
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 27 March 2025
Sec. Addictive Disorders
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1494309
 Maximilian Meyer1
Maximilian Meyer1 Aline Wagner2
Aline Wagner2 André Schmidt1
André Schmidt1 Anna-Chiara Schaub1
Anna-Chiara Schaub1 Undine E. Lang1
Undine E. Lang1 Marc Walter2,3
Marc Walter2,3 Flora Colledge4*
Flora Colledge4*Introduction: Individuals with exercise addiction (EA) report being unable to stop exercising despite its negative psychological, physical, or social impact. Due to a lack of evidence, EA has so far not been officially recognized as a behavioral addiction. Only one study exists, that investigated mental disorders in individuals with EA by utilizing the Structured Clinical Interview for DSM-5 Disorders (SCID-5). The present study followed up on this sample, providing the first longitudinal data on EA.
Methods: All participants of the baseline study were invited to complete validated psychometric instruments assessing symptoms of depression, attention deficit hyperactivity disorder, trauma, and EA. Furthermore, an exhaustive diagnostic assessment with the SCID-5-CV, the SCID-5-PD (following a SAPAS screening), and a self-designed clinical interview to assess EA criteria were conducted.
Results: The response rate was 59.4% (n=19) and the mean duration of follow-up was 634.5 (SD=155.8) days. Number of fulfilled EA criteria in the sample remained largely stable over time with no change in seven (36.8%), a reduction in nine (47.4%), and an increase in three (15.8%). Eighteen out of 19 participants fulfilled the criteria for at least one mental disorder. The most prevalent disorders were major depressive disorder (lifetime prevalence 73.7%; n=14) and obsessive-compulsive personality disorder (52.6%; n=10).
Discussion: This data suggests that EA is a temporary stable and distinct disorder with affected individuals suffering from severe psychological distress. Further studies are necessary to investigate potential cause-effect relationships between co-occurring mental disorders and EA.
Exercise addiction (EA) is a clinical phenomenon that was first reported on in the 1970s (1). It refers to a behavioral pattern comprised of rigid engagement in physical exercise, the inability to stop exercising despite its negative psychological, physical, or social impact, and experiencing psychological and physical distress when reducing or stopping physical exercise (2). To date, a variety of terms, among them “exercise dependence”, “compulsive exercise” and “excessive exercise”, have been introduced in the scientific literature to describe this behavioral pattern (3).
Unlike gambling disorder, EA has not yet been categorized as a behavioral addiction in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (4). This is due to insufficient scientific evidence for the phenomenon; to date, no official diagnostic criteria exist (5). In the past ten years popular interest and case reports of EA have increased substantially (6). However, research conducted in the area suffers from a variety of methodological weaknesses (7). For the identification of EA, researchers have so far mostly relied on self-report instruments, with the Exercise Dependence Scale-21 (EDS-21) being one of the most widely used (8). This scale assesses EA, symptoms but has been demonstrated to overestimate the prevalence of EA if validated with clinical interviews (9). Furthermore, many of these measurement tools are unable to distinguish primary EA from instrumental or secondary EA (10). Whereas primary EA emerges independently from co-occurring disorders, instrumental EA serves the function of achieving a goal unrelated to exercise itself (11). This distinction is particularly relevant in case of co-occurring eating disorders, where exercise can be instrumental in controlling weight, but the physical activity itself is not directly rewarding for the affected individual (12).
Other co-occurring disorders in individuals with EA symptoms are depression, personality disorders, obsessive-compulsive disorders, anxiety disorders, ADHD, and substance use disorders (13–16). It is possible that exercise represents a maladaptive coping strategy for the affected individuals. However, comorbidities in these studies are usually derived from cross-sectional self-report surveys rather than structured diagnostic interviews conducted by clinicians. Hence, these studies do not allow inferences about the relationship between EA symptoms and comorbidities over time.
To date, the development of EA is not fully understood. Following the self-medication hypothesis, individuals suffering from these disorders might use exercise to alleviate symptoms of their “primary” condition (17). Likewise, EA could be understood as a symptom of the underlying disorder, rather than its own entity, thereby complicating diagnostic efforts. To provide a better understanding of the phenomenon and its aetiology, the interactional model of EA was proposed by Egorov and Szabo (2013) (18) and was expanded in 2021 (19). It provides a comprehensive framework, consisting of several intrinsic and extrinsic factors that may predispose or protect an individual from EA behavior in case of trigger events (described by the authors as “sudden or progressively intolerable life-stress”). Besides personal and situational factors, the interactional model considers a variety of underlying exercising motivations, explaining why some individuals might develop EA symptoms, whereas others express healthy exercising patterns. Since various paths may lead to EA, depending on life-circumstances and intrinsic factors, the interactional model explains the methodological hurdles previous EA researchers have encountered.
Currently, only one study has investigated mental disorders in individuals with EA by utilizing the Structured Clinical Interview for DSM-5 Disorders (SCID-5) (16). Meyer et al. recruited individuals who stated to exercise 10 h a week or more and continue their workout despite illness or injury. Flyers were distributed in gyms, universities, on public transportation, and via newspaper advertisements, inviting all persons between ages 18 to 70, who felt they did “too much exercise”, to contact the study group. These individuals were then asked to complete the Exercise Dependence Scale (EDS-21) (8), Beck’s Depression Inventory (BDI-II) (20), Homburger ADHS-Skalen für Erwachsene (HASE; Homburg ADHD Scale for Adults) (21), and the Childhood Trauma Questionnaire (CTQ) (22). Participants who met the EDS-21 cut-off for being “at risk for exercise dependence” (i.e., scoring 5 or 6 on three or more subscales) were subsequently invited to a second examination. In the second examination, all 32 participants completed a semi-structured interview about their exercising habits as well as the SCID-5-CV (23), which assesses all mental disorders aside from personality disorders. Furthermore, all participants completed the Standardized Assessment of Personality - Abbreviated Scale (SAPAS), a brief screening tool for personality disorders (24). In cases in which the SAPAS cut-off was met, the SCID-5-PD, which assesses personality disorders, was additionally employed. In total, 75% (n=24) of the sample fulfilled the diagnostic criteria for at least one mental disorder. The most common disorders in the sample were depressive disorders (56%), personality disorders (47%) and obsessive-compulsive disorders (31.3%) (16). However, the study followed a cross-sectional design and does not allow for conclusions about the stability of EA symptoms and co-occurring mental disorders over time.
