 Marisol Lila
Marisol Lila Cristina Expósito-Álvarez
Cristina Expósito-Álvarez Manuel Roldán-Pardo
Manuel Roldán-Pardo- Department of Social Psychology, Faculty of Psychology and Speech Therapy, University of Valencia, Valencia, Spain
Introduction: The incorporation of motivational strategies has shown promising results in increasing the effectiveness of intervention programs for intimate partner violence perpetrators, such as enhancing treatment adherence and decreasing risk of intimate partner violence recidivism. This could be particularly important for participants with alcohol and/or other drug use problems (ADUPs), who are at higher risk of recidivating and dropping out from the intervention. Consequently, there is a need to study whether motivational strategies are also effective for high-risk and highly resistant participants. The aim of this study was to determine whether the incorporation of motivational strategies led to improved outcomes in participants with ADUPs compared to those without.
Methods: Participants were intimate partner violence male perpetrators who received a standard intervention (n = 349) or a standard intervention adding an individualized motivational plan (n = 367). Data on official intimate partner violence recidivism, intervention dose, and dropout were collected after the end of the intervention. Comparisons were made between participants with and without ADUPs in each intervention condition.
Results: Results showed that in the full sample of participants, irrespective of their condition, those with ADUPs presented a higher recidivism (p = .007) and dropout rate (p = .003) and lower intervention dose than those without ADUPs (p = .005). When only considering participants in the standard intervention, results also showed that intimate partner violence perpetrators with ADUPs had a higher recidivism (p = .025) and dropout rate (p = .015) and lower intervention dose (p = .048) than those without. However, there were no significant differences between participants with and without ADUPs in the standard intervention adding an individualized motivational plan.
Discussion: When incorporating motivational strategies into the standard interventions for intimate partner violence perpetrators, disparities between participants with and without ADUPs were mitigated. Specifically, participants with ADUPs showed similar outcomes to those without ADUPs after receiving the standard intervention adding an individualized motivational plan. Our results suggest that motivational strategies may be effective in reducing intimate partner violence recidivism and improving treatment adherence in high-risk and highly resistant intimate partner violence perpetrators.
Introduction
Intimate partner violence (IPV) represents the most prevalent form of violence against women worldwide, with severe consequences for women’s health and wellbeing, and for the welfare of children and the broader societal structure (1). IPV has been recognized as a human rights and social problem of pandemic proportions (2, 3). Specifically, 27% of ever-partnered women aged 15-29 have suffered physical and/or sexual violence from their current or former male intimate partner at least once in their lifetime (2).
Given that IPV perpetrators often exhibit patterns of repeated abuse, either involving multiple victims or maintaining relationships with the same victim, it remains crucial to prevent IPV through direct intervention with perpetrators (4, 5). Intervention programs for IPV perpetrators have been developed in response to the recognition of IPV as a pervasive social issue, aiming to facilitate change in men and reduce IPV recidivism (6, 7). These programs represent a fundamental strategy within the criminal justice system to mitigate IPV among men convicted of such offenses, often providing an alternative to incarceration by court-mandating individuals to attend community-based intervention programs for IPV perpetrators (8, 9). As a result, there has been a growing interest in evaluating the effectiveness of perpetrator programs (10–12). However, significant challenges remain, with limited evidence supporting the effectiveness of these interventions, as highlighted in systematic reviews and meta-analyses (13–16).
The group-based structure of intervention programs for IPV perpetrators has often relied on a “one-size-fits-all” model, in which standardized interventions are applied uniformly without addressing the specific risk factors associated with IPV. In response, well-established approaches, such as the Risk-Needs-Responsivity (RNR) approach (17) and the Principles of Effective Interventions [(PEI) (18)], underscore the importance of conducting rigorous risk assessments and developing individualized strategies that address the unique risks and needs of each participant (15). These approaches offer a more sensitive and responsive intervention framework, aiming to improve outcomes by aligning program strategies with the participants’ specific needs (19, 20). Specifically, the RNR model, traditionally applied to criminogenic risk reduction, targets the “Big Eight” criminogenic risks domains, including history of antisocial behavior, antisocial personality and associates, family/marital relationship problems, substance abuse, employment, education and leisure problems (21). The core principles of the RNR framework can be articulated as follows: the ‘risk’ principle addresses who should be prioritized for treatment, the ‘need’ principle focuses on what specific factors should be targeted during intervention, and the ‘responsivity’ principle emphasizes how treatment should be delivered to maximize effectiveness (17). While the RNR framework is well-established, its application specifically to IPV remains more nascent. As such, it remains crucial to carefully tailor intervention programs for IPV perpetrators to the assessed needs and risk levels of participants (22). Research indicates that the RNR and PEI approaches show promise in reducing IPV recidivism more effectively than standardized models (15, 23–25).
Another critical challenge for perpetrator programs is effectively engaging high-risk IPV perpetrators who exhibit significant resistance to treatment (26–28). Notably, IPV perpetrators with alcohol and/or other drug use problems (ADUPs) constitute a high-risk, highly resistant group of IPV perpetrators (29, 30). This group not only demonstrates lower levels of treatment engagement but also tends to perpetrate more severe violence and has higher rates of dropout and recidivism than those without ADUPs (31). This is of particular concern given that approximately 50% of participants in perpetrator programs have ADUPs (32, 33). In addition, this group of participants present with complex, multi-level risk factors for IPV associated with ADUPs. At the individual level, participants with ADUPs often present lower anger management skills, diminished cognitive abilities, and increased psychological distress (34–36). Indeed, and consistent with the self-medication hypothesis (37), participants may use alcohol or other drugs to alleviate emotional pain (38, 39). In turn, ADUPs may exacerbate mental health issues through their impact on emotional and cognitive processes and on self-regulation (40). Moreover, at the social-relational level, participants with ADUPs are more likely to have experienced childhood trauma, complex relational trauma, and limited intimate support (34, 41–44). In addition, at the attitudinal level, participants with ADUPs frequently attribute responsibility for their violent behaviors to their substance use (45). Consequently, participants with ADUPs may exhibit greater individual, social-relational and attitudinal specific risk factors that warrant attention within intervention programs (30, 35). Improving outcomes for these participants, particularly by increasing their treatment engagement and reducing their elevated risk of IPV recidivism, could significantly enhance the overall effectiveness of perpetrator programs. Achieving this, however, requires rigorous evaluation of specific intervention strategies that show promise for this high-risk group of perpetrators (19, 23).
One of the key intervention strategies gaining attention is the incorporation of motivational-based approaches, which have been identified as a promising way to overcome intervention challenges and enhance the effectiveness of intervention programs for IPV perpetrators (46–48). For example, a recent systematic review by Wilson et al. (16) found inconclusive results regarding the overall effectiveness of IPV programs but highlighted the encouraging potential of integrating motivational strategies in newer programs. Originally developed in the field of addiction, motivational strategies have proven effective with highly resistant patients in addiction treatment (49). These strategies adopt a person-centered, collaborative approach designed to address ambivalence towards change (50). In addition, motivational strategies are grounded in four key principles: 1) expressing empathy and exploring the participant’s internal emotions, 2) evoking discrepancies between their values, goals, and current behaviors, 3) acknowledging and working with resistance rather than engaging in direct confrontation, and 4) enhancing the participant’s resources and strengths to bolster their confidence in their ability to change (51).
When incorporated into intervention programs for IPV perpetrators, motivational strategies involve specific humanistic techniques, including motivational interviewing (49), retention techniques (52, 53) and strength-based approaches such as the Good Lives Model (54), alongside the solution-focused brief therapy (55), goal setting (56–58), and the transtheoretical model of change (59). The transtheoretical model of change (59) outlines how individuals move through a series of stages when working toward intentional behavior change: precontemplation (resistance to change and avoidance of information), contemplation (ambivalence about change), preparation (taking concrete steps toward change), action (actively modifying behavior and implementing strategies for change), and maintenance (sustaining changes and preventing relapse). By aligning intervention strategies with the individual’s stage of change, these approaches may help promote greater treatment engagement and sustained progress throughout the intervention process (60).
