
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 11 April 2025
Sec. Addictive Disorders
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1562622
 Lorenzo Zamboni1,2*
Lorenzo Zamboni1,2* Giulia Benvegnù3
Giulia Benvegnù3 Francesca Fusina4
Francesca Fusina4 Roberta Vesentini5Francesca Locatelli5
Roberta Vesentini5Francesca Locatelli5 Matteo Mattiello1,3
Matteo Mattiello1,3 Vanessa Mannari6Simone Campagnari1Silvia Toldo3
Vanessa Mannari6Simone Campagnari1Silvia Toldo3 Alessio Congiu1Maria Brendolan1
Alessio Congiu1Maria Brendolan1 Giuseppe Verlato5*
Giuseppe Verlato5* Cristiano Chiamulera3
Cristiano Chiamulera3 Fabio Lugoboni1
Fabio Lugoboni1Introduction: Benzodiazepines (BDZs) are among the most abused substances worldwide, and high-dose BDZ abuse is considered a specific type of addiction. Cue reactivity (CR) is a hypersensitivity to motivational stimuli and, in substance use disorders, it increases craving and facilitates relapse, especially in chronic users. Virtual reality (VR) may be a viable technology to implement in CR paradigms. The general objective of this study is the implementation of a VR protocol to identify the causal relationship between the environmental features of a specific setting and craving responses in BDZ abusers.
Methods: Moreover, we investigated the correlation between the degree of BDZ craving and measures of mood, affect, attention, sense of presence, and cybersickness in the subjects, and evaluated the effectiveness that different VR environments have in discriminating between BDZ abusers and controls by comparing the degree of BDZ craving and all of the aforementioned variables in the two groups.
Results: Our data suggest that cues can indeed become conditioned to elicit craving responses in high-dose BDZ abusers, but more studies are necessary to confirm this hypothesis.
Conclusion: Moreover, the use of VR can be a good choice to observe environmental craving for BDZs since it presents a realistic simulation of real-world settings.
Benzodiazepines (BDZs) are positive allosteric modulators of the GABA-A (Gamma-Aminobutyric Acid Type A) receptor (1) and they are widely employed in the treatment of insomnia and anxiety. Despite their widespread use, studies have shown that BDZs should only be prescribed in specific clinical conditions and preferably either intermittently or for short periods of time (2–5). Long-term BDZ use is found in 6% to 76% of total BDZ users (6). It is associated with both adverse effects and dependence, and, therefore, it should only be considered with extreme caution. In particular, it has been associated with cognitive impairments in attention, memory and learning, as well as to a higher risk of incurring in accidents, cognitive decline and delirium (7–16). Moreover, 15 to 44% of long-term BDZ users present moderate-to-severe withdrawal symptoms, and 3–4% exhibit dependence (6).
High-dose (HD) BDZ dependence is considered a specific substance use disorder (SUD) (17), and it has shown to be consistently associated with a lower quality of life (18, 19). A study conducted in Switzerland reports HD BDZ abusers being around 1.5 million in Europe and 600000 in the United States (20), while a cross-sectional survey in France, Germany, Italy, and the UK, reported that approximately 0.14% of the general population took higher-than-recommended doses of anxiolytic drugs (21).
The recommended treatment to reduce BDZs’ impairing withdrawal symptoms comprises either gradual tapering of the dosage or the substitution of the target BDZ with an equivalent dose of another long-acting benzodiazepine, followed by tapering (22, 23).
Concerning the concurrent use of other drugs, it has been noted that BDZs are usually secondary drugs of abuse for most patients. Opioids (54.2%) and alcohol (24.7%) are the two substances that patients most commonly abuse in association with BDZs. Jones et al., in their 2012 review, reported that about 1 in 5 people who abuse alcohol also abuse BDZs.
Craving is one of the most important criteria in the diagnosis of substance use disorders (SUDs; 24) and it is described as a sudden urge to consume a substance of interest (25, 26). This behavior often escalates into compulsively seeking the substance and other conduct related to substance use (27, 28). Indeed, craving is crucial in maintaining abstinence in the long term, and it also has an important impact on other factors, such as the development of the SUD itself, as well as on the course of the treatment (29–31).
Cue reactivity (CR) is a hypersensitivity to motivational stimuli and situations (32). It is considered an adaptive response to environmental cues that represent salient information that the person processes and learns. It can be evaluated psychologically (by assessing changes in mood, craving ratings), physiologically (via skin conductance and heart rate) and behaviorally (gestures/actions) (33). In SUDs, CR is particularly relevant since it increases craving and facilitates relapse. Indeed, subjects that chronically abuse various substances are particularly sensitive to stimuli and situations that have been linked to the pleasurable effects of the target substance (34). In this respect, CR is an evolutionary response which may be both a risk factor, when cues are present, and a protective one, when cues are absent: for example, relapse in smokers has been shown to be reduce in households with no smoking-related cues (35). For this reason, studying the characteristics and the protective or potentially unfavorable valence of various contexts, including external environments, is crucial in the treatment and prevention of abuse-related behaviors. It is also important to use this information in the design of motivationally healthy environments for patients (36). Indeed, the role of domestic and urban settings in inducing goal-directed behaviors is still largely unknown, although the effects of spatial features on affect and perception have been widely examined (37).
Considering this, virtual reality (VR) may be a viable technology to implement in CR paradigms (29, 38, 39). VR simulates multisensory real-life contexts and environments, which are presented in 3D and comprise auditory, visual and/or tactile inputs (40). Compared with traditional CR paradigms, such as photos or 2D images, VR would thus have the advantage of being more ecological, enhancing participants’ sense of presence, a state of mind in which virtual environments are perceived as similar to real-world ones. This would increase the validity of this research method compared with traditional ones (41–43).
Furthermore, technical VR features such as immersion within the VR environment, the inclusion of substance-related cues, the presentation of highly realistic settings, and allowing subjects to actively interact with the system through real-time feedback would further enhance this method’s efficacy (44–47).
