 Solveig Kemna1*†
Solveig Kemna1*† Van Tuan Nguyen2,3†
Van Tuan Nguyen2,3† Kerem Böge1
Kerem Böge1 Malek Bajbouj1
Malek Bajbouj1 Max Bringmann1
Max Bringmann1 Sebastian Weyn-Banningh1
Sebastian Weyn-Banningh1 Luisa Eilinghoff1
Luisa Eilinghoff1 Van Phi Nguyen1,2,4
Van Phi Nguyen1,2,4 Laura Elisabeth Tuturea1
Laura Elisabeth Tuturea1 Thien Le Cong2,3
Thien Le Cong2,3 Thi Thu Ha Le2,3
Thi Thu Ha Le2,3 Thi Minh Tam Ta1†
Thi Minh Tam Ta1† Eric Hahn1†
Eric Hahn1†- 1Department of Psychiatry and Neuroscience, Charité University Medicine Berlin, Berlin, Germany
- 2Department of Psychiatry, Hanoi Medical University, Hanoi, Vietnam
- 3National Institute of Mental Health, Bach Mai Hospital, Hanoi, Vietnam
- 4Department of Mental Health, National Geriatric Hospital, Hanoi, Vietnam
Introduction: This cross-sectional, explorative study examines university students’ attitudes (n = 610) in Hanoi, Vietnam, toward the rights of psychiatric patients.
Methods: Medical students responded to self-report questionnaires investigating their attitudes towards restrictions and compulsory admissions in case of severe mental illness after attending a psychiatry course. Medical students and non-medical students who did not participate in the course served as two control groups.
Results: In all groups, the majority of students opposed restricting the civil rights of psychiatric patients, but most supported compulsory admissions in certain situations. Medical students who had not attended a psychiatry course were generally more in favor of compulsory admissions compared to those who had attended a psychiatry course and non-medical students. However, when investigating attitudes on compulsory admission in specific scenarios, students that had attended a psychiatry course were more likely to endorse compulsory admissions, except when admission was based on the patient’s family request.
Discussion: Medical and psychiatric training seem to encourage more differentiated opinions on the use of compulsory admissions in psychiatric care. Future research, including longitudinal designs and a broader geographical scope, is needed to better understand the impact of psychiatric education in medical studies on attitudes toward mental health.
1 Introduction
Although mental health care was defined as a national priority by the government in Vietnam, psychiatric infrastructure remains insufficient (1, 2). For every 100.000 inhabitants, there are 0.62 psychiatrists, and only 143 clinical psychologists and psychotherapists in the public health sector overall (3, 4). Additionally, the general population and many health professionals show limited mental health literacy (5, 6). This has been attributed at least partly to misinformation in the media regarding mental health, as well as the low number of licensed non-medical mental health professionals and psychiatrists (4). Negative attitudes toward psychiatry as a medical profession may discourage medical students from following a career in this field (7, 8). Moreover, undergraduate medical students often have only limited knowledge of psychiatric diagnoses and treatment, such as depression and anxiety, and show low proficiency in providing first-aid support to these populations (9–12).
This lack of understanding of mental illnesses and knowledge of psychiatric care can lead to negative beliefs and social distancing from psychiatric patients (13, 14) and, in turn, negatively impact the quality of provided health care and help-seeking behavior (10, 15, 16). Furthermore, societal stigmatization of psychiatric patients can also have broader implications. In many countries, persons with mental health disorders are still faced with the restriction of civil rights such as voting (17–19).
Attitudes toward the mental health care system and psychiatric conditions are also reflected in views on the role of compulsory admissions, i.e., admitting psychiatric patients – under certain conditions – against their will to a hospital. On the one hand, advocating for stricter policies of compulsory admissions can be interpreted as a sign of a desire for social distance and negative attitudes towards psychiatric patients as they might be deemed dangerous. On the other hand, support for compulsory admissions can also be a signal of trust in the mental health care system as a place where patients receive appropriate support. A differentiated assessment of admission conditions provides insights into population’s attitudes toward mental health care (20). Previous studies in an urban Vietnamese population have shown a preference for caring for psychiatric patients within families instead of admitting them to a hospital (8).
Although globally, attitudes towards the restrictions of rights and compulsory admission of psychiatric patients have been researched (20–31), in Vietnam specifically research is scarce and has focused on attitudes toward restrictions and compulsory admissions in the general population (32).
Overall, mental health stigma can be reduced by improving knowledge and enabling contact with persons with mental disorders (33). In medical professionals specifically, mental health literacy can be improved by including mandatory psychiatry courses in the medical curriculum (13, 14, 34–47). This has previously been demonstrated in Vietnamese medical students, who hold more benevolent attitudes towards psychiatric patients than non-medical students, and a psychiatry course positively impacted opinions on psychiatry (9). However, research on the attitudes of Vietnamese students toward psychiatric patients and mental health literacy remains scarce.
This cross-sectional, explorative study aimed to assess the attitudes of Vietnamese students towards the restriction of civil rights and compulsory admissions of patients with severe mental illness. Specifically, attitudes of medical students that had attended a psychiatry course, those that had not yet attended one, and non-medical students were compared. Generally, it was hypothesized that higher mental health literacy is associated with lower endorsement of civil rights infringements of psychiatric patients. Overall, this study aims to contribute to research on non-Western attitudes towards severe mental illnesses.
2 Methods
2.1 Study participants
Data from university students in Hanoi, Vietnam, was collected between September 2020 and May 2021. After excluding 15 participants due to incomplete data, the total sample (n = 610) comprised medical students from Hanoi Medical University (HMU), including those who had already attended a psychiatry course (MSPS n = 168), and two control groups: medical students who had not yet taken the course (MSNPS; n = 223) and non-medical students (NMS; n = 219) from the Hanoi University of Science and Technology (HUST). Ethical approval was obtained from the ethical committee of HMU (IRB-VN01.00IIIRB00003121IFWA00004148). All participants provided informed consent before data collection.
2.2 Psychiatry course
The psychiatry course was part of the regular curriculum of the fifth semester of medical school at HMU. The course duration was four weeks and consisted of two parts. Firstly, the medical students attended a one-week theoretical course on psychiatric diseases, diagnostic procedures, and treatment options. Secondly, students interned at a general psychiatric hospital for three weeks. Here, they assisted physicians and participated in individual therapy sessions. The course ended after passing a final exam (9).
2.3 Self-report questionnaires
MSPS filled out self-report questionnaires after participating in a psychiatry course. MSNPS filled out self-report questionnaires before participating in a psychiatry course. NMS received questionnaires at a non-specific point during the study period. One aim of the study was to investigate the impact of psychiatric training on students’ general perceptions and attitudes. Therefore, no explanations or descriptions about the nature of severe psychiatric disorders was provided prior to the interviews. All items included in the final questionnaires were jointly decided on by the Global Mental Health research team of the Department of Psychiatry, Charité - Universitätsmedizin Berlin and researchers and psychiatrists from the Department of Psychiatry, HMU and the associated National Institute of Mental Health (NIMH). The translation and back-translation methods were used to provide questionnaires in Vietnamese (48).
