
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 26 March 2025
Sec. Public Mental Health
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1541316
This article is part of the Research Topic Innovative Approaches in Psychosocial and Mental Health View all 3 articles
 Nurten Elkin1
Nurten Elkin1 Ashifa Kariveliparambil Mohammed2*
Ashifa Kariveliparambil Mohammed2* Şenay Kılınçel3
Şenay Kılınçel3 Ayse Mücella Soydan4
Ayse Mücella Soydan4 Sultan Çakmak Tanrıver5
Sultan Çakmak Tanrıver5 Şebnem Çelik1
Şebnem Çelik1 Maharishi Ranganathan6
Maharishi Ranganathan6The present study tried to assess university students’ mental health literacy (MHL) and happiness levels and whether a relationship existed between these. The study used a descriptive quantitative methodology, utilizing Likert-type scales to collect data. A private university in Istanbul’s Faculty of Health Sciences had a sample of 443 students. Information was collected using a Personal Data Collection PR Form, the Oxford Happiness Questionnaire Short Form (OHQ-SF), and the Mental Health Literacy Scale (MHLS). Descriptive statistics and one-way analysis of variance (ANOVA) were used to analyze the data. The participants’ mean MHLS score was 23.00 ± 4.70, and the OHQ-SF score was 23.50 ± 4.70. We detected a significant difference in the MHL subscale owing to age, gender, department, class, maternal education, maternal employment status, income level, academic success, family attitude, smoking status, and exercise status. There were also differences in OHQ-SF scores by students’ department, class level, mother’s education level, father’s income level, academic success status, resident status, family attitude type smoking status, health perception of chronic illness, family history of chronic illness, exercise habit, nutritional status psychological problems, and family mental illness history. Knowledge-oriented and belief-oriented MHL subscales were weak but significantly negatively related, according to the findings. A weak correlation but a significant one was found for subscale Resource-Oriented MHL with happiness level and MHL Total. According to the above-stated research, people who can access mental health resources are more likely to be happy. These findings highlight how making mental health resources available could improve people’s mental well-being with a prolonged social work perspective. As happiness is a primary goal of life, more research contributing to our understanding of it is essential. The mental health literacy indicators for university students relate to realizing happiness and fostering well-being.
The transition to university represents a critical developmental milestone for young adults, bringing significant academic, social, and psychological changes (1). This stage requires students to gain independence, handle academic workloads, and adapt to new social and economic settings. Many people are experiencing increased stress, anxiety, and other mental health problems (2). Young people aged 15–29 years are particularly at risk of mental health disorders. Notably, suicide is the second leading cause of death in this age group, as per WHO (3). Studies show that anxiety and depression are very common within university populations, with estimates suggesting that about 39% of students have at least one diagnosed mental illness (4). The widespread occurrence of this urges action and study among this population.
Mental health literacy (MHL) is one’s knowledge, skills, and attitude to identify, assess, and manage mental health issues, which is important for psychological well-being. It helps people notice signs, reduce stigma, and ask for help when necessary (5, 6). MHL is under-researched, especially in a university context, and there is no study yet on its relationship with other well-being, like happiness. Happiness is defined as the state of positive emotions and satisfaction with life sustained over time, which is key to mental health (7). Research has shown that being happy can help beach those bad times and boost well-being, which, in turn, improves academic performance, social life, etc. Very few studies have explored the relationship between MHL and the happiness of university students (8), which is an important gap in the literature.
This research is important for both individual and societal welfare. Improving MHL among students can help them manage their mental health better, seek help on time, and adopt healthier coping strategies. By helping individuals understand mental health better, MHL can reduce the stigma associated with mental illness that threatens help-seeking in several cultures and societies (9). At the level of society, universities are seen as a miniature version of society, enhanced by the possibility of testing interventions that can subsequently be scaled up (10). Having a high level of mental health literacy (MHL) enables students to not only do better academically but also help them deal with mental health-related problems throughout life and, thus, build healthier communities.
In addition, happiness is increasingly seen as a determinant of mental health and a predictor of success in many spheres of life. At a university, happier students are likelier to do well in school, have friends, and participate on campus (11). Being aware of things that can lead to one’s happiness, particularly concerning mental health literacy, can lead to doing something useful for the academic setup. Happiness may be thought of as an end goal. Nevertheless, it may also be considered a means target as it builds resilience and buffers stress (12).
Even though MHL and happiness are clearly important, not much research exists to examine the link between the two. This gap hinders our ability to accurately assess how knowledge, attitudes, and access to mental health resources are translated to emotional or psychological well-being (13). Looking into this connection is relevant to university students who are at a developmental stage of identity formation and exploring life goals while becoming subject to increased exposure to stressors (14).
The link between MHL and happiness is academically meaningful and practically beneficial. Universities are key to influencing mental health outcomes across generations (2). If these issues are not attended to, the students will suffer from academic burnout and unsatisfactory interpersonal relationships, together with mental health conditions in the future. Through investigating the link between MHL and happiness, the study intends to facilitate a targeted intervention that university policies and programs can adopt. This is especially useful because the evidence suggests that education and intervention can improve mental health and quality of life.
This study is also necessitated by the difficulties involved in conceptualizing happiness. Happiness is more subjective, unlike physical health, which is assessed through objective measures. Happiness depends upon a person’s personality, social relations, and culture. By looking at how MHL interacts with these factors, we can better understand happiness. Additionally, the results of this research may pave the way for effective and relevant strategies to promote mental health in a culturally sensitive manner.
1. To evaluate the levels of mental health literacy among university students and identify gaps in their knowledge, attitudes, and behaviors related to mental health.
2. Measuring happiness levels by university students is an inquiry to assess emotional and psychological indicators of flowering mental health.
3. To investigate the relationship between mental health literacy and happiness, analyzing how mental health knowledge and practices influence students’ well-being.
4. To examine the demographic, socioeconomic, and behavioral factors that shape mental health literacy and happiness among university students.
5. To propose evidence-based recommendations for developing interventions and policies that improve mental health literacy and enhance happiness among university students.
MHL is an emerging research area examining the connection between happiness and mental health literacy. University students, in particular, are uniquely vulnerable to mental health issues. This assessment analyzes the literature on MHL, its dimensions, and happiness, including the significance of context and demographic factors (15).
Mental health literacy refers to knowing about the mental illness, implying being able to identify a particular mental illness, know about the available treatment options, and attitude facilitating help (16). The term ‘stress’ refers to a multidimensional construct important for mental health management (17). In universities, students suffer from various stressors such as academics, social adaptation, and finances. Research shows that low mental health literacy is linked to poorer mental health among students (18). Many university students are unable to identify symptoms of the common disorders of anxiety and depression, which delays their help-seeking behavior. Moreover, like the other findings, stigmas and misunderstandings regarding mental health continue to limit access to care (19). According to Wei and his colleagues’ research paper published in 2015, higher Mental Health Literacy is associated with improved utilization of counseling services (20).
Although it is important, MHL is not sufficiently covered in many schools. Programs that promote mental health literacy, psychoeducation, peer counselling, and stigma reduction have shown promising results but are not universally implemented (21). For instance, students exposed to mental health literacy interventions are more likely to seek help and have less stigma toward mental illness (22).
Happiness is often understood to be an enduring experience of positive emotions and life satisfaction. It is a key element of mental health. It includes one’s feelings and evaluation of life (5). In the context of university life, happiness has been related to academic success, resilience, and social engagement, and a student at a university feels less happy due to stressors like workload, peer competition, and financial instability (23). Happiness does not only depend on luck. It depends on psychological and behavioral causes, too. According to Jiang et al. (24), students with a strong support system, regular exercise, and life purpose felt happier than average. This indicates that happiness is a variable that can be altered due to internal and external factors or influences.
The present research suggests that mental health might be important for happiness. Someone with a higher MHL (Mental Health Literacy) can better manage stress symptoms and experience positive moods (25). Moreover, information on mental health encourages adaptive coping strategies like seeking support or engaging in self-care which is linked with greater life satisfaction and emotional well-being.
Reavley and Jorm (26) propose that mental health literacy contributes to happiness in an indirect manner. The way they do so is by reducing the stigma attached to mental health problems, which consequently facilitates the use of mental health resources. When people understand mental health conditions and feel capable of dealing with them, they can maintain positive mental health. On the flip side, having low MHL can lead to misconceptions, avoidance, and delays in addressing the issues, consequently heightening distress and lowering happiness. Research into this area may be limited, but the result highlights a possible link between MHL and happiness. The explanation for this relationship is still unclear in a university context. For instance, does MHL lead to decreased depression, or does it cause increased well-being, such as confidence, social support, and resilience, for the individual?
Many demographic and behavioral variables affect both MHL and happiness. The most important determinants of mental health include age, sex, and wealth. According to Gagnon et al. (27), females may have higher mental health literacy than males, but they also report experiencing higher stress and anxiety, which suggests that knowledge is not everything. Socioeconomic factors are associated with financial constraints, access to mental health-related resources, and overall life satisfaction, which forms the basis of the relationship between MHL and happiness (28). Physical activity, connections with others, and doing meaningful things also matter a lot. Regular exercise can improve MHL (mental health literacy) and happiness by reducing anxiety (29). Social support networks help enhance mental health literacy by mutual sharing of knowledge and information while supporting happiness through emotional and instrumental support.
Another important consideration is cultural context. In societies where collective idealism is more celebrated, the stigma against mental illness may be more pronounced (30). MHL intervention here needs to address barriers to help-seeking by creating more help-giving. Culturally tailored mental health literacy (MHL) programs are more effective than universal programs at reducing stigma and promoting positive mental health outcomes (31). While previous studies provide a better understanding of MHL and happiness, there are still gaps. The author writes that research exploring the direct relationship between mental health literacy and happiness is limited among university students. Also, the role of mediating factors like self-efficacy or resilience is unclear. There is a need for longitudinal studies to determine the causality and the long-term effects of MHL interventions on happiness and mental health. Also, there is a lack of studies investigating how institutional factors, like university policies and mental campus health services, influence MHL and happiness. These contextual factors underpinning the issue will help formulate the solutions.
It is evident from the literature that mental health literacy plays an essential role in mental health and happiness. Individuals can tackle their mental health issues and become more robust thanks to High MHL rising to the occasion, ultimately strengthening their lasting happiness. How MHL associates with happiness is not studied much especially in students. The study aimed to shed light on the relationship between mental health literacy and happiness in a university environment while considering demographic and behavioral variables. By participating in this evolving research area, the examination seeks to speak about evidence-based procedures to promote pupil well-being and establish positive mental health outcomes.
Based on the Review of literature the following research questions were developed:
How does mental health literacy (MHL) influence the happiness levels of university students, and do these effects vary based on age and gender?
What is the relationship between student employment status and happiness levels, and how does MHL moderate this?
To what extent do family attitudes toward mental health impact university students’ mental health literacy and overall happiness?
How do different lifestyle choices correlate with mental health literacy and happiness among university students?
How does academic success shape university students’ mental health, literacy, and happiness?
This study, which aims to evaluate university students’ mental health literacy and happiness levels, is a descriptive study conducted with a quantitative design and Likert-type scales. Data were collected through face-to-face survey methods. An attempt was made to reach the entire population, but due to reasons such as unwillingness to continue, incomplete responses, and absenteeism, 752 students were excluded from the study. The sample size was calculated for a known population with a 95% confidence interval and a 5% margin of error. As a result of these calculations, the minimum sample size was determined to be 291 people based on the total number of individuals in the population. Students who left the survey incomplete or did not wish to continue were excluded from the study, and the data were collected based on voluntary participation. Missing data resulting from incomplete markings in the face-to-face surveys are noted in the tables.
Study Population and Sample. The study population in this research consists of private university students who enrolled in Istanbul during the spring semester of the 2023–2024 academic year. A stratified random sampling of main subgroups will select the final sample of 443 students. Researchers divided students on the basis of demographics and academic characteristics, namely age, gender, year of study, and academic program, to ensure diversity and representation in the student population. The sampling method ensured that students from different years (freshman, sophomore, junior, senior) and varied fields of the university were adequately represented. This made the findings more applicable to undergraduate students at private universities in Istanbul.
In this study, a Personal Information Form, the Short Form of the Oxford Happiness Questionnaire (OHQ-SF) (32, 32), and the Mental Health Literacy Scale (MHLS) (33) were used.
Personal Information Form: The 30-item Personal Information Form developed by the researchers includes questions about the participants’ demographic characteristics, smoking habits, alcohol use, chronic illnesses of the participant or their family, exercise habits, healthy eating habits, and psychological health of the participant or their family.
Oxford Happiness Questionnaire Short Form (OHQ-SF): The Oxford Happiness Questionnaire Short Form, developed by Hills and Argyle (32), is an 8-item scale assessing happiness. This scale was translated into Turkish and adapted by Doğan and Çötok (34). As a result of item analysis, item 4 (“I do not think I look attractive”) was removed due to a total correlation of.17, and the scale was analyzed with 7 items. The item-total correlation values of the scale ranged between.36 and.55 (34). The scale uses a 5-point Likert-type rating system: (1- Strongly Disagree, 2- Disagree, 3- Slightly Agree, 4- Agree, 5- Strongly Agree). Items 1 and 7 are reverse-coded, and a high score indicates higher happiness. The internal consistency coefficient of the scale was calculated as 74 using Cronbach’s alpha, indicating sufficient reliability. The test-retest reliability coefficient was also found to be.85, demonstrating the scale’s consistency over time.