Systematic reviews and meta-analysis assessing the effectiveness of motivational strategies demonstrate that integrating these approaches into perpetrator intervention programs can lead to improved treatment outcomes (14, 15). Indeed, a growing body of research suggests that incorporating motivational components enhances program effectiveness by fostering treatment engagement, strengthening participants’ motivation to change, and reducing dropout and recidivism rates (5, 61–65). For instance, recent meta-analyses have shown that participants receiving motivational strategies exhibited lower dropout rates than those attending standard perpetrators programs (48, 66).
Research suggests that the empathetic, non-confrontational nature of motivational strategies may facilitate that participants feel less resistant to the intervention, thus fostering treatment engagement (67). For instance, a study conducted by Crane and Eckhardt (61) showed that participants who received a brief motivational interviewing session prior to the intervention attended significantly more sessions than those in the control group. Furthermore, the Individualized Motivational Plan (IMP) developed by Lila et al. (68) has demonstrated greater effectiveness than standard interventions by increasing the intervention dose, facilitating progression in participants’ stages of change, and reducing physical IPV perpetration and risk of IPV recidivism among court-mandated male participants in perpetrator programs. Moreover, the use of individualized motivational strategies through the IMP could enable the intervention to be tailored to the specific needs of each participant (69).
Given that participants with ADUPs represent a high-risk and highly resistant group of perpetrators, this group of participants may particularly benefit from the IMP. This framework integrates both individual and group work within a humanistic, collaborative framework aimed at enhancing motivation to change and reducing resistance to intervention (67, 70, 71). However, while existing evidence suggests that the IMP can be effective for IPV perpetrators, further research is needed to assess the specific impact of these motivational strategies within this high-risk population (32, 72, 73). The aim of this study was to evaluate whether incorporating an IMP into a standard perpetrator program led to improved intervention outcomes, specifically, dropout rates, intervention dose, risk of IPV recidivism and official IPV recidivism, among IPV perpetrators with ADUPs. We hypothesized that the IMP would help reduce the disparities in these outcomes between IPV perpetrators with and without ADUPs.
Method
Participants
The sample consisted of 716 men who were court-mandated to participate in a community-based intervention program for IPV perpetrators at the University of Valencia [Contexto Program (68)]. Participants were part of 73 intervention groups conducted between November 2012 and October 2022. The sample included only those participants who met the following criteria: a) age 18 or older, b) convicted of IPV and court-referred to participate in an intervention program for IPV perpetrators, c) absence of serious mental health problems and/or disruptive behavior, and d) signed the informed consent form. Regarding the participants’ sociodemographic characteristics (see Table 1 for a more detailed description), the mean age was 39.5 (SD = 11.3). Approximately one-third of the participants (28.6%) had immigrant status. Specifically, 14.7% were from Latin America, 7.1% were from Europe (except Spain), 5.4% were from Africa, and 1.4% were from Asia. Regarding the educational level, 7.4% had no studies, 45.5% had completed elementary studies, 36.9% had obtained a high school diploma, and 10.2% had completed a college degree. Most of the participants were not partnered: 35.6% were single, 12.3% were separated, 26.5% were divorced, and 0.60% were widowed. The remaining (25%) were married or in a partnership. The unemployment rate among participants reached 40.6%, while the median annual family household income fell between €6000 and €12000.
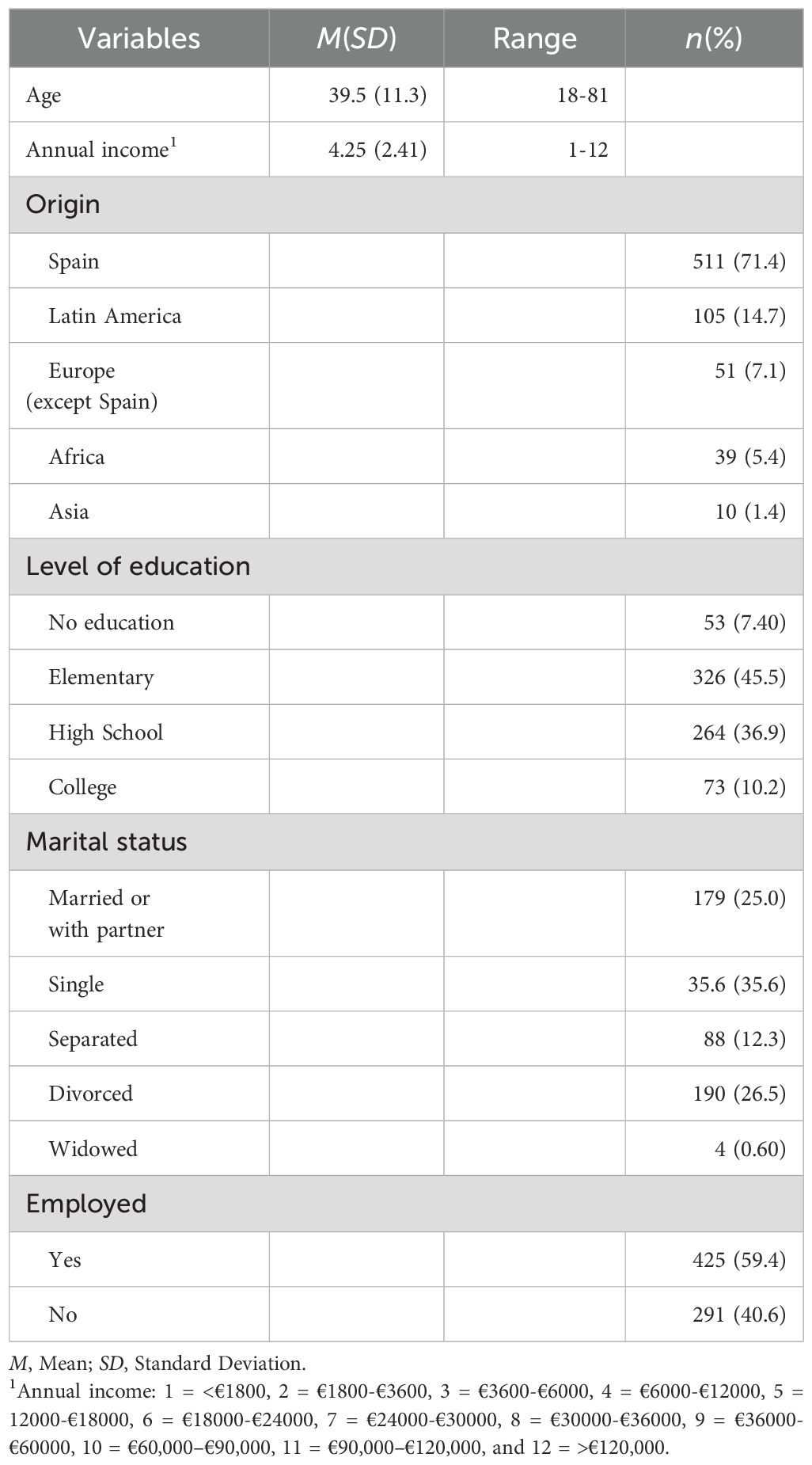
Table 1. Sample sociodemographic characteristics.
Instruments
Dropout. A value of 0 was assigned to participants who completed the intervention program, while a value of 1 was assigned to those who ceased attendance.
Intervention dose. The ratio of the number of sessions attended by the participant to the total number of sessions in the intervention group.
Official IPV recidivism. Data on recidivism rates were obtained from VioGén (74), the monitoring system of the Ministry of Home Affairs. The system provides data on any new incident of IPV, formal complaint, or breach of the conditions prescribed by the judge (e.g., restraining order). The data is derived from all the institutions engaged in the provision of victim protection services. Data were collected in May 2024. Any new incident occurring within 12 months of the conclusion of the intervention was deemed to be recidivism.
