 Yuanping Liao1
Yuanping Liao1 Yunhui Zhong
Yunhui Zhong Xiang-Yang Zhang
Xiang-Yang Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 06 March 2025
Sec. Schizophrenia
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1517540
This article is part of the Research TopicStandardizing Cognitive Endophenotype Profiling in Bipolar Disorder and SchizophreniaView all 5 articles
Background: Alexithymia and cognitive dysfunction are common in patients with schizophrenia. However, only a few studies have investigated the cognitive performance of patients with schizophrenia and comorbid alexithymia. This study aimed to investigate the relationship between alexithymia and neurocognitive impairment in patients with schizophrenia.
Methods: A total of 695 patients who met the DSM-IV diagnostic criteria for schizophrenia were included in this cross-sectional study (male/female = 464/231). Demographic and clinical data were collected using self-reported questionnaires. The severity of alexithymia was assessed using the Toronto Alexithymia Scale (TAS-20), cognitive function was assessed using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) tool, and the severity of psychiatric symptoms was assessed using the Positive and Negative Syndrome Scale (PANSS).
Results: The prevalence of comorbid alexithymia in patients with chronic schizophrenia was 31.40%, with a male preponderance. Patients with alexithymia had higher PANSS negative symptom subscale scores and PANSS total scores than those without alexithymia (p < 0.05 for all). In addition, patients with alexithymia had more severe deficits in immediate memory, delayed memory, and language and lower RBANS scores than those without alexithymia. Stepwise multivariate regression analysis showed that alexithymia was a risk factor for language deficits and indicated low total RBANS scores in patients with schizophrenia.
Conclusion: This study suggests that patients with chronic schizophrenia with alexithymia have poorer cognitive function than those without alexithymia. Some demographic characteristics and alexithymia are risk factors for cognitive dysfunction in patients with chronic schizophrenia.
Alexithymia was initially introduced by Sifneos in 1973 within the context of psychosomatic disorders (1). It is clinically characterized by the inability to verbally articulate emotions, an absence of inner fantasy, the use of mundane and specific words and thoughts predominantly associated with external events, a tendency to describe physical symptoms over emotions, difficulty recognizing internal emotions or bodily sensations, and the inability to use these sensations or feelings as indicators of emotional distress (2). Studies have highlighted a strong relationship between alexithymia and schizophrenia (SCZ) (3). Compared with healthy individuals, patients with SCZ have a higher risk of developing alexithymia (4). Yi et al. reported that the prevalence of alexithymia in patients with SCZ was as high as 35.2% (5). Notably, alexithymia has a strong influence on psychopathological conditions (6), sleep quality (7), suicidal ideation (8), social functioning (4), and neurocognition (9) in patients with SCZ.
Neurocognition, defined as the process of connecting and evaluating information, encompasses processing speed, attention, verbal and visual learning, memory, working memory, and reasoning and problem-solving skills (10). Approximately 75% of patients with SCZ experience cognitive impairment (11), which is not only a core feature of the disorder (12–14) but also a strong predictor of functional outcomes (15). This impairment can lead to compromised work and social functioning, resulting in unemployment and an inability to live independently (16, 17).
Some studies have shown a relationship between alexithymia and neurocognitive impairment, particularly in memory and executive functioning (18–20). Hyper-referential alexithymia has been identified as a risk factor for cognitive decline (12). However, existing studies on the relationship between alexithymia and neurocognition in patients with SCZ have shown inconsistent findings. For instance, Fogley et al. discovered that alexithymia, specifically difficulty identifying feelings (DIF) and externally oriented thinking (EOT) rather than difficulty describing feelings (DDF), was associated with processing speed and working memory in patients with SCZ (18). On the contrary, He et al. found that DIF, DDF, and EOT in alexithymia were correlated with poorer visuospatial functioning, executive functioning, and delayed memory but not with verbal functioning (21). Moreover, Peng et al. demonstrated an independent relationship between language and DDF (9). These divergent findings emphasize the requirement for a comprehensive investigation into the relationship between alexithymia and neurocognition.
To address these inconsistencies, the current study aims to more comprehensively examine the relationship between alexithymia and neurocognitive performance in patients with chronic SCZ. By including a large sample of 695 patients and utilizing validated measures such as the Toronto Alexithymia Scale (TAS-20) for alexithymia, the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) for cognitive function, and the Positive and Negative Syndrome Scale (PANSS) for symptom severity, this study provides a more robust analysis of the potential impact of alexithymia on various cognitive domains, including memory, attention, and language.
In this study, we hypothesize that patients with SCZ and comorbid alexithymia will exhibit more severe cognitive impairment, particularly in memory and language, than those without alexithymia. By exploring this hypothesis, we aim to provide a clearer understanding of how alexithymia contributes to cognitive deficits in chronic schizophrenia, thereby informing both clinical interventions and future research in this area.
This cross-sectional study recruited 720 patients with chronic schizophrenia (SCZ) from Wuhan Xinzhou Mental Health Center and Guangzhou Huiai Hospital, China, from January to April 2019. The data used in this study were shared with a previously published paper by the last author (DOI: 10.30773/pi.2023.0004), which also utilized data collected under the same ethical approval from the Institutional Review Board of the Institute of Psychology, Chinese Academy of Sciences (IRB: H18031). The cohort used in both studies includes patients with chronic SCZ diagnosed based on the Chinese version of the Structured Clinical Interview for Diagnostic and Statistical Mental Disorders-5 (DSM-5), and all participants had signed informed consent forms.
