 DeAnn Liska1*
DeAnn Liska1* Eunice Mah
Eunice Mah- 1Biofortis, Mérieux NutriSciences, Addison, IL, United States
- 2Michael Kelley Nutrition Consulting, Chicago, IL, United States
Background: The objective of this systematic review was to assess the scope and breadth of publicly available prospective cohort and randomized controlled trial (RCT) literature on 100% fruit juice and dental caries or tooth erosion in humans.
Methods: We performed a systematic search in MEDLINE/PubMed, EMBASE, and Web of Science for studies published from inception through May 2018, and the Cochrane Library databases for reports published through January 2018. Prospective cohort studies or RCTs conducted on dental health and 100% fruit juice, and published in English were selected. No restrictions were set for age, sex, geographic location, or socioeconomic status.
Results: Eight publications representing five independent prospective cohort studies and nine publications on nine RCTs were included. All prospective cohort studies were in children or adolescents, and all RCTs were in adults. Prospective cohort studies on tooth erosion found no association between juice intake and tooth erosion, while those on dental caries incidence reported either no association or an inverse association between 100% fruit juice intakes and dental caries incidence. RCTs on tooth erosion showed decreased microhardness, increased surface enamel loss, increased erosion depth, greater enamel softening, and/or increased pellicle layer with 100% fruit juice, and those on dental caries showed increased demineralization of enamel slabs with 100% fruit juice.
Conclusions: The existing evidence on 100% fruit juice intake and caries and tooth erosion are not conclusive. Overall, prospective cohort studies in children and adolescents found no association between 100% fruit juice intake and tooth erosion or dental caries, but, RCT data in adults suggests that 100% fruit juice could contribute to tooth erosion and dental caries. The RCT data, however, were from small, short-term studies that utilized intra-oral devices generally devoid of normal plaque or saliva action, and generally employed conditions that are not reflective of normal juice consumption.
Introduction
In the United States, dental caries and tooth erosion affect 19 and 30% of school-going children, respectively (1, 2) while 32% of adults have untreated dental caries (1). Dental caries and tooth erosion have been indicated as the outcomes most related to food intake and dietary practices and have, therefore, been assessed by many authoritative organizations as part of dietary recommendations, primarily with respect to sugar (3, 4). For example, the 2015 Dietary Guidelines for Americans included dental caries as one of the chronic health conditions assessed with respect to added sugars (5). The committee relied on a review of sugars and dental caries conducted for the World Health Organization (WHO) (6, 7), which combined data on total, free, added, and non-milk extrinsic sugars (8). Likewise, the Scientific Advisory Committee on Nutrition (SACN) in the United Kingdom has also included oral health as a primary outcome in its scientific report on carbohydrates and health (9), and included all sources of sugars and polysaccharides, such as polyols, sugar-added beverages, and fruit and fruit juices in its assessment.
Dental caries refers to damage to the hard surfaces of teeth. The dental caries process is complex and many factors play a role in the risk and prevalence of caries in a population. In general, the etiology of dental caries involves three main factors: (1) presence of cariogenic microorganisms, (2) exposure to fermentable substrates (e.g., carbohydrates), and (3) a susceptible tooth surface/host (10). Cariogenic bacteria produce organic acids from fermentable substrates, mainly sugars and starches, and these acids can damage enamel through demineralization to cause the loss of enamel. Because sugars and starches are commonly found within the foods and beverages of many societies, the risk of developing dental caries extends to nearly all individuals. In the absence of fermentable substrates, the pH within dental plaque is close to neutral. Saliva contains calcium, phosphorus, and bicarbonate and the calcium and phosphorus can contribute to the hydroxyapatite structure of enamel, while the bicarbonate functions to return and maintain plaque pH above 5.7. Remineralization of enamel can occur following transient demineralization, and thus, remineralization and demineralization are in a dynamic balance with the progression of caries occurring when the effects of demineralization predominate. A number of factors can modify caries risk, including eating behavior, socioeconomic status, birth weight, genetics, and age (10).
Tooth wear is also a concern, as it increases the risk of caries and other dental health issues. Tooth wear increases with age and is also influenced by modifiable factors, most notably diet (9, 11, 12). Three types of tooth wear are recognized: abrasion, attrition, and erosion. Abrasion and attrition occur from physical forces, whereas erosion occurs from demineralization. Tooth erosion is defined as the progressive, irreversible loss of dental hard tissues by a chemical process without bacterial involvement. Erosion is differentiated from demineralization associated with caries as it is caused by exogenous acid, most commonly from foods or beverages. The process of demineralization is the same as described for caries, but the acid supplied by foods or beverages affects a much larger surface area of enamel, while the acid effects in the caries process are localized where the plaque exists. Thus, dental erosion is often found in areas that are plaque-free, whereas dental caries are in sites of plaque accumulation.
As mentioned earlier, dental health, particularly caries, have been included as an outcome related to intakes of sugar-containing foods and beverages. Much of the concern has focused on the content of either naturally occurring free sugars or added sugars. However, foods fitting this category are heterogeneous. In particular, 100% fruit and vegetable juices, as well as whole fruits and vegetables, at times have been included in this category. For example, the majority of reports used for policy assessment have combined data from sugar-sweetened beverages, fruit drinks, whole fruits, desserts, confectioneries, and 100% fruit juice (8, 9, 13). Specifically, data for 100% fruit juice, which provides nutrients expressed from the fruit, has often been combined with data on sugar-sweetened beverages and/or foods devoid of these nutrients.
The validity of combining 100% fruit juice with other sugar-sweetened beverages has been recently questioned in light of reports suggesting that 100% fruit juice may function differently with respect to dental health. For example, Salas et al. (14) conducted a meta-analysis on tooth erosion and diet and reported that the association of caries with natural fruit juices (OR, 1.20; 95% CI 0.02–1.42) was lower than that of carbonated beverages (OR, 1.60; 95% CI, 1.29-1.99) and sports drinks (OR, 2.13; 95% CI, 0.95–4.77), based on cross-sectional and prospective cohort data (14). Further, the 2015 Dietary Guidelines for Americans (DGA) specifically recommended the consumption of 100% fruit juice, and not fruit drinks (15). Additionally, the American Academy of Pediatrics (AAP) concluded that 100% fresh or reconstituted fruit juice can be part of a healthy diet of children older than 1 year, whereas fruit drinks are not considered nutritionally equivalent and are not recommended (16). However, it is not clear whether available evidence supports limiting or eliminating the intake of 100% fruit juice based on possible effects on dental health. Thus, the objective of this systematic review was to assess the scope and breadth of the publicly available prospective cohort and randomized controlled trial (RCT) research literature on 100% fruit juice and dental caries or tooth erosion in humans.
Methods
Standards
The search strategy and selection process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (17). The study was registered on PROSPERO (an international prospective register of systematic reviews) prior to data extraction (ID: CRD42018095619).
Search Strategy
Comprehensive literature searches were conducted independently in three databases (MEDLINE/PubMed, EMBASE, Web of Science [WOS]) for reports published from inception through the date of the search (initial search conducted on January 3, 2018 with an updated search conducted on May 7, 2018). The Cochrane Library database (http://www.cochranelibrary.com/about/central-landing-page.html) was also searched from inception through January 20, 2018. Search terms included “juice or juices” and terms related to dental health (including oral, tooth, teeth, dental, caries, and cavities) and beverage(s). The search included the use of terms for fruits as well as sugar-sweetened beverages to assure coverage of studies with beverages and dental health (full search terms for each database are provided in Supplementary Table S1). Searches were specific to literature published in English and in humans, but were not restricted to any age or publication date ranges. Hand-searching of selected reviews and publications was also conducted. Specifically, the studies presented in the SACN report were included in the hand-searching, with searches on cohorts conducted in-depth to identify data on 100% fruit juice and dental health.
