
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 20 January 2025
Sec. Schizophrenia
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1540153
 Zhen-Juan Qin1†
Zhen-Juan Qin1† Zhan-Ming Shi2†
Zhan-Ming Shi2† Li-Juan Li3†
Li-Juan Li3† Xin Wei1
Xin Wei1 Hui-Lin Hu1Wei Wei1Zhi-Yuan Xie1Hang-Xi Ji2Yu-Hua Wei1*
Hui-Lin Hu1Wei Wei1Zhi-Yuan Xie1Hang-Xi Ji2Yu-Hua Wei1* Wei Zheng4,5*
Wei Zheng4,5*Background: The efficacy and safety of metformin for addressing neurocognitive dysfunction in schizophrenia remain inconclusive. This systematic review evaluates the evidence from randomized controlled trials (RCTs) on the effects of metformin on neurocognitive function in patients with schizophrenia.
Methods: A comprehensive search of Chinese databases (WanFang, Chinese Journal Net) and English databases (PubMed, EMBASE, PsycINFO, and Cochrane Library) was conducted to identify RCTs assessing metformin’s impact on neurocognitive outcomes in schizophrenia.
Results: Four RCTs involving 271 patients with schizophrenia were included. Three RCTs (75%) demonstrated significant improvements in neurocognitive function with metformin compared to controls, as assessed by the MATRICS Consensus Cognitive Battery, Repeatable Battery for the Assessment of Neuropsychological Status, and Mini-Mental State Examination, but not the Brief Assessment of Cognition in Schizophrenia. Two RCTs (50%) evaluated metformin's effects on total psychopathology and found no significant differences between groups. Adverse events were reported in two RCTs, with inconsistent findings on decreased appetite and diarrhea. Other adverse events and discontinuation rates were comparable between groups.
Conclusion: Preliminary evidence suggests that metformin may improve neurocognitive function in schizophrenia. However, further large-scale, double-blind, high quality RCTs are warranted to validate these findings.
Schizophrenia is a chronic and severe psychiatric disorder characterized by positive and negative symptoms, neurocognitive dysfunction, and social dysfunction (1). Despite its relatively low lifetime prevalence of approximately 1% (2, 3), schizophrenia imposes substantial socioeconomic burdens and contributes significantly to disability worldwide (4). Long-term or lifelong administration of antipsychotics (APs), such as olanzapine and aripiprazole, is essential for preventing disease recurrence (5). However, these medications fail to address neurocognitive dysfunction (6) and may even exacerbate it (7, 8). Thus, there is an urgent need for effective therapeutic strategies targeting neurocognitive symptoms.
Guidelines from the European Psychiatric Association (9) recommend managing neurocognitive dysfunction in schizophrenia through pharmacological interventions, psychosocial strategies, and somatic treatments, which include non-invasive brain stimulation techniques such as transcranial direct current stimulation (tDCS) (10) and repetitive transcranial magnetic stimulation (rTMS) (11). However, these interventions provide only modest improvements in neurocognitive performance (9). Neurocognitive symptoms in schizophrenia often persist despite the resolution of positive symptoms, posing a significant therapeutic challenge (12). Therefore, it is urgent to improve neurocognitive function with effective pharmacological agents.
Metformin, a biguanide hypoglycaemic agent commonly prescribed for type 2 diabetes management (6, 13), has garnered attention for its potential neuroprotective effects. It readily crosses the blood-brain barrier and enhances neurocognitive function through anti-inflammatory mechanisms and improved cerebral energy metabolism (14). Concurrently, neuroimaging modalities such as magnetic resonance imaging and positron emission tomography have implicated neuroinflammation and cerebral metabolic stress in neurocognitive impairment (15, 16). Supporting these mechanisms, animal studies have demonstrated that metformin ameliorates clozapine-induced learning deficits (17) and dizocilpine-induced working memory impairments (18). Additionally, a longitudinal cohort study linked metformin use to improved performance in verbal learning, working memory, and executive function (19). However, randomized controlled trials (RCTs) (20–23) investigating metformin for neurocognitive dysfunction in individuals with schizophrenia and comorbid physical disease (e.g., type 2 diabetes) have reported inconsistent findings.
While previous systematic reviews and meta-analyses (6, 24–26) have focused on the efficacy of metformin in addressing antipsychotic-induced dyslipidemia and weight gain, no systematic review of RCTs has evaluated its effects on neurocognitive function in schizophrenia. To understand the current literature on the role of metformin for neurocognitive effects in schizophrenia, and to provide a more comprehensive and robust basis for clinical application, this systematic review systematically examines the neurocognitive effects of metformin in patients with schizophrenia.
A systematic search was conducted in Chinese databases (WanFang and Chinese Journal Net) and English databases (PubMed, Cochrane Library, PsycINFO, and EMBASE) from their inception to August 29, 2024, by three independent authors (ZJQ, ZMS, and LJL). The search terms used in PubMed included: (‘schizophrenia’[MeSH] OR schizophrenic disorder OR schizophrenia OR dementia praecox) AND (‘cognition’[MeSH] OR cognit* OR neurocognit*) AND (‘metformin’[MeSH] OR metformin OR dimethylbiguanidium OR glucophage OR glucovance). Additional articles were identified by manually screening the reference lists of included studies (20–23), relevant reviews (27, 28) and prior meta-analyses (6, 29).
Studies were selected based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (30), following the PICOS framework: Participants (P): adult patients suffering from schizophrenia with or without physical comorbidities, such as type 2 diabetes. Intervention (I) versus Comparison (C): metformin plus treatment as usual (TAU) versus placebo plus TAU or TAU. Outcomes (O): the primary outcome was considered as changes in neurocognitive function assessed using standardized scales (e.g., the Brief Assessment of Cognition in Schizophrenia (BACS) (31), the MATRICS Consensus Cognitive Battery (MCCB) (32), the Mini-Mental State Examination (MMSE) (33) and Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) (34)). Key secondary outcomes were as follows: 1) changes in total psychopathology as measured by standardized scales (e.g., Brief Psychiatric Rating Scale (BPRS) (35) and Positive and Negative Syndrome Scale (PANSS) (36)), 2) adverse events and 3) discontinuation rate. Study design (S): published RCTs examining the neurocognitive effects of metformin in adults with schizophrenia, with or without physical comorbidities were included. RCTs focusing on metformin versus acarbose (37), AP-induced hyperprolactinemia (38), weight gain (39), or metabolic syndrome (40) that did not examine neurocognitive effects of metformin were excluded. Furthermore, Case reports/series, animal trials, non-randomized studies, reviews and meta-analyses were also excluded.