The data collection protocols were consistent with those described in the previously published paper (DOI: 10.30773/pi.2023.0004), and all participants or their legal guardians provided written informed consent prior to participation.
A data collection form was used to obtain information regarding the demographic and clinical characteristics of the participants, including age, sex, level of education, marital status, BMI, age at the onset of SCZ, duration of the illness, and smoking behavior. BMI was calculated using the formula: BMI = weight (kg)/height (migh Height and weight were measured by trained researchers using standardized procedures. A questionnaire was administered by a researcher through a one-on-one semi-structured interview. Subsequently, the researcher collected the clinical data of patients by reviewing their medical records and conducting clinical interviews with them.
The Toronto Alexithymia Scale (TAS-20) was used to assess the severity of alexithymia (22). TAS-20 is a self-reporting tool widely used to evaluate the severity of alexithymia in various populations, including patients with SCZ (18, 23). The responses are scored on a scale of 1–5 (from “strongly disagree” to “strongly agree”, respectively). The total score on the scale ranges from 20 to 100, with higher scores indicating higher severity of alexithymia. In this study, patients with a TAS-20 score of >60 were considered to have alexithymia. TAS-20 has demonstrated good internal consistency and retest reliability in previous studies (22). In this study, the Cronbach’s α value for total TAS-20 scores was 0.86.
The severity of clinical psychiatric symptoms was assessed using the Positive and Negative Syndrome Scale (PANSS) (24). PANSS traditionally contains three subscales, namely, positive symptom, negative symptom, and general psychopathology. To ensure the reliability and consistency of the scores, two psychiatrists from our team attended a training program on the use of PANSS. In repeated assessments, the inter-observer correlation coefficient for the total PANSS score was maintained at >0.8. Higher scores indicated more severe symptoms. PANSS has been demonstrated to have strong construct validity and has been widely used in patients with SCZ (25).
Cognitive function was assessed using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The RBANS tool consists of 12 subtests used to calculate five age-adjusted index scores and a total score. The five test indices include immediate memory, visuospatial/constructional skills, language, attention, and delayed memory. We provided appropriate training to each patient so that they could adapt to the testing environment and the computerized task. In repeated assessments, the intra-rater correlation coefficient was 0.92.
Continuous demographic and clinical variables were compared between patients with and without alexithymia using analysis of variance (ANOVA), whereas categorical variables were compared using the chi-square test. In addition, The correlation coefficient matrix between Cognitive performance and alexithymia was calculated using Pearson correlation analyses on each RBANS score and the matching TAS-20 total scores and subscales. The Bonferroni method was used to adjust for multiple tests. We then performed partial correlations by controlling covariates (including sex, Negative symptom and PANSS Total score) and investigating the interconnections between Cognitive performance and alexithymia. Binary logistic regression analysis was performed to identify risk factors closely associated with comorbid alexithymia. Furthermore, stepwise multiple regression analysis was used to examine the relationship between the total TAS-20 score and the PANSS or RBANS score.
All data were statistically analyzed using the SPSS (version 21.0) software (IBM, Armonk, NY, USA) and were expressed as the mean ± standard deviation (mean ± SD). A two-tailed p-value of <0.05 indicated statistically significant differences.
A total of 25 patients who refused to participate in the study or whose scales were filled incompletely were excluded from this study. Finally, a total of 695 patients with SCZ, including 464 men and 231 women, were included in this study. The duration of the illness of the included patients was 20.69 ± 11.80 years. The mean age of the included patients was 45.95 ± 12.41 years, ranging from 20 to 70 years. The mean duration of education was 9.49 ± 3.17 years, ranging from 1 to 21 years. The mean age at the onset of SCZ was 25.26 ± 7.56 years, ranging from 9 to 63 years. The mean BMI was 24.797 ± 4.44, ranging from 14.88 to 56.24. On the PANSS, the mean scores for positive symptom, negative symptom, and general psychopathology were 15.90 ± 5.23, 20.49 ± 6.39, and 38.82 ± 8.14, respectively, whereas the mean total score was 75.21 ± 16.30.
As shown in Table 1, 218 (31.40%) of the 695 patients with SCZ had comorbid alexithymia. A significant sex difference was observed in the prevalence of alexithymia, with the proportion of male patients being higher than that of female patients (35.34% versus 23.37%; χ2 = 10.261, p = 0.001). After age and educational qualification were controlled for, the prevalence rate of alexithymia was 0.56 times higher in men than in women (B = 0.583, Wald statistic = 10.125, p < 0.001, OR = 0.558, 95% CI = 0.390–0.799). However, no significant differences in any other demographic variables were observed between patients with and without alexithymia (p > 0.05 for all). Compared with patients without alexithymia, those with alexithymia had higher PANSS negative symptom scores (p < 0.001) and total PANSS scores (p = 0.012). Furthermore, a logistic regression model showed that sex (Wald χ2 = 9.496, df = 1, p < 0.01) and PANSS negative symptom scores (Wald χ2 = 20.807, df = 1, p < 0.01) were independent factors contributing to comorbid alexithymia. Correlation analysis indicated that the total TAS-20 score was significantly positively associated with the PANSS negative symptom score (r = 0.24, p < 0.001), PANSS general psychopathology score (r = 0.14, p < 0.001), and total PANSS score (r = 0.17, p < 0.001). These correlations remained significant after Bonferroni correction (p < 0.001 for all). Subsequently, multiple regression analysis validated that the total TAS-20 score was significantly associated with the PANSS negative symptom score (β = 0.26, t = 2.91, p < 0.01).