Risk of recidivism evaluated by the facilitators. The Spousal Assault Risk Assessment Guide [SARA (75); Spanish version by Andrés-Pueyo et al. (76)] was employed to evaluate the risk of recidivism. The SARA is completed by the facilitators and comprises a 20-item checklist protocol on a 3-point Likert-type scale (0 = absent, 1 = possibly present, and 2 = present). SARA also comprises two independent items designed to assess the risk of recidivism towards a partner and others. These items are presented on a 3-point Likert-type scale (0 = low risk, 1 = moderate risk, and 2 = high risk). In the present study, only these two items were utilized. The SARA has been shown to have predictive validity (77), and the Spanish version has been employed in research with samples of IPV perpetrators (68, 78).
Alcohol use. The Alcohol Use Disorders Identification Test [AUDIT (79); Spanish version by Contel-Guillamón et al. (80)] was used to screen the level and frequency of current and past 12-month alcohol use. The instrument comprises 10 Likert-type items, which are scored on a 3-point or 5-point scale (for example, 0 = never, 1 = less than once in a month, 2 = once a month, 3 = once a week, and 4 = daily or almost daily). A score of 8 or above was indicative of hazardous alcohol use. The AUDIT has been shown to have construct and discriminant validity and sensitivity (81), and the Spanish version has been employed in studies of IPV male perpetrators (78, 82). In the present study, Cronbach’s alpha reliability coefficient was .78.
Clinical syndromes of alcohol and substance dependence. The alcohol dependence and substance dependence scales of the Millon Clinical Multiaxial Inventory-III [MCMI-III (83); Spanish version by Cardenal and Sánchez (84)] were used to screen participants for alcohol and/or other drug dependence. The self-reported inventory consists of 175 true-false items, and only the two aforementioned scales were used. A score of 75 or above was indicative of a potential issue or proclivity towards a clinical dependence syndrome. The Spanish version of the scale has been utilized in studies involving male perpetrators of IPV (28, 57). The Cronbach’s alpha reliability coefficients for alcohol dependence and substance dependence were .71 and .80, respectively (84).
Procedure
Men convicted of IPV who consented to participate in the present study signed a written consent form during the assessment phase. It was explicitly conveyed to participants that neither their decision to participate nor their refusal to do so would have any bearing on their legal standing. Participants were assigned to a treatment condition based on the availability and training of the facilitators. While all facilitators were trained to deliver the standard intervention (SI) condition, a specific group of facilitators were also trained to deliver the standard intervention with the Individualized Motivational Plan (SI-IMP) condition. The SI condition comprised 70 hours of intervention (35 weekly two-hour group sessions) based on cognitive-behavioral techniques addressing topics such as sexism, gender equality, and IPV. The six-module program sought to cultivate group trust, address IPV responsibility, enhance communication, empathy, and emotion management, challenge traditional gender roles, and prevent relapses. The SI-IMP condition comprised the standard intervention in conjunction with the IMP. The IMP employed a package of motivational strategies aimed at enhancing treatment compliance and motivation to change. Based on approaches such as motivational interviewing and the Good Lives Model, it included five individual sessions, three group sessions for goal sharing, ongoing facilitator reinforcement, and retention techniques throughout the intervention. For a more detailed description of each of the treatment conditions, refer to Lila et al. (68). In total, 349 participants received the SI, and 367 received the SI-IMP.
Data on sociodemographic characteristics, alcohol use, and clinical syndromes of alcohol and substance dependence were collected as a part of the initial assessment for participants. This data was gathered through a self-report assessment instrument administered by the program staff over two sessions, each spanning two hours. After the end of the assessment phase, facilitators reported data on the risk of IPV recidivism. Individuals who scored above the established cut-off point on the AUDIT [≥ 8 (79)] or the alcohol or substance dependence scale of the MCMI-III [≥ 75 (83)] at the time of intake were classified as ADUPs. This procedure has been utilized previously in IPV male perpetrators studies (34, 78). Profile validity of the MCMI-III was evaluated using its validity scale. When invalid profiles were detected, the assessment was readministered to ensure accurate and reliable results. Finally, data on dropout, official recidivism, and intervention dose were collected subsequent to the conclusion of the intervention period. Dropout and intervention dose data were reported by the facilitators, while the research staff were responsible for collecting the data on official recidivism. The data presented in this study were collected in accordance with the approved procedures established by the Ethics Committee of the University of Valencia (H1537520365110).
Data analysis
First, the baseline characteristics of the participants in each treatment condition (SI vs. SI-IMP) were examined. Sociodemographic characteristics and risk of IPV recidivism were included. Chi-square and t tests were used to compare categorical and continuous variables, respectively, across treatment conditions. Continuous variables with non-normal distributions were analyzed using the Mann-Whitney U test.
Second, different analyses were conducted to analyze the differences between participants with and without ADUPs. Chi-square and Mann-Whitney U tests were conducted for categorical (i.e., dropout and official IPV recidivism) and continuous (i.e., intervention dose) variables, respectively. The effect size for categorical and continuous variables was calculated using Cramér’s V and eta-squared statistics, respectively. These analyses were performed for the full sample and each of the treatment conditions. All analyses were conducted using the IBM SPSS statistical software, version 28.0.1.1.
Results
Baseline characteristics
Table 2 provides a comparison of the baseline characteristics and risk of IPV assessed by facilitators of the participants who were allocated to each treatment condition. Seven variables were compared between groups, and none of the comparisons reached statistical significance (p >.05). Therefore, the groups were found to be statistically equivalent in terms of their baseline characteristics and risk of IPV.
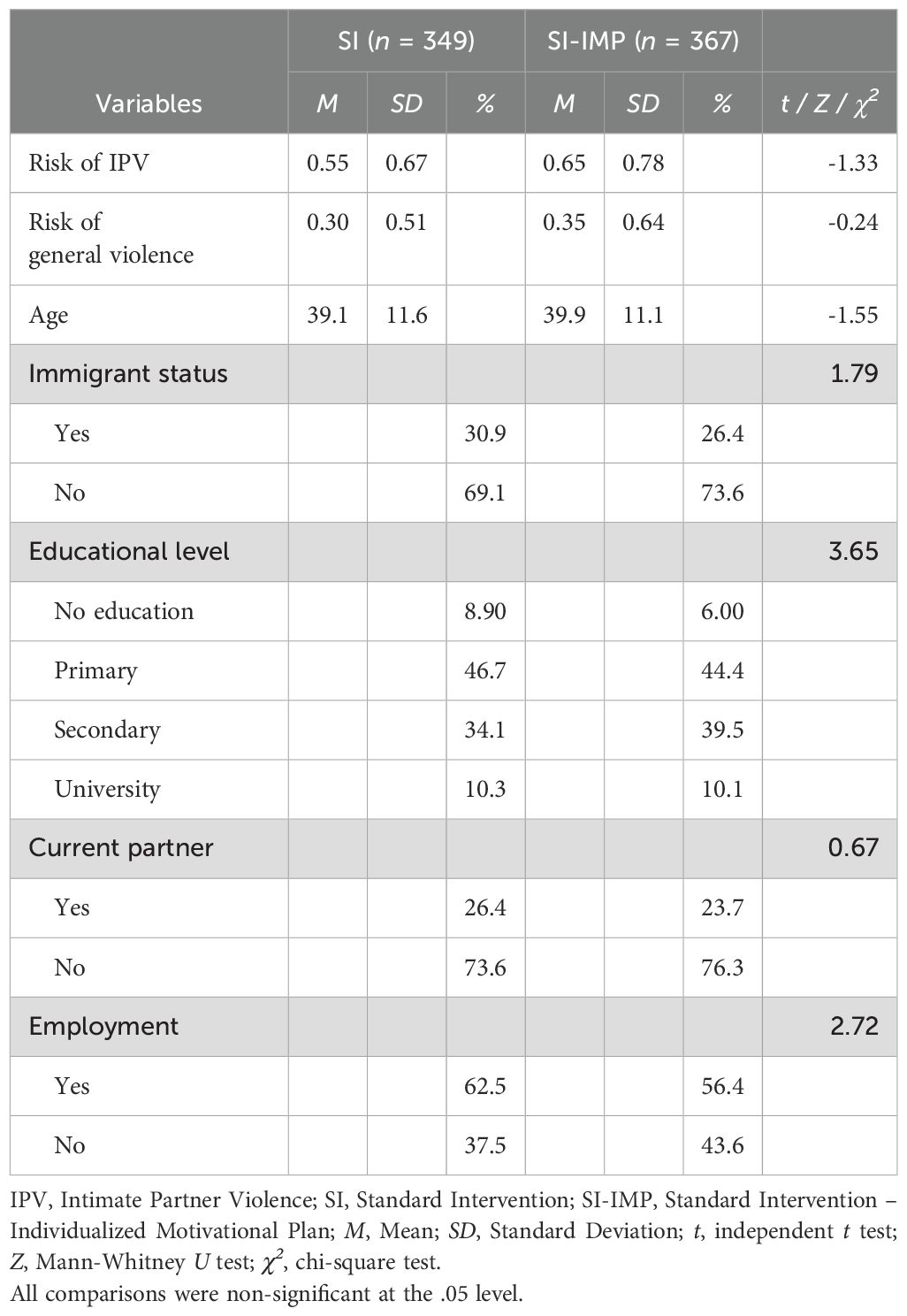
Table 2. Comparison of baseline characteristics and risk of IPV.