Three investigators (ZJQ, ZMS, and LJL) independently extracted data from each eligible RCT and verified the information. Discrepancies were resolved through discussions with a senior author (WZ). Missing data were requested from the corresponding or first authors via email or phone.
The same three investigators (ZJQ, ZMS, and LJL) independently evaluated the quality of the included studies using both the Cochrane risk of bias tool (41) and the Jadad scale (0–5 points) (42). Studies with a Jadad score of 3 or higher were categorized as ‘high quality’ (43).
Four RCTs conducted between 2019 and 2023 (20–23) were included in this systematic review. The study selection process is illustrated in Figure 1.
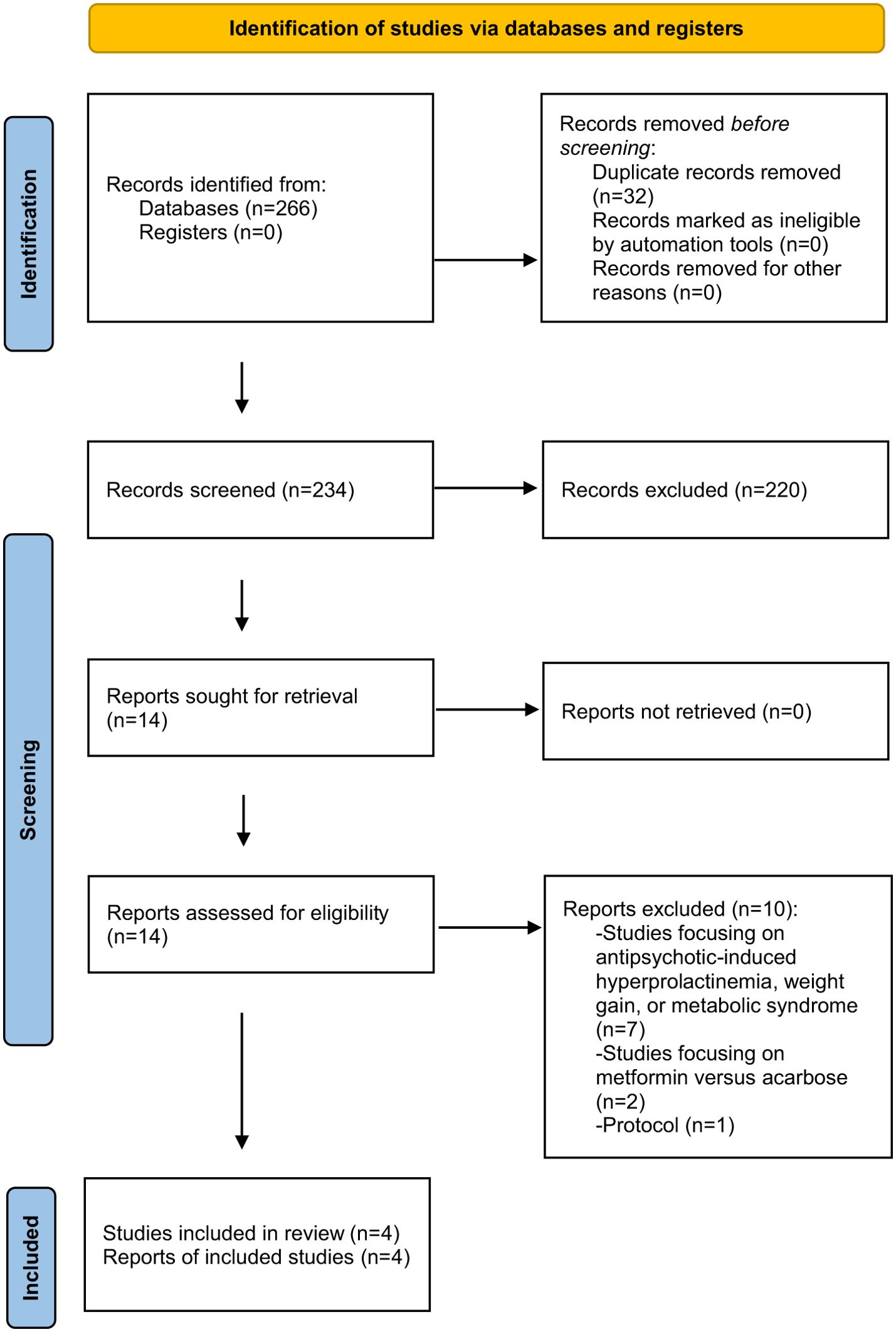
Figure 1. PRISMA flow diagram.
A total of 271 patients were analyzed across the four RCTs, with 152 participants in the metformin group (750–1500 mg/day) and 119 in the control group. The weighted average age of participants was 34.9 years, and 47.2% of them were male. The trial durations ranged from 8 to 24 weeks. Of the included RCTs, all enrolled patients with schizophrenia and comorbid physical illnesses or high risk of Metabolic syndrome. The detailed characteristics of the studies were summarized in Table 1.