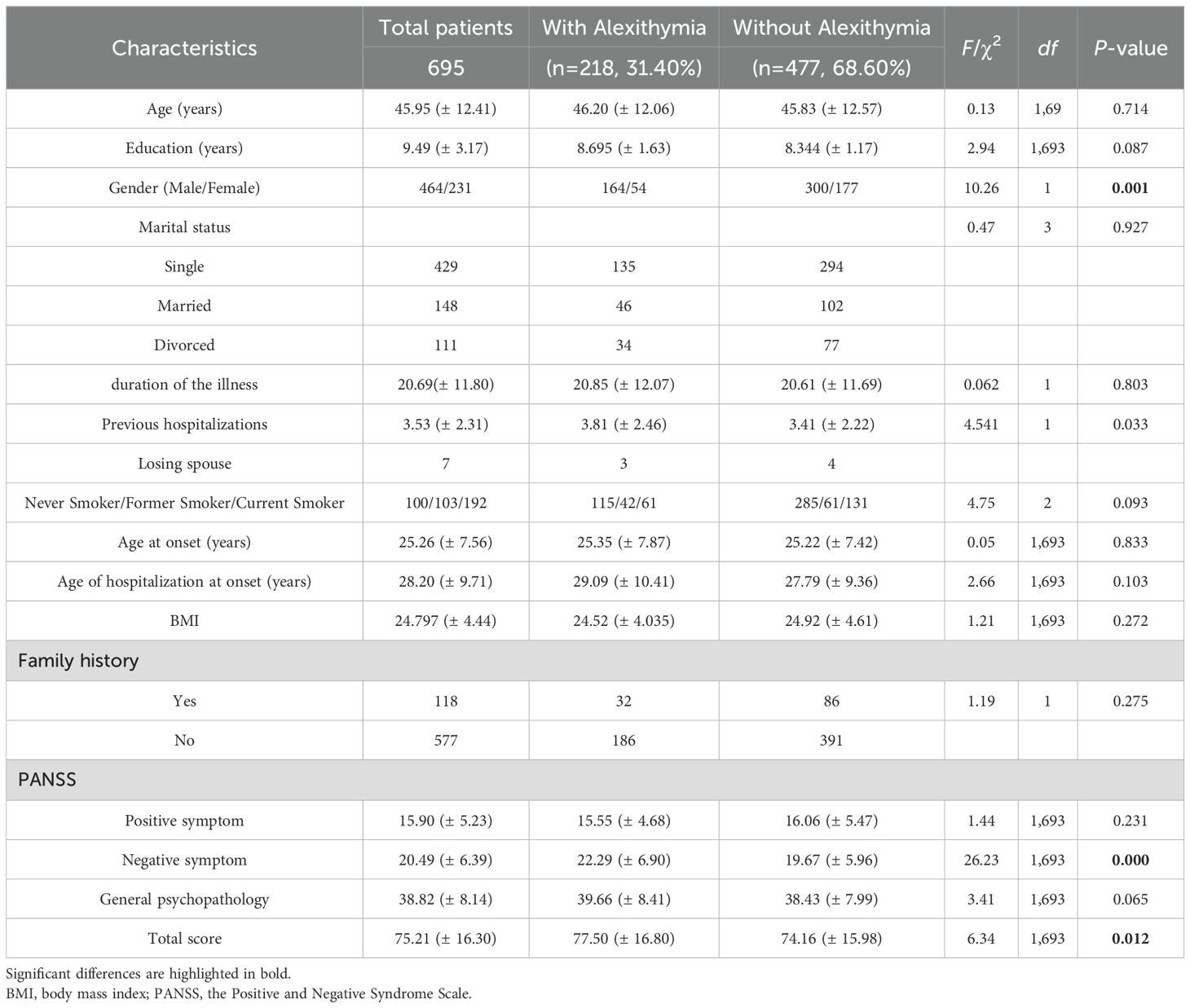
Table 1. Characteristics of schizophrenia patients with or without Alexithymia.
Table 2 shows the cognitive performance of patients with and without alexithymia evaluated using ANOVA. Compared with patients without alexithymia, those with alexithymia had more severe dysfunction with regard to immediate memory (F = 5.185; df = 1,693; p = 0.023), language (F = 9.767; df = 1,693; p = 0.002), and delayed memory (F = 4.844; df = 1,693; p = 0.028) and had lower total index scores (F = 8.700; df = 1,693; p = 0.003).