By conducting follow-up diagnostic and EA interviews, this study is the first to report longitudinal data from the Meyer et al. sample of individuals with EA. This study aimed to investigate the stability of co-occurring mental disorders as well as EA symptoms and severity over time. No hypothesis was formulated prior to study conduction, as the goal of this exploratory study was to find out, whether EA symptoms increase, decrease, or remain stable over time. Elucidating the course of EA improves the understanding of the phenomenon. This would allow the improvement of diagnostic tools, as well as the development of targeted therapeutic interventions.
A cross-sectional study was initiated in 2019, with the goal of identifying individuals who report possible EA symptoms (16). The present study followed up on participants of this study, who underwent the clinical interview process. All 32 individuals were contacted between twelve and eighteen months after completion of baseline data collection and invited to repeat completion of the baseline assessments (EDS-21, HASE, CTQ, and BDI-II) the interview process. The repeated use of these questionnaires was partly in order to ensure consistency over both measurement points, and partly as a manipulation check. Therefore, the follow-up EDS score was not used as a threshold below which certain participants might be excluded; all participants from baseline were interviewed if they agreed to follow-up, regardless of follow-up EDS score. Equally, the baseline inclusion criterion of exercising at least 10 hours per week did not apply for this study. This ensured that potential improvements in exercise addiction status were not overlooked due to the exclusion of participants, which would bias the narrative on the time-course of this disorder. Additionally, though assessments addressing past events like childhood trauma can be measured via a baseline screening and should not vary on repetition, we included all baseline screening measures again at follow-up to assess consistency of reporting, and flag possible discrepancies.
It is this follow-up study which we report on in this paper. All assessments were conducted through the online conference platform “Zoom”. Participants received CHF 150 for participating in the interviews.
All participants of the follow-up completed a brief semi-structured interview about their exercising habits and behavior. Participants were asked how their exercise habits developed and whether those habits changed over time. Moreover, participants were asked about their emotional state when exercise was impossible, and the impact of their exercising on their social life and physical health. An additional question inquired about changes in exercise habits since baseline study participation. The interview guide is provided in the Supplementary Materials 1. Exercise Addiction Symptoms – Interview Guide. The interview data were transcribed, coded, and compared to Colledge et al.’s 10 item symptom checklist (Table 1) to assess EA severity (2, 25). Grading spanned from subclinical (0-4 criteria), mild (5-6 criteria), moderate (7-8 criteria) to severe (9-10 criteria). Due to the brief nature of these interviews, no specific analysis framework for qualitative data was employed.
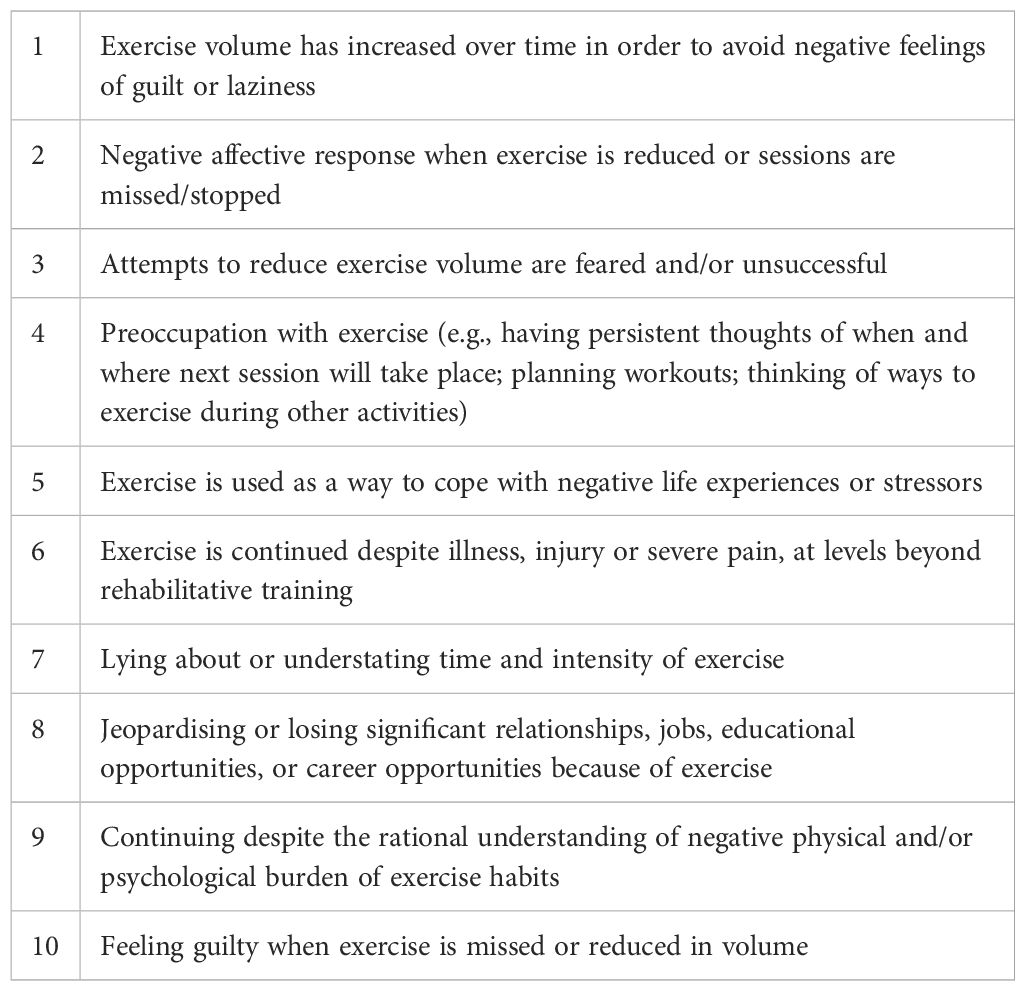
Table 1. Exercise addiction criteria by Colledge et al. used for severity grading (2).