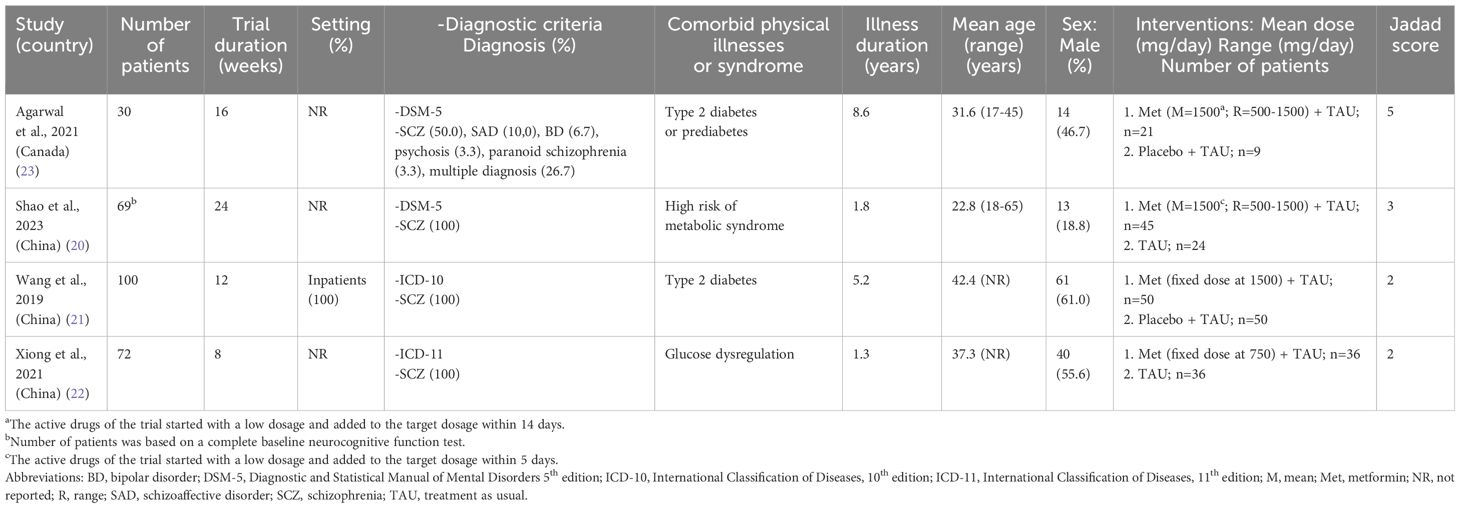
Table 1. Summary of the characteristics of the included studies.
The Jadad scores of the included RCTs ranged from 2 to 5, with two studies (50%) (20, 23) classified as high quality (Jadad score ≥ 3). According to the Cochrane risk of bias assessment (Figure 2), all included studies demonstrated a ‘low risk’ for random sequence generation, addressing incomplete outcome data and selective reporting.
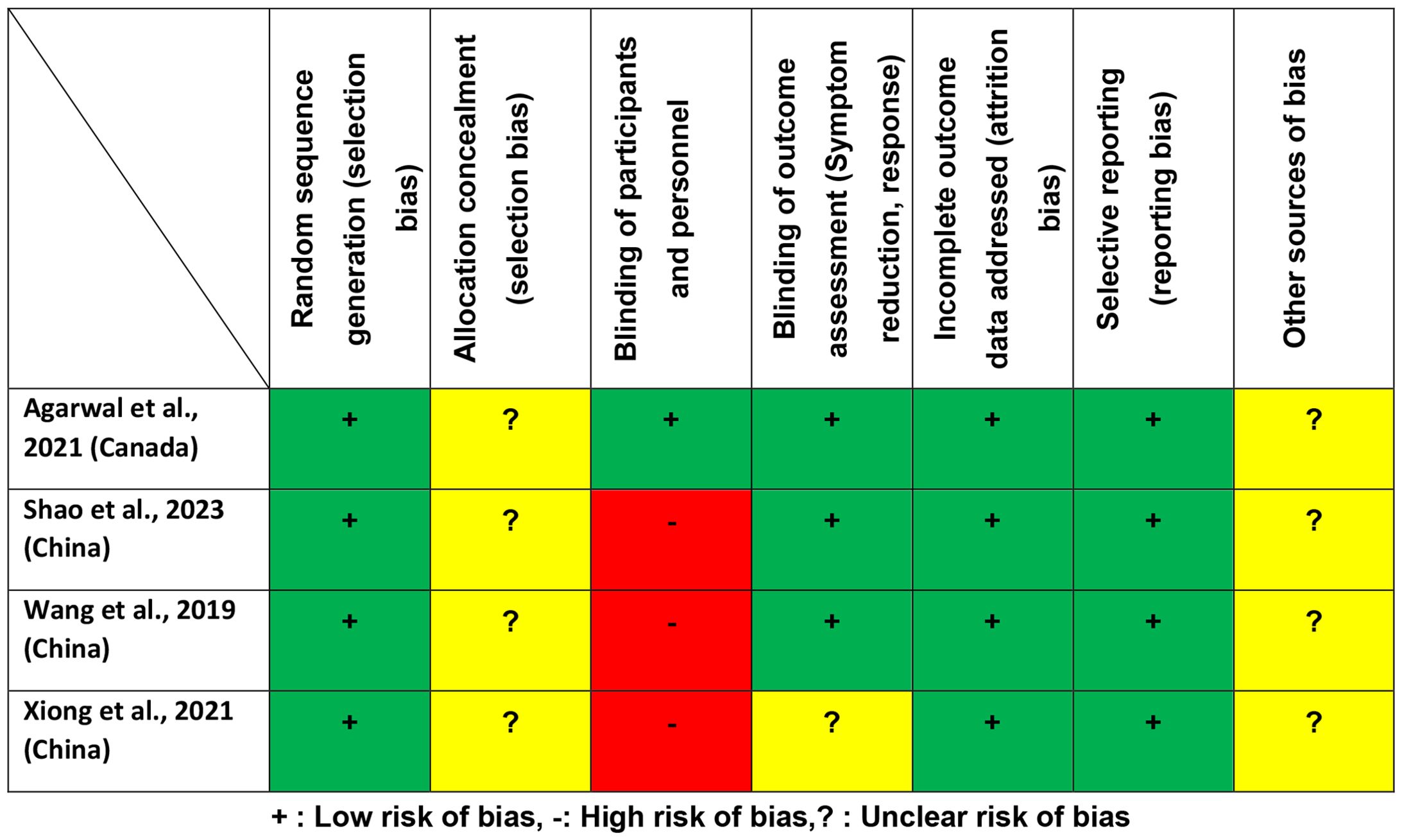
Figure 2. Cochrane risk of bias.