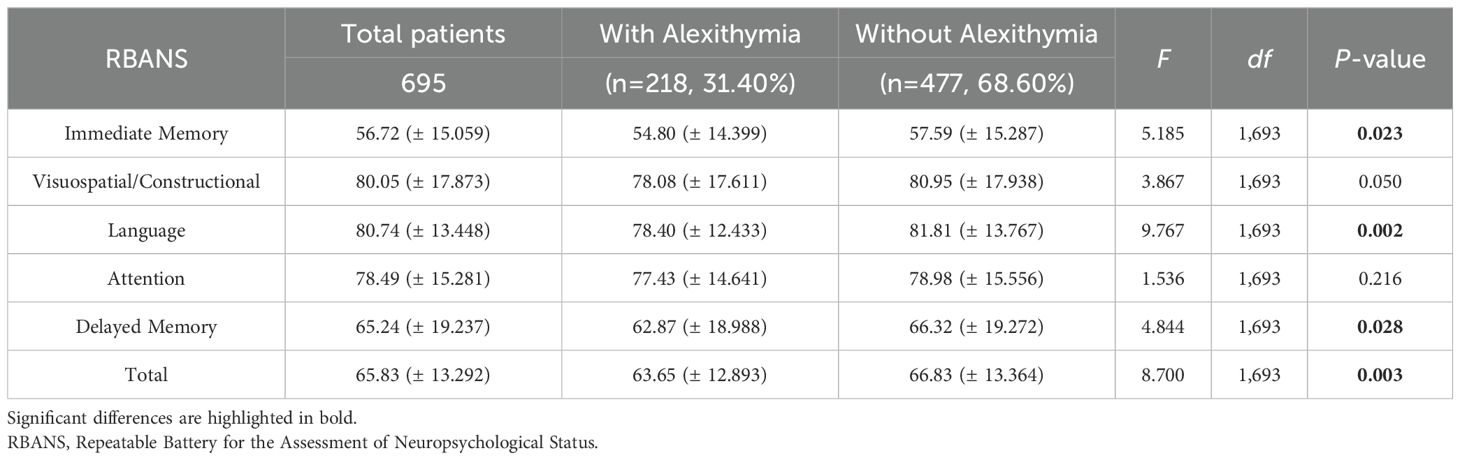
Table 2. Cognitive variables of schizophrenia patients with or without Alexithymia.
We used Pearson correlation to investigate the relationship between the total TAS-20 score and the RBANS index and total scores in patients with SCZ. The results revealed a significant negative correlation between the total TAS-20 score and the RBANS index and total scores in patients with SCZ. After Bonferroni correction, the correlations between the total TAS-20 score and all RBANS index scores, except for visuospatial/constructional index scores, or RBANS total scores remained significant (α = 0.05/21 = 0.0024). Table 3 shows the relationship between TAS-20 scores and RBANS index and total scores. However, alexithymia showed weak but statistically significant correlations with RBANS scores (range: r=−0.133 to −0.192, p<0.01), suggesting modest associations.

Table 3. Association between Alexithymia and Cognitive variables.
Furthermore, stepwise multivariate regression analysis was performed for all patients to investigate the effects of alexithymia on cognitive function in patients with SCZ. The results showed that TAS-20 scores (β = -0.079, t = -2.191, 95% CI = [-0.210, -0.012], p = 0.029), educational qualification (β = 0.107, t = 3.010, 95% CI = [0.158, 0.749], p = 0.003), and PANSS general psychopathology scores (β = -0.122, t = -2.633, 95% CI = [-0.353, -0.051], p = 0.009) were associated with the RBANS language index score. In addition, TAS-20 scores (β = -0.077, t = -2.340, 95% CI = [-0.196, -0.017], p = 0.020), age (β = -0.073, t = -2.291, 95% CI = [-0.145, -0.011], p = 0.022), and BMI (β = 0.069, t = 2.139, 95% CI = [0.017, 0.394], p = 0.033) were associated with the RBANS total score.
This study revealed the effects of comorbid alexithymia on cognitive function in Han Chinese patients with chronic SCZ. The main findings of this study are as follows: (1) The prevalence of comorbid alexithymia in patients with SCZ was 31.40%. Symptoms of alexithymia were associated with some clinical features, including the PANSS negative symptom score. (2) Compared with patients without alexithymia, those with alexithymia had worse neurocognitive deficits with regard to immediate memory and delayed memory and had lower RBANS total scores. (3) Alexithymia was identified as a risk factor for language deficits and overall cognitive dysfunction (based on RBANS scores) in patients with SCZ.
The prevalence of alexithymia in patients with chronic SCZ observed in this study (31.4%) is consistent with that reported in previous studies from different cultures (5, 9, 26, 27). The prevalence of alexithymia in patients with chronic SCZ observed in this study (31.4%) is consistent with that reported in previous studies (5, 9, 14, 26–28) from different cultures. Notably, the prevalence of alexithymia observed in this study significantly exceeds that observed in healthy populations, which ranges from 5% to 25.3% (29–31). This finding suggests that patients with SCZ are at an increased risk of developing difficulties in identifying and expressing emotions. The increased prevalence of alexithymia may be partially attributed to the overlapping symptoms of alexithymia and schizophrenia, particularly concerning emotional blunting, emotional disengagement, and negative symptoms (32). In this study, patients with alexithymia had a higher number of hospitalizations, which may have contributed to their extended hospital stays. Prolonged social isolation and limited interpersonal interactions during these extended hospitalizations could have further exacerbated the challenges associated with emotional recognition and expression (33).
A notable finding of this study is sex disparity in the prevalence of alexithymia, with the proportion of male patients (35.34%) being higher than that of female patients (23.37%). This difference has been reported in many previous studies (9, 34, 35). The higher risk of alexithymia in male patients can be explained as follows: First, according to the Normative Male Alexithymia (NMA) hypothesis proposed by Levant, men raised within traditional paradigms are subject to emotional constriction, which impedes their ability to articulate emotions and feelings verbally. These traditional norms, ostensibly geared toward reinforcing power dynamics and concealing vulnerabilities within patriarchal social structures, may increase the risk of alexithymia in men (36). Second, empirical evidence indicates that compared with female patients with SCZ, male patients with SCZ exhibit more pronounced negative symptoms (e.g., anhedonia and avolition) and diminished social functioning (37–39), both of which are closely associated with dysphoria. However, contradictory findings have also been reported (26, 29), necessitating further investigation into the sex-specific risk of alexithymia to validate the findings of this study.
