 Yaru Guo
Yaru Guo Xiaojian Yin
Xiaojian Yin Jianyi Xu3
Jianyi Xu3 Feng Zhang
Feng Zhang Yuan Liu
Yuan Liu- 1Key Laboratory of Adolescent Health Assessment and Exercise Intervention, Ministry of Education, College of Physical Education & Health, East China Normal University, Shanghai, China
- 2College of Economics and Management, Shanghai Institute of Technology, Shanghai, China
- 3Physical Education Department, Xiamen Shuangshi Middle School of Fujian, Xiamen, China
- 4Physical Education Department, Guangxi Vocational Normal University, Guangxi, China
- 5Physical Education College, Shanghai University, Shanghai, China
Background: The objective of this study was to explore the relationship between sedentary behavior and non-suicidal self-injury (NSSI), and to provide a theoretical basis for preventing and reducing the occurrence of NSSI behavior and the development of intervention measures.
Methods: Between September and December 2021, a sedentary behavior and NSSI survey was administered to 10327 Chinese adolescents aged 12–17 who had been randomly selected using the stratified cluster random sampling method. The results were analyzed using the chi-square test and logistic regression analysis to explore the relationship between sedentary behavior and NSSI in this population.
Results: The study found an overall NSSI detection rate among the participants of 25.1%, with occasional NSSI and frequent NSSI detection rates of 11.0% and 14.1%, respectively. The NSSI detection rate is higher in girls than in boys. After controlling for related influencing factors, the NSSI detection rates among adolescents with sedentary behavior duration ≥8 hours and screen time ≥2 hours were 1.393(β= 0.332, P <0.01) and 1.569(β= 0.451, P <0.01) times higher than those with sedentary behavior duration <8 hours and screen time <2 hours, respectively.
Conclusion: Sedentary behavior, especially that related to screen time is closely related to the occurrence of NSSI in adolescents. To reduce the occurrence of NSSI, we should therefore pay attention to the harmful effects of sedentary behavior on the physical and mental health of teenagers, take corresponding measures to limit sedentary behavior and screen time, and guide teenagers to use electronic devices correctly.
1 Introduction
Non-suicidal self-injury (NSSI) is a significant predictor of suicidal ideation and behavior among adolescents. With the increasing frequency and severity of adolescent NSSI behavior, the risk of suicidal ideation and attempted suicide will increase (1). Adolescent NSSI behavior has become a public health problems that seriously endanger the physical and mental health of teenagers. In China, the social and cultural factors such as academic pressure, the one-child policy's legacy, and the rapid societal changes contribute to the unique context in which NSSI behaviors may emerge and persist. The severity of NSSI is underscored by its association with long-term mental health issues and the need for immediate intervention.
Studies have reported that the global detection rate of NSSI behavior among adolescents is 17.2% (2), and the incidence of NSSI behavior among adolescents in China is also concerning, with a detection rate that ranges from 11% to 23%, and shows a significant growth trend (3). The high incidence, recurrence, and serious clinical risks of NSSI behavior have prompted many psychologists and neurologists to explore its related influencing factors and occurrence mechanisms. Research has found that NSSI behavior may be caused by the combined effects of various influencing factors, including demographic and sociological, psychological, behavioral, and neurobiological factors (4–6). However, different studies report significant differences in influencing factors, and the intervention programs that target the known risk factors generally have modest effects. There is therefore a need for studies to explore other risk factors for NSSI behavior to generate new ideas and serve as references for its prevention and intervention.
The occurrence and development of chronic diseases such as obesity, cardiovascular disease, bone loss, and psychological diseases such as depression, anxiety, and suicidal behavior in adolescents have been associated with sedentary behavior and screen time (7–9). Sedentary behavior patterns undergo significant changes during adolescence and have a serious and negative impact on the physical and mental health of teenagers, but the relationship between sedentary behavior and adolescent NSSI behavior has not yet received sufficient domestic and international research attention. Relevant investigations report that the global average daily sedentary behavior duration of children and adolescents is more than eight hours (10–12). Studies have confirmed that even if the level of physical activity reaches the recommended amount, too much time spent sitting will increase all-cause mortality, and the health risks of sedentary behavior are independent of physical activity (13). The high incidences of excessive sedentary behavior and NSSI among adolescents represent two major public health problems worldwide. At present, the domestic research on the NSSI behavior of adolescents is focused on its epidemiology. Additionally, existing research abroad has only investigated the relationship between NSSI behavior and sedentary behavior involving screen time. However, an independent relationship between the two has not yet been confirmed. Research on the impact of sedentary behavior on NSSI behavior is even more scarce.