Diagnostic assessments with the SCID-5-CV were repeated for all follow-up participants (23). Participants who had been diagnosed with a personality disorder at baseline again completed the SCID-5-PD. All other participants completed the SAPAS and the SCID-5-PD was only conducted if the cut-off was reached (24). The SAPAS is a validated 8 item screening tool for personality disorders and the cut-off score of 3 correctly identifies the presence of a personality disorder with a sensitivity and specificity of.94 and.85 respectively (24).
Two participants reported a past episode of depression when interviewed at baseline, but did not mention this again at follow-up, a discrepancy likely due to erroneous reporting by participants. In these cases, we have taken the baseline assessment of major depressive disorder incidence and carried it forward.
All data was analyzed using SPSS version 26. No inferential statistics were calculated. Descriptive statistics calculated comprise means (M), standard deviation (SD) and percentages (%) and were employed for age, follow-up time, number of EA criteria, and number of diagnosed mental disorders. In addition, qualitative interview data was selected and summarized to characterize the study sample further.
This study was approved by the responsible ethics committee (Ethikkommission Nordwest und Zentralschweiz) and conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent before inclusion in the study.
All 32 participants of the baseline study were contacted, 19 (59.4%) of which responded and agreed to participate. The mean duration of follow-up was 634.5 (SD=155.8) days. Characteristics of the full sample are provided in detail in the baseline study (16).
The mean age of the sample (n=19) was 32.5 (SD=14.5) years, and 10 participants (52.6%) were female. Table 2 provides an overview of fulfilled EA criteria and exercise volume in the current sample. Table 3 shows the baseline and follow-up values of the screening questionnaires.
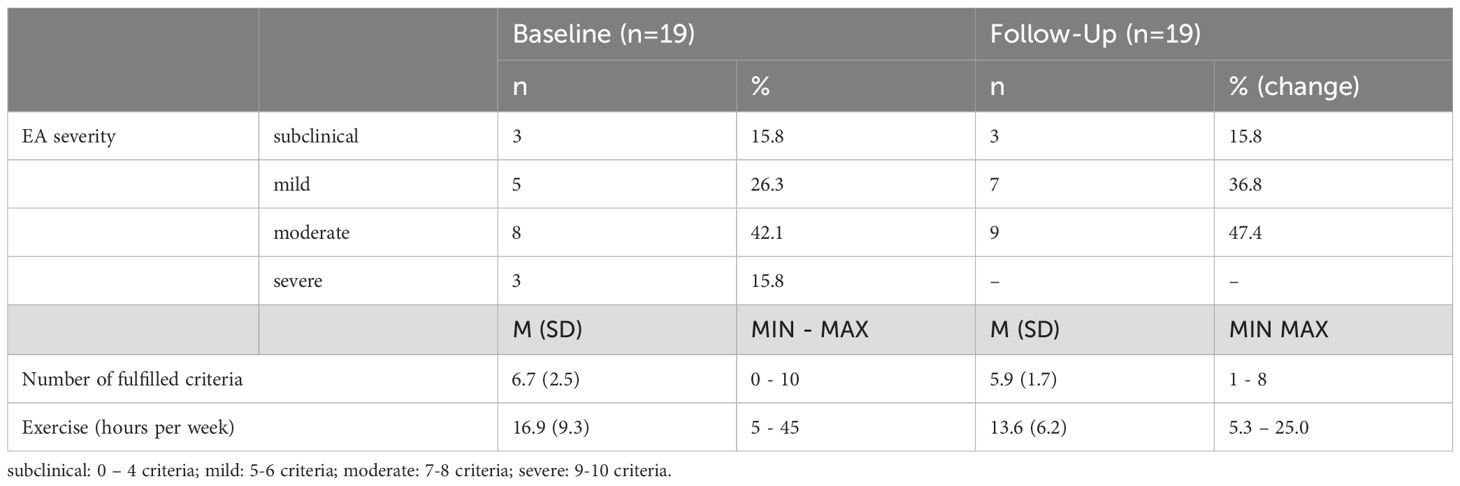
Table 2. Exercise addiction criteria and exercise volume in the sample.
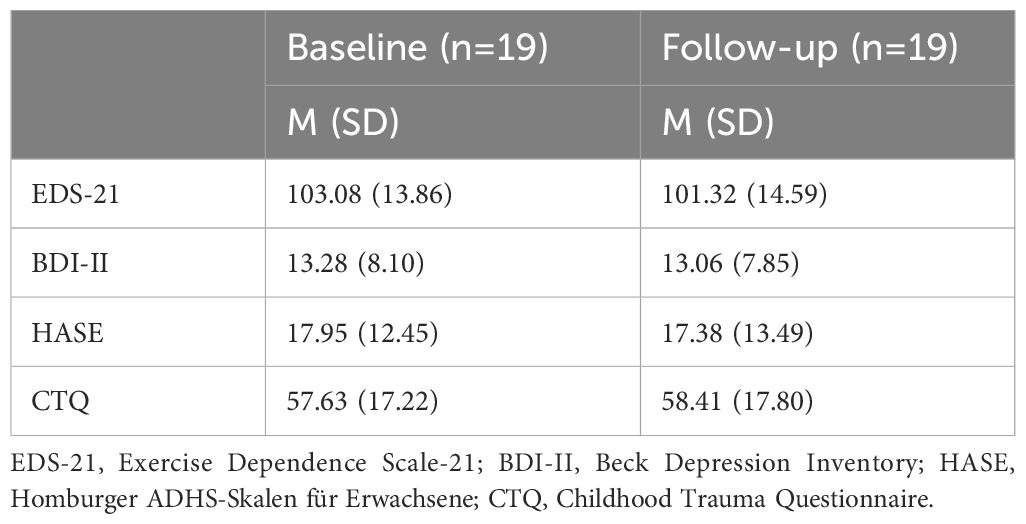
Table 3. Development of screening questionnaire values.
