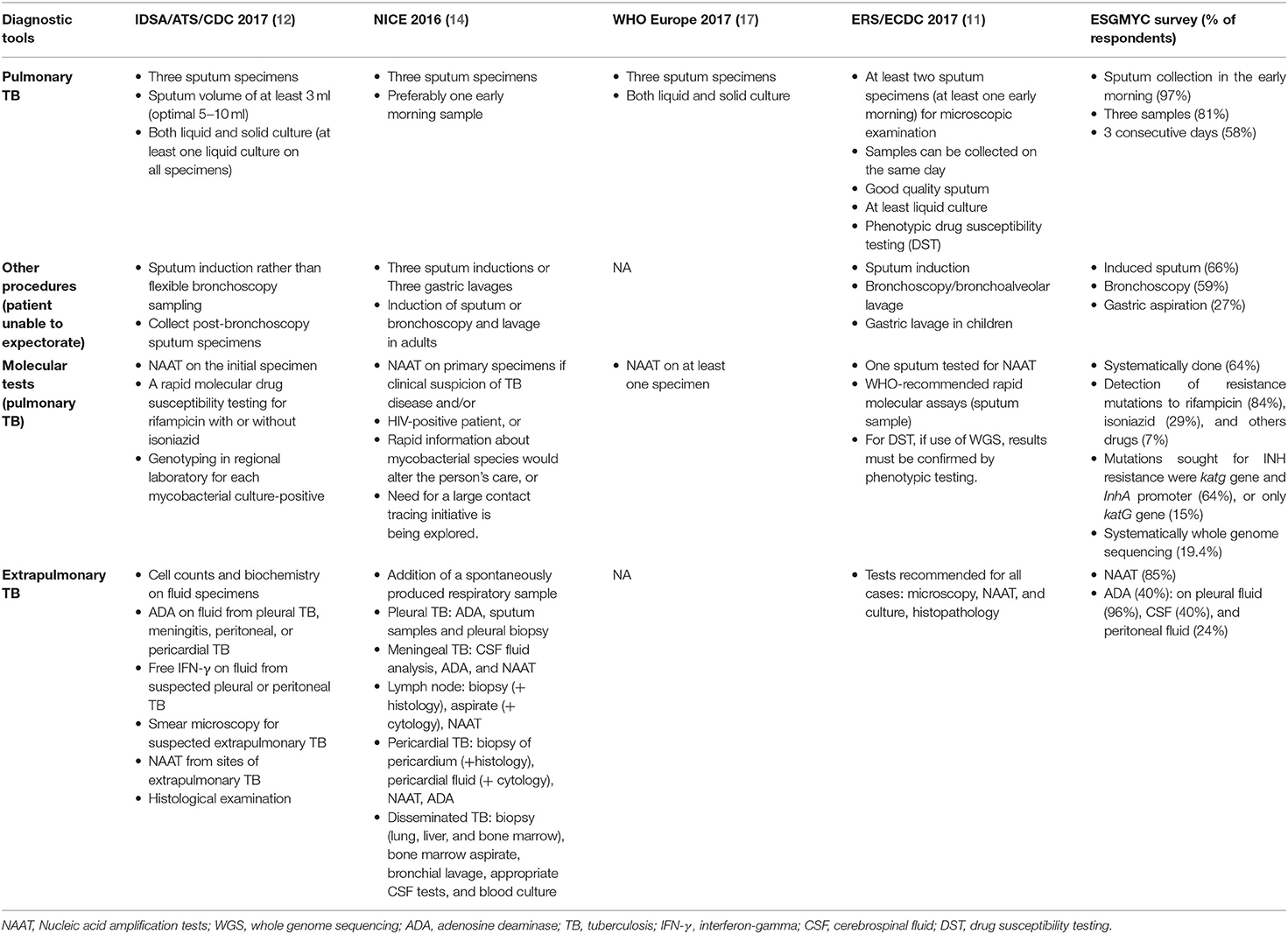
Table 2. Microbiological TB diagnosis: synthesis of the international recommendations and main results from the ESGMYC survey.