Literature Selection
Selected studies were restricted to peer-reviewed human intervention and prospective cohort studies that were relevant to the general population with no age, sex, socioeconomic status or geographic limitations. Studies conducted in populations with a defined systemic disease were excluded, but assessment of a periodontal disease as an outcome was not an exclusion criterion. However, if the study was conducted specifically in individuals with established gum disease, the study was excluded. Reviews, editorials, in vitro studies, animal studies, and non-peer-reviewed reports were not included. Only publications in English were selected. In addition, consistent with the criteria in the SACN report, single meal studies as well as studies in preterm infants, or those with combinatorial interventions (e.g., drugs, toothpaste, behavioral) were also excluded (9). Observational studies other than prospective cohorts (e.g., cross-sectional, case-control, case series) were also excluded consistent with the SACN report and recommendations from the Food and Drug Administration and National Evidence Library (18, 19) due to the low level of evidence provided by these types of studies.
Although the focus was 100% fruit juice consumed as a beverage, the initial selection (abstract searching) was not restricted to indication of 100% fruit juice given the potential that study publications reporting on sugar-sweetened beverage, particularly in cohort analyses, may include data on 100% fruit juice in the body of the article or supplemental materials. If these studies included a relevant endpoint and met the study design criteria, the full-text and other publically-available information were further screened for data specifically on 100% fruit juice.
Outcome Measures
Outcomes for dental health were consistent with the SACN report (9) and included dental caries and tooth erosion. In addition, outcomes of tooth mineralization/ demineralization were also included, as these processes are part of the mechanism of dental caries and tooth erosion, and are measured in short-term clinical studies. The oral health outcomes of periodontal disease and oral cancer were not included.
Dental caries outcomes included mineralization/ demineralization of caries lesions and/or white spot lesions, as well as standard dental health indices. The standard approaches to assessment of dental caries include the Decayed, Missing, or Filled Teeth (DMFT or dmft when assessing permanent dentition or deciduous dentition, respectively) Index used for decay to crown of the tooth only, as well as the Decayed, Missing, or Filled tooth Surfaces (DMFS or dmfs when assessing permanent dentition or deciduous dentition, respectively) Index of decay activity that is valid when a large number of teeth are present (9, 10, 20). The International Caries Assessment and Detection System (ICDAS), which uses a 7-point scoring range, is designed to give gradation of severity of carious lesions, and radiological scoring and is used to detect the amount of demineralization of the enamel and/or dentin from a dental radiograph (9, 10, 20). Direct assessment of dental caries by a dentist is also used as a general measure. Tooth erosion is most often measured by microscopy and/or visual exam, and reported with respect to the amount of loss of the surface enamel, underlying dentin, and pulp exposure and several indices exist, with the overall measure the amount of tooth surface loss (9, 11).
Data Selection, Extraction, and Analysis
Title and abstract screenings were conducted by two independent investigators (DL, EM), and if discrepancies occurred in the title/abstract screen, the records were included in the full-text search listing for resolution. The full-texts of potentially eligible studies were retrieved and assessed for confirmation of meeting inclusion, and not meeting any exclusion criteria independently by two investigators (DL, EM). Disagreements between the two investigators were resolved by discussion. The rationale for selection and exclusion were documented in detail.
Extraction of data from selected studies included population, intervention, control, and outcome (PICO) chart and were performed by two investigators (DL, MK). Populations and outcome definitions and methods, as well as background factors were documented in detail for comparison of study designs. In addition, consideration of statistical approaches and noted confounder included in analyses were also documented.
Risk of Bias Assessment
Risk of bias for RCTs was performed using Version 2.0 of the Cochrane risk-of-bias tool for randomized trials (i.e., RoB 2) (https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool?authuser=0). One non-randomized study [i.e., (21)] was assessed using the ROBINS-I, tool which was developed to assess risk of bias in the results of non-randomized studies that compare health effects of two or more interventions included in Cochrane Reviews (https://sites.google.com/site/riskofbiastool/welcome/home?authuser=0). Finally, prospective cohort studies were assessed using the Newcastle-Ottawa Scale (NOS), which is an assessment tool that is also recommended by the Cochrane Collaboration (22). All quality assessments were independently performed by two investigators (DL, EM), whereby disagreements were discussed and resolved prior to finalization of the ratings.
Results
Search and Selection
The findings of the literature search-and-select are summarized in the PRISMA diagram (Figure 1). Search findings from databases and hand-searching were combined and duplicate records removed prior to title and abstract screening, resulting in 2,080 records. After title and abstract screening, 1983 records were excluded (no beverage or relevant oral health outcome, n = 1,675; non-relevant reviews, n = 66; animal or in vitro study, n = 147; not a prospective observational study or RCT, n = 95). Full-text publications were obtained for the remaining records (n = 97). The 97 full-text publications were screened in detail against the prospectively defined inclusion/exclusion criteria, and 17 studies were included in this analysis, with 80 excluded (Figure 1). A listing of the 80 excluded studies with rationale for exclusion per study is provided in Supplementary Tables S2a,b.
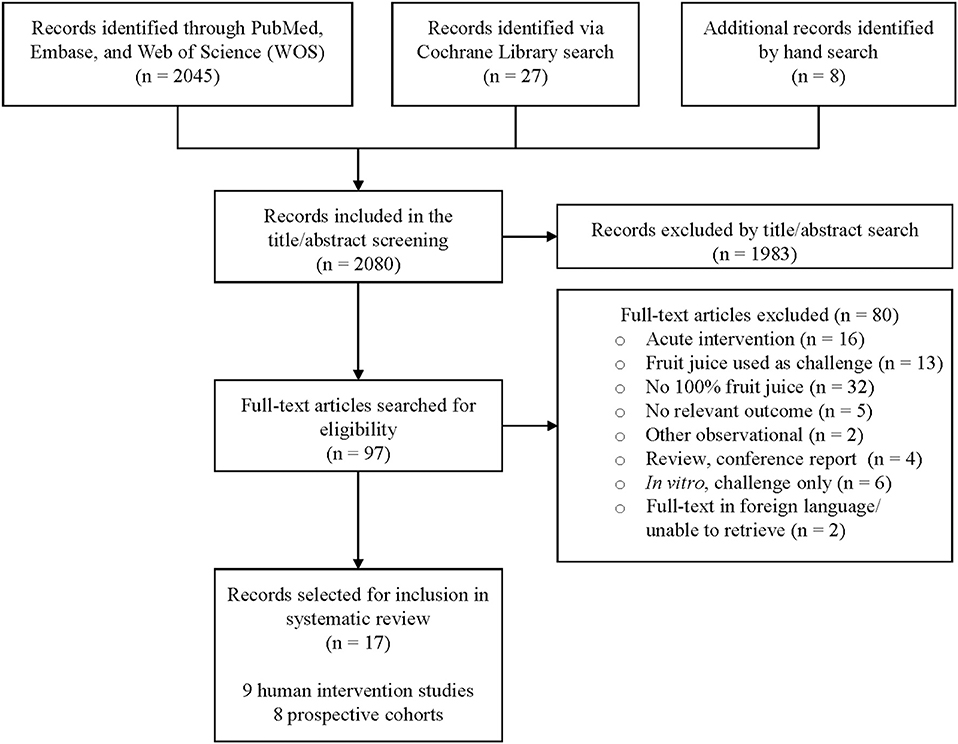
Figure 1. PRISMA diagram.