To the best of our knowledge, there are currently no studies in literature that examine CR and VR in BDZ abuse. Some research groups have investigated CR, smoking and alcohol abuse (45, 48, 49) and have emphasized the influence that environmental settings have on craving in alcoholism and smoking.
This study has several aims: the general objective of the study is the implementation of a VR protocol for the purpose of identifying the causal relationship between environmental features of a specific setting and craving responses in BDZ abusers.
Also, there are two secondary objectives: 1) investigating the correlation between the degree of BDZ craving in the various scenarios and measures of mood, affect, attention, sense of presence, and cybersickness in subjects who abuse BDZs (50); 2) the evaluation of the effectiveness that the three different VR environments have in discriminating between BDZ abusers and control subjects by comparing the degree of BDZ craving and measures of mood, affect, attention, sense of presence, and VR malaise in the control group vs those in the experimental group.
This research is an experimental study based on the study protocol by Zamboni et al. (51). It aimed to measure the degree of BDZ craving induced by VR exposure to environments containing cues associated with BDZ use after immersion in a VR setting.
The study consisted in a single session lasting approximately 45 mins. Participants filled out the Profile of Mood States (POMS) questionnaire before and after the session as a pre-VR baseline measure concerning their mood and affective state. After a 3-minute VR baseline, we administered three scenarios, each lasting 3 minutes. After the baseline and each of the scenarios, subjects were required to fill out the VAS to report craving, and a modified version of the Alcohol Attention Scale (AAS) questionnaire. At the end of the experimental session, in addition to the POMS, subjects were also asked to fill in the Presence Questionnaire (PQ) to assess their sense of presence, and the Simulator Sickness Questionnaire (SSQ) to assess the presence of possible adverse effects due to VR exposure.
Approval for the research was obtained from the Ethics Committee for Clinical Trials (CESC) of the Provinces of Verona and Rovigo based at the Integrated University Hospital of Verona, Italy (approval code: 3624CESC with Protocol No. 16883 of 09-03-2022). The latest revision of the Declaration of Helsinki as well as the Oviedo Declaration was the basis for the ethical conduct of the study. The study protocol was designed and conducted to ensure adherence to the principles and procedures of Good Clinical Practice and to comply with Italian law, as described in the following documents and accepted, by signature, by the study investigators: ICH Harmonized Tripartite Guidelines for Good Clinical Practice 1996. Directive 91/507/EEC, The Rules Governing Medicinal Products in the European Community. D. L.vo n. 211 of June 24, 2003. D. L.vo n. 200, November 6 2007. Ministerial Decree of December 21, 2007. AIFA Determination, March 20, 2008. All essential clinical records will be retained to demonstrate the validity of the study and the integrity of the data collected. The promoter of this study, in accordance with the responsibilities required by the rules of good clinical practice (Legislative Decree 211/2003) and in accordance with the laws and regulations regarding data protection (including the European Regulation on the protection of personal data 2016/679), will process the personal data that will be collected exclusively for the implementation of the study and for the purpose of device surveillance.
The sample was composed by fifty-four native Italian speakers of both sexes (males = 28; age range = 18-65 years), with an average age of 36.89 years (SD ± 11.89).
The following inclusion criteria were applied to the experimental group (N = 27, males = 13): i) BDZ use disorder diagnosis following DSM 5TR criteria (24); ii) being ready to start a treatment at the Addiction Medicine Unit due to the inability to autonomously quit BDZ use; iii) high-dose BDZ abuse (i.e., BDZ intake must be at least five times higher than the defined maximum daily dose -DDD-).
In contrast, the control group (N = 27, males = 15) included subjects without SUDs (including a BDZ use disorder) according to ICD 10 F10-F19.
The following exclusion criteria were applied to both groups: i) having a history of epilepsy or having first-degree family members with epilepsy; ii) having a history of severe cardiovascular or chronic disease; iii) pregnancy; iv) presence of a cardiac pacemaker or other metallic devices on the head and neck, with the exception of piercings and dental braces; v) intake of psychoactive substances which may have interfered with the results of the study.
We used the HTC-Vive VR device, consisting of a Head Mounted Display (HMD), two controllers for interacting with the virtual environment, and two external infrared sensors. All VR scenarios (Figure 1) were modelled with the software Blender 2.8 and implemented in Unity 2017.4. Four scenarios were developed: i), a tutorial environment to familiarize participants with VR technology, consisting of a room with a graspable object (a cube). This is the only scenario in which subjects could interact with the experimenter; ii), a neutral scenario representing the entrance of a house. In this scenario, the subject could move freely in the virtual environment, but there were no interactive objects; iii), the No Cue scenario. In this scenario, representing a bedroom, the subject could move freely but no interactive objects were present; and iv), the Cue scenario. This scenario represents the same bedroom as the No Cue scenario but in this case the subject, in addition to moving freely, could interact with BDZ-related graspable objects (i.e., a bottle of Lormetazepam and a box of Alprazolam tablets).

Figure 1. Virtual Reality scenarios. The tutorial scenario (A), the neutral scenario (B), the No Cue scenario (C) and the Cue scenario (D).
For a more detailed description of the materials and methods, and in particular of the measures used, see Zamboni et al., (51). The questionnaires employed in the present study are given below.
-Ad hoc questionnaire to measure Benzodiazepine (BDZ) craving. The instrument consists of a single-item 10-point scale based on the literature and adapted from Benvegnù et al. (49) and Traylor et al. (48), with a score ranging from 0 (absent) to 9 (extreme).
-Ad hoc questionnaire to measure the attention given to BDZ-related cues. The questionnaire is a modified version of the Alcohol Attention Scale (AAS) (52) and it consists of two BDZ-themed questions investigating the attention paid to BDZs (item 1) and the intention to use them (item 2), with an 11-point response scale ranging from 0 to 10.
-Profile of Mood States (POMS). The questionnaire (53) comprises 58 items, with a 5-point scale response, measuring six factors: Tension/Anxiety (T), Depression/Dejection (D), Anger/Hostility (A), Vigor/Activity (V), Fatigue/Inertia (S), and Confusion/Bewilderment (C). The total score is calculated as the sum of the five negative scales (T, D, A, S) minus the positive one (V).
