 Sarah L. Mullane
Sarah L. Mullane Douglas Connolly2
Douglas Connolly2 Matthew P. Buman
Matthew P. Buman- 1School of Nutrition and Health Promotion, Arizona State University, Phoenix, AZ, United States
- 2Stewart Transport, Phoenix, AZ, United States
Purpose: To conduct rapid qualitative analysis early in the intervention design process to establish the perceived value of reducing sedentary behavior in the truck driver population.
Methods: A rapid assessment process for qualitative data collection was used to examine managerial and employee perceptions quickly and iteratively to inform intervention design. Managerial insights were collected during semi-structured interviews and employee insights were collected via an online survey and focus group. Thematic analyses were guided by the constructs of the Health Belief Model to establish; (a) perceived susceptibility to the health problem; (b) perceived severity of the health problem; (c) perceived benefits of the potential solutions; (d) perceived barriers to adopting the recommended solution; (e) cues to action; and (f) self-efficacy.
Results: Three managers (2 females; 1 male) participated in semi-structured interviews. Seven truck drivers (1 female; 6 males) took part in a focus group. Sixteen survey responses (all male, mean age 49.8 ± 12.4 years, 86% white Caucasian) were collected in total (11 paper based; 6 online). The most important managerial motivators for engagement in an intervention included; improved sleep, alertness and quality of life. The most important employee motivators included; stress reduction (3.3 ± 1.3), improved quality of life (3.3 ± 1.3) and alertness (3.2 ± 1.4). Managerial and employee perspectives indicated that sedentary behavior may be of lower priority than diet and exercise, and may not resonate with the truck driving population as a health risk.
Conclusion: Application of the Health Belief Model indicated a disconnect between the researcher, managerial and employee perspective and the perceived value of a sedentary behavior reduction intervention. Within the truck driving population, researchers should endeavor to include safety as well as health outcomes, use multi-level strategies, design for outcomes of high perceived value and leverage health communication strategies to communicate benefits that resonate with the end-user.
Introduction
Truck drivers are classified as one of the highest-risk occupational segments due to a complex interplay of health behavior barriers across the socioecological spectrum (1). In the commercial driving population, rates of obesity have been reported to be as high as 50%, while the prevalence of diabetes is 50% higher than the general population (2). Contributory factors include occupational influences on diet, exercise, sleep and more recently sedentary behaviors (1). Detrimental associations have been observed between prolonged sedentary time [any waking behavior in a seated or reclining posture with low energy expenditure (<1.5 metabolic equivalents [METS])] (3) and BMI (4), waist circumference and 2-hr plasma glucose (5). Bouts of standing (6–8), light-intensity physical activity (LPA) (7, 9–11) or non-exercise activity thermogenesis (NEAT) (12) may attenuate these effects. Despite a recent shift toward environmental changes (sit-stand/active workstations) in office-based work environment (13–15), further challenges exist in non-office environments where prolonged sitting is prevalent (e.g., occupational driver settings). Existing environmental, cultural and social solutions for sedentary office workers do not translate to this challenging setting and evidence on how to intervene is extremely limited (16).
Health promotion efforts within the truck driving population have primarily focused on exercise and/or diet based interventions (17). However, low engagement or high attrition rates are typically reported, which has led to concerns regarding sustainability and impact (18). Lack of engagement may be further amplified when targeting sedentary behavior reduction for two reasons. Firstly, the basic premise in ecological models of health behavior is that efforts to change individuals' behavior cannot be effective if environments make it difficult (19). As standing and moving is not conducive to occupational driving, it is likely the barriers are even higher than those associated with diet and exercise interventions. Secondly, health-related risk perceptions play an important role in motivating health behavior change (20). Although individual level factors such as family history may influence perceived susceptibility to disease, risk perceptions are often influenced by the frequency with which a threat is represented in media exposure (21). As an emerging health risk factor, which may not have substantive evidence and/or consistent media exposure, sedentary behavior may not be considered to be a “real” or high priority risk factor within the trucking population.
The Health Belief Model is a Cognitive Value-Expectancy Theory which emphasizes the perceived value of the outcome, and the subjective expectation that a behavior will result in the outcome (22). A person must feel personally susceptible to a disease with serious or severe consequences and must believe that the benefits of taking the preventive action outweigh the perceived barriers to (and/or costs of) preventive action, in order to adopt a recommended preventive health action. Personal values must be considered along with factual evidence of treatment efficacy in order to facilitate health promotion “by the person.” Determining how to intervene is contingent on the perceived susceptibility and perceived value of an intervention.