Prospective Cohort Studies
Eight publications identified for inclusion were prospective cohort studies. These publications represented seven different studies on five independent cohorts in children or adolescents that included fruit juice and a relevant dental health outcome. Descriptions of these studies, including NOS quality ratings, are provided in Table 1, and the results of the studies are summarized in Table 2. Two of these studies (20, 29) did not clearly identify 100% fruit juice, but were included in the Salas et al. review (14) as representing data on natural fruit juices separate from fruit drinks and other sugar-containing beverages. The overall dataset includes three reports on the Iowa Fluoride Study cohort (23, 26, 27, 29), and one report each from the Low Income African American cohort in Michigan (28), the Low Income African American Cohort in Alabama (20), a Leicestershire UK cohort (24), and a cohort consisting of children in a small community in the Netherlands (25). Two of these cohorts (the Iowa Fluoride cohort and the Low Income African American cohort in Michigan) were also included in the SACN report, another two (the Leicestershire UK cohort and the Netherland children cohort) were reported in the Salas et al. (14) review, while the fifth cohort (the Low Income African American Cohort in Alabama) appears not to have been included in previous systematic reviews. Three studies reported on erosion and juice (23–25) and four reported on caries and juice (20, 26–29). Using the NOS tool, four studies (23, 25, 27, 28) were rated as Good, one study (20) was rated as Fair, and the remaining three studies (24, 26, 29) were rated as Poor. Studies rated as Poor had low quality for the outcome/exposure domain mainly due to unclear description of blinding of outcome assessment and inadequate follow-up of cohorts.
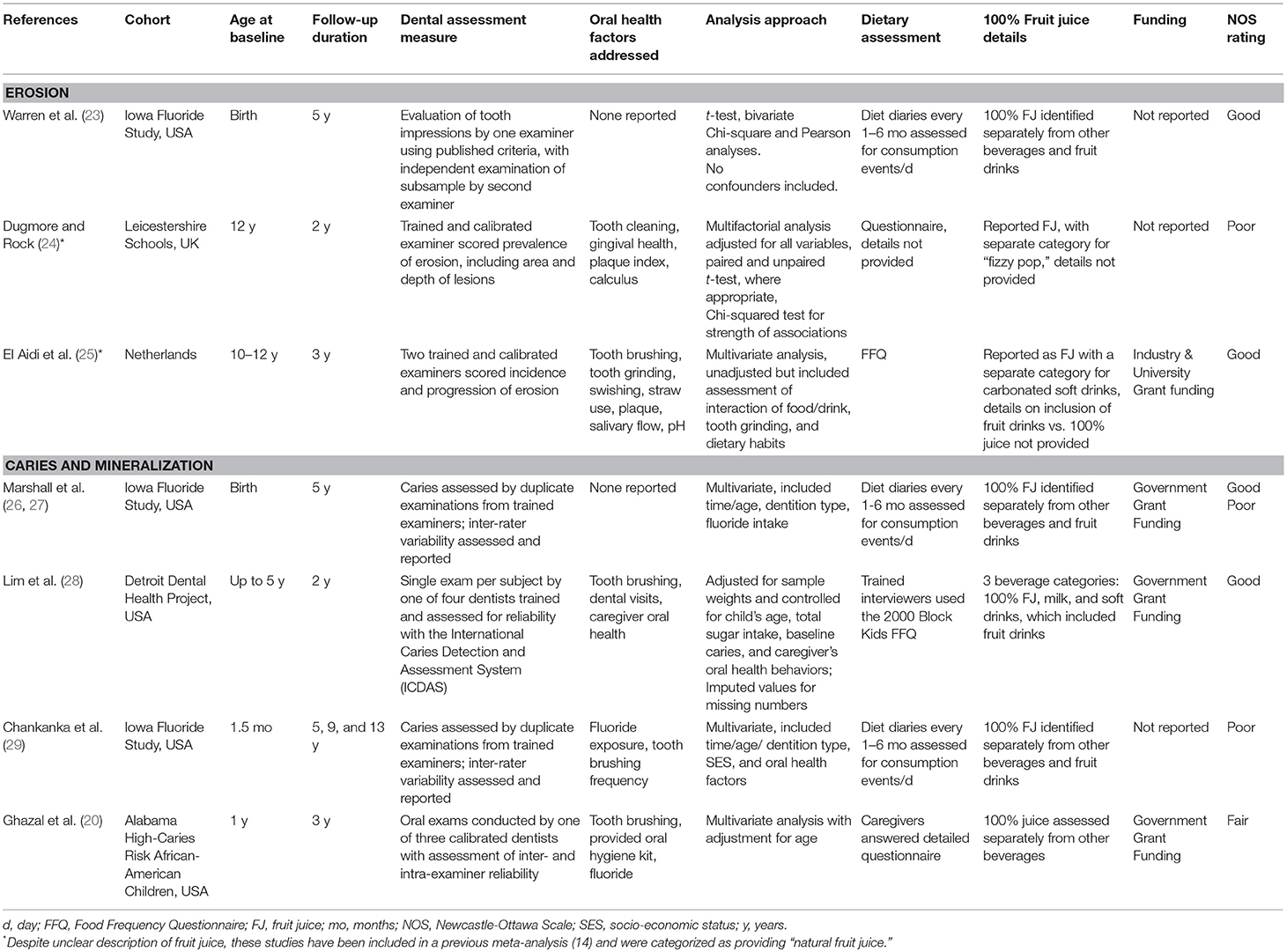
Table 1. Description of prospective cohort studies on 100% fruit juice and dental health.