-Simulator Sickness Questionnaire (SSQ). The possible presence of symptoms associated with cybersickness was assessed using the SSQ (54). The questionnaire consists of 16 items, 4-point response scale, and provides a total score and 3 subscales (Nausea, Oculomotor Disturbance, and Disorientation).
-Presence Questionnaire (PQ). The perception of “being present” in the virtual environment was measured using the PQ (55), a questionnaire with a 7-point scale response.
Each participant was asked to sit in the VR station and received all the necessary information regarding the experiment. After signing the informed consent and verification of eligibility, the subject filled out the questionnaires. Before the VR session began, the POMS and the craving questionnaire were administered (Figure 2). The experimenter then instructed the participant on how to use the HTC-VIVE VR device and how to move in the virtual environment. The first scenario was a 3-min baseline simulation (tutorial scenario) during which the subject familiarized with VR and practiced with the device. In a fixed sequence, the other three scenarios were administered, for 3 minutes each: house entrance (neutral scenario), bedroom without BDZs (No Cue scenario), and bedroom with BDZ bottles (Cue scenario). The participant did not have to undertake a specific task but could freely explore the virtual environments by using the joystick and moving their head. At the end of each scenario, the subject removed the visor and headphones and filled out the craving questionnaire and the modified AAS. At the end of the last one, the craving questionnaire, the modified AAS, the POMS, the SSQ, and the PQ were administered. All procedures were approved by the local academic ethical committee (Ethics Committee for Clinical Trials -CESC- of the Provinces of Verona and Rovigo; approval code: 3624CESC with Protocol No. 16883 of 09-03-2022) and followed the principles of the Declaration of Helsinki.
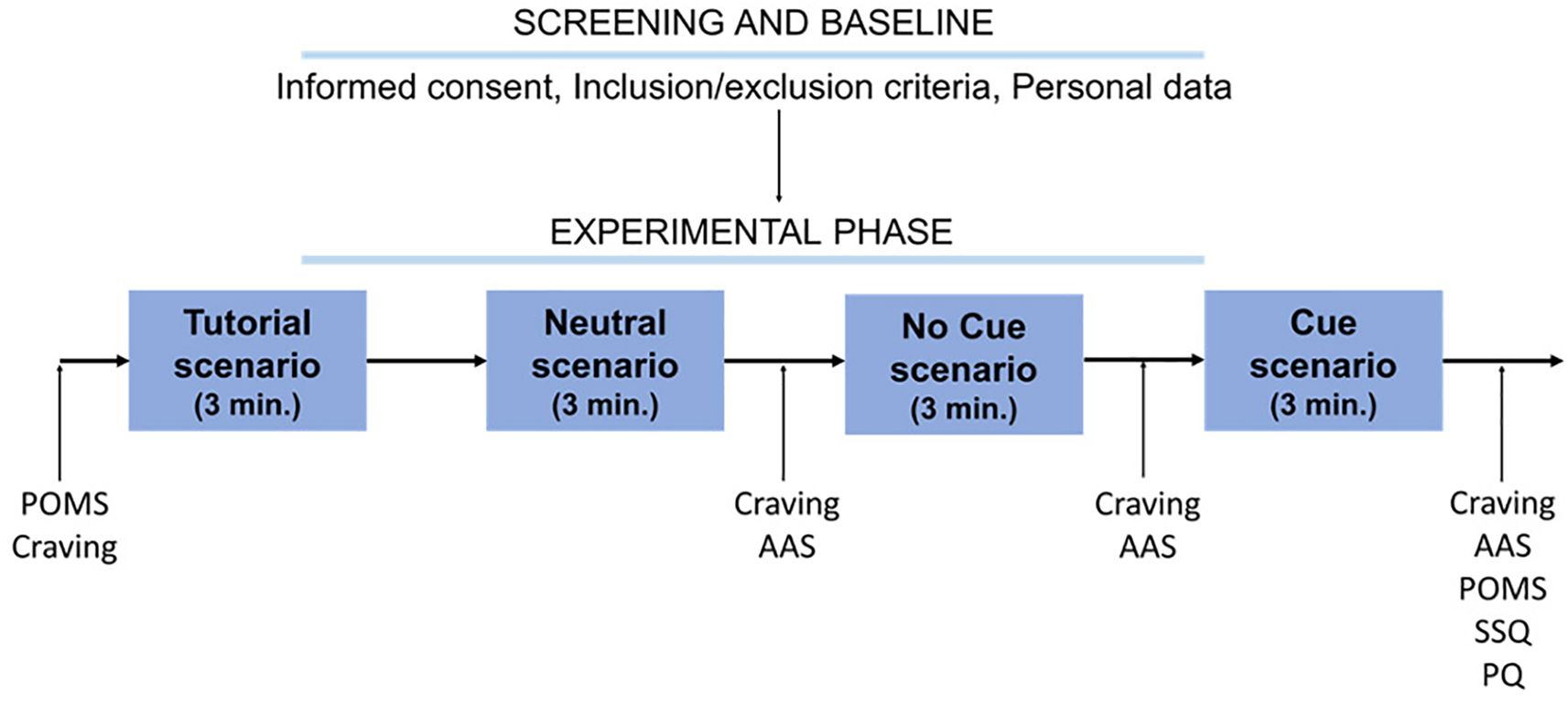
Figure 2. Schematic representation of the procedure. POMS, Profile of Mood States; Craving, craving ad hoc questionnaire; AAS, modified Alcohol Attention Scale; SSQ, Simulator Sickness Questionnaire; PQ, Presence Questionnaire.
Sample size was estimated by using the G*Power 3.1.5.1 software (56) with an a-priori analysis (α level: 0.017, power level, 1-β: 0.80, effect size f: 0.7. For more details on sample size computation see Zamboni et al., 51).
Since the assumptions for the ANOVA were violated, a Friedman test was performed to test for craving differences between the different timepoints in the experimental group. In case of significance, Dunn’s multiple comparison tests were conducted. The same analysis was also carried out for the scores of the two items in the modified version of the AAS (henceforth, AAS 1 and AAS 2).