First, socio-demographic data, including gender, age, and marital status, were assessed. Additionally, information on choosing a medical discipline as a profession, previous contact with the psychiatric healthcare system, having a family member diagnosed with a psychiatric illness, and religious beliefs was obtained. Furthermore, participants received eleven questionnaires assessing attitudes toward stigmatization and discrimination of mental illness and mental health care in general. Attitudes towards restrictions and compulsory admissions in psychiatric patients were assessed by a questionnaire previously used in a study by 22, which assessed agreement with restricting certain individual rights of patients with severe psychiatric disorders (22). These included the right to vote, possession of a driver’s license, being in favor of abortion if a mentally ill female becomes pregnant, and whether sterilization in persons with a psychiatric illness is favored. To assess attitudes toward compulsory admissions in case of severe mental illness, respondents were asked whether a mentally ill person should, under certain conditions, be admitted to a hospital, even if it is against their will. Subsequently, different specific scenarios are described in which a patient could be admitted against their will, such as suicidality, violence towards others, self-neglect, delusions, social withdrawal, non-adherence to a prescribed medicine, causing a public disturbance, and upon the request of the patient’s family (22).
2.4 Statistical analysis
Statistical analyses were calculated with R (Version 4.3.1, 2023). First, socio-demographic data, including gender (binarized into female and male), age (in years), and marital status (binarized into “no partner” and “in partnership”), living area (binarized into “city and larger” and “< city”), semester (binarized into “At least fourth academic year” and “< fourth academic year”), considering oneself mentally ill, and having a close person who had been to a mental health practitioner were assessed. Socio-demographic variables were described by frequency, percentage, median, and interquartile range (Table 1). The first question was excluded from the analysis of attitudes towards restrictions as it assessed attitudes on compulsory admissions, which was already included in the compulsory admissions questionnaire. Additionally, the last question - assessing agreement to sterilization of mentally ill people against their will - was excluded since the previous question already assessed agreement to sterilization in general. Next, a sum score of the responses across the remaining four questions on restrictions was created for the primary analysis. Results were binarized into “at least one question answered ‘Yes’” and “no question answered ‘Yes’”. Then, two logistic regression analyses were calculated to capture all three comparisons between the student groups, with the first model employing MSPS, and the second model NMS as reference category. For both models, all demographic variables included in analyses were used as covariates except for age, since there was little variation in age across the sample. In a secondary analysis, group comparisons were calculated separately for each item of the Restrictions questionnaire using χ²-tests. This two-step analysis was selected to have an overall comparison between attitudes while considering covariates without losing statistical power due to correction for multiple comparisons. The secondary analysis aimed to generate tentative evidence on more nuanced attitudes in the study population.
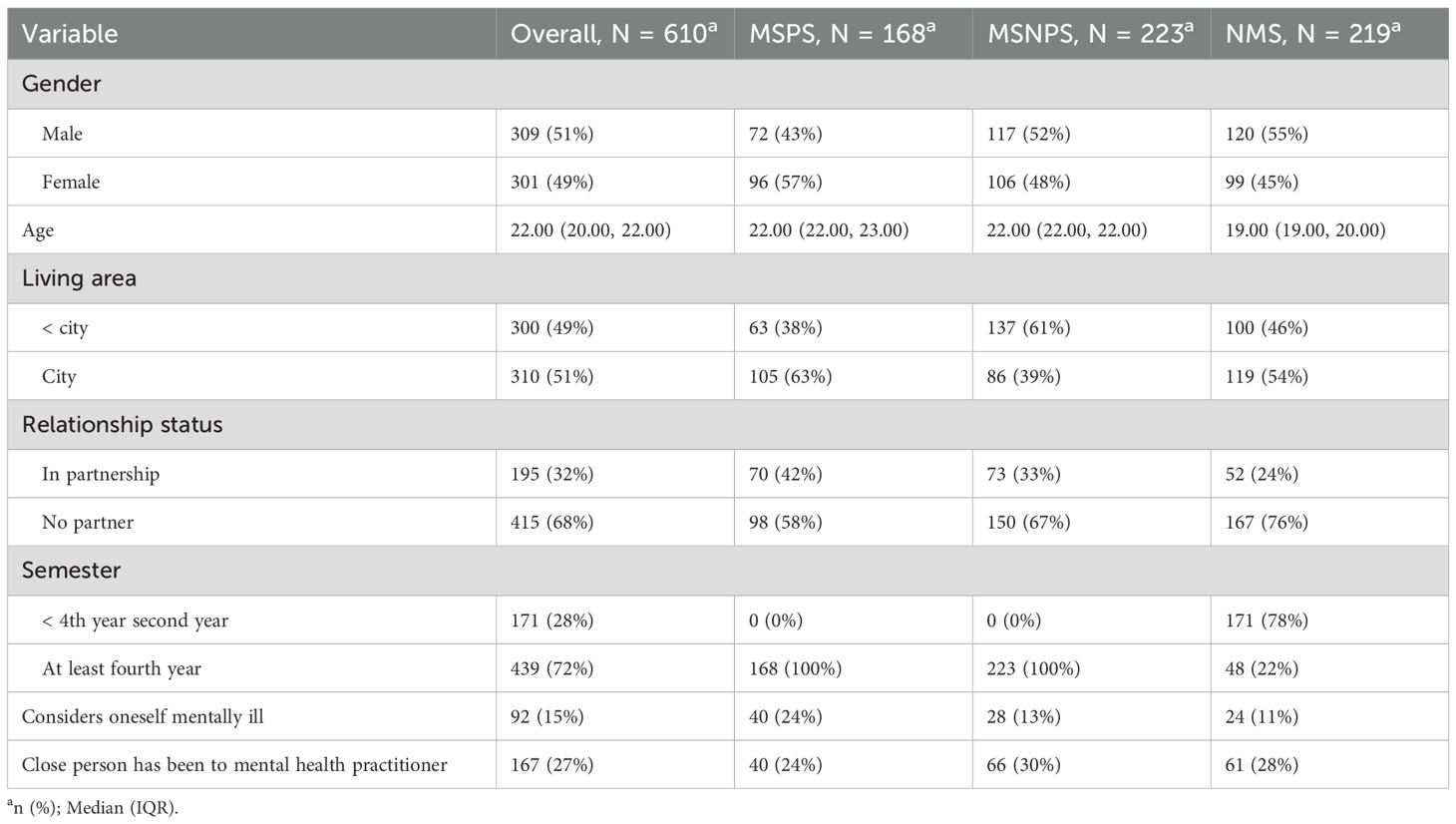
Table 1. Demographics of study sample.
Similarly, for the general analysis of the attitudes toward compulsory admissions, two logistic regressions were calculated for the first question on compulsory admissions to compare the general attitudes of all three student groups. The same covariates as in the previous models were used. Next, as a secondary analysis, group comparisons for each subsequent item describing a specific scenario were calculated separately with χ²-tests. The level of significance was set at p <0.05.