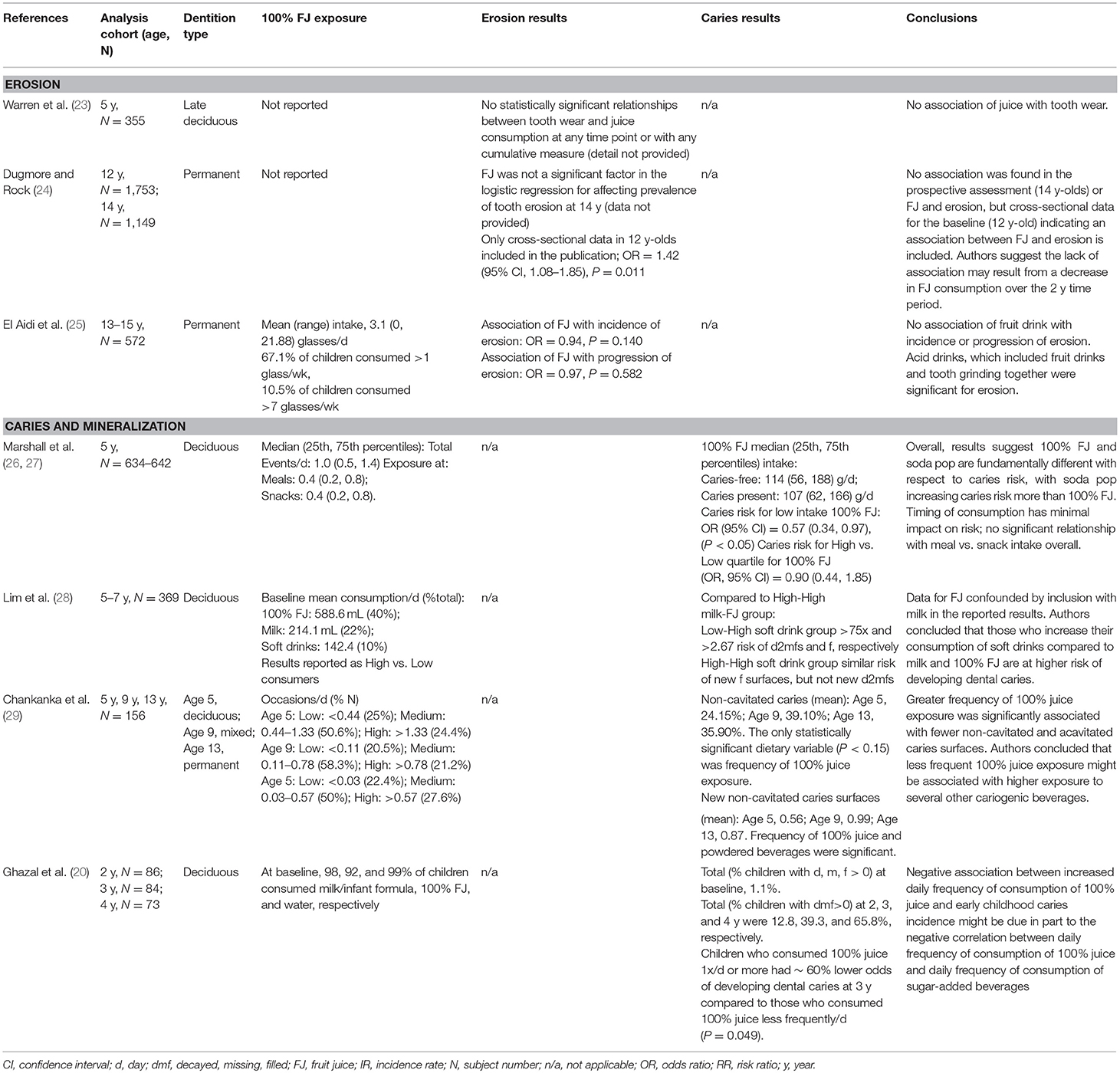
Table 2. Results of prospective cohorts on 100% fruit juice and dental health.
The three cohort studies on erosion and juice included one study (23) in children with deciduous teeth (N = 355, age 5 y), and two studies (24, 25) in adolescents with permanent teeth (N = 2,325, age 12–15 y), with follow-up of 2–5 y. All three studies found no association between juice and tooth erosion, although only two (24, 25) of the three provide quantitative data. One of the studies also included a cross-sectional assessment of the baseline data for the cohorts, which indicated an association; however, the 2-year follow-up data from cohorts did not indicate an association (24). The studies on erosion utilized similar evaluation approaches, with two including oral examinations by trained and calibrated examiners (24, 25), and one utilizing tooth impressions that were assessed by two independent examiners (23). The approach to assessing fruit juice exposure, however, varied considerably, with only one of the three reports clearly differentiating fruit drinks from fruit juice (23). The other reports mentioned juice, but did not clearly indicate that only 100% fruit juice was included (24, 25). The approach to analysis also varied, with one not including confounders or adjusting for multiple comparisons (23), while the other two used an approach for multivariate analysis and/or addressed confounding, albeit different factors were included (24, 25). One of the studies indicated some funding from industry (25), and the other two did not report funding source (23, 24).
The studies on caries and juice were more varied in the population studies, but similar to the erosion studies, only included children and adolescents. Overall, the five studies on caries and/or mineralization represented data from 1,232 to 1,253 children ranging in age from 2 to 13 y, which included children with deciduous and permanent teeth, with follow-up of 2–13 y (20, 26–29). These studies reported either no association or an inverse association between intakes of 100% fruit juice and the incidence of dental caries.
Randomized Controlled Trials
Nine RCTs that assessed the effect of 100% fruit juice on an aspect of dental health were identified, with six of these on fruit juice and erosion, and three on fruit juice and caries. The RCTs on erosion and fruit juice are summarized in Table 3, and those on dental caries and fruit juice outlined in Table 4.
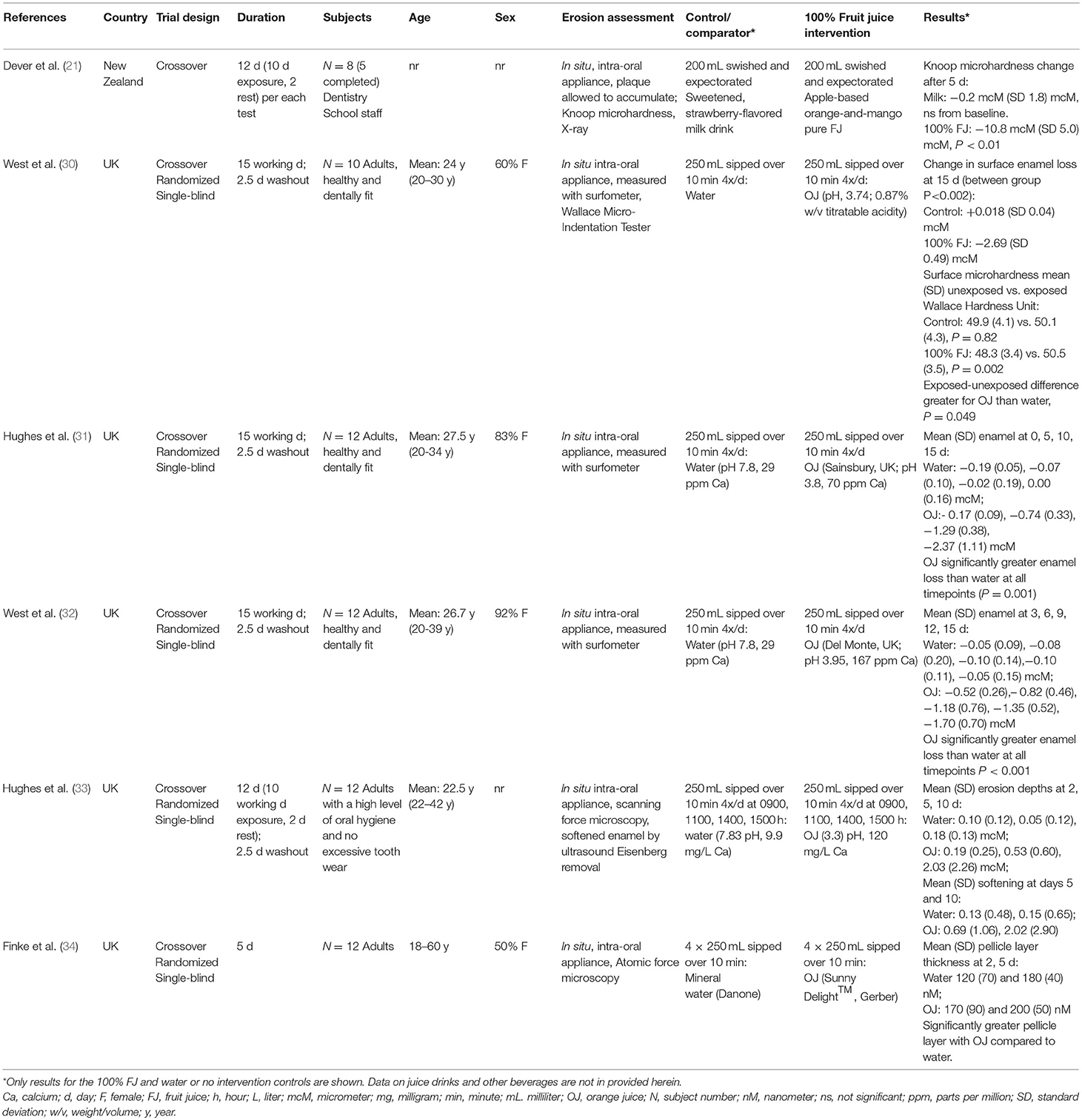
Table 3. Description of randomized controlled trials on 100% fruit juice and tooth erosion.