The Mental Health Literacy Scale (MHLS) developed by Jung et al. (33) consists of 26 items and three subscales. During the Turkish validation and reliability study conducted by Göktaş et al. (35), two items (items 9 and 14) were removed following Exploratory Factor Analysis, and two more items (items 11 and 18) were excluded after Confirmatory Factor Analysis (35). The internal consistency coefficient (Cronbach’s alpha) of the scale was found to be.71. The scale consists of 22 items divided into three subscales: Knowledge-Oriented MHLS (11 items), Belief-Oriented MHLS (8 items), and Resource-Oriented MHLS (4 items). The Belief-Oriented subscale is reverse-coded. The first 18 questions, comprising the first and second subscales, are rated on a Likert scale: “1- Strongly Agree,” “2- Agree,” “3- Neutral,” “4- Disagree,” “5- Strongly Disagree,” “6- Do not Know.” The last four questions of the Resource-Oriented subscale are answered with “yes” or “no.”.
This study analyzed data using descriptive statistics and one-way ANOVA. The ANOVA test was used to determine whether there were statistically significant differences between groups, and the F and p values were evaluated. Variables such as gender, education level, chronic illness, smoking, healthy eating, and medication use were examined. The results indicated a significant relationship between healthy eating, chronic illness, and happiness levels (measured by OHQ-SF), while no significant differences were found for other variables. The analyses are presented in tables.
This study’s analysis section will cover the nature of the relationship between mental health literacy (MHL) and the happiness levels of university students. Analysis of selected socio-demographics, lifestyle behavior, and psychological characteristics assesses their effects on the Mental Health Literacy Scale (MHLS) and Oxford Happiness Questionnaire (OHQ-SF) scores. Descriptive statistics, ANOVA, and correlation statistical techniques will be used to determine the significance of the result. The study results provide a better understanding of mental health awareness, resource utilization, belief systems, and emotional states among students.
The socio-demographic characteristics of the study participants are depicted in Table 1. More than half of the respondents aged between 21–25 belong to the 61.5%. Only a few respondents were aged between 26–30 (5.6%) and above 30 (1.3%). The Sample had more women (60.9%) than men (39.1%). The majority of participants were single (94.6%); a smaller portion of them were married (5.0%); and the least was widowed/divorced (0.5%). Most students (74.0%) claimed not to be employed, while 26.0% were employed. Among the surveyed population, 75.2% indicated having an average income, while 20.8% reported a good income and 4.1% high income. Academic performance was rated mostly average (52.8%) and sound (46.5%), while only 0.7% rated it as poor. Most of the individuals lived with their family (62.3%), whereas (24.2%) lived in a dormitory, (4.5%) lived with friends, and (9.0%) lived in other accommodations; most of the participants lived in a city (69.8%), district (25.5%), and village (4.7%). Most families described their attitudes as protective (38.8%) and democratic (30.0%). Less often, they reported their family attitude as authoritarian (23.5%) and inconsistent (7.7%). The most prevalent type of family arrangement was the nuclear type, which constituted about 78.6% of the family structure. Traditional family systems were reported by 15.6% of the respondents. While 2.7% were from a single parent and 3.2% were from other family arrangements, this descriptive profile provides valuable information about the interaction between socio-demographic characteristics with mental health literacy and happiness among the participants.
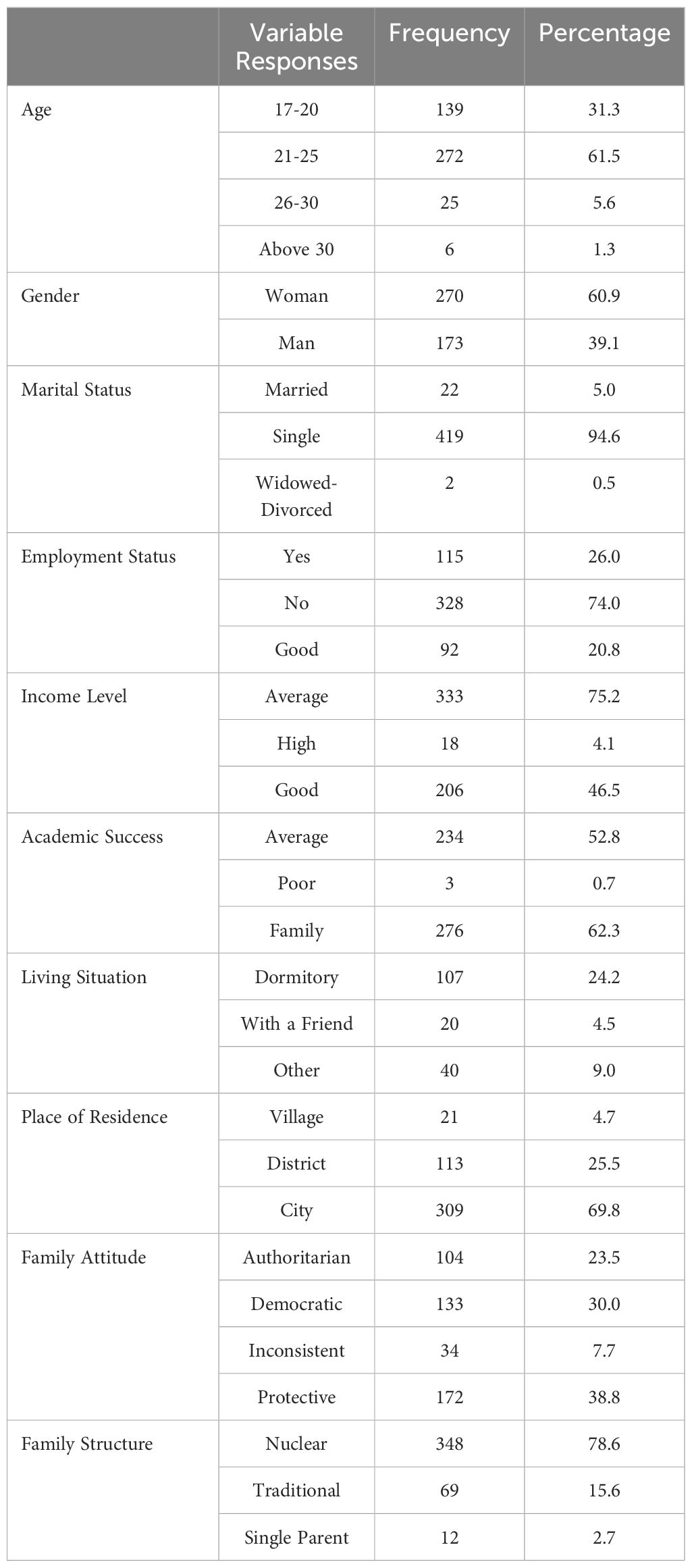
Table 1. Socio-demographic profile.
The participants’ lifestyle, health, and psychological characteristics give great insights (Table 2). Most of the participants (74.7%) reported that they did not smoke, while (25.3%) reported smoking. Of the participants, 75.6% practiced non-drinking, while 24.4% reported drinking alcohol. Based on these findings show that most people in the population do not smoke or drink. However, quite a lot of the participants do smoke and drink. Over 61.4% of respondents claimed they perceived their health to be good. Of the total respondents, 39 percent considered their health above average, while 368 percent rated theirs as average. Only a tiny fraction, 1.8 percent, rated theirs as bad. Most participants appear to have a positive perception of their health, which may contribute to their happiness and mental well-being. 11.8% of the participants reported chronic illness, while the majority (88.2%) reported no chronic illness. The participants’ perception of their health status was positive in this situation, consistent with the low prevalence of chronic conditions. In relation to chronic disease family history, the response was fairly balanced, as 48.1% had a family history of chronic disease, whereas 51.9% did not have a family history of chronic illnesses. Out of the total sample, 11.1% used medication, while 88.9% did not. This is consistent with the overall trend towards good health and low chronic illness. However, a segment of our population that relies on medication may suffer from a health condition that negatively affects their mental health, literacy, or happiness. According to our findings, 22.8% of participants exercised regularly, while a considerable % of the population, 77.2%, did not exercise regularly. Limited levels of physical activity participation are a potential concern as participation in physical activity is associated with a beneficial increase in mental health. Regarding healthy eating habits, 53.0% of participants followed a healthy diet, while 47.0% did not eat healthily. Just over half the population adhered to healthy eating, which leaves a large percentage of the population who are likely able to eat more healthily. Almost one-fourth of the study’s participants were found to have had psychological problems, according to 24.4% of the participants. On the other hand, 75.6% of people face no psychological issues. Support status was especially low, with just 18.7% of the respondents stating that they received support, while 81.3% stated there was no support. The participants reveal a lack of support systems. Consequently, it could adversely affect their offer when dealing with psychological or emotional issues. Finally, 11.1% of participants said their family has a mental health problem, while 88.9% said their family does not have any. The indication is that most of the respondents do not have exposure to mental health problems in their family. However the number might be less for some. This extensive analysis of lifestyle, health, and psychological characteristics is a great protocol for understanding the relationship between mental health literacy and happiness levels in university students.
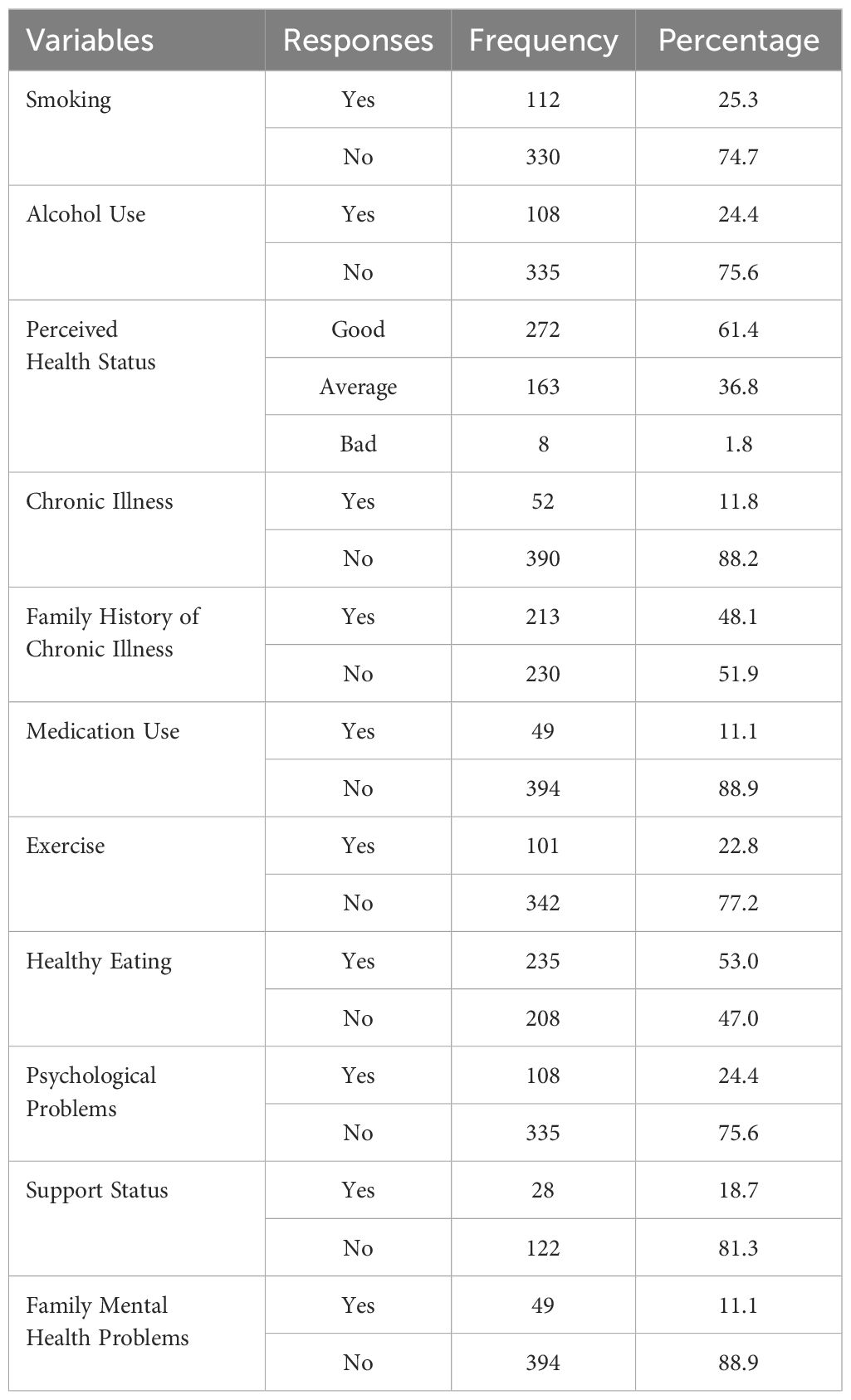
Table 2. Lifestyle, health, and psychological characteristics of the participants.