3 Results
The analyzed sample showed a balanced gender distribution (301 females; 309 males). 168 (27.2%) participants had attended a psychiatry course, 223 (36.1%) were medical students who hadn’t attended a psychiatry course, and 219 (35.5%) participants were students at the HUST. It can be noted that 11 to 24% of students considered themselves to be mentally ill. This question was aimed at understanding the respondent’s self-assessment of the likelihood that they were mentally ill, not whether a specific mental disorder had been professionally diagnosed. The participants were not asked to disclose the nature of a potentially diagnosed mental illness. An overview of the distribution of socio-demographic data can be found in Table 1. The three groups show significant differences in the gender distribution, with more male students in the NMS than in the MSPS (χ² = 4.95; p = 0.026). Furthermore, MSPS (χ² = 13.33; p < 0.001) and MSNPS (χ² = 3.97; p = 0.046) were significantly more often in a relationship than NMS. Group comparisons can be found in the appendix.
Across all groups, the majority of the study sample did not support restricting the rights of persons with mental illness. However, 55.7% of respondents endorsed restricting psychiatric patients’ right to vote. 5.2% of participants reported being in favor of revoking the driver’s license of someone who has been treated once in a mental hospital. Overall, 7.5% of participants were in favor of abortion if a mentally ill female becomes pregnant, and 15.4% agreed with sterilizing persons with severe mental illness.
Restriction questionnaire responses per group, per item can be found in Table 2; both logistic regression models for overall agreement with restrictions can be found in the Supplementary Material. There were no significant differences between the attitudes of the three observed student groups (MSNPS vs. MSPS: OR = 0.68, p = 0.08; NMS vs. MSPS: OR = 1.16, p = 0.7; MSNPS vs. NMS: OR = 0.59, p = 0.12) and no socio-demographic covariates significantly influenced these attitudes (see Supplementary Table 1). Furthermore, no difference in attitudes was seen in the secondary analysis investigating group differences on the item level, as displayed in Figure 1.
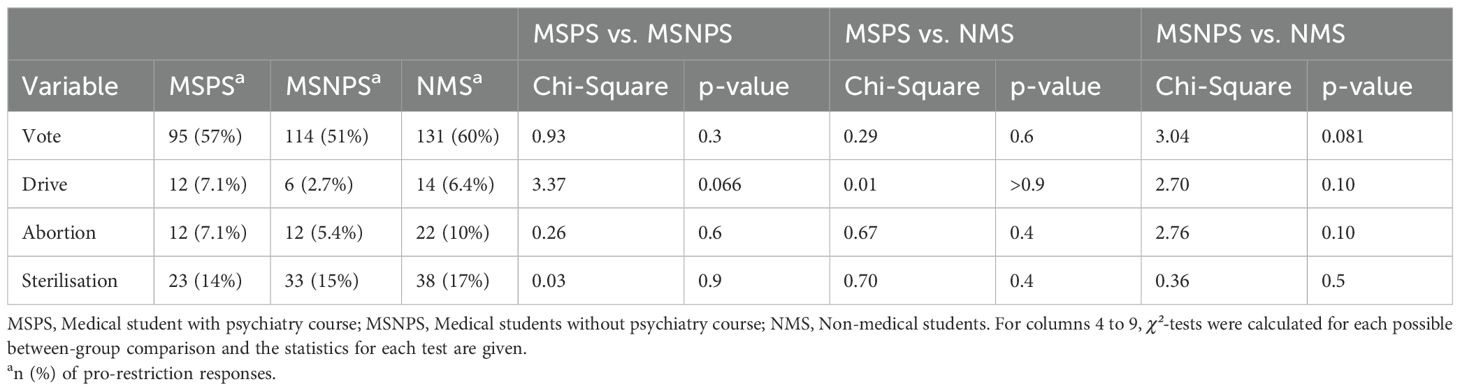
Table 2. Restrictions questionnaire – per-group responses.
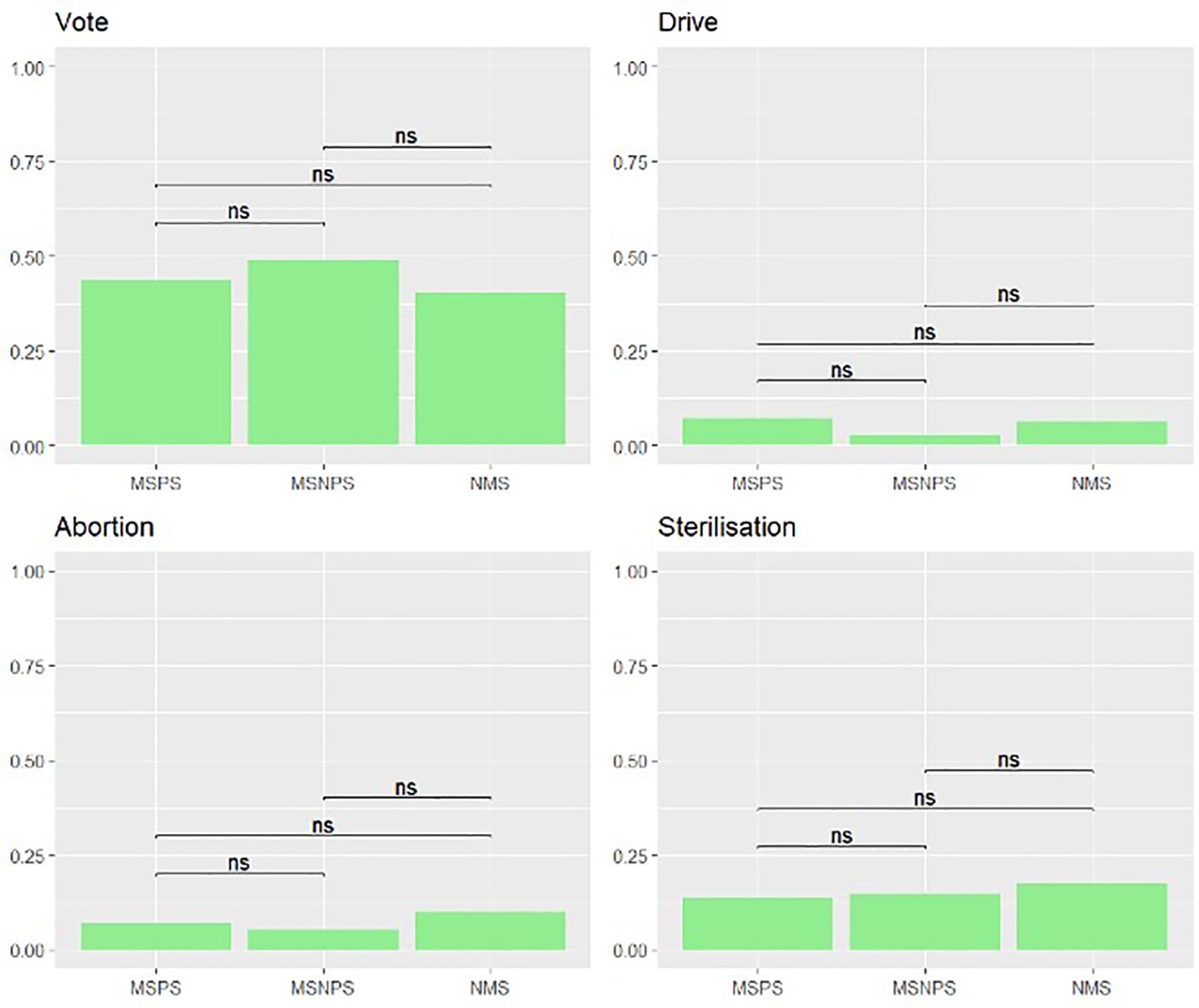
Figure 1. Restrictions questionnaire - Secondary analysis. Secondary analysis for each item of the Restrictions questionnaire with group comparisons with Chi-Square tests with 1 signifying agreement and 0 disagreement with the restriction of a specific right. MSPS, Medical student with psychiatry course; MSNPS, Medical students without psychiatry course; NMS, Non-medical students. ns, non-significant.