To test whether the No Cue and Cue scenarios elicited an effect on the experimental group compared with the control group, a Mann-Whitney series was performed for craving, AAS 1 and AAS 2 scores.
To check for possible associations between craving and the other measures, Spearman correlations were made between the craving, AAS 1 and AAS 2, POMS, SSQ, and PQ scores measured at the same timepoints in the experimental group.
All statistical analyses were conducted using the GraphPad Prism 9.1.0. software (GraphPad, CA, USA).
The Friedman test on craving scores showed no significant differences between the different timepoints [χ2(3) = 6.45, p = 0.09]. In contrast, the Friedman test on AAS 1 was statistically significant [χ2(2) = 45.23, p < 0.0001]. Post-hoc comparisons (Figure 3) showed a significant increase in scores in the Cue scenario, both compared to the neutral scenario (p < 0.0001) and compared to the No Cue scenario (p < 0.0001). The Friedman test of AAS 2 showed no significant differences [χ2(2) = 5.09, p = 0.07].
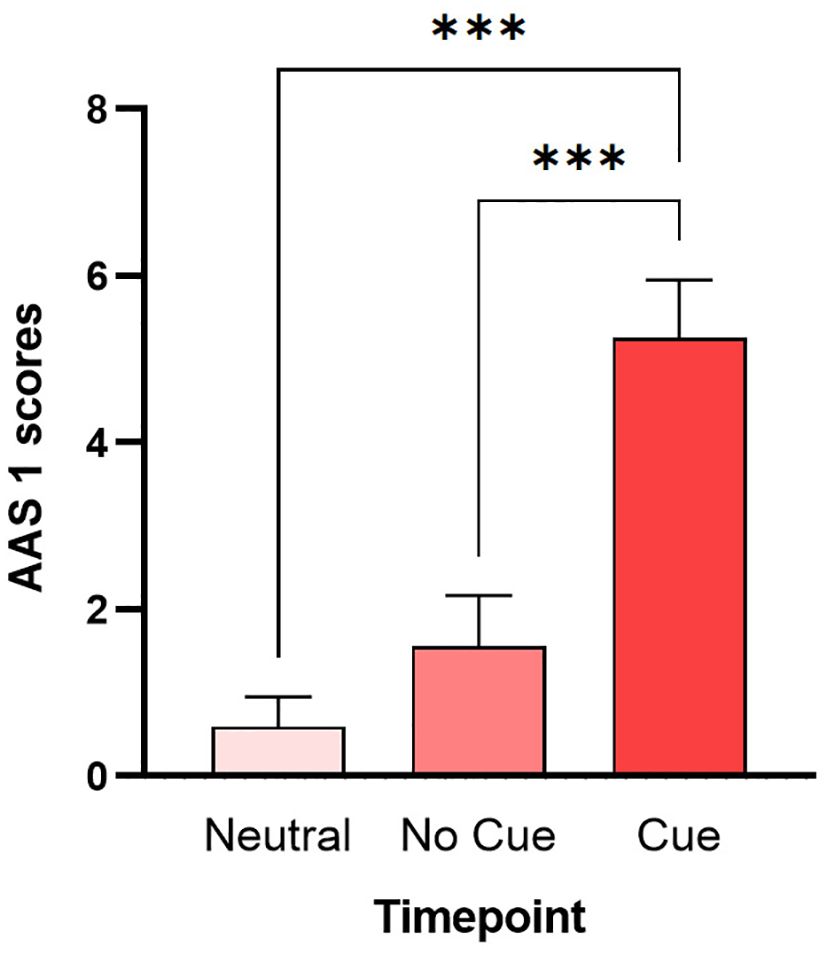
Figure 3. Multiple comparisons of AAS 1. Bars represent the average scores and the S.E.M. of AAS 1 measured after the neutral scenario (Neutral), after the bedroom without BDZs (No Cue), and after the bedroom with BDZ bottles (Cue). *** (p < 0.001) (Dunn’s multiple comparisons test).
The Mann-Whitney on craving scores showed greater craving in the experimental group than in the control group in both the No Cue scenario (U = 290.5, p = 0.031) and the Cue scenario (U = 248, p = 0.006) (Figure 4). In contrast, the Mann-Whitneys of AAS 1 and AAS 2 did not reveal significant differences.
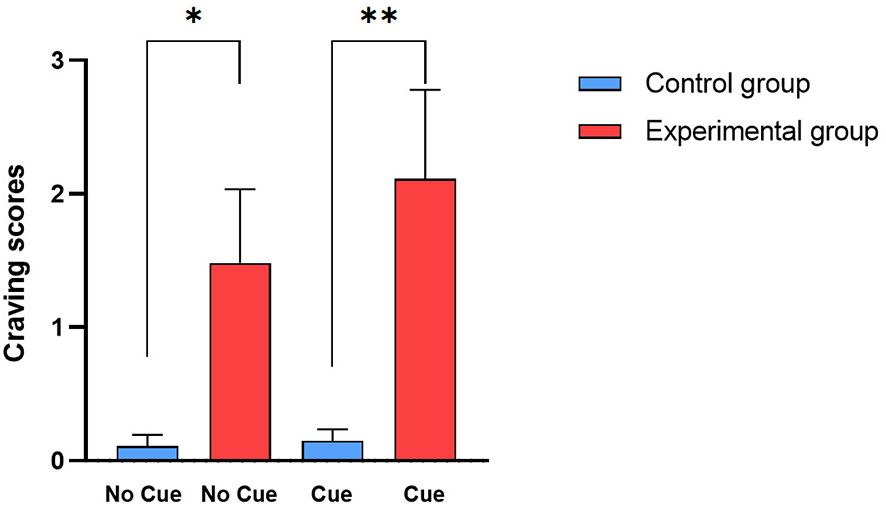
Figure 4. Mann-Whitney of craving scores. Bars represent the average scores and the S.E.M. of craving measured after the bedroom without BDZs (No Cue) and after the bedroom with BDZ bottles (Cue) in the control group (cyan bars) and in the experimental group (red bars). * (p < 0.05) and ** (p < 0.01) (Mann-Whitney test).
