
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 14 April 2025
Sec. Public Mental Health
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1569709
This article is part of the Research TopicThe Intersection of Psychology, Healthy Behaviors, and its OutcomesView all 85 articles
 Zhengyang Mei1
Zhengyang Mei1 Chenyi Cai1
Chenyi Cai1 Tingfeng Wang2
Tingfeng Wang2 Yuanzhuo Zhang1
Yuanzhuo Zhang1 Wen Zhao3
Wen Zhao3 Chifong Lam4
Chifong Lam4 Shulai Luo1
Shulai Luo1 Yu Shi1
Yu Shi1 Shi Luo1*
Shi Luo1*Objective: This systematic review and meta-analysis aimed to evaluate the potential multidomain benefits of mind-body therapies (MBTs) for behavioral and psychological symptoms of dementia (BPSD) in older people with dementia (OPWD).
Methods: Relevant randomized controlled trials (RCTs) were identified using electronic databases and manual searches. Two independent researchers evaluated the risk of bias in the included trials using the Revised Cochrane Risk-of-Bias tool for randomized trials. A standardized mean difference (SMD) with a 95% confidence interval (CI) was used to combine effect sizes.
Results: This review included 35 RCTs comprising 4,043 patients, of whom 24 were included in the meta-analyses. MBTs effectively improved BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01), anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02), and depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02), with no significant improvements observed in agitation (SMD = -0.09; 95% CI -0.25 to 0.07; p = 0.27) among patients with dementia. The certainty of evidence across the outcomes ranged from low to very low, based on the Grading of Recommendations, Assessment, Development, and Evaluations ratings.
Conclusion: Effective nursing for patients with dementia is vital, as they are undergoing a major transition in their physical and mental health. In clinical practice, healthcare and social care therapists should develop personalized intervention programs based on patient individual differences and the actual dose-response relationship, which will help maximize the clinical benefits of non-pharmacological treatments in the context of limited medical resources. More high-quality RCTs could be conducted to compare the differential efficacy of non-pharmacological treatments on various aspects of BPSD in OPWD to provide a better evidence base to guide individual care and policy guidance.
Systematic review registration: PROSPERO, identifier CRD42024559809.
Dementia is a progressive cognitive disorder that impairs daily functioning and is a primary contributor to dependency, disability, and death (1, 2). It is characterized by cognitive decline, deteriorating functional status, and worsening of neuropsychiatric symptoms (3). Currently, over 50 million individuals worldwide are affected by dementia, and projections indicate this figure could rise to 131 million by 2050 (3, 4). Moreover, the overall prevalence of dementia, from all causes, stands at 7.0%, with its rate of occurrence increasing sharply with age for both men and women (5), suggesting the growing public health challenge posed by dementia as the global population continues to age.
Old age is not only a critical stage for changes in physical and mental health but also a vulnerable period for the development of dementia. During this period, older people are often exposed to multiple risk factors for developing dementia, which are classified as immutable (age, sex, ethnicity, etc.) or potentially modifiable (diabetes, smoking, social isolation, physical inactivity, etc.) (6, 7). Moreover, compelling evidence suggests that dementia is prevalent among older people and may increase their susceptibility to physical and mental health problems, including cognitive impairment (8), suicidal behavior (9), epilepsy (10), disability (11), anxiety (12), and depression (13).
Dementia can be diagnosed based on medical history, cognitive and physical examination, laboratory testing, and brain imaging (3). As dementia is a progressive, incurable illness, several medications have been developed to help older people with dementia (OPWD) alleviate the physical and mental discomfort, including donepezil, cholinesterase inhibitors, memantine, and statins (14, 15). However, prolonged use of these drugs can result in numerous adverse outcomes. Specifically, the increasing use of cholinesterase inhibitors results in increased adverse drug reactions, such as cardiovascular and gastrointestinal adverse effects (16); treatment with antipsychotics in older people is associated with an increased risk of cardiovascular incidents and mortality (17). Therefore, no compelling evidence supports the use of these drugs in such patients (14).
In this regard, complementary therapies could offer potential solutions to these challenges. Mind-body therapies (MBTs), rooted in ancient Eastern practices, are a non-pharmacological approach that focuses on interactions between mind, body, and spirit to improve mental and physical well-being (18, 19). Compared with other medications, MBTs are characterized by low risk and high therapeutic benefits and can be alternatives or adjuvant approaches to conventional treatments (20, 21). Common MBTs include Mindfulness training, Tai Chi, Qigong, Baduanjin, Yoga, Pilates, and Music therapy, which have been proven to exert beneficial effects on the physical and mental health of OPWD (22–28). However, evidence regarding the efficacy of MBTs in managing the behavioral and psychological symptoms of dementia (BPSD) in OPWD is inconsistent, and some studies do not support the significant efficacy of MBTs in this area (29–33). This study aimed to evaluate the potential multidomain benefits of MBTs for BPSD in OPWD.
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 (34) and was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42024559809.
Using Medical Subject Headings in conjunction with Boolean and proximity operators, a search was conducted across six electronic databases: PubMed, Embase, Web of Science, Scopus, EBSCOhost, and APA PsycINFO, to identify relevant literature. The search covered the period from the inception of each database up to June 2024, and the strategy adhered to the Population, Intervention, Comparator, Outcome, and Study design framework. Details of the search strategy are outlined in Table 1, as per the PubMed database.
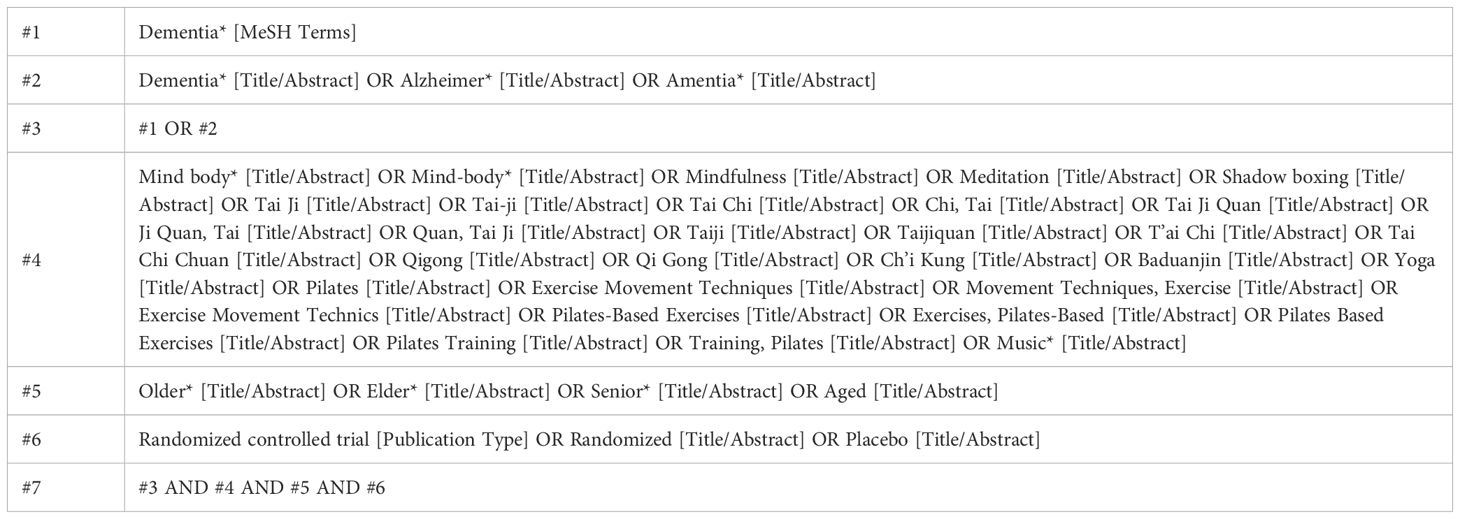
Table 1. PubMed search strategy.
The criteria for inclusion and exclusion of studies are presented in Table 2.
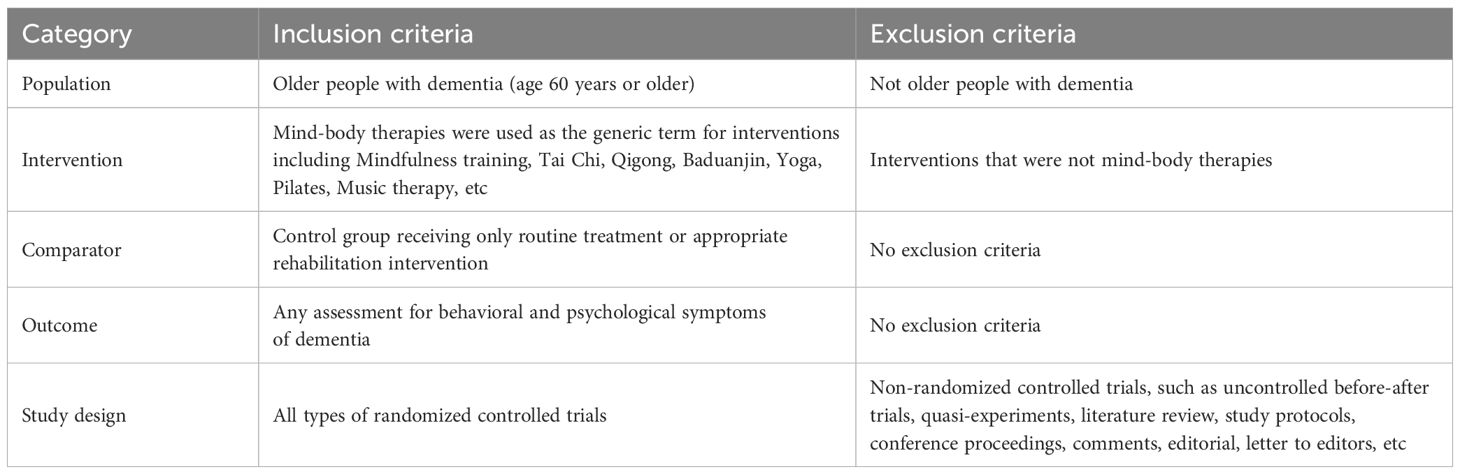
Table 2. Inclusion and exclusion criteria.
Two independent researchers, following predefined inclusion and exclusion criteria, utilized EndNote 20.6 for study selection. After duplicates were eliminated, the remaining references were independently reviewed by both researchers based on titles, abstracts, and full texts. Quality appraisal of the included trials was conducted using the Revised Cochrane risk-of-bias tool for randomized trials, with evaluation across five bias domains: (a) randomization process, (b) deviations from intended interventions, (c) missing outcome data, (d) measurement of the outcome, and (e) selection of the reported result (35). Disagreements during study selection and quality appraisal processes were resolved through consultation with a third author.