Next, the attitudes toward compulsory admissions of psychiatric patients were analyzed; the results per group, per item are displayed in Table 3 and both logistic regression models for overall agreement with compulsory admissions are displayed in the Supplementary Material.
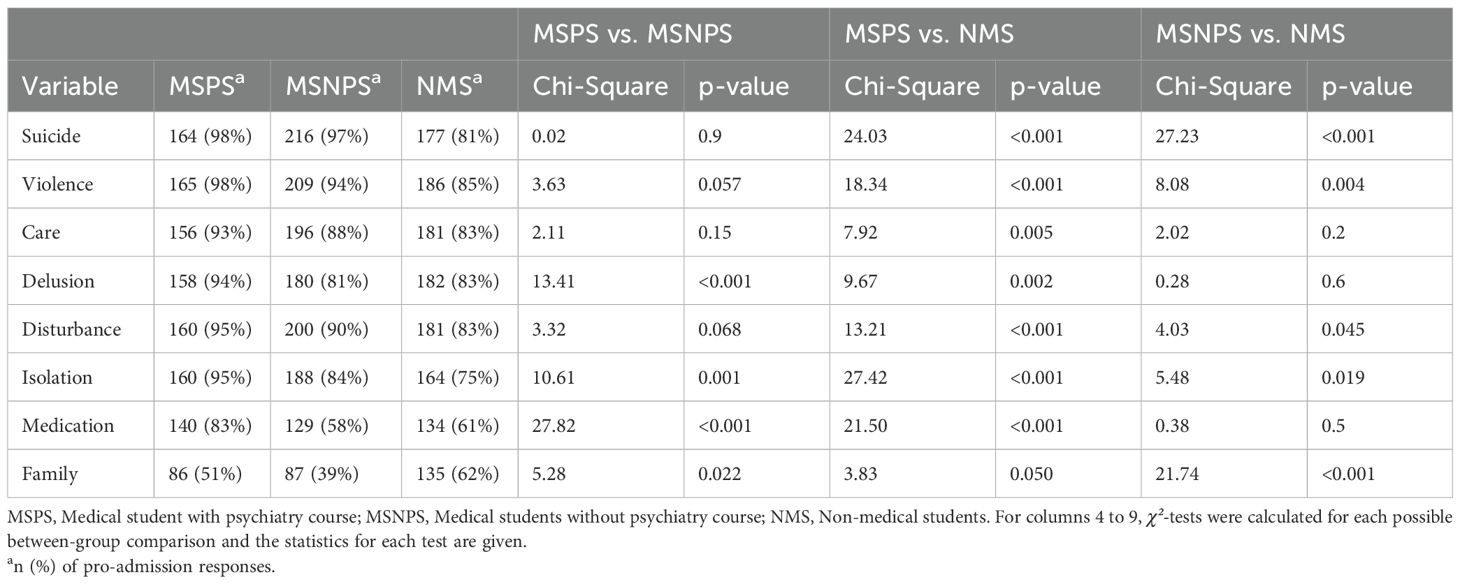
Table 3. Compulsory admissions questionnaire – per-group responses.
The majority of the study population endorsed compulsory admissions under certain conditions (91.6%). A significant group difference was seen between MSNPS and MSPS (OR = 3.21; p = 0.006), as well as MSNPS and NMS (OR = 3.30; p = 0.033), with MSPS and NMS being significantly less in favor of compulsory admissions than MSNPS. No significant difference was seen between the attitudes of NMS and MSPS towards compulsory admissions. Additionally, socio-demographic covariates in both models did not significantly influence these attitudes (see Supplementary Table 2).
The secondary analysis assessing group differences on single items about compulsory admissions showed that, generally, MSPS were more likely to endorse compulsory admissions in specific situations than MSNPS and NMS (Figure 2). The differences between attitudes of MSPS and MSNPS were especially relevant for delusions (χ² = 13.41; p <.001), social withdrawal (χ² = 10.61; p = 0.001), non-adherence to prescribed medication (χ² = 27.82; p <.001), and if the family requested compulsory admission (χ² = 5.28; p = 0.022). MSPS were significantly more likely to endorse compulsory admissions in all scenarios than NMS except if the family of a mentally ill person wanted it this way. In this situation, NMS were significantly more likely to approve compulsory admission than MSNPS (χ² = 21.74; p <.001). MSNPS were more likely to endorse compulsory admissions than NMS if patients were suicidal (χ² = 27.23; p <.001), violent towards others (χ² = 8.08; p = 0.004), caused a disturbance (χ² = 4.03; p = 0.045) or withdrew socially (χ² = 5.48; p = 0.019).