Final outcomes
Table 3 presents the descriptive statistics of the final outcomes for the full sample and for each treatment condition. In consideration of the full sample, participants with ADUPs exhibited elevated rates of dropout (χ2 = 8.58; p = .003; V = .11) and IPV recidivism (χ2 = 7.18; p = .007; V = .10), as well as a diminished intervention dose (Z = -2.78; p = .005; d = .38), in comparison to the participants without ADUPs. When only the participants assigned to the SI condition were considered, it was observed that those with ADUPs also demonstrated elevated rates of dropout (χ2 = 5.87; p = .015; V = .13) and recidivism (χ2 = 4.99; p = .025; V = .12), as well as a diminished intervention dose (Z = -1.97; p = .048; d = .47), in comparison to those without ADUPs. However, when considering only participants assigned to the SI-IMP condition, no statistically significant differences were observed in dropout, IPV recidivism, and intervention dose (p >.05).
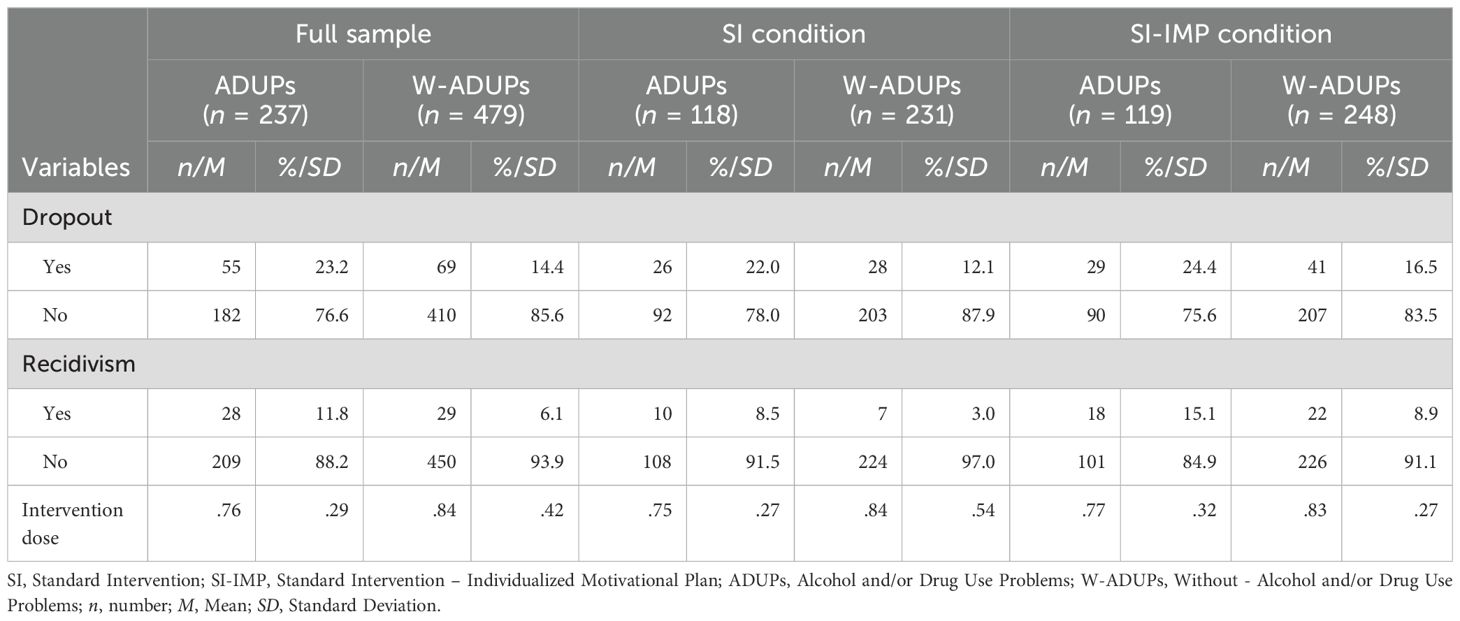
Table 3. Descriptive statistics on final outcomes in the full sample and each treatment condition.
Discussion
This study aimed to evaluate whether the incorporation of a motivational tool, the IMP, helped reduce risk factors between IPV perpetrators with ADUPs and those without, in a large sample of men court-mandated to attend an intervention program for IPV perpetrators. Our results indicated that, both in the full sample and specifically within the standard condition (SI), participants with ADUPs showed higher dropout rates, increased official IPV recidivism, and received a lower intervention dose (i.e., lower treatment attendance) compared to participants without ADUPs. This is consistent with previous literature showing that presenting ADUPs among IPV perpetrators was predictive of higher dropout and lower treatment adherence (29, 85–87). In this vein, a study conducted by Expósito-Álvarez et al. (57) revealed that perpetrator programs’ participants with ADUPs had 123% higher odds of dropping out than those without such problems. This result is of significant concern given the well-known association between dropout and a higher likelihood of IPV recidivism (27, 29, 88). Moreover, and consistent with our results, IPV perpetrators with ADUPs have been consistently found to display higher IPV recidivism rates compared to those without ADUPs (31, 89). Nonetheless, it is important to note that while ADUPs may contribute to and exacerbate violence among IPV perpetrators, IPV is a complex phenomenon influenced by a range of multifaceted risk factors (90). These factors, which may interact with ADUPs, include emotional dysregulation, trauma, gendered power dynamics, and diminished executive functions, among others, all of which increase the likelihood of IPV (35, 41, 45, 91). Therefore, our findings, in alignment with existing literature, indicate that IPV perpetrators with ADUPs are a high-risk group of participants who may present specific risks that need to be targeted in perpetrator programs (92).
Importantly, our results also showed that when incorporating the IMP into the standard intervention (SI-IMP), participants with and without ADUPs did not differ in terms of intervention dose, dropout and official recidivism rates. This suggests that the disparities commonly observed between IPV perpetrators with and without ADUPs were mitigated when the IMP was integrated into the standard perpetrator program. The observed reduction in risk factors often associated with ADUPs may be attributed to the motivational strategies of the IMP, which are well-documented for their ability to enhance treatment engagement and improve retention in interventions (60, 63–65). Moreover, participants with ADUPs, who have been shown to exhibit higher levels of anger and impulsivity (34, 36, 93), may have particularly benefited from the motivational components of goal setting and strategies to help them identify personal reasons for change, thereby promoting more effective engagement in the intervention process and reducing the likelihood of IPV recidivism (56, 57, 94–96). Therefore, our findings underscore the encouraging potential of incorporating motivational strategies in perpetrator programs, particularly for high-risk participants such as those with ADUPs. Prior randomized controlled trials (RCTs) have also shown that implementing brief motivational interviewing sessions at intake may show promising results for IPV perpetrators with ADUPs compared to standard interventions (70, 71, 73).