The comparison of mental health literacy (MHL) subscale scores and happiness levels as measured by OHQ-SF across age groups is shown in Table 3. One MHL subscale has a significant difference, whereas other subscales and happiness scores do not differ significantly. A statistical analysis showed that the Knowledge-Oriented MHLS scores varied significantly according to age (F = 11.317, p < 0.001). Those aged 21–25 had the highest mean score of 8.74 and an SD of 1.69. This indicates they were more aware of mental health knowledge. The age bracket 17–20 and the age group 26–30 scored lower, with M = 7.73, SD = 1.774, and M = 7.75, SD = 1.962, respectively. Participants aged 30 and above scored slightly higher (M = 8.57, SD = 1.813), though the sample size for this group was very small (N = 7). No difference was found across age brackets in the Belief-Oriented MHLS scores (F = 1.476, p = 0.22). The difference between the means of these groups was 0.48, with positive effect size being only meaningful in the 26-30 group because the higher mean was not in that 30 and above group. The 21-25 year-old had a mean score of 6.14 (SD = 1.937), while the 17-20 year-old had a mean score of 6.42 (SD = 1.281).
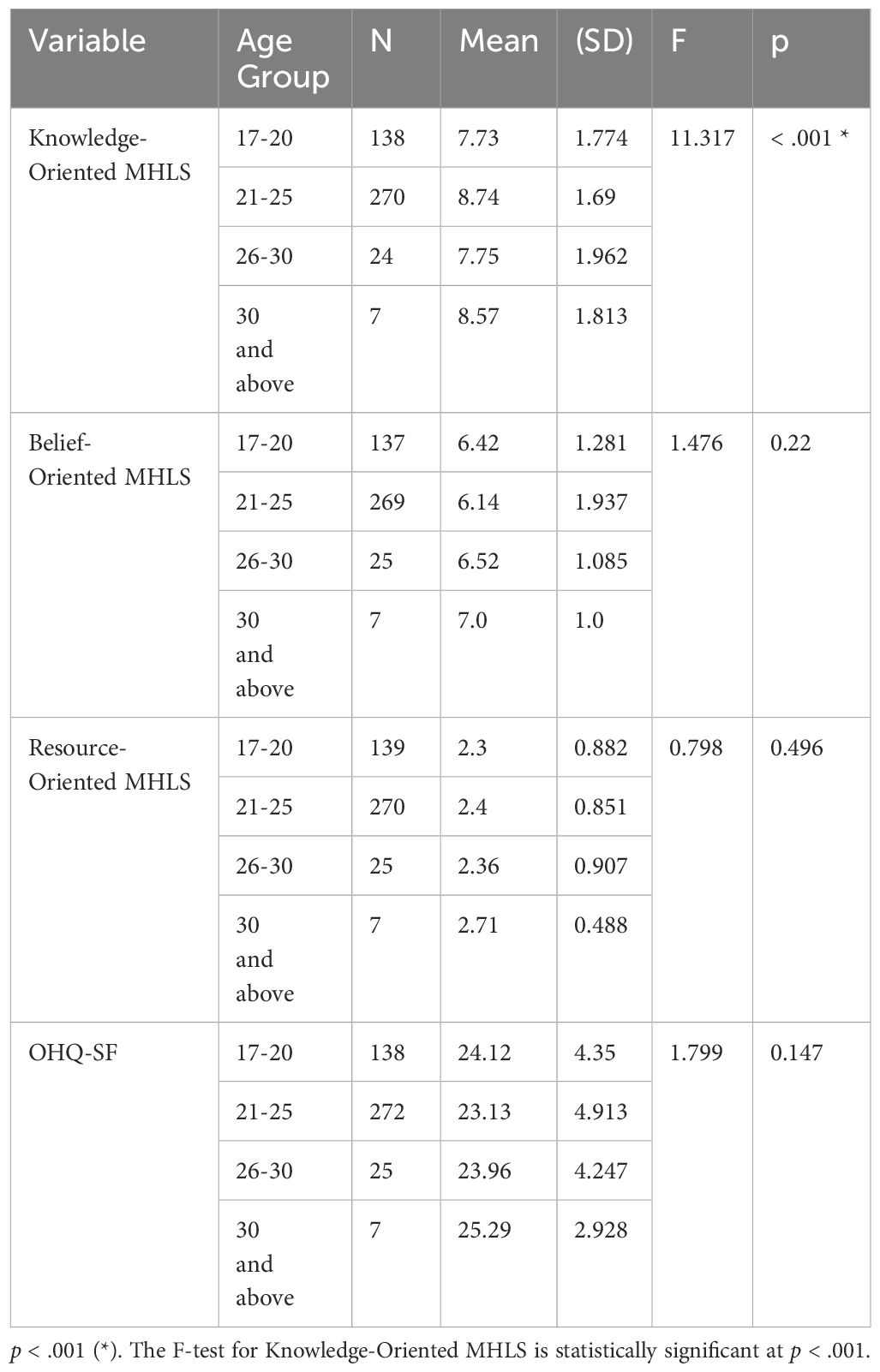
Table 3. Comparison of MHLS and OHQ-SF scores by students’ age.
The Resource-Oriented MHLS scores showed no significant differences across age groups (F = 0.798, p = 0.496). People of all age groups scored the same on the test. However, those aged 30 and above scored slightly higher (M = 2.71, SD = 0.488). The group of people who were 21-25 was found to have a mean score of 2.4 (SD=0.851), while the 17-20 and 26-30 groups happened to have similar mean scores of 2.3 (SD=0.882) and 2.36 (SD=0.907) respectively. No statistically significant differences in happiness (OHQ-SF scores) between age groups (F = 1.799, p = 0.147) exist. The mean score revealed similarities, where the maximum mean of 30 and above group (M = 25.29, SD = 2.928) followed by the 17–20 group (M = 24.12, SD = 4.35). The happiness score for participants between 21 and 25 was slightly lower (M = 23.13, SD = 4.913), and the score for participants aged 26 to 30 was 23.96 (SD = 4.247).
Table 4 compares mental health literacy (MHL) subscales and happiness levels (OHQ-SF) of gender groups. There exists a significant gender difference in one of the MHL subscales, while others and the happiness levels of men and women were similar. Both genders significantly differed in Knowledge-Oriented MHLS score F=22.5908, p<0.001. Women had a significantly higher average score of 8.68 compared to men, whose average score was 7.86. Women have more awareness and knowledge of mental health than men. The Belief-Oriented MHLS scores did not differ much between genders (F = 0.0249, p = 0.875). Women scored 6.25 (SD = 1.733) while men scored 6.28 (SD = 1.675), meaning the attitudes and beliefs of both women and men about mental illness and its plight were similar. There was no significant difference in the Resource-Oriented MHLS scores between males and females (F = 1.2983, p = 0.255). The difference was statistically insignificant, while men scored somewhat higher (M=2.43, SD=0.79) than women (M=2.34, SD=0.901). This shows that both men and women are equally familiar with mental health services. Happiness levels, as given OHQ-SF, did not differ significantly between the genders (F = 0.3023, p = 0.583). The mean happiness score for women was 23.62 (SD 4.932), which is not much different from that of men at 23.37 (SD 4.316). According to this finding, both males and females are equally happy.
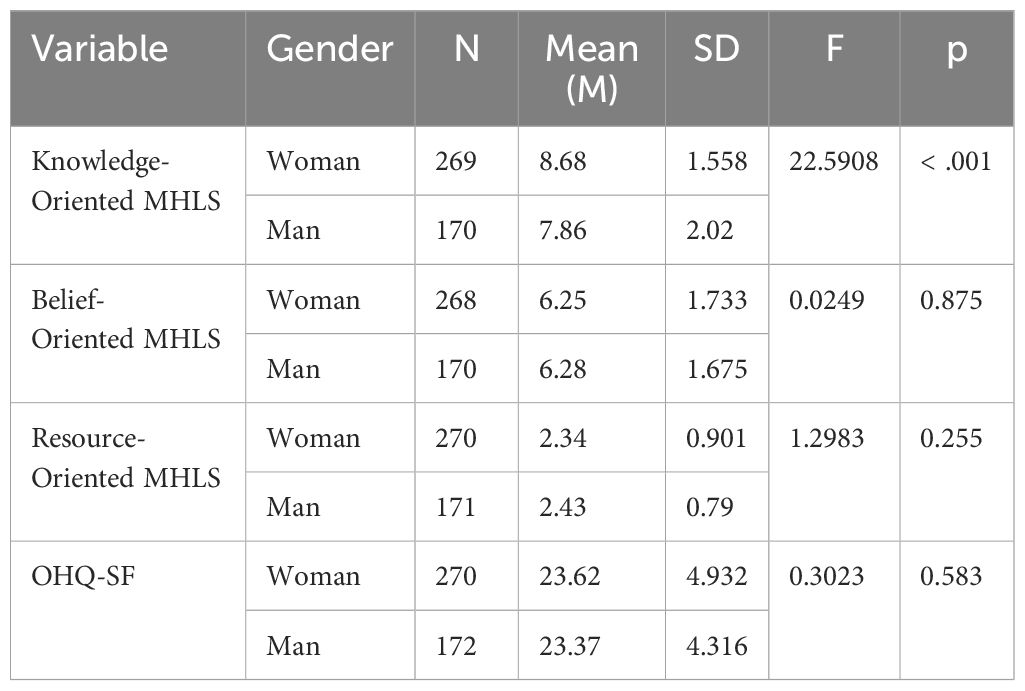
Table 4. Comparison of MHLS and OHQ-SF scores by gender.
Table 5 displays MHL subscales and happiness (OHQ-SF) scores obtained by students according to their employment status. The Knowledge-Oriented MHLS values of employed and unemployed students did not significantly differ (F = 2.225, p = 0.137). The average score of employed students was 8.15 (SD = 1.924), less than that of unemployed students, 8.44 (SD = 1.743). However, a statistically significant difference was found in the Belief-Oriented MHLS subscale (F = 7.15, p = 0.008). Students with no jobs scored more (M = 6.39, SD = 1.596) than those with jobs (M = 5.89, SD = 1.957). The employed students (M = 2.4, SD = 0.896) did not score differently from unemployed students (M = 2.37, SD = 0.848; F = 0.14, p = 0.708) on the Resource-Oriented MHLS subscale. Therefore, employed and unemployed students have the same familiarity with mental health resources. Like that, there were no sizeable differences in happiness scores (OHQ-SF) across employment status (F=0.11, p=0.741). The average happiness score of employed students was 23.39 (SD = 4.794), which was not too different from that of unemployed students (M = 23.56, SD = 4.672). So, based on the findings, it can be said that although beliefs regarding mental health differ significantly on the basis of employment status, knowledge-oriented and resource-oriented mental health literacy, and happiness do not differ significantly.
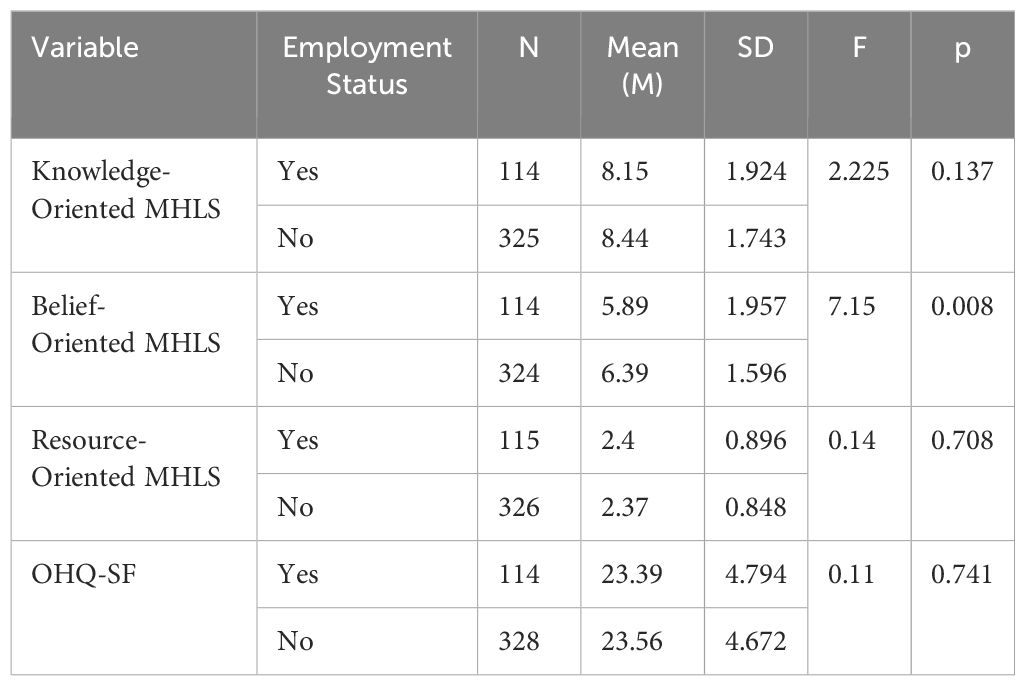
Table 5. Comparison of MHLS and OHQ-SF scores by students’ employment status.