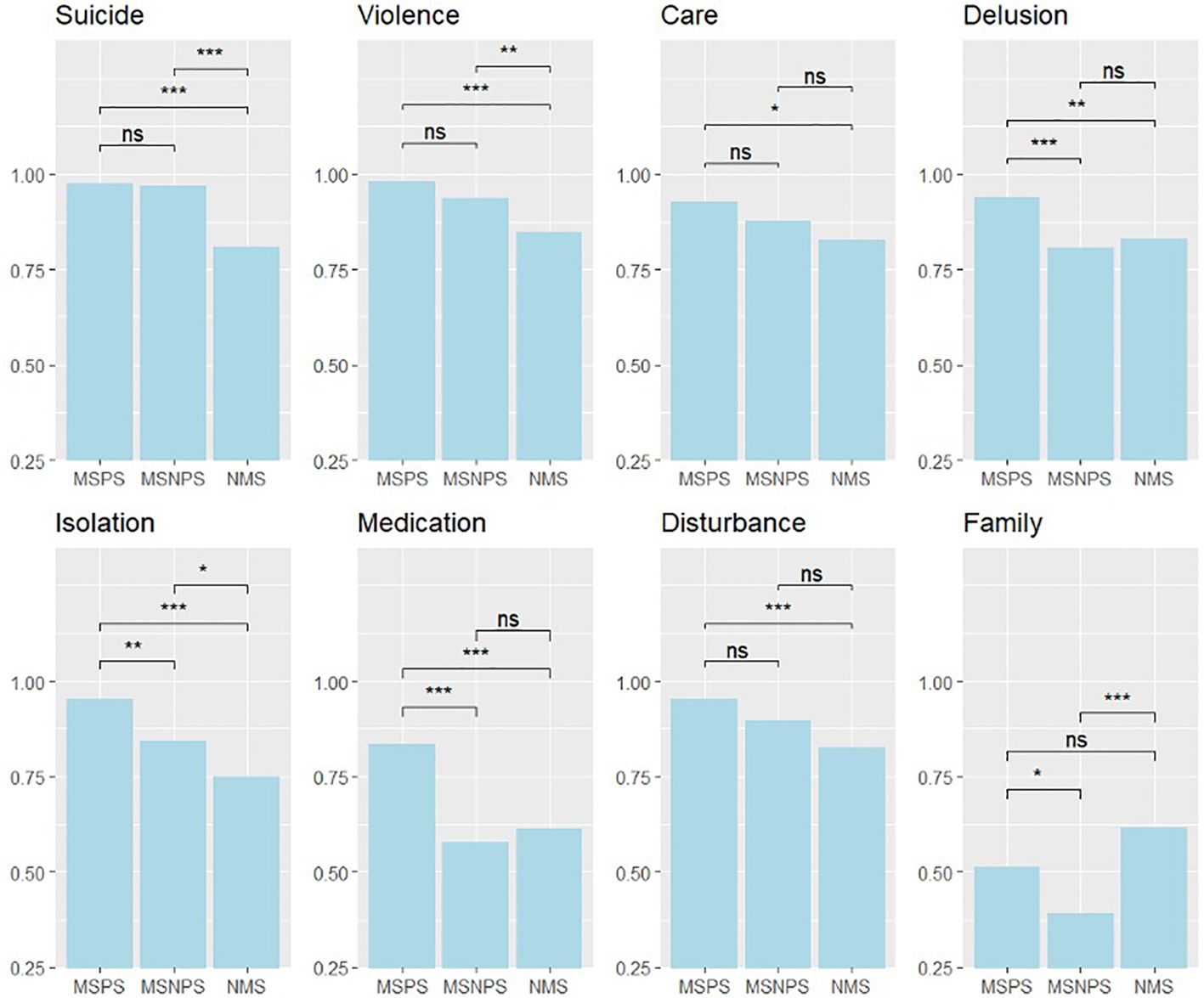
Figure 2. Compulsory Admissions questionnaire – secondary analysis. Secondary analysis for each item of the compulsory admissions questionnaire with group comparisons with Chi-Square tests; MSPS, Medical student with psychiatry course; MSNPS, Medical students without psychiatry course; NMS, Non-medical students. ns, non-significant, * ≤ 0.05, ** ≤ 0.01, *** ≤ 0.001.
4 Discussion
This study investigated attitudes of Vietnamese students towards restrictions of rights and compulsory admissions of psychiatric patients. Generally, international studies on these questions are limited, especially in the Global South. The existing comparable studies have been considered here to embed this research’s findings into a global context, albeit being geographically limited to a few European and Vietnamese studies. Overall, Vietnamese students in the present study showed lower acceptance rates of restrictions of mentally ill people than in comparable studies from Switzerland (49) or Germany (22). The same is true when comparing attitudes towards restrictions with a study of the general population in the Hanoi urban area (32). Here, researchers found that 11.9% of respondents were in favor of revoking a driver’s license from a mentally ill person compared to 5.2% of students in the present study. 7.5% of students were in favor of abortion if a mentally ill female becomes pregnant, compared to 21.4% of the general population, and 15.4% of students, compared with 21.6% of the general population, agreed with sterilizing mentally ill persons (32). Previous studies have shown that endorsement of abortion was higher in older population groups, thus providing an explanation for the lower rates in the current study (32). Although numbers are generally lower than in the general population, the approval rate of such invasive procedures like abortion or sterilization is still substantial. This may be due to Vietnamese societal beliefs that the development of the child is strongly influenced by the physical and emotional state of the mother in pregnancy (50) resulting in more restrictive views on childbearing in psychiatric patients.
Furthermore, it is striking to find that more than half of respondents endorsed restricting psychiatric patients’ right to vote, especially when considering that Vietnam adopted the UN Convention on the Rights of People with Disabilities (CRPD) in 2014 (51). The convention affirms that persons with disabilities, including persons with severe mental illness, are to be guaranteed full enjoyment of human rights and fundamental freedoms without discrimination, including the right and opportunity to vote. These attitudes may be explained by the fact that severely mentally ill patients in Vietnam present more exacerbated clinical conditions due to the country’s psychiatric infrastructure (1). Due to limited clinical and outpatient facilities, where psychiatric disorders can be treated earlier, conditions may worsen, leading to a more negative public perception of mental disorders. A recent study on the belief systems of the general population of the Hanoi region about patients with schizophrenia and depression showed that a vast majority of participants correctly conceptualized vignettes of the two mentioned diagnoses as mental disorders. Nevertheless, the majority was not able to correctly identify the diagnoses, nor explicitly recommended medical or psychological treatment (52). This indicates that overall, an understanding of severe mental illness is present in the general population but knowledge on appropriate treatment possibilities is still lacking. In the scope of Vietnam’s National Mental Health Strategy 2015–2025, measures are being implemented to scale up mental health services and psychological interventions (53). The study further underlines the importance of these measures to ensure equal civil rights for psychiatric patients.
Vietnamese students were more accepting of compulsory admissions of psychiatric patients compared to the general population in other national and international studies. For instance, a survey of the change in public opinions of the general German population between the years 1993 and 2011 towards compulsory admissions showed acceptance rates of 74% in 1993 and 71% in 2011 compared to 91.6% in the present study (22). A study in the Swiss population, also showed lower acceptance rates than in the present study, ranging between 68 and 78% (54). Vietnamese students also showed higher acceptance rates of compulsory admissions than the general population in the greater Hanoi urban area (32). This may be due to the difference in academic levels in the two populations, with the study sample solely including university students with a median age of 22, which is in line with previous studies, demonstrating that higher education increased the acceptance of compulsory admission (54–56). Another study conducted in Germany by Zogg et al. underlines this, showing that involuntary admissions were accepted by 98.9% of psychiatrists and only 72.2% of non-specialists (57). Higher education levels may be associated with lower stigma towards mental illnesses and higher levels of trust in the psychiatric care system, thus increasing endorsement of compulsory admissions. Overall, these socio-demographic factors (i.e., higher levels of educational attainment and younger age) have been shown to be associated with a reluctance to accept civil rights infringements of psychiatric patients and be more accepting of involuntary admissions (22, 32, 49, 54, 57).
On the other hand, contrasting to previous studies, an influence of gender on attitudes was not found in the present study (22, 32, 49, 54). This may indicate that gender differences become less important with higher education levels (58). For instance, the increased risk for mental health disorders in women in Vietnam has been shown to be significantly reduced when controlling for years of education (59). Studies on gender roles in Vietnam show that high education levels of women are associated with a more equal distribution of caretaking tasks between genders, and traditional views on female and male roles are more widely spread in the older population (60, 61). The high endorsement of compulsory admissions may also reflect a high level of trust of Vietnamese students in the psychiatric health care system.