In an effort to address the disparate health risks of the truck driver population and to inform the development of interventions specifically targeting sedentary behavior, we seek to understand the perception of sedentary behavior in the truck driving population. The purpose of this research within the truck driving community was to examine the perceptions of sitting as a health risk factor. We have used the Health Belief Model as a guiding framework, including the barriers, motivators, the perceived value of and receptivity to potential health interventions, that may target sedentary behavior in the truck driving population.
Methods
A rapid assessment process for qualitative data collection was used to develop a preliminary understanding of a situation from the insider's perspective quickly and iteratively to inform intervention design (23). Using a mixed-methods approach, formative research was conducted with a local Phoenix based truck company to retrospectively examine attitudes toward sedentary behaviors at work and the perceived opportunity for intervention (including barriers and motivators). An in-person, semi-structured interview (which allowed for expansion) was conducted by SM with managers of the trucking company to gather managerial insights. Employee insights were collected during an onsite visit to a driver training day which facilitated a focus group with active truck drivers. Due to the rapid assessment process and early stage of the partnership, detailed notes (rather than audio) were recorded (23). Finally, further employee insights were collected via a survey which could be completed online (via Qualtrics) or using a paper based version that was distributed in-person to truck drivers as they visited the headquarters. All responses were de-identified as soon as the response was recorded and a $10 gift card incentive delivered to each participant. In addition to demographic information, respondents were asked a series of 5-point Likert scale questions (not at all [1] to extremely [5]) to rate; (a) the likelihood of engaging in behaviors to reduce