This study showed a significant correlation between alexithymia and the clinical symptoms of SCZ, particularly emphasizing the potential of alexithymia as an independent risk factor for negative symptoms (5, 9, 26). This relationship may be explained based on neurobiological alterations, specifically the changes in the structure and function of the amygdala, which are involved in the development of negative symptoms in SCZ (40). Changes in brain structure and function may also serve as the neurobiological basis of alexithymia (41). The salience network in the brain is responsible for the negative symptoms of SCZ, and reduced functioning of the salience network has been associated with alexithymia (42). These neurological impairments have led to the identification of a relationship between alexithymia and negative symptoms. Furthermore, personality traits may contribute to this relationship. Specifically, negative symptoms have been significantly positively correlated with the severity of depressive symptoms and the personality trait of harm avoidance (43). Previous studies have also shown that harm avoidance independently predicts alexithymia (43, 44). However, the findings of this study are not consistent with those of previous studies. Some studies have shown no correlation between alexithymia and negative symptoms (19, 32), whereas others have shown a correlation between alexithymia and positive symptoms (45, 46). Additionally, alexithymia has been positively correlated with the severity of hallucinations (19). In a longitudinal study, alexithymia in outpatients with SCZ was not found to be associated with negative symptoms. Moreover, the study showed significant improvements in the severity of negative symptoms but no significant changes in the severity of alexithymia over time (32). These discrepancies highlight the complexity of the relationship between alexithymia and SCZ, emphasizing the necessity of maintaining methodological uniformity in future studies.
Consistent with previous studies (9, 18, 21), this study showed that patients with SCZ with alexithymia had significantly poorer neurocognitive function. Alexithymia is a personality trait that affects the cognitive–emotional interaction (20). Therefore, it may be an important factor contributing to cognitive impairment in patients with SCZ. Furthermore, neurophysiological and neuroimaging studies have shown that cognitive dysfunction and alexithymia may stem from a common neural basis, specifically the corpus callosum, cingulate gyrus, orbital frontal cortex, and insulae. These regions are involved in the regulation of emotions (47, 48). However, some studies have shown a correlation between only a specific score and cognitive performance in alexithymia. For instance, a study showed that only the TAS-20 externally oriented thinking subscale score was associated with basic cognitive functions, such as working memory, attention, and spatial visualization abilities. The study found no relationship between difficulty in identifying feelings and most neurocognitive domains, except for attention (19). Fogley et al. used data from the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) project and found that deficits in processing speed, working memory, and abstract thinking were associated with DIF and EOT (18). However, no relationship was observed between cognitive deficits and DDF.
In this study, we found that patients with SCZ with alexithymia had worse cognitive function with regard to immediate and delayed memory. Alexithymia has been associated with memory. In a study, the memory of healthy individuals was assessed using the Rivermead Behavioral Memory Test (RBMT) Story Subtest. The results showed that individuals with a higher degree of EOT had poorer delayed memory (12). Nielson and Meltzer used an incidental memory task to investigate the impact of physiological arousal on memory in patients with alexithymia. Specifically, they compared the memory for neutral words between patients with high and low degrees of alexithymia. On an immediate recall task, patients with a high degree of alexithymia exhibited more severe memory impairments than those with a low degree of alexithymia (49). Another study showed that alexithymia led to impairments in immediate memory (50). DiStefano and Koven used the Wechsler Memory Scale-III, a non-emotional neuropsychological test, and found that patients with a low degree of alexithymia had better immediate and delayed visual memory than those with a high degree of alexithymia (51). These findings suggest an important relationship between alexithymia and both immediate and delayed memory. While univariate analyses suggested associations between alexithymia and memory deficits, these relationships were attenuated in multivariate models accounting for negative symptoms and other confounders. This indicates that the observed memory differences in univariate tests may reflect shared variance with clinical symptoms (e.g., PANSS negative scores) rather than a direct effect of alexithymia. These results highlight the importance of controlling for psychiatric symptoms when investigating cognitive correlates of alexithymia in schizophrenia. In this study, alexithymia was identified as a risk factor for language impairment. A study showed that patients with language impairment caused by a penetrating brain injury had more severe alexithymia than healthy individuals. In addition, the extent of brain damage in the inferior frontal gyrus (IFG), a key part of the language network, was associated with a higher degree of alexithymia (52). These findings are consistent with the linguistic hypothesis of alexithymia (53), which states that language impairments may contribute to the development of alexithymia. Therefore, further investigation is warranted to assess whether therapeutic interventions aimed at mitigating language impairments may alleviate alexithymia in patients with SCZ.
