 Wendell C. Taylor
Wendell C. Taylor Richard R. Suminski
Richard R. Suminski Bhibha M. Das
Bhibha M. Das Raheem J. Paxton
Raheem J. Paxton Derek W. Craig
Derek W. Craig- 1Department of Health Promotion and Behavioral Sciences, Center for Health Promotion and Prevention Research, School of Public Health, The University of Texas Health Science Center at Houston, Houston, TX, United States
- 2Department of Behavioral Health and Nutrition, Center for Innovative Health Research, University of Delaware, Newark, DE, United States
- 3Department of Kinesiology, East Carolina University, Greenville, NC, United States
- 4Department of Community Medicine and Population Health, University of Alabama, Tuscaloosa, AL, United States
Background: Time spent in sedentary behaviors is an independent risk factor for several chronic diseases (e.g., cardiometabolic diseases, obesity, type 2 diabetes, and hypertension). Recently, interventions to reduce sitting time at work (a prominent sedentary behavior) have been developed and tested. Organizational culture plays a critical role in the success of workplace interventions. However, there are a limited number of studies that have examined the role of organizational culture in reducing sitting time in the workplace.
Objectives: Therefore, in this systematic review, we summarized the empirical literature investigating organizational culture and sedentary behavior in the workplace and identify gaps in the knowledge base.
Methods: We described the procedures of our systematic review and included two study flow diagrams that detailed the step by step process. Combinations of several search terms were used; the databases searched were PubMed, Medline, Academic Search Complete, and Google Scholar. We started with thousands of citations. After applying the inclusion and exclusion criteria, eight relevant articles were identified.
Results: For each identified article, the data extracted included citation, sample, objective, intervention, assessment of organizational culture and workplace sitting, findings, and implications. Each article was rated for risk of bias by population, intervention, comparator, outcomes, and study design (PICOS) analysis. The classification for each study was either: high-, moderate-, or low-quality evidence. Given the paucity of data, no definitive conclusions were presented; however, positive trends were highlighted.
Conclusions: Work place interventions to reduce sitting time at work may benefit from considering elements of organizational culture; however, the evidence to date is sparse and more high-quality studies in this area are needed. To advance the field of workplace health promotion, organizational culture, and interventions to reduce sitting at work, we present 11 recommendations.
Key Concepts
Organizational culture: Organizational culture is the shared values, beliefs, or perceptions held by employees within an organization or organizational unit (1).
Sedentary behavior: Any waking behavior characterized by energy expenditure ≤ 1.5 metabolic equivalents, while in a sitting, reclining, or lying posture (2).
Culture of health (COH): Environments with a culture of health, place value on, and are conducive to, employee health and well-being (3). A concern for employee health must permeate all aspects of an organization and its corporate identity (4).
Introduction
On average, Americans spend ~9 h sleeping or engaging in personal care activities (5). In addition, Americans spend ~8 h working or doing work-related activities; therefore, one-half of waking hours are related to work (5). So, what happens at work has undeniable consequences for physical, psychological, emotional, and social well-being. Unfortunately, in the workplace, sitting remains the dominant posture for office-based workers. Although there are detrimental health consequences associated with prolonged sitting, limited data exist on the variety of factors that contribute to this cultural norm.
Rationale
High levels of sitting are associated with increased risk of several adverse health outcomes including diabetes, heart disease, type-2 diabetes, and obesity. Sedentary behavior may be an independent risk factor for chronic diseases especially among adults with insufficient or low physical activity levels (6–8).
To reduce sedentary behavior in the workplace, understanding the influence of organizational culture on these behaviors is critical. Even though there are different definitions of organizational culture, an accepted definition is artifacts, espoused beliefs and values, and underlying assumptions (9). Artifacts are behaviors, rituals, language, myths, and dress. Espoused beliefs and values are typically reported by management as core to the organization. Underlying assumptions relate to organizational life and illuminates why organizational members go about their day-to-day work lives as they do (9). In essence, organizational culture is enduring, stable, and can take a long time to develop. In simple terms, organizational culture represents shared basic assumptions, values, and beliefs that characterize a setting and are taught to newcomers as the proper way to think and feel as employees of the organization.
Objectives
The importance of organizational culture and health outcomes has been documented. There is evidence that health promotion programs that incorporate more cultural elements in their strategies result in a reduction of employee health risks by as much as 5% per year, a level 2.5 times greater than health promotion programs without a cultural component (10). Another study found that most organizations with cultural support (66%) reported greater improvements in health behaviors compared to organizations with little or no cultural support (26%) (11). From a related perspective, organizations with very supportive leadership were almost 4 times more likely to report substantial improvements in employee health risks and 2.5 times more likely to report substantial improvements in medical cost trends. Importantly, the inverse was true. Organizations with minimally supportive leadership were ~4 times more likely to report minimal improvements in both employee health risks and medical cost trends (12). Based on existing literature, we hypothesize that organizational culture can hinder or enhance intervention programs to reduce sedentary behavior in the workplace.
Research Questions/Specific Aims
Therefore, to reduce sedentary behavior, the implications and effects of organizational culture on sedentary behavior interventions merit systematic and thorough investigation. We found no reviews that specifically addressed this important topic. To fill this critical gap in our knowledge base, the objectives of this paper were to: (1) identify and describe the current literature related to organizational culture and sitting behavior at work; (2) identify gaps in the knowledge base; and (3) provide recommendations to advance the field related to reducing sedentary behavior among office-based workers.
Materials and Methods
Study Design
All study designs were included and evaluated. The designs included randomized controlled trials (RCTs), cross-over RCTs, cluster-randomized controlled trials (cluster-RCTs), quasi-RCTs of interventions, non-randomized controlled trials, focus groups, and structured interviews.
Participants, Interventions, Comparators
The participants were any employees at the workplace. The interventions were designed to reduce sitting at work. The comparators were employees at the workplace who did not participate in the intervention.
Systematic Review Protocol
The systematic review protocol involved independent reviews of identified articles by study investigators. Then consensus was achieved as to conformity with the inclusion and exclusion criteria. There were no disagreements that required a third party to adjudicate.