This study intends to contribute to this gap in our knowledge by exploring the dose–effect relationship between sedentary behavior and NSSI behavior and identifying the influence of sedentary behavior—especially screen time—on NSSI behavior. From the perspective of physical activity, it provides a relevant theoretical basis for preventing, reducing, and intervening with in the occurrence of NSSI among adolescents as well as further improving the physical and mental health of teenagers in China. By focusing on Chinese adolescents, this study addresses a significant and growing public health concern within a population that represents a substantial proportion of the global youth demographic.
2 Materials and methods
2.1 Study design and data source
The sample size for this study was determined using the epidemiological survey formula: N=deff u2p(1–p)/δ2, which comprehensively considered the design effect (deff = 0.8), the Z-score corresponding to a significance level of α=0.05 (u = 1.96), the expected detection rate (p = 20%), and the allowable error (δ = 0.10p) (2, 14, 15). According to this calculation, each age group required 1,229 individuals, totaling 7,374 individuals across six age groups. To compensate for an expected non-response rate of 10%, the final sample size was determined to be 8,193 individuals. After excluding invalid questionnaires and missing data, a total of 10,327 participants were recruited, with a recovery rate of 95.41%, meeting the sample size requirements.
From September to December 2021, we conducted a field survey and test in five cities in China: Shanghai, Kunming, Urumqi, Suzhou, and Changsha. In each region, we applied a stratified cluster random sampling method to select one to two junior high or high schools based on their geographical distribution and type. Within these schools, we randomly selected natural classes and then chose approximately 180 male and female students aged 12–17 from each age group, ensuring representation across different demographics. This process resulted in a total of 10,327 adolescents (5231 males and 5096 females) to participate in the study (Figure 1). The study was approved in advance by the Human Subject Protection Committee of East China Normal University (approval number: HR319-2021), and student participants and their parents provided informed consent.
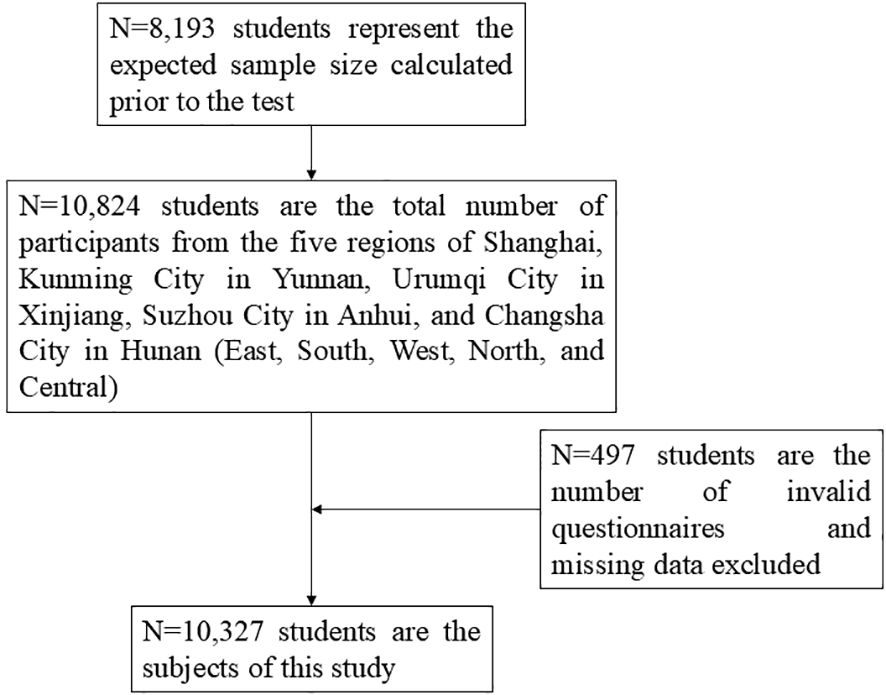
Figure 1. Flowchart of participant involvement.
2.2 Methods
2.2.1 Sedentary behavior and screen time questionnaire
The sedentary behavior of participants was evaluated by administering the ‘Evaluation of physical activity level of children and adolescents aged 7–18 years old’ questionnaire (16), which asks participants about their activity levels over the past week. This includes questions on sedentary behavior items (video, traffic, social and other categories), days of participation, average duration of each activity, etc. This measure has been evaluated and tested by many professionals in the fields of children’s health, psychology, and sports. In order to assess the reliability of the questionnaire, we administered the survey to the same group of participants twice over a two-week period. The test-retest reliability coefficient was calculated to be 0.606, indicating a moderate degree of consistency in the participants’ responses between the two tests. This result is considered acceptable in social science research as it reflects the consistency and stability of the questionnaire in measuring sedentary behavior. The correlation between the sedentary behavior part of the questionnaire and the sedentary behavior duration measured by the three-axis accelerometer was 0.689, proving that it has good validity. Studies from various countries indicate that the average daily sedentary behavior duration for children and adolescents is about eight hours (9, 17, 18); therefore, this study used an average daily sedentary behavior duration of 8 hours as the cutoff point, with those participants spending ≥8 hours/day sitting considered the high sedentary behavior group, and those sitting <8 hours/day the low sedentary behavior group. An average daily screen time duration of two hours was used as the cutoff point, with those using screens for ≥2 hours/day categorized as the high screen time group and those with <2 hours/day of screen time as the low screen time group (16).