In alignment with emerging frameworks, such as the RNR model (17) and the PEI approach (25), there is an urgent need for interventions that address the specific risks and needs of IPV perpetrators to effectively mitigate key risk factors, including ADUPs (18, 23). However, IPV perpetrators with co-occurring ADUPs have traditionally been referred to separate programs for IPV intervention and addiction treatment, often located in different facilities and administered by distinct services, which is both time- and cost-consuming (92, 97, 98). This lack of integrated approaches contributes to negative outcomes, including the high dropout rates and low treatment engagement often found in these participants (27, 29, 99). Integrated approaches that concurrently address IPV and ADUPs while incorporating motivational strategies, may offer a more effective approach to improve treatment outcomes among IPV perpetrators with ADUPs. In this vein, a recently published RCT has shown that incorporating an IMP tailored to addressing ADUPs was more effective than a standard IMP in reducing alcohol use, increasing active participation, and promoting more advanced stages of change among IPV perpetrators (78). These findings suggest that integrated, motivation-based interventions hold significant promise for addressing the needs of IPV perpetrators with co-occurring ADUPs (71–73). However, as Eckhardt et al. (97) recently emphasized: “effective interventions that break this robust and complicated association are under development but are limited in number and availability” (p. 2412). Thus, more intervention and research efforts are needed to implement motivational-based and integrated approaches in perpetrator programs.
Our findings have important treatment implications, since they revealed that IPV perpetrators with ADUPs exhibit a higher risk of official IPV recidivism, dropout, and lower treatment adherence, thus showing that this high-risk group of perpetrators require tailored interventions within group-based intervention programs (30, 31). In addition, integrating motivational strategies appears particularly beneficial in reducing their risk factors for IPV (71, 78). The person-centered, non-confrontational approach of motivational strategies may help these individuals resolve ambivalence toward change, given the potential discrepancy between their behavior (e.g., consequences of substance use, conflictive and violent behavior) and their core values (52, 54). In fact, previous studies indicate that IPV perpetrators with ADUPs demonstrate greater motivation and are often at a more advanced stage of change than those without ADUPs (34, 100). Thus, enhancing treatment engagement and promoting their internal motivation to change could foster positive change in their intimate relationship dynamics, ultimately decreasing their elevated risk of IPV recidivism (45, 47).
This study has certain limitations. Bivariate comparisons may not fully capture the complex relationships between variables and may overlook confounding factors that could impact outcomes across intervention conditions (101). Future studies should consider using RCTs to directly compare the effectiveness of these interventions in reducing risks associated with ADUPs in IPV perpetrators (68, 70, 78). Additionally, equivalence testing should be considered as a rigorous method to evaluate whether treatment outcomes are truly equivalent across groups (102). Future studies could also include a wider range of variables that reflect other risk factors for IPV associated with ADUPs, such as attitudinal and social-relational variables, beyond recidivism and treatment engagement (68, 78). Further research is also needed to assess the specific types of substances used by IPV perpetrators and their levels of use (e.g., hazardous drinking, alcohol dependence) to inform the design of more tailored intervention strategies for IPV perpetrators with ADUPs (103). Another limitation is that this study used a specific sample of men court-mandated to attend an intervention program for IPV perpetrators following a conviction for a gender-based violence offense, thus limiting the generalizability of these results to other populations. Additional research should focus on understudied problems such as IPV among men who have sex with men (5). This study also exhibited several strengths. Notably, it utilized a large sample size (n = 716), which is particularly significant given the challenges associated with recruiting participants from this population. In addition, while research on motivational approaches within perpetrator programs often focuses on the incorporation of motivational interviewing solely at intake, thereby limiting its sustained use across the intervention, this study evaluated the implementation of the IMP, which was integrated throughout the intervention. Specifically, the IMP used both individualized strategies and group-based methods for sharing goals and progress, potentially enhancing treatment engagement (65, 103).
In conclusion, IPV perpetrators with ADUPs represent a high-risk and highly resistant group of IPV perpetrators who require tailored intervention approaches. Integrating motivational strategies, such as the IMP, could enhance treatment outcomes by improving engagement and reducing IPV recidivism. Such improvements have the potential to increase the effectiveness of perpetrator programs, thereby contributing to greater safety for victims.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité Ético de Investigación en Humanos de la Comisión de Ética en Investigación Experimental, University of Valencia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ML: Conceptualization, Project administration, Supervision, Writing – review & editing. CE: Investigation, Writing – original draft, Writing – review & editing. MR: Formal analysis, Investigation, Methodology, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by Generalitat Valenciana, grant number CIPROM/2021/46, PROMETEO 2022: Projects for Research Excellence Groups and by “Profesionales en la intervención con hombres que ejercen violencia de género: un análisis comparado de necesidades y desafíos (PROF-VG)” -Programa Prismas y Problemas of the BBVA Foundation 2023. Manuel Roldán-Pardo was supported by Generalitat Valenciana, grant number ACIF/2021/362, ACIF Program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet. (2022) 399:803–13. doi: 10.1016/S0140-6736(21)02664-7
2. World Health Organization. Violence against women prevalence estimates 2018: Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. 1st ed. Geneva, Switzerland: World Health Organization (2021). 112 p.