sitting; (b) the motivators for participating in an intervention to reduce sitting; and (c) the perceived value of supporting tools or mechanisms to increase engagement. This study was approved by the Arizona State University Institutional Review Board. All participants consented using an online or paper based consent form.
Analyses
A thematic analysis of the key requirements and points raised during the semi-structured interviews and focus group was conducted. All closed survey question responses were imported and analyzed using SAS Enterprise Guide 7.1. All open ended questions were reviewed individually and word repetition used to identify the most prominent barriers and motivators (24). Findings were summarized using the constructs of the Health Belief Model (22) which included; (a) perceived susceptibility to the health problem; (b) perceived severity of the health problem; (c) perceived benefits of the potential solutions; (d) perceived barriers to adopting the recommended solution; (e) cues to action; and (f) self-efficacy.
Results
Three managers (2 females; 1 male) participated in semi-structured interviews. Seven truck drivers (1 female; 6 males) attended the driver training day and took part in a focus group. Sixteen survey responses were collected in total (11 paper based; 6 online), five of which were responses from those who also participated in the focus group. Of those that completed the survey, all were male, mean age 49.8 ± 12.4years and 86% white Caucasian. All survey and semi-structured interview findings are summarized in Table 1. Specific survey results pertaining to motivators for engagement, the likelihood of engaging in preventative behaviors and receptivity to suggested health solutions are presented in Figures 1–3, respectively.
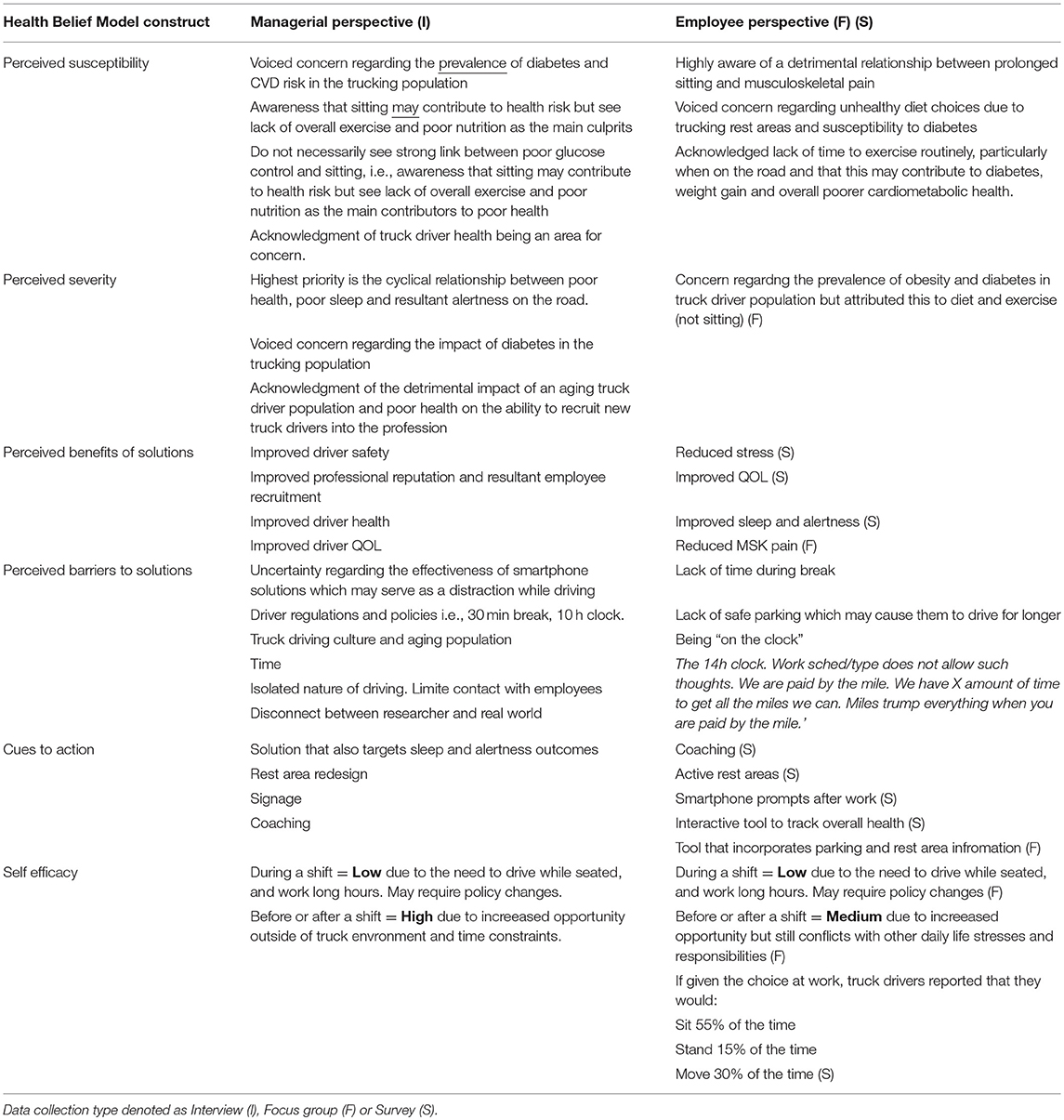
Table 1. Managerial and employee perspectives categorized by the Health Belief Model constructs.
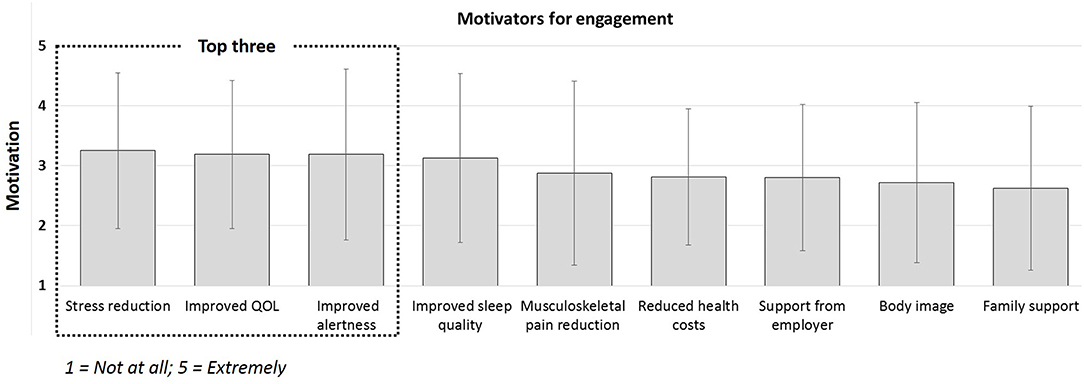
Figure 1. Employee motivators for engaging in preventative behaviors to reduce sedentary behavior (not at all [1] to extremely [5]).