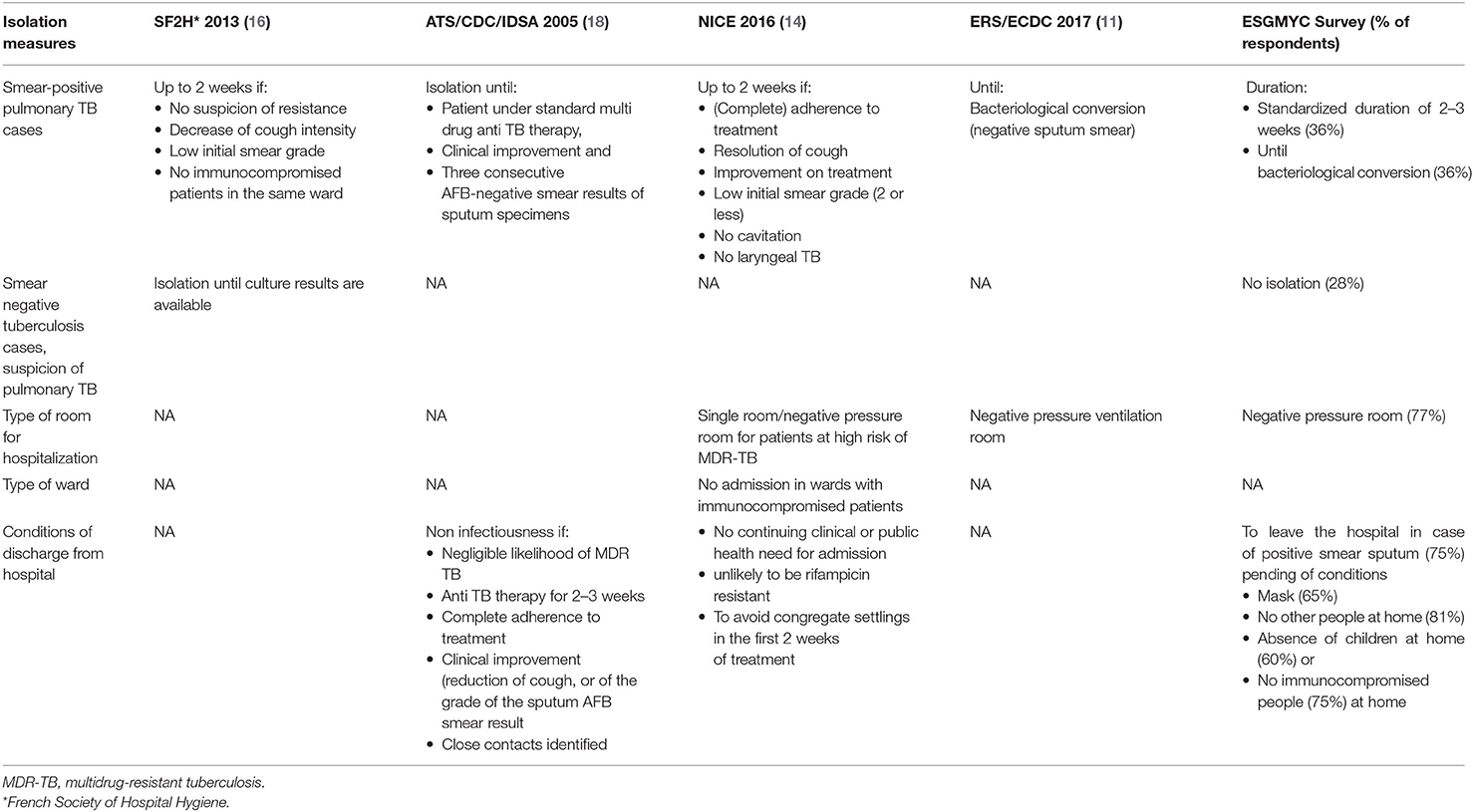
Table 3. Isolation measures recommended for pulmonary tuberculosis patients in healthcare settings: synthesis of international recommendations and ESGMYC survey main results.
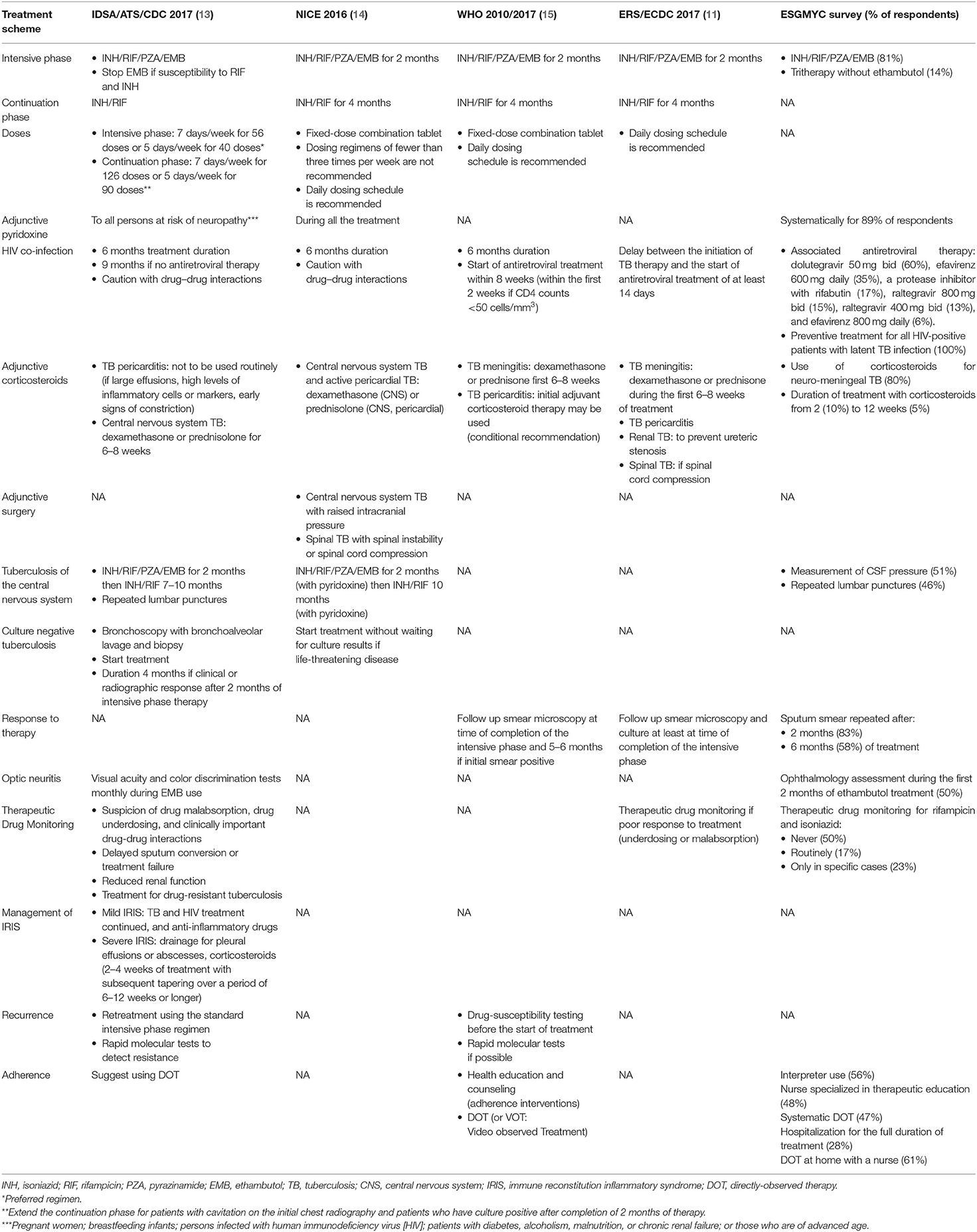
Table 4. Drug-susceptible tuberculosis treatment: synthesis of international recommendations and ESGMYC survey main results.
Among 136 ESGMYC members, 64 (47.1%) responded to the questionnaire representing 14 European countries (Albania, Croatia, Denmark, Germany, Greece, France, Italy, Netherlands, Norway, Romania, Spain, Sweden, Switzerland, Turkey, and the United Kingdom), with 1–13 per country, and 3 non-European countries (New Zealand, Singapore, and Australia; Figure 