All four RCTs evaluated the neurocognitive effects of metformin in schizophrenia, but their data could not be pooled due to variations in measurement tools. As summarized in Table 2, three RCTs (75%, 3/4) demonstrated significant superiority of metformin over controls in improving neurocognitive function, with outcomes assessed using the MCCB (20), RBANS (21), and MMSE (22). However, one RCT (25%, 1/4) reported no significant differences between groups when using the BACS (23).
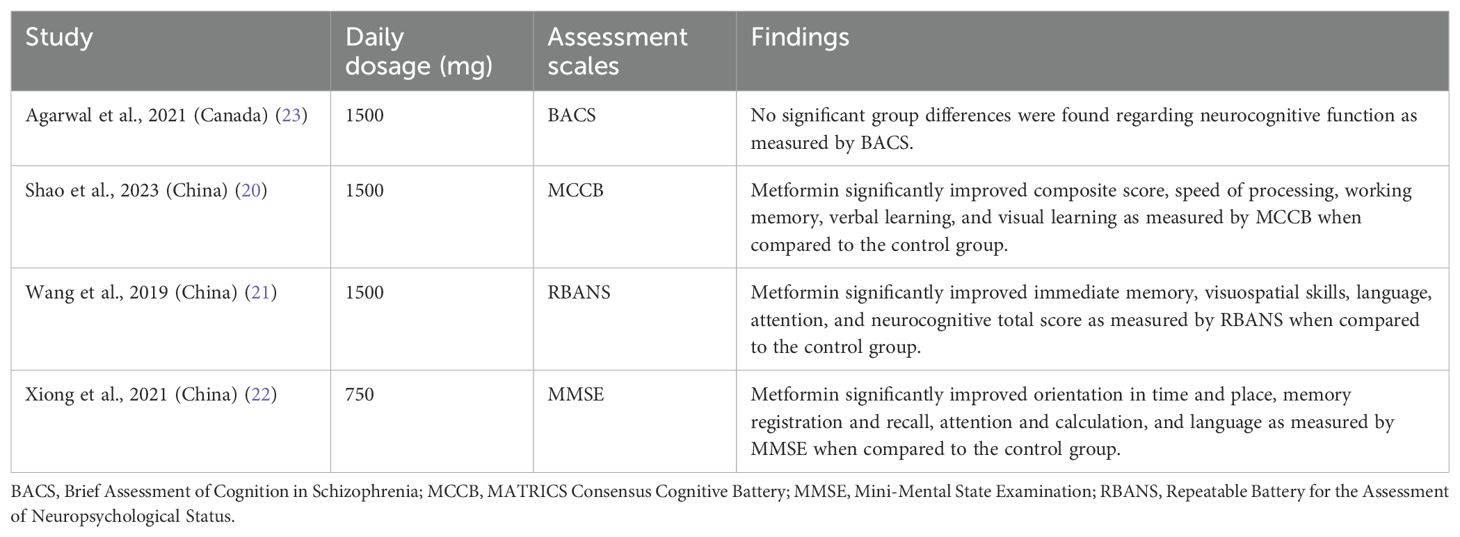
Table 2. Metformin for neurocognitive dysfunction in schizophrenia: neurocognitive function.
Two RCTs (50%, 2/4) (20, 23) examined the effects of adjunctive metformin on total psychopathology in schizophrenia. Both studies reported no significant differences between the metformin and control groups (Table 3).

Table 3. Metformin for neurocognitive dysfunction in schizophrenia: total psychopathology.
Two RCTs (50%, 2/4) (20, 23) reported adverse events, with inconsistent findings regarding decreased appetite and diarrhea. Other adverse events, including nausea, as well as discontinuation rates, were comparable between the metformin and control groups (Supplementary Table S1).
This systematic review, which included four RCTs and 271 participants, is the first to examine the neurocognitive effects of metformin in patients with schizophrenia. The primary findings are as follows: 1) metformin demonstrated significant superiority over controls in improving neurocognitive function as measured by the MCCB, RBANS, and MMSE, but not the BACS; 2) metformin combined with TAU did not significantly improve total psychopathology; and 3) metformin is safe and well-tolerated for enhancing neurocognitive function, though further studies with larger sample sizes are warranted.
In this review, 75% of the included RCTs (20–22) reported that metformin outperformed controls in improving neurocognitive function. However, one study (23) did not observe significant improvements as assessed using the BACS. This inconsistency may stem from the differing assessment tools employed across studies. Evidence suggests that the MCCB has become the gold standard for evaluating neurocognitive impairments in schizophrenia due to its comprehensive scope and strong psychometric properties. Specifically developed for schizophrenia populations, the MCCB has been extensively validated across diverse settings and populations (44). In contrast, the BACS, while more concise, may not fully capture the breadth of neurocognitive deficits as effectively as the MCCB (45). Such inconsistencies have also been reported in previous studies examining neurocognitive function in schizophrenia using different assessment tools. For instance, Hei et al. (46) found that adjunctive sulforaphane significantly improved working memory and verbal learning in schizophrenia, as measured by the MCCB and Hopkins Verbal Learning Test, but showed no significant effects on other measures, including the BACS. Collectively, these findings highlight the importance of employing standardized neurocognitive test batteries, such as MCCB, to ensure consistent and robust assessments. Future research should focus on elucidating the neurocognitive effects of metformin in patients with schizophrenia using standardized tools and well-powered study designs (47).