Table 6 displays MHL subscales and OHQ-SF scores according to students’ academic success. There were no significant differences in Knowledge-Oriented MHLS scores based on the level of academic success (F=1.544, p=0.215). Those with good academic success rated their academic success at 8.52 (SD = 1.706), whereas those with academic success rated their academic success at 8.23 (SD = 1.855). Lastly, those with poor academic success rated their academic success at 8.0 (SD = 2.646). Likewise, the Belief-Oriented MHLS (F = 0.282, p = 0.754) score does not differ significantly among the groups. The good academic success group score was M = 6.26 (SD = 1.716). The average group score was M = 6.25 (SD = 1.716). Finally, the poor academic success group score was M = 7.0 (SD = 0.0). However, the sample size for this group is very small. Concerning the Resource-Oriented subscale of MHLS, significant differences were obtained (p = 0.02, F = 3.953). Students with poor academic success were significantly lower (M = 1.0, SD = 1.0) compared to those with good (M = 2.37, SD = 0.84) and average academic success (M = 2.39, SD = 0.865). This means students with low academic performance probably know less about mental health resources.
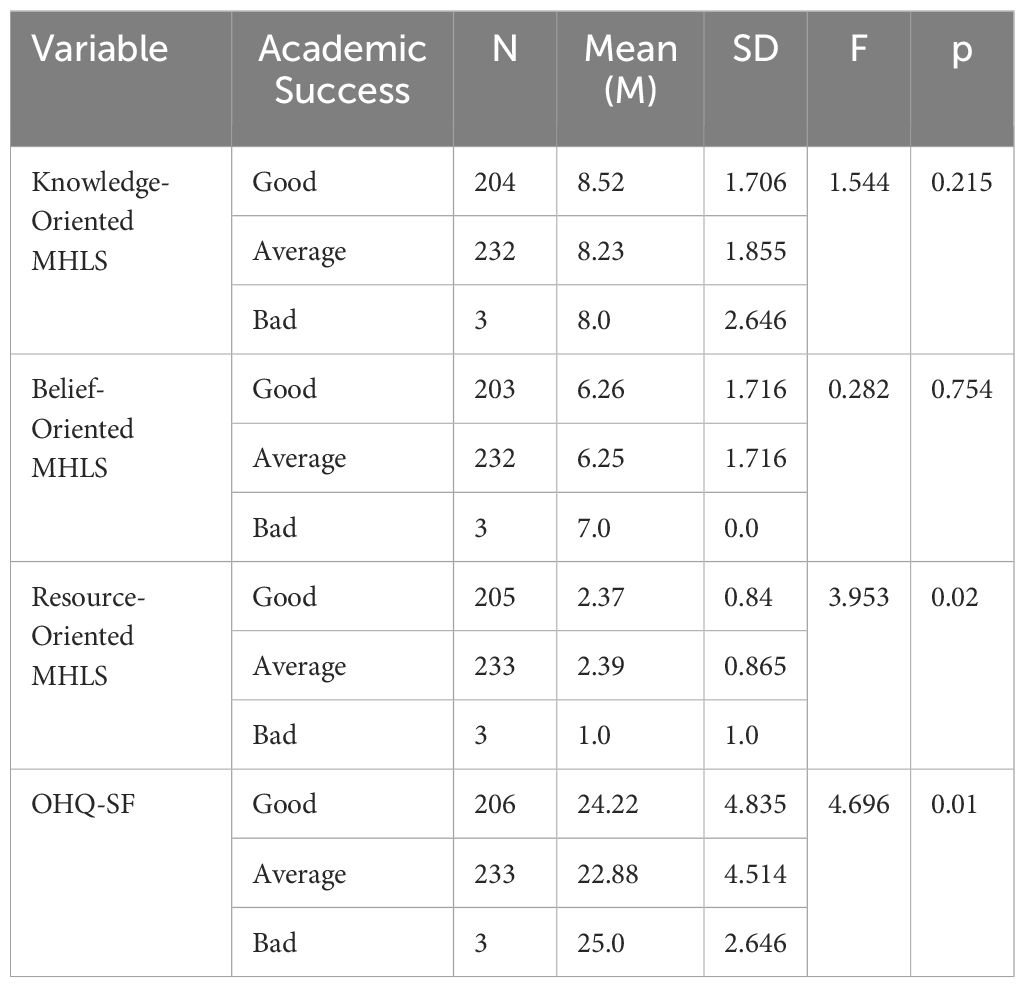
Table 6. Comparison of MHLS and OHQ-SF scores by students’ academic success.
The happiness scores (OHQ-SF) significantly differed due to the academic success levels (F = 4.696, p = 0.01). Based on students’ academic performance, the happiest group was students with good academic performance, whose mean is 24.22 while the standard deviation is 4.835. Followed by students with poor academic performance, whose mean is 25.0 and whose standard deviation is 2.646, and lastly, students with average academic performance, whose mean is 22.88, whose standard deviation is 4.514. According to these findings, academic achievement impacts happiness and knowledge of mental health resources, but the knowledge and beliefs about mental health remain constant.
Table 7 shows the results of the MHL subscales and OHQ-SF scores by Students’ living situations. Results showed no significant difference (F 1.186; p 0.315) in the Knowledge-Oriented MHLS score of the student that lives with family (M 8.41; SD 1.79), dormitory (M 8.12; SD 1.931), friends (M 8.35; SD 1.309) and other (M 8.7; SD 1.62). This data demonstrates that mental health knowledge does not differ due to living situations. The scores of Belief-Oriented MHLS are not significantly different for their living situation (F= 0.819, p= 0.484). According to the results, students staying with their families were scoring a bit higher (M = 6.35, SD = 1.61) than those staying in the dormitories (M = 6.16, SD = 1.792), with friends (M = 5.95, SD = 1.669), and others (M = 6.05, SD = 2.124). The Resource-Oriented scores on the MHLS were also similar across the groups (F = 1.16, p = 0.325). The score ranged from 2.25 (SD=0.972) of dormitory residents to 2.5 (SD=0.688) of friends’ council residents. The same score message was for those living with family and other residents. Nonetheless, the OHQ-SF (happiness) score varied significantly between the different living situations (F=4.457, p=0.004). Students who lived in “other” arrangements reported the greatest happiness mean scores (M = 25.93, SD = 4.172) followed by those who lived with families (M = 23.47, SD = 4.564) and friends (M = 23.25, SD = 4.518) respectively. Dormitory residents reported the lowest happiness scores (M = 22.8, SD = 5.02). The study found that the arrangement of the space has an impact on happiness. In particular, dormitory living has been noted for contributing to lesser happiness.
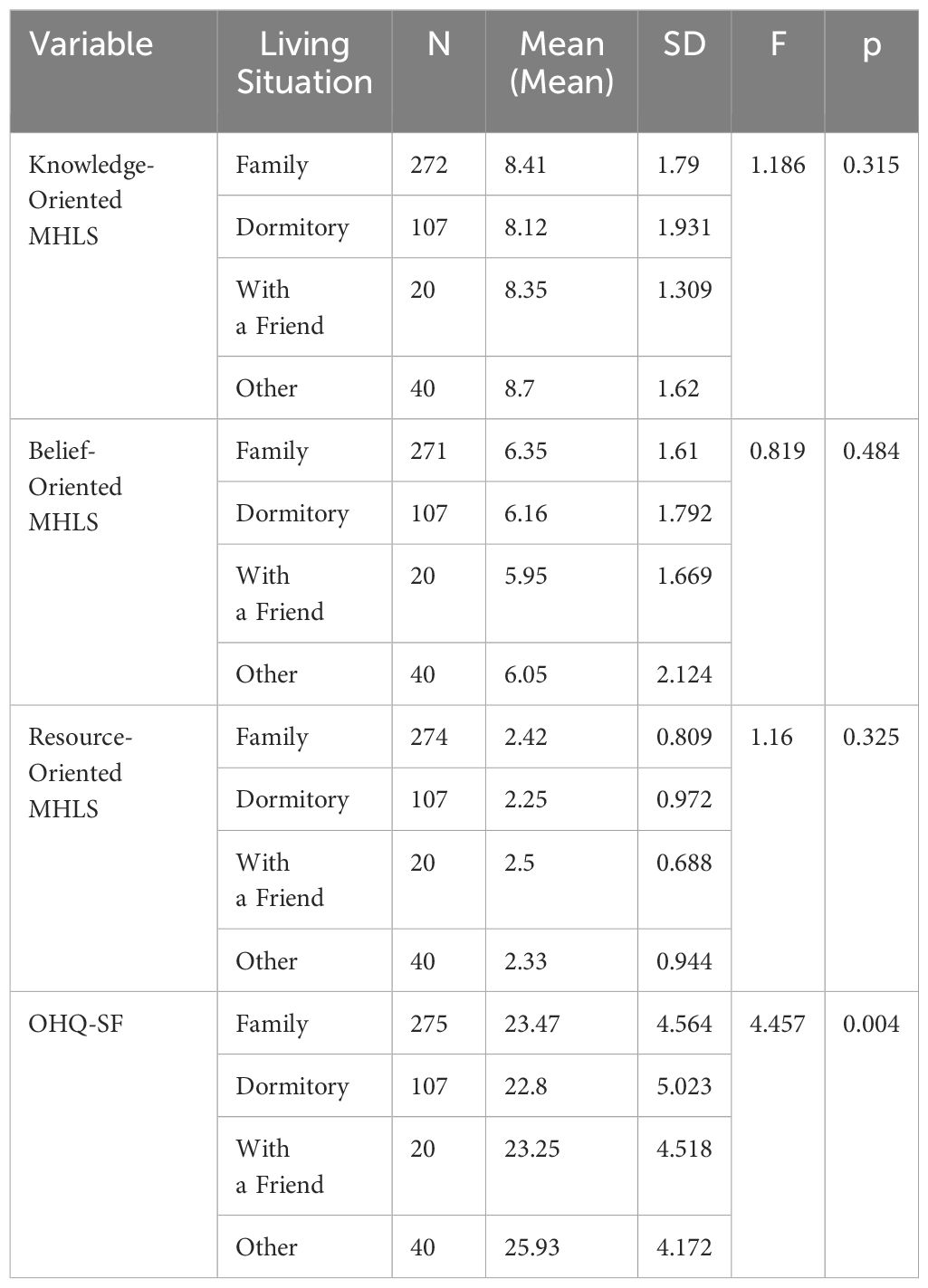
Table 7. Comparison of MHLS and OHQ-SF scores by students’ living situation.
Table 8 depicts the comparison of mental health literacy (MHL) subscales and happiness (OHQ-SF) scores and their different family attitudes (Authoritarian, Democratic, Inconsistent, and Protective). No meaningful differences were found regarding the Knowledge-Oriented MHLS (F = 1.83, p = 0.141). Participants belonging to families with an inconsistent attitude had the highest average score (M = 9.0, SD = 1.541) followed by those with a protective attitude (M = 8.37, SD = 1.766). Thereafter came democratic attitudes (M = 8.35, SD = 1.569) followed by authoritarian attitudes (M = 8.16, SD = 2.128). The difference in Scores was Not Significant. The Belief-Oriented MHLS did not demonstrate significant differences (F=1.21, p=0.304). Participants from republican families had a mean score of 6.05. Participants from democratic families had a mean score of 6.48. Participants who grew up in a protective family had a mean score of 6.39 (SD = 1.516), and those in an authoritarian family had a mean score of 6.24 (SD = 1.743). The Resource-Oriented MHLS demonstrated a significant variance in family attitudes (F = 2.66, p = 0.048). Participants with authoritarian families had the highest mean comparison in parenting styles with a mean of 2.48 (SD = 0.776), followed by protective families with a mean of 2.39 (SD = 0.835), democratic families with a mean of 2.37 (SD =0.866) and inconsistent family with a mean of 2.0 (SD = 1.118). It can be interpreted from the findings that participants from the democratic family are fewer cellular phone addicts. This indicates that families’ attitudes probably have some impact on the awareness of mental health resources, with authoritarian families being more scored on probably impactful variable. There were significant differences for the OHQ-SF (Happiness Scores) (F = 9.89, p < 0.001). People from protective families were the happiest (M = 24.23, SD = 4.321). Moreover, those from democratic families were right behind them (M = 24.14, SD = 4.518). Participants coming from authoritarian families had significantly lower scores (M = 22.68, SD = 4.975). An inconsistent family-type participant was reported with the lowest happiness level (M = 20.06, SD = 4.632). The findings of the study also showed that family attitudes could play an important part in happiness, with greater family attitudes having better effects.