2.2.2 Non-suicidal self-injury behavior assessment questionnaire
This study investigated participants’ engagement in NSSI behavior within the past year. This was evaluated using the measure “Adolescent NSSI Behavior Assessment Questionnaire” (19), which was compiled by Wan Yuhui ‘s team. The Cronbach’s α coefficient of the questionnaire was 0.921, the retest reliability was 0.843, and the correlation coefficient of criterion validity was 0.859, indicating that the questionnaire had high credibility and stability. It can be used as an evaluation tool to assess NSSI behavior in adolescents. According to the form and frequency of self-injury behavior, participants with a frequency of NSSI behavior of more than five times in the past year were categorized as the ‘frequent NSSI behavior group’, those engaging one-to-four times were designated the ‘occasional NSSI behavior group’, and those with zero occurrences of NSSI behavior formed the ‘no NSSI behavior group’.
2.3 Quality control
The team of investigators administering the surveys comprised teachers and graduate students who had passed the training and assessment. They were divided into different groups to visit schools in each province at the same time. Before administering the questionnaire, the investigators explained the purpose, significance, and requirements of the study to the participants using the guidance language prepared in advance. Any participant questions or issues were addressed by the investigators. Participants used an anonymous number to fill out the questionnaire. The questionnaire was distributed and recovered immediately after completion. When questionnaires were collected, investigators checked they had been filled in accurately, and participants were asked to complete any wrong or missing items in time to ensure the survey’s validity.
2.4 Statistical methods
SPSS 25.0 software (IBM, NY, USA) was utilized to conduct the statistical analyses. Missing data were addressed using multiple imputation methods to ensure the robustness of the research findings. Descriptive analyses were performed on the static behavior of adolescents and the basic characteristics of NSSI. Chi-square tests were performed to compare the detection rates of NSSI for different durations of sedentary behavior and screen time. For the binary logistic regression analysis to explore the impact of sedentary behavior on NSSI among adolescents. The presence or absence of NSSI was the dependent variable (yes = 1, no = 0), and the different durations of sedentary behavior and screen time were the independent variables. Potential confounding factors were controlled for, such as school stage, gender, family type, sleep compliance and study time (Supplementary Tables S1–S3), with daily sedentary behavior duration < 8 hours and daily screen time < 2 hours as the reference. P<0.05 was considered statistically significant.
3 Research results
3.1 Basic characteristics of adolescents’ sedentary behavior
As seen in Table 1 and Figure 2, the rate of adolescents’ daily sedentary behavior duration ≥8h shows an increasing trend with age, from 65.9% at the age of 12 to 89.4% at the age of 17. Additionally, there was a significant difference in the prevalence of daily sedentary behavior duration ≥8 hours among adolescents of different ages (P < 0.01). Sedentary behavior duration among boys increased from 66.1% at the age of 12 to 89.8% at the age of 17; in girls, it increased from 65.7% at the age of 12 to 89.0% at the age of 17. The overall detection rate of girls’ daily sedentary behavior duration ≥8 hours was 78.3%, higher than boys’ 77.0%.