Search Strategy
The two study flow diagrams represent the major search strategy with four databases (PubMed, Medline, Academic Search Complete, and Google Scholar) and three key search terms—workplace health, organizational culture, and sedentary behavior. The inclusion criteria were primary data collection for organizational culture and sedentary behavior in the workplace. The exclusion criteria were non-English language study; theses or dissertations (not published in peer-reviewed journals); unable to obtain publication; and no primary data related to organizational culture and sedentary behavior in the workplace. Time frame was not limited given the novelty of research in this area. In addition to the main search strategy presented in Study Flow Diagrams One and Two (Figures 1, 2), we conducted additional searches using combinations of key search terms from the following Medical Subject Headings (MeSH) terms: workplace culture, workplace, worksite, sitting, occupational sitting, and sedentary behavior. Furthermore, we reviewed the references of relevant articles such as review papers. We found no other appropriate references to add to the articles retrieved from the main search strategy.
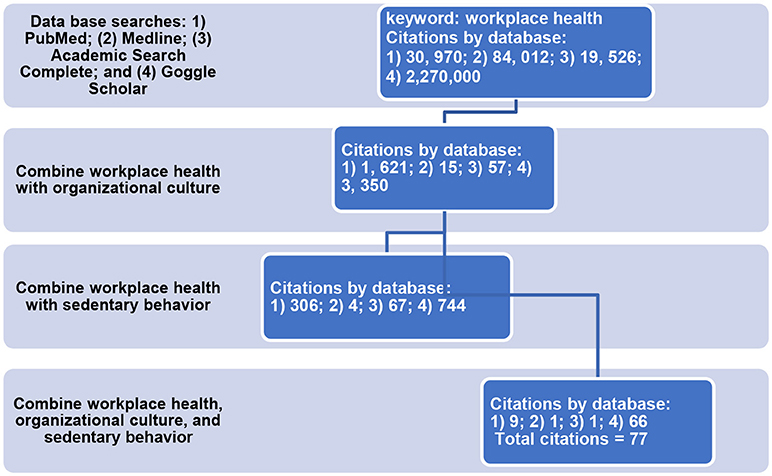
Figure 1. Study flow diagram one: sequence of database searches. Keywords: workplace health, organizational culture, and sedentary behavior. Inclusion criteria for systematic review: primary data collection from employees or employers; data related to organizational culture and sedentary behavior. For Medline, we used the search term workplace health promotion instead of workplace health to meet the accepted terms for the database.
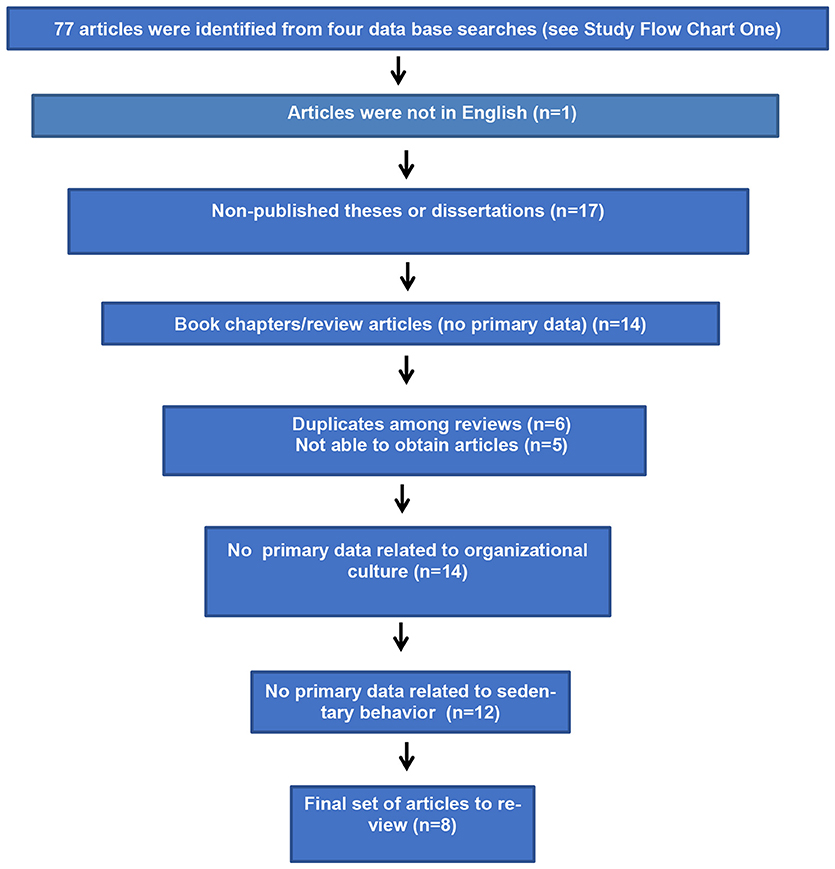
Figure 2. Study flow diagram two: apply inclusion and exclusion criteria to 77 articles identified from four data searches (see Flow Chart One). Inclusion criteria for systematic review: primary data from employees or employers and primary data related to organizational culture and sedentary behavior. Exclusion criteria for systematic review: non-English language, thesis or dissertation (not published in peer-reviewed journal); unable to obtain publication; no primary data related to organizational culture and sedentary behavior.
Data Sources and Data Extraction
The data sources were: PubMed, Medline, Academic Search Complete, and Google Scholar. For each article, the data extracted included citation, sample, objective, intervention, assessments of organizational culture and sitting time, findings, and implications (Table 1). Each article was rated for risk of bias by population, intervention, comparator, outcomes, and study design (PICOS) analysis. The classification of each article was either: high-, moderate-, or low-quality evidence.