Two independent researchers used a data extraction form to gather relevant information from each included trial. The extracted data comprised the following: (1) basic details such as the first author, country, and year of publication; (2) participant characteristics, including mean age (with standard deviation), sample size, and the percentage of male participants; (3) diagnostic criteria for dementia; (4) intervention and control conditions; and (5) outcome and measure.
Given the differences in the measurement scales used for continuous variables (BPSD, anxiety, depression, and agitation) across the included trials, standardized mean differences (SMDs; Cohen’s d) with 95% confidence intervals (CIs) for each outcome were pooled and presented in forest plots using Stata software, version 18.0 (36). Statistical heterogeneity between trials was assessed using the chi-square test based on Q-test and I2 statistics, with a significance threshold of p-value < 0.10 (37). A sensitivity analysis was performed for each outcome using a stepwise elimination method to assess whether the pooled results were significantly affected by individual studies (36). Given the number of included trials, publication bias was examined by visual inspection of funnel plots and using Egger’s test (38, 39). The trim-and-fill method was used to assess the robustness of the findings in the presence of a publication bias (40). The certainty of evidence for each outcome was evaluated by two independent researchers using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) guidelines (41). All statistical analyses were performed using Stata 18.0.
Searches of electronic databases and additional sources yielded 2,120 results, of which 918 were duplicates. After the titles and abstracts of the remaining 1,202 records were screened, the full text of 441 articles was assessed, resulting in 35 eligible randomized controlled trials (RCTs) (42–76). After 11 additional trials with missing quantitative data were excluded, 24 were included in the meta-analyses. A PRISMA flow diagram of the literature search is presented in Figure 1.
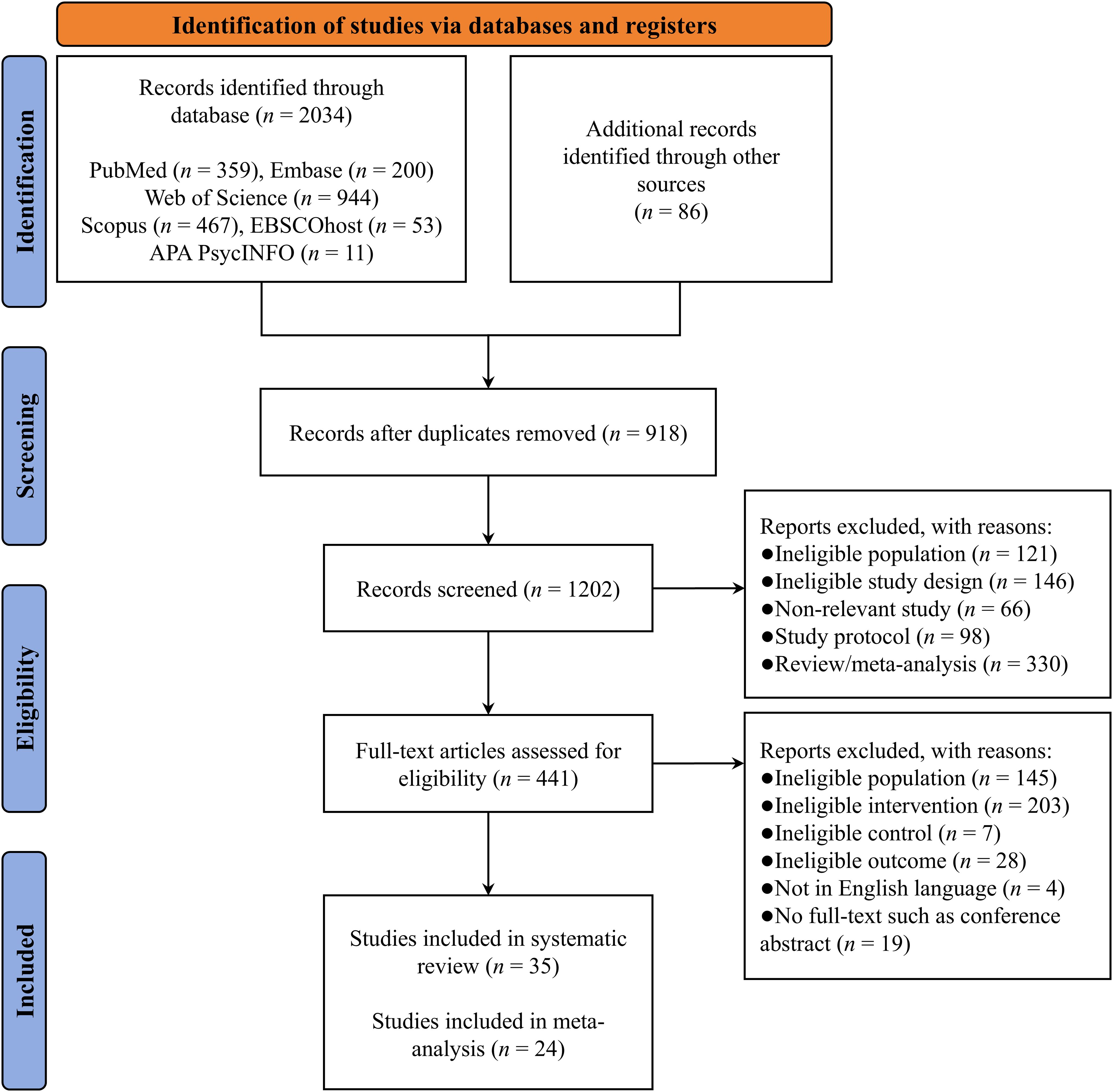
Figure 1. PRISMA flow diagram.
The 35 included trials (see Table 3) were published between 2006 and 2024 and were conducted in various countries, including China (13 trials), Italy (6 trials), the United States (4 trials), Australia (3 trials), Germany (2 trials), the Netherlands (2 trials), the United Kingdom (2 trials), Denmark, France, and Japan (one trial each). In total, 2,065 patients were assigned to the experimental group, with a mean age ranging from 76.78 to 86.56 years, while 1,978 patients were assigned to the control group, with a mean age of 76.80 to 87.20 years.
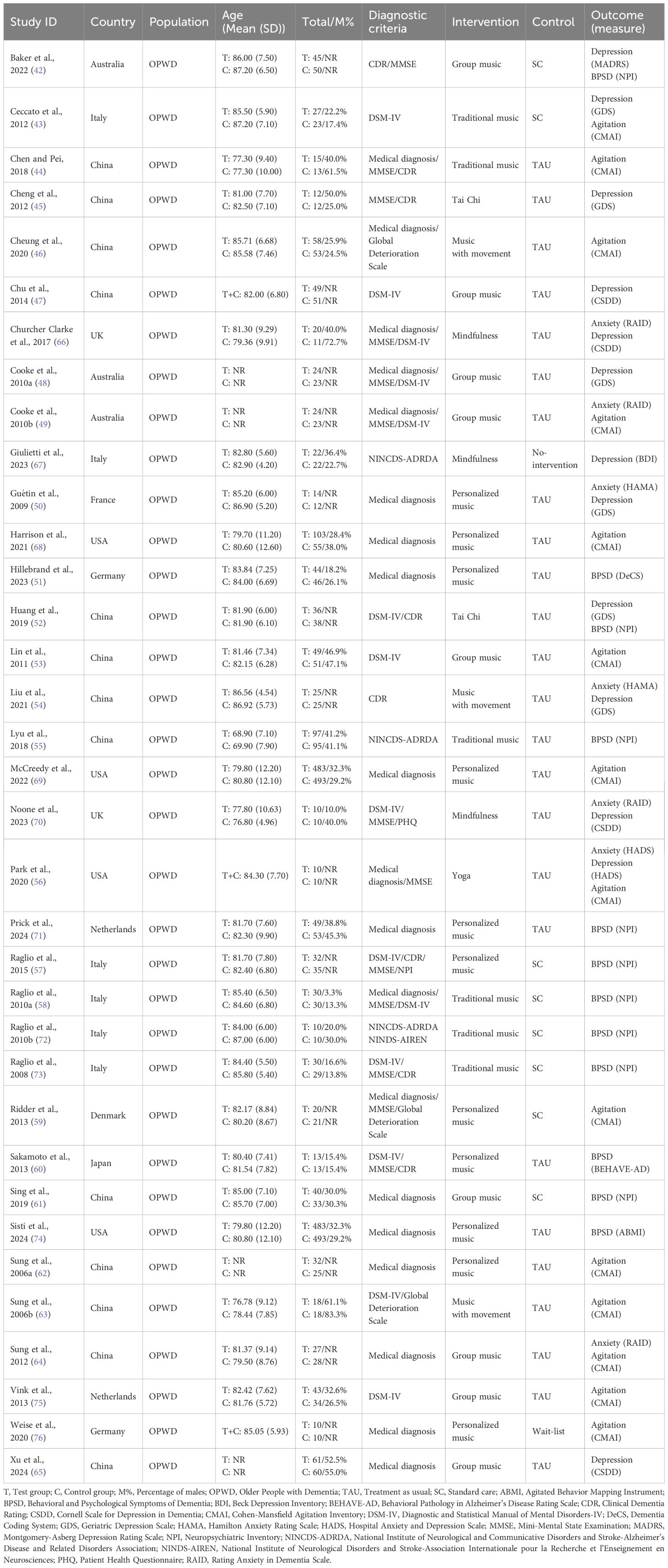
Table 3. Main characteristics of the included randomized controlled trials.
Among the 35 included trials, the diagnostic criteria for dementia primarily consisted of medical diagnosis, Diagnostic and Statistical Manual of Mental Disorders-IV, Mini-Mental State Examination, Clinical Dementia Rating, and the Global Deterioration Scale. The interventions included personalized music (11 trials), group music (9 trials), traditional music (6 trials), mindfulness (3 trials), music with movement (3 trials), Tai Chi (2 trials), and yoga (1 trial). The controls included treatment as usual (25 trials), standard care (8 trials), no-intervention (1 trial), and wait-list (1 trial). In addition, the deliverers of the intervention primarily included music therapists, musicians, nursing staff, psychotherapist, and trained facilitators, all of whom were qualified to be responsible for the implementation of the intervention.
The risk of bias ranged from some concern to high (see Figure 2, Table 4). The main flaws (≥10% high risk) across the included trials were the randomization process (94.3% low risk, 5.7% some concerns, and 0.0% high risk); deviations from intended interventions (45.7% low risk, 54.3% some concerns, and 0.0% high risk); missing outcome data (48.6% low risk, 48.6% some concerns, and 2.8% high risk); outcome measurement (97.2% low risk, 2.8% some concerns, and 0.0% high risk); and selection of the reported results (14.3% low risk, 77.1% some concerns, and 8.6% high risk).