Comparing the severity of EA on a case-by-case basis showed no change in seven (36.8%) participants. Nine (47.4%) participants fulfilled fewer EA criteria compared to baseline and three participants (15.8%) fulfilled more criteria compared to baseline. Figure 1 presents each participants’ EA severity score as a connected baseline and follow-up datapoint.
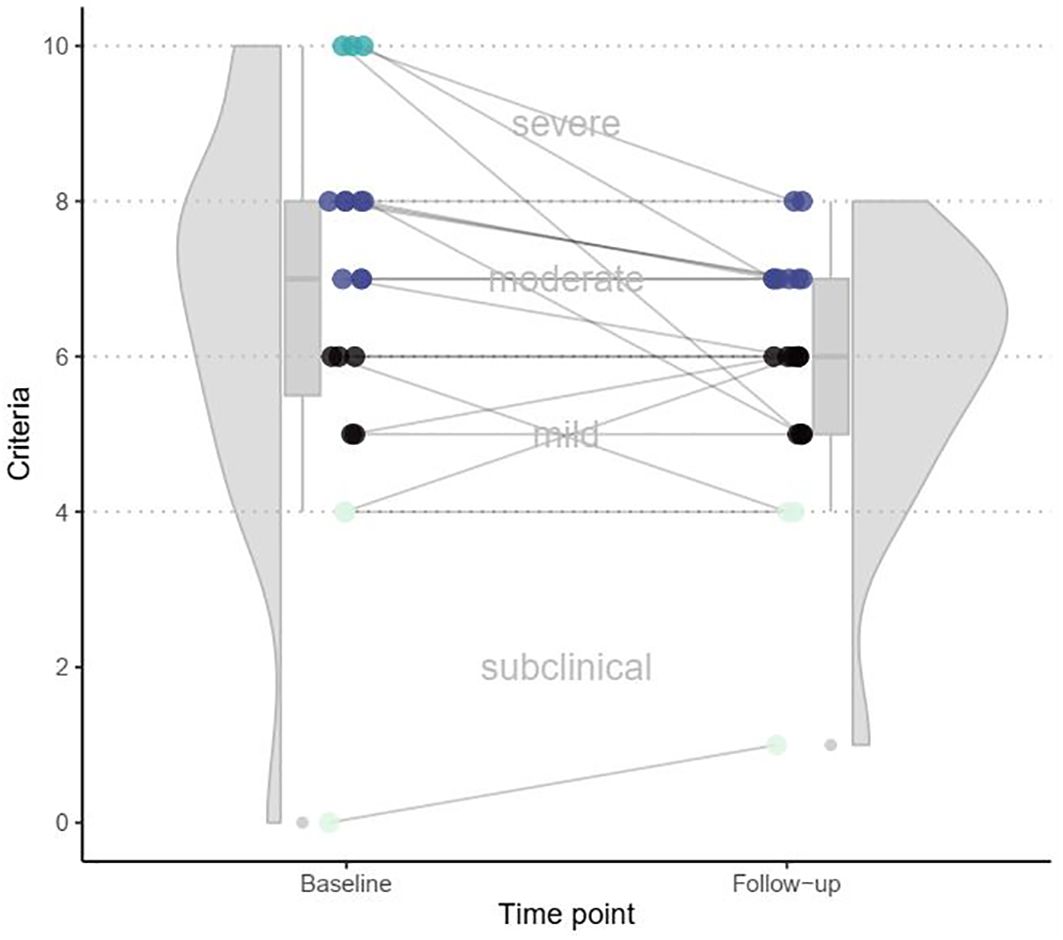
Figure 1. Development of fulfilled exercise addiction criteria over time.
Most participants reported doing multiple sports. The most common were fitness/strength training (n=15), running (n=9), cycling (n=7), and hiking (n=5). Other disciplines included handball, skiing, swimming, volleyball, bouldering, rock climbing, triathlon, yoga, and cross-country skiing. In total, 6 subjects (31.6%) reported having professional ambitions or participating in competitions.
When asked about their feelings in case of missed workout sessions, participants reported feeling tense, irritable, angry, aggressive, out of balance, weak, and in a bad mood. Some participants stated to develop sleeping problems. Participants reported regulating their emotions with exercise and using it to cope with sensory overload, stress, unpleasant situations, and fights/arguments. One participant explicitly stated that exercise gives them the feeling of running away from their problems.
Some participants reported planning their social life around their exercising schedule. Skipping social events to exercise was a repeating theme, with friends and family showing a lack of understanding. One participant reported planning a sabbatical to be able to focus on sports fully, whereas another participant stated to have joined the military with the intention to make exercising/workouts their job.
When asked about physical problems related to their exercising, shoulder pain and inflammation, tendon ruptures, and hip- and knee joint problems were most commonly reported. Participants also commonly reported working around the affected body parts when exercising or not altering their workouts at all. One participant reported suffering from a double disc herniation, which forced them to switch to a more balanced workout regimen. Despite experiencing initial pain from a tendon rupture, another participant reported continuing with their exercising habits, noting that the pain had gradually decreased over time. A male participant reported suffering from a myocardial infarction recently, requiring four operations and multiple stents, forcing him to reduce his workout volume.
Participants were asked whether their exercising habits had changed since the baseline assessment. Most did not report a substantial increase or decrease in their workout volume. However, many participants reported that their gyms had closed because of COVID-19 lockdown regulations, leading to them increasing or picking up endurance sports like cycling or running. One participant reported becoming “more reasonable” and better able to cope in case of missing a workout session. Another participant reported substantially increasing their workout volume during the COVID-19 lockdown. Subsequently, they developed psychological and physical distress, which led to them seek psychiatric counselling and prescription of an antidepressant. This was accompanied by a span of nine months without any physical exercise, until they started exercising again.