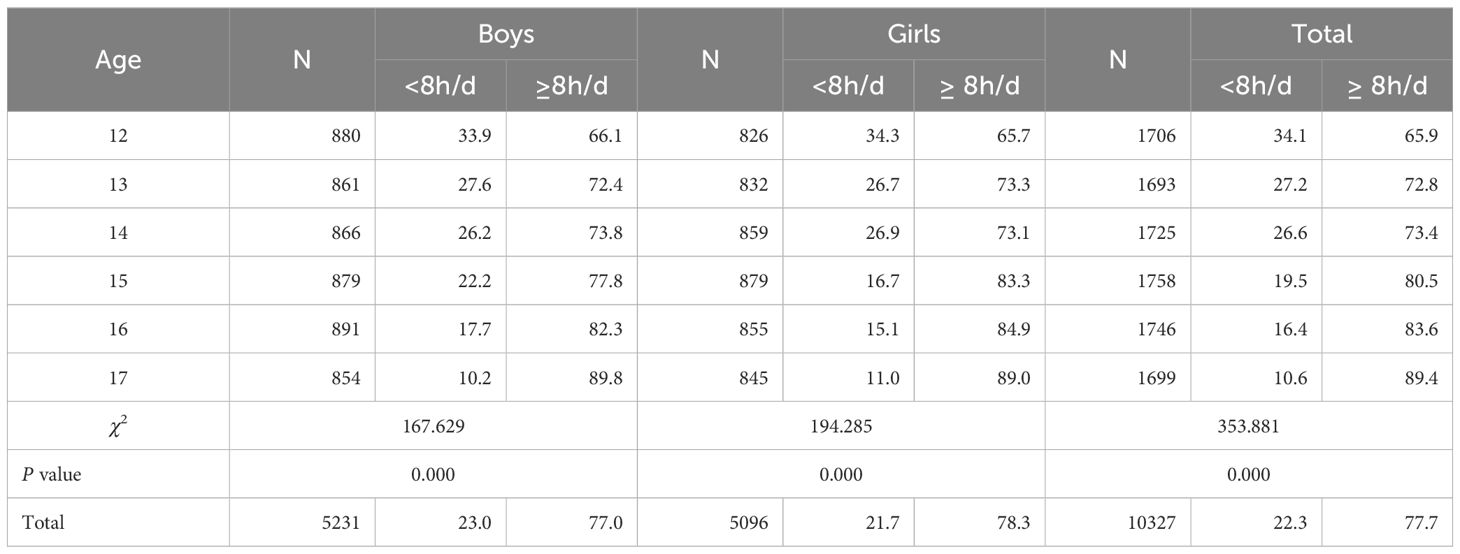
Table 1. 12-17 years old adolescent’ detection rates in different duration groups of sedentary behaviors (%).
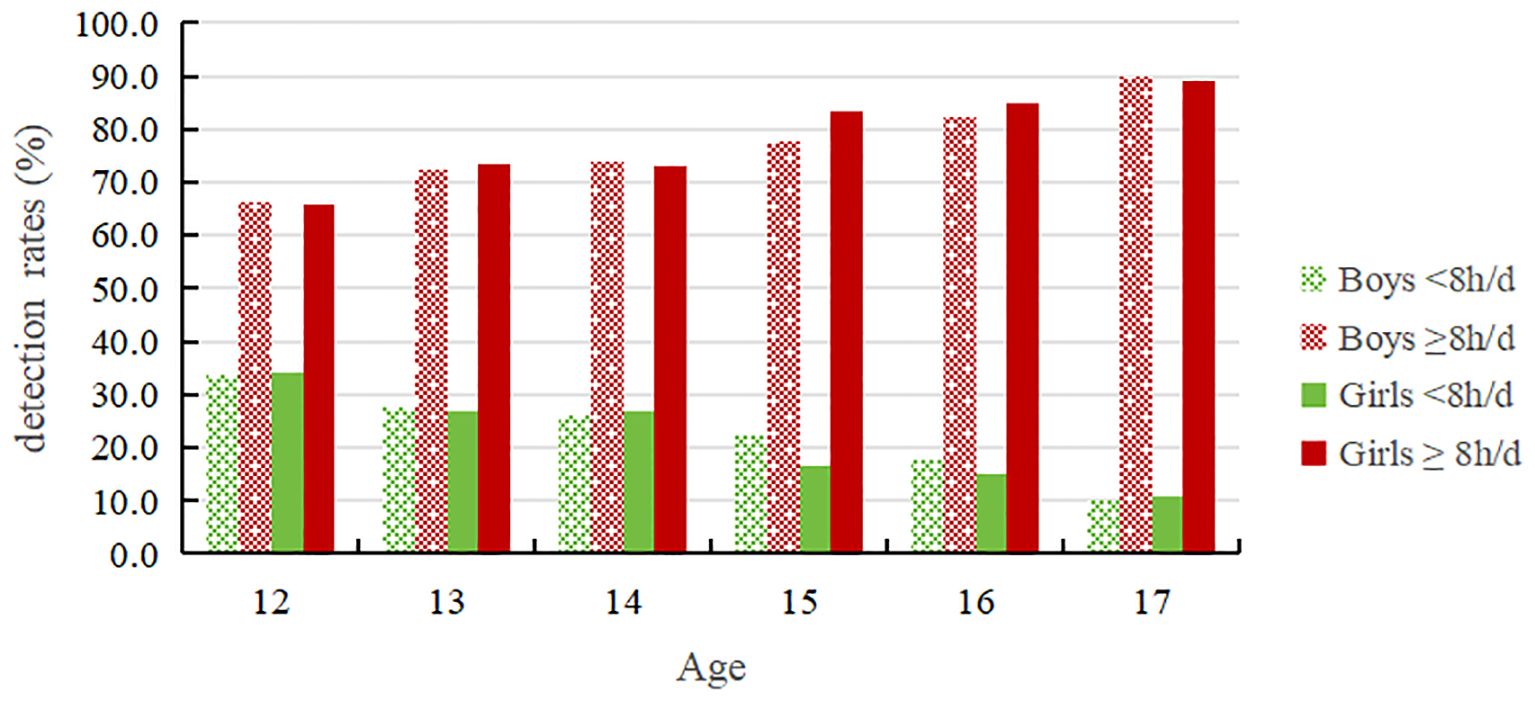
Figure 2. 12-17 years old adolescents' detection rates in different duration groups of sedentary behaviors.