No significant differences appeared between the student groups when comparing overall attitudes on restrictions. In contrast, MSPS and MSNPS differed significantly in their attitudes toward compulsory admissions, with MSNPS showing overall significantly stronger agreement with this measure than MSPS and NMS. MSPS and NMS showed comparable attitudes. However, when assessing attitudes on specific scenarios in which psychiatric patients may be involuntarily admitted to in-patient treatment, MSPS were more likely to endorse compulsory admission (in case of suicidal ideation, violence towards others, neglecting self-care, delusions, social withdrawal, non-adherence to prescribed medication, or causing a public disturbance) than MSNPS and NMS. This, however, was not true for the item “A mentally ill person should be admitted against his will if the family wants it this way.” Here, NMS were significantly more likely to agree with compulsory admission than MSNPS and showed higher levels of agreement than MSPS. This may reflect the fact that with increasing mental health literacy, professional medical judgment is more important than families’ opinions when deciding on compulsory admission. This is in line with a previous study on the impact of a psychiatry course on Vietnamese medical students’ attitudes toward psychiatric patients (9). Additionally, witnessing more severely ill patients in clinical rotations may reinforce agreement with involuntary treatment.
Nevertheless, interpretation of associations between attending a psychiatry course on students’ attitudes is limited due to the assessment via self-report questionnaires. This may lead to a social desirability bias as respondents may answer questions in a manner they believe is more acceptable or desirable rather than providing their true thoughts or feelings. This may further be compounded by the fact that the study was conducted by the Department of Psychiatry of the Hanoi Medical University, possibly leading to an over-reporting of positive attitudes. Additionally, the employed questionnaires used theoretically derived items and not psychometrically tested instruments.
Moreover, the current study was limited to the urban area of Hanoi. Future studies should expand the geographical scope to other Vietnamese universities, and specifically, more rural areas of Vietnam. Additionally, a randomized controlled longitudinal study design could shine a light on the causal influence of a psychiatry course on medical students’ attitudes, and qualitative methods could support the interpretation of results. In addition to a longitudinal design, including a follow-up to assess the long-term effect of stigma-reducing measures would be beneficial. A behavioral assessment could help evaluate how the change in attitudes toward psychiatric patients impacts their behavior toward them.
In conclusion, Vietnamese students showed lower levels of acceptance of restrictions and higher levels of acceptance of compulsory admissions rights in psychiatric patients compared to the general population in the Hanoi urban area and international comparisons. Furthermore, we provide tentative evidence that a psychiatry course may encourage more differentiated opinions on the use of compulsory admissions in psychiatric care. Psychoeducation may be a useful tool to reduce mental health stigma. This underlines the importance of introducing courses with direct clinical contact with psychiatric patients into the medical curriculum. The psychiatry courses should be spread more broadly, specifically to other universities, considering they are currently only part of the medical curriculum at Hanoi Medical University. Additionally, education on mental health should be introduced earlier, such as in school, and in a broader sense, such as in the workplace to increase mental health literacy.
Further research, particularly in a longitudinal study design, is needed to explore causal relationships and the long-term effects of a psychiatry course on medical students’ attitudes toward psychiatric patients in Vietnam.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Hanoi Medical University (IRB-VN01.00IIIRB00003121IFWA00004148). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SK: Formal Analysis, Writing – original draft, Writing – review & editing, Conceptualization, Investigation, Visualization. VTN: Data curation, Project administration, Supervision, Writing – review & editing. KB: Funding acquisition, Project administration, Supervision, Writing – review & editing. MBa: Funding acquisition, Supervision, Writing – review & editing. MBr: Formal Analysis, Methodology, Software, Visualization, Writing – original draft. SW-B: Investigation, Writing – review & editing. LE: Methodology, Validation, Writing – review & editing. VPN: Investigation, Project administration, Validation, Writing – review & editing. LT: Methodology, Writing – review & editing. TC: Data curation, Investigation, Project administration, Writing – review & editing. TL: Investigation, Project administration, Writing – review & editing. TT: Conceptualization, Funding acquisition, Investigation, Project administration, Supervision, Writing – review & editing. EH: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was conducted in part within the subproject D03 of the CRC 1171 ‘Affective Societies – Dynamics of Coexistence in Mobile Worlds’ granted by the German Research Foundation (DFG – Deutsche Forschungsgemeinschaft).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1542247/full#supplementary-material
References
1. Murphy JK, Chau LW, Nguyen VC, Minas H, Anh DV, O'Neil J. An integrated knowledge translation (iKT) approach to advancing community-based depression care in Vietnam: lessons from an ongoing research-policy collaboration. BMC Health Serv Res. (2024) 24:142. doi: 10.1186/s12913-023-10518-3
2. Weiss B, Dang H-M, Le G, Vu V, Forman S. Mixed-methods needs assessment for development of school-based mental health implementation science capacity in low- and middle-income countries: Vietnam as a case example. School Psychol (Washington, D.C.). (2024) 39:167–75. doi: 10.1037/spq0000586
3. WHO. WHO–AIMS report on mental health system in Vietnam (2006). Available online at: http://www.who.int/mental_health/evidence/who_aims_report_viet_nam.pdf (Accessed 01.2009).
4. Le SM, Hahn E, Tran TA, Mavituna S, Ta TMT. Human Resources for Mental Health Service Delivery in Viet Nam: Toward Achieving Universal Health Coverage. International Development in Focus. Washington, DC: World Bank. (2024) http://hdl.handle.net/10986/41623 License: CC BY 3.0 IGO.