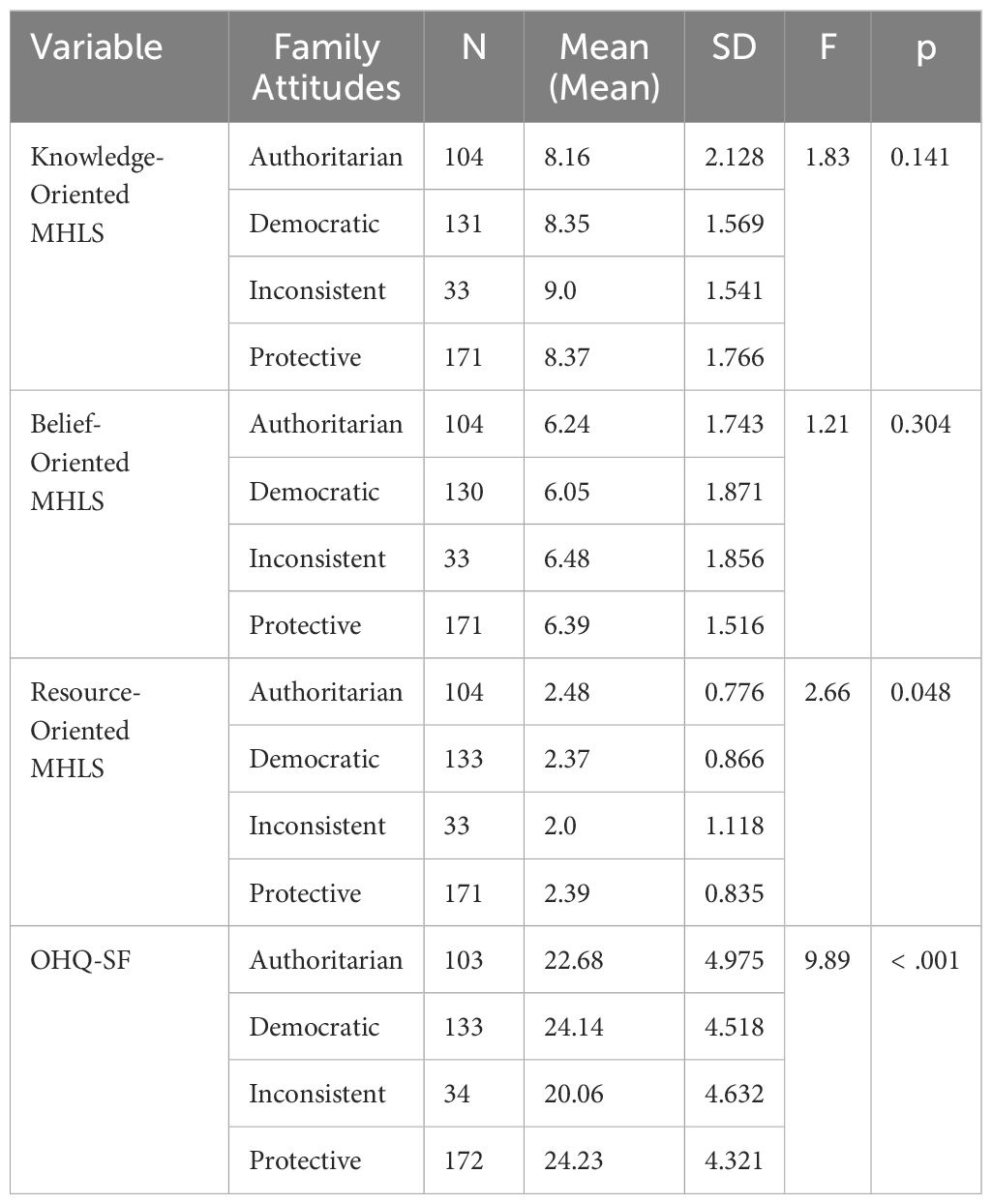
Table 8. Comparison of MHLS and OHQ-SF scores by students’ family attitudes.
Lifestyle Factors and Their Influence on MHLS and OHQ-SF Scores are depicted in Table 9. The examination of lifestyle factors (smoking, alcohol use, exercise, and healthy nutrition) towards happiness (OHQ-SF) and mental health literacy (MHL) subscales presented several significant findings, especially for happiness and specific mental health literacy sub-scales.
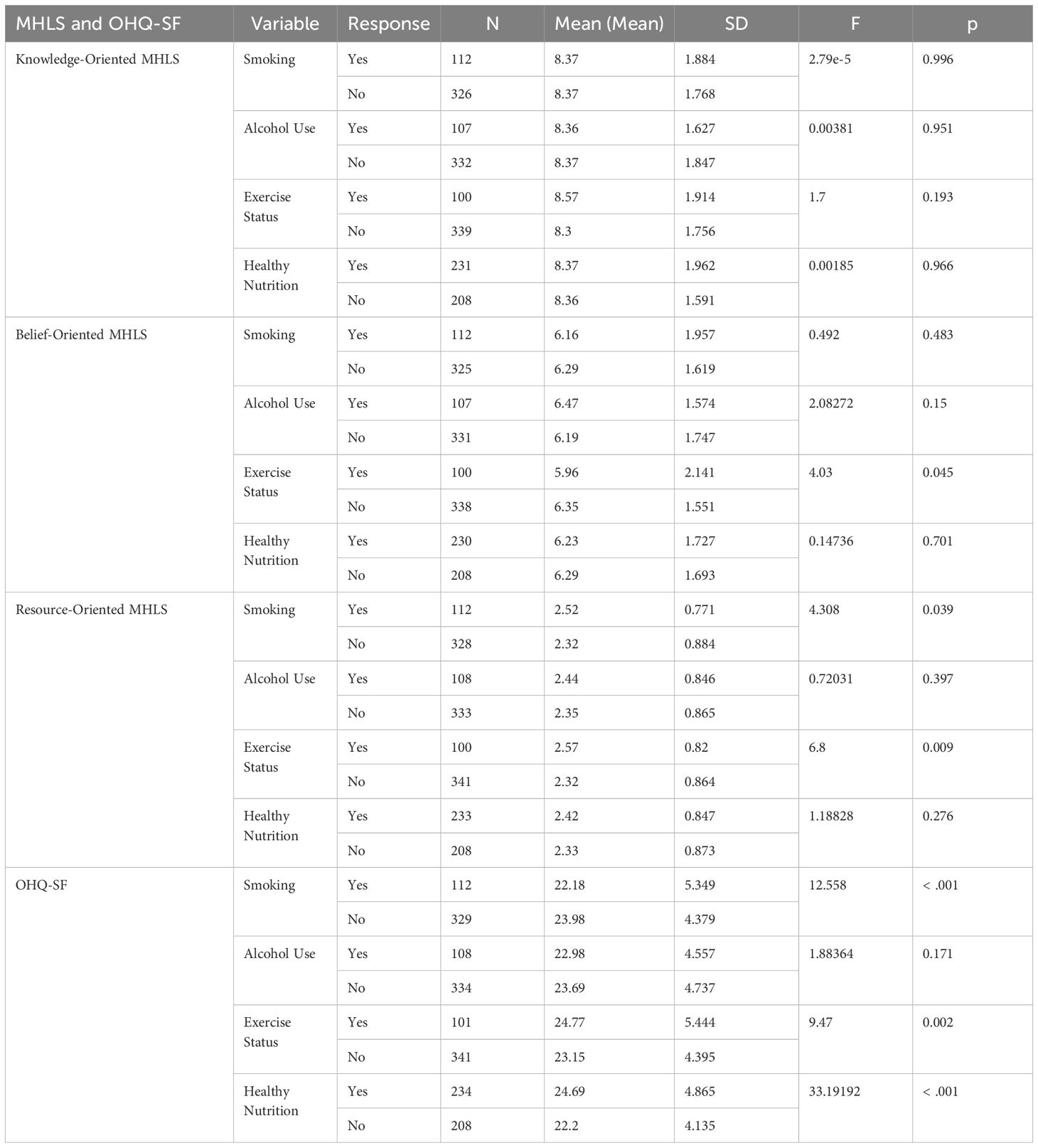
Table 9. Lifestyle factors and their influence on MHLS and OHQ-SF scores.
There were no significant differences among Knowledge-Oriented MHLS scores across all lifestyles. The means of smokers (M = 8.37, SD = 1.884) and the means of non-smokers (M = 8.37, SD = 1.768) were the same (F = 2.79e-5, p = 0.996). Smoking does not affect knowledge of mental illness. In the same way, drinkers (M = 8.36, SD = 1.627) and non-drinkers (M = 8.37, SD = 1.847) showed no difference in scores (F = 0.00381, p = 0.951). Participants who engaged in regular exercise (M = 8.57, SD = 1.914) scored higher than non-exercising participants (M = 8.3, SD = 1.756), but the difference was not significant (F = 1.7, p = 0.193). Again, no difference was observed with healthy nutrition habits since those who normally eat healthy (M = 8.37, SD = 1.962) and those who do not (M = 8.36, SD = 1.591; p = 0.966). The mental health literacy of young adults is not greatly affected by lifestyle choices.
According to the results, the exercise status of participants was significantly associated with the Belief-Oriented MHLS score. Not exercising participants (M=6.35, SD=1.551) scored higher than exercising participants (M=5.96, SD=2.141), possibly owing to beliefs or attitudes imparted by lifestyle habits. For smoking (F = 0.492, p = 0.483), alcohol use (F = 2.08272, p = 0.15), and healthy nutrition (F = 0.14736, p = 0.701), there are no significant differences with comparable scores across groups. Thus, any differences in mental health beliefs seen among humans are not due to the aforementioned Lifestyle.
There were notable differences in Resource-Oriented MHLS rates on smoking (F = 4.308, p = 0.039) and exercise status (F = 6.8, p = 0.009). Smokers (M = 2.52, SD = 0.771) were more familiar with the available mental health resources than non-smokers (M = 2.32, SD = 0.884). In the same way, subjects who train (M = 2.57, SD = 0.82) perform better than those who do not (M = 2.32, SD = 0.864). This finding implies that exercise may increase exposure to or knowledge of mental health resources. The study found that there were no significant differences in the use of alcohol (F = 0.72031, p = 0.397) and healthy nutrition (F = 1.18828, p = 0.276) based on the level of knowledge regarding mental health services.
Smoking, exercise, and healthy nutrition significantly affected the happiness scores of people. Non-smokers (M = 23.98, SD = 4.379) were significantly happier than smokers (M = 22.18, SD = 5.349; F = 12.558, p < 0.001). Likewise, participants who exercised regularly (M = 24.77, SD = 5.444) were happier than those who did not exercise (M = 23.15, SD = 4.395; F = 9.47, p = 0.002). From the table, it can be observed that healthy nutrition (F = 33.19192, p < 0.001) registered the most significant difference since individuals who practice healthy eating (M = 24.69, SD = 4.865) reported much higher happiness than individuals who do not practice healthy eating (M = 22.2, SD = 4.135). The use of alcohol did not significantly affect the happiness levels (F = 1.88364, p = 0.171) of the participants who drank alcohol (M = 22.98, SD = 4.557) when compared with their counterparts who abstained from alcohol (M = 23.69, SD = 4.737).
According to the analysis in Table 10, the significance of health-related factors (perceived health status, chronic diseases) and mental health-related factors (psychological problems, family mental health) on the sub-scales of MHL and OHQ-SF happiness is examined.