A recent meta-analysis (6) highlighted that, beyond improving neurocognitive function, metformin also provides benefits for weight management and metabolic syndrome in patients with schizophrenia. Furthermore, several studies have demonstrated metformin's potential to enhance neurocognitive function in other neurological conditions, including Parkinson’s disease (48), Alzheimer’s disease (49), and pediatric brain tumors (50). In the broader context of pharmacological treatments for neurocognitive dysfunction, drugs such as sulforaphane (46), erythropoietin (51), and huperzine A (52) also show promise in improving neurocognitive outcomes. However, no head-to-head studies have compared the neurocognitive effects of metformin with sulforaphane or erythropoietin in adults with schizophrenia. As a result, the relative efficacy of these drugs for neurocognitive enhancement remains unclear.
The mechanisms underlying metformin’s role in improving neurocognitive function in schizophrenia are not yet fully understood. One plausible explanation involves its ability to improve insulin resistance (6, 53, 54), a key pathophysiological factor associated with neurocognitive impairment (55). Insulin resistance has also been linked to weight gain (25), and metformin’s weight-reduction effects may further contribute to neurocognitive improvements. Studies have demonstrated that weight loss is associated with better neurocognitive outcomes, particularly in individuals with obesity or metabolic syndrome (56, 57). Furthermore, metformin’s positive effects on other metabolic indicators, such as lipid levels and glycemic control (25, 58), may also play a role in indirectly enhancing neurocognitive function. Besides its impact on metabolism, metformin decreases inflammation by altering pro-inflammatory cytokines, potentially enhancing neurocognitive function. In an animal study, metformin reduced the levels of pro-inflammatory cytokines like interleukin (IL)-1β, potentially aiding in the enhancement of spatial memory in diabetic animals (59). Furthermore, elevated levels of peripheral cytokines such as IL-1β are found in some patients with schizophrenia and are associated with neurocognitive impairment (60). This multifaceted approach underscores the potential of metformin in the integrated management of neurocognitive impairment in patients with schizophrenia.
Two RCTs reported mixed findings regarding the effects of metformin on decreased appetite and diarrhea compared with controls (20, 23), while both groups exhibited similar rates of discontinuation and other adverse events. Consistent with prior research, daily metformin at recommended dosages (61), is considered notably safe for both short-term and long-term use, with no significant adverse effects reported (6, 20, 24). Gastrointestinal side effects, such as diarrhea and decreased appetite, were the most commonly reported adverse events in this systematic review. These effects, typically observed at the onset of therapy, can be mitigated by lowering the dose, implementing gradual dose titration, or taking the medication with meals (61). Metformin has also demonstrated safety and tolerability in patients with schizophrenia (25), Alzheimer’s disease (49), pediatric brain tumors (50), and bipolar depression (62). However, prolonged use of metformin has been associated with reduced vitamin B12 levels and, in some cases, biochemical B12 deficiency (63, 64). Therefore, it is advisable for patients with schizophrenia receiving metformin to undergo regular monitoring of blood lactate, serum B12, and folate levels (63).
Several limitations of this systematic review should be acknowledged. First, the included RCTs utilized diverse methodologies, including four distinct assessment tools to measure neurocognitive function. This heterogeneity prevented the conduct of a meta-analysis. Importantly, it is different to determine the superiority of metformin over controls in improving a specific neurocognitive function. Second, this review included only four RCTs with a small sample size (n=271, ranging from 30 to 100 participants), necessitating caution in interpreting the findings. Third, the four RCTs focused on the use of metformin in adult patients with schizophrenia, limiting the generalizability of the findings to broader populations. Fourth, this systematic review of metformin for neurocognitive dysfunction in schizophrenia is not registered. Finally, the RCTs included participants with varying conditions, such as schizophrenia combined with glucose metabolism disorder, type 2 diabetes or prediabetes, which may have influenced the outcomes.
Preliminary evidence suggests that metformin may have beneficial effects on neurocognitive function in schizophrenia. However, to validate these findings, future research should focus on conducting large-scale, double-blind, and high quality RCTs.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Z-JQ: Conceptualization, Data curation, Writing – original draft. Z-MS: Conceptualization, Data curation, Writing – original draft. L-JL: Conceptualization, Data curation, Writing – original draft. XW: Funding acquisition, Writing – original draft. H-LH: Validation, Writing – original draft. WW: Validation, Writing – original draft. Z-YX: Formal analysis, Writing – original draft. H-XJ: Formal analysis, Writing – original draft. Y-HW: Conceptualization, Supervision, Writing – review & editing. WZ: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by Guangxi Zhuang Autonomous Region Health Commission Self-Funded Research Project (Z20211399), Guangxi Zhuang Autonomous Region Health Commission Self-Funded Research Project (Z-B20240375), the Science and Technology Program of Guangzhou (2023A03J0839, 2023A03J0436), Science and Technology Planning Project of Liwan District of Guangzhou (202201012), National Clinical Key specialty construction project ((2023) 33), The Natural Science Foundation Program of Guangdong (2023A1515011383, 2024A1515012578), the Science and Technology Program of Guangzhou (202206010077), Guangzhou Municipal Key Discipline in Medicine (2021-2023), Guangzhou Municipal Key Discipline in Medicine (2021-2023), Guangzhou Science and Technology Plan Project (2023A03J0827), Guangzhou Traditional Chinese Medicine and Integrated Traditional Chinese and Western Medicine Science and Technology Project (20232A010014), Guangzhou High-level Clinical Key Specialty, Department of Emergency Medicine of National clinical key specialty, Guangzhou Research-oriented Hospital, Hainan Provincial Natural Science Foundation of China (821QN0987), and Hainan Province Clinical Medical Center (2021). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1540153/full#supplementary-material
Supplementary Table 1 | Metformin for neurocognitive dysfunction in schizophrenia: discontinuation rate and adverse events.