Eighteen out of 19 participants fulfilled the criteria for at least one mental disorder. The total number of different mental disorders as identified by the SCID-5-CV and SCID-5-PD in the sample was 75. A comprehensive overview is provided in Table 4.
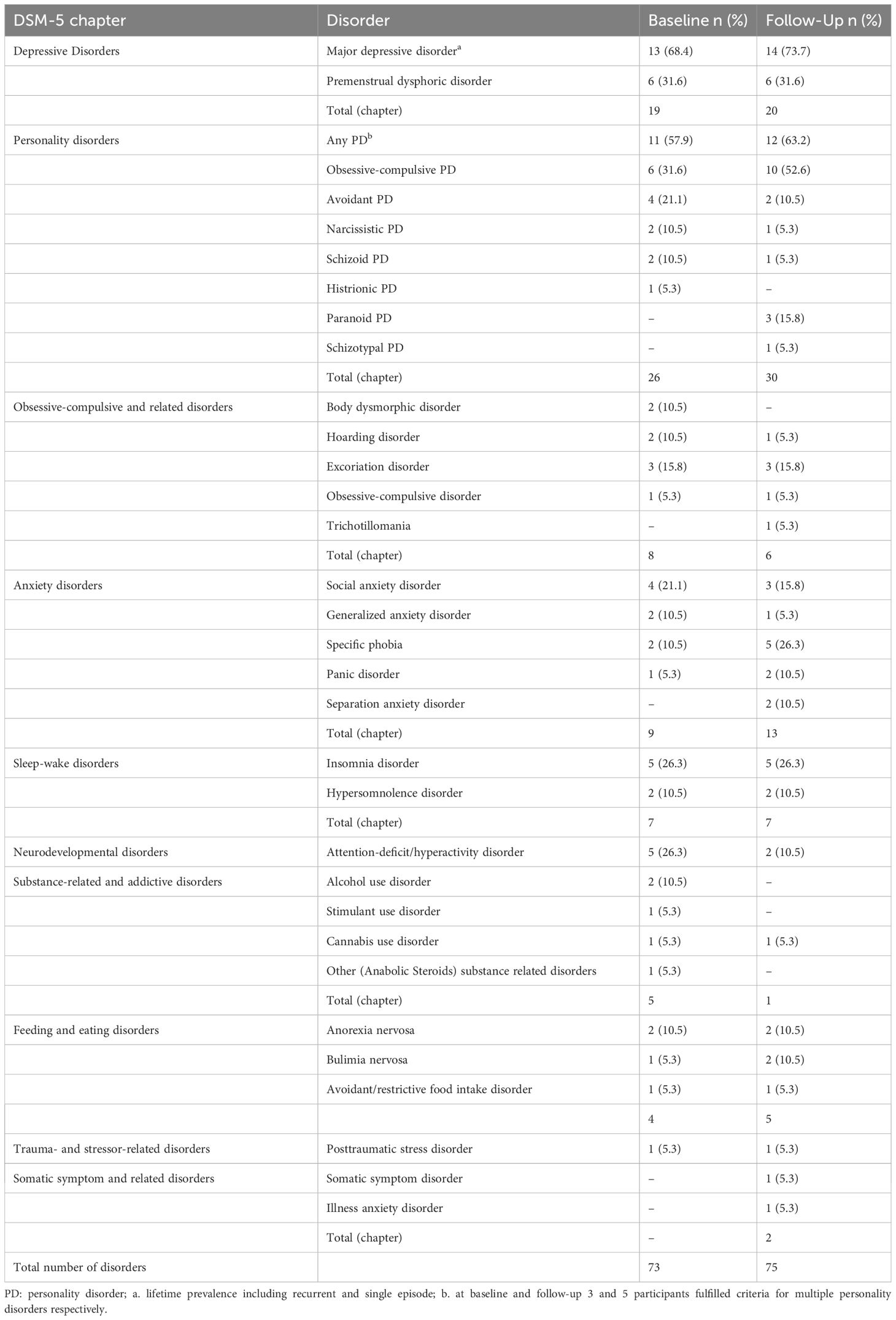
Table 4. Mental disorders in the sample as diagnosed through SCID-5-CV and SCID-5-PD interviews (n=19).
A total of six (31.6%) participants fulfilled the same number of psychiatric disorders at baseline and follow-up. The number of psychiatric disorders increased in seven (36.8%) participants and decreased in six (31.6%) (Table 5).