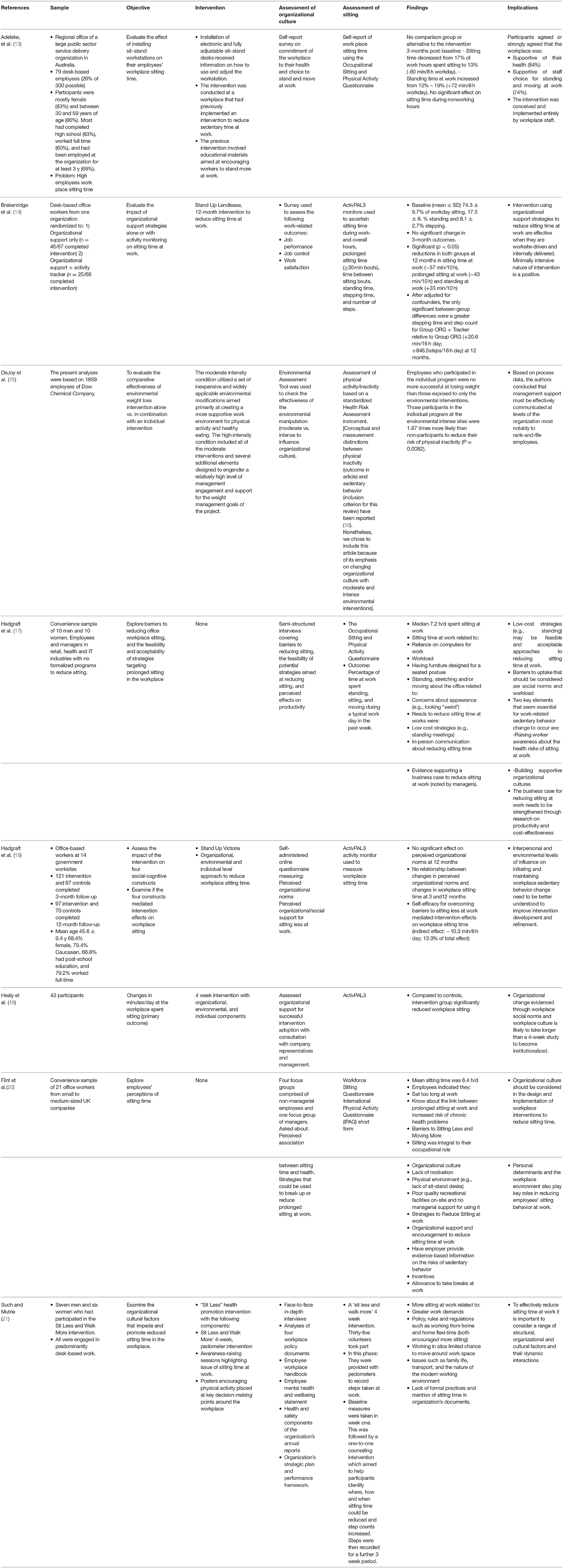
Table 1. Organizational culture and sitting at the workplace: literature review.
Data Analysis
From the main search strategy, two study flow diagrams show that we began with thousands of citations, applied all three keywords, and identified 77 potentially relevant articles. The inclusion and exclusion criteria were applied to the 77 articles and 8 relevant publications were identified to include in the data analysis. We reviewed eight articles and the data extracted were: citation, sample, objective, intervention, assessments of organizational culture and sitting time, findings, and implications (Table 1). Then, each article was rated based on high-, moderate-, or low-quality evidence and described in the text of the results section.
Results
Provide a Flow Diagram of the Studies Retrieved for the Review
Study flow charts one and two represent the main search strategy from beginning to end. We started with thousands of citations and applied the inclusion and exclusion criteria which resulted in 77 articles; the final set included 8 articles.
Study Selection and Characteristics
The eight articles were summarized and evaluated based on population, intervention, comparator, outcomes, and study design (PICOS). High-quality evidence is characterized by studies with large sample sizes that are racially and ethnically diverse. An appropriate comparison group is identified. The study designs are RCTs, cross-over RCTs, cluster-randomized controlled trials (cluster-RCTs), and quasi-RCTs of interventions. The studies with high-quality evidence have low risk of bias. Low-quality evidence is characterized by studies with small sample sizes, no comparison group, demographically homogeneous participants, no or flawed intervention, and weak study design (e.g., pre- and post-single sample). The studies with low-quality evidence have high risk of bias. One purpose of focus groups is to generate hypotheses for future studies. Nonetheless, from the perspective of the PICOS framework, focus group studies are low-quality evidence. Moderate-quality evidence is characterized by studies that do not meet the criteria for high quality evidence but are promising and superior to studies with low quality (e.g., non-randomized controlled trials). The studies with moderate-quality evidence have medium risk of bias.
High Quality Evidence
In a cluster-randomized controlled trial with 153 desk-based workers, organizational-support strategies designed to reduce sitting in office workers with and without an activity tracker were evaluated (14). The authors assessed the short-term (3 months) and long-term (12 months) effectiveness of the intervention. The organizational-support strategies consisted of a wellness champion choosing from a menu of choices and selecting options appropriate for each organization. The options included: an information booklet about sitting and health implications; five nightly emails with activity-promoting tips and images of active participants; participation of senior executives was communicated to employees; the workplace champion presented at least 10 workplace presentations, and informal discussions with managers continued throughout the study. The average time spent sitting during work and overall were the primary outcomes. A secondary outcome was the number of steps per day.
With or without an activity tracker, organizational-support strategies showed improvements in sitting and standing. At 3 months, both interventions resulted in small and non-significant differences in sitting time and activity outcomes. At 12 months, both interventions resulted in statistically significant reductions in sitting time. The activity tracker condition showed increases in overall stepping time and step counts. Improvements were most evident at 12 months. The authors concluded that embedding changes in an organization is not a rapid process and it takes time to generate organizational culture change. Furthermore, behavioral improvements can occur without environmental modifications. This study was the first to report the impact of organizational support and activity tracker strategies on office workers' sitting time (14).