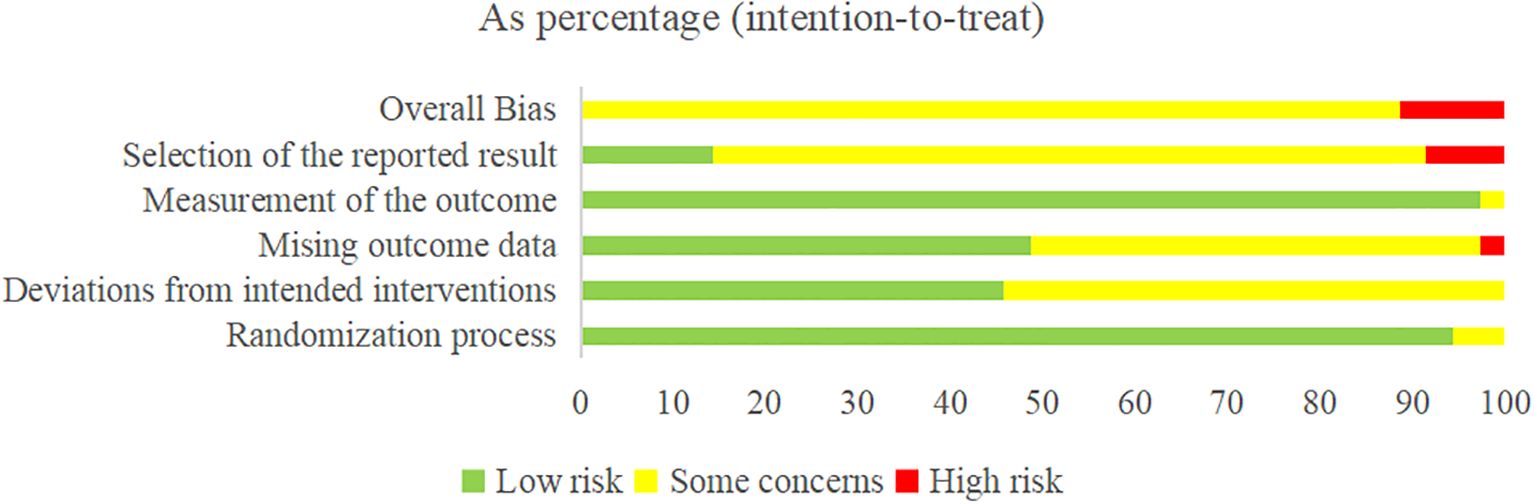
Figure 2. Risk-of-bias summary.
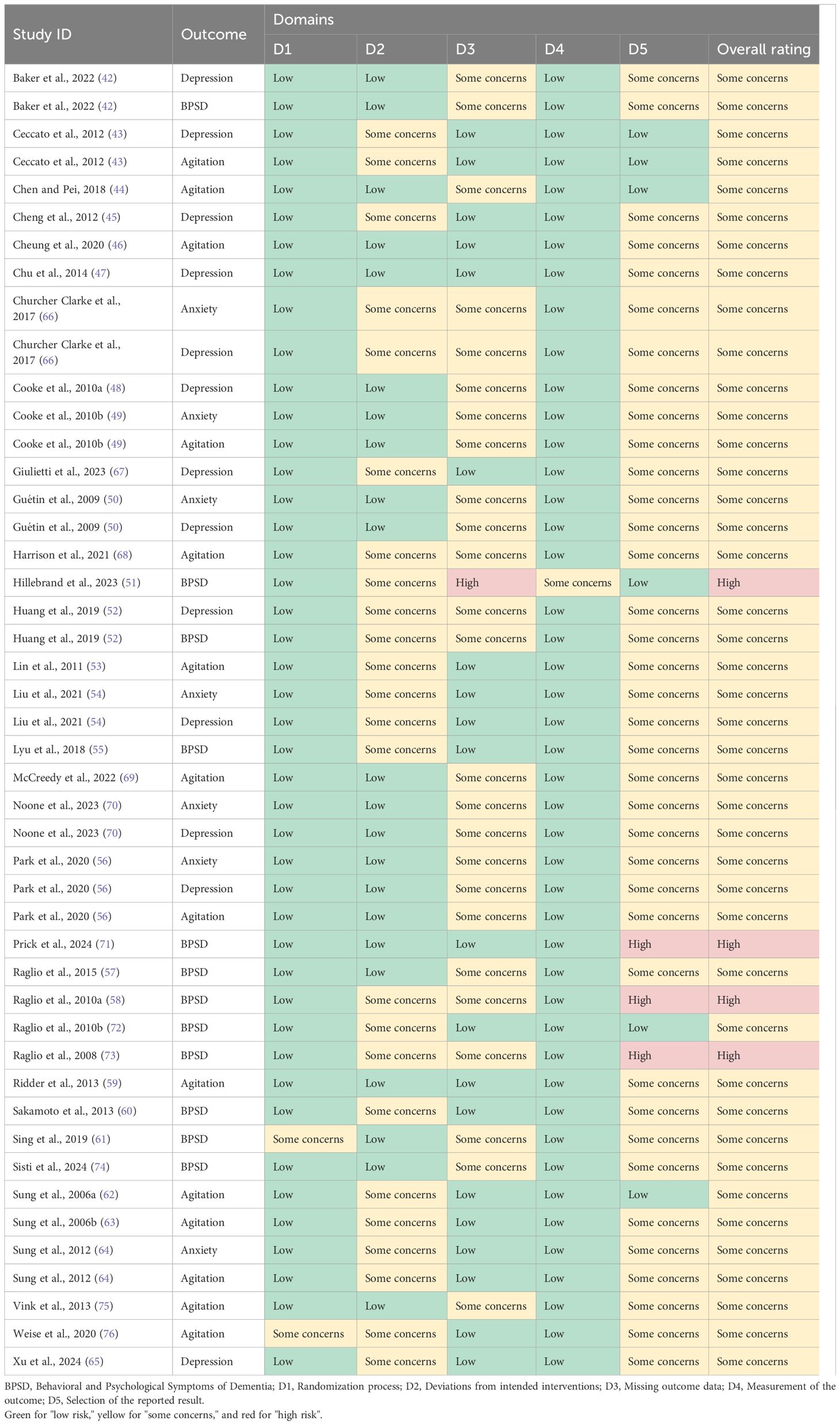
Table 4. Risk of bias summary for the included effect estimates.
A meta-analysis of 7 RCTs (N = 564 patients) exhibited a significant improvement in BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01) in OPWD, with no significant heterogeneity between RCTs (I2 = 43.68%; Q = 10.65; p = 0.10). A forest plot for BPSD is presented in Figure 3.
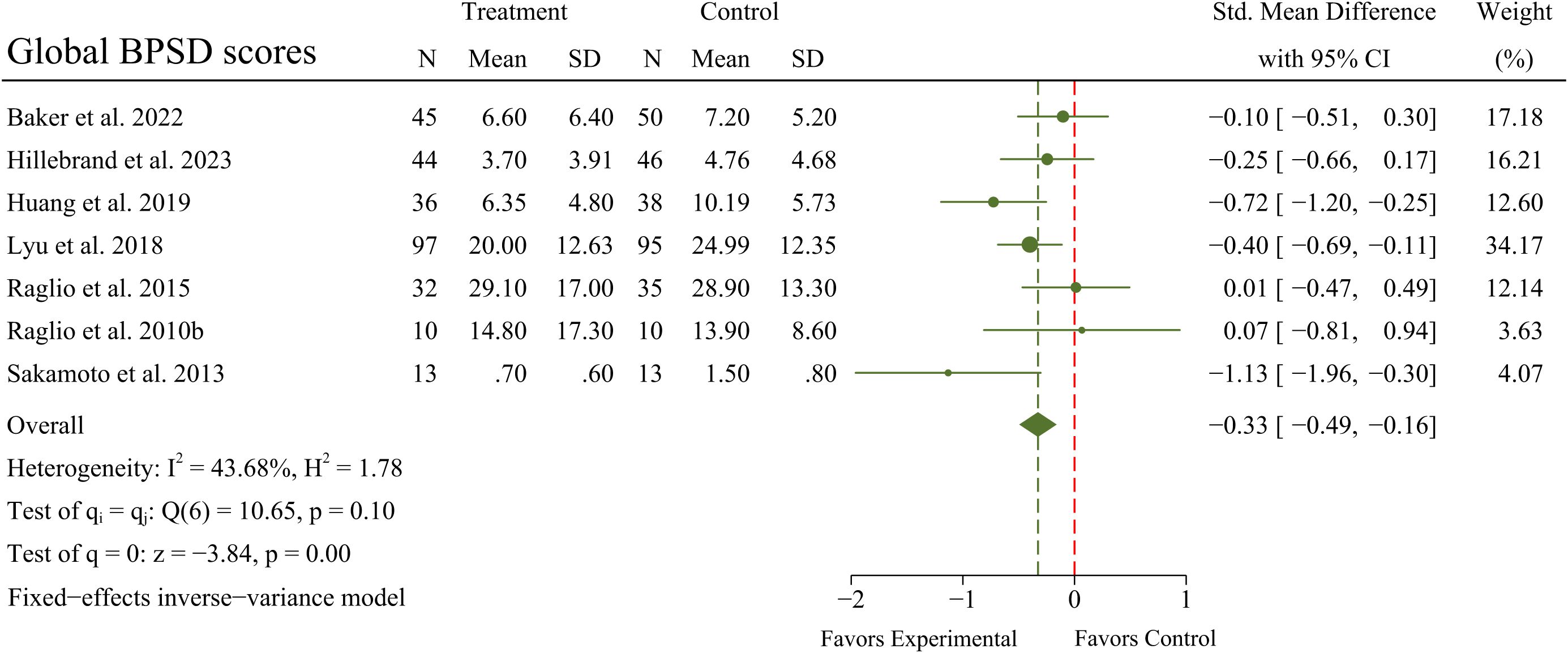
Figure 3. Main analyses for the effects of MBTs on BPSD.
A meta-analysis of 6 RCTs (N = 224 patients) exhibited a significant improvement in anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02) in OPWD, but with significant heterogeneity between RCTs (I2 = 83.69%; Q = 30.66; p < 0.01). A forest plot for anxiety is presented in Figure 4.