1). Median age was 44 years (interquartile range = 38–51 years). The participants were working in an infectious diseases (67%, n = 43/64) or clinical microbiology (30%, n = 19/64) department. Sources of medical information for their practice were national guidelines alone for 8% (n = 5/64) of them, international guidelines only for 11% (n = 7/64), and an association of both for 64% (n = 41/64). TB specialist opinion was consulted, alone or together with other sources, by 50% (n = 32/64) of respondents. Among international recommendations, the main source was the WHO guidelines for 34% of respondents (n = 15/44).
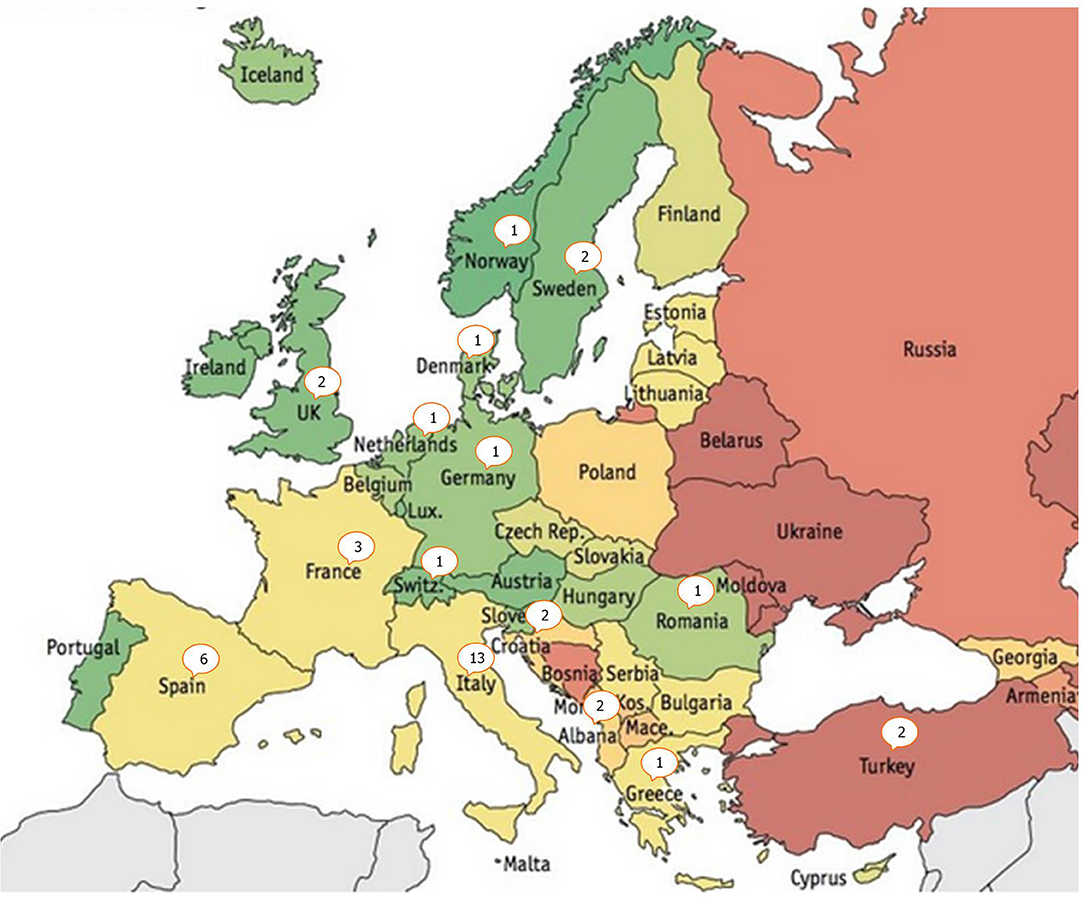
Figure 1. Europe map presenting the number of respondents per country.