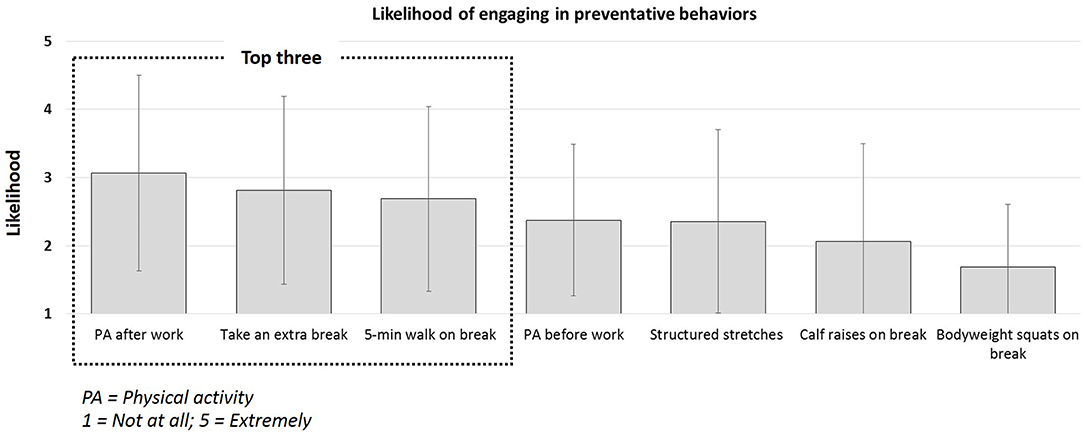
Figure 2. Employee likelihood of engaging in preventative behaviors to reduce sedentary behavior (not at all [1] to extremely likely [5]).
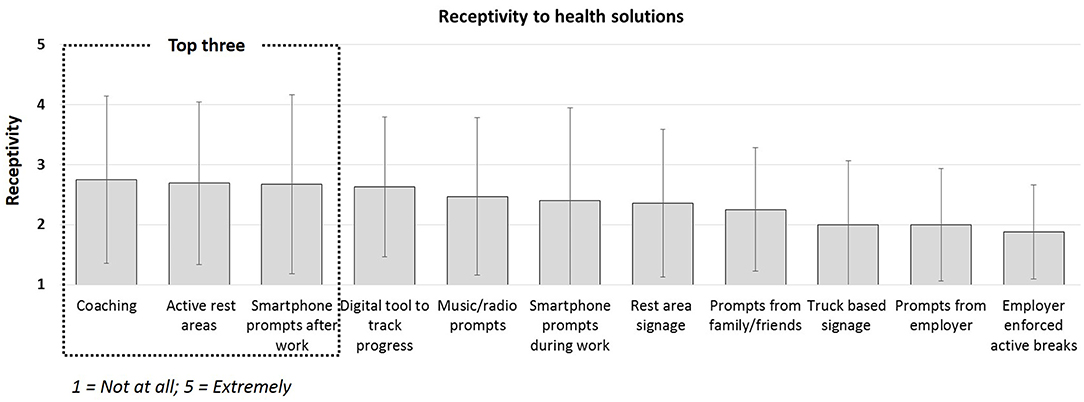
Figure 3. Employee receptivity to sedentary behavior reduction intervention components (not at all [1] to extremely [5]).
Manager Perspective
The results presented in Table 1 (employer perspective) indicated that managers acknowledged high susceptibility to diabetes and overall increased cardiovascular disease (CVD) risk in the truck driver population compared to the general population. However, they did not necessarily attribute this risk to prolonged sitting but instead a combination of poor diet and lack of exercise due to being “on the road.” Perceived severity was considered high due to their concern regarding the cyclical relationship between poor health, poor sleep and alertness and potential impact on driver safety. Perceived benefits were consistently related to driver safety by potentially improving sleep, alertness, well-being and quality of life. A notable managerial perceived benefit included the ability to change the public perception of the profession as being detrimental to health, which may facilitate future recruitment efforts. Perceived barriers included the potential for driver distraction that may arise via digital solutions and existing policies which dictated work breaks and time on the road. Additional concerns were raised regarding the isolated nature of driving and being able to distribute change across the organization with limited group based contact. Finally, concerns were also raised regarding the disconnect between research and the real world and the extent to which the driving culture may override researcher efforts.
Managerial cues to action included an intervention designed to monitor sleep and alertness, in addition to glucose control. Rest area redesign, signage and coaching were identified as being desirable components of the health solution. Digital solutions were only deemed appealing if they targeted rest areas, breaks and out of work hours (i.e., not while driving). Overall perceived self-efficacy of being able to reduce prolonged sitting and increase levels of activity during the work day was low given the nature of the job. However, targeting outside work hours was considered much more feasible.