1. Coyle JT. Schizophrenia: basic and clinical. Adv neurobiol. (2017) 15:255–80. doi: 10.1007/978-3-319-57193-5_9
2. Denis F, Millot I, Abello N, Carpentier M, Peteuil A, Soudry-Faure A. Study protocol: a cluster randomized controlled trial to assess the effectiveness of a therapeutic educational program in oral health for persons with schizophrenia. Int J Ment Health sys. (2016) 10:65. doi: 10.1186/s13033-016-0096-0
3. Qi C, Yu Y, Lv H, Ju X, Ji X, Li P, et al. Integrated network pharmacology and molecular docking to explore the mechanisms of ningshen wendan decoction in the treatment of schizophrenia. Alpha Psychiatry. (2024) 25:456–64. doi: 10.5152/alphapsychiatry.2024.241560
4. Huang A, Amos TB, Joshi K, Wang L, Nash A. Understanding healthcare burden and treatment patterns among young adults with schizophrenia. J Med econ. (2018) 21:1026–35. doi: 10.1080/13696998.2018.1500370
5. Emsley R, Chiliza B, Asmal L, Harvey BH. The nature of relapse in schizophrenia. BMC Psychiatry. (2013) 13:50. doi: 10.1186/1471-244x-13-50
6. Battini V, Cirnigliaro G, Leuzzi R, Rissotto E, Mosini G, Benatti B, et al. The potential effect of metformin on cognitive and other symptom dimensions in patients with schizophrenia and antipsychotic-induced weight gain: a systematic review, meta-analysis, and meta-regression. Front Psychiatry. (2023) 14:1215807. doi: 10.3389/fpsyt.2023.1215807
7. Baldez DP, Biazus TB, Rabelo-da-Ponte FD, Nogaro GP, Martins DS, Kunz M, et al. The effect of antipsychotics on the cognitive performance of individuals with psychotic disorders: Network meta-analyses of randomized controlled trials. Neurosci Biobehav Rev. (2021) 126:265–75. doi: 10.1016/j.neubiorev.2021.03.028
8. Kaar SJ, Natesan S, McCutcheon R, Howes OD. Antipsychotics: Mechanisms underlying clinical response and side-effects and novel treatment approaches based on pathophysiology. Neuropharmacology. (2020) 172:107704. doi: 10.1016/j.neuropharm.2019.107704
9. Vita A, Gaebel W, Mucci A, Sachs G, Barlati S, Giordano GM, et al. European Psychiatric Association guidance on treatment of cognitive impairment in schizophrenia. Eur Psychiatry. (2022) 65:e57. doi: 10.1192/j.eurpsy.2022.2315
10. Sun CH, Jiang WL, Cai DB, Wang ZM, Sim K, Ungvari GS, et al. Adjunctive multi-session transcranial direct current stimulation for neurocognitive dysfunction in schizophrenia: A meta-analysis. Asian J Psychiatr. (2021) 66:102887. doi: 10.1016/j.ajp.2021.102887
11. Chou YH, Ton That V, Sundman M. A systematic review and meta-analysis of rTMS effects on cognitive enhancement in mild cognitive impairment and Alzheimer's disease. Neurobiol Aging. (2020) 86:1–10. doi: 10.1016/j.neurobiolaging.2019.08.020
12. Li R, Hei G, Yang Y, Wu R, Zhao J. Research advances in add-on treatment for negative symptoms and cognitive dysfunction in schizophrenia. Zhong nan da xue xue bao Yi xue ban = J Cent South Univ Med Sci. (2020) 45:1457–63. doi: 10.11817/j.issn.1672-7347.2020.190556
13. Lazarus B, Wu A, Shin JI, Sang Y, Alexander GC, Secora A, et al. Association of metformin use with risk of lactic acidosis across the range of kidney function: A community-based cohort study. JAMA Internal Med. (2018) 178:903–10. doi: 10.1001/jamainternmed.2018.0292
14. Ying MA, Maruschak N, Mansur R, Carvalho AF, Cha DS, McIntyre RS. Metformin: repurposing opportunities for cognitive and mood dysfunction. CNS neurol Disord Drug targets. (2014) 13:1836–45. doi: 10.2174/1871527313666141130205514
15. De Felice FG, Lourenco MV. Brain metabolic stress and neuroinflammation at the basis of cognitive impairment in Alzheimer's disease. Front Aging Neurosci. (2015) 7:94. doi: 10.3389/fnagi.2015.00094
16. Lee YJ, Han SB, Nam SY, Oh KW, Hong JT. Inflammation and Alzheimer's disease. Arch pharmacal Res. (2010) 33:1539–56. doi: 10.1007/s12272-010-1006-7
17. Horvath G, Kis G, Kekesi G, Büki A, Adlan LG, Szűcs E, et al. Interaction of clozapine with metformin in a schizophrenia rat model. Sci Rep. (2021) 11:16862. doi: 10.1038/s41598-021-96478-2
18. Wang X, Luo C, Mao XY, Li X, Yin JY, Zhang W, et al. Metformin reverses the schizophrenia-like behaviors induced by MK-801 in rats. Brain Res. (2019) 1719:30–9. doi: 10.1016/j.brainres.2019.05.023
19. Herath PM, Cherbuin N, Eramudugolla R, Anstey KJ. The effect of diabetes medication on cognitive function: evidence from the PATH through life study. BioMed Res Int. (2016) 2016:7208429. doi: 10.1155/2016/7208429
20. Shao T, Huang J, Zhao Y, Wang W, Tian X, Hei G, et al. Metformin improves cognitive impairment in patients with schizophrenia: associated with enhanced functional connectivity of dorsolateral prefrontal cortex. Trans Psychiatry. (2023) 13:315. doi: 10.1038/s41398-023-02616-x
21. Wang C, Shi X, Zhu W, Meng Z, Jiang M, Yi Z. Effects of metformin on cognitive function in schizophrenia patients with diabetes(In Chinese). J Neurosci Ment Health. (2019) 19:52–5. doi: 10.3969/j.issn.1009-6574.2019.01.013
22. Xiong J, Jiang S. Effect of metformin on glucose metabolism disorder in schizophrenia patients induced by clozapine drug evaluation(In chinese). Drug Evaluation. (2021) 18:84–7. doi: 10.19939/j.cnki.1672-2809.2021.02.07