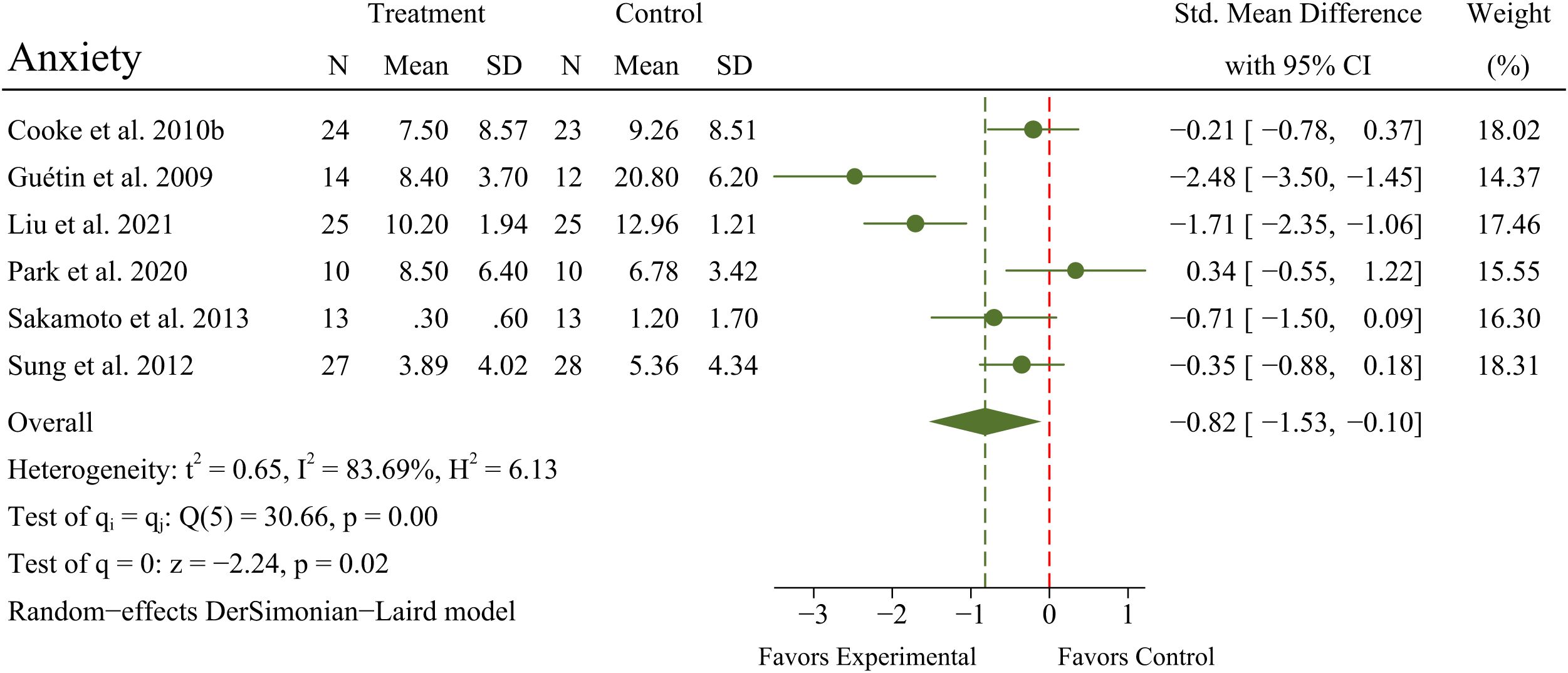
Figure 4. Main analyses for the effects of MBTs on anxiety.
A meta-analysis of 10 RCTs (N = 607 patients) exhibited a significant improvement in depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02) in OPWD, but with significant heterogeneity between RCTs (I2 = 87.39%; Q = 71.40; p < 0.01). A forest plot for depression is presented in Figure 5.
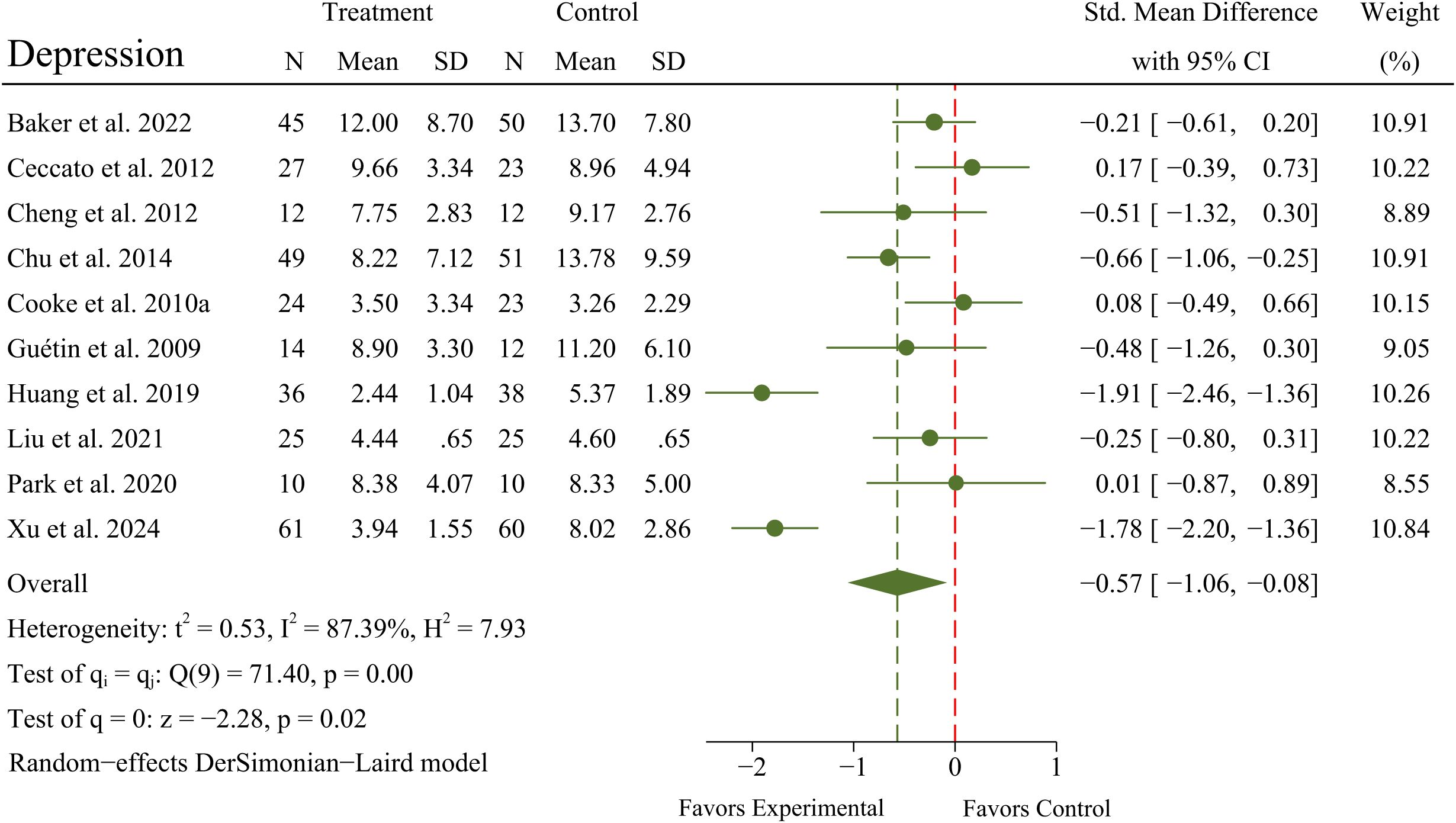
Figure 5. Main analyses for the effects of MBTs on depression.
A meta-analysis of 11 RCTs (N = 618 patients) exhibited no significant improvement in agitation (SMD = -0.09; 95% CI -0.25 to 0.07; p = 0.27) in OPWD, with no significant heterogeneity between RCTs (I2 = 34.66%; Q = 15.31; p = 0.12). A forest plot for agitation is presented in Figure 6.
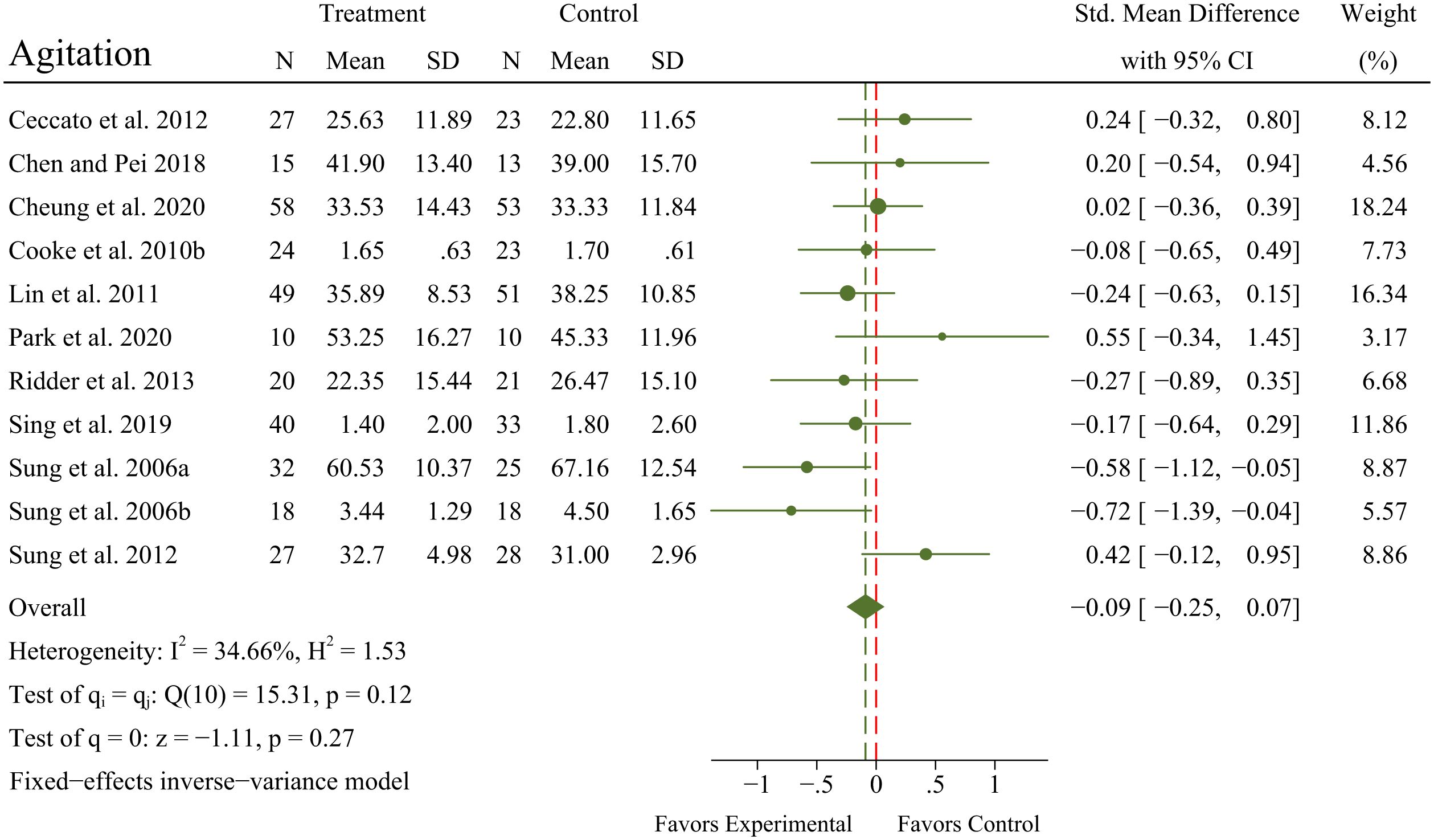
Figure 6. Main analyses for the effects of MBTs on agitation.