Employee Perspective
The results presented in Table 1 (employee perspective) indicate that employees voiced stronger susceptibility concerns regarding the detrimental effects of sitting but as a contributing factor to musculoskeletal pain rather than diabetes. Similar to managers, they attributed diabetes and CVD risk to poor diet choices and lack of exercise “on the road.” Although truck drivers recognized the prevalence of diabetes and CVD risk in their profession, perceived severity was lower than the manager perspective. More emphasis was placed on the severity and detrimental effects of stress on the truck driver population. Perceived benefits derived from the survey responses (see Figure 1) indicated that stress reduction (3.3 ± 1.3) was the most important motivator and benefit of engagement. Additionally, improved quality of life (3.3 ± 1.3), alertness (3.2 ± 1.4), sleep (3.1 ± 1.4) and pain reduction (2.8 ± 1.5) were considered important motivators. The least important motivator was identified as family support (2.6 ± 1.4). Perceived barriers were similar to those voiced by the managers with an additional concern regarding the availability of safe parking areas which, in some cases, causes drivers to drive for longer than planned. Lack of time to engage in any health solution was consistently identified in both group discussion and survey responses as a significant barrier.
Cues to action identified from survey responses (see Figure 2) indicated that participants were most receptive to engaging in physical activity after work (3.1 ± 1.4) but least likely to engage in bodyweight squats during a break to reduce sedentary behavior (1.7 ± 0.8). The survey responses presented in Figure 3, indicated that participants were most receptive to the idea of health coaching (2.8 ± 1.4), active rest areas (2.7 ± 1.4) and smartphone prompts after work (2.7 ± 1.5). They were least receptive to employer enforced active breaks (1.9 ± 0.8). Finally, employees reported that if they were given the opportunity, they would prefer to sit (54.6 ± 38.9%), stand (15.4 ± 23.6%) and move (30.0 ± 31.4%) of the time during their working day. However, the perceived ability to do so was low during the work day, and slightly higher outside of work hours.
Discussion
Efforts to promote health are likely to be ineffective if they ignore what a person values, which influences the appraisal of the risk-benefit ratio for different treatments or lifestyle practices (25). Application of the Health Belief Model indicated that there was a disconnect between the perceived value of an intervention designed to reduce sedentary behavior between the researcher, managerial and employee perspective. Based on these findings, pertinent insights that may increase perceived value and future engagement in truck driving health interventions are outlined below.
Leveraging Safety as Well as Health
Our results support existing evidence advocating for health interventions in the trucking population that integrate occupational safety with health promotion (26). Initially, managerial hesitancy toward a digital intervention was apparent due to possible driver distraction. However, this hesitancy was reduced when considering the possibility of targeting sleep and alertness outcomes, for which the perceived value was high. Accumulating evidence suggests that obesity (27) and insulin resistance (28) may play a significant role in the pathogenesis of excessive daytime sleepiness (EDS) which is associated with “drowsy driving” and may result in 1,500 road deaths and 40,000 injuries annually (27, 29). Interestingly, research has also indicated that intermittent bouts of LPA have been linked to increased alertness (30, 31). Leveraging this evidence and incorporating it into a multi-component intervention may increase the perceived value within the trucking driving community. To increase perceived value from all parties, future interventions should consider additional measures of sleep and alertness (in addition to activity levels and glycemic control).
Social Ecological Determinants of Health
Both employers and employees voiced concern regarding factors outside their control- hours of service laws and parking availability at either rest areas or truck stops which dampened any efforts to engage in health interventions. These results support the notion that determinants of health extend beyond individual lifestyle and health services factors, with social, economic, organizational, environmental, and cultural factors all determinants in health (17). Ecological domains, such as governmental, corporate, organizational, community, and built-environment factors, can support or inhibit opportunities and resources available for physical and recreational activities (32, 33). Alternatively, both managers and employees expressed increased perceived value in efforts to promote active rest areas. This is in support of previous research which identified highway rest areas as the highest scoring active living setting for the truck driver population (35.3%) compared to warehouses which were identified as the lowest scoring (11.6%). We recommend that researchers engage multiple stakeholders representing key user personas early in the design process. This may help identify motivators and barriers at the individual, social, cultural and organizational level, and facilitate translation into real world settings.
The Importance of the End-User
Emerging theories suggest that lack of user involvement early in the intervention design process has been identified as one of the major contemporary difficulties encountered during intervention implementation (34). While it is important to acknowledge the high perceived value of safety from the managerial perspective as a motivator to facilitate health intervention for employees, it is important to not lose sight of those who will ultimately participate- i.e., truck drivers. Stress reduction and improved quality of life were perceived as the greater motivators and may therefore be a key component for engagement. We recommend that researchers be creative in the design of an intervention to incorporate higher priority factors as perceived by the end-user, rather than focusing on the researcher and/or stakeholder primary aim alone, e.g., improved glycemic control or alertness.