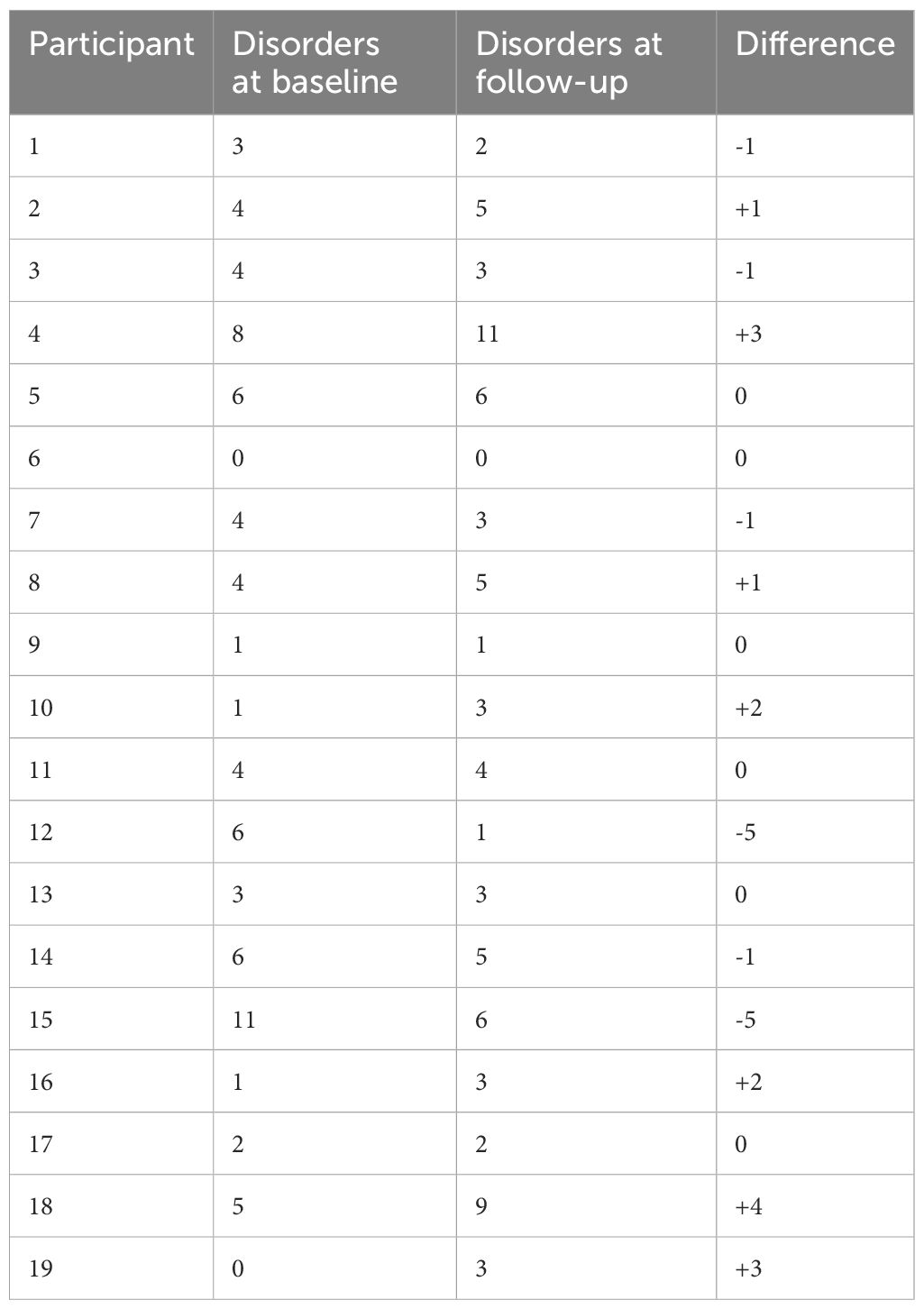
Table 5. Difference in number of psychiatric disorders as diagnosed through SCID-5-CV and SCID-5-PD interviews at baseline and follow-up.
When compared to the followed up sample, participants lost to follow-up on average fulfilled fewer EA criteria at baseline (M=5.8, SD=2.2 versus M=6.7, SD=2.5), had a lower average number of mental disorders (M=2.0, SD=3.1 versus M=3.84, SD=2.8) and spent more hours exercising per week (M=17.7, SD=11.9 versus M=16.9, SD=9.3).
This is the first longitudinal clinical study of exercise addiction. The key finding of this study is that symptoms of EA remain largely stable over an average follow-up time of 1.7 years, adding weight to the increasing evidence that this is not a transient symptom cluster, but a distinct and persistent psychiatric disorder. Furthermore, the psychiatric comorbidities identified in affected individuals also remain broadly unchanged. Although participants in our sample suffered from severe psychological distress, the total number of 75 mental disorders present in a rather small sample may seem excessive. The amount is partly explained by us considering all DSM-5 disorders, including highly prevalent conditions such as a history of depression or insomnia (26).
Exercise addiction, like shopping, sex, or smartphone addiction, has received growing attention in recent years, as a society with increasing leisure time is exposed to these ostensibly harmless pastimes with greater frequency. As noted above, however, none of these phenomena is yet included in the non-substance-related disorder category of the DSM-5. As Potenza writes, this is due to the current lack of high-quality evidence for the characteristics of these potential disorders (27). In the case of EA in particular, it has been noted that current self-report questionnaires tend to lead to prevalence overestimates, and a general muddying of the waters surrounding this issue (28). Our study therefore addresses these methodological weaknesses on two fronts – by providing a detailed clinical picture of individuals reporting symptoms of EA, and a follow-up assessment to understand EA over a longer time frame.
Our results add yet another layer of evidence to the assertion that EA is indeed worthy of the name. Affected individuals report psychological distress caused by their behavior, yet feel unable to stop. The effects of exercise “withdrawal” ranged from feeling irritable and tense to the development of sleeping problems, which participants reported to avoid by organizing their social- and work-life around their workout regimen. Furthermore, exercise was continued despite the presence of physical injuries, which often likely directly resulted from their workout frequency and intensity. These apparent similarities to the behaviors observed in patients with substance use disorders underline the clinical significance of EA, while also providing reference points for clinicians aiming to treat the condition with targeted interventions in the future.
Almost two years later, just over half the sample reported no change or a worsening of symptoms, while 47% showed a reduction in symptoms. However, as shown in Figure 1, large increases or decreases in EA severity remained an exception in the sample. This is the first clinical evidence of the stability and persistence of EA symptoms.
It should be noted that the end of the baseline study and the entirety of the follow-up study took place during the first outbreak and repeated waves of the COVID-19 pandemic. While Switzerland had fairly relaxed regulations for the general public (no restrictions on time spent outside, while respecting social distancing), at numerous times gyms, pools and sporting goods stores were closed, and the practice of team sports was forbidden or limited. If EA were a subclinical, transient phase, one might expect a reduction in exercise-focused activity over this time period – the persistence of symptoms despite COVID-related challenges lends more weight to the claims regarding the severity of EA. In other countries, this time represented a period of significant distress that highlighted the compulsive nature of EA for affected individuals (29).