The results of the sensitivity analyses indicated that the pooled results for agitation and BPSD remained stable after excluding individual studies, indicating that these results were robust and insensitive to study selection. However, the pooled results for anxiety and depression were sensitive to study selection and were less robust when individual studies were excluded. The results of the sensitivity analyses are presented in Table 5.
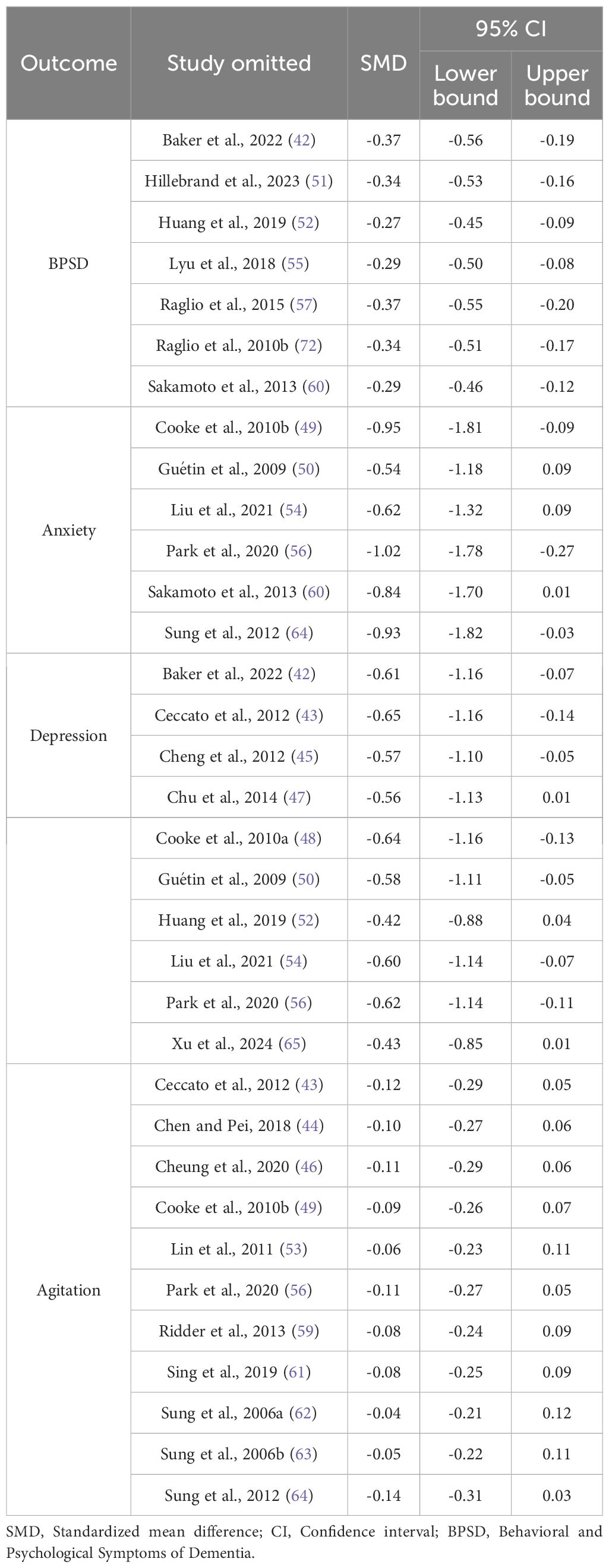
Table 5. Sensitivity analyses for outcomes by omitting individual studies.
Given the number of included trials with pooled results for depression and agitation, publication bias was assessed using funnel plots and the Egger’s test. Funnel plots for depression and agitation are presented symmetrically in Figure 7. The p-values of Egger’s test for depression and agitation were 0.42 and 0.55, respectively, indicating that publication bias did not affect this type of study. According to the GRADE ratings, the certainty of evidence across the outcomes ranged from low to very low, owing to inconsistency, indirectness, imprecision, and publication bias (see Table 6).
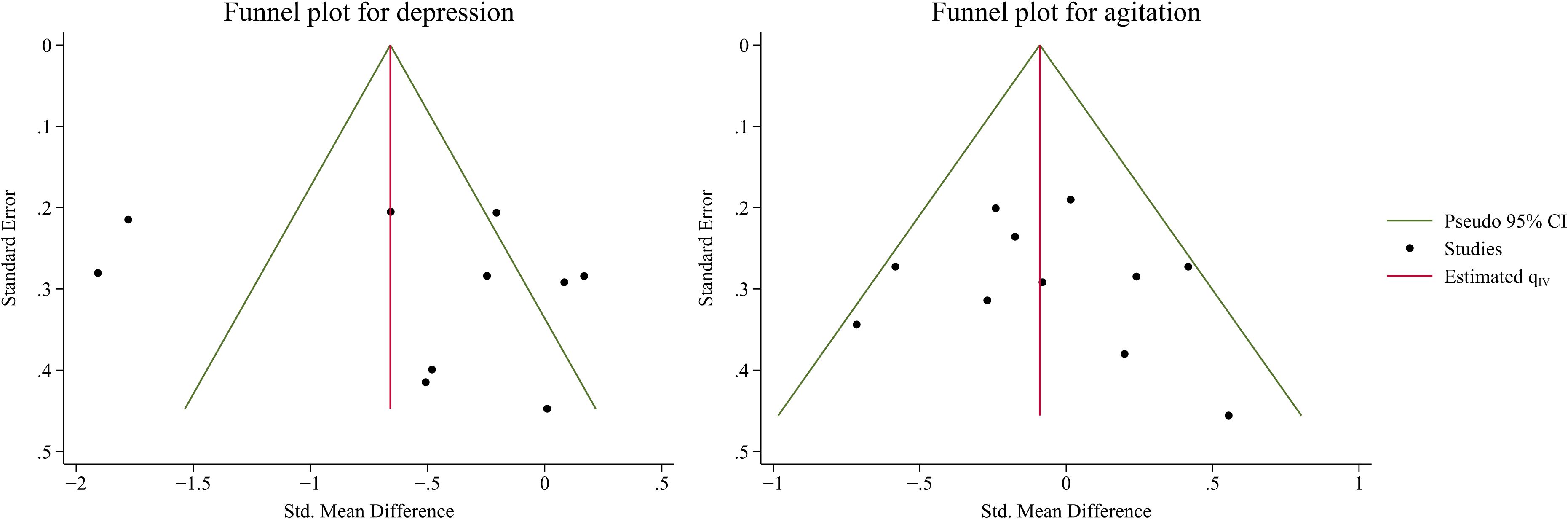
Figure 7. Publication bias for depression (left) and agitation (right).
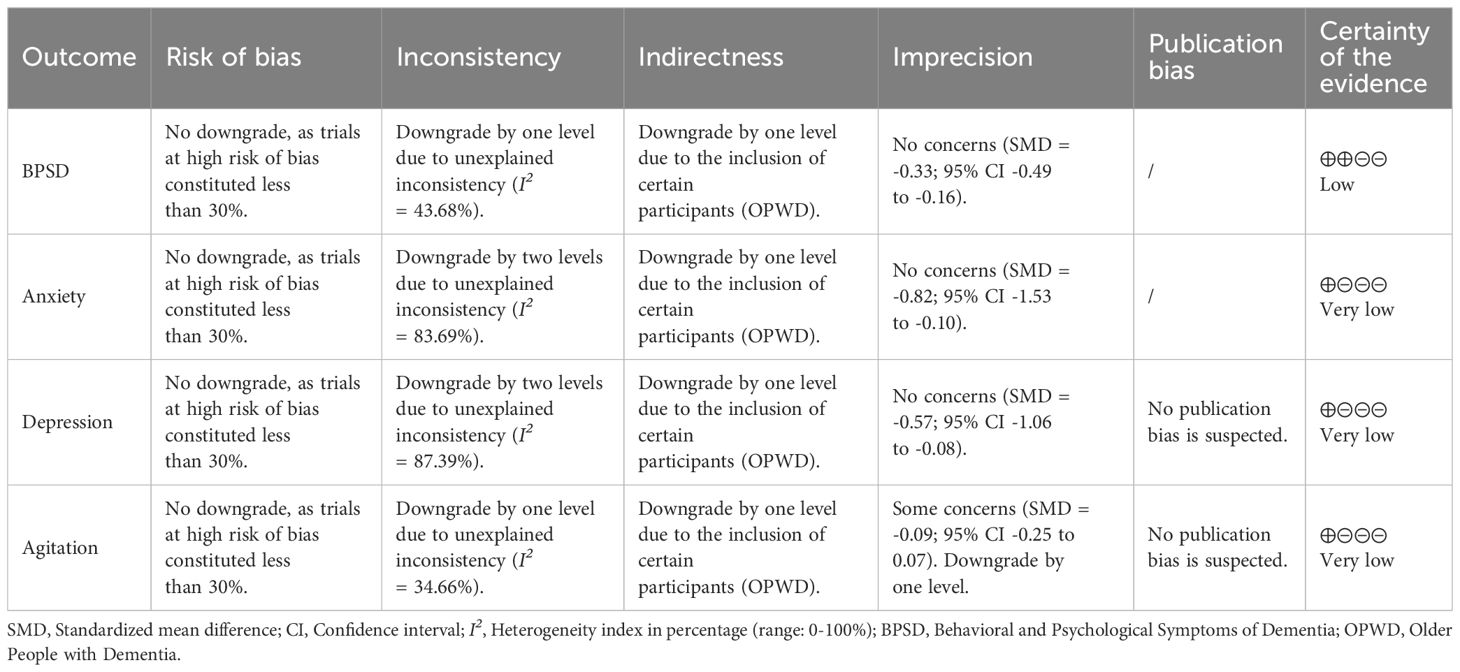
Table 6. Certainty of evidence rating (GRADE).