In another study, building on a multi-component trial that successfully reduced sitting in the workplace, the purpose was to provide insights into the mechanisms (mediators) to explain the results (i.e., reduced sitting) by examining short- and long-term mediation effects (18). Two hundred and thirty-one office-based workers were randomly assigned to intervention and control conditions by worksite. Workplace sitting was measured with the activPAL3 device. Participants reported spending 7.2 h (median) of their working hours sitting. The intervention was composed of organizational, environmental, and individual level components. The organizational level intervention was tailored management emails. To evaluate perceived organizational norms, levels of agreement were assessed to the statement; “My workplace is committed to supporting staff choices to stand or move more at work.” Based on mediation analysis, social norms around appropriate workplace behavior and workload pressures were perceived as barriers. Furthermore, the intervention significantly improved perceived organizational norms at 3 months but not at 6 months. The authors noted that the organizational level intervention designed to improve workplace culture was discontinued at 3 months. It was recommended that future workplace interventions invest in longer organizational cultural change strategies to sustain perceived cultural changes related to moving more and sitting less (18).
A quasi-experimental research design, with 1,859 employees, was used to compare the outcomes for two levels of environmental interventions and for participants who did or did not simultaneously self-select into an individually focused weight loss intervention (15). In essence, the comparative effectiveness of environmental weight loss interventions alone vs. in combination with an individual intervention was evaluated. The outcomes of interest were weight loss and physical activity/inactivity. The goal for the moderate environmental interventions was to utilize a set of simple, low cost interventions that would be easy to implement in a wide variety of workplaces and that could be sustainable over time. The intense environmental condition was designed to engage leadership and create a more positive and supportive climate for health. The individually focused program consisted of setting a weight-related goal and reporting baseline weight at sign up and providing self-reported weight information three times after signup at 3-month intervals. The results were that employees who participated in the individual intervention were no more successful at losing weight than those exposed to only the environmental interventions. However, those who participated in the individual program at the intense environmental intervention sites were 1.87 times more likely than non-participants to reduce their risk of physical inactivity (P = 0.0082).
The moderate and intense environmental conditions differed significantly across time in terms of supports for nutrition and weight management and general organizational supports; the environmental manipulation was effective with some fading during year 2 of the intervention. However, the authors noted that leadership engagement failed to impact frontline employees at a subjective or perceptual level. The recommendation from this study was that management support must be effectively communicated so that visible actions and tangible changes that impact the daily work life of rank-and-file employees can be observed. Environmental interventions may be most effective when they are publicized through multiple channels and accompanied by policy actions that reinforce the desired behaviors. [An explanatory note about the inclusion of this article in our review; conceptual and measurement distinctions between physical inactivity (outcome in article) and sedentary behavior (inclusion criterion for this review) have been reported (16). Nonetheless, we included this article because of its emphasis on changing organizational culture with moderate and intense environmental interventions].
Moderate-Quality Evidence
During a 4-week, two arm, non-randomized controlled trial, an intervention with organizational, environmental, and individual elements was implemented (19). The primary outcome of interest was workplace sitting time. There were 43 participants. The organizational support included emails providing “standing tip of the week” and a workshop focusing on the health consequences of excessive sitting. Organizational support strategies were adjusted based on consultation with organization's representatives and management. Environmental strategies were the installation of dual display sit-stand workstations. The individual interventions were an initial 30-min face-to-face consultation between a health coach and each intervention participant followed by three telephone calls (one per week). The sessions emphasized behavior change strategies such as goal setting, self-monitoring, and problem solving. In comparison to the control group, the intervention group significantly reduced workplace sitting time; workplace sitting was almost exclusively replaced by standing. Because the intervention period was 4 weeks, the authors reported that most of the change was attributable to environmental and individual strategies; however, it was acknowledged that organizational support was essential. The authors concluded that organizational strategies to change workplace social norms and workplace culture will take longer that a 4-week intervention to become institutionalized (19).
Low Quality Evidence (i.e., Convenience Sample, Focus Group, and Interview Studies)
A study examined the impact of installing sit–stand workstations on their employees' sitting time at work (13). The intervention was conducted with a convenience sample of 79 desk-based employees working at a large, service delivery organization in Australia. Employee perceptions of organizational culture and sitting time at work were assessed before and after the employees were given sit-stand work stations. No comparison group was used. Results were positive and indicated that the intervention decreased sitting time at work by an average of 80 min/8 h workday and increased standing time by an average of 72 min/8 h workday. In addition, employees believed that the workplace was supportive of their health (i.e., organizational culture) and the employees had a choice of standing and moving at work. This study was deemed low-quality evidence because it had many limitations related to its study design (e.g., small percentage of staff participated) and no comparison group.
In another research project, the volunteers for a qualitative sub-study were part of a larger study that included pedometers to record steps and one-to-one counseling sessions to reduce sitting and increase step counts (21). Based on a model of organizational culture, qualitative, face-to-face, in-depth interviews were conducted with 13 volunteers. The model of organizational culture included the constructs of values and belief system, strategy, structure, and operations affected by the external environment. The findings from the qualitative study were that the “inevitability of time pressure” and the work ethic to “get things done” undermined the motivation to reduce sedentary behavior. It was recommended that the organization appoint a “champion for sitting less.” Basically, the norm of sedentary time was unchallenged by the work hierarchy (21). The authors concluded that to change sitting as a norm, a whole systems approach is needed that includes workplace policy and norm-changing interventions. Co-produced interventions (employees, employers, management and scientists working in partnership) can challenge sedentary behavior at different and interconnected organizational levels.
In another qualitative study, with a convenience sample of 21 employees, self-reported occupational sitting time was 6.4 h (20). The purpose of the five focus groups was to explore perceptions of health risks associated with prolonged sitting and potential strategies to reduce sitting at work. Four focus groups consisted of non-managerial employees and one focus group was exclusively managers. The majority of participants had experienced negative symptoms associated with sitting at work including neck and back pain, poor posture, weight gain, and reduced concentration. In addition to personal determinants, employees highlighted the key role of workplace environment and organizational culture in reducing sitting behavior at the workplace. One of the barriers to reducing sitting time was the chargeable time culture; everything needs to contribute to the organization's productivity. One respondent cited “Sit at your desk for a lunch break and eat while working.” To change culture, it was recommended to have corporate endorsement of well-being champions and communication at all levels within the organization (20).