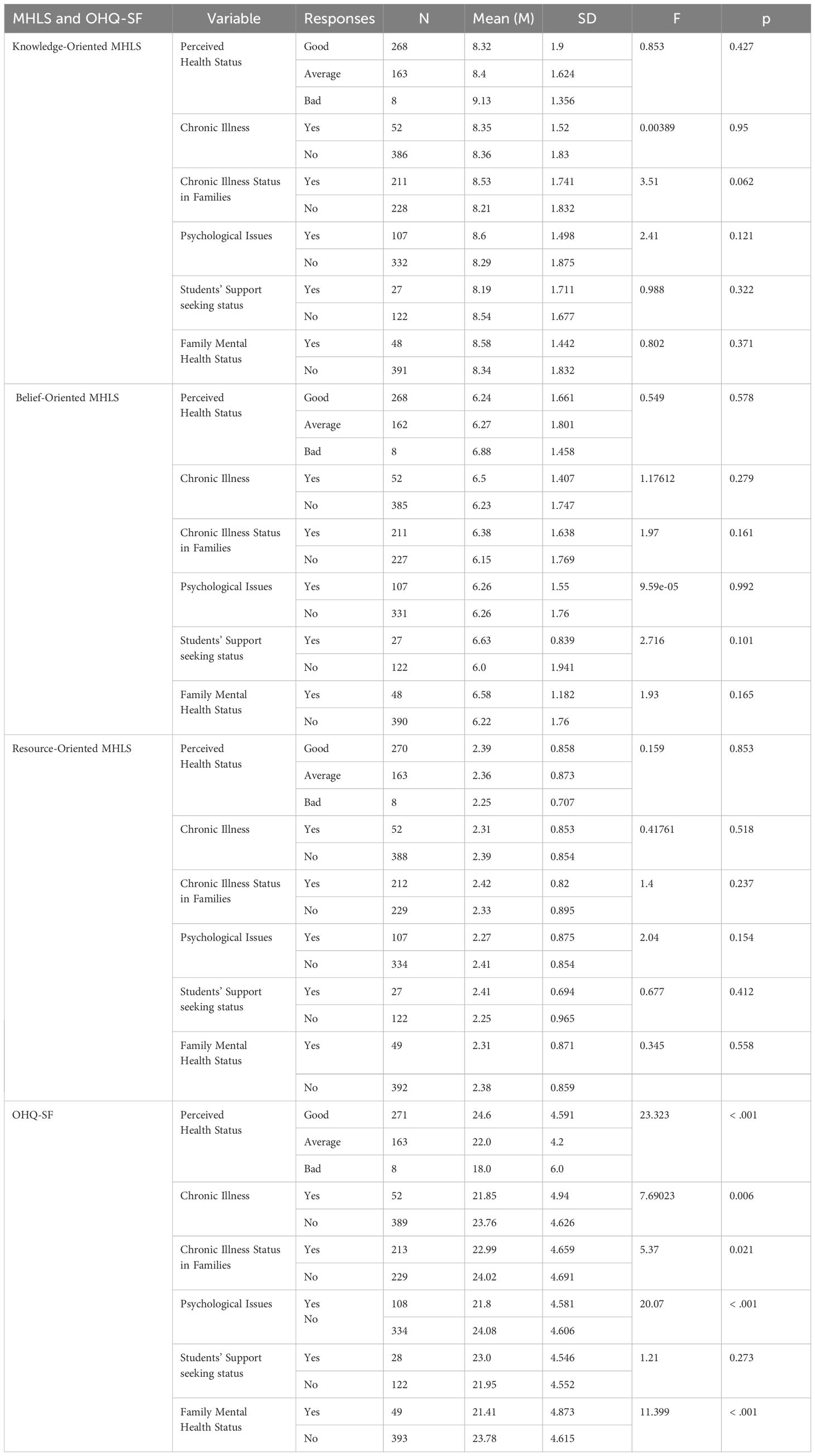
Table 10. Comparison of MHLS and OHQ-SF scores by students’ health and mental health.
Most health-related factors didn’t show any significant change in Knowledge-Oriented MHLS score. Perceived health status did not have a significant effect on knowledge scores (F = 0.853, p = 0.427). Good health status students (M = 8.32, SD = 1.9); average health status students (M = 8.4, SD = 1.624); bad health status students (M = 9.13, SD = 1.356). Likewise, the presence of chronic illness (F = 0.00389, p = 0.95) or family chronic illness history (F = 3.51, p = 0.062) demonstrated no significant differences. Students with psychological issues had slightly more knowledge (M = 8.6, SD = 1.498) than students with no psychological issues (F = 2.41, p = 0.121). However, it was not statistically significant. The knowledge-oriented literacy was established to have no significant results for the utilization of services by the families. Also, the families’ mental health was seen not to have significant results as well as the families’ tendency to seek out support for help.
There are no meaningful differences in the Belief-Oriented MHLS scores on perceived health status (F = 0.549, p = 0.578), chronic illness (F = 1.17612, p = 0.279) or family chronic illness status (F = 1.97, p = 0.161). Psychological problems did have a significant impact (F = 9.59e-05, p = 0.992) as the scores of students with psychological problems (M = 6.26, SD = 1.55) and without psychological problems (M = 6.26, SD = 1.76) were similar. In terms of support-seeking behavior, students who sought support scored higher (M = 6.63, SD = 0.839) compared to students who did not seek support (M = 6.0, SD = 1.941) but it was nearly significant (F = 2.716, p = 0.101) Family mental health was not statistically significant (F = 1.93, p = 0.165).
The MHLS scores that are resource-oriented were not affected by health status conditions or chronic disease. (F value = 0.159, P value = 0.853;F value = 0.41761, P value = 0.518). A survey of students with occupational therapy shows no significant difference in their chronic illness between the two groups of students (F = 1.4, p = 0.237). It was because students with and without family histories of chronic illness show no significant difference. The same goes for students with and without psychological problems. In the same way, support-seeking behavior (F = 0.677, p = 0.412) and mental health issues in the family (F = 0.345, p = 0.558) had no significant effect. These findings suggest that knowledge of and access to mental health resources are stable across these health variables.
Multiple health-related factors significantly impacted happiness levels (OHQ-SF). The effect of perceived health status was significant. (F=23.323, p<0.001). Students who reported good health have the highest scores (M=24.6, SD=4.591). Followed by those who reported with average health (M=22.0, SD=4.2) and bad health (M=18.0, SD=6.0). Happiness was significantly influenced by chronic illness (F = 7.69023, p = 0.006), where students without chronic illness (M = 23.76, SD = 4.626) scored higher than those with chronic illness (M = 21.85, SD = 4.94). The family’s chronic illness status illustrates significant effects, F = 5.37, p = 0.021. Nonetheless, students coming from families with no history of chronic illness demonstrated higher mean scores, M = 24.02, SD = 4.691, than those with a history of family chronic illness, M = 22.99, SD = 4.659. Psychological issues also played an essential role (F=20.07, p<0.001). The non-psychological issues group showed higher marks (M=24.08, SD=4.606) in comparison to the psychological issues group (M=21.8, SD=4.581). In conclusion, family mental health issues have significantly impacted happiness (F=11.399, p<0.001). The students from families without any mental health issues had a higher score (M=23.78, SD=4.615) compared to those with family mental health issues (M=21.41, SD=4.873) in the scale measuring happiness.
Table 11 performs the analysis regarding the correlations among the students’ happiness outcomes as measured by the OHQ-SF and the three subscales of mental health literacy Knowledge-Oriented, Belief-Oriented and Resource-Oriented MHLS. The findings show that relationships between the variables of interest are both significant and non-significant.
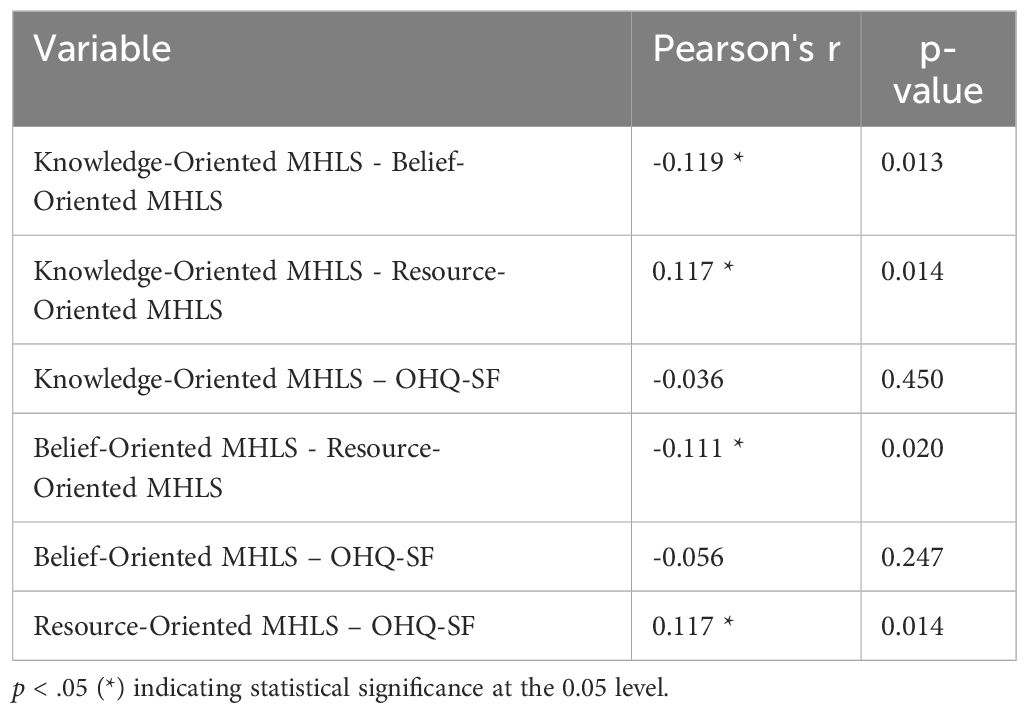
Table 11. Correlation between students’ happiness levels and mental health literacy.
The findings revealed a significant negative correlation (r = -0.119, p = 0.013) between the Knowledge-Oriented MHLS and Belief-Oriented MHLS sub-scales, suggesting that individuals with a higher level of mental health knowledge possess a slightly lower level of belief and attitude towards mental health. This finding could mean that people with more knowledge are less influenced by subjective beliefs. That is, people with a lot of factual knowledge may not be that influenced by subjective knowledge/beliefs.
A positive and significant correlation (r = 0.117, p = 0.014) was noted between the Knowledge-oriented MHLS and Resource-oriented MHLS, indicating that students who possess more knowledge about mental health are also aware of the resources available to them. This connection shows that knowledge could help someone get or know about resources, and it’s an essential part of mental health literacy. On the negative side, there is a significant correlation between the Resource-Oriented MHLS and the Belief-Oriented MHLS (r = −0.111, p = 0.020). That means that with the increase in beliefs and attitudes, the familiarity will decrease and vice-versa. The finding may show that people feel they can rely on beliefs if they do not have direct experience with tangible resources, possibly due to different exposure to mental health or education.
Since the correlation between Resource-Oriented MHLS and happiness score was 0.117 and significant at 0.05 level, it can be stated that the students who are familiar with mental health resources have higher happiness scores. The findings suggest that being aware of and having access to resources can lead to feelings of calmness. Furthermore, being able to access resources could provide the support needed when one is feeling stressed. Nevertheless, the study did not find a statistically significant correlation between the Knowledge-Oriented MHLS and happiness scores (r = −0.036, p = 0.450). As a result, this shows that they have an inverse relationship. The Mental Helplessness Scale (MHLS) score regarding a person’s belief was related to the score on the happiness scale. The correlation was also insignificant. Also, the correlation was negative in value (-0.056), and the p-value was also significant (0.247).
The results reveal that some aspects of mental health literacy, like knowing where help is available, are very closely related to happiness. However, knowing and their beliefs are not so strongly related to happiness. The inverse correlations between subscales such as Knowledge-Oriented and Belief-Oriented MHLS or Belief-Oriented and Resource-Oriented MHLS indicate that students may reasonably be integrating the two. For example, students who emphasize facts may de-emphasize beliefs, and students who believe in something may not care much about things. An intervention to enhance mental health literacy may improve the mental well-being of the public, and encourage an effective help-seeking process.
These outcomes reveal that mental health literacy and happiness have a complex relationship. Using practical resources may be positively related to emotional well-being, whereas wider knowledge or belief-driven factors may have an indirect relationship or require fuller investigation of their interactions. The analysis shows targeted intervention areas that need to be looked at, especially in relation to access to resources and integration of knowledge with beliefs to promote mental health literacy and happiness among students.
Table 12 presents the descriptive statistics of scores obtained by students for the subscales of the Mental Health Literacy Scale (MHLS) namely Knowledge-Oriented, Belief-Oriented, Resource-Oriented, Oxford Happiness Questionnaire (OHQ-SF) and Total MHLS. This information shows what was most likely to occur, the distance of scores from one another, and how far away the scores were. The mean for the Knowledge-Oriented MHLS subscale was 8.36 (SD = 1.79) with a median of 9.0 with most students scoring at the higher end. The minimum score was 0.0, and the maximum score was 10.0, which reflects a huge variation in the knowledge of participants. The accumulated score on this subscale was 3672.0 which means the students had a good level of knowledge about the same. The average score on the Belief-Oriented MHLS subscale (score of 6.26) was higher than for the Knowledge-Oriented subscale. Its range (i.e., lowest to highest score) was a little narrower, however (1.71), compared with the other subscale. The median on this subscale also indicates that the higher score (i.e., 7.0) was more common than the lower scores. The range of score is from 0.0 to 8.0 and the total sum is 2742.0. Based on these results, it can be concluded that students’ health beliefs and attitudes are fairly varied; although most are weighted towards the higher end. For this Resource-Oriented MHLS subscale, the mean was 2.37 (SD = .86), and the median was 3.0. Scores with a range of 0.0 as minimum and 4.0 as maximum had a narrow range. The whole score was 1047.0 which means low scores overall in all other subscales. This implies that even though students have good knowledge and beliefs regarding mental health, they have little knowledge about the resources.