Applying Health Communication Theory
In addition to designing for the end-user, researchers may need to incorporate Health Communication theory to better communicate benefits that resonate with the target population (35). The power of effective communication and “framing,” or conversely, the impact of miscommunication, is reflected in our results. Conflicting priorities are evident between the likelihood of engagement in behaviors (Figure 2) and receptivity to potential health solutions (Figure 3). Although “taking an extra break” was identified by employees as the second most likely behavior they would engage in to reduce sedentary behavior, “employer enforced active breaks” was the least preferred health solution. The terminology “enforced” eludes to having less control over the working day and although it would indeed reduce sedentary behavior, the negative perception of less control from the employee perspective may impact employee morale, cause more stress and reduce quality of life. We posit that redefining this option as “support from employer to take an active break,” may have elicited a more favorable result. Researchers should be encouraged to consider the unintended consequences of health solutions and health communication, which although may align with researchers and stakeholder goals, may detrimentally impact the end-user perception (36).
Measures and Method of Data Collection
Truck driving is reported as a primarily isolated profession that does not require regular group based contact with work colleagues (17). Therefore, the employer has intermittent contact with each employee. Only ~32% of the surveys were completed online, the rest were completed on paper. Email communication is not required for the job and thus, the employer does not have an email address for all employees. This reduces the opportunity for interaction with employees and may impact both recruitment and assessment strategies for future trials. Only by gaining trust and through support from the employer were we able to collect a small number of survey responses. The difficulty experienced during recruitment, is reflective of the challenges faced in previous studies reporting low engagement or high attrition (1, 17), and further highlights the need to incorporate our recommendations to; include safety as well as health outcomes, use multi-level strategies, design for outcomes of greater perceived value and communicate the benefits that resonate with the end-user.
Limitations
We acknowledge that these insights are not generalizable given the small sample size. Similarly, formative research was not audio recorded and there was little variation across the receptivity and motivators for engagement results. However, using rapid assessment processes, we obtained early user feedback quickly and cost-effectively, that may significantly impact intervention design. Too often, researchers do not provide enough insight regarding user research and resultant design decision-making process that may help to inform future research. This is supported by Yeager et al. (37), who recently proposed a framework for “Design Thinking for Psychosocial Interventions” defining different “lenses” to incorporate users i.e., participants, communities, stakeholders etc., early in the intervention design process to avoid easily discoverable flaws that impede real world application (37). Such novel insights are also shared by Community-Based Participatory Research (CBPR)-which aims to unite health professionals, academics, and communities in giving underserved communities a genuine voice in research to increase the likelihood of an intervention's success (38). An important facet of CBPR is the identification of “gate keepers” within the community- without their support and collaboration, an intervention is likely to fail regardless of community demand (38). Our formative research has nurtured relationships and fostered negotiation to provide a more sustainable partnership that can support real world application.
Conclusions
Truck drivers are exposed to prolonged sitting and rest areas are not perceived as “healthy” environments, and the associations between, obesity and insulin resistance could be fatal. However, the disconnect between what a researcher may perceive as a valuable intervention may not be reflected in the target population. Establishing perceived value is critical to health solution dissemination and true health impact and may require some negotiation in order to gain “buy-in” (not necessarily consensus) from all parties involved. Identifying motivators to participation may impact the intervention measures and communication of the study and should be considered when designing within the community. Such findings can be elicited quickly, cost-effectively and early in the design process using rapid assessment processes to collect and analyze qualitative data. Our findings indicated that while prolonged sitting may be considered a major topic within research, it is yet to resonate with the truck driving population as a “health risk.” Although a researcher may endeavor to target a specific behavior, if the value of the perceived intervention is not high enough, it is unlikely that the participant will continue to engage in the preventative behavior. The ability to design sustainable interventions is crucial to public health impact and must be aligned with perceived value of the intervention. There is continued need for user feedback from truck drivers and associated stakeholders to understand the perception of sedentary behavior and potential receptivity to reducing it, to improve the level of engagement and resultant effectiveness of future trials.
Ethics Statement
This study was approved by the Arizona State University Institutional Review Board and all participants consented using an online or paper based consent form.
Author Contributions
SM was responsible for the concept and design of the study. SM and DC were primarily responsible for data collection. SM performed data analysis and interpreted the data. SM wrote the initial draft of the manuscript. SM, MB, and DC reviewed and edited the manuscript, and approved the final version prior to submission. All authors reviewed and approved the final manuscript as submitted.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Stewart Transport, Phoenix AZ, USA, for their support and cooperation throughout this study.