For the microbiological diagnosis of pulmonary TB, 97% (n = 62/64) of respondents used to collect at least one sputum in the early morning on an empty stomach, with 19% (n = 12/64) and 81% collecting two or three samples, respectively. The two remaining responders collected induced or spontaneous sputum at admission or randomly timed sputum sample. Multiple samples are usually taken during 3 consecutive days (58%, n = 37/64), or 2 (33%, n = 21/64) or within the same day (17%, n = 11/64). If the patient could not produce sputum, the alternatives were induced sputum (66%, n = 42/64), bronchoscopy aspirate (59%, n = 38/64), and gastric aspiration (27%, n = 17/64).
A rapid molecular test was performed systematically by 41/64 (64%) respondents, on one (31%, n = 14/45) or multiple respiratory specimens (33%, n = 15/45). In case of strong suspicion of pulmonary TB with negative sputum smears, 16/64 (25%) respondents would start treatment, 11/64 (17%) would wait for the culture result before starting, and 44/64 (78.6%) would perform additional diagnostic tests, namely, rapid molecular tests (66%), or bronchoscopy aspirate testing (61.3%). In case of positive sputum smear, a rapid molecular test was performed to detect mutations conferring resistance to rifampicin by 84% (n = 52/64), to isoniazid by 29% (n = 18/62), and to other drugs by 7% (n = 4/62), whereas 10 (16%) did not perform any rapid molecular test. Regarding the type of mutation sought for isoniazid resistance, among the 26 microbiologists who gave an answer, 17 (65%) perform rapid molecular tests to detect mutations in both katG gene and the inhA promoter, and four only in the katG gene (15%). Eight respondents (31%) were looking for genotypic resistance to other drugs besides rifampicin and isoniazid, with five of them performing whole-genome sequencing.
In the case of positive culture, of 61 respondents, 38 (62%) were asking for molecular detection of rifampicin resistance mutation, 24 (39%) for an isoniazid resistance mutation, and 9 (15%) for resistance mutations to other drugs, whereas 23 (38%) were not looking for genotypic resistance.
For the diagnosis of extrapulmonary TB, nucleic acid amplification test (NAAT), and measurement of adenosine deaminase (ADA) were performed in 85% (n = 52/61 responses) and 40% (n = 25/62 responses) of cases, respectively. ADA was performed mainly for the diagnosis of pleural effusion (96%, n = 24/25), but also on the cerebrospinal fluid (CSF) (40%, n = 10/25) in case of suspicion of TB meningitis and on peritoneal fluid (24%, n = 6/25). Sputum smear was repeated after 2 and 6 months of treatment by 53/63 (83%) and 37/63 (58%) participants, respectively. Overall, interferon-γ release assays (IGRAs) and tuberculin skin testing (TST) were performed by 31% (n = 20/64) and 23% (n = 15/64) of respondents, respectively, even for the diagnosis of active TB.
Overall, 23% (n = 15/63) of respondents used a conventional single room to isolate pulmonary TB patients, whereas 77% (n = 50/63) reported using a negative-pressure room whatever the drug susceptibility profile of the strain. Regarding the duration of isolation for pulmonary TB with smear-positive sputum, 23/64 (36%) respondents adopted a standardized duration of 2 to 3 weeks, whereas 23/64 (36%) reported waiting for the sputum smear-negative conversion. In case of patients hospitalized with a suspicion of pulmonary TB but negative sputum smears and pending culture results, 18/64 (28%) of the respondents did not isolate the patient. Patients with a positive sputum smear were allowed to leave the hospital by 75% (n = 48/64) of respondents, in the following cases: if they agreed to wear a mask (n = 31/48, 65%), if there were no other people at home (n = 39/48, 81%), and in the absence of children (n = 29/48, 60%) or of immunocompromised individuals (n = 36/48, 75%) at home.