Table 2 and Figure 3 demonstrates a fluctuating upward trend in the rate of adolescents’ daily screen time ≥2h with increasing age, with a rate of 14.7% at age 14 and then gradually increasing to 19.4% at age 17. Additionally, there was a significant difference in the prevalence of daily screen time ≥2 hours among adolescents of different ages (P < 0.01). The detection rate for boys’ daily screen time ≥2 hours was 18.4%, higher than the rate for girls (16.0%). The detection rate for boys’ daily screen time ≥2 hours was lowest at the age of 12(15.3%) and highest at the age of 17(20.7%); The percentage of girls with daily screen time use of ≥2 hours was lowest at the age of 12(13.8%) and highest at the age of 17, reaching 18.1%.
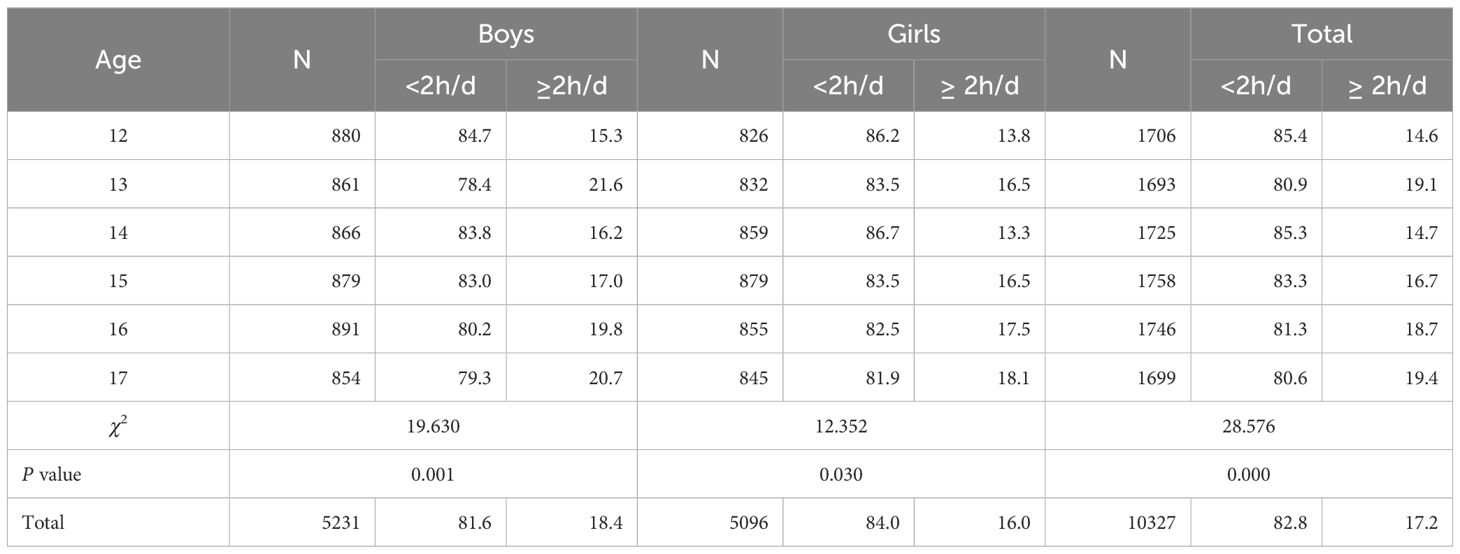
Table 2. 12-17 years old adolescent detection rates in different duration groups of screen time (%).