References
1. Apostolopoulos Y, Shattell MM, Sönmez S, Strack R, Haldeman L, Jones V. Active living in the trucking sector: Environmental barriers and health promotion strategies. J Phys Activ Health. (2012) 9:259–69. doi: 10.1123/jpah.9.2.259
2. Sieber WK, Robinson CF, Birdsey J, Chen GX, Hitchcock EM, Lincoln JE, et al. Obesity and other risk factors: The national survey of US Long-Haul truck driver health and injury. Am J Indus Med. (2014) 57:615–26. doi: 10.1002/ajim.22293
3. Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours.” Appl Physiol Nutr Metab. (2012) 37:540–2. doi: 10.1139/h2012-024
4. Henson J, Edwardson CL, Morgan B, Horsfield MA, Bodicoat DH, Biddle S., et al. Associations of sedentary time with fat distribution in a high-risk population. Med Sci Sports Exerc. (2014) 47:1727–34. doi: 10.1249/MSS.0000000000000572
5. Healy GN, Wijndaele K, Dunstan DW, Shaw JE, Salmon J, Zimmet PZ, et al. Objectively measured sedentary time, physical activity, and metabolic risk: the australian diabetes, obesity and lifestyle study (AusDiab). Diabetes Care. (2008) 31:369–71. doi: 10.2337/dc07-1795
6. Buckley JP, Mellor DD, Morris M, Joseph F. Standing-based office work shows encouraging signs of attenuating post-prandial glycaemic excursion. Occup Environ Med. (2014) 71:109–11. doi: 10.1136/oemed-2013-101823
7. Crespo NC, Mullane SL, Zeigler ZS, Buman MP, Gaesser GA. Effects of standing and light-intensity walking and cycling on 24-h glucose. Med Sci Sports Exerc. (2016) 48:2503–11. doi: 10.1249/MSS.0000000000001062
8. Thorp AA, Healy GN, Winkler E, Clark BK, Gardiner PA, Owen N, et al. Prolonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Activ. (2012) 9:128. doi: 10.1186/1479-5868-9-128
9. Bailey DP, Locke CD. Breaking up prolonged sitting with light-intensity walking improves postprandial glycemia, but breaking up sitting with standing does not. J Sci Med Sport. (2015) 18:294–8. doi: 10.1016/j.jsams.2014.03.008
10. Dunstan DW, Kingwell BA, Larsen R, Healy GN, Cerin E, Hamilton MT, et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. (2012) 35:976–83. doi: 10.2337/dc11-1931
11. Zeigler ZS, Mullane S, Crespo NC, Buman MP, Gaesser GA. Effects of standing and light-intensity activity on ambulatory blood pressure. Med Sci Sports Exerc. (2015) 48:175–81. doi: 10.1249/MSS.0000000000000754
12. Levine JA. Non-exercise activity thermogenesis (NEAT). Nutr Rev. (2004) 62:S82–97. doi: 10.1301/nr.2004.jul.S82-S97
13. Buman MP, Mullane SL, Toledo MJ, Rydell SA, Gaesser GA, Crespo NC, et al. An intervention to reduce sitting and increase light-intensity physical activity at work: design and rationale of the ‘Stand & move at work'group randomized trial. Contemp Clin Trials. (2016) 53:11–9. doi: 10.1016/j.cct.2016.12.008
14. Danquah IH, Kloster S, Holtermann A, Aadahl M, Bauman A, Ersboll AK, et al. Take a stand!-a multi-component intervention aimed at reducing sitting time among office workers-a cluster randomized trial. Int J Epidemiol. (2016) 46:128–40. doi: 10.1093/ije/dyw009
15. Healy GN, Eakin EG, Owen N, LaMontagne AD, Moodie M, Winkler EA, et al. A cluster RCT to reduce office workers' sitting time: impact on activity outcomes. Med Sci Sports Exerc. (2016) 48:1787–97. doi: 10.1249/MSS.0000000000001328
16. Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: The population health science of sedentary behavior. Exerc Sport Sci Rev. (2010) 38:105–13. doi: 10.1097/JES.0b013e3181e373a2
17. Lemke MK, Meissen GJ, Apostolopoulos Y. Overcoming barriers in unhealthy settings: a phenomenological study of healthy truck drivers. Global Qual Nurs Res. (2016) 3:2333393616637023. doi: 10.1177/2333393616637023
18. Greenfield R, Busink E, Wong CP, Riboli-Sasco E, Greenfield G, Majeed A, et al. Truck drivers' perceptions on wearable devices and health promotion: a qualitative study. BMC Public Health. (2016) 16:677. doi: 10.1186/s12889-016-3323-3