3. Devries KM, Mak JYT, García-Moreno C, Petzold M, Child JC, Falder G, et al. The global prevalence of intimate partner violence against women. Science. (2013) 340:1527–8. doi: 10.1126/science.1240937
4. Lila M, Oliver A, Lorenzo M-V, Catalá A. Valoración del riesgo de reincidencia en violencia contra la mujer en las relaciones de pareja: Importancia del apoyo social. Rev Psicol Soc. (2013) 28:225–36. doi: 10.1174/021347413806196681
5. Eckhardt CI, Murphy CM, Whitaker DJ, Sprunger J, Dykstra R, Woodard K. The effectiveness of intervention programs for perpetrators and victims of intimate partner violence. Partn Abuse. (2013) 4:196–231. doi: 10.1891/1946-6560.4.2.196
6. Lila M, Gilchrist G. Treatment resistant perpetrators of intimate partner violence: Research advances. Psychosoc Interv. (2023) 32:55–8. doi: 10.5093/pi2023a10
7. Rivas C, Ramsay J, Sadowski L, Davidson LL, Dunnes D, Eldridge S, et al. Advocacy interventions to reduce or eliminate violence and promote the physical and psychosocial well-being of women who experience intimate partner abuse: A systematic review. Campbell Syst Rev. (2016) 12:1–202. doi: 10.4073/csr.2016.2
8. Cunha O, Caridade S. Batterer intervention program (BIP). In: Shackelford TK, editor. Encyclopedia of Domestic Violence. Springer International Publishing, Cham, Switzerland (2023). p. 1–11. doi: 10.1007/978-3-030-85493-5_88-1
9. Babcock JC, Armenti N, Cannon C, Lauve-Moon K, Buttell F, Ferreira R, et al. Domestic violence perpetrator programs: A proposal for evidence-based standards in the United States. Partn Abuse. (2016) 7:355–460. doi: 10.1891/1946-6560.7.4.355
10. Cheng S-Y, Davis M, Jonson-Reid M, Yaeger L. Compared to what? A Meta-analysis of batterer intervention studies using nontreated controls or comparisons. Trauma Violence Abus. (2021) 22:496–511. doi: 10.1177/1524838019865927
11. Nesset MB, Lara-Cabrera ML, Dalsbø TK, Pedersen SA, Bjørngaard JH, Palmstierna T. Cognitive behavioural group therapy for male perpetrators of intimate partner violence: a systematic review. BMC Psychiatry. (2019) 19:1–13. doi: 10.1186/s12888-019-2010-1
12. Babcock JC, Green CE, Robie C. Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clin Psychol Rev. (2004) 23:1023–53. doi: 10.1016/j.cpr.2002.07.001
13. Arce R, Arias E, Novo M, Fariña F. Are interventions with batterers effective? A meta-analytical review. Psychosoc Interv. (2020) 29:153–64. doi: 10.5093/pi2020a11
14. Karakurt G, Koç E, Çetinsaya EE, Ayluçtarhan Z, Bolen S. Meta-analysis and systematic review for the treatment of perpetrators of intimate partner violence. Neurosci Biobehav Rev. (2019) 105:220–30. doi: 10.1016/j.neubiorev.2019.08.006
15. Travers Á, McDonagh T, Cunningham T, Armour C, Hansen M. The effectiveness of interventions to prevent recidivism in perpetrators of intimate partner violence: A systematic review and meta-analysis. Clin Psychol Rev. (2021) 84:101974. doi: 10.1016/j.cpr.2021.101974
16. Wilson DB, Feder L, Olaghere A. Court-mandated interventions for individuals convicted of domestic violence: An updated Campbell systematic review. Campbell Syst Rev. (2021) 17:e1151. doi: 10.1002/cl2.1151
17. Andrews DA, Bonta J. Rehabilitating criminal justice policy and practice. Psychol Public Policy Law. (2010) 16:39–55. doi: 10.1037/a0018362
18. Richards TN, Gover AR, Branscum C, Nystrom A, Claxton T. Assessing states’ intimate partner violence offender treatment standards using a principles of effective intervention framework. J Interpers Violence. (2022) 37:NP20288–NP20310. doi: 10.1177/08862605211050091
19. Massa AA, Maloney MA, Eckhardt CI. Interventions for perpetrators of intimate partner violence: An I 3 model perspective. Partn Abuse. (2020) 11:437–46. doi: 10.1891/PA-2020-0031
20. Finkel EJ. Impelling and inhibiting forces in the perpetration of intimate partner violence. Rev Gen Psychol. (2007) 11:193–207. doi: 10.1037/1089-2680.11.2.193
21. Bonta J, Andrews DA. The psychology of criminal conduct. 6th ed. New York: Routledge (2016). doi: 10.4324/9781315677187
22. Marlowe DB. The most carefully studied, yet least understood, terms in the criminal justice lexicon: Risk, need, and responsivity. Policy Res Assoc. (2018). https://www.prainc.com/risk-need-responsitivity/ (Accessed January 8, 2025).
23. Butters RP, Droubay BA, Seawright JL, Tollefson DR, Lundahl B, Whitaker L. Intimate partner violence perpetrator treatment: Tailoring interventions to individual needs. Clin Soc Work J. (2021) 49:391–404. doi: 10.1007/s10615-020-00763-y
24. Turner W, Morgan K, Hester M, Feder G, Cramer H. Methodological challenges in group-based randomised controlled trials for intimate partner violence perpetrators: A meta-summary. Psychosoc Interv. (2023) 32:123–36. doi: 10.5093/pi2023a9
25. Radatz DL, Wright EM. Integrating the principles of effective intervention into batterer intervention programming: The case for moving toward more evidence-based programming. Trauma Violence Abus. (2016) 17:72–87. doi: 10.1177/1524838014566695
26. Tutty LM, Babins-Wagner R, Rothery MA. The responsible choices for men IPV offender program: Outcomes and a comparison of court-mandated to non-court-mandated men. J Aggress Maltreatment Trauma. (2020) 29:292–313. doi: 10.1080/10926771.2019.1578316
27. Olver ME, Stockdale KC, Wormith JS. A meta-analysis of predictors of offender treatment attrition and its relationship to recidivism. J Consult Clin Psychol. (2011) 79:6–21. doi: 10.1037/a0022200
28. Carbajosa P, Catalá-Miñana A, Lila M, Gracia E, Boira S. Responsive versus treatment-resistant perpetrators in batterer intervention programs: Personal characteristics and stages of change. Psychiatry Psychol Law. (2017) 24:936–50. doi: 10.1080/13218719.2017.1347933
29. Jewell LM, Wormith JS. Variables associated with attrition from domestic violence treatment programs targeting male batterers: A meta-analysis. Crim Justice Behav. (2010) 37:1086–113. doi: 10.1177/0093854810376815
30. Leonard KE, Quigley BM. Thirty years of research show alcohol to be a cause of intimate partner violence: Future research needs to identify who to treat and how to treat them. Drug Alcohol Rev. (2017) 36:7–9. doi: 10.1111/dar.12434
31. Cafferky BM, Mendez M, Anderson JR, Stith SM. Substance use and intimate partner violence: A meta-analytic review. Psychol Violence. (2018) 8:110–31. doi: 10.1037/vio0000074
32. Crane CA, Eckhardt CI, Schlauch RC. Motivational enhancement mitigates the effects of problematic alcohol use on treatment compliance among partner violent offenders: Results of a randomized clinical trial. J Consult Clin Psychol. (2015) 83:689–95. doi: 10.1037/a0039345
33. Kraanen FL, Scholing A, Emmelkamp PMG. Substance use disorders in perpetrators of intimate partner violence in a forensic setting. Int J Offender Ther Comp Criminol. (2010) 54:430–40. doi: 10.1177/0306624X08330189
34. Expósito-Álvarez C, Lila M, Gracia E, Martín-Fernández M. Risk factors and treatment needs of batterer intervention program participants with substance abuse problems. Eur J Psychol Appl Leg Context. (2021) 13:87–97. doi: 10.5093/ejpalc2021a9
35. Expósito-Álvarez C, Santirso FA, Gilchrist G, Gracia E. Lila M. Participants in court-mandated intervention programs for intimate partner violence perpetrators with substance use problems: A systematic review of specific risk factors. Psychosoc Interv. (2023) 32:89–108. doi: 10.5093/pi2023a7
36. Oberleitner LMS, Mandel DL, Easton CJ. Treatment of co-occurring alcohol dependence and perpetration of intimate partner violence: The role of anger expression. J Subst Abuse Treat. (2013) 45:313–8. doi: 10.1016/j.jsat.2013.03.001
37. Khantzian EJ. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv Rev Psychiatry. (1997) 4:231–44. doi: 10.3109/10673229709030550
38. Hawn SE, Cusack SE, Amstadter AB. A systematic review of the self-medication hypothesis in the context of posttraumatic stress disorder and comorbid problematic alcohol use. J Trauma Stress. (2020) 33:699–708. doi: 10.1002/jts.22521
39. Lawrence TI, Mcfield AA, Byrne MM, S.Tarver S, Stewart TK. Depression and substance use as consequences of exposure to family violence: A moderation mediation and self-medication hypothesis study. J Child Adolesc Trauma. (2023) 16:69–79. doi: 10.1007/s40653-022-00464-3
40. Steele CM, Josephs RA. Alcohol myopia: Its prized and dangerous effects. Am Psychol. (1990) 45:921–33. doi: 10.1037/0003-066X.45.8.921
41. Thomas MD, Bennett LW, Stoops C. The treatment needs of substance abusing batterers: A comparison of men who batter their female partners. J Fam Violence. (2013) 28:121–9. doi: 10.1007/s10896-012-9479-4
42. Siria S, Fernández-Montalvo J, Echauri JA, Arteaga A, Azkárate JM, Martínez M. Differential MCMI-III psychopathological profiles between intimate partner violence perpetrators with and without childhood family violence. Clin Psychol Psychother. (2021) 28:1020–9. doi: 10.1002/cpp.2557
43. Semiatin JN, Torres S, LaMotte AD, Portnoy GA, Murphy CM. Trauma exposure, PTSD symptoms, and presenting clinical problems among male perpetrators of intimate partner violence. Psychol Violence. (2017) 7:91–100. doi: 10.1037/vio0000041
44. Kwong MJ, Bartholomew K, Henderson AJZ, Trinke SJ. The intergenerational transmission of relationship violence. J Fam Psychol. (2003) 17:288–301. doi: 10.1037/0893-3200.17.3.288
45. Gilchrist G, Dennis F, Radcliffe P, Henderson J, Howard LM, Gadd D. The interplay between substance use and intimate partner violence perpetration: A meta-ethnography. Int J Drug Policy. (2019) 65:8–23. doi: 10.1016/j.drugpo.2018.12.009
46. Pinto E Silva T, Cunha O, Caridade S. Motivational interview techniques and the effectiveness of intervention programs with perpetrators of intimate partner violence: A systematic review. Trauma Violence Abus. (2023) 24:2691–710. doi: 10.1177/15248380221111472
47. Soleymani S, Britt E, Wallace-Bell M. Motivational interviewing for enhancing engagement in Intimate Partner Violence (IPV) treatment: A review of the literature. Aggress Violent Behav. (2018) 40:119–27. doi: 10.1016/j.avb.2018.05.005
48. Santirso FA, Gilchrist G, Lila M, Gracia E. Motivational strategies in interventions for intimate partner violence offenders: A systematic review and meta-analysis of randomized controlled trials. Psychosoc Interv. (2020) 29:175–90. doi: 10.5093/pi2020a13
49. Miller WR, Rollnick S. Motivational interviewing: Helping people change. 3rd ed. New York: Guilford Press (2012). 482 p.