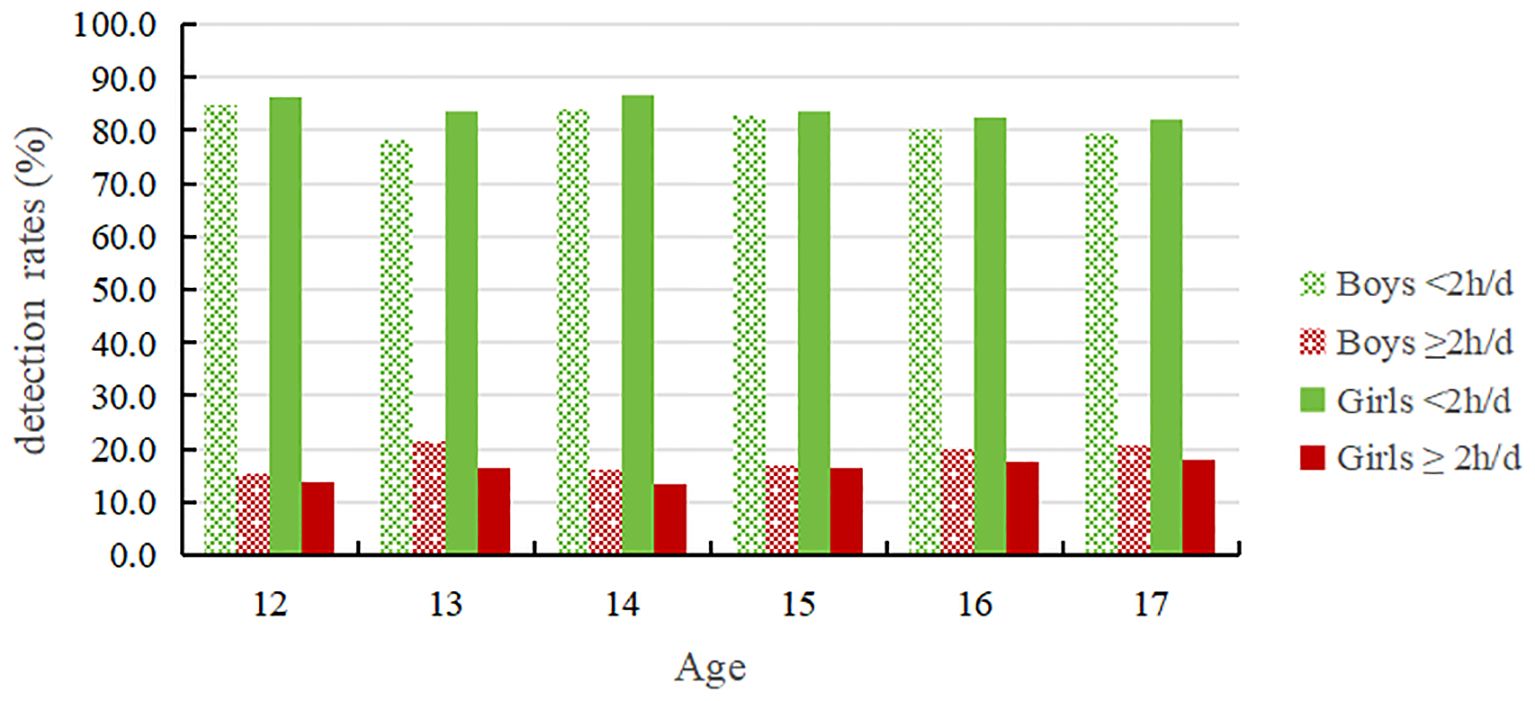
Figure 3. 12-17 years old adolescents' detection rates in different duration groups of screen time.
3.2 The incidence and behavioral characteristics of non-suicidal self-injury among adolescents
Table 3 shows that the total detection rate of NSSI behavior among adolescents over the past year was 25.1 %. The detection rates of occasional NSSI behavior and frequent NSSI behavior were 11.0 % and 14.1 %, respectively. The detection rate of NSSI behavior first increased with increasing age and then decreased. At the age of 14, the total detection rate for NSSI behavior was the highest at 27.9 %. At the age of 15, the detection rate of frequent NSSI behavior was the highest at 16.5 %. Moreover, there was a significant difference in the prevalence of NSSI behavior among adolescents of different ages (P < 0.01). Comparing the sexes, the total NSSI behavior detection rates for male and female students were 23.6 % and 26.7 %, respectively. Female students exhibited higher rates of NSSI behavior and occasional and frequent NSSI behavior than male students.