19. Sallis JF, Owen N, Fisher E. Ecological models of health behavior. Health Behav Theor Res Pract. (2015) 5:43–64.
20. Sheeran P, Harris PR, Epton T. Does heightening risk appraisals change people's intentions and behavior? A meta-analysis of experimental studies. Psychol Bull. (2014) 140:511. doi: 10.1037/a0033065
22. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. (1984) 11:1–47. doi: 10.1177/109019818401100101
24. Ryan GW, Bernard HR. Techniques to identify themes. Field Methods. (2003) 15:85–109. doi: 10.1177/1525822X02239569
25. Fulford K. Bringing together values-based and evidence-based medicine: UK department of health initiatives in the ‘Personalization’ of care. J Eval Clin Pract. (2011) 17:341–3. doi: 10.1111/j.1365-2753.2010.01578.x
26. Sorensen G, Barbeau EM. Integrating occupational health, safety and worksite health promotion: opportunities for research and practice. La Med Del Lavor. (2006) 97:240–57.
27. Anderson JE, Govada M, Steffen TK, Thorne CP, Varvarigou V, Kales SN, et al. Obesity is associated with the future risk of heavy truck crashes among newly recruited commercial drivers. Accid Anal Prev. (2012) 49:378–84. doi: 10.1016/j.aap.2012.02.018
28. Bixler E, Vgontzas A, Lin H, Calhoun S, Vela-Bueno A, Kales A. Excessive daytime sleepiness in a general population sample: the role of sleep apnea, age, obesity, diabetes, and depression. J Clin Endocrinol Metabol. (2005) 90:4510–5. doi: 10.1210/jc.2005-0035
29. Vgontzas AN. Does obesity play a major role in the pathogenesis of sleep apnoea and its associated manifestations via inflammation, visceral adiposity, and insulin resistance? Archiv Physiol Biochem. (2008) 114:211–23. doi: 10.1080/13813450802364627
30. Chang Y, Labban J, Gapin J, Etnier J. The effects of acute exercise on cognitive performance: a meta-analysis. Brain Res. (2012) 1453:87–101. doi: 10.1016/j.brainres.2012.02.068
31. Mullane SL, Buman MP, Zeigler ZS, Crespo NC, Gaesser GA. Acute effects on cognitive performance following bouts of standing and light-intensity physical activity in a simulated workplace environment. J Sci Med Sport. (2016) 20:489–93. doi: 10.1016/j.jsams.2016.09.015
32. Ball K, Timperio AF, Crawford DA. Understanding environmental influences on nutrition and physical activity behaviors: Where should we look and what should we count? International J Behav Nutr Phys Activ. (2006) 3:33. doi: 10.1186/1479-5868-3-33
33. French SA, Harnack LJ, Toomey TL, Hannan PJ. Association between body weight, physical activity and food choices among metropolitan transit workers. Int J Behav Nutr Phys Activ. (2007) 4:52. doi: 10.1186/1479-5868-4-52
34. Lyon AR, Koerner K. User-Centered design for psychosocial intervention development and implementation. Clin Psychol Sci Pract. (2016) 23:180–200. doi: 10.1111/cpsp.12154
35. Rimal RN, Lapinski MK. Why health communication is important in public health. Bull World Health Organ. (2009) 87:247. doi: 10.2471/BLT.08.056713
36. Cho H, Salmon CT. Unintended effects of health communication campaigns. J Commun. (2007) 57:293–317. doi: 10.1111/j.1460-2466.2007.00344.x
37. Yeager DS, Romero C, Paunesku D, Hulleman CS, Schneider B, Hinojosa C, et al. Using design thinking to improve psychological interventions: The case of the growth mindset during the transition to high school. J Edu Psychol. (2016) 108:374. doi: 10.1037/edu0000098
Keywords: truck drivers, sedentary behavior, perceived value, Health Belief Model, engagement
Citation: Mullane SL, Connolly D and Buman MP (2019) The Perceived Value of Reducing Sedentary Behavior in the Truck Driving Population. Front. Public Health 7:214. doi: 10.3389/fpubh.2019.00214
Received: 27 May 2018; Accepted: 18 July 2019;
Published: 07 August 2019.
Edited by:
Yolande Esquirol, INSERM U1027 Epidémiologie et analyses en santé publique: Risques, Maladies Chroniques et Handicap, FranceReviewed by:
Melanie M. Adams, Keene State College, United StatesYuke Tien Fong, Singapore General Hospital, Singapore
Copyright © 2019 Mullane, Connolly and Buman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah L. Mullane, c2xtdWxsYW5AYXN1LmVkdQ==