A majority of respondents (81%, n = 52/64) used the standard first-line treatment with isoniazid, rifampicin, pyrazinamide, and ethambutol for 2 months, followed by 4 months of treatment with isoniazid and rifampicin; but 14% (n = 9/64) of respondents offered an initial treatment without ethambutol. Fluoroquinolones were never prescribed as part of first-line treatment by 29/61 (45%) of respondents; conversely, 5/61 (8%) and 26/61 (41%), respectively, used them under certain conditions such as bone TB or suspicion of resistance to isoniazid. Overall, 30% (n = 19/63) of respondents reported to discontinue ethambutol treatment in the absence of mutations conferring resistance to isoniazid. Among respondents, 89% (n = 57/63) systematically gave B6 vitamin therapy. With regard to treatment monitoring, 50% (n = 32/62) of respondents performed an ophthalmology assessment during the first 2 months of ethambutol treatment. Overall, 50% (n = 32/64) of respondents never performed therapeutic drug monitoring for rifampicin and isoniazid, 17% (n = 11/64) routinely performed it, and 23% (n = 15/64) performed it only in specific cases (i.e., HIV infection, overweight, renal insufficiency). For neuromeningeal TB cases, 80% (43/54) of respondents added corticosteroids to the TB treatment for a variable duration, from 2 (10%, n = 4/40 respondents) to 12 weeks (5%, n = 2/40). The measurement of CSF pressure and repeated lumbar punctures were performed by 51% and 46% of the 59 respondents, respectively. In case of HIV coinfection, the most frequently used antiretroviral drugs were dolutegravir 50 mg twice a day (BID) (60%, n = 29/48 respondents), efavirenz 600 mg daily (35%, n = 17/48), a protease inhibitor with rifabutin (17%, n = 8/48), raltegravir 800 mg BID (15%, n = 7/48), raltegravir 400 mg BID (13%, n = 6/48), and efavirenz 800 mg daily (6%, n = 3/48). All respondents offered preventive treatment to HIV-positive patients with latent TB infection, using the following: isoniazid for 6 months (84%, n = 43/51 respondents), isoniazid and rifampicin for 3 months (24%, n = 12/51), rifampicin for 3–4 months (24%, n = 12/51), or isoniazid plus rifapentine for 3 months (4%, n = 2/51). To optimize adherence and treatment support, clinicians used an interpreter (56%, n = 36/64), a nurse specialized in therapeutic education (48%, n = 31/64), systematic Directly Observed Therapy (DOT) (47%, n = 30/64), or hospitalization for the full duration of treatment (28%, n = 18/64). As an alternative to hospitalization, 39/64 (61%) offered a DOT at home with a nurse.
TB continues to be a priority public health challenge in high-income countries. While EU/EEA countries adopted the key principles of TB control and elimination through the Europe-specific consensus-based documents born within the Wolfheze initiative and subsequent documents, a uniform set of guidelines summarizing essential standards to guide European clinicians and health care workers was developed only in 2012 (7, 8). Both International Standards for Tuberculosis Control (ISTC) and ESTC prescribe a widely accepted level of TB care, to guide all health care providers and clinicians, both public and private, in achieving optimal standards in managing individuals who have active TB, latent TB infection, or signs and symptoms compatible with the disease. The standards are designed to complement existing national or international guidelines and are consistent with the WHO definitions and recommendations (15, 17).
Our survey of TB management shows that practical attitudes currently can differ in some respects.
Regarding the diagnosis of TB, the practices are relatively consensual with the continued use of sputum examination, although the modalities may differ in number or timeframe (19). It should be noted, however, that 13.8% of participants performed only one sputum examination, whereas the guidelines always recommend performing at least two sputum smears (Table 1). Alternative examinations when patients were unable to provide a sputum sample vary according to the centers with equally heterogeneous guidelines: IDSA/ATS/CDC recommendations favor sputum induction compared to bronchoscopy. NICE guidelines are the only ones to propose gastric lavage, whereas 25.9% of respondents use it in clinical practice (Table 1) (20, 21). We observed that almost all centers use NAAT, although these tests are not yet carried out systematically for the diagnosis of TB (only 62.1% of respondents) as recommended by the guidelines (19, 22, 23). Despite recommendations to look for mutations conferring resistance to rifampicin and isoniazid, 16% of participants did not perform rapid molecular detection testing for rifampicin resistance in case of smear-positive patients (24, 25). For extrapulmonary TB, a majority of participants (86.3%) in the survey performed several rapid molecular tests as recommended by international guidelines. In contrast, the measurement of ADA was not universally used (40%), and it was mainly confined to pleural fluid. This recommendation is not consistent across all guidelines, because the ADA is used only for the ATS/ IDSA/CDC and NICE guidelines for pleural fluid, peritoneal fluid, and CSF. The monitoring of sputum smear microscopy and sputum culture is only recommended in the ERS/ECDC and WHO guidelines at least at the end of completion of intensive phase and actually performed after 2 months of treatment by most participants (82.5%). Finally, it should be noted that almost a third and a quarter of the responders, respectively, used IGRA and TST tests for diagnosis, whereas this is not recommended in most guidelines. These tests cannot effectively differentiate active and latent TB, even though a phlyctenular TST could predict rather an active TB (26).