50. Lundahl BW, Kunz C, Brownell C, Tollefson D, Burke BL. A meta-analysis of motivational interviewing: Twenty-five years of empirical studies. Res Soc Work Pract. (2010) 20:137–60. doi: 10.1177/1049731509347850
51. Moyers TB, Rollnick S. A motivational interviewing perspective on resistance in psychotherapy. J Clin Psychol. (2002) 58:185–93. doi: 10.1002/jclp.1142
52. DiClemente CC, Corno CM, Graydon MM, Wiprovnick AE, Knoblach DJ. Motivational interviewing, enhancement, and brief interventions over the last decade: A review of reviews of efficacy and effectiveness. Psychol Addict Behav. (2017) 31:862–87. doi: 10.1037/adb0000318
53. Taft CT, Murphy CM, King DW, Musser PH, DeDeyn JM. Process and treatment adherence factors in group cognitive-behavioral therapy for partner violent men. J Consult Clin Psychol. (2003) 71:812–20. doi: 10.1037/0022-006X.71.4.812
54. Langlands RL, Ward T, Gilchrist E. Applying the good lives model to male perpetrators of domestic violence. Behav Change. (2009) 26:113–29. doi: 10.1375/bech.26.2.113
55. Lee MY, Uken A, Sebold J. Accountability for change: Solution-focused treatment with domestic violence offenders. Fam Soc J Contemp Soc Serv. (2004) 85:463–76. doi: 10.1606/1044-3894.1832
56. Bolton KW, Lehmann P, Jordan C, Frank L, Moore B. Self-determined goals in a solution-focused batterer intervention program: Application for building client strengths and solutions. J Hum Behav Soc Environ. (2016) 26:541–8. doi: 10.1080/10911359.2016.1172996
57. Expósito-Álvarez C, Gilchrist G, Gracia E, Lila M. Evaluating the role of goal setting in reducing dropout for men with and without substance use problems attending a court-mandated intimate partner violence perpetrator program. Vict Offenders. (2024) 19:1175–207. doi: 10.1080/15564886.2024.2322960
58. Expósito-Álvarez C, Roldán-Pardo M, Lila M. Análisis de las estrategias motivacionales en los programas de intervención para agresores de pareja: El impacto de las metas de cambio. Rev Iberoam Justicia Ter. (2024) (8):1–13.
59. Prochaska JO, DiClemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychother Theory Res Pract. (1982) 19:276–88. doi: 10.1037/h0088437
60. Kistenmacher BR, Weiss RL. Motivational interviewing as a mechanism for change in men who batter: A randomized controlled trial. Violence Vict. (2008) 23:558–70. doi: 10.1891/0886-6708.23.5.558
61. Crane CA, Eckhardt CI. Evaluation of a single-session brief motivational enhancement intervention for partner abusive men. J Couns Psychol. (2013) 60:180–7. doi: 10.1037/a0032178
62. Santirso FA, Lila M, Gracia E. Motivational strategies, working alliance, and protherapeutic behaviors in batterer intervention programs: A randomized controlled trial. Eur J Psychol Appl Leg Context. (2020) 12:77–84. doi: 10.5093/ejpalc2020a7
63. Alexander PC, Morris E, Tracy A, Frye A. Stages of change and the group treatment of batterers: A randomized clinical trial. Violence Vict. (2010) 25:571–87. doi: 10.1891/0886-6708.25.5.571
64. Musser PH, Semiatin JN, Taft CT, Murphy CM. Motivational interviewing as a pregroup intervention for partner-violent men. Violence Vict. (2008) 23:539–57. doi: 10.1891/0886-6708.23.5.539
65. Scott K, King C, McGinn H, Hosseini N. Effects of motivational enhancement on immediate outcomes of batterer intervention. J Fam Violence. (2011) 26:139–49. doi: 10.1007/s10896-010-9353-1
66. Cunha O, Pereira B, Sousa M, Rodrigues AC. Cognitive behavioural “third wave” therapies in the treatment of justice-involved individuals: A systematic review. Aggress Violent Behav. (2024) 76:101923. doi: 10.1016/j.avb.2024.101923
67. Murphy CM, Ting LA. Interventions for perpetrators of intimate partner violence: A review of efficacy research and recent trends. Partn Abuse. (2010) 1:26–44. doi: 10.1891/1946-6560.1.1.26
68. Lila M, Gracia E, Catalá-Miñana A. Individualized motivational plans in batterer intervention programs: A randomized clinical trial. J Consult Clin Psychol. (2018) 86:309–20. doi: 10.1037/ccp0000291
69. Romero-Martínez Á, Lila M, Gracia E, Moya-Albiol L. Improving empathy with motivational strategies in batterer intervention programmes: Results of a randomized controlled trial. Br J Clin Psychol. (2019) 58:125–39. doi: 10.1111/bjc.12204
70. Easton CJ, Crane CA, Mandel D. A randomized controlled trial assessing the efficacy of cognitive behavioral therapy for substance-dependent domestic violence offenders: An integrated substance abuse-domestic violence treatment approach (SADV). J Marital Fam Ther. (2018) 44:483–98. doi: 10.1111/jmft.12260
71. Murphy CM, Ting LA, Jordan LC, Musser PH, Winters JJ, Poole GM, et al. A randomized clinical trial of motivational enhancement therapy for alcohol problems in partner violent men. J Subst Abuse Treat. (2018) 89:11–9. doi: 10.1016/j.jsat.2018.03.004
72. Stuart GL, Shorey RC, Moore TM, Ramsey SE, Kahler CW, O’Farrell TJ, et al. Randomized clinical trial examining the incremental efficacy of a 90-minute motivational alcohol intervention as an adjunct to standard batterer intervention for men: Alcohol clinical trial for batterers. Addiction. (2013) 108:1376–84. doi: 10.1111/add.12142
73. Mbilinyi LF, Neighbors C, Walker DD, Segar K, Walton TO, Roffman RA, et al. What’s in it for me? Motivating the untreated abuser to consider treatment. J Fam Violence. (2023) 38:333–46. doi: 10.1007/s10896-022-00375-9
74. López-Ossorio JJ, González-Álvarez JL, Andrés-Pueyo A. Eficacia predictiva de la valoración policial del riesgo de la violencia de género. Psychosoc Interv. (2016) 25:1–7. doi: 10.1016/j.psi.2015.10.002
75. Kropp PR, Hart S, Webster C, Eaves D. Spousal risk assessment guide user’s manual. Toronto, Canada: Multi-Health Systems and BC Institute Against Family Violence (1999). 50 p.