Despite notable findings, this study has some limitations that should be acknowledged. First, the use of a cross-sectional study design limited the in-depth investigation of the causal relationship between SCZ with comorbid alexithymia and cognitive impairment or negative symptoms. Long-term longitudinal studies may provide a more comprehensive understanding of this relationship. Second, this study included only Han Chinese patients with chronic SCZ. Therefore, further studies are warranted to confirm the relevance of the findings in patients with acute schizophrenia and diverse cultural backgrounds. Various medications and treatment factors can influence alexithymia and may obscure its relationship with clinical symptoms and cognitive functioning. Third, we did not thoroughly analyze the relationship between the individual TAS-20 subscales and cognitive functioning. Additionally, the severity of alexithymia was assessed solely based on self-reported questionnaires, without the use of clinical interviews. Fourth, although the RBANS tool enables a valid and reliable assessment of neurocognition, it does not include executive functioning, which is closely associated with alexithymia. Therefore, to validate and strengthen the findings of this study, comprehensive instruments should be used to assess affective disorders and neurocognition in future in-depth longitudinal studies. Fifth, we did not assess whether participants had sought or received psychotherapy or counseling interventions, which may have had an impact on their symptomatology. In future studies, we will aim to incorporate assessments of these non-prescriptive interventions to better understand their role in preventing or alleviating symptoms in individuals with schizophrenia.
In conclusion, this study revealed not only the prevalence of alexithymia in Han Chinese patients with chronic SCZ but also its significant relationship with negative symptoms and neurocognitive deficits. These findings suggest that early alexithymia screening should be incorporated into the diagnostic and therapeutic framework of schizophrenia and personalized treatment strategies should be developed to address challenges associated with comorbid alexithymia. In addition, future studies should focus on elucidating the pathological mechanisms underlying alexithymia in patients with SCZ and developing innovative treatment modalities for enhancing the well-being and quality of life of patients with schizophrenia with comorbid alexithymia.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by The Institutional Review Board of the Institute of Psychology, Chinese Academy of Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YL: Writing – original draft, Formal analysis. YZ: Formal Analysis, Writing – original draft. KY: Data curation, Writing – original draft. X-YZ: Conceptualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the CAS Pioneer Hundred Talents Program (X-YZ).
We thank all the clinical psychiatrists and nurses in Guangzhou Huiai Hospital and Wuhan Xinzhou Mental Health Center for all of their hard work and significant contributions toward the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sifneos PE. The prevalence of ‘Alexithymic’ Characteristics in psychosomatic patients. Psychother And Psychosomatics. (1973) 22:255–62. doi: 10.1159/000286529
2. Lesser IM. Current concepts in psychiatry. Alexithymia N Engl J Med. (1985) 312:690–2. doi: 10.1056/NEJM198503143121105
3. O’Driscoll C, Laing J, Mason O. Cognitive emotion regulation strategies, alexithymia and dissociation in schizophrenia, a review and meta-analysis. Clin Psychol Rev. (2014) 34:482–95. doi: 10.1016/j.cpr.2014.07.002
4. Ospina LH, Shanahan M, Perez-Rodriguez MM, Chan CC, Clari R, Burdick KE. Alexithymia predicts poorer social and everyday functioning in schizophrenia and bipolar disorder. Psychiatry Res. (2019) 273:218–26. doi: 10.1016/j.psychres.2019.01.033
5. Yi Y, Huang Y, Jiang R, Chen Q, Yang M, Li H, et al. The percentage and clinical correlates of alexithymia in stable patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. (2023) 273:679–86. doi: 10.1007/s00406-022-01492-8
6. Picardi A, Caroppo E, Porcelli P, Di Maria G, Munittola G, Martinotti G. Alexithymia and severe psychopathology: A study on psychiatric inpatients. Psychopathology. (2012) 45:159–66. doi: 10.1159/000330261
7. Alimoradi Z, Majd NR, Broström A, Tsang H, Singh P, Ohayon MM, et al. Is alexithymia associated with sleep problems? A systematic review and meta-analysis. Neurosci Biobehav Rev. (2022) 133:104513. doi: 10.1016/j.neubiorev.2021.12.036
8. Demirkol ME, Tamam L, Namli Z, Karaytuğ MO, Uğur K. Association of psychache and alexithymia with suicide in patients with schizophrenia. J Nerv Ment Dis. (2019) 207:668–74. doi: 10.1097/NMD.0000000000001023
9. Peng P, Wang D, Wang Q, Zhou Y, Hao Y, Chen S, et al. Alexithymia in Chinese patients with chronic schizophrenia: Prevalence, clinical correlates, and relationship with neurocognition and empathy. Asia-Pac Psychiatry. (2023) 15:e12547. doi: 10.1111/appy.12547