In a different qualitative study (semi-structured interviews), with a convenience sample of 20 participants from three organizations, the objective was to assess perceptions about reducing workplace sitting (17). None of the workplaces had implemented any formal interventions to reduce prolonged sitting time. The purpose of the study was to identify barriers to reduce sitting and perceptions about a range of sitting reduction strategies. On average, participants reported sitting at work 7.2 h per day (minimum was 4.0 h and maximum was 9.5 h). The three prominent barriers to reduce workplace sitting were: the nature of work, organizational social norms, and office furniture and layout. Organizational social norms were perceptions of what was considered normal as workplace behavior. Related to organizational influences, the respondents were asked: “What level of priority do you think your organization places on reducing sitting time at work.” The authors concluded that building a supportive organizational culture and raising awareness of the adverse health effects of prolonged sitting may be important to improve individual level and other strategies for change (17).
Synthesized Findings
In summary, the empirical database is limited; no definitive conclusions are presented. The majority of the studies were focus groups and qualitative interviews with data to generate hypotheses for interventions. Basically, more intervention studies are needed. Our preliminary assessments to be confirmed with additional studies are that workplace interventions to reduce sitting time: (a) can be low-cost (e.g., stand rather than sit at meetings); (b) should include efforts to raise awareness regarding the negative health effects of prolonged sitting at work; (c) need to target multiple levels (e.g., employees, employers, individual, social, environmental, and organizational); (d) need to have strong and clear components that focus on organizational culture and; (e) should make a business case (e.g., increased productivity) related to reduced sitting at work.
Risk of Bias
In a recent Cochrane review (22), risk of bias was assessed in the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome data, validity of outcome measure, and baseline comparability/imbalance for age, gender, and occupation of groups. Each potential source of bias was graded as high, low, or unclear with justification for the judgments. These eight domains have marginal relevance and applicability to a database with eight studies. There were three high-quality evidence papers; one moderate-quality evidence paper; and four low-quality evidence papers. The low-quality evidence papers were primarily focus group studies or semi-structured interviews. Given the limited database and predominance of qualitative studies, the risk of bias is unclear.
Discussion
Summary of Main Findings
As noted in the Introduction section, definitions of organizational culture are essential to workplace health promotion. A clear definition is needed for the field to move forward. A pioneer in the study of organizational culture, Schein (23) in his recent book, presents a dynamic definition of organizational culture.
“The culture of a group can be defined as the accumulated shared learning of that group as it solves its problems of external adaptation and internal integration; which has worked well-enough to be considered valid and, therefore, to be taught to new members as the correct way to perceive, think, feel, and behave in relation to those problems. This accumulated learning is a pattern or system of beliefs, values, and behavioral norms that come to be taken for granted as basic assumptions and eventually drop out of awareness” (page 6) (23).
What is noteworthy about this definition from the perspective of researchers and practitioners is that there are distinct levels of observability for learned patterns of beliefs, values, assumptions, and behavioral norms. Of the constructs noted above, behavioral norms are the most visible and represent an expression and manifestation of assumptions, values, and beliefs.
Given this definition, the primary conclusion from this review is that literature documenting the role of organizational culture on sedentary behaviors at work is sparse (i.e., only eight studies) and fairly recent (i.e., six of eight papers published since 2016). The outcomes, however, from the available studies suggest that efforts to reduce sitting time at work are promising when organizational culture is considered. Further research in this area is warranted. Therefore, we present 11 recommendations to guide and advance the field.
Recommendations
• Mechanisms, mediators, and processes that influence organizational culture include leadership, organization's mission statement, management and strategic communication, management behavior, employee autonomy/empowerment, coworker support, employee engagement, values, belief systems, environmental supports, policies, and practices (24). Similar to an earlier study (24), we recommend identifying what matters most for changing how employees think and feel about the organization's support for health and reducing sedentary behavior. The potential targets are policies, environmental supports, and clear and favorable upper- and mid-management communication.
• In a comprehensive review of the measurement of workplace culture, most instruments did not focus on workplace health culture (12). Instead, subscales related to the culture of health were identified. One exception is the Lifegain Wellness Culture Survey (also known as the Lifegain Health Culture Audit), which measures five core dimensions of culture—values, norms, touch points, peer support, and climate (11). The validity and reliability of this instrument have been measured in several studies (11). Instruments related to the overall culture of the organization include: The Organizational Culture Inventory, the Denison Organizational Culture Survey, and the Organizational Culture Profile (25). The challenge of measuring organizational culture has been noted by several authors (25). Most quantitative measures of culture capture the espoused values and/or behavioral norms in organizations and not the full richness of the construct—including myths and stories. A focus on intangibles related to organizational culture makes a complete reliance on quantitative approaches unsatisfactory, emphasis should be placed on qualitative assessments (25).
• Organizational culture should be studied in conjunction with organizational climate. Climate and culture can be mutually supportive. Climate is more sensitive to workgroup norms and highly variable across an organization, whereas culture is more enduring and stable across the entire organization (12). Organizational climate is defined as the mood or unique “personality” of a workplace (26). Organizational climate, also, has been defined as the shared perceptions of and the meaning attached to the policies, practices, and procedures employees experience and the behaviors they observe getting rewarded and that are supported and expected (25). On the other hand, as noted earlier, organizational culture is defined as the shared basic assumptions, values, and beliefs that characterize a setting and are taught to newcomers as the proper way to think and feel and are communicated by the myths and stories people tell about how the organization came to be the way it is (25). In this paper, we focused on organizational culture because it is more enduring and stable than organizational climate. For example, a charismatic leader affects the organizational climate. When a charismatic leader departs a company the organizational climate can change dramatically; however, the organizational culture remains basically intact. Nonetheless, the relationships between climate and culture can be mutually reinforcing and both merit empirical analysis.
• Organizational culture should be studied as potential antecedents, consequences, moderators, and mediators for interventions designed to reduce sedentary behavior. In previous research, organizational culture was studied as a contextual variable that moderated relationships between and among other constructs (25). For example, can dimensions of organizational culture weaken or strengthen the relationship between organizational justice and leader-member exchanges (25)?