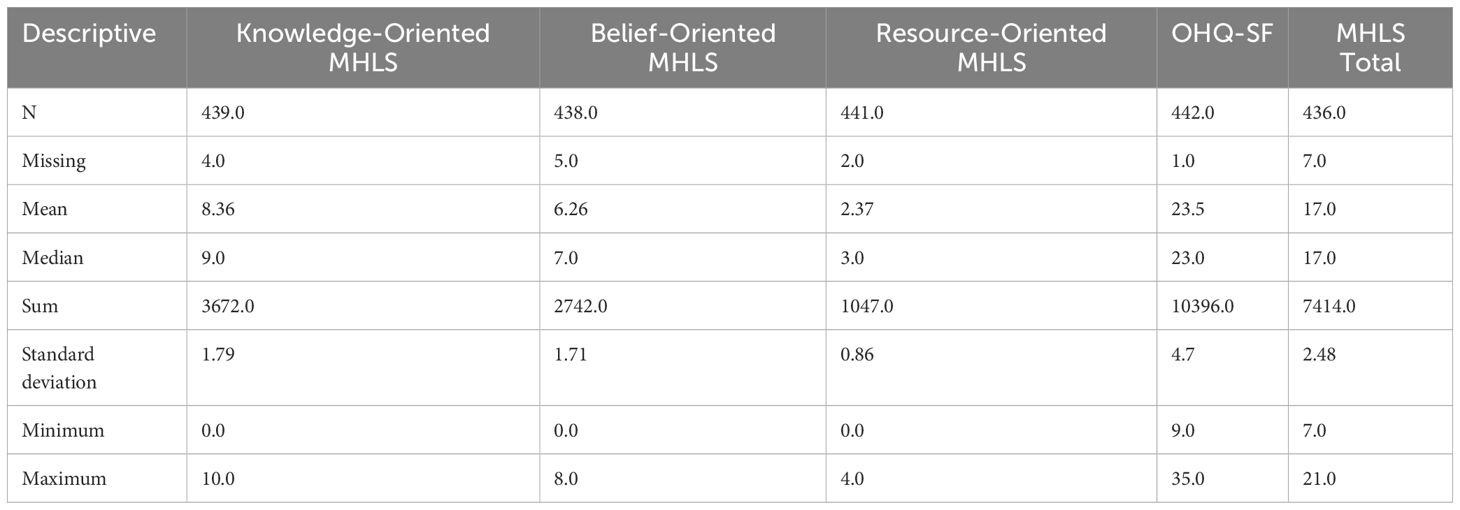
Table 12. The scores that students obtained from the scales and subgroups.
The mean for the OHQ-SF (Happiness) was 23.5 (SD=4.7), the median was 23.0. The minimum score was 9.0 and the maximum score was 35.0, reflecting considerable variation in the students’ happiness. The overall average happiness is moderate, summarizing a total score of 10396.0. Ultimately, the average for the MHLS Total score, which is the value of the three subscales, was 17.0 (SD = 2.48) with a median of 17.0, minimum of 7.0, and maximum of 21.0. Taking all the dimensions together, the sum was 7414.0, indicating a moderately high mental health literacy level. These stats show key patterns in students’ mental health literacy and happiness. Information and beliefs around mental health are relatively strong, but knowledge of resources is weak. Moreover, the high variation in the happiness score makes one further probe who is responsible for their happiness. With mostly equal median and mean values across most scales, the distributions can be said to be fairly symmetric. This report can be a basis for understanding the relationship between mental health literacy and happiness.
The relationship between mental health literacy (MHL) and happiness among university students was analyzed broadly. Further, the acceptance of the influence of demographic, lifestyle, health, and psychological factors was discussed. The study results fit well with established theories like Keyes’ Dual-Continua Model and improve on what is already known while offering fresh insights.
MHL shows notable differences based on gender, age, and demographic findings. Women demonstrated greater Knowledge-Oriented MHL, probably due to norms and expectations around emotions, help-seeking, etc. Some studies have shown that knowing more does not always make one happier. Being informed may not improve one’s feelings or emotions (27). According to Pedrelli et al., women are likely to experience a depression gap due to the demands of multitasking and stress, which negates the power of knowledge. On the other hand, men had lower Knowledge-Oriented scores for MHL, which may reflect how stigma and masculine ideologies still discourage emotionality (22). The small gender differences in MHL signal a universal need for improvement among all students.
Students aged 21–25 had the highest score on Knowledge-Oriented MHL. This is possibly due to their greater exposure to academic and social pressures and increased opportunities to use such mental health resources. Nevertheless, the lack of significant differences in happiness across age groups suggests that family support, resilience, and access to resources may be more important in promoting happiness (36).
Family dynamics became an essential determinant of happiness. Students from democratic and protective family setups feel happier than other children. Families with authoritarian or inconsistent dynamics were correlated with lower happiness but slightly higher Resource-Oriented MHL levels. This could show that people lean on outside help because family members are missing (39). The study’s results enhance the significance of family-based psychoeducation, proving it to be an important addition to any mental health intervention.
Lifestyle and health factors also played a critical role in happiness and MHL. According to Vaillant, it is a well-established fact that those with better physical health levels tend to be happier, as it is thought that physical and mental health are interconnected. Exercise regularly and eating healthily are strongly related to higher Resource-Oriented Mental Health Literacy (MHL) and happiness. This finding is consistent with existing literature showing that the relationship between physical and mental health is bidirectional (24). On the other hand, smokers had a greater Resource-Oriented MHL than non-smokers but were less happy. Thus, knowing about resources does not help.
Happiness also depended on living arrangements. College students who lived in dorms reported lower happiness scores than at home or with friends. This result shows that social support can help to relieve stress and improve emotional stability. Dormitories lacking stable support systems may add to academic pressure and social isolation (40). Initiatives focused on community-building in dorms may fill this gap and enhance students’ well-being.
Academic success was strongly associated with happiness, with students who performed better reporting more significant happiness levels. This indicates that children experiencing academic success tend to be emotionally stable and resilient. When students do well, they feel more purposeful, accomplished, and confident, contributing to happiness (11). On the other hand, poor academic achievement may lead to increased stress and anxiety in competitive universities. The significance of bridging academic counseling with mental health support is highlighted in the findings as students’ mental health and academic performance impact shaping in school.
The correlation analysis provided important information about the relationship between mental health literacy (MHL) subscales and happiness.
The greatest positive connection was noticed in Resource-Oriented MHL with happiness. This shows that people will be happy if they have access to knowledge and resources. Students with high resource-oriented MHL were most likely to be confident in seeking help when things got difficult, thus reducing stress and promoting resilience. According to Keyes (36), the Dual-Continua model supports the notion that resource utilization plays a promotive function for mental health. Moreover, this outcome lends credence to Fredrickson’s (37) broaden-and-build theory, which describes how positive emotions– emotions elicited through resource accessibility– broaden our thoughts and actions and foster happiness and resilience (37). The strong connection between these two variables highlights the importance of interventions enhancing student awareness and resource access.
The link between Knowledge-Oriented MHL and happiness was less strong, showing that knowledge does not always lead to happiness. Students with higher knowledge scores may have greater recognition of mental health problems, but this awareness does not make them feel any less distressed or more flourishing. Previous studies have found that knowledge-based interventions seldom target the emotional and behavioral aspects essential for well-being (26). Knowing all the reasons that should make us happy is different from actually doing it. This means that theories should not try to stick to the ‘ideal happy state’ but rather focus on skills to help us manage our day-to-day emotional experiences.
The finding showed that Belief-Oriented MHL and happiness had an insignificant or weak relationship, indicating that subjective mental health attitudes may not directly influence emotional feelings. According to Griffiths et al. (22), this finding is consistent with criticisms of belief-based approaches, which emphasize individual attitudes but overlook systemic or environmental structures that facilitate well-being. Some correlations were negative, specifically in the case of Knowledge-Oriented MHL and Belief-Oriented MHL, which might suggest a contradiction between knowledge and beliefs. Conflicting mental models, such as stigmatized attitudes versus evidence-based awareness, may prevent students from acting knowledgeably on their symptoms, which is reflected in this disparity. Initiatives to reduce stigma may help to reconcile these dimensions.
The interplay between the MHL subscales provided added insight. As an illustration, the Resource-Oriented MHL positively correlates with both the Knowledge-Oriented and Belief-Oriented MHL, meaning that resource awareness is usually built on knowledge and beliefs. The weak relationship between knowledge-oriented and belief-oriented mental health literacy (MHL) calls for integrative interventions to align them. The correlation patterns suggest that the MHL dimensions have different levels of importance for promoting happiness. Resource-Oriented MHL is probably the construct influencing well-being enhancement through the most directly actionable pathways. In contrast, Knowledge-Oriented MHL and Belief-Oriented MHL are arguably too far removed from practical outcomes to be strong enough. These ideas highlight the importance of utilizing resources when building mental health literacy knowledge and belief systems in a multi-faceted manner. The descriptive statistics accentuate the gap between MHL and students’ happiness in which a significant variation exists in the Resource-Oriented MHL score. This variation emphasizes the need for targeted interventions that cater to specific subgroups’ needs.
To sum up, the study shows a very complex relationship between MHL and Happiness. It emphasizes the need for resource-oriented interventions, gender sensitivity, and enabling environments for emotional well-being. According to these results, mental health literacy significantly contributes to happiness. It provides further insight and guidance for future studies and practices.
The research study’s results coincide with the work of Keyes (36) in the Dual-Continua Model, which argues that mental health is more the opposite of the absence of mental illness but rather the joint occurrence of positive mental states and the absence of psychological distress. The strong relationship between Resource-Oriented MHL scores and happiness shows that awareness of mental health resources plays a crucial role in happiness. This gives weight to the idea that flourishing can be promoted through both preventing and promoting practices, as emphasized in Keyes’ model (38); the findings indicating no other significant correlations between MHL subscales such as Knowledge-Oriented and happiness imply that knowledge may not be enough to help someone flourish. In other words, research should focus on self-efficacy, social support, and coping strategies that mediate the effect of mental health literacy on mental well-being.
Fredrickson (37) developed a useful broaden-and-build theory of positive emotions in interpreting this finding. Fredrickson’s broaden-and-build theory states that positive emotions widen one’s thoughts-and-action repertoire. Moreover, it builds lasting personal resources. According to the study, access to mental health resources, whether real or imagined, triggers positive emotions and reinforces happiness. For instance, students aware of the available resources tend to experience less stress as they know they can find help when faced with difficulties. Research into whether these factors happen simultaneously or whether one brings about the other is called causation.
The research also provides insight into gender dynamics and mental health literacy. Women scored higher than men on knowledge-oriented mental health literacy, which means they are better at acquiring mental health knowledge and applying it to their lives because they do the work on themselves emotionally more than men do. The finding suggests that women’s greater engagement with emotions may build resilience from using resources. This is according to Fredrickson’s theory. However, gender-based interventions are needed to tackle coping strategies, including enhanced stress and anxiety among females (27).
The study contributes to understanding family dynamics and their link to mental health and happiness. The positive implications of democratic and protective family orientations are connected to Keyes’ focus on the social dimension of flourishing, whereby relationships and social environments are important (39). These findings highlight the importance of studying the relationship between family support and resource-oriented literacy and emotional health to design holistic intervention models.
The result gives rise to several recommendations to universities, policymakers, and mental health professionals to enhance students’ mental health literacy.
1. Designing deliberate mental health literacy programs: Universities must develop holistic MHL programs that maintain knowledge and promote using resources and practically getting help. These programs could include digital and in-person workshops on identifying and navigating campus mental health services. Role-playing exercises are simulations that help reduce stigma and encourage students to seek help. MHL sessions should be made compulsory during student orientation or as part of the general education curriculum to reach all students early (26).
2. Promoting gender-sensitive strategies: Tailored interventions are needed, given the gender differences in mental health literacy. The campaigns for male students must address the cultural norms and stigma that stop them from seeking help. It can include peer mentors or male role models to engage them. Programs must promote the ability to use mindfulness, coping skills, and other stress-reducing strategies (40).
3. Making academic course of education mental health: Mental health literacy should become part of the academic curriculum. Courses on MHL could be included in the core syllabus of fields like psychology, sociology, and health sciences. Students not majoring in health-related fields could take elective courses on well-being, which could help normalize mental health and happiness (24).
4. Improving access and visibility of resources. Low Resource-Oriented MHL scores show gaps in resource awareness—ways to beam up the profile.
a. Digital Platforms: Affordable and easy-to-use mobile apps or websites providing central access to campus mental health information. Campus campaigns will be held regularly to create awareness of the available counseling services and de-stigmatization.
b. Having resource guides in dorms, libraries, and student centers is a good idea since that is where most students go (22).
5. Incorporating family-centered interventions: It shows us that family-based programs are necessary. Families could engage through universities.
a. Workshops for Parents: Teaching democratic and supportive parenting styles. We hold sessions with families to communicate openly with students.
b. Family Counseling Programs: Support students struggling with family relationships (39).
6. Zoning in on subsets of at-risk behavior: Insights obtained from smokers and unhealthy lifestyles are a call for action. Campaigns targeting smokers can use their knowledge of healthcare to promote a wider array of services. Customized programs for sedentary or unhealthy eaters could also incorporate physical and mental health literacy (25).
7. Using technology for MHL interventions: Digital platforms have solutions that can grow with the need for MHL. Mobile applications and digital subscriptions could be afforded.
a. Self-Paced Learning: Mental health literacy and coping strategy modules.
b. Availability of Counseling and Peer Support in Real Time.
c. Anonymous assistance refers to online help students can access if they are unwilling to seek face-to-face assistance (41).