10. Kovasznay B. Integrated psychological therapy (IPT) for the treatment of neurocognition, social cognition and social competency in schizophrenia patients. Psychiatr Serv. (2013) 42:64–64U68. doi: 10.1026/1616-3443/a000159
11. Talreja BT, Shah S, Kataria L. Cognitive function in schizophrenia and its association with socio-demographics factors. Ind Psychiatry J. (2013) 22:47–53. doi: 10.4103/0972-6748.123619
12. Correro AN 2nd, Paitel ER, Byers SJ, Nielson KA. The role of alexithymia in memory and executive functioning across the lifespan. Cognit Emot. (2021) 35:524–39. doi: 10.1080/02699931.2019.1659232
13. Gebreegziabhere Y, Habatmu K, Mihretu A, Cella M, Alem A. Cognitive impairment in people with schizophrenia: an umbrella review. Eur Arch Psychiatry Clin Neurosci. (2022) 272:1139–55. doi: 10.1007/s00406-022-01416-6
14. McGillivray L, Becerra R, Harms C. Prevalence and demographic correlates of alexithymia: A comparison between Australian psychiatric and community samples. J Clin Psychol. (2017) 73:76–87. doi: 10.1002/jclp.22314
15. Javitt DC. Cognitive impairment associated with schizophrenia: from pathophysiology to treatment. Annu Rev Pharmacol Toxicol. (2023) 63:119–41. doi: 10.1146/annurev-pharmtox-051921-093250
16. Foster Green M. What are the functional consequences of neurocognitive deficits in schizophrenia. Am J Psychiatry. (1996) 153:321–30. doi: 10.1176/ajp.153.3.321
17. Kern RS, Gold JM, Dickinson D, Green MF, Nuechterlein KH, Baade LE, et al. The MCCB impairment profile for schizophrenia outpatients: Results from the MATRICS psychometric and standardization study. Schizophr Res. (2011) 126:124–31. doi: 10.1016/j.schres.2010.11.008
18. Fogley R, Warman D, Lysaker PH. Alexithymia in schizophrenia: Associations with neurocognition and emotional distress. Psychiatry Res. (2014) 218:1–6. doi: 10.1016/j.psychres.2014.04.020
19. Gawęda Ł, Krężołek M. Cognitive mechanisms of alexithymia in schizophrenia: Investigating the role of basic neurocognitive functioning and cognitive biases. Psychiatry Res. (2019) 271:573–80. doi: 10.1016/j.psychres.2018.12.023
20. Luminet O, Nielson KA, Ridout N. Cognitive-emotional processing in alexithymia: an integrative review. Cognit Emot. (2021) 35:449–87. doi: 10.1080/02699931.2021.1908231
21. He C, Zhang X, Xia Q. Exploring the link between cognitive deficit, self-esteem, alexithymia, and depressive symptom of schizophrenia. Brain Behav. (2022) 12:e2648. doi: 10.1002/brb3.v12.7
22. Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto Alexithymia Scale–I. Item selection and cross-validation of the factor structure. J Psychosom Res. (1994) 38:23–32. doi: 10.1016/0022-3999(94)90005-1
23. Heshmati R, Allahverdipour H, Tabatabaei MG, Kamrani S. Toronto alexithymia scale (TAS-20): A study of patients with schizophrenia spectrum disorders. Proc - Soc Behav Sci. (2011) 30:771–5. doi: 10.1016/j.sbspro.2011.10.150
24. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
25. Shafer A, Dazzi F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J Psychiatr Res. (2019) 115:113–20. doi: 10.1016/j.jpsychires.2019.05.008
26. Shang Z, Fang C, Lang X, Zhang X. Gender difference in association between clinical symptoms and alexithymia in chronic schizophrenia: A large sample study based on Chinese Han population. J Affect Disord. (2024) 344:519–27. doi: 10.1016/j.jad.2023.10.088
27. Zhong Y, Li Y, Hu A, Zhang XY. Prevalence, demographics and clinical characteristics of Internet addiction among Chinese adolescents with schizophrenia. Front Psychiatry. (2024) 15:1398479. doi: 10.3389/fpsyt.2024.1398479
28. Etchepare A, Roux S, Destaillats JM, Cady F, Fontanier D, Couhet G, et al. What are the specificities of social cognition in schizophrenia? A cluster-analytic study comparing schizophrenia with the general population. Psychiatry Res. (2019) 272:369–79. doi: 10.1016/j.psychres.2018.12.042
29. De Barros ACS, Furlan AER, Marques LHN, De Araújo Filho GM. Gender differences in prevalence of psychiatric disorders, levels of alexithymia, and coping strategies in patients with refractory mesial temporal epilepsy and comorbid psychogenic nonepileptic seizures. Epilepsy Behav. (2018) 82:1–5. doi: 10.1016/j.yebeh.2018.02.026
30. Zhang X, Bai X, Bian L, Wang M. The influence of personality, alexithymia and work engagement on burnout among village doctors in China: a cross-sectional study. BMC Public Health. (2021) 21:1507. doi: 10.1186/s12889-021-11544-8
31. Zhao F, Lung H, Chen P, Chang M, Lung F. Religion and the mediating role of alexithymia in the mental distress of healthcare workers during the coronavirus disease 2019 pandemic in a psychiatric hospital in China. Front Psychiatry. (2022) 13:837916. doi: 10.3389/fpsyt.2022.837916
32. Todarello O, Porcelli P, Grilletti F, Bellomo A. Is alexithymia related to negative symptoms of schizophrenia? A preliminary longitudinal study. Psychopathology. (2005) 38:310–4. doi: 10.1159/000088919
33. Chen L, Xu L, You W, Zhang X, Ling N. Prevalence and associated factors of alexithymia among adult prisoners in China: A cross-sectional study. BMC Psychiatry. (2017) 17:287. doi: 10.1186/s12888-017-1443-7