Concerning the prevention of the risk of transmission of TB, the ERS/ECDC and NICE guidelines clearly specify the need to isolate the patient in a negative-pressure chamber, whereas 22% of the participants did not (14, 18). The isolation duration of contagious patients remains controversial, with 36% of respondents having adopted standardized isolation duration of 2–3 weeks, like the guidelines of NICE and the French Hospital Hygiene Society (14, 16); 43% prefer to wait for sputum smear conversion, as recommended by WHO and ATS/IDSA/CDC guidelines (13, 15). It should be noted that the conditions for patients discharged from health care facilities remains poorly studied, and this lack of evidence is reflected in the international recommendations from academic societies.
Regarding the treatment of TB, the initial treatment with four drugs is highly consensual between the respondents and the different recommendations; however, 14% still prescribed an initial treatment with only three drugs (respondents from different countries). The role of rapid molecular tests for resistance to isoniazid in guiding the withdrawal of ethambutol from the intensive phase treatment is yet unclear. The role of fluoroquinolones in first-line treatment, pyridoxine prophylaxis, CSF pressure measurement, and therapeutic drug monitoring should be better defined with additional studies. Similarly, monthly ophthalmologic monitoring of ethambutol patients is recommended only by the North American ATS/IDSA/CDC guidelines (13). On the other hand, the use of corticosteroids in the treatment of central nervous system TB is well established in the literature and among the various guidelines, whereas 20% of the participants in our survey did not routinely prescribe corticosteroids. Among HIV-positive patients, it is well established that the duration of TB treatment should be identical to that of HIV-negative patients. The importance of managing drug–drug interactions is also well emphasized in the different guidelines, although there is no clear recommendation on which antiretrovirals should be used in combination with rifampicin. Counseling is mostly developed in WHO guidelines, which target low-resource countries. The collaboration of the interpreter and the nurse in therapeutic education is still infrequent for the stakeholders of our study: 57 and 50%, respectively, whereas most European countries report increasing TB rates among newly arrived migrants (27, 28).
It is difficult to analyze the variability of practices observed between the different respondents. There may be variability between countries due to different local recommendations but also a disparity of human or economic resources. The availability of medications, funding of TB programs, laboratory practice, staff availability, and TB epidemiology can differ between countries, but this phenomenon is probably lower in high-resource European countries than on other continents. Furthermore, in our survey, 7% of respondents used only local recommendations for TB care management, whereas 78% also relied on international recommendations, which should also limit the variability between countries. It must also be emphasized that interindividual variability within the same country is possible. Although the respondents are among the TB experts for each country, their management practice cannot be fully representative of their respective countries. For instance, the practice survey conducted in France in 2013 with specialists in infectious diseases, pneumology, and internal medicine showed that different doctors often had very different habits concerning the treatment of TB or the isolation of active TB (29). Finally, the heterogeneity of practices can also be partially explained by the heterogeneity between the different national or international recommendations, as we have seen above. This lack of consistency across the different guidelines, as it is the case, for example, with regard to isolation practices, can be confusing for the clinician.
The ISTC defined the essential level of care for managing patients who have or are presumed to have TB or are at increased risk of developing the disease. In a high-resource setting, such as the EU/EEA, higher standards of care can be attained with regard to TB diagnosis, prevention, and treatment. On this basis, the ESTC was published in 2012 as standards specifically tailored to the European setting. Since the publication of the ESTC, new scientific evidence has become available, and therefore, the standards were reviewed and updated in 2017. Despite these new standards tailored to the EU setting, the harmonization of practices needs to be further improved. This is conditioned by a better standardization of national and international recommendations, a wider communication with people in charge of TB, and complementary studies to increase the level of evidence on controversial aspects of TB care. If we take the example of the joint ERS and ESCMID guidelines on the management of infections due to nontuberculous mycobacteria, which are being updated, collaboration between the various European academic societies would probably be beneficial.