8. Creating institutional guidelines on mental health: Policymakers must incorporate mental health into institutional strategic planning. This entails financing for counseling centers, routine evaluations of campus requirements, and compulsory MHL training for all new students (20).
9. Evaluating program effectiveness: We should study all interventions to know their level of effectiveness. Strategies for developing the program reaches will be provided together with the revised logic model in Section 5.
Future studies should adopt longitudinal designs to investigate how mental health literacy (MHL) changes happiness. Such work will help to pinpoint causality and the longer-term impact of intervention. Researching these varied concepts in different cultures, institutions, and family situations would give more insight into their roles and impact on MHL and happiness. Similarly, the availability of resources matters too. Also, research into gender-specific interventions is important. One should look into reducing stigma for male populations. Moreover, one should also research stress and resilience-building interventions for women. Including self-efficacy, coping strategies, and emotional intelligence into the mental health literacy (MHL) frameworks would enhance understanding of how MHL can lead to positive outcomes. Researching the behavioral outcomes of MHL related to help-seeking and lifestyle modification could make awareness beneficial. Tech solutions like mobile applications and online counseling tools must also be evaluated to improve MHL and emotional well-being, especially among under-resourced people. In summary, future research can examine how academic performance may lead to the development of stress, which ultimately results in happiness. These directions provide roads for progressing with mental health literacy and happiness and related research, policy, and practice.
Limitations of this study include its reliance on self-reported data, which may introduce bias due to social desirability or inaccurate self-assessment. The sample was drawn from a single private university in Istanbul, limiting the generalizability of the findings to other institutions or cultural contexts. The study used a cross-sectional design, preventing causal inferences between mental health literacy and happiness. Additionally, the study focused on quantitative data and did not explore deeper psychological or contextual factors affecting these variables. Finally, potential confounding factors, such as personality traits and life experiences, were not considered, which may influence the observed relationships.
The research outcomes shed light on the relationship between mental health literacy (MHL) and the happiness of university students with reference to their demographic, health, lifestyle, and psychological characteristics. The results point to the importance of Resource Oriented MHL in improving emotional well-being, as happiness increases when we are aware of and have access to mental health resources. Weaker correlations between Knowledge-Oriented and Belief-oriented mental Health Literacy (MHL) and happiness show that knowledge and beliefs are insufficient without actions and support. Research has shown that there are differences in MHL between genders. For example, while women (on average) trump men in MHL studies, they report lower happiness than men. The health and lifestyle behaviors of a person’s family further dictate the outcome of mental health problems. The differences in MHL and happiness by subgroup call for equity interventions focusing on the sub-groups contexts like academic pressure and dormitory isolation. This research highlights the need for resource-oriented literacy in mental health, gender-specific approaches, and an enabling environment. By tackling these multifarious needs of students, universities, policymaking bodies, and mental healthcare officials can build resilience, alleviate distress, and promote flourishing among students. This understanding of MHL contributes to happiness and is a primary foundation for future research and applications.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Istanbul Gelisim University, Istanbul Turkey. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
NE: Conceptualization, Formal Analysis, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. AKM: Conceptualization, Formal Analysis, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. ŞK: Conceptualization, Data curation, Visualization, Writing – original draft, Writing – review & editing. AS: Investigation, Resources, Writing – original draft, Writing – review & editing. SÇT: Data curation, Investigation, Resources, Writing – original draft, Writing – review & editing. ŞÇ: Data curation, Investigation, Resources, Writing – original draft, Writing – review & editing. MR: Formal Analysis, Methodology, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Volstad C, Hughes J, Jakubec SL, Flessati S, Jackson L, Martin-Misener R. You have to be okay with okay”: Experiences of flourishing among university students transitioning directly from high school. Int J Qual Stud Health Well-Being. (2020) 15:1834259. doi: 10.1080/17482631.2020.1834259
2. Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens TE. College students: Mental health problems and treatment considerations. Acad Psychiatry. (2014) 39:503–11. doi: 10.1007/s40596-014-0205-9
3. Värnik P. Suicide in the world. Int J Environ Res Public Health. (2012) 9:760–71. doi: 10.3390/ijerph9030760
4. Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, et al. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J Abnormal Psychol. (2018) 127:623–38. doi: 10.1037/abn0000362
5. Sequeira C, Sampaio F, Pinho LG, Araújo O, Lluch-Canut T, Sousa L. Editorial: Mental health literacy: How to obtain and maintain positive mental health. Front Psychol. (2022) 13:1036983. doi: 10.3389/fpsyg.2022.1036983
6. Gaiha SM, Sunil GA, Kumar R, Menon S. Enhancing mental health literacy in India to reduce stigma: The fountainhead to improve help-seeking behaviour. J Public Ment Health. (2014) 13:146–58. doi: 10.1108/jpmh-06-2013-0043
7. Vaillant GE. Positive mental health: Is there a cross-cultural definition? World Psychiatry. (2012) 11:93–9. doi: 10.1016/j.wpsyc.2012.05.006
8. Akbari B. Investigation of relationship between “happiness and life quality” and “psychological health” in students of grade-2 in high school of Rasht City, Iran. Mediterr J Soc Sci. (2014) 5:3105. doi: 10.5901/mjss.2014.v5n20p3105
9. Naal H, Tavitian L, Yacoubian HA. Predictors of mental health literacy in a sample of university students in Lebanon. Int J Ment Health. (2020) 51:381–91. doi: 10.1080/00207411.2020.1838239
10. Furnham A, Hamid A. Mental health literacy in non-western countries: A review of the recent literature. Ment Health Rev J. (2014) 19:84–98. doi: 10.1108/mhrj-01-2013-0004
11. Howell AJ. Flourishing: Achievement-related correlates of students’ well-being. J Positive Psychol. (2009) 4:1–13. doi: 10.1080/17439760802043459
12. Keosybounheuang BS. Everyday happiness: A mental health lesson to help students focus on the positive during the pandemic. Strategies. (2021) 34:38–42. doi: 10.1080/08924562.2021.1920305
13. Carr A. Positive mental health: A research agenda. World Psychiatry. (2012) 11:100–1. doi: 10.1016/j.wpsyc.2012.05.016
14. Biggins Y. Purpose in adolescence: A review of the literature and an intervention plan (2018). Available online at: https://repository.upenn.edu/cgi/viewcontent.cgi?article=1152&context=mapp_capstone (Accessed September 15, 2024).
15. Bjørnsen HN, Eilertsen MB, Ringdal R, Espnes GA, Moksnes UK. Positive mental health literacy: Development and validation of a measure among Norwegian adolescents. BMC Public Health. (2017) 17:4733. doi: 10.1186/s12889-017-4733-6
16. Richardson R, Dale HE, Robertson L, Meader N, Wellby G, McMillan D, et al. Mental Health First Aid as a tool for improving mental health and well-being. Cochrane Library. (2023) 2023(8):CD013127. doi: 10.1002/14651858.cd013127.pub2
17. Shah AA, Beinecke RH. Global mental health needs, services, barriers, and challenges. Int J Ment Health. (2009) 38:14–29. doi: 10.2753/imh0020-7411380102
18. Gorczynski P, Sims-Schouten W, Hill DM, Wilson JC. Examining mental health literacy, help-seeking behaviours, and mental health outcomes in UK university students. J Ment Health Train Educ Pract. (2017) 12:111–22. doi: 10.1108/jmhtep-05-2016-0027
19. Wada M, Suto M, Lee M, Sanders D, Sun C, Le TN, et al. University students’ perspectives on mental illness stigma. Ment Health Prev. (2019) 14:200159. doi: 10.1016/j.mph.2019.200159
20. Wei Y, McGrath PJ, Hayden JA, Kutcher S. Mental health literacy measures evaluating knowledge, attitudes, and help-seeking: A scoping review. BMC Psychiatry. (2015) 15:15. doi: 10.1186/s12888-015-0681-9
21. Teich JL, Robinson G, Weist MD. What kinds of mental health services do public schools in the United States provide? Adv School Ment Health Promotion. (2008) 1:13–22. doi: 10.1080/1754730x.2008.9715741
22. Griffiths KM, Carron-Arthur B, Parsons A, Reid R. Effectiveness of programs for reducing the stigma associated with mental disorders: A meta-analysis of randomized controlled trials. World Psychiatry. (2014) 13:161–75. doi: 10.1002/wps.20129
23. Wrench A, Garrett R, King S. Managing health and well-being: Student experiences in transitioning to higher education. Asia-Pacific J Health Sport Phys Educ. (2014) 5:151–66. doi: 10.1080/18377122.2014.906059
24. Jiang Y, Lu C, Chen J, Miao Y, Li Y, Deng Q. Happiness in university students: Personal, familial, and social factors. Int J Environ Res Public Health. (2022) 19:4713. doi: 10.3390/ijerph19084713
25. Makki N, Mohanty MS. Mental health and happiness. Indian J Econ. (2019) 100:661–73. doi: 10.1177/0569434518822266
26. Reavley NJ, Jorm AF. Stigmatizing attitudes towards people with mental disorders: Findings from an Australian national survey of mental health literacy and stigma. Aust New Z J Psychiatry. (2011) 45:1086–93. doi: 10.3109/00048674.2011.621061
27. Gagnon MM, Gelinas BL, Friesen LN. Mental health literacy interventions: Promoting knowledge and treating stigma in young adults. J Ment Health. (2017) 26:388–96. doi: 10.1080/09638237.2017.1294747
28. Pratama RA, Tamara FH, Wahyuni H. Happiness: An approach to measure economics of well-being. Adv Econ Business Manage Res. (2020) 144:346–51. doi: 10.2991/aebmr.k.200520.056
29. Zhang Z, Chen W. A systematic review of the relationship between physical activity and happiness. J Happiness Stud. (2018) 20:1305–32. doi: 10.1007/s10902-018-9976-0
30. Dardas LA, Simmons LA. The stigma of mental illness in Arab families: A concept analysis. J Psychiatr Ment Health Nurs. (2015) 22:668–79. doi: 10.1111/jpm.12237
31. Chao H-J, Lien Y-J, Kao Y, Tasi I-C, Lin H-S, Lien Y-Y. Mental health literacy in healthcare students: An expansion of the Mental Health Literacy Scale. Int J Environ Res Public Health. (2020) 17:948. doi: 10.3390/ijerph17030948
32. Hills P, Argyle M. The Oxford Happiness Questionnaire: A compact scale for the measurement of psychological well-being. Pers Individ Dif. (2002) 33:1073–82. doi: 10.1016/S0191-8869(01)00213-6
33. Jung H, von Sternberg K, Davis K. The Mental Health Literacy Scale (MHLS): A new scale-based measure of mental health literacy. Psychiatr Serv. (2016) 67:523–8. doi: 10.1176/appi.ps.201500244
34. Doğan T, Çötok NA. Adaptation of the short form of the Oxford Happiness Questionnaire into Turkish: A validity and reliability study. Turkish J Psychiatry. (2011) 22:13–20.
35. Göktaş C, Bilici M, Göktaş Z. The adaptation of the Mental Health Literacy Scale into Turkish and its psychometric properties. Anatolian J Psychiatry. (2019) 20:256–65. doi: 10.5455/apd.45457
36. Keyes CLM. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consultn Clin Psychol. (2005) 73:539–48. doi: 10.1037/0022-006X.73.3.539
37. Fredrickson BL. The role of positive emotions in positive psychology: The broaden-and build theory of positive emotions. American Psychologist. (2001) 56(3):218–26. doi: 10.1037/0003-066X.56.3.218
38. Keyes CLM. Mental health in adolescence: Is America's youth flourishing? Am J Orthopsychiatry. (2006) 76(3):395–402. doi: 10.1037/0002-9432.76.3.395
39. Keyes CLM, Michalec B. Viewing mental health from the complete state paradigm. In: Keyes CLM, Michalec B, editors. Flourishing in life. Cambridge, United Kingdom: Cambridge University Press (2009). p. 125–134. doi: 10.1017/cbo9780511984945.010
40. Singh K, Junnarkar M. Correlates and predictors of positive mental health for school-going children. Pers Individ Dif. (2014) 76:82–7. doi: 10.1016/j.paid.2014.11.047
Keywords: mental health literacy, happiness, university students, social work interventions, well-being
Citation: Elkin N, Mohammed AK, Kılınçel Ş, Soydan AM, Tanrıver SÇ, Çelik Ş and Ranganathan M (2025) Mental health literacy and happiness among university students: a social work perspective to promoting well-being. Front. Psychiatry 16:1541316. doi: 10.3389/fpsyt.2025.1541316
Received: 07 December 2024; Accepted: 26 February 2025;
Published: 26 March 2025.
Edited by:
Thomas Probst, University of Salzburg, AustriaReviewed by:
Hasan Kütük, Istanbul Sabahattin Zaim University, TürkiyeCopyright © 2025 Elkin, Mohammed, Kılınçel, Soydan, Tanrıver, Çelik and Ranganathan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashifa Kariveliparambil Mohammed, YWthcml2ZWxpcGFyYW1iaWxAZ2VsaXNpbS5lZHUudHI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.