Previous studies have predominantly investigated the efficacy of single interventions for OPWD and have provided inconsistent evidence regarding various outcomes (23–33). This study aimed to evaluate the potential multidomain benefits of MBTs for BPSD in OPWD. The pooled results of the meta-analyses indicated that MBTs effectively improved BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01), anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02), and depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02), with no significant improvements observed in agitation (SMD = -0.09; 95% CI -0.25 to 0.07; p = 0.27) among patients with dementia.
Music-based interventions are likely the most common MBT for alleviating BPSD in OPWD, as evidenced in 26 of the 35 trials. Previous studies have confirmed the effectiveness of music-based interventions, particularly in improving anxiety and depression (77–81). Music-based interventions are among the most effective approaches for managing BPSD in OPWD. However, a recent systematic review revealed that music-based interventions may not have achieved the anticipated efficacy, suggesting that the generalizability and applicability of this evidence require further examination (82). Overall, MBTs have significant therapeutic benefits in alleviating BPSD in OPWD, and the underlying mechanisms may be explained from several perspectives. Dementia is associated with the hypothalamus-pituitary-adrenal (HPA) axis and the autonomic nervous system (ANS), which are the main components of emotional regulation (83, 84). By reducing the HPA axis activation and reactivity, MBTs may alleviate the effects of stress and foster multiple positive downstream effects by shifting the ANS balance from primarily sympathetic to parasympathetic, leading to positive changes in cardiac vagal function, mood, energy state, and related neuroendocrine, metabolic, and inflammatory responses (85–89), which may play a potential role in mediating BPSD in OPWD. In addition, an increase in neurotransmitters such as serotonin and dopamine (responsible for regulating emotions and behavior) can be induced through exercise interventions included in MBTs (e.g., Tai Chi, Qigong, and Yoga), which help improve BPSD in OPWD (90).
BPSD represents a heterogeneous group of non-cognitive symptoms and behaviors that occur in patients with dementia, including anxiety, depression, agitation, irritability, apathy, and delusions (91–93). Therefore, in the quantitative analysis, BPSD was subdivided based on existing data to further clarify the efficacy of MBTs for these specific symptoms. Although the pooled results of the meta-analyses indicated that MBTs effectively improved BPSD in OPWD, this impact did not include all symptoms. For instance, according to the pooled results for agitation in OPWD, MBTs did not provide significant therapeutic benefits as previously assumed, which is consistent with previous evidence (30, 32). This may be because, for OPWD, especially those with advanced dementia, the inability to perform activities of daily living, often accompanied by clinical complications such as dysphagia and infections (14), presents a significant challenge in addressing behavioral disorders (including agitation and aggressive tendencies) with short-term MBTs. Finally, in terms of improving anxiety and depression in OPWD, evidence confirming the therapeutic benefits of MBTs is urgently required because of the significant heterogeneity or sensitivity to study selection in the pooled results. This may stem from the fact that the specific interventions, implementation steps, and duration of the interventions varied between studies, resulting in large differences in effect sizes. Additionally, the CIs for certain pooled results were near the threshold of statistical significance after excluding individual studies. This indicates that the sample size and experimental design need to be further increased and refined to more precisely evaluate the potential benefits of MBTs on these outcomes.
Although MBTs are promising complementary therapies for enhancing physical and mental health in OPWD, their differential efficacy should be further explored and validated. Most existing trials focus on the efficacy of a single intervention for BPSD in OPWD while ignoring the differential efficacy between various interventions. This may lead to an overestimation of the actual efficacy of MBTs in clinical practice. In the context of limited medical resources and the increasing prevalence of dementia, MBTs that can be effectively applied to clinical practice should be identified. Doctors and nurses are inclined to use non-pharmacological treatments more than pharmacological treatments in clinical practice (94). Therefore, comparisons between non-pharmacological treatments should receive more attention. A network meta-analysis suggests that individualized nursing, behavior therapy, and reminiscence therapy have significant potential in improving BPSD in OPWD, particularly in reducing anxiety and depression (95). Thus, the differential efficacy of non-pharmacological treatments in improving various aspects of BPSD should be further examined to maximize the clinical benefits of non-pharmacological treatments in the context of limited medical resources. Notably, the efficacy of MBTs in improving BPSD in OPWD may vary depending on the intervention period, frequency, and duration, suggesting that the dose-response relationship of MBTs in this regard is also an important area for investigation. Although this study did not reveal the optimal dosage of MBTs for improving BPSD in OPWD, existing research indicates that the intervention period, frequency, and duration are critical factors influencing efficacy (31, 33, 96). Short-term, high-frequency interventions may lead to faster clinical improvements to some extent, while long-term, low-frequency interventions may help maintain long-term efficacy. Therefore, more high-quality RCTs must be conducted to explore the dose-response relationship of MBTs in improving BPSD in OPWD, and intervention programs should be flexibly adjusted in clinical practice based on patients’ individual differences to achieve the best therapeutic outcomes.
The findings of this systematic review and meta-analysis should be interpreted in the context of these limitations. First, owing to the limited information available on the study population from existing trials, this study mainly examined the overall therapeutic benefit of MBTs for OPWD and did not make specific distinctions based on the type and course of dementia. Second, although there was significant heterogeneity in the pooled results for some outcomes, sources of heterogeneity were not identified because of study data limitations. To address this problem, more comprehensive data should be collected in future studies. Finally, for some outcomes such as anxiety and depression, the pooled results were sensitive to study selection and were less robust; thus, the findings should be interpreted cautiously.
Effective nursing for patients with dementia is vital, as they are undergoing a major transition in their physical and mental health. Although MBTs effectively improved BPSD in OPWD to some extent, the dose-response relationship of MBTs in improving various aspects of BPSD remains unclear, and these relationships may be influenced by the intervention period, frequency, and duration. In clinical practice, healthcare and social care therapists should develop personalized intervention programs based on patient individual differences and the actual dose-response relationship, which will help maximize the clinical benefits of non-pharmacological treatments in the context of limited medical resources.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
ZYM: Conceptualization, Data curation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing. CYC: Conceptualization, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. TFW: Data curation, Resources, Visualization, Writing – original draft. YZZ: Formal analysis, Validation, Writing – original draft, Software. WZ: Conceptualization, Data curation, Software, Writing – review & editing. CFL: Methodology, Software, Visualization, Writing – review & editing. SLL: Data curation, Writing – review & editing, Validation, Visualization. YS: Validation, Visualization, Writing – review & editing. SL: Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the National Social Science Fund of China (project 24BTY098).
Research team would like to thank Southwest University for the support of this research, and also thank Shi Luo for the help in developing the research program.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Malik R, Kalra S, Bhatia S, Al Harrasi A, Singh G, Mohan S, et al. Overview of therapeutic targets in management of dementia. Biomed Pharmacother. (2022) 152:1–15. doi: 10.1016/j.biopha.2022.113168
2. Kornblith E, Bahorik A, Boscardin WJ, Xia F, Barnes DE, Yaffe K. Association of race and ethnicity with incidence of dementia among older adults. JAMA. (2022) 327:1488–95. doi: 10.1001/jama.2022.3550
3. Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia. JAMA. (2019) 322:1589–99. doi: 10.1001/jama.2019.4782
4. Grande G, Qiu C, Fratiglioni L. Prevention of dementia in an ageing world: Evidence and biological rationale. Ageing Res Rev. (2020) 64:101045. doi: 10.1016/j.arr.2020.101045
5. Cao Q, Tan C-C, Xu W, Hu H, Cao X-P, Dong Q, et al. The prevalence of dementia: a systematic review and meta-analysis. J Alzheimer’s Dis. (2020) 73:1157–66. doi: 10.3233/JAD-191092
6. Licher S, Ahmad S, Karamujić-Čomić H, Voortman T, Leening MJ, Ikram MA, et al. Genetic predisposition, modifiable-risk-factor profile and long-term dementia risk in the general population. Nat Med. (2019) 25:1364–9. doi: 10.1038/s41591-019-0547-7
7. Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
8. Amariglio RE, Donohue MC, Marshall GA, Rentz DM, Salmon DP, Ferris SH, et al. Tracking early decline in cognitive function in older individuals at risk for Alzheimer disease dementia: the Alzheimer’s Disease Cooperative Study Cognitive Function Instrument. JAMA Neurol. (2015) 72:446–54. doi: 10.1001/jamaneurol.2014.3375
9. Alothman D, Card T, Lewis S, Tyrrell E, Fogarty AW, Marshall CR. Risk of suicide after dementia diagnosis. JAMA Neurol. (2022) 79:1148–54. doi: 10.1001/jamaneurol.2022.3094
10. Stefanidou M, Beiser AS, Himali JJ, Peng TJ, Devinsky O, Seshadri S, et al. Bi-directional association between epilepsy and dementia: The Framingham Heart Study. Neurology. (2020) 95:e3241–e7. doi: 10.1212/WNL.0000000000011077
11. Lisko I, Kulmala J, Annetorp M, Ngandu T, Mangialasche F, Kivipelto M. How can dementia and disability be prevented in older adults: where are we today and where are we going? J Internal Med. (2021) 289:807–30. doi: 10.1111/joim.13227
12. Becker E, Rios CLO, Lahmann C, Ruecker G, Bauer J, Boeker M. Anxiety as a risk factor of Alzheimer’s disease and vascular dementia. Br J Psychiatry. (2018) 213:654–60. doi: 10.1192/bjp.2018.173
13. Rubin R. Exploring the relationship between depression and dementia. JAMA. (2018) 320:961–2. doi: 10.1001/jama.2018.11154
15. Byun J, Lee DY, Jeong C-W, Kim Y, Rhee HY, Moon KW, et al. Analysis of treatment pattern of anti-dementia medications in newly diagnosed Alzheimer’s dementia using OMOP CDM. Sci Rep. (2022) 12:1–9. doi: 10.1038/s41598-022-08595-1
16. Ruangritchankul S, Chantharit P, Srisuma S, Gray LC. Adverse drug reactions of acetylcholinesterase inhibitors in older people living with dementia: a comprehensive literature review. Ther Clin Risk Manage. (2021) 17:927–49. doi: 10.2147/TCRM.S323387
17. Zhai Y, Yin S, Zhang D. Association between antipsychotic drugs and mortality in older persons with Alzheimer’s disease: a systematic review and meta-analysis. J Alzheimer’s Dis. (2016) 52:631–9. doi: 10.3233/JAD-151207
18. Laird KT, Paholpak P, Roman M, Rahi B, Lavretsky H. Mind-body therapies for late-life mental and cognitive health. Curr Psychiatry Rep. (2018) 20:1–12. doi: 10.1007/s11920-018-0864-4
19. Medicine SoI. Mind-body therapies in children and youth. Pediatrics. (2016) 138:e1–e12. doi: 10.1542/peds.2016-1896
20. Anderson JG, Rogers CE, Bossen A, Testad I, Rose KM. Mind–body therapies in individuals with dementia: An integrative review. Res Gerontol Nursing. (2017) 10:288–96. doi: 10.3928/19404921-20170928-01
21. Mei Z, Jiang W, Zhang Y, Luo S, Luo S. Mind-body therapies for resilience in adolescents: A systematic review of randomized controlled trials. Gen Hosp Psychiatry. (2024) 91:43–51. doi: 10.1016/j.genhosppsych.2024.08.014
22. Wang Y, Tang C, Fan X, Shirai K, Dong J-Y. Mind–body therapies for older adults with dementia: a systematic review and meta-analysis. Eur Geriatric Med. (2022) 13:881–91. doi: 10.1007/s41999-022-00639-z
23. Karamacoska D, Tan T, Mathersul DC, Sabag A, de Manincor M, Chang D, et al. A systematic review of the health effects of yoga for people with mild cognitive impairment and dementia. BMC Geriatrics. (2023) 23:1–12. doi: 10.1186/s12877-023-03732-5
24. Moreno-Morales C, Calero R, Moreno-Morales P, Pintado C. Music therapy in the treatment of dementia: A systematic review and meta-analysis. Front Med. (2020) 7:160. doi: 10.3389/fmed.2020.00160
25. Dorris JL, Neely S, Terhorst L, VonVille HM, Rodakowski J. Effects of music participation for mild cognitive impairment and dementia: A systematic review and meta-analysis. J Am Geriatrics Soc. (2021) 69:2659–67. doi: 10.1111/jgs.17208
26. Lim KH-L, Pysklywec A, Plante M, Demers L. The effectiveness of Tai Chi for short-term cognitive function improvement in the early stages of dementia in the elderly: a systematic literature review. Clin Interventions Aging. (2019) 14:827–39. doi: 10.2147/CIA.S202055
27. Nyman SR, Ingram W, Sanders J, Thomas PW, Thomas S, Vassallo M, et al. Randomized controlled trial of the effect of Tai Chi on postural balance of people with dementia. Clin Interventions Aging. (2019) 14:2017–29. doi: 10.2147/CIA.S228931
28. Keune PM, Bernard F, Meister R, Keune J, Springer R, Arlt R, et al. Mindfulness in persons with mild dementia and their caregivers: exploring trait rumination as a clinical outcome measure. Mindfulness. (2023) 14:1908–17. doi: 10.1007/s12671-023-02192-7
29. Fusar-Poli L, Bieleninik Ł, Brondino N, Chen X-J, Gold C. The effect of music therapy on cognitive functions in patients with dementia: a systematic review and meta-analysis. Aging Ment Health. (2018) 22:1103–12. doi: 10.1080/13607863.2017.1348474
30. Han A. Mindfulness-based interventions for older adults with dementia or mild cognitive impairment: A meta-analysis. Clin Gerontol. (2022) 45:763–76. doi: 10.1080/07317115.2021.1995561
31. Chan J, Leung DK, Walton H, Wong GH, Spector A. Can mindfulness-based interventions benefit people with dementia? Drawing on the evidence from a systematic review in populations with cognitive impairments. Expert Rev Neurother. (2020) 20:1143–56. doi: 10.1080/14737175.2020.1810571
32. Wang FL, Tang QY, Zhang LL, Yang JJ, Li Y, Peng H, et al. Effects of mindfulness-based interventions on dementia patients: a meta-analysis. West J Nurs Res. (2020) 42:1163–73. doi: 10.1177/0193945920916750
33. Hofbauer LM, Ross SD, Rodriguez FS. Music-based interventions for community-dwelling people with dementia: A systematic review. Health Soc Care Commun. (2022) 30:2186–201. doi: 10.1111/hsc.13895
34. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Internal Med. (2015) 162:777–84. doi: 10.7326/M14-2385
35. Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomized trials. BMJ. (2019) 366:1–8. doi: 10.1136/bmj.l4898
36. Deeks JJ, Higgins JP, Altman DG. Analyzing data and undertaking meta-analyses. In: Higgins J, Thomas J, Chandler J, Cumpston M, Li TPM, Welch V, editors. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons, Hoboken (2019). p. 241–84.
37. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
38. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
39. Tang J-L, Liu JL. Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol. (2000) 53:477–84. doi: 10.1016/S0895-4356(99)00204-8
40. Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. (2000) 56:455–63. doi: 10.1111/j.0006-341X.2000.00455.x
41. Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. (2011) 64:380–2. doi: 10.1016/j.jclinepi.2010.09.011
42. Baker FA, Lee YC, Sousa TV, Stretton-Smith PA, Tamplin J, Sveinsdottir V, et al. Clinical effectiveness of music interventions for dementia and depression in elderly care (MIDDEL): Australian cohort of an international pragmatic cluster-randomized controlled trial. Lancet Health Long. (2022) 3:e153–e65. doi: 10.1016/s2666-7568(22)00027-7
43. Ceccato E, Vigato G, Bonetto C, Bevilacqua A, Pizziolo P, Crociani S, et al. STAM protocol in dementia: A multicenter, single-blind, randomized, and controlled trial. Am J Alzheimer’s Dis other Dementias. (2012) 27:301–10. doi: 10.1177/1533317512452038
44. Chen YL, Pei YC. Musical dual-task training in patients with mild-to-moderate dementia: A randomized controlled trial. Neuropsychiatr Dis Treat. (2018) 14:1381–93. doi: 10.2147/NDT.S159174
45. Cheng ST, Chow PK, Yu EC, Chan AC. Leisure activities alleviate depressive symptoms in nursing home residents with very mild or mild dementia. Am J Geriatric Psychiatry. (2012) 20:904–8. doi: 10.1097/JGP.0b013e3182423988
46. Cheung DSK, Lai CKY, Wong FKY, Leung MCP. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate dementia? A randomized controlled trial. Dementia. (2020) 19:1413–25. doi: 10.1177/1471301218800195
47. Chu H, Yang C-Y, Lin Y, Ou K-L, Lee T-Y, O’Brien AP, et al. The impact of group music therapy on depression and cognition in elderly persons with dementia: A randomized controlled study. Biol Res Nursing. (2014) 16:209–17. doi: 10.1177/1099800413485410
48. Cooke M, Moyle W, Shum D, Harrison S, Murfield J. A randomized controlled trial exploring the effect of music on quality of life and depression in older people with dementia. J Health Psychol. (2010) 15:765–76. doi: 10.1177/1359105310368188
49. Cooke ML, Moyle W, Shum DH, Harrison SD, Murfield JE. A randomized controlled trial exploring the effect of music on agitated behaviors and anxiety in older people with dementia. Aging Ment Health. (2010) 14:905–16. doi: 10.1080/13607861003713190
50. Guétin S, Portet F, Picot MC, Pommié C, Messaoudi M, Djabelkir L, et al. Effect of music therapy on anxiety and depression in patients with Alzheimer’s type dementia: Randomized, controlled study. Dementia Geriatric Cogn Disord. (2009) 28:36–46. doi: 10.1159/000229024
51. Hillebrand MC, Weise L, Wilz G. Immediate effects of individualized music listening on behavioral and psychological symptoms of dementia: A randomized controlled trial. Int J Geriatric Psychiatry. (2023) 38:1–9. doi: 10.1002/gps.5893
52. Huang N, Li W, Rong X, Champ M, Wei L, Li M, et al. Effects of a modified Tai Chi program on older people with mild dementia: A randomized controlled trial. J Alzheimer’s Dis. (2019) 72:947–56. doi: 10.3233/JAD-190487
53. Lin Y, Chu H, Yang C-Y, Chen C-H, Chen S-G, Chang H-J, et al. Effectiveness of group music intervention against agitated behavior in elderly persons with dementia. Int J Geriatric Psychiatry. (2011) 26:670–8. doi: 10.1002/gps.2580
54. Liu MN, Liou YJ, Wang WC, Su KC, Yeh HL, Lau CI, et al. Group music intervention using percussion instruments to reduce anxiety among elderly male veterans with Alzheimer disease. Med Sci Monitor. (2021) 27:e928714. doi: 10.12659/MSM.928714
55. Lyu J, Zhang J, Mu H, Li W, Champ M, Xiong Q, et al. The effects of music therapy on cognition, psychiatric symptoms, and activities of daily living in patients with Alzheimer’s disease. J Alzheimer’s Dis. (2018) 64:1347–58. doi: 10.3233/jad-180183
56. Park J, Tolea MI, Sherman D, Rosenfeld A, Arcay V, Lopes Y, et al. Feasibility of conducting nonpharmacological interventions to manage dementia symptoms in community-dwelling older adults: A cluster randomized controlled trial. Am J Alzheimer’s Dis Other Dementias. (2020) 35:1–12. doi: 10.1177/1533317519872635
57. Raglio A, Bellandi D, Baiardi P, Gianotti M, Ubezio MC, Zanacchi E, et al. Effect of active music therapy and individualized listening to music on dementia: A multicenter randomized controlled trial. J Am Geriatrics Soc. (2015) 63:1534–9. doi: 10.1111/jgs.13558
58. Raglio A, Oasi O, Gianotti M, Manzoni V, Bolis S, C Ubezio M, et al. Effects of music therapy on psychological symptoms and heart rate variability in patients with dementia. A pilot study Curr Aging Sci. (2010) 3:242–6. doi: 10.2174/1874609811003030242
59. Ridder HMO, Stige B, Qvale LG, Gold C. Individual music therapy for agitation in dementia: an exploratory randomized controlled trial. Aging Ment Health. (2013) 17:667–78. doi: 10.1080/13607863.2013.790926
60. Sakamoto M, Ando H, Tsutou A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int Psychoger. (2013) 25:775–84. doi: 10.1017/s1041610212002256
61. Sing CY, Lee PHT, Leung ABK, Chung KSM, Kwok JKL, Ho RTH, et al. Managing behavioral and psychological symptoms in Chinese elderly with dementia via group-based music intervention: A cluster randomized controlled trial. Dementia. (2019) 18:2785–98. doi: 10.1177/1471301218760023
62. Sung HC, Chang AM, Abbey J. The effects of preferred music on agitation of older people with dementia in Taiwan. Int J Geriatric Psychiatry. (2006) 21:999–1000. doi: 10.1002/gps.1585
63. Sung Hc, Chang Sm, Lee Wl, Lee Ms. The effects of group music with movement intervention on agitated behaviors of institutionalized elders with dementia in Taiwan. Complement Ther Med. (2006) 14:113–9. doi: 10.1016/j.ctim.2006.03.002
64. Sung HC, Lee WL, Li TL, Watson R. A group music intervention using percussion instruments with familiar music to reduce anxiety and agitation of institutionalized older adults with dementia. Int J Geriatric Psychiatry. (2012) 27:621–7. doi: 10.1002/gps.2761
65. Xu H, Li A, Apuke OD. The impact of group music therapy in ameliorating the depression among patients with dementia in care homes: A randomized control trial. Geriatric Nursing. (2024) 56:304–11. doi: 10.1016/j.gerinurse.2024.02.021
66. Churcher Clarke A, Chan JMY, Stott J, Royan L, Spector A. An adapted mindfulness intervention for people with dementia in care homes: feasibility pilot study. Int J Geriatric Psychiatry. (2017) 32:e123–e31. doi: 10.1002/gps.4669
67. Giulietti MV, Spatuzzi R, Fabbietti P, Vespa A. Effects of mindfulness-based interventions (MBIs) in patients with early-stage Alzheimer’s disease: A pilot study. Brain Sci. (2023) 13:1–12. doi: 10.3390/brainsci13030484
68. Harrison TC, Blozis SA, Schmidt B, Johnson A, Moreno R, Mead S, et al. Music compared with auditory books: A randomized controlled study among long-term care residents with Alzheimer’s disease or related dementia. J Am Med Direct Assoc. (2021) 22:1415–20. doi: 10.1016/j.jamda.2021.01.086
69. McCreedy EM, Sisti A, Gutman R, Dionne L, Rudolph JL, Baier R, et al. Pragmatic trial of personalized music for agitation and antipsychotic use in nursing home residents with dementia. J Am Med Direct Assoc. (2022) 23:1171–7. doi: 10.1016/j.jamda.2021.12.030
70. Noone D, Payne J, Stott J, Aguirre E, Patel-Palfreman MM, Stoner C, et al. The feasibility of a mindfulness intervention for depression in people with mild dementia: A pilot randomized controlled trial. Clin Gerontol. (2023) 46:346–58. doi: 10.1080/07317115.2022.2094741
71. Prick AEJC, Zuidema SU, van Domburg P, Verboon P, Vink AC, Schols JMGA, et al. Effects of a music therapy and music listening intervention for nursing home residents with dementia: a randomized controlled trial. Front Med. (2024) 11:1304349. doi: 10.3389/fmed.2024.1304349
72. Raglio A, Bellelli G, Traficante D, Gianotti M, Ubezio MC, Gentile S, et al. Efficacy of music therapy treatment based on cycles of sessions: A randomized controlled trial. Aging Ment Health. (2010) 14:900–4. doi: 10.1080/13607861003713158
73. Raglio A, Bellelli G, Traficante D, Gianotti M, Ubezio MC, Villani D, et al. Efficacy of music therapy in the treatment of behavioral and psychiatric symptoms of dementia. Alzheimer Dis Assoc Disord. (2008) 22:158–62. doi: 10.1097/WAD.0b013e3181630b6f
74. Sisti A, Gutman R, Mor V, Dionne L, Rudolph JL, Baier RR, et al. Using structured observations to evaluate the effects of a personalized music intervention on agitated behaviors and mood in nursing home residents with dementia: results from an embedded, pragmatic randomized controlled trial. Am J Geriatric Psychiatry. (2024) 32:300–11. doi: 10.1016/j.jagp.2023.10.016
75. Vink AC, Zuidersma M, Boersma F, de Jonge P, Zuidema SU, Slaets JP. The effect of music therapy compared with general recreational activities in reducing agitation in people with dementia: a randomized controlled trial. Int J Geriatric Psychiatry. (2013) 28:1031–8. doi: 10.1002/gps.3924
76. Weise L, Töpfer NF, Deux J, Wilz G. Feasibility and effects of individualized recorded music for people with dementia: A pilot RCT study. Nordic J Music Ther. (2020) 29:39–56. doi: 10.1080/08098131.2019.1661507
77. Ueda T, Suzukamo Y, Sato M, Izumi S-I. Effects of music therapy on behavioral and psychological symptoms of dementia: a systematic review and meta-analysis. Ageing Res Rev. (2013) 12:628–41. doi: 10.1016/j.arr.2013.02.003
78. Scott S, Kidd A. A scoping review of music and anxiety, depression and agitation in older people with dementia in residential facilities and specialist care units. Eur Geriatric Med. (2016) 7:488–91. doi: 10.1016/j.eurger.2016.07.007
79. Ing-Randolph AR, Phillips LR, Williams AB. Group music interventions for dementia-associated anxiety: A systematic review. Int J Nurs Stud. (2015) 52:1775–84. doi: 10.1016/j.ijnurstu.2015.06.014
80. Tsoi KK, Chan JY, Ng Y-M, Lee MM, Kwok TC, Wong SY. Receptive music therapy is more effective than interactive music therapy to relieve behavioral and psychological symptoms of dementia: a systematic review and meta-analysis. J Am Med Direct Assoc. (2018) 19:568–76. e3. doi: 10.1016/j.jamda.2017.12.009
81. Zhang Y, Cai J, An L, Hui F, Ren T, Ma H, et al. Does music therapy enhance behavioral and cognitive function in elderly dementia patients? A systematic review and meta-analysis. Ageing Res Rev. (2017) 35:1–11. doi: 10.1016/j.arr.2016.12.003
82. Mei Z, Zhang Y, Zhao W, Lam C, Luo S, Wang S, et al. Music-based interventions for anxiety and depression in older adults with dementia: A systematic review of randomized controlled trials. Complement Ther Clin Pract. (2025) 59:1–8. doi: 10.1016/j.ctcp.2025.101951
83. Milligan Armstrong A, Porter T, Quek H, White A, Haynes J, Jackaman C, et al. Chronic stress and A lzheimer’s disease: the interplay between the hypothalamic–pituitary–adrenal axis, genetics and microglia. Biol Rev. (2021) 96:2209–28. doi: 10.1111/brv.12750
84. Hafizi S, Rajji TK. Modifiable risk factors of dementia linked to excitation-inhibition imbalance. Ageing Res Rev. (2023) 83:1–10. doi: 10.1016/j.arr.2022.101804
85. Taylor AG, Goehler LE, Galper DI, Innes KE, Bourguignon C. Top-down and bottom-up mechanisms in mind-body medicine: development of an integrative framework for psychophysiological research. Explore. (2010) 6:29–41. doi: 10.1016/j.explore.2009.10.004
86. Lindsay EK, Young S, Smyth JM, Brown KW, Creswell JD. Acceptance lowers stress reactivity: Dismantling mindfulness training in a randomized controlled trial. Psychoneuroendocrinology. (2018) 87:63–73. doi: 10.1016/j.psyneuen.2017.09.015
87. Nyklíček I, Mommersteeg P, Van Beugen S, Ramakers C, Van Boxtel GJ. Mindfulness-based stress reduction and physiological activity during acute stress: a randomized controlled trial. Health Psychol. (2013) 32:1110–3. doi: 10.1037/a0032200
88. Pant U, Frishkopf M, Park T, Norris CM, Papathanassoglou E. A neurobiological framework for the therapeutic potential of music and sound interventions for post-traumatic stress symptoms in critical illness survivors. Int J Environ Res Public Health. (2022) 19:1–19. doi: 10.3390/ijerph19053113
89. Gothe NP, Keswani RK, McAuley E. Yoga practice improves executive function by attenuating stress levels. Biol Psychol. (2016) 121:109–16. doi: 10.1016/j.biopsycho.2016.10.010
90. Matura S, Carvalho A F, Alves G S, Pantel J. Physical exercise for the treatment of neuropsychiatric disturbances in Alzheimer’s dementia: possible mechanisms, current evidence and future directions. Curr Alzheimer Res. (2016) 13:1112–23. doi: 10.2174/1567205013666160502123428
91. Lawlor B. Managing behavioral and psychological symptoms in dementia. Br J Psychiatry. (2002) 181:463–5. doi: 10.1192/bjp.181.6.463
92. Azermai M, Petrovic M, Elseviers MM, Bourgeois J, Van Bortel LM, Vander Stichele RH. Systematic appraisal of dementia guidelines for the management of behavioral and psychological symptoms. Ageing Res Rev. (2012) 11:78–86. doi: 10.1016/j.arr.2011.07.002
93. Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. (2012) 3:73. doi: 10.3389/fneur.2012.00073
94. Janus SI, van Manen JG, Van Til JA, Zuidema SU, IJzerman MJ. Pharmacological and non-pharmacological treatment preferences of healthcare professionals and proxies for challenging behaviors in patients with dementia. Int Psychoger. (2017) 29:1377–89. doi: 10.1017/S1041610217000485
95. Li W, Xu X, Wu F, Ni Y, Lan J, Hu X. Comparative efficacy of non-pharmacological interventions on behavioral and psychological symptoms in elders with dementia: A network meta-analysis. Nurs Open. (2021) 8:2922–31. doi: 10.1002/nop2.1049
Keywords: mind-body therapies, older people, dementia, mental health, gerontology
Citation: Mei Z, Cai C, Wang T, Zhang Y, Zhao W, Lam C, Luo S, Shi Y and Luo S (2025) Are mind-body therapies beneficial for older people with dementia? A Systematic Review and meta-analysis of randomized controlled trials. Front. Psychiatry 16:1569709. doi: 10.3389/fpsyt.2025.1569709
Received: 01 February 2025; Accepted: 12 March 2025;
Published: 14 April 2025.
Edited by:
Yibo Wu, Peking University, ChinaReviewed by:
Andrew Clifton, University of Suffolk, United KingdomCopyright © 2025 Mei, Cai, Wang, Zhang, Zhao, Lam, Luo, Shi and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shi Luo, bHVvc2hpMDYwNEAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.