• In understanding culture, the socialization experiences of newcomers can be critical because typically, newcomers see everything with fewer preconceptions and fresh perspectives. If a newcomer affiliates him/herself with individuals who embody the positive values of the organizations, s/he will embrace the culture quickly. In the context of sedentary behavior, regular displays of reducing sedentary behavior and an active workplace culture will facilitate positive behavioral changes. However, the reverse is also true. Zappos is a prime and clear example of hiring according to cultural standards and insuring that newcomers embrace the culture. This company, which specializes in shoes (online sales), hires employees based on their potential to fit into the organizational culture (referred to as cultural fit interviews). Consistent with this mission, new hires are offered $2,000 to quit after 1 week if they perceive the job or company culture is not for them. The bottom line is that Zappos values its culture and does not want anyone who is unhappy or dissatisfied to disturb and disrupt the organizational culture. The objective is to have the entire corporation and brand supported by a loyal and dedicated workforce who provides great customer service (https://www.entrepreneur.com/article/249174).
• More research studying the effectiveness of integrating and combining individual approaches with cultural components to reduce sedentary behavior is needed. Thus, should organizations focus both on top-down and bottom-up approaches to create the needed paradigm shift to move behavior from one norm to another? Policy and environmental supports combined with individual level interventions need further research to understand what shifts organizational culture.
• Related to recommendation #6, what elements of an intervention are needed to embed the processes and mechanisms to change an organizational culture to a “culture of health?” Well-designed investigations are needed to determine what proportion of employee health improvement is due to cultural support (12). If shown to be reliable and valid, an assessment can be used by organizations to document improvements in the organization's culture of health. This information is valuable because it can document whether policy and environmental changes are sufficient to influence organizational culture in a meaningful way. In addition, such a tool could assist organizations in evaluating the impact of organizational culture on employee health and outcomes (12). More research in this area can be impactful.
• To what extent is workplace culture influenced by societal, cultural, or national norms? An international group of experts convened to provide guidance for employers to promote the avoidance of prolonged periods of sedentary work (27). The recommendations are: for those occupations which are predominantly desk-based, workers should aim to initially progress toward accumulating 2 h per day of standing and light activity (light walking) during working hours, eventually progressing to a total accumulation of 4 h per day (prorated to part-time hours). To achieve these recommendations, seated-based work should be regularly broken up with standing-based work, the use of sit–stand desks, or taking short active standing breaks (27). To what extent these recent guidelines are known and embraced by organizations including managers and employees has not been documented. Nonetheless, societal norms can influence a workplace's organizational culture.
• To what extent is a “culture of health” influenced by life cycles of organizations? Are newer or more established (mature) organizations more likely to have a “culture of health” or a “wellness culture?” To what extent is a “culture of health” influenced by the profitability and/or organizational effectiveness of the company? The culture of health may depend on the bottom line. If a company is struggling or still fighting for survival, then health may not be a priority. If an organization is thriving, perhaps it has greater flexibility and can embrace healthy practice policies and a culture of health. More research is needed in this area.
• The prevalence of workplaces with “cultures of health” is unknown. Large organizations with established health promotion programs may be more likely to have some level of cultural support for health. Perhaps, in mid-size and small companies, the presence of workplace wellness efforts may be less common and information regarding the existence of supportive cultures more difficult to assess. On the other hand, smaller companies may be able to create and retain a culture of health more easily than large companies that have many more employees and greater organizational complexity. The size of an organization and workplace “culture of health” merits further study (12).
• Related to reducing sedentary behavior is promoting physical activity during the workday. There have been several reviews and empirical studies related to promoting physical activity during the work day (28–38). For example, research has documented that mid-management support is critical in determining whether employees can consistently participate in 15-min, group physical activity breaks during the work day (39, 40). The lessons learned from physical activity promotion during the workday can inform research on reducing sedentary behavior during the workday and organizational culture change.
Limitations
In this systematic review, an inclusion criterion was peer-reviewed published articles. We did not search sources of gray literature and unpublished studies and data; unpublished theses and dissertations were excluded. A limitation of this review is publication bias. In addition, we excluded articles published in languages other than English. Our review may be subject to language biases. Furthermore, studies with interventions that incorporated individual, environmental, and organizational elements were excluded unless specific measures of organizational or workplace culture were assessed. Some consideration of organizational or workplace culture had to be acknowledged. We found no similar reviews to compare our findings.
Conclusions
Prolonged sitting, aggregated from work and in leisure time, may significantly and independently increase the risk of cardiometabolic diseases and premature mortality (6–8). To reduce sedentary behavior at work, organizational culture merits careful analysis. Allen presented a metaphor that workplace or organizational culture creates fertile ground in which healthy lifestyles (the good seeds), can take root and flourish (11). The organizational culture can be strong or weak. Nevertheless, organizational culture influences the meaning of workplace behaviors as well as the adoption, implementation, and effectiveness of health promotion initiatives. In a national meeting of thirty-five of the most experienced practitioners and researchers in workplace health promotion (i.e., professional think tank), four research priorities were identified. Of the four top ranked research priorities, healthy organizational culture was ranked number one as a research priority (41). The experts in health promotion and wellness concluded that a health-oriented or wellness workplace culture permits and enables healthy lifestyle choices and significantly enhances long-term program success. In other words, a strong cultural foundation sustains health-promotion initiatives in contrast to a primary reliance on targeted individual intervention strategies.
For example, prior to the development of the intervention, a formative research study was conducted to reduce workplace sitting time using height-adjustable workstations (not focused on organizational culture; thus, ineligible for our literature review) (42). A systematic assessment was implemented to inform the development of the intervention. The guiding theoretical frameworks were: Theoretical Domains Framework, Community Readiness Model, and the Behavior Change Wheel (incorporating capability, opportunity, and motivation). The assessment included eight steps. The findings were that motivation to change behavior was low because of the dominant work culture of sitting. The authors acknowledged that their comprehensive and participatory approach to identify barriers and facilitators to reduce sitting time and their focus on individual behavior change that excluded organizational policies and practices were a major limitation of their approach (42).