Regarding correlational analyses, craving scores correlated positively with AAS 2 measured after the neutral scenario (rs = 0.62, p = 0.001), after the No Cue scenario (rs = 0.63, p = 0.001) and after the Cue scenario (rs = 0.80, p < 0.0001) and with AAS 1 scores measured after the Cue scenario (rs = 0.51, p = 0.018). AAS 1 and AAS 2 scores measured after the neutral scenario show a positive correlation (rs = 0.58, p = 0.003) (Figure 5).
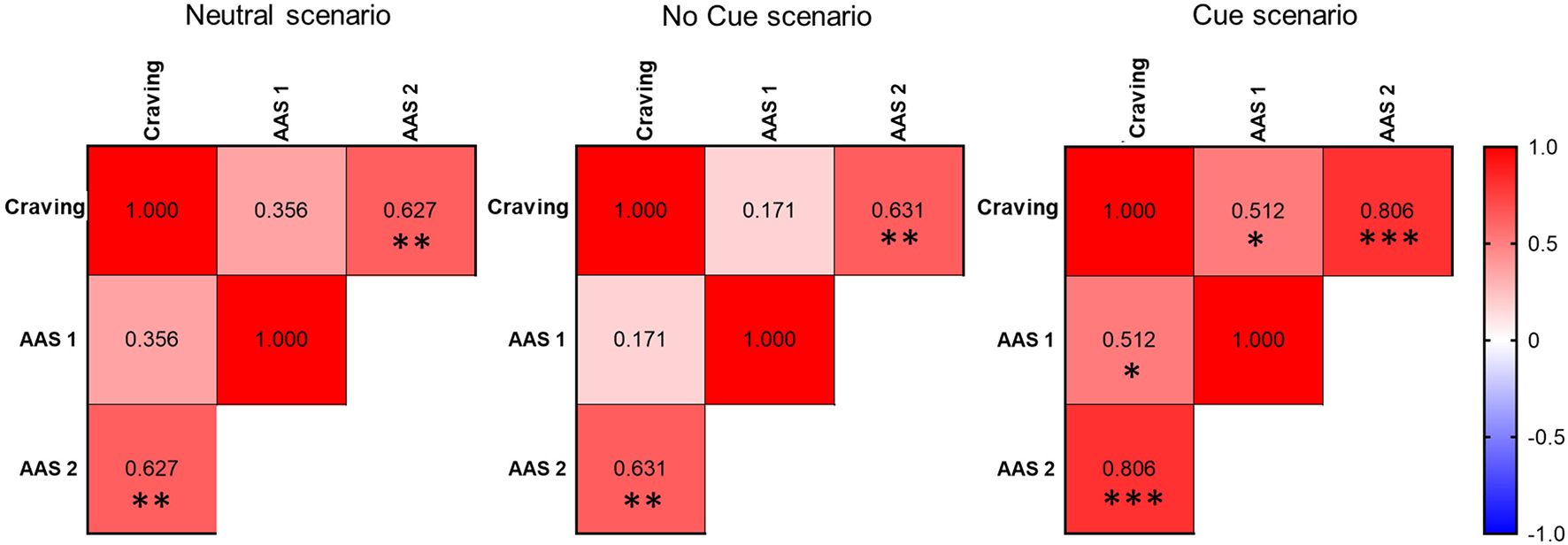
Figure 5. Correlational analysis. Heat map of correlations between craving, AAS 1, and AAS 2 scores measured after the neutral scenario, after the No Cue scenario, and after the Cue scenario. Spearman’s Rho are shown in the cells. * (p < 0.05), ** (p < 0.01) and *** (p < 0.001).
Several papers address BDZ craving, but they address it as a factor concerning abstinence rather than environmental cues (6, 17). There is only a study by McHough et al. (57) that suggests BDZ cues can become conditioned to elicit craving responses and that the degree of cue reactivity is correlated with known risk factors for benzodiazepine misuse. However, this study does not use VR and presents a heterogeneous sample. To overcome these methodological issues, we have included only monoabusers of high-dose BDZs in our study. Furthermore, we used VR to observe if the BDZ cues could elicit a craving response in a sample of BDZ high-dose abusers.
The results show that the experimental group showed an increased attention to BDZ-related stimuli compared to other scenarios in which there were no related cues. This result confirms our expectations and is in agreement with other studies on alcohol and tobacco addiction (58, 59).
Regarding craving, we observed a difference between the control group and the experimental group at the VAS craving scales. The experimental group registered higher craving levels both in no cue and cue scenarios. Similar data was found in studies examining other addictions, particularly tobacco and alcohol (60–63).
Moreover, our study revealed a correlation between craving and attention to BDZs, and between craving and the desire to use BDZ. These data support the hypothesis of cue reactivity in high-dose BDZ abusers. Indeed, the presence of BDZ-related cues in the virtual scenario elicits craving, attention towards BDZs and the desire to use these drugs.
Our study confirms the feasibility of VR as a research method because no subjects withdrew from the experiment due to motion sickness or other issues related to VR simulation; this data is therefore encouraging concerning the use of VR to observe behaviors related to BDZ addiction.
This is the first study analyzing CR in the high-dose BDZ abuser population, revealing a correlation between these two aspects. The data is significant as it has never been collected before. Additionally, this aspect may pave the way for new future therapeutic scenarios, placing greater emphasis on the lifestyle context of this type of patients. Just like with other substance addictions (alcohol, smoking, etc.), intervening in such a context could lead to a reduction in the number of relapses.
In addition, the use of VR in the treatment of high dose BDZ abuser could become a valuable clinical tool. However, as emphasized in the review written by Wiebe et al. (64), the times are not yet ripe to strongly assert the effectiveness of this methodology. In this regard, further studies will be needed.
Our study presents several limitations: we measured craving using only a VAS scale; also, the sample is small, and although we have respected the initial power analysis results, nevertheless a large sample size could strengthen our results, finally, we did not collect certain sociodemographic information (time of onset of BDZ use disorder, the lifetime use of other substances, or a family history of SUD and other psychiatric diseases) that could have enriched the analysis. Another potential bias could be the mean age difference between two groups, and also the fact that the patients’ BDZ intake data were missing. This aspect could increase data specificity, since, in our study, the BDZ dosage was only self-reported by the subjects.