5. Dang H-M, Lam TT, Dao A, Weiss B. Mental health literacy at the public health level in low and middle income countries: An exploratory mixed methods study in Vietnam. PLoS One. (2020) 15:e0244573. doi: 10.1371/journal.pone.0244573
6. Ta TM, Zieger A, Schomerus G, Cao TD, Dettling M, Do XT, et al. Influence of urbanity on perception of mental illness stigma: a population based study in urban and rural Hanoi, Vietnam. Int J Soc Psychiatry. (2016) 62:685–95. doi: 10.1177/0020764016670430
7. Fino E, Agostini A, Mazzetti M, Colonnello V, Caponera E, Russo PM. There is a limit to your openness: mental illness stigma mediates effects of individual traits on preference for psychiatry specialty. Front Psychiatry. (2019) 10:775. doi: 10.3389/fpsyt.2019.00775
8. van der Ham L, Wright P, Van TV, Doan VDK, Broerse JEW. Perceptions of mental health and help-seeking behavior in an urban community in Vietnam: an explorative study. Community Ment Health J. (2011) 47:574–82. doi: 10.1007/s10597-011-9393-x
9. Eilinghoff L, Nguyên VT, Hahn E, Nguyên VP, Lê CT, Lê TTH, et al. Changes in attitudes toward persons with mental disorders after attendance of a psychiatric curriculum among medical students in Vietnam: A cross-sectional study. Asian J Psychiatr. (2024) 93:103949. doi: 10.1016/j.ajp.2024.103949
10. Kamimura A, Trinh HN, Johansen M, Hurley J, Pye M, Sin K, et al. Perceptions of mental health and mental health services among college students in Vietnam and the United States. Asian J Psychiatry. (2018) 37:15–9. doi: 10.1016/j.ajp.2018.07.012
11. Nguyen Thai QC, Nguyen TH. Mental health literacy: knowledge of depression among undergraduate students in Hanoi, Vietnam. Int J Ment Health Syst. (2018) 12:19. doi: 10.1186/s13033-018-0195-1
12. Pham Tien N, Pham Thanh T, Nguyen Hanh D, Duong Hoang A, Bui Dang The A, Kim Bao G, et al. Utilization of mental health services among university students in Vietnam. Int J Ment Health. (2021) 50:113–35. doi: 10.1080/00207411.2020.1816114
13. Henderson C, Noblett J, Parke H, Clement S, Caffrey A, Gale-Grant O, et al. Mental health-related stigma in health care and mental health-care settings. Lancet Psychiatry. (2014) 1:467–82. doi: 10.1016/S2215-0366(14)00023-6
14. Oliveira AM, MaChado D, Fonseca JB, Palha F, Silva Moreira P, Sousa N, et al. Stigmatizing attitudes toward patients with psychiatric disorders among medical students and professionals. Front Psychiatry. (2020) 11:326. doi: 10.3389/fpsyt.2020.00326
15. Druss BG, Rosenheck RA, Desai MM, Perlin JB. Quality of preventive medical care for patients with mental disorders. Med Care. (2002) 40(2):129–36. doi: 10.1097/00005650-200202000-00007
16. Knaak S, Mantler E, Szeto A. Mental illness-related stigma in healthcare: Barriers to access and care and evidence-based solutions. Healthcare Manage Forum. (2017) 30:111–6. doi: 10.1177/0840470416679413
17. Bhugra D, Pathare S, Gosavi C, Ventriglio A, Torales J, Castaldelli-Maia J, et al. Mental illness and the right to vote: a review of legislation across the world. Int Rev Psychiatry. (2016) 28:395–9. doi: 10.1080/09540261.2016.1211096
18. Okwerekwu JA, McKenzie JB, Yates KA, Sorrentino RM, Friedman SH. Voting by people with mental illness. J Am Acad Psychiatry Law Online. (2018) 4:151–76. doi: 10.29158/jaapl.003780-18
19. Patel V, Saxena S, Lund C, Kohrt B, Kieling C, Sunkel C, et al. Transforming mental health systems globally: principles and policy recommendations. Lancet. (2023) 402:656–66. doi: 10.1016/s0140-6736(23)00918-2
20. Schomerus G, Sander C, Schindler S, Baumann E, Angermeyer MC. Public attitudes towards protecting the human rights of people with mental illness: a scoping review and data from a population trend study in Germany. Int Rev Psychiatry. (2023) 35:167–79. doi: 10.1080/09540261.2022.2087494
21. Angermeyer MC, Matschinger H. Auswirkungen der Reform der psychiatrischen Versorgung in den neuen Ländern der Bundesrepublik Deutschland auf die Einstellung der Bevölkerung zur Psychiatrie und zu psychisch Kranken: Ergebnisse einer empirischen Erhebung. Nomos Verlagsgesellschaft mbH & Co. KG Waldseestraβe 3 - 576530 Baden-Baden, Deutschland: Nomos-Verlag-Ges (1995).
22. Angermeyer MC, Matschinger H, Schomerus G. Attitudes of the German public to restrictions on persons with mental illness in 1993 and 2011. Epidemiol Psychiatr Sci. (2014) 23:263–70. doi: 10.1017/s2045796014000183
23. Borrmann B, Preckel J, Rosenkötter N. Wissen und Einstellungen in Bezug auf psychische Erkrankungen in der Bevölkerung. Das Gesundheitswesen. (2016) 78:A150. doi: 10.1055/s-0036-1586660
24. Chen H, Wang Z, Phillips MR. Assessing knowledge and attitudes about mental illness in Ningxia, China. Transcultural Psychiatry. (2018) 55:94–119. doi: 10.1177/1363461517748847
25. Grausgruber A, Moosbrugger R, Hackl E. Monitoring public stigma in Austria 1998–2018. Research Report. Johannes Kepler University (2018).
26. Henderson C, Robinson E, Evans-Lacko S, Corker E, Rebollo-Mesa I, Rose D, et al. Public knowledge, attitudes, social distance and reported contact regarding people with mental illness 2009–2015. Acta Psychiatrica Scandinavica. (2016) 134:23–33. doi: 10.1111/acps.2016.134.issue-S446
27. Quirke E, Klymchuk V, Suvalo O, Bakolis I, Thornicroft G. Mental health stigma in Ukraine: cross-sectional survey. Glob Ment Health (Camb). (2021) 8:e11. doi: 10.1017/gmh.2021.9
28. Reta Y, Tesfaye M, Girma E, Dehning S, Adorjan K. Public stigma against people with mental illness in Jimma Town, Southwest Ethiopia. PLoS One. (2016) 11:e0163103. doi: 10.1371/journal.pone.0163103
29. Schomerus G, Stolzenburg S, Bauch A, Speerforck S, Janowitz D, Angermeyer MC. Shifting blame? Impact of reports of violence and mental illness in the context of terrorism on population attitudes towards persons with mental illness in Germany. Psychiatry Res. (2017) 252:164–8. doi: 10.1016/j.psychres.2017.02.053
30. Tesfaye Y, Agenagnew L, Terefe Tucho G, Anand S, Birhanu Z, Ahmed G, et al. Attitude and help-seeking behavior of the community towards mental health problems. PLoS One. (2020) 15:e0242160. doi: 10.1371/journal.pone.0242160
31. Winkler P, Mladá K, Janoušková M, Weissová A, Tušková E, Csémy L, et al. Attitudes towards the people with mental illness: comparison between Czech medical doctors and general population. Soc Psychiatry Psychiatr Epidemiol. (2016) 51:1265–73. doi: 10.1007/s00127-016-1263-y
32. Laqua C, Hahn E, Böge K, Martensen LK, Nguyen TD, Schomerus G, et al. Public attitude towards restrictions on persons with mental illness in greater Hanoi area, Vietnam. Int J Soc Psychiatry. (2018) 64:335–43. doi: 10.1177/0020764018763685
33. Thornicroft G, Mehta N, Clement S, Evans-Lacko S, Doherty M, Rose D, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet. (2016) 387:1123–32. doi: 10.1016/S0140-6736(15)00298-6
34. Ahuja KK, Dhillon M, Juneja A, Sharma B. Breaking barriers: An education and contact intervention to reduce mental illness stigma among Indian college students. Psychosocial Intervention. (2017) 26:103–9. doi: 10.1016/j.psi.2016.11.003