Substantial and enduring health promotion improvements depend upon individual initiatives and organizational culture working in partnership (i.e., mutually supportive) (11). To create a favorable organizational culture, senior leadership commitment, front-line managers' engagement, “boots-on-the-ground” personnel mobilizing grassroots efforts, strong supportive policies, health-promoting environments, and highlighting employee health as an important business objective are recommended as essential elements to “building a culture of health” in a sustained way at the workplace.
In summary, a purpose of this systematic review was to add clarity and depth to the existing literature. Even though the findings are promising from a limited database, basic questions remain: What is the evidence that strategies to reduce workplace sitting (e.g., workplace champion and management communication) influence organizational culture? What is the time frame to observe changes in organizational culture? What is the evidence that changes in organizational culture from interventions contribute to behavior change in the workplace? As more rigorous research is conducted and evaluated to address these challenges, we will move closer to achieving our goal of reducing sedentary behavior at the workplace and improving the health of all employees.
Author Contributions
WT conceived of the study. RS, BD, RP, and DC contributed to the development and design of the study. WT and RS organized the literature review. WT and RS conducted the literature review and wrote the results section. WT wrote the first complete draft of the manuscript. RS, BD, RP, and DC revised sections of the manuscript. All authors contributed to manuscript revisions, read, and approved the submitted version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors gratefully acknowledge Karen L. Pepkin, MA, for her reviews and creation of Figure 2.
References
2. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary Behavior Research Network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
3. Kent K, Goetzel RZ, Roemer EC, Prasad A, Freundlich N. Promoting healthy workplaces by building cultures of health and applying strategic communications. J Occup Environ Med. (2016) 58:114–22. doi: 10.1097/JOM.0000000000000629
4. Goetzel RZ, Shechter D, Ozminkowski RJ, Marmet PF, Tabrizi MJ, Roemer EC. Promising practices in employer health and productivity management efforts: findings from a benchmarking study. J Occup Environ Med. (2007) 49:111–30. doi: 10.1097/JOM.0b013e31802ec6a3
5. U.S. Bureau of Labor Statistics. Average Hours per Day Spent in Selected Activities on Days Worked by Employment Status and Sex, 2016 Annual Averages (2016).
6. Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet (2016) 388:1302–10. doi: 10.1016/S0140-6736(16)30370-1
7. Gale J, Chau JY, Hardy LL, Mackey M, Johnson N, et al. Who is at risk of chronic disease? Associations between risk profiles of physical activity, sitting and cardio-metabolic disease in Australian adults. Aust N Z J Public Health (2017) 41:178–83. doi: 10.1111/1753-6405.12627
8. Rezende LFM, Sá TH, Mielke GI, Viscondi JYK, Rey-López JP, Garcia LMT. All-cause mortality attribuable to sitting time: analysis of 54 countries worldwide. Am J Prev Med. (2016) 51:253–63. doi: 10.1016/j.amepre.2016.01.022
9. Schein EH. (2010). Organizational Culture and Leadership. 4th ed. San Francisco, CA: Jossey-Bass.
10. Terry PE, Seaverson EL, Grossmeier J, Anderson DR. Association between nine quality components and superior worksite health management program results. J Occup Environ Med. (2008) 50:633–41. doi: 10.1097/JOM.0b013e31817e7c1c
11. Allen J. Transforming organizational cultures to support good health. In: O'Donnell MP, editor. Health Promotion in the Workplace. 5th Ed. Troy, MI: Art & Science of Health Promotion Institute (2017). p. 633–48.
12. Aldana SG, Anderson DR, Adams TB, Whitmer W, Ray M, Merrill RM, et al. A review of the knowledge base on healthy worksite culture. J Occup Env Med. (2012) 54:414–9. doi: 10.1097/JOM.0b013e31824be25f
13. Adeleke SO, Healy GN, Smith C, Goode AD, Clark BK. Effect of a workplace-driven sit–stand initiative on sitting time and work outcomes. Transl J ACSM (2017) 2:20–6. doi: 10.1016/j.amepre.2012.05.027
14. Brakenridge CL, Fjeldsoe BS, Young DC, Winkler EA, Dunstan DW, Straker LM, et al. Evaluating the effectiveness of organisational-level strategies with or without an activity tracker to reduce office workers' sitting time: a cluster-randomised trial. Int J Behav Nutr Phys Act. (2016) 13:115. doi: 10.1186/s12966-016-0441-3
15. DeJoy DM, Parker KM, Padilla HM, Wilson MG, Roemer EC, Goetzel RZ. Combining environmental and individual weight management interventions in a work setting results from the Dow Chemical Study. J Occup Environ Med. (2011) 53:245–52. doi: 10.1097/JOM.0b013e31820c9023
16. Pate RR, O'Neill JR, Lobelo F. The evolving definition of “Sedentary.” Exerc. Sport Sci. Rev. (2008) 36:173–8. doi: 10.1097/JES.0b013e3181877d1a
17. Hadgraft NT, Brakenridge CL, LaMontagne AD, Fjeldsoe BS, Lynch BM, Dunstan DW, et al. Feasibility and acceptability of reducing workplace sitting time: a qualitative study with Australian office workers. BMC Public Health (2016) 16:933. doi: 10.1186/s12889-016-3611-y
18. Hadgraft NT, Winkler EAH, Healy GN, Lynch BM, Neuhaus M, Eakin EG, et al. Intervening to reduce workplace sitting: mediating role of social-cognitive constructs during a cluster randomised controlled trial. Int J Behav Nutr Phys Act. 14:27 (2017) doi: 10.1186/s12966-017-0483-1
19. Healy GN, Eakin EG, Neville Owen N, Winkler EA, Glen Wiesner G, et al. Reducing sitting time in office workers: short-term efficacy of a multicomponent intervention. Prev Med. (2013) 57:43–8. doi: 10.1016/j.ypmed.2013.04.004
20. Flint SW, Crank H, Tew G, Till S. “It's not an obvious issue is it?” Office-based employees' perceptions of prolonged sitting at work: a qualitative study. JOEM (2017) 59:1161–5. doi: 10.1097/JOM.0000000000001130
21. Such E, Mutrie N. Using organisational cultural theory to understand workplace interventions to reduce sedentary time. Int J Health Promot. (2017) 55:18–29. doi: 10.1080/14635240.2016.1196382
22. Shrestha N, Verbeek JH, Ijaz S, Hermans V. Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev. (2018) 6:CD010912. doi: 10.1002/14651858.CD010912.pub4