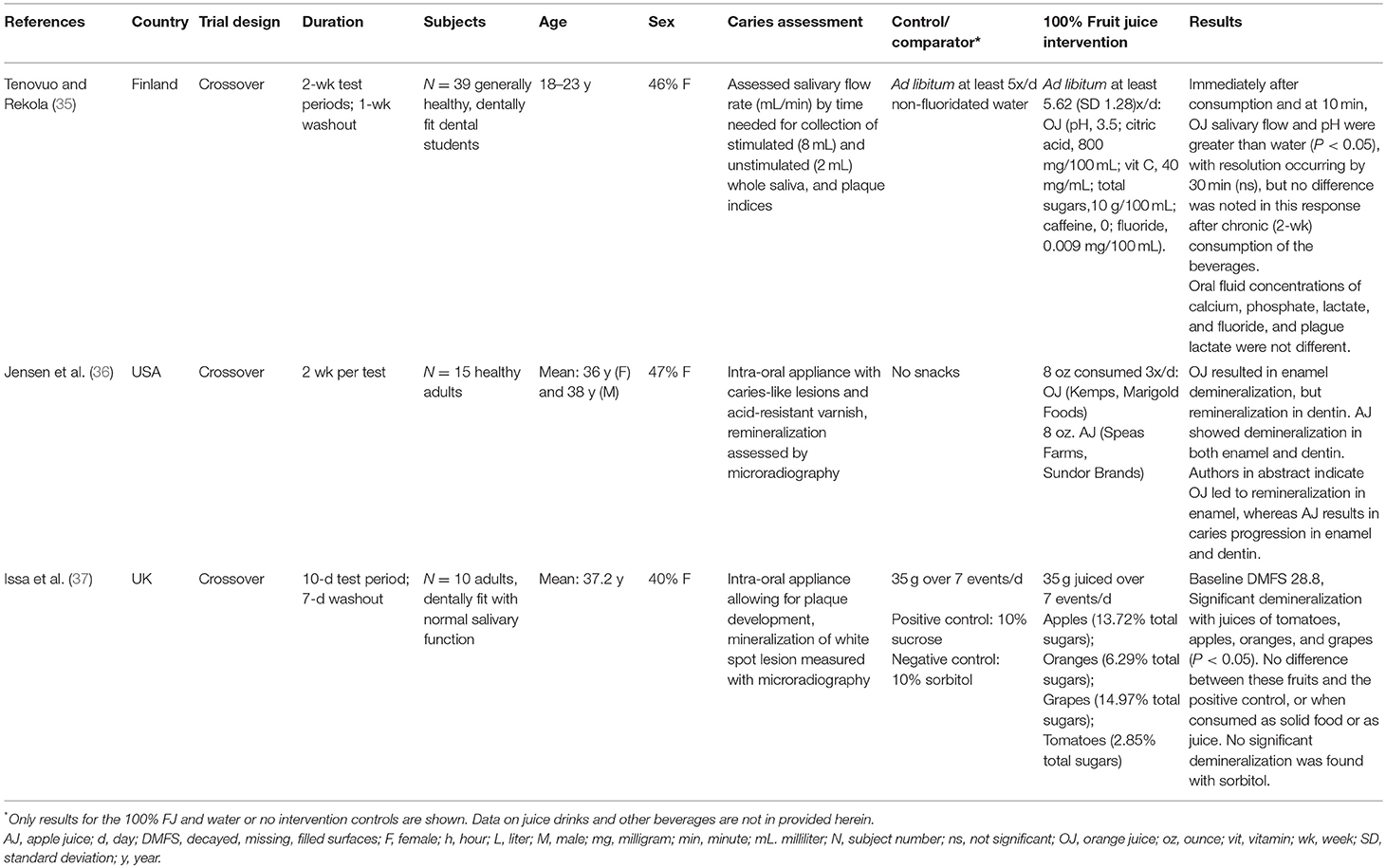
Table 4. Description of randomized controlled trials on 100% fruit juice and caries.
Of the six RCTs which addressed fruit juice and erosion, one compared fruit juice to milk (21), while the other five compared fruit juice to water (30–34). All but one (21) of these studies used orange juice as the 100% fruit juice, and several of these included orange juice as a positive control. All studies were crossover designs, varying from 5 to 15 days of beverage exposure, and small, having only 5–12 evaluable subjects. The subjects in the studies were adults. Five studies indicated using a randomized single-blind approach, with no detail provided by one study (21). Four (30–33) of the six studies measured enamel loss, one measured thickness of the pellicle (34), which is a protein film on the surface of the enamel, and one study assessed the hardness of the enamel and dentin (21). Each study was conducted as an in situ analysis using an intra-oral device developed with a machined enamel slab, and the device was cleaned of plaque every day. Therefore, these data did not assess enamel loss in the presence of normally accumulated plaque. All RCTs were rated as having some concerns using the RoB 2 tool due to possible presence of bias arising from the randomization process and effect of assignment to intervention. Meanwhile, the Dever et al. (21) study was rated as having critical risk of bias using the ROBINS-I assessment tool. Concerns of bias for this study were mostly due to confounding, classification of interventions, and missing data.
All six RCTs on tooth erosion and fruit juice (21, 30–34) showed a positive relationship between 100% juice consumption and decreased microhardness, surface enamel loss, erosion depth, enamel softening, and increased pellicle layer. However, the data on erosion and fruit juice are limited, with the data comparing fruit juice to water or no intervention. In addition, four (30–33) of the six studies were conducted by the same research team. The other two studies either indicated co-funding by industry, or did not indicate a funding source (Table 5). Therefore, independent data on fruit juice and erosion were not found.