An important hurdle to overcome in the establishment of diagnostic criteria for EA is the occasionally-made suggestion that EA symptoms are not a distinct disorder, but are a subset of eating disorder symptoms, representing purging behavior. While the majority of the literature now accepts the distinction of primary and instrumental or secondary forms of EA, it would nevertheless change the nature of research on the topic if nearly all cases were observed in individuals with eating disorders (7). In the majority of our sample, this behavior is not explained by the primary goal of weight management or loss; with four diagnoses at baseline and five at follow-up, eating disorders were present in approximately a quarter of our sample. This is in line with other studies reporting instances of EA in the absence of any eating disorder (30). As a reason to exclude EA from the DSM-5, we feel that comorbidity with eating disorders can now be conclusively ignored. While future screening for other psychiatric comorbidities in individuals with EA is advisable, there is no grounds to expect a particularly high prevalence of eating disorders.
With regards to comorbid mental disorders, the most prevalent in our sample are major depressive disorder, and personality disorders, both of which appear in approximately 60% to 70% of the sample at both baseline and follow-up. As reported in an analysis of our original baseline sample, the depressive episodes generally pre-date the onset of EA, lending support to the claim that EA, like other addictive disorders, may be an attempt to self-medicate (31). Exercise is established as a rewarding behavior, and its effectiveness in reducing symptoms of depression matches that of pharmacotherapy (32). It is therefore intuitively plausible that the stability of depressive symptoms in our sample is matched by the stability in (potentially compensatory) EA. Notably, regarding compulsive personality traits, an increase from approximately 30% to 50% of the sample received a diagnosis of obsessive-compulsive personality disorder. This further supports the findings of a recent study, in which obsessive passion significantly predicted the occurrence of EA (33). Weinstein and Szabo also recently argued that EA lies within the obsessive-compulsive spectrum of behavioral addictions (7). In the literature, amongst the numerous synonyms for EA are “obsessive exercise” and “compulsive exercise”. These studies address the symptoms of panic and distress felt by individuals who cannot complete their planned exercise routine, as well as the perceived single-mindedness of pursuing opportunities to exercise (34). It is possible that exercising behavior originates as a way to reduce distress caused by obsessive-compulsive traits, with a negative spiral in some individuals leading to the same problematic symptoms affecting their exercise habits.
This study addresses several weaknesses of previous EA research. First, it provides longitudinal data, therefore allowing inferences about symptom stability over time. Second, it uses gold-standard diagnostic assessments. Third, it utilized in-depth semi-structured interviews rather than relying on measurement tools that have been shown to overestimate EA prevalence and severity. However, it must be noted that the findings are based on a small sample size, with numerous baseline participants lost to follow-up. This limits our results to being purely descriptive and future studies should attempt to employ inferential statistics, to test for the stability of exercise addiction symptoms and mental disorders. Furthermore, since SCID-5 interviews were conducted in an online video-conferencing format, their reliability may have been lowered.
This study is the first longitudinal clinical investigation of EA. The results suggest that EA is a temporally stable, distinct disorder. Furthermore, in this present sample, the numerous psychiatric comorbidities present at baseline also remained stable, suggesting that compromised mental health is a factor in EA. This data should provide a starting point for future clinical investigations of the potential cause-effect relationships between EA and comorbid psychiatric disorders.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study involving humans was approved by Ethikkommission Nordwest- und Zentralschweiz. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MM: Data curation, Investigation, Writing – original draft. AW: Investigation, Writing – review & editing. AS: Methodology, Writing – review & editing. AS: Visualization, Writing – review & editing. UL: Resources, Writing – review & editing. MW: Conceptualization, Supervision, Writing – review & editing. FC: Conceptualization, Funding acquisition, Investigation, Project administration, Writing – original draft.
The author(s) declare that financial support was received for the research and/or publication of this article. Flora Colledge received funding for this research by the Gertrud Thalmann Fonds of the University Psychiatric Clinics Basel.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors AS and FC declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1494309/full#supplementary-material
1. Baekeland F. Exercise deprivation. Sleep and psychological reactions. Arch Gen Psychiatry. (1970) 22:365–9. doi: 10.1001/ARCHPSYC.1970.01740280077014
2. Colledge F, Cody R, Buchner UG, Schmidt A, Pühse U, Gerber M, et al. Excessive exercise—A meta-review. Front Psychiatry. (2020) 11:521572. doi: 10.3389/FPSYT.2020.521572
3. Colledge F, Meyer M. Exercise addiction - status, identification and treatment. Praxis. (2022) 111:317–21. doi: 10.1024/1661-8157/A003875
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders - DSM-5-TR. 5th ed. United States: American Psychiatric Pub (2022).
5. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American psychiatric association (2013).