23. Schein EH. Organizational Culture and Leadership. 5th ed. Hoboken, NJ: John Wiley & Sons, Inc. (2017).
24. Payne J, Cluff L, Lang J, Matson-Koffman D, Morgan-Lopez A. Elements of a workplace culture of health, perceived organizational support for health, and lifestyle risk. Am J Health Prom. (2018) 32:1555–67. doi: 10.1177/0890117118758235
25. Schneider B, Ehrhart MG, Macey WH. Organizational climate and culture. Annu Rev Psychol. (2013) 64:361–88. doi: 10.1146/annurev-psych-113011-143809
26. Steckler A, Goodman RM, Kegler MC. Mobilizing organizations for health enhance-ment: theories of organizational change. In: Glanz K, Rimer BK, Lewis FM, editors. Health Behavior and Health Education. San Francisco, CA: Jossey-Bass (2002). p. 335–60.
27. Buckley JP, Hedge A, Yates T, Copeland RJ, Loosemore M, Hamer M, et al. The sedentary office: an expert statement on the growing case for change towards better health and productivity. Br J Sports Med. (2015) 49:1353. doi: 10.1136/bjsports-2015-094618
28. Barr-Anderson DJ, AuYoung M, Whitt-Glover MC, Glenn BA, Yancey AK. Integration of short bouts of physical activity into organizational routine: a systematic review of the literature. Am J Preve Med. (2011) 40:76–93. doi: 10.1016/j.amepre.2010.09.033
29. Crawford PB, Gosliner W, Strode P, Samuels SE, Burnett C, Craypo L, et al. Walking the talk: fit WIC wellness programs improve self-efficacy in pediatric obesity prevention counseling. Am J Public Health (2004) 94:1480–5. doi: 10.2105/AJPH.94.9.1480
30. Dishman RK, DeJoy DM, Wilson MG, Vandenberg RJ. Move to improve: a randomized workplace trial to increase physical activity. Am J Prev Med. (2009) 36:133–41. doi: 10.1016/j.amepre.2008.09.038
31. Dishman RK, Vandenberg RJ, Motl RW, Wilson MG, DeJoy DM. Dose relations between goal setting, theory-based correlates of goal setting and increases in physical activity during a workplace trial. Health Educ Res. (2010) 25:620–31. doi: 10.1093/her/cyp042
32. Galinsky T, Swanson N, Sauter S, Dunkin R, Hurrell J, Schleifer L. Supplementary breaks and stretching exercises for data entry operators: a follow-up field study. Am J Ind Med. (2007) 50:519–27. doi: 10.1002/ajim.20472
33. Gilson ND, Puig-Ribera A, McKenna J, Brown WJ, Burton NW, Cooke CB. Do walking strategies to increase physical activity reduce reported sitting in workplaces: a randomized control trial. Int J Behav Nutr Phys Act. (2009) 6:43. doi: 10.1186/1479-5868-6-43
34. Taylor WC. Transforming work breaks to promote health. Am J Prev Med. (2005) 29:461–465. doi: 10.1016/j.amepre.2005.08.040
35. Taylor WC. Booster Breaks: an easy-to-implement workplace policy designed to improve employee health, increase productivity, and lower healthcare costs. J Workplace Behav Health (2011) 26:70–84. doi: 10.1080/15555240.2011.540991
36. Taylor WC, Shegog R, Chen V, Rempel DM, Baun MP, Bush CL, et al. The Booster Break program: description and feasibility test of a worksite physical activity daily practice. Work (2010) 37:433–443. doi: 10.3233/WOR-2010-1097
37. Taylor WC, Paxton RJ, Shegog R, Coan SP, Dubin A, Page TF, et al. Impact of Booster Breaks and computer prompts on physical activity and sedentary behavior among desk-based workers: a cluster-randomized controlled trial. Prev Chronic Dis. (2016) 13:160231. doi: 10.5888/pcd13.160231
38. Yancey AK, McCarthy WJ, Taylor WC, Merlo A, Gewa C, Weber MD, et al. The Los Angeles Lift Off: a sociocultural environmental change intervention to integrate physical activity into the workplace. Prev Med. (2004) 38:848–56. doi: 10.1016/j.ypmed.2003.12.019
39. Taylor WC, King KE, Shegog R, Paxton RJ, Evans-Hudnall G, Rempel DM, et al. Booster Breaks in the workplace: participants' perspectives on health-promoting work breaks. Health Educ Res. (2013) 28:414–25. doi: 10.1093/her/cyt001
40. Taylor WC, Horan A, Pinion C, Liehr P. Evaluation of Booster Breaks in the workplace. J Occup Environ Med. (2014) 56:529–34. doi: 10.1097/JOM.0000000000000144
41. Terry PE. The mutualism of culture and engagement. Am J Health Promot. (2012) 26:1–12. doi: 10.4278/ajhp.26.6.tahp
Keywords: organizational culture, sit less, workplace intervention, sitting time, sedentary behavior, prolonged sitting, workplace culture, culture of health
Citation: Taylor WC, Suminski RR, Das BM, Paxton RJ and Craig DW (2018) Organizational Culture and Implications for Workplace Interventions to Reduce Sitting Time Among Office-Based Workers: A Systematic Review. Front. Public Health 6:263. doi: 10.3389/fpubh.2018.00263
Received: 09 May 2018; Accepted: 24 August 2018;
Published: 24 September 2018.
Edited by:
Frederic Dutheil, Centre Hospitalier Universitaire de Clermont-Ferrand, FranceReviewed by:
Siti Munira Yasin, Universiti Teknologi MARA, MalaysiaSok King Ong, Universiti Brunei Darussalam, Brunei
Copyright © 2018 Taylor, Suminski, Das, Paxton and Craig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wendell C. Taylor, d2VuZGVsbC5jLnRheWxvckB1dGgudG1jLmVkdQ==