76. Andrés-Pueyo A, López S, Álvarez A. Valoración del riesgo de violencia contra la pareja por medio de la SARA. Papeles Psicólogo. (2008) 29:107–22.
77. Messing JT, Thaller J. The average predictive validity of intimate partner violence risk assessment instruments. J Interpers Violence. (2013) 28:1537–58. doi: 10.1177/0886260512468250
78. Expósito-Álvarez C, Roldán-Pardo M, Gilchrist G, Lila M. Integrated motivational strategies for intimate partner violence perpetrators with substance use: A randomized controlled trial. Psychosoc Interv. (2024) 33:187–200. doi: 10.5093/pi2024a13
79. Babor TF, Grant M. From clinical research to secondary prevention: International collaboration in the development of the Alcohol Disorders Identification Test (AUDIT). Alcohol Health Res World. (1989) 13:371–5.
80. Contel Guillamón M, Gual Solé A, Colom Farran J. Test para la identificación de transtornos por uso de alcohol (AUDIT): Traducción y validación del AUDIT al catalán y castellano. Adicciones. (1999) 11:337. doi: 10.20882/adicciones.613
81. Allen JP, Litten RZ, Fertig JB, Babor T. A review of research on the alcohol use disorders identification test (AUDIT). Alcohol Clin Exp Res. (1997) 21:613–9. doi: 10.1111/j.1530-0277.1997.tb03811.x
82. Romero-Martínez Á, Lila M, Sarrate-Costa C, Comes-Fayos J, Moya-Albiol L. Neuropsychological performance, substance misuse, and recidivism in intimate partner violence perpetrators. Psychosoc Interv. (2023) 32:69–77. doi: 10.5093/pi2022a7
83. Millon T. Inventario clínico multiaxial de Millon-III [MCMI-III. Millon clinical multiaxial inventory-III. Manual]. Madrid, España: TEA Ediciones (2007). 190 p.
84. Cardenal V, Sánchez MP. Adaptación y baremación al español del Inventario Clínico Multiaxial de Millon-III (MCMI-III) [Spanish adaptation and scaling of the Millon Clinical Multiaxial Inventory-III]. Madrid, España: TEA Ediciones (2007). 190 p.
85. Lila M, Gracia E, Catalá-Miñana A. More likely to dropout, but what if they don’t? Partner violence offenders with alcohol abuse problems completing batterer intervention programs. J Interpers Violence. (2020) 35:1958–81. doi: 10.1177/0886260517699952
86. Richards TN, Jennings WG, Murphy C. Risk and protective factors for batterer intervention treatment program attrition: How completers are distinct from dropouts and no-shows. J Interpers Violence. (2021) 36:7351–70. doi: 10.1177/0886260519834096
87. Gover AR, Jennings WG, Davis C, Tomsich EA, Tewksbury R. Factors related to the completion of domestic violence offender treatment: The Colorado experience. Vict Offenders. (2011) 6:137–56. doi: 10.1080/15564886.2011.557323
88. Lila M, Martín-Fernández M, Gracia E, López-Ossorio JJ, González JL. Identifying key predictors of recidivism among offenders attending a batterer intervention program: A survival analysis. Psychosoc Interv. (2019) 28:157–67. doi: 10.5093/pi2019a19
89. Crane CA, Testa M, Schlauch RC, Leonard KE. The couple that smokes together: Dyadic marijuana use and relationship functioning during conflict. Psychol Addict Behav. (2016) 30:686–93. doi: 10.1037/adb0000198
90. Leonard KE, Quigley BM. Drinking and marital aggression in newlyweds: an event-based analysis of drinking and the occurrence of husband marital aggression. J Stud Alcohol. (1999) 60:537–45. doi: 10.15288/jsa.1999.60.537
91. Siria S, Leza L, Fernández-Montalvo J, Echauri JA, Azkarate JM, Martínez M. Differential psychopathological profile of male intimate partner violence perpetrators depending on problematic alcohol use. Addict Behav. (2021) 118:106887. doi: 10.1016/j.addbeh.2021.106887
92. Gilchrist G, Hegarty K. Tailored integrated interventions for intimate partner violence and substance use are urgently needed. Drug Alcohol Rev. (2017) 36:3–6. doi: 10.1111/dar.12526
93. Easton CJ, Sacco KA, Neavins TM, Wupperman P, George TP. Neurocognitive performance among alcohol dependent men with and without physical violence toward their partners: A preliminary report. Am J Drug Alcohol Abuse. (2008) 34:29–37. doi: 10.1080/00952990701764326
94. Curwood SE, DeGeer I, Hymmen P, Lehmann P. Using strength-based approaches to explore pretreatment change in men who abuse their partners. J Interpers Violence. (2011) 26:2698–715. doi: 10.1177/0886260510388283
95. Lee MY, Uken A, Sebold J. Self-determined goals and treatment of domestic violence offenders: What if we leave it up to them? Partn Abuse. (2014) 5:239–58. doi: 10.1891/1946-6560.5.3.239
96. Lee MY, Uken A, Sebold J. Role of self-determined goals in predicting recidivism in domestic violence offenders. Res Soc Work Pract. (2007) 17:30–41. doi: 10.1177/1049731506294375
97. Eckhardt CI, Parrott DJ, Massa AA. Substance use and intimate partner violence perpetration. In: Geffner R, White JW, Hamberger LK, Rosenbaum A, Vaughan-Eden V, Vieth VI, editors. Handbook of Interpersonal Violence and Abuse Across the Lifespan. Springer International Publishing, Cham (2022). p. 2399–418. doi: 10.1007/978-3-319-89999-2_156
98. Bennett LW. Substance abuse by men in partner abuse intervention programs: Current issues and promising trends. Violence Vict. (2008) 23:236–48. doi: 10.1891/0886-6708.23.2.236
99. Klostermann KC. Substance abuse and intimate partner violence: treatment considerations. Subst Abuse Treat Prev Policy. (2006) 1:24. doi: 10.1186/1747-597X-1-24
100. Alexander PC, Morris E. Stages of change in batterers and their response to treatment. Violence Vict. (2008) 23:476–92. doi: 10.1891/0886-6708.23.4.476
101. Sun G-W, Shook TL, Kay GL. Inappropriate use of bivariable analysis to screen risk factors for use in multivariable analysis. J Clin Epidemiol. (1996) 49:907–16. doi: 10.1016/0895-4356(96)00025-X
102. Lakens D, Scheel AM, Isager PM. Equivalence testing for psychological research: A tutorial. Adv Methods Pract Psychol Sci. (2018) 1:259–69. doi: 10.1177/2515245918770963
103. Stephens-Lewis D, Johnson A, Huntley A, Gilchrist E, McMurran M, Henderson J, et al. Interventions to reduce intimate partner violence perpetration by men who use substances: A systematic review and meta-analysis of efficacy. Trauma Violence Abuse. (2021) 22:1262–78. doi: 10.1177/1524838019882357
Keywords: intimate partner violence perpetrators, intervention programs, motivational strategies, individualized motivational plan, substance use problems
Citation: Lila M, Expósito-Álvarez C and Roldán-Pardo M (2025) Motivational strategies reduce recidivism and enhance treatment adherence in intimate partner violence perpetrators with substance use problems. Front. Psychiatry 16:1538050. doi: 10.3389/fpsyt.2025.1538050
Received: 02 December 2024; Accepted: 15 January 2025;
Published: 30 January 2025.
Edited by:
Cory A Crane, Rochester Institute of Technology (RIT), United StatesReviewed by:
Jaymes Fairfax-Columbo, Non-Profit Agency, United StatesTeresa Pinto E Silva, University of Minho, Portugal
Copyright © 2025 Lila, Expósito-Álvarez and Roldán-Pardo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marisol Lila, TWFyaXNvbC5MaWxhQHV2LmVz