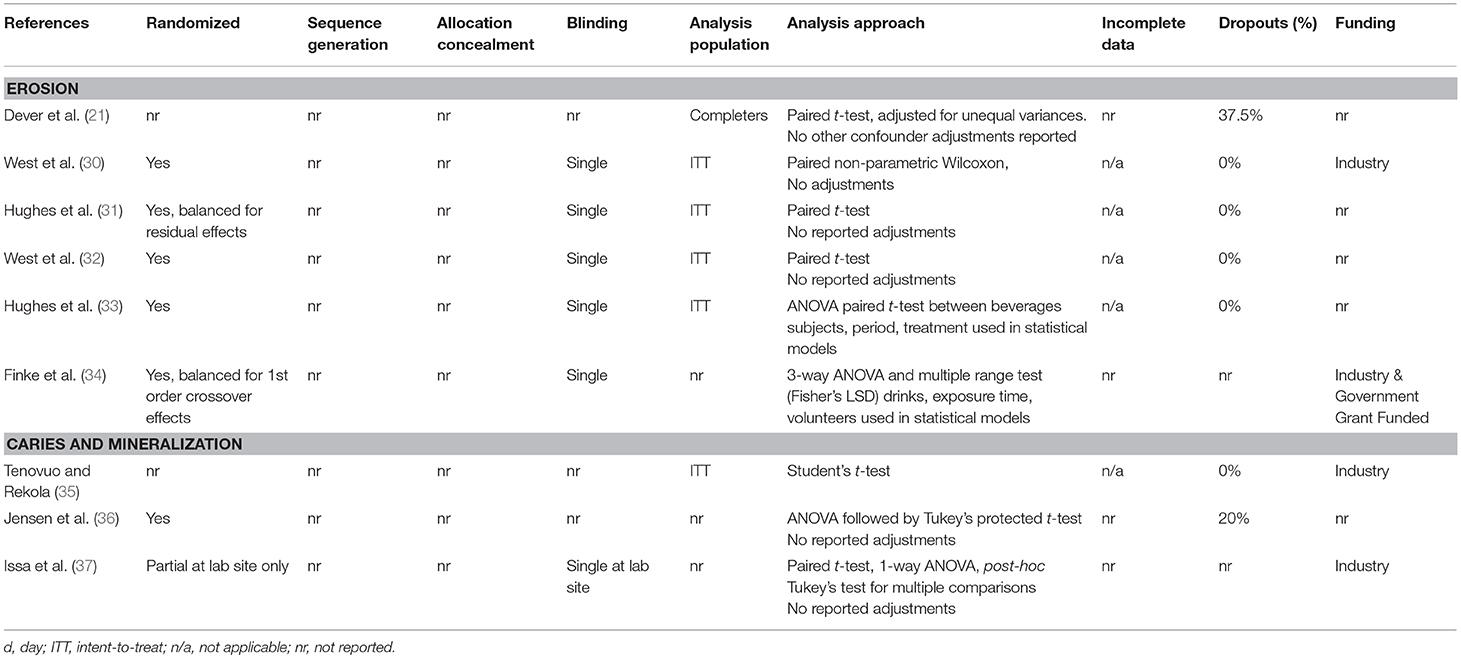
Table 5. Risk of bias assessment of randomized controlled studies on 100% fruit juice and dental health.
Of the three RCTs which assessed caries or mineralization/demineralization, two (35, 36) assessed orange juice, with one of these also including apple juice (36), while the other study compared a number of fruits, including orange, grapes, and apples consumed as freshly juiced beverages or as whole fruits (37). Although these studies tended to have similar designs (e.g., crossover, duration 10–14 days, dentally fit adults), they varied substantially with respect to analyses. One study assessed salivary and plaque indices (35), while the other two utilized an in situ approach with intra-oral appliances and reported on aspects of mineralization (36, 37). Overall, there is limited RCT data for fruit juice and caries, and the study designs were quite varied. One study suggested orange juice did not lead to pro-cariogenic changes in salivary and plaque parameters (35), and the two studies on mineralization indicated demineralization occurs with fruit juices (36, 37), although one of these reported mixed results for orange juice (36). Two of the studies indicated funding from industry (35, 37), and one did not report a funding source (36). Only one of the studies clearly indicated randomization (36), while one indicated the study design did not allow for full randomization (37), and the other study did not report randomization (35). There was some suggestion that not all subjects were included in the respective analyses in two of the studies (36, 37).
Discussion
Sugar-containing foods and beverages have been a focus of public policy recommendations related to dental health, principally dental caries and tooth erosion (6, 38). However, these reports have combined data from multiple sources of foods and have not specifically addressed 100% fruit juices. Instead, conclusions on 100% fruit juice have most often been developed from data on sugar-sweetened beverages and/or foods that have either combined the 100% fruit juice data with data on other foods or beverages, or from data which did not include 100% fruit juice. This report provides the results of intervention and prospective cohort studies that have specifically addressed the effects of 100% fruit juice on outcomes or markers of dental health. Results from prospective studies in adolescents and children indicate that 100% fruit juice consumption is not associated with incidence of dental caries and tooth erosion. However, intervention studies in adults suggest that 100% fruit juice could contribute to increased tooth erosion or negative effects on markers of dental caries, although these studies primarily utilized in-situ intra-oral enamel appliances.
To the best of our knowledge, only one systematic review has assessed 100% fruit juice and dental health as its primary focus, which included five cross-sectional studies with two prospective cohort studies that assessed erosion as a sub-analysis only, and reported a possible association with 100% fruit juice (OR = 1.20; 95% CI 0.02–1.42, p = 0.03), although the data indicated high heterogeneity (I2 = 74.6%, p = 0.001) (14). Most notably, the two prospective cohorts in that analysis reported no association, indicating the positive association was found only in the cross-sectional data and was not supported by prospective studies. The present review did not include cross-sectional studies and identified one additional prospective cohort that also reported no association between juice intake and tooth erosion (23). Although the present review did not include case-controls, two case-controls studies on tooth erosion and 100% fruit juice were identified during the search process and results were mixed. One study reported no significant relationship between fruit juice consumption and tooth wear in children in Liverpool, UK (N = 60, 15 y) (39), while another found a significant association between the duration of intake of orange juice and tooth wear in Malaysian children (N = 576, 16 y) (40). However, neither of these case-control studies clearly described the fruit juice as being 100% fruit juice.
Meanwhile, the five prospective cohort studies on 100% juice intakes and caries incidence reported herein found either no association or an inverse association. The search process also identified three case-control studies on caries and fruit juice and results were also mixed, with two reports of a positive association between fruit juices and root caries in adults (N = 275) and early childhood caries (N = 119) (41, 42) and one report of an inverse relationship between fruit juice consumption and early childhood caries in preschool children in Egypt (N = 60) (43). However, similar to those on tooth erosion, none of these case-control studies clearly described the fruit juice as being 100% fruit juice.
With respect to RCT data, three RCTs were identified that assessed caries or mineralization/demineralization and six RCTs reported on 100% fruit juice and erosion (21, 30–34). All six studies reported a positive relationship between 100% fruit juice consumption and erosion or markers for cavities (e.g., decreased microhardness, increased surface enamel loss, increased erosion depth, greater enamel softening, and/or increased pellicle layer). Additionally, studies on caries and fruit juice showed increased demineralization of enamel slabs despite increased acute saliva production, which is considered a protective factor. With the exception of one study that assessed saliva production, all the clinical trials identified in this review employed in situ intra-oral appliances, whereby enamel samples were placed in dental appliances worn by subjects who were then instructed to consume the test beverages generally throughout the day. This allowed changes to be observed within the context of the subjects' normal diet and dental hygiene, although the appliances were cleaned of plaque daily. The studies were generally short (≤ 15 days) and small (all but one study included ≤ 12 subjects). In addition, the frequency of juice consumption in these studies was often greater compared to normal conditions of consumption, with the intake of the fruit juice and/or number or events several times higher (generally>750 mL or at least 4 events per day) than average intakes [<250 mL per day (5)]. Therefore, the clinical studies do not represent the normal intake conditions, and instead, were designed to detect potential changes using aggressive methods.