35. De Witt C, Smit I, Jordaan E, Koen L, Niehaus DJH, Botha U. The impact of a psychiatry clinical rotation on the attitude of South African final year medical students towards mental illness. BMC Med Educ. (2019) 19:114. doi: 10.1186/s12909-019-1543-9
36. Depasse JW, Lee PT. A model for 'reverse innovation' in health care. Global Health. (2013) 9:40. doi: 10.1186/1744-8603-9-40
37. Economou M, Kontoangelos K, Peppou LE, Arvaniti A, Samakouri M, Douzenis A, et al. Medical students’ attitudes to mental illnesses and to psychiatry before and after the psychiatric clerkship: Training in a specialty and a general hospital. Psychiatry Res. (2017) 258:108–15. doi: 10.1016/j.psychres.2017.10.009
38. Eksteen H-C, Becker PJ, Lippi G. Stigmatization towards the mentally ill: Perceptions of psychiatrists, pre-clinical and post-clinical rotation medical students. Int J Soc Psychiatry. (2017) 63:782–91. doi: 10.1177/0020764017735865
39. Kassam A, Glozier N, Leese M, Loughran J, Thornicroft G. A controlled trial of mental illness related stigma training for medical students. BMC Med Educ. (2011) 11:51. doi: 10.1186/1472-6920-11-51
40. Lee HJ, Jang HJ, Jang S, Bong SH, Won GH, Yoon S, et al. Psychiatry curriculum: How does it affect medical students’ attitude toward psychiatry? Asian J Psychiatry. (2022) 67:102919. doi: 10.1016/j.ajp.2021.102919
41. Li J, Li J, Thornicroft G, Yang H, Chen W, Huang Y. Training community mental health staff in Guangzhou, China: evaluation of the effect of a new training model. BMC Psychiatry. (2015) 15:263. doi: 10.1186/s12888-015-0660-1
42. Lingeswaran A. Psychiatric curriculum and its impact on the attitude of Indian undergraduate medical students and interns. Indian J psychol Med. (2010) 32:119–27. doi: 10.4103/0253-7176.78509
43. Lyons Z, Janca A. Impact of a psychiatry clerkship on stigma, attitudes towards psychiatry, and psychiatry as a career choice. BMC Med Educ. (2015) 15:34. doi: 10.1186/s12909-015-0307-4
44. Oakley C, Oyebode F. Medical students' views about an undergraduate curriculum in psychiatry before and after clinical placements. BMC Med Educ. (2008) 8:26. doi: 10.1186/1472-6920-8-26
45. Pal T, Singh S. Impact of clinical posting in psychiatry on the attitude towards mental illness in undergraduate final year medical students. Asian J Psychiatry. (2022) 69:103001. doi: 10.1016/j.ajp.2021.103001
46. Waqas A, Malik S, Fida A, Abbas N, Mian N, Miryala S, et al. Interventions to reduce stigma related to mental illnesses in educational institutes: a systematic review. Psychiatr Q. (2020) 91:887–903. doi: 10.1007/s11126-020-09751-4
47. Yadav T, Arya K, Kataria D, Balhara YPS. Impact of psychiatric education and training on attitude of medical students towards mentally ill: A comparative analysis. Ind Psychiatry J. (2012) 21:22–31. doi: 10.4103/0972-6748.110944
48. WHO. WHODAS 2.0 Translation Package (Version 1.0) Translation and linguistic evaluation protovol and supporting material (2012). Available online at: https://terrance.who.int/mediacentre/data/WHODAS/Guidelines/WHODAS%202.0%20Translation%20guidelines.pdf (Accessed November 01, 2024).
49. Lauber C, Nordt C, Falcato L, Rössler W. Public acceptance of restrictions on mentally ill people. Acta Psychiatrica Scandinavica. (2000) 102:26–32. doi: 10.1034/j.1600-0447.2000.00005.x
50. Pashigian MJ. The womb, infertility and the vicissitudes of kin-relatedness in Vietnam. J Vietnamese Stud. (2009) 4:34–68. doi: 10.1525/vs.2009.4.2.34
51. Minas H, Edington C, La N, Kakuma R. Mental Health in Vietnam BT - mental health in Asia and the Pacific: historical and cultural perspectives. Minas H, Lewis M, editors. Boston: Springer US (2017) p. 145–61. doi: 10.1007/978-1-4899-7999-5_10
52. Mobashery M, Ta TMT, Cao DT, Böge K, Eilinghoff L, Nguyen VP, et al. Mental health literacy and the public perception of persons with depression and schizophrenia in Vietnam. Front Psychiatry. (2024) 15:1430272. doi: 10.3389/fpsyt.2024.1430272
53. Vietnamese Legal System. Decision No. 155/QD-TTg dated January 29, 2022 On approval of the national plan for prevention and control of non-communicable diseases (ncds) and mental disorders for the period of 2022-2025 (2022). Available online at: https://hethongphapluat.com/decision-no-155-qd-ttg-dated-january-29-2022-on-approval-of-the-national-plan-for-prevention-and-control-of-non-communicable-diseases-ncds-and-mental-disorders-for-the-period-of-2022-2025.html (Accessed February 4, 2025).
54. Lauber C, Nordt C, Falcato L, Rössler W. Public attitude to compulsory admission of mentally ill people. Acta Psychiatr Scand. (2002) 105:385–9. doi: 10.1034/j.1600-0447.2002.1o267.x
55. Kinner SA, Harvey C, Hamilton B, Brophy L, Roper C, McSherry B, et al. Attitudes towards seclusion and restraint in mental health settings: findings from a large, community-based survey of consumers, carers and mental health professionals. Epidemiol Psychiatr Sci. (2017) 26:535–44. doi: 10.1017/s2045796016000585
56. Roe D, Weishut DJ, Jaglom M, Rabinowitz J. Patients' and staff members' attitudes about the rights of hospitalized psychiatric patients. Psychiatr Serv. (2002) 53:87–91. doi: 10.1176/appi.ps.53.1.87
57. Zogg H, Lauber C, Ajdacic-Gross V, Rössler W. Expert's and lay attitudes towards restrictions on mentally ill people. Psychiatr Prax. (2003) 30:379–83. doi: 10.1055/s-2003-43247
58. Rivera-Garrido N. Can education reduce traditional gender role attitudes? Economics Educ Rev. (2022) 89:102261. doi: 10.1016/j.econedurev.2022.102261
59. Collier KM, Weiss B, Pollack A, Lam T. Explanatory variables for women’s increased risk for mental health problems in Vietnam. Soc Psychiatry Psychiatr Epidemiol. (2020) 55:359–69. doi: 10.1007/s00127-019-01761-3
60. Knodel J, Loi VM, Jayakody R, Huy VT. Gender roles in the family. Asian Population Stud. (2005) 1:69–92. doi: 10.1080/17441730500125888
Keywords: medical students, psychiatry, stigma, restrictions, compulsory admissions, mental health literacy
Citation: Kemna S, Nguyen VT, Böge K, Bajbouj M, Bringmann M, Weyn-Banningh S, Eilinghoff L, Nguyen VP, Tuturea LE, Le Cong T, Le TTH, Ta TMT and Hahn E (2025) Attitudes of Vietnamese University students on restrictions of rights and compulsory admissions in patients with severe mental illness – a cross-sectional study. Front. Psychiatry 16:1542247. doi: 10.3389/fpsyt.2025.1542247
Received: 09 December 2024; Accepted: 24 February 2025;
Published: 19 March 2025.
Edited by:
Roy Abraham Kallivayalil, Pushpagiri Medical College, IndiaReviewed by:
Devashish Konar, Mental Health Care Centre, IndiaMafalda Silva, Piaget Institute, Portugal
M S V K Raju, Consultant in Psychiatry in Private Practice, India
Copyright © 2025 Kemna, Nguyen, Böge, Bajbouj, Bringmann, Weyn-Banningh, Eilinghoff, Nguyen, Tuturea, Le Cong, Le, Ta and Hahn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Solveig Kemna, c29sdmVpZy5rZW1uYUBjaGFyaXRlLmRl
†These authors have contributed equally to this work