34. Huo L, Qu D, Pei C, Wu W, Ning Y, Zhou Y, et al. Alexithymia in chronic schizophrenia and its mediating effect between cognitive deficits and negative symptoms. Schizophr Res. (2023) 261:275–80. doi: 10.1016/j.schres.2023.10.006
35. van ‘t Wout M, Aleman A, Bermond B, Kahn RS. No words for feelings: alexithymia in schizophrenia patients and first-degree relatives. Compr Psychiatry. (2007) 48:27–33. doi: 10.1016/j.comppsych.2006.07.003
36. Levant RF, Hall RJ, Williams CM, Hasan NT. Gender differences in alexithymia. Psychol Men Masculinities. (2007) 10:190–203. doi: 10.1016/j.comppsych.2006.07.003
37. Barendse M, Lara GA, Guyer AE, Swartz JR, Taylor SL, Shirtcliff EA, et al. Sex and pubertal influences on the neurodevelopmental underpinnings of schizophrenia: A case for longitudinal research on adolescents. Schizophr Res. (2023) 252:231–41. doi: 10.1016/j.schres.2022.12.011
38. Chan KN, Chang WC, Ng CM, Lee HC, Chan SI, Chiu SY, et al. Sex differences in symptom severity, cognition and psychosocial functioning among individuals with at-risk mental state for psychosis. Early Interv Psychiatry. (2022) 16:61–8. doi: 10.1111/eip.13131
39. Hanlon MC, Campbell LE, Single N, Coleman C, Morgan VA, Cotton SM, et al. Men and women with psychosis and the impact of illness-duration on sex-differences: The second Australian national survey of psychosis. Psychiatry Res. (2017) 256:130–43. doi: 10.1016/j.psychres.2017.06.024
40. Rahm C, Liberg B, Reckless G, Ousdal O, Melle I, Andreassen OA, et al. Negative symptoms in schizophrenia show association with amygdala volumes and neural activation during affective processing. Acta Neuropsychiatrica. (2015) 27:213–20. doi: 10.1017/neu.2015.11
41. Xu P, Opmeer EM, van Tol MJ, Goerlich KS, Aleman A. Structure of the alexithymic brain: A parametric coordinate-based meta-analysis. Neurosci Biobehav Rev. (2018) 87:50–5. doi: 10.1016/j.neubiorev.2018.01.004
42. Lee SK, Lee JS, Shin YB, Kim HE, Kim BH, Kim JJ. The relationship between ambivalence, alexithymia, and salience network dysfunction in schizophrenia. Psychiatry Res Neuroimaging. (2021) 310:111271. doi: 10.1016/j.pscychresns.2021.111271
43. Vrbova K, Prasko J, Holubova M, Slepecky M, Ociskova M. Positive and negative symptoms in schizophrenia and their relation to depression, anxiety, hope, self-stigma and personality traits - a cross-sectional study. Neuro Endocrinol Lett. (2018) 39:9–18. doi: 10.26226/morressier.5a7070e4d462b80290b566dc
44. Grabe HJ, Spitzer C, Freyberger HJ. Alexithymia and the temperament and character model of personality. Psychother Psychosom. (2001) 70:261–7. doi: 10.1159/000056264
45. İnanç L, Sevinç E, Semiz ÜB. Relationship between alexithymia, depression and the negative symptoms in schizophrenia with and without deficit syndrome. Turk Psikiyatri Derg. (2019) 30:225–35.
46. Tian Y, Zhou H, Wang D, Zhang X. Association of alexithymia with positive symptoms in chinese chronic schizophrenia patients with and without obesity. Psychiatry Investig. (2023) 20:689–95. doi: 10.30773/pi.2023.0004
47. Li W, Liu Y, Qiu J, Li Y. Bidirectional relationship between insular grey matter volume and alexithymia: Evidence from a longitudinal study. J Affect Disord. (2023) 339:799–806. doi: 10.1016/j.jad.2023.07.041
48. Wingbermühle E, Theunissen H, Verhoeven WM, Kessels RP, Egger JI. The neurocognition of alexithymia: evidence from neuropsychological and neuroimaging studies. Acta Neuropsychiatrica. (2012) 24:67–80. doi: 10.1111/j.1601-5215.2011.00613.x
49. Nielson KA, Meltzer MA. Modulation of long-term memory by arousal in alexithymia: the role of interpretation. Conscious Cogn. (2009) 18:786–93. doi: 10.1016/j.concog.2009.06.001
50. Majerus S, Linden MVD, Mulder L, Meulemans T, Peters F. Verbal short-term memory reflects the sublexical organization of the phonological language network: Evidence from an incidental phonotactic learning paradigm. J Mem Lang. (2004) 51:297–306. doi: 10.1016/j.jml.2004.05.002
51. DiStefano RA, Koven NS. Dysfunctional emotion processing may explain visual memory deficits in alexithymia. Pers And Individ Differences. (2012) 52:611–5. doi: 10.1016/j.paid.2011.12.007
52. Hobson H, Hogeveen J, Brewer R, Catmur C, Gordon B, Krueger F, et al. Language and alexithymia: Evidence for the role of the inferior frontal gyrus in acquired alexithymia. Neuropsychologia. (2018) 111:229–40. doi: 10.1016/j.neuropsychologia.2017.12.037
Keywords: schizophrenia, alexithymia, cognitive impairment, RBANS, comorbid
Citation: Liao Y, Zhong Y, Yang K and Zhang X-Y (2025) Effects of comorbid alexithymia on cognitive impairment in chronic schizophrenia: a large-sample study on the Han Chinese population. Front. Psychiatry 16:1517540. doi: 10.3389/fpsyt.2025.1517540
Received: 26 October 2024; Accepted: 12 February 2025;
Published: 06 March 2025.
Edited by:
Patricia Correa-Ghisays, Center for Biomedical Research in Mental Health Network (CIBERSAM), SpainCopyright © 2025 Liao, Zhong, Yang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiang-Yang Zhang, emhhbmd4eUBwc3ljaC5hYy5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.