Our study has several limitations. First, our sample is too small to be representative. Second, the responders were selected within the ESGMYC group, with mainly microbiologists and infectious disease specialists. Therefore, this sample does not include a lot of pulmonary physicians, although they are also very involved in TB care. Third, as mentioned above, the management practice of the responders could not be fully representative of their respective countries. Nevertheless, we think that this survey gives an interesting overview of different practices in Europe and highlights a heterogeneity in the management of TB that should be confirmed by a study with larger sample. In conclusion, WHO's international recommendations for TB management are focused on countries with high incidence. Recommendations that are more adapted to the European socioeconomic and epidemiological context have also been developed under the auspices of the ERS and the ECDC. This study shows that the management of TB is probably still heterogeneous within high-income countries, in particular for the prevention of transmission and the treatment. Concerning microbiological diagnosis, the practices seem to be better standardized, as rapid molecular testing takes an important role across most European centers. With the main objective of control and eventual elimination of TB, it seems necessary to better harmonize and disseminate the recommendations for the management of TB in Europe. European scholarly societies, and in particular ESCMID, should play a prominent role.
The datasets analyzed in this article are not publicly available. Requests to access the datasets should be directed to ZnJlZGVyaWMubWVjaGFpQGFwaHAuZnI=.
All authors participated in the writing and editing of the article, the analysis of the data as well as the dissemination that the investigation at the origin of this work.
This work was supported by ESGMYC funding (ESCMID).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Alexander Eliza, Andresen David, Anibarro Luis, Armstrong Mark, Balas Iulia, Bradbury Ross, Burke Andrew, Calcagno Andrea, Chew Rusheng, Choong Keat, Cirillo Daniella, Comelli Agnese, Davis Joshua, Del Bravo Paola, Denholm Justin, Di Carlo Paola, Edmond Tess, Esteban Jaime, Faliero Domenico, García-Gasalla Mercedes, Garcia-Goez Jofer, Giordani Maria Teresa, Goic-Barisic Ivana, Gonzalez-Galan Verónica, Gray Thimoty, Grimwade Kate, Hasan Tasnim, Huang Khai, Iulia Balas, Jenkin Grant, Khatami Ameneh, Kocagoz Tanil, Lim Lyn-li, Mahony Andrew, Maurer Florian, Mazzarelli Antonio, Motta Ilaria, Oman Kimberly, Onya Opota, Ozturk-Engin Derya, Papaventsis Dimitrios, Paues Jakob, Pham David, Pickles Robert, Puca Edmond, Rajakaruna Gawri, Riccardi Niccolo, Saralardo, Sanchez Francesca, Syre Heidi, Tafaj Silva, Thomas Schön, Tiberi Simon, Timothy Gray, Wang Dingyuan Alvin, Wejse Christian, Whitmore Timothy, Woolley Ian, Van Ingen Jakko, Veziris Nicolas, Yograjsinh Sagar, Mohamad-Ali Trad.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00443/full#supplementary-material
1. Furin J, Cox H, Pai M. Tuberculosis. Lancet. (2019) 393:1642–56. doi: 10.1016/S0140-6736(19)30308-3
3. European Centre for Disease Prevention and Control/WHO Regional Office for Europe. Tuberculosis Surveillance and Monitoring in Europe 2018-2016 Data. Stockholm, European Centre for Disease Prevention and Control (2018). Available online at: https://ecdc.europa.eu/sites/portal/files/documents/ecdc-tuberculosis-surveillance-monitoring-Europe-2018-19mar2018.pdf
4. World Health Organization Regional Office for Europe. Roadmap to Implement the Tuberculosis Action Plan for the European Region 2016-2020. Towards Ending Tuberculosis and Multidrug-Resistant Tuberculosis. Copenhagen, WHO Regional Office for Europe, 2016.
5. Van der Werf MJ, Kodmon C, Zucs P, Hollo V, Amato-Gauci AJ, Pharris A. Tuberculosis and HIV coinfection in Europe: looking at one reality from two angles. AIDS. (2016) 30:2845–53. doi: 10.1097/QAD.0000000000001252
6. Sotgiu G, Centis R, D'ambrosio L, De Lorenzo S, D'Arcy Richardson M, Lange C, et al. Development of a standardized tool to survey MDR-/XDR-TB case management in Europe. Eur Resp J. (2010) 36:208–11. doi: 10.1183/09031936.00186409
7. Migliori GB, Sotgiu G, Blasi F, Zumla A, Loddenkemper R, Raviglione MC, et al. Towards the development of EU/EEA Standards for Tuberculosis Care (ESTC). Eur Respir J. (2011) 38:493–5. doi: 10.1183/09031936.00094211
8. Migliori GB1, Zellweger JP, Abubakar I, Ibraim E, Caminero JA, De Vries G, et al. European union standards for tuberculosis care. Eur Respir J. (2012) 39:807–19. doi: 10.1183/09031936.00203811
9. van der Werf MJ, Sandgren A, D'Ambrosio L, Blasi F, Migliori GB. The European Union standards for tuberculosis care: do they need an update? Eur Respir J. (2014) 43:933–42. doi: 10.1183/09031936.00216613
10. Lonnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de Vries G, Diel R. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J. (2015) 45:928–52. doi: 10.1183/09031936.00214014
11. Migliori GB, Sotgiu G, Rosales-Klintz S, Centis R, D'Ambrosio L, Abubakar I, et al. ERS/ECDC Statement: European Union standards for tuberculosis care, 2017 update. Eur Respir J. (2018) 51:1702678 doi: 10.1183/13993003.02678-2017
12. Lewinsohn DM, Leonard MK, LoBue PA, Cohn DL, Daley CL, Desmond E, et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: diagnosis of tuberculosis in adults and children. Clin Infect Dis. (2017) 64:e1–e33. doi: 10.1093/cid/ciw694
13. Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, et al. Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: treatment of drug-susceptible tuberculosis. Clin Infect Dis. (2016) 63:e147–e95. doi: 10.1093/cid/ciw376
15. World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care, 2017 Update. Geneva: World Health Organization (2017).