6. Juwono ID, Szabo A. 100 cases of exercise addiction: more evidence for a widely researched but rarely identified dysfunction. Int J Ment Health Addict. (2021) 19:1799–811. doi: 10.1007/S11469-020-00264-6
7. Weinstein A, Szabo A. Exercise addiction: A narrative overview of research issues. Dialogues Clin Neurosci. (2023) 25:1–13. doi: 10.1080/19585969.2023.2164841
8. Hausenblas HA, Downs DS. How much is too much? The development and validation of the exercise dependence scale. Psychol Health. (2010) 17:387–404. doi: 10.1080/0887044022000004894
9. Müller A, Cook B, Zander H, Herberg A, Müller V, de Zwaan M. Does the German version of the Exercise Dependence Scale measure exercise dependence? Psychol Sport Exerc. (2014) 15:288–92. doi: 10.1016/J.PSYCHSPORT.2013.12.003
10. de Coverley Veale DMW. Exercise dependence. Br J Addict. (1987) 82:735–40. doi: 10.1111/J.1360-0443.1987.TB01539.X
11. Szabo A, Demetrovics Z. Passion and Addiction in Sports and Exercise. 1st ed. New York: Taylor and Francis (2022) p. 1–238 p. doi: 10.4324/9781003173595
12. Zou L, Yang P, Herold F, Liu W, Szabo A, Taylor A, et al. The contribution of BMI, body image inflexibility, and generalized anxiety to symptoms of eating disorders and exercise dependence in exercisers. Int J Ment Health Promotion. (2022) 24:811–23. doi: 10.32604/IJMHP.2022.024862
13. Habelt L, Kemmler G, DeFrancesco M, Spanier B, Henningsen P, Halle M, et al. Why do we climb mountains? An exploration of features of behavioural addiction in mountaineering and the association with stress-related psychiatric disorders. Eur Arch Psychiatry Clin Neurosci. (2022) 1:1–9. doi: 10.1007/S00406-022-01476-8
14. Gunnarsson B, Entezarjou A, Fernández-Aranda F, Jiménez-Murcia S, Kenttä G, Håkansson A. Understanding exercise addiction, psychiatric characteristics and use of anabolic androgenic steroids among recreational athletes – An online survey study. Front Sports Act Living. (2022) 4:903777. doi: 10.3389/FSPOR.2022.903777
15. Colledge F, Buchner U, Schmidt A, Wiesbeck G, Lang U, Pühse U, et al. Individuals at risk of exercise addiction have higher scores for depression, ADHD, and childhood trauma. Front Sports Act Living. (2022) 3:761844. doi: 10.3389/FSPOR.2021.761844
16. Meyer M, Sattler I, Schilling H, Lang UE, Schmidt A, Colledge F, et al. Mental disorders in individuals with exercise addiction—A cross-sectional study. Front Psychiatry. (2021) 12:751550. doi: 10.3389/FPSYT.2021.751550
17. Khantzian EJ. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv Rev Psychiatry. (1997) 4:231–44. doi: 10.3109/10673229709030550
18. Egorov AY, Szabo A. The exercise paradox: An interactional model for a clearer conceptualization of exercise addiction. J Behav Addict. (2013) 2:199–208. doi: 10.1556/JBA.2.2013.4.2
19. Dinardi JS, Egorov AY, Szabo A. The expanded interactional model of exercise addiction. J Behav Addict. (2021) 10:626–31. doi: 10.1556/2006.2021.00061
20. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/ARCHPSYC.1961.01710120031004
21. Rösler M, Retz-Junginger P, Retz W, Stieglitz R-D. Homburger ADHS-Skalen für Erwachsene (HASE). Göttingen: Hogrefe (2008).
22. Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. (1994) 151(8):1132–6. doi: 10.1176/ajp.151.8.1132
23. First MB, Williams JBW, Karg RS, Spitzer RL. User’s guide for the SCID-5-CV Structured Clinical Interview for DSM-5® disorders: Clinical version Vol. 158. Arlington, VA, US: American Psychiatric Publishing, Inc (2016) p. xii, 158–xii p.
24. Moran P, Leese M, Lee T, Walters P, Thornicroft G, Mann A. Standardised Assessment of Personality - Abbreviated Scale (SAPAS): preliminary validation of a brief screen for personality disorder. Br J Psychiatry. (2003) 183:228–32. doi: 10.1192/BJP.183.3.228
25. Colledge F. Sport und Leistung: Gibt es eine Sportsucht? Z für Komplementärmedizin. (2020) 12:14–7. doi: 10.1055/A-1086-1179
26. Morin CM, Jarrin DC. Epidemiology of insomnia: prevalence, course, risk factors, and public health burden. Sleep Med Clin. (2022) 17:173–91. doi: 10.1016/J.JSMC.2022.03.003
27. Potenza MN. Clinical neuropsychiatric considerations regarding nonsubstance or behavioral addictions. Dialogues Clin Neurosci. (2017) 19:281. doi: 10.31887/DCNS.2017.19.3/MPOTENZA
28. Szabo A. Addiction, passion, or confusion? New theoretical insights on exercise addiction research from the case study of a female body builder. Eur J Psychol. (2018) 14:296. doi: 10.5964/EJOP.V14I2.1545
29. Wyszomirska J, Martyniak E, Bąk-Sosnowska M, Piekarska-Bugiel K, Chwalba A, Krzystanek M. Exercise addiction symptoms and mental health during the forced exercises deprivation in greatest COVID-19 pandemic restrictions in Poland. Psychiatr Pol. (2022) 58(1):153–68. doi: 10.12740/PP/ONLINEFIRST/147190
30. Grandi S, Clementi C, Guidi J, Benassi M, Tossani E. Personality characteristics and psychological distress associated with primary exercise dependence: an exploratory study. Psychiatry Res. (2011) 189:270–5. doi: 10.1016/J.PSYCHRES.2011.02.025
31. Tschopp A, Meyer M, Sattler I, Walter M, Colledge F. Exercise addiction and major depressive disorder – clinical diagnoses and longitudinal course. Addict Health. (2023) 15:144–8. doi: 10.34172/AHJ.2023.1404
32. Rethorst CD, Wipfli BM, Landers DM. The antidepressive effects of exercise: a meta-analysis of randomized trials. Sports Med. (2009) 39:491–511. doi: 10.2165/00007256-200939060-00004
33. Kovacsik R, Soós I, de la Vega R, Ruíz-Barquín R, Szabo A. Passion and exercise addiction: Healthier profiles in team than in individual sports. Int J Sport Exerc Psychol. (2018) 18:176–86. doi: 10.1080/1612197X.2018.1486873
Keywords: exercise addiction, excessive exercising, clinical interview, behavioral addiction, compulsive exercising, exercise dependence, longitudinal data, diagnostic assessment
Citation: Meyer M, Wagner A, Schmidt A, Schaub A-C, Lang UE, Walter M and Colledge F (2025) Stability of exercise addiction symptoms and co-occurring mental disorders – a follow-up study. Front. Psychiatry 16:1494309. doi: 10.3389/fpsyt.2025.1494309
Received: 10 September 2024; Accepted: 05 March 2025;
Published: 27 March 2025.
Edited by:
Carlos Roncero, University of Salamanca, SpainReviewed by:
Nadja Walter, Leipzig University, GermanyCopyright © 2025 Meyer, Wagner, Schmidt, Schaub, Lang, Walter and Colledge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Flora Colledge, ZmxvcmEuY29sbGVkZ2VAdW5pbHUuY2g=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.