23. Agarwal SM, Panda R, Costa-Dookhan KA, MacKenzie NE, Treen QC, Caravaggio F, et al. Metformin for early comorbid glucose dysregulation and schizophrenia spectrum disorders: a pilot double-blind randomized clinical trial. Trans Psychiatry. (2021) 11:219. doi: 10.1038/s41398-021-01338-2
24. Zheng W, Zhang QE, Cai DB, Yang XH, Ungvari GS, Ng CH, et al. Combination of metformin and lifestyle intervention for antipsychotic-related weight gain: A meta-analysis of randomized controlled trials. Pharmacopsychiatry. (2019) 52:24–31. doi: 10.1055/s-0044-101466
25. Zheng W, Li XB, Tang YL, Xiang YQ, Wang CY, de Leon J. Metformin for weight gain and metabolic abnormalities associated with antipsychotic treatment: meta-analysis of randomized placebo-controlled trials. J Clin Psychopharmacol. (2015) 35:499–509. doi: 10.1097/jcp.0000000000000392
26. Zhuo C, Xu Y, Liu S, Li J, Zheng Q, Gao X, et al. Topiramate and metformin are effective add-on treatments in controlling antipsychotic-induced weight gain: A systematic review and network meta-analysis. Front Pharmacol. (2018) 9:1393. doi: 10.3389/fphar.2018.01393
27. Salvi V, Tripodi B, Cerveri G, Migliarese G, Bertoni L, Nibbio G, et al. Insulin-resistance as a modifiable pathway to cognitive dysfunction in schizophrenia: A systematic review. Schizophr Res. (2024) 274:78–89. doi: 10.1016/j.schres.2024.09.008
28. Whitney Z, Procyshyn RM, Fredrikson DH, Barr AM. Treatment of clozapine-associated weight gain: A systematic review. Eur J Clin Pharmacol. (2015) 71:389–401. doi: 10.1007/s00228-015-1807-1
29. Zhang L, Qi H, Xie YY, Zheng W, Liu XH, Cai DB, et al. Efficacy and safety of adjunctive aripiprazole, metformin, and paeoniae-glycyrrhiza decoction for antipsychotic-induced hyperprolactinemia: A network meta-analysis of randomized controlled trials. Front Psychiatry. (2021) 12:728204. doi: 10.3389/fpsyt.2021.728204
30. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Clinical Res ed). (2009) 339:b2535. doi: 10.1136/bmj.b2535
31. Keefe RS, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The Brief Assessment of Cognition in Schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. (2004) 68:283–97. doi: 10.1016/j.schres.2003.09.011
32. Nuechterlein KH, Barch DM, Gold JM, Goldberg TE, Green MF, Heaton RK. Identification of separable cognitive factors in schizophrenia. Schizophr Res. (2004) 72:29–39. doi: 10.1016/j.schres.2004.09.007
33. Folstein MF, Folstein SE, McHugh PR. Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
34. Gold JM, Queern C, Iannone VN, Buchanan RW. Repeatable battery for the assessment of neuropsychological status as a screening test in schizophrenia, I: sensitivity, reliability, and validity. The American journal of psychiatry (1999) 156(12):1944–50. doi: 10.1176/ajp.156.12.1944
35. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychological reports (1962) 10:799–812. doi: 10.2466/PR0.10.3.799–812
36. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
37. Yuan QH. Analysis of the therapeutic effect of risperidone combined with metfor-min on diabetes mellitus complicated with schizophrenia(In chinese). Diabetes New World. (2022) 25:75–8. doi: 10.16658/j.cnki.1672-4062.2022.17.075
38. Zhu C, Li R, Ju M, Xiao X, Yuan TF, Jin Z, et al. Metformin in the treatment of amisulpride-induced hyperprolactinemia: A clinical trial. Front Mol Neurosci. (2022) 15:892477. doi: 10.3389/fnmol.2022.892477
39. Wu RR, Jin H, Gao K, Twamley EW, Ou JJ, Shao P, et al. Metformin for treatment of antipsychotic-induced amenorrhea and weight gain in women with first-episode schizophrenia: a double-blind, randomized, placebo-controlled study. Am J Psychiatry. (2012) 169:813–21. doi: 10.1176/appi.ajp.2012.11091432
40. Chen CH, Huang MC, Kao CF, Lin SK, Kuo PH, Chiu CC, et al. Effects of adjunctive metformin on metabolic traits in nondiabetic clozapine-treated patients with schizophrenia and the effect of metformin discontinuation on body weight: a 24-week, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. (2013) 74:e424–30. doi: 10.4088/JCP.12m08186
41. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ (Clinical Res ed). (2011) 343:d5928. doi: 10.1136/bmj.d5928
42. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clin trials. (1996) 17:1–12. doi: 10.1016/0197-2456(95)00134-4
43. Linde K, Clausius N, Ramirez G, Melchart D, Eitel F, Hedges LV, et al. Are the clinical effects of homoeopathy placebo effects? A meta-anal placebo-control trials. (1997) 350:834–43. doi: 10.1016/s0140-6736(97)02293-9
44. Jędrasik-Styła M, Ciołkiewicz A, Styła R, Linke M, Parnowska D, Gruszka A, et al. The polish academic version of the MATRICS consensus cognitive battery (MCCB): evaluation of psychometric properties. Psychiatr quarter. (2015) 86:435–47. doi: 10.1007/s11126-015-9343-9
45. Kaneda Y, Ohmori T, Okahisa Y, Sumiyoshi T, Pu S, Ueoka Y, et al. Measurement and Treatment Research toImprove Cognition in Schizophrenia Consensus Cognitive Battery: validation of the Japanese version. Psychiatry Clin Neurosci. (2013) 67:182–8. doi: 10.1111/pcn.12029
46. Hei G, Smith RC, Li R, Ou J, Song X, Zheng Y, et al. Sulforaphane effects on cognition and symptoms in first and early episode schizophrenia: A randomized double-blind trial. Schizophr Bull Open. (2022) 3:sgac024. doi: 10.1093/schizbullopen/sgac024