16. Recommendations Nationales. Prévention de la Transmission Croisée par Voie Respiratoire Air ou Gouttelettes. Vol. 20. Société Française d'Hygiène Hospitalière (SF2H) (2013).
17. World Health Organization Regional Office for Europe. Algorithm for Laboratory Diagnosis and Treatment-Monitoring of Pulmonary Tuberculosis and Drug-Resistant Tuberculosis Using state-of-the-Art Rapid Molecular Diagnostic Technologies. Expert opinion of the European Tuberculosis Laboratory Initiative core group members for the WHO European Region. Copenhagen, WHO Regional Office for Europe (2017).
18. Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep. (2005) 54:1–141.
19. European Centre for Disease Prevention and Control. Handbook on TB Laboratory Diagnostic Methods for the European Union. Stockholm, ECDC (2016).
20. Datta S, Shah L, Gilman RH, Evans CA. Comparison of sputum collection methods for tuberculosis diagnosis: a systematic review and pairwise and network meta-analysis. Lancet Glob Health. (2017) 5:e760–e71. doi: 10.1016/S2214-109X(17)30201-2
21. Schoch OD, Rieder P, Tueller C, Alpeter E, Zellweger JP, Rieder HL. Diagnostic yield of sputum, induced sputum, and bronchoscopy after radiologic tuberculosis screening. Am J Respir Crit Care Med. (2007) 175:80–6. doi: 10.1164/rccm.200608-1092OC
22. Boehme CC, Nabeta P, Hillemann D, Nicol MP, Shenai S, Krapp F, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. (2010) 363:1005–15. doi: 10.1056/NEJMoa0907847
23. Nathavitharana RR, Cudahy PG, Schumacher SG, Steingart KR, Pai M, Denkinger CM. Accuracy of line probe assays for the diagnosis of pulmonary and multidrug-resistant tuberculosis: a systematic review and meta-analysis. Eur Respir J. (2017) 49:1601075. doi: 10.1183/13993003.01075-2016
24. Pankhurst LJ, Del Ojo Elias C, Votintseva AA, Walker TM, Cole K, Davies J, et al. Rapid, comprehensive, and affordable mycobacterial diagnosis with whole-genome sequencing: a prospective study. Lancet Respir Med. (2016) 4:49–58. doi: 10.1016/S2213-2600(15)00466-X
25. Walker TM, Cruz ALG, Peto TE, Smith EG, Esmail H, Crook DW, et al. Tuberculosis is changing. Lancet Infect Dis. (2017) 17:359–61. doi: 10.1016/S1473-3099(17)30123-8
26. Cao D, Zhang Z, Yang Z, Ma S, Sun Z, Duan H, et al. The association between tuberculin test and active tuberculosis risk of college students in Beijing, China: a retrospective cohort study. BMC Infect Dis. (2019) 19:619. doi: 10.1186/s12879-019-4238-2
27. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J, et al. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. (2007) 4:e238. doi: 10.1371/journal.pmed.0040238
28. Volmink J, Matchaba P, Garner P. Directly observed therapy and treatment adherence. Lancet. (2000) 355:1345–50. doi: 10.1016/S0140-6736(00)02124-3
Keywords: tuberculosis, survey, Europe, guidelines, harmonization, diagnosis, treatment
Citation: Méchaï F, Cordel H, Guglielmetti L, Aubry A, Jankovic M, Viveiros M, Santin M, Goletti D and Cambau E (2020) Management of Tuberculosis: Are the Practices Homogeneous in High-Income Countries? Front. Public Health 8:443. doi: 10.3389/fpubh.2020.00443
Received: 12 November 2019; Accepted: 20 July 2020;
Published: 04 September 2020.
Edited by:
Vitali Sintchenko, The University of Sydney, AustraliaReviewed by:
Florence Doucet-populaire, Université Paris-Sud, FranceCopyright © 2020 Méchaï, Cordel, Guglielmetti, Aubry, Jankovic, Viveiros, Santin, Goletti and Cambau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frédéric Méchaï, ZnJlZGVyaWMubWVjaGFpQGFwaHAuZnI=
†ESCMID (European society on clinical microbiology and infectious diseases) study group on mycobacterial infections
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.