Studies on the effect of diet on dental health are challenging. For example, the methodology for assessing tooth erosion and caries is heterogeneous, likely because techniques for assessing erosive damage or demineralization are heterogeneous. While there are several techniques that have found acceptance in published studies, none have achieved scientific consensus or certification by an authoritative body (44, 45). Another limitation of the clinical studies of erosion and dental caries is the challenge of blinding subjects to the intervention. The identities of different juices are virtually impossible to conceal due to distinct and identifiable color and sensory differences. The enamel slabs may be more susceptible to erosion as they are either human enamel slabs which can have reduced hardness because they are taken from below the outer surface of extracted human teeth, where the enamel is the hardest (30); or bovine enamel which is more porous than human enamel (46). In addition, the number of available subjects has generally been small, often recruited from the students and faculty of dental schools. Where multiple products have been tested, the order of testing of products assigned to individuals or groups of subjects can be randomized, which has been the case for crossover studies of multiple products.
Limitations
All prospective cohort studies were conducted in children and adolescents while RCTs were only in adults, and the differences in populations between the two types of studies may contribute to the observed differential outcomes. The prospective studies also reflect more normal intakes of the juices and dental hygiene practices, compared with the clinical studies, which utilized high intake and consumption approaches. For example, prospective cohort studies used either food frequency questionnaires or diet records to assess habitual intakes of fruit juice, which better reflects normal consumption of fruit juice relative to the identified clinical studies, and thus, the progression of tooth erosion or caries. Furthermore, the prospective cohort studies also have the advantage of assessments of outcomes, i.e., erosion or caries, rather than the surrogate markers found in the clinical studies. However, as with other observational studies, prospective cohort studies strongly aid in studying causal associations but cannot distinguish true causality.
The studies included in this review may not represent all prospective cohort and intervention studies on 100% fruit juice and dental health because studies not published in English were excluded and those not cited in the databases used may have been missed. However, effort was made during this review to hand search all references in selected reviews and reports. In addition, this review excludes single meal studies and those in diseased populations, and thus does not contribute information about the acute effects of 100% fruit juice on dental health and in diseased individuals. Finally, observational studies other than prospective cohorts (e.g., cross-sectional, case-control, case series) were not included as these are generally not considered in many evidence-based reviews due to the likelihood of high bias.
Conclusions
Products meeting the definition of 100% fruit juice comprise a distinct class of beverage and have been identified as candidates for limited consumption by the general population by virtue of their content of sugars and relatively low pH. The rationale for such a recommendation stemmed from the perception that the consumption of fruit juices might contribute to tooth erosion, dental caries, or both. However, the existing evidence on 100% fruit juice intake and dental caries or tooth erosion are not conclusive. Prospective cohort studies in children and adolescents found no association between 100% fruit juice intake and tooth erosion and no association or inverse association between 100% fruit juice intake dental caries, whereas RCTs in adults suggest that 100% fruit juice could contribute to tooth erosion and dental caries. Although the RCT is the gold-standard for demonstrating cause-and-effect, the RCTs on 100% fruit juice and dental health have employed conditions that were extreme for amounts and exposures relative to normal intakes of 100% fruit juices. In addition, other methodological concerns, such as using more susceptible enamel slabs for experiments, could have contributed to the differential results found with the RCTs. Further, due to the challenges in clinical studies on dental health outcomes, particularly in vulnerable populations such as children, the development of consensus study techniques which more accurately reflect the dynamics of healthy teeth is also warranted. Therefore, well-designed, larger intervention studies on 100% fruit juice and dental health outcomes that implement consensus study techniques which more accurately reflect the dynamics of healthy teeth in both adults and children are needed for policy-making and clinical recommendations on intake of 100% fruit juice.
Author Contributions
DL and EM were responsible for the systematic search, screening, and data extraction. DL and MK prepared the original draft manuscript. All authors reviewed and edited the manuscript and approved the final version.
Conflict of Interest Statement
DL and EM received partial funding from Juice Products Associations to conduct this systematic review. MK received a consulting fee from the Juice Products Association for his contributions to this manuscript. DL, EM, and MK provide consulting services in nutrition science to industry associations, companies and other organizations. Juice Product Association was involved in the conceptualization of this project, but was not involved in the screening, data extraction, interpretation, and writing of this manuscript.
Acknowledgments
The authors thank Deena Wang for assistance with the searches and publication retrieval.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00190/full#supplementary-material
References
1. Centers for Disease Control and Prevention. Oral and Dental Health. (2017) Available online at: https://www.cdc.gov/nchs/fastats/dental.htm (accessed March 19, 2019).
2. Salas MM, Nascimento GG, Huysmans MC, Demarco FF. Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis. J Dent. (2015) 43:42–50. doi: 10.1016/j.jdent.2014.10.012
3. Heilmann A, Tsakos G, Watt RG. Oral Health Over the Life Course. In: Burton-Jeangros C, Cullati S, Sacker A, Blane D, editors. A Life Course Perspective on Health Trajectories and Transitions. Cham: Springer (2015) p. 39–59. doi: 10.1007/978-3-319-20484-0_3
4. Antunes JL, Toporcov TN, Bastos JL, Frazao P, Narvai PC, Peres MA. Oral health in the agenda of priorities in public health. Rev Saude Publ. (2016) 50:57. doi: 10.1590/S1518-8787.2016050007093
5. Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture. U.S. Department of Agriculture. Agricultural Research Service. (2015). Available online at: https://health.gov/dietaryguidelines/2015-scientific-report/pdfs/scientific-report-of-the-2015-dietary-guidelines-advisory-committee.pdf (accessed October 2, 2018).
7. WHO. Expert Consultation on Public Health Intervention against Early Childhood Caries: report of a meeting, Bangkok, Thailand, 26-28 January 2016. Geneva (2017).
8. Moynihan PJ, Kelly SA. Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. (2014) 93:8–18. doi: 10.1177/0022034513508954
9. Scientific Advisory Committee on Nutrition (SACN). Systematic Review of Evidence: Carbohydrates and Health July 17, 2015. (2015).
10. Anil S, Anand PS. Early childhood caries: prevalence, risk factors, and prevention. Front Pediatr. (2017) 5:157. doi: 10.3389/fped.2017.00157
11. Taji S, Seow WK. A literature review of dental erosion in children. Aust Dent J. (2010) 55:358–67; quiz 475. doi: 10.1111/j.1834-7819.2010.01255.x
12. Richards D. Impact of diet on tooth erosion. Evid Based Dent. (2016) 17:40. doi: 10.1038/sj.ebd.6401164
13. Moynihan P. Sugars and dental caries: evidence for setting a recommended threshold for intake. Adv Nutr. (2016) 7:149–56. doi: 10.3945/an.115.009365
14. Salas MM, Nascimento GG, Vargas-Ferreira F, Tarquinio SB, Huysmans MC, Demarco FF. Diet influenced tooth erosion prevalence in children and adolescents: results of a meta-analysis and meta-regression. J Dent. (2015) 43:865–75. doi: 10.1016/j.jdent.2015.05.012
15. Department of Health and Human Services, Agriculture Do. 2015–2020 Dietary Guidelines for Americans. 8th ed. (2015).Available online at: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed March 19, 2019).
16. Heyman MB, Abrams SA. Section on gastroenterology h, nutrition, committee on n. fruit juice in infants, children, and adolescents: current recommendations. Pediatrics. (2017) 139:967. doi: 10.1542/peds.2017-0967
17. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) 339:b2535. doi: 10.1136/bmj.b2535
18. Nutrition Evidence Library. 2010 Dietary Guidelines Advisory Committee (DGAC) Nutrition Evidence Library Methodology. (2017). Available online at: https://www.cnpp.usda.gov/sites/default/files/usda_nutrition_evidence_flbrary/2010DGAC-SR-Methods.pdf (accessed March 19, 2019).