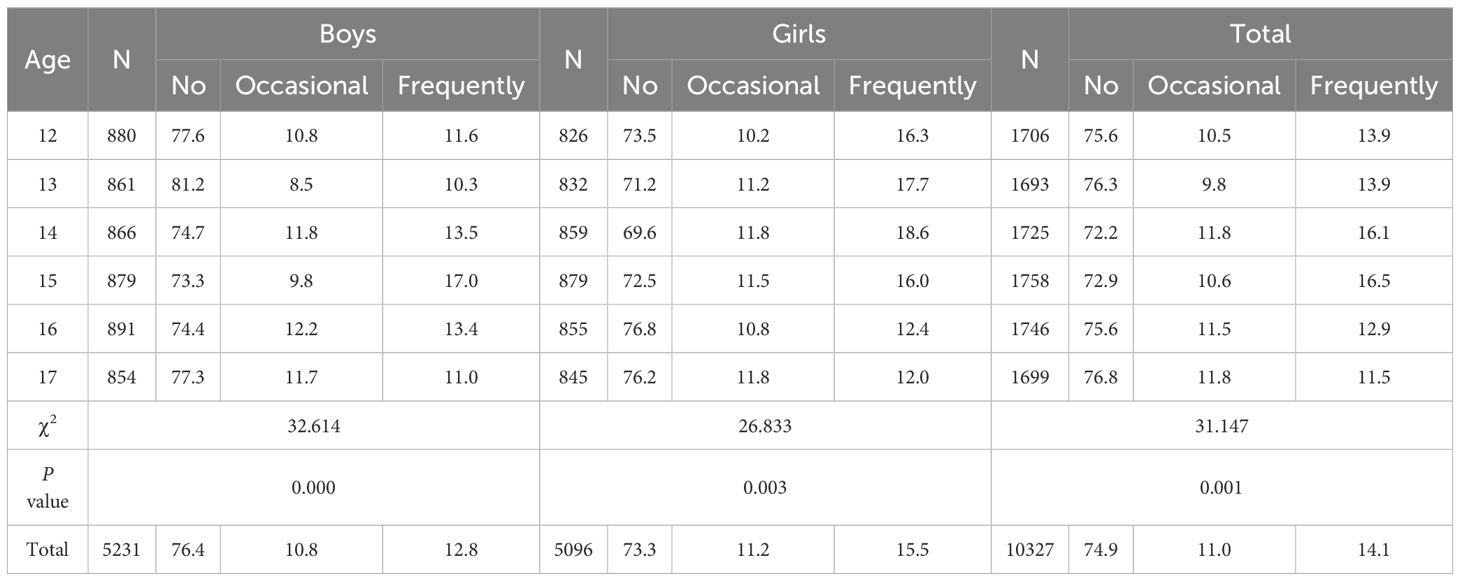
Table 3. Detection of NSSI in adolescents of different genders and ages(%).
3.3 Comparison of non-suicidal self-injurious behavior in adolescents under different durations of sedentary behavior
As can be seen from Table 4 and Figure 4, the detection rates of occasional NSSI and frequent NSSI for junior and senior high school students with sedentary behavior durations ≥8h are both higher than those with sedentary behavior duration <8h and the differences are statistically significant (P < 0.01). For both male and female students, those with sedentary behavior durations ≥8h have higher detection rates for occasional and frequent NSSI than those with sedentary behavior durations <8h; the differences are statistically significant (P < 0.01). Additionally, in different sedentary behavior duration groups, the detection rates of occasional NSSI and frequent NSSI for female students were higher than those for male students.
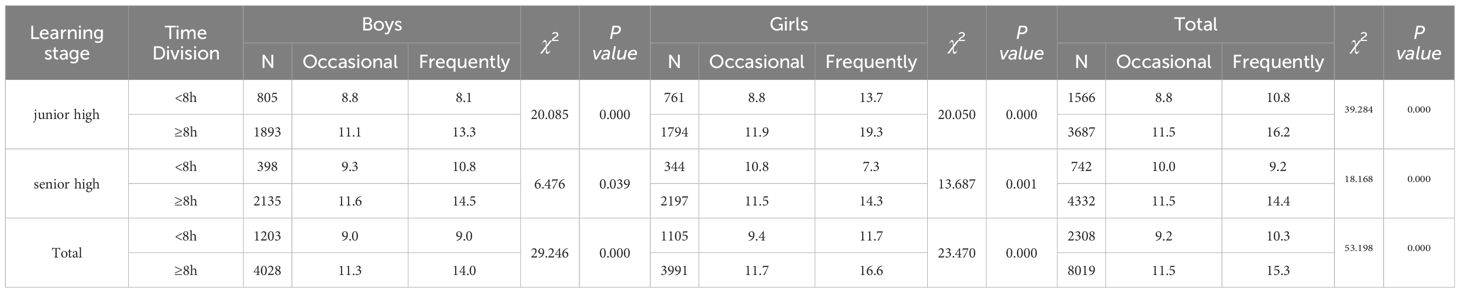
Table 4. The detection of NSSI in adolescents with different sedentary behavior duration groups(%).