47. Marder SR, Fenton W. Measurement and Treatment Research to Improve Cognition in Schizophrenia: NIMH MATRICS initiative to support the development of agents for improving cognition in schizophrenia. Schizophr Res. (2004) 72:5–9. doi: 10.1016/j.schres.2004.09.010
48. Ryu YK, Park HY, Go J, Choi DH, Kim YH, Hwang JH, et al. Metformin inhibits the development of L-DOPA-induced dyskinesia in a murine model of Parkinson’s disease. Mol Neurobiol. (2018) 55:5715–26. doi: 10.1007/s12035-017-0752-7
49. Luchsinger JA, Perez T, Chang H, Mehta P, Steffener J, Pradabhan G, et al. Metformin in amnestic mild cognitive impairment: results of a pilot randomized placebo controlled clinical trial. J Alzheimer's disease: JAD. (2016) 51:501–14. doi: 10.3233/jad-150493
50. Ayoub R, Ruddy RM, Cox E, Oyefiade A, Derkach D, Laughlin S, et al. Assessment of cognitive and neural recovery in survivors of pediatric brain tumors in a pilot clinical trial using metformin. Nat Med. (2020) 26:1285–94. doi: 10.1038/s41591-020-0985-2
51. Li XB, Zheng W, Ning YP, Cai DB, Yang XH, Ungvari GS, et al. Erythropoietin for cognitive deficits associated with schizophrenia, bipolar disorder, and major depression: A systematic review. Pharmacopsychiatry. (2018) 51:100–4. doi: 10.1055/s-0043-114670
52. Zheng W, Xiang YQ, Li XB, Ungvari GS, Chiu HF, Sun F, et al. Adjunctive huperzine A for cognitive deficits in schizophrenia: a systematic review and meta-analysis. Hum psychopharmacol. (2016) 31:286–95. doi: 10.1002/hup.2537
53. Malin SK, Stewart NR, Ude AA, Alderman BL. Brain insulin resistance and cognitive function: influence of exercise. J Appl Physiol (Bethesda Md: 1985). (2022) 133:1368–80. doi: 10.1152/japplphysiol.00375.2022
54. Ruegsegger GN, Vanderboom PM, Dasari S, Klaus KA, Kabiraj P, McCarthy CB, et al. Exercise and metformin counteract altered mitochondrial function in the insulin-resistant brain. JCI Insight. (2019) 4(18):e130681. doi: 10.1172/jci.insight.130681
55. Agarwal SM, Kowalchuk C, Castellani L, Costa-Dookhan KA, Caravaggio F, Asgariroozbehani R, et al. Brain insulin action: Implications for the treatment of schizophrenia. Neuropharmacology. (2020) 168:107655. doi: 10.1016/j.neuropharm.2019.05.032
56. Raman J, Hay P, Tchanturia K, Smith E. A randomised controlled trial of manualized cognitive remediation therapy in adult obesity. Appetite. (2018) 123:269–79. doi: 10.1016/j.appet.2017.12.023
57. Hartman SJ, Nelson SH, Marinac CR, Natarajan L, Parker BA, Patterson RE. The effects of weight loss and metformin on cognition among breast cancer survivors: Evidence from the Reach for Health study. Psycho-oncology. (2019) 28:1640–6. doi: 10.1002/pon.5129
58. Jiang WL, Cai DB, Yin F, Zhang L, Zhao XW, He J, et al. Adjunctive metformin for antipsychotic-induced dyslipidemia: a meta-analysis of randomized, double-blind, placebo-controlled trials. Trans Psychiatry. (2020) 10:117. doi: 10.1038/s41398-020-0785-y
59. Oliveira WH, Nunes AK, França ME, Santos LA, Lós DB, Rocha SW, et al. Effects of metformin on inflammation and short-term memory in streptozotocin-induced diabetic mice. Brain Res. (2016) 1644:149–60. doi: 10.1016/j.brainres.2016.05.013
60. Fillman SG, Weickert TW, Lenroot RK, Catts SV, Bruggemann JM, Catts VS, et al. Elevated peripheral cytokines characterize a subgroup of people with schizophrenia displaying poor verbal fluency and reduced Broca’s area volume. Mol Psychiatry. (2016) 21:1090–8. doi: 10.1038/mp.2015.90
61. Fitzgerald I, O'Connell J, Keating D, Hynes C, McWilliams S, Crowley EK. Metformin in the management of antipsychotic-induced weight gain in adults with psychosis: development of the first evidence-based guideline using GRADE methodology. Evidence-Based Ment Health. (2022) 25:15–22. doi: 10.1136/ebmental-2021-300291
62. Calkin CV, Chengappa KNR, Cairns K, Cookey J, Gannon J, Alda M, et al. Treating insulin resistance with metformin as a strategy to improve clinical outcomes in treatment-resistant bipolar depression (the TRIO-BD study): A randomized, quadruple-masked, placebo-controlled clinical trial. J Clin Psychiatry. (2022) 83(2):21m14022. doi: 10.4088/JCP.21m14022
63. Andrade C. Use of metformin for cardiometabolic risks in psychiatric practice: need-to-know safety issues. J Clin Psychiatry. (2016) 77:e1491–e4. doi: 10.4088/JCP.16f11263
Keywords: metformin, schizophrenia, neurocognitive dysfunction, systematic review, efficacy
Citation: Qin Z-J, Shi Z-M, Li L-J, Wei X, Hu H-L, Wei W, Xie Z-Y, Ji H-X, Wei Y-H and Zheng W (2025) Metformin for neurocognitive dysfunction in schizophrenia: a systematic review. Front. Psychiatry 15:1540153. doi: 10.3389/fpsyt.2024.1540153
Received: 05 December 2024; Accepted: 24 December 2024;
Published: 20 January 2025.
Edited by:
Tianhong Zhang, Shanghai Jiao Tong University, ChinaReviewed by:
Lei Xia, Chaohu Hospital of Anhui Medical University, ChinaCopyright © 2025 Qin, Shi, Li, Wei, Hu, Wei, Xie, Ji, Wei and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu-Hua Wei, MjcyNjIyNzgyQHFxLmNvbQ==; Wei Zheng, emhlbmd3ZWkwNzAyQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.