Our data suggest that cues can indeed become conditioned to elicit craving responses in BDZ high-dose abusers, but more studies are necessary to confirm this hypothesis. Moreover, the use of VR can be a good choice to observe environmental craving for BDZs since it presents a realistic simulation. Future studies could measure craving by using more objective measures (EEG, heart rate, skin conductance etc.), and not only in high-dose abusers but also in long-term abusers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comitato etico per la sperimentazione clinica delle province di Verona e Rovigo degli studi No profit. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LZ: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. GB: Formal analysis, Methodology, Writing – original draft. FF: Writing – review & editing. RV: Data curation, Formal analysis, Methodology, Writing – review & editing. FrL: Formal analysis, Methodology, Writing – review & editing. MM: Data curation, Writing – review & editing. VM: Data curation, Investigation, Writing – review & editing. SC: Investigation, Writing – review & editing. ST: Conceptualization, Data curation, Investigation, Writing – review & editing. AC: Investigation, Writing – review & editing. MB: Investigation, Writing – review & editing. GV: Formal analysis, Methodology, Writing – review & editing. CC: Conceptualization, Supervision, Writing – review & editing. FaL: Conceptualization, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Soyka M. Treatment of benzodiazepine dependence. New Engl J Med. (2017) 376:1147–57. doi: 10.1056/NEJMra1611832
2. Baldwin DS, Aitchison K, Bateson A. Benzodiazepines: Risks and benefits. A reconsideration. J Psychopharmacol. (2013) 27:967–71. doi: 10.1177/0269881113503509
3. Lader M. Benzodiazepine harm: How can it be reduced? Br J Clin Pharmacol. (2014) 77:295–301. doi: 10.1111/j.1365-2125.2012.04418.x
4. López-Muñoz F, Alamo C, García-García P. The discovery of chlordiazepoxide and the clinical introduction of benzodiazepines: Half a century of anxiolytic drugs. J Anxiety Disord. (2011) 25:554–62. doi: 10.1016/j.janxdis.2011.01.002
5. Sirdifield C, Anthierens S, Creupelandt H. General practitioners’experiences and perceptions of benzodiazepine prescribing: Systematic review and meta-synthesis. BMC Family Pract. (2013) 14:191. doi: 10.1186/1471-2296-14-191
6. Faccini M, Leone R, Opri S, Casari R, Resentera C, Morbioli L, et al. Slow subcutaneous infusion of flumazenil for the treatment of long-term, high-dose benzodiazepine users: A review of 214 cases. J Psychopharmacol. (2016) 30:1047–53. doi: 10.1177/0269881116647505
7. Barker MJ, Greenwood KM, Jackson M, Crowe SF. Cognitive effects of long-term benzodiazepine use: A meta-analysis. CNS Drugs. (2004) 18:37–48. doi: 10.2165/00023210-200418010-00004
8. Boeuf-Cazou O, Bongue B, Ansiau D, Lapeyre-Mestre M. Impact of long-term benzodiazepine use on cognitive functioning in young adults: The VISAT cohort. Eur J Clin Pharmacol. (2011) 67:1045–52. doi: 10.1007/s00228-011-1047-y
9. Finkle WD, Der JS, Greenland S, Adams JL, Ridgeway G, Blaschke T, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J Am Geriatrics Soc. (2011) 59:1883–90. doi: 10.1111/j.1532-5415.2011.03591.x
10. Fond G, Berna F, Boyer L, Godin O, Brunel L, Andrianarisoa M. Benzodiazepine long-term administration is associated with impaired attention/working memory in schizophrenia: Results from the national multicentre FACE-SZ data set. Eur Arch Psychiatry Clin Neurosci. (2018) 268:17–26. doi: 10.1007/s00406-017-0787-9
11. Helmes E, Østbye T. Associations between benzodiazepine use and neuropsychological test scores in older adults. Can J Aging. (2015) 34:207–14. doi: 10.1017/S0714980815000082
12. Kok L, Slooter AJ, Hillegers MH, van Dijk D, Veldhuijzen DS. Benzodiazepine use and neuropsychiatric outcomes in the ICU: A systematic review. Crit Care Med. (2018) 46:1673–80. doi: 10.1097/CCM.0000000000003300
13. Picton JD, Marino AB, Nealy KL. Benzodiazepine use and cognitive decline in the elderly. Am J Health-System Pharm. (2018) 75:e6–e12. doi: 10.2146/ajhp160381
14. Puustinen J, Laühteenmaüki R, Polo-Kantola P, Salo P, Vahlberg T, Lyles A, et al. Effect of withdrawal from long-term use of temazepam, zopiclone or zolpidem as hypnotic agents on cognition in older adults. Eur J Clin Pharmacol. (2014) 70:319–29. doi: 10.1007/s00228-013-1613-6
15. van der Sluiszen NNJJM, Vermeeren A, Jongen S, Jongen S, Vinckenboschm F, Ramaekers JG. Influence of long-term benzodiazepine use on neurocognitive skills related to driving performance in patient populations: A review. Pharmacopsychiatry. (2017) 50:189–96. doi: 10.1055/s-0043-112755
16. Wedmann F, Himmel W, Nau R. Medication and medical diagnosis as risk factors for falls in older hospitalized patients. Eur J Clin Pharmacol. (2019) 75:1117–24. doi: 10.1007/s00228-019-02668-3