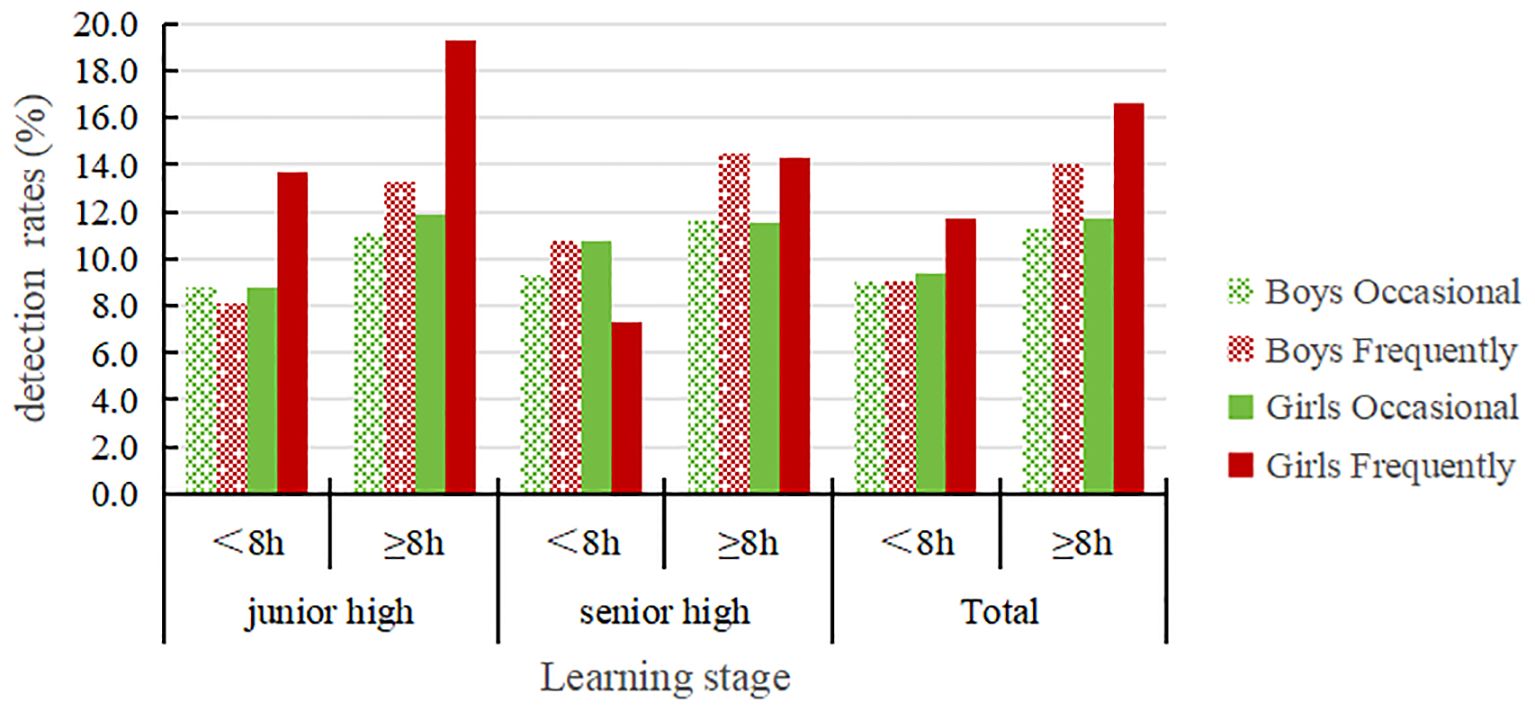
Figure 4. The detection of NSSI in adolescents with different sedentary behavior duration groups.
Table 5 and Figure 5 shows that the detection rates for both occasional and frequent NSSI in junior and senior high school students with screen time ≥2h are higher than those with screen time <2h and the differences are statistically significant (P < 0.01). For both male and female students with screen time ≥2h, the detection rates of occasional and frequent NSSI are both higher than for students with screen time <2h; the differences are statistically significant (P < 0.01). Additionally, female students in the different screen time groups had higher rates of, occasional and frequent NSSI than male students.
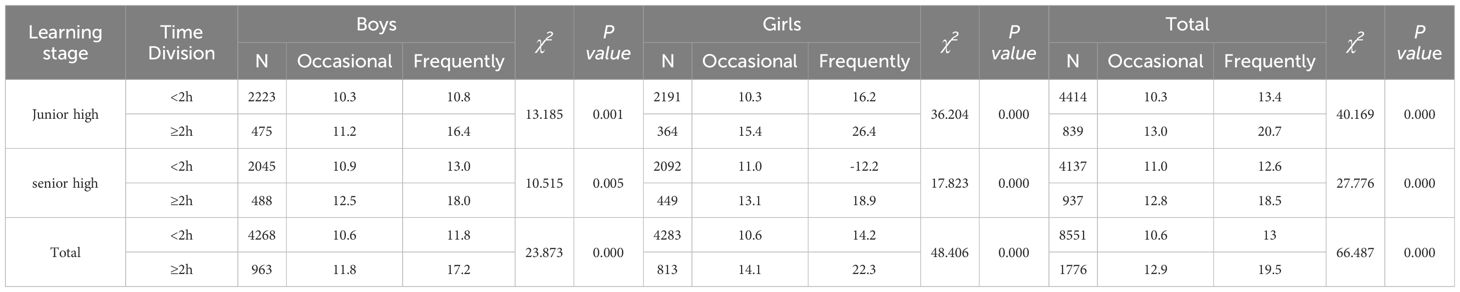
Table 5. The detection of NSSI in adolescents with different screen time groups(%).