19. US Department of Health and Human Services, Food and Drug Administration, Center for Food Safety and Applied Nutrition. Guidance for Industry: Evidence-Based Review System for the Scientific Evaluation of Health Claims. (2009). Available online at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-evidence-based-review-system-scientific-evaluation-health-claims (accessed March 18, 2019).
20. Ghazal T, Levy SM, Childers NK, Broffitt B, Cutter GR, Wiener HW, et al. Factors associated with early childhood caries incidence among high caries-risk children. Community Dent Oral Epidemiol. (2015) 43:366–74. doi: 10.1111/cdoe.12161
21. Dever JG, Thomson ME, Hampton M. Fruit juice and flavoured milk: effects on enamel in an intra-oral model. N Z Dent J. (1987) 83:7–10.
22. Cochrane handbook for systematic reviews of interventions. In: Higgins JPT, Green S, editors. The Cochrane Collaboration (2011). Available online at: https://training.cochrane.org/handbook
23. Warren JJ, Yonezu T, Bishara SE. Tooth wear patterns in the deciduous dentition. Am J Orthod Dentofacial Orthop. (2002) 122:614–8. doi: 10.1067/mod.2002.129193
24. Dugmore CR, Rock WP. A multifactorial analysis of factors associated with dental erosion. Br Dent J. (2004) 196:283–6; discussion 273. doi: 10.1038/sj.bdj.4811041
25. El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ. Multifactorial analysis of factors associated with the incidence and progression of erosive tooth wear. Caries Res. (2011) 45:303–12. doi: 10.1159/000328671
26. Marshall TA, Levy SM, Broffitt B, Warren JJ, Eichenberger-Gilmore JM, Burns TL, et al. Dental caries and beverage consumption in young children. Pediatrics. (2003) 112(3Pt 1):e184–191. doi: 10.1542/peds.112.3.e184
27. Marshall TA, Broffitt B, Eichenberger-Gilmore J, Warren JJ, Cunningham MA, Levy SM. The roles of meal, snack, and daily total food and beverage exposures on caries experience in young children. J Public Health Dent. (2005) 65:166–73. doi: 10.1111/j.1752-7325.2005.tb02807.x
28. Lim S, Sohn W, Burt BA, Sandretto AM, Kolker JL, Marshall TA, et al. Cariogenicity of soft drinks, milk and fruit juice in low-income african-american children: a longitudinal study. J Am Dent Assoc. (2008) 139:959–67; quiz 995. doi: 10.14219/jada.archive.2008.0283
29. Chankanka O, Cavanaugh JE, Levy SM, Marshall TA, Warren JJ, Broffitt B, et al. Longitudinal associations between children's dental caries and risk factors. J Public Health Dent. (2011) 71:289–300. doi: 10.1111/j.1752-7325.2011.00271.x
30. West NX, Maxwell A, Hughes JA, Parker DM, Newcombe RG, Addy M. A method to measure clinical erosion: the effect of orange juice consumption on erosion of enamel. J Dent. (1998) 26:329–35. doi: 10.1016/S0300-5712(97)00025-0
31. Hughes JA, West NX, Parker DM, Newcombe RG, Addy M. Development and evaluation of a low erosive blackcurrant juice drink. 3. Final drink and concentrate, formulae comparisons in situ and overview of the concept. J Dent. (1999) 27:345–50. doi: 10.1016/S0300-5712(98)00068-2
32. West NX, Hughes JA, Parker DM, Newcombe RG, Addy M. Development and evaluation of a low erosive blackcurrant juice drink. 2. Comparison with a conventional blackcurrant juice drink and orange juice. J Dent. (1999) 27:341–4. doi: 10.1016/S0300-5712(98)00070-0
33. Hughes JA, Jandt KD, Baker N, Parker D, Newcombe RG, Eisenburger M, et al. Further modification to soft drinks to minimise erosion. A study in situ. Caries Res. (2002) 36:70–4. doi: 10.1159/000057594
34. Finke M, Parker DM, Jandt KD. Influence of soft drinks on the thickness and morphology of in situ acquired pellicle layer on enamel. J Colloid Interface Sci. (2002) 251:263–70. doi: 10.1006/jcis.2002.8428
35. Tenovuo J, Rekola M. Some effects of sugar-flavored acid beverages on the biochemistry of human whole saliva and dental plaque. Acta Odontol Scand. (1977) 35:317–30. doi: 10.3109/00016357709064131
36. Jensen ME, Donly K, Wefel JS. Assessment of the effect of selected snack foods on the remineralization/demineralization of enamel and dentin. J Contemp Dent Pract. (2000) 1:1–17.
37. Issa AI, Toumba KJ, Preston AJ, Duggal MS. Comparison of the effects of whole and juiced fruits and vegetables on enamel demineralisation in situ. Caries Res. (2011) 45:448–52. doi: 10.1159/000330597
38. U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary Guidelines for Americans 2015-2020. (2015). Available online at: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed 19 March, 2019).
39. Milosevic A, Lennon MA, Fear SC. Risk factors associated with tooth wear in teenagers: a case control study. Commun Dent Health. (1997) 14:143–7.
40. Saerah NB, Mastura N, bin Ismail AR, Sadiq MA. Associated factors of tooth wear among Malaysian 16-year-olds: a case-control study in Kota Bharu, Kelantan. Commun Dent Health. (2012) 29:33–8.
41. Papas AS, Joshi A, Belanger AJ, Kent RL Jr, Palmer CA, DePaola PF. Dietary models for root caries. Am J Clin Nutr. (1995) 61:417S−22S. doi: 10.1093/ajcn/61.2.417S
42. Paglia L, Scaglioni S, Torchia V, De Cosmi V, Moretti M, Marzo G, et al. Familial and dietary risk factors in early childhood caries. Eur J Paediatr Dent. (2016) 17:93–9.
43. AbdelAziz WE, Dowidar KM, El Tantawi MM. Association of healthy eating, juice consumption, and bacterial counts with early childhood caries. Pediatr Dent. (2015) 37:462–7.
44. Oliveira GC, Tereza GPG, Boteon AP, Ferrairo BM, Goncalves PSP, Silva TCD, et al. Susceptibility of bovine dental enamel with initial erosion lesion to new erosive challenges. PLoS ONE. (2017) 12:e0182347. doi: 10.1371/journal.pone.0182347
45. Young A, Tenuta LM. Initial erosion models. Caries Res. (2011) 45(Suppl. 1):33–42. doi: 10.1159/000325943
Keywords: caries, erosion, sugar, teeth, oral, sugar-sweetened beverage
Citation: Liska D, Kelley M and Mah E (2019) 100% Fruit Juice and Dental Health: A Systematic Review of the Literature. Front. Public Health 7:190. doi: 10.3389/fpubh.2019.00190
Received: 14 December 2018; Accepted: 24 June 2019;
Published: 12 July 2019.
Edited by:
Dohyeong Kim, The University of Texas at Dallas, United StatesReviewed by:
Le Jian, Curtin University, AustraliaAnthony Pascual Calibo, Department of Health (Philippines), Philippines
Copyright © 2019 Liska, Kelley and Mah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: DeAnn Liska, ZGVhbm4ubGlza2FAbXhucy5jb20=