17. Tamburin S, Faccini M, Casari R, Federico A, Morbioli L, Franchini E, et al. Low risk of seizures with slow flumazenil infusion and routine anticonvulsant prophylaxis for high-dose benzodiazepine dependence. J Psychopharmacol. (2017) 31:1369–73. doi: 10.1177/0269881117714050
18. Lugoboni F, Mirijello A, Faccini M, Casari R, Cossari A, Musi, et al. Quality of life in a cohort of high-dose benzodiazepine dependent patients. Drug Alcoh. Depend. (2014) 142:105–9. doi: 10.1016/j.drugalcdep.2014.06.020
19. Tamburin S, Federico A, Faccini M, Casari R, Morbioli L, Sartore V, et al. Determinants of quality of life in high-dose benzodiazepine misusers. Int J Environ Res Public Health. (2017) 14:38. doi: 10.3390/ijerph14010038
20. Petitjean S, Ladewig D, Meier CR, Amrein R, Wiesbeck GA. Benzodiazepine prescribing to the Swiss adult population: Results from a national survey of community pharmacies. Int Clin Psychopharmacol. (2007) 22:292–8. doi: 10.1097/YIC.0b013e328105e0f2
21. Ohayon MM, Lader MH. Use of psychotropic medication in the general population of France, Germany, Italy, and the United Kingdom. J Clin Psychiatry. (2002) 63:817–25. doi: 10.4088/jcp.v63n0912
22. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. (2005) 18:249–55. doi: 10.1097/01.yco.0000165594.60434.84
23. Lader M. Benzodiazepines revisited–will we ever learn? Addiction. (2011) 106:2086–109. doi: 10.1111/j.1360-0443.2011.03563.x
24. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed. (2022). doi: 10.1176/appi.books.9780890425787
25. Drummond DC. Theories of drugs craving, ancient and modern. Addiction. (2001) 96:33–46. doi: 10.1046/j.1360-0443.2001.961333.x
26. Hartwell EE, Ray LA. Craving as a DSM-5 symptom of alcohol use disorder in non-treatment seekers. Alcohol Alcohol. (2018) 53:235–40. doi: 10.1093/alcalc/agx088
27. Carvalho AF, Heilig M, Perez A, Probst C, Rehm J. Alcohol use disorders. Lancet. (2019) 394:781–92. doi: 10.1016/S0140-6736(19)31775-1
28. Grodin EN, Lim AC, MacKillop J, Karno MP, Ray LA. An examination of motivation to change and neural alcohol cue reactivity following a brief intervention. Front Psychiatry (2019) 10:408. doi: 10.3389/fpsyt.2019.00408
29. Hone-Blanchet A, Wensing T, Fecteau S. The use of virtual reality in craving assessment and cue-exposure therapy in substance use disorders. Front Hum Neurosci. (2014) 8:844. doi: 10.3389/fnhum.2014.00844
30. Keyes KM, Krueger RF, Grant BF, Hasin DS. Alcohol craving and the dimensionality of alcohol disorders. Psychol Med. (2011) 41:629–40. doi: 10.1017/S003329171000053X
31. Stohs ME, Schneekloth TD, Geske JR, Biernacka JM, Karpyak VM. Alcohol craving predicts relapse after residential addiction treatment. Alcohol Alcohol. (2019) 54:167–72. doi: 10.1093/alcalc/agy093
32. Chiamulera C. Cue reactivity in nicotine and tobacco dependence: a "dual-action" model of nicotine as a primary reinforcement and as an enhancer of the effects of smoking -associated stimuli. Brain Res Rev. (2005) 48:74–97. doi: 10.1016/j.brainresrev.2004.08.005
33. Betts JM, Dowd AN, Forney M, Hetelekides E, Tiffany ST. A meta-analysis of cue reactivity in tobacco cigarette smokers. Nicotine Tob Res. (2021) 23:249–58. doi: 10.1093/ntr/ntaa147
34. Shiffman S, Hickox M, Paty JA, Gnys M, Kassel JD, Richards TJ. Progression from a smoking lapse to relapse: prediction from abstinence violation effects, nicotine dependence, and lapse characteristics. J Consult Clin Psychol. (1996) 64:993–1002. doi: 10.1037/0022-006X.64.5.993
35. Gilpin EA, Messer K, Pierce JP. Population effectiveness of pharmaceutical aids for smoking cessation: what is associated with increased success? Nicotine Tob. Res. (2006) 8:661–9. doi: 10.1080/14622200600910801
36. Chiamulera C, Ferrandi E, Benvegnù G, Ferraro S, Tommasi F, Maris B, et al. Virtual reality for neuroarchitecture: cue reactivity in built spaces. Front Psychol. (2017) 8:185. doi: 10.3389/fpsyg.2017.00185
37. Ulrich RS. Effects of interior design on wellness: theory and recent scientific research. J Health Care Inter. Des. (1991) 3:97–109.
38. Ghiţă A, Gutiérrez-Maldonado J. Applications of virtual reality in individuals with alcohol misuse: A systematic review. Addict. Behav. (2018) 81:1–11. doi: 10.1016/j.addbeh.2018.01.036
39. Segawa T, Baudry T, Bourla A, Blanc JV, Peretti CS, Mouchabac S, et al. Virtual reality in assessment and treatment of addictive disorders: A systematic review. Front Neurosci. (2019) 13:1409. doi: 10.3389/fnins.2019.01409
40. Bohil CJ, Alicea B, Biocca FA. Virtual reality in neuroscience research and therapy. Nat Rev Neurosci. (2011) 12:752–62. doi: 10.1038/nrn3122
41. Gutiérrez-Maldonado J, Ferrer-García M, Dakanalis A, Riva G. Virtual Reality: Applications to eating disorders. In: Oxford Hand Eat Disor (UK Oxford University Press) (2018). p. 470–91.
42. Iachini T, Maffei L, Masullo M, Senese VP, Rapuano M, Pascale A, et al. The experience of virtual reality: Are individual differences in mental imagery associated with sense of presence? Cogn. Process. (2019) 20:291–8. doi: 10.1007/s10339-018-0897-y
43. Riva G. Virtual reality: An experiential tool for clinical psychology. Br J Guid. Counc. (2009) 37:335–43. doi: 10.1080/03069880902957056
44. Lee J, Kim M. A study on immersion and VR sickness in walking interaction for immersive virtual reality applications. Symmetry. (2017) 9:78–95. doi: 10.3390/sym9050078
45. Bordnick PS, Traylor A, Copp HL, Graap KM, Carter B, Ferrer M, et al. Assessing reactivity to virtual reality alcohol based cues. Addict Behav. (2008) 33:743–56. doi: 10.1016/j.addbeh.2007.12.010
46. Culbertson C, Nicolas S, Zaharovits I, London ED, Garza R, Brody AL, et al. Methamphetamine craving induced in an online virtual reality environment. Pharmacol Biochem Behav. (2010) 96:454–60. doi: 10.1016/j.pbb.2010.07.005
47. Saladin ME, Brady KT, Graap K, Rothbaum BO. A preliminary report on the use of virtual reality technology to elicit craving and cue reactivity in cocaine dependent individuals. Addict. Behav. (2006) 31:1881–94. doi: 10.1016/j.addbeh.2006.01.004
48. Traylor AC, Parrish DE, Copp HL, Bordnick TS. Using virtual reality to investigate complex and contextual cue reactivity in nicotine dependent problem drinkers. Addictive Behaviors. (2011) 36:1068–75. doi: 10.1016/j.addbeh.2011.06.014
49. Benvegnù G, Tommasi F, Ferraro S, Libener E, Di Chio M, Bosi S, et al. Smokers "Context reactivity" in virtual domestic environments. Eur Addict Res. (2021) 27:439–46. doi: 10.1159/000515301
50. Weech S, Kenny S, Barnett-Cowan M. Presence and cybersickness in virtual reality are negatively related: a review. Front Psychol (2019) 10:158. doi: 10.3389/fpsyg.2019.00158
51. Zamboni L, Toldo S, Fusina F, Mattiello M, Mannari V, Campagnari S, et al. Study protocol-Evoked craving in high-dose benzodiazepine users. Front Psychiatry. (2022) 13:956892. doi: 10.3389/fpsyt.2022.956892
52. Monti PM, Rohsenow D, Rubonis S, Niaura R, Sirota A, Colby S, et al. Alcohol cue-reactivity: Effects of detoxification and extended exposure. J Stud Alcohol. (1993) 54:235–45. doi: 10.15288/jsa.1993.54.235
53. Morfeld M, Petersen C, Krüger-Bödeker A, von Mackensen S, Bullinger M. The assessment of mood at workplace - psychometric analyses of the revised Profile of Mood States (POMS) questionnaire. Psychosoc Med. (2007) 4:Doc06.
54. Kennedy RSRS, Lane NENE, Berbaum KSKS, Lilienthal MGMG, Kevin S, Lilienthal MGMG. Simulator sickness questionnaire : an enhanced method for quantifying simulator sickness. Int J Aviation Psychol. (1993) 3:203–20. doi: 10.1207/s15327108ijap0303
55. Witmer BG, Jerome CJ, Singer MJ. The factor structure of the Presence Questionnaire. Presence: Teleoperators and Virtual Environments (2005) 14:298–312. doi: 10.1162/105474605323384654
56. Erdfelder E, Faul F, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Methods. (2009) 41:1149–60. doi: 10.3758/BRM.41.4.1149
57. McHugh RK, Korte FM, McCarthy MD, Geyer RB. A pilot study of benzodiazepine cue-induced craving. Drug Alcohol Depend. (2022) 235:109443. doi: 10.1016/j.drugalcdep.2022.109443
58. García-Rodríguez O, Pericot-Valverde I, Gutiérrez-Maldonado J, Ferrer-García M, Secades-Villa R. Validation of smoking-related virtual environments for cue exposure therapy. Addict Behav. (2012) 37:703–8. doi: 10.1016/j.addbeh.2012.02.013.S0306-4603(12)00066-4
59. Simon J, Etienne AM, Bouchard S, Quertemont E. Alcohol craving in heavy and occasional alcohol drinkers after cue exposure in a virtual environment: the role of the sense of presence. Front Hum Neurosci. (2020) 14:124. doi: 10.3389/fnhum.2020.00124
60. García-Rodríguez O, Weidberg S, Gutiérrez-Maldonado J, Secades-Villa R. Smoking a virtual cigarette increases craving among smokers. Addict Behav. (2013) 38:2551–4. doi: 10.1016/j.addbeh.2013.05.007
61. Ghiţă A, Teixidor L, Monras M, Ortega L, Mondon S, Gual A, et al. Identifying triggers of alcohol craving to develop effective virtual environments for cue exposure therapy. Front Psychol. (2019) 10:74. doi: 10.3389/fpsyg.2019.00074
62. Hernández-Serrano O, Ghiţă A, Fernández-Ruiz J, Monràs M, Gual A, Gacto M, et al. Determinants of cue-elicited alcohol craving and perceived realism in virtual reality environments among patients with alcohol use disorder. J Clin Med. (2021) 10:2241. doi: 10.3390/jcm10112241
63. Culbertson CS, Shulenberger S, de la Garza R, Newton TF, Brody AL. Virtual reality cue exposure therapy for the treatment of tobacco dependence. J Cyber Ther Rehabil. (2012) 5:57–64.
Keywords: cue reactivity, benzodiazepine, addiction, virtual reality, abuse
Citation: Zamboni L, Benvegnù G, Fusina F, Vesentini R, Locatelli F, Mattiello M, Mannari V, Campagnari S, Toldo S, Congiu A, Brendolan M, Verlato G, Chiamulera C and Lugoboni F (2025) Evoked craving in high-dose benzodiazepine users. Front. Psychiatry 16:1562622. doi: 10.3389/fpsyt.2025.1562622
Received: 17 January 2025; Accepted: 04 March 2025;
Published: 11 April 2025.
Edited by:
Liana Fattore, CNR Neuroscience Institute (IN), ItalyReviewed by:
Giovanni Biggio, University of Cagliari, ItalyCopyright © 2025 Zamboni, Benvegnù, Fusina, Vesentini, Locatelli, Mattiello, Mannari, Campagnari, Toldo, Congiu, Brendolan, Verlato, Chiamulera and Lugoboni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorenzo Zamboni, bG9yZW56by56YW1ib25pODhAZ21haWwuY29t; Giuseppe Verlato, Z2l1c2VwcGUudmVybGF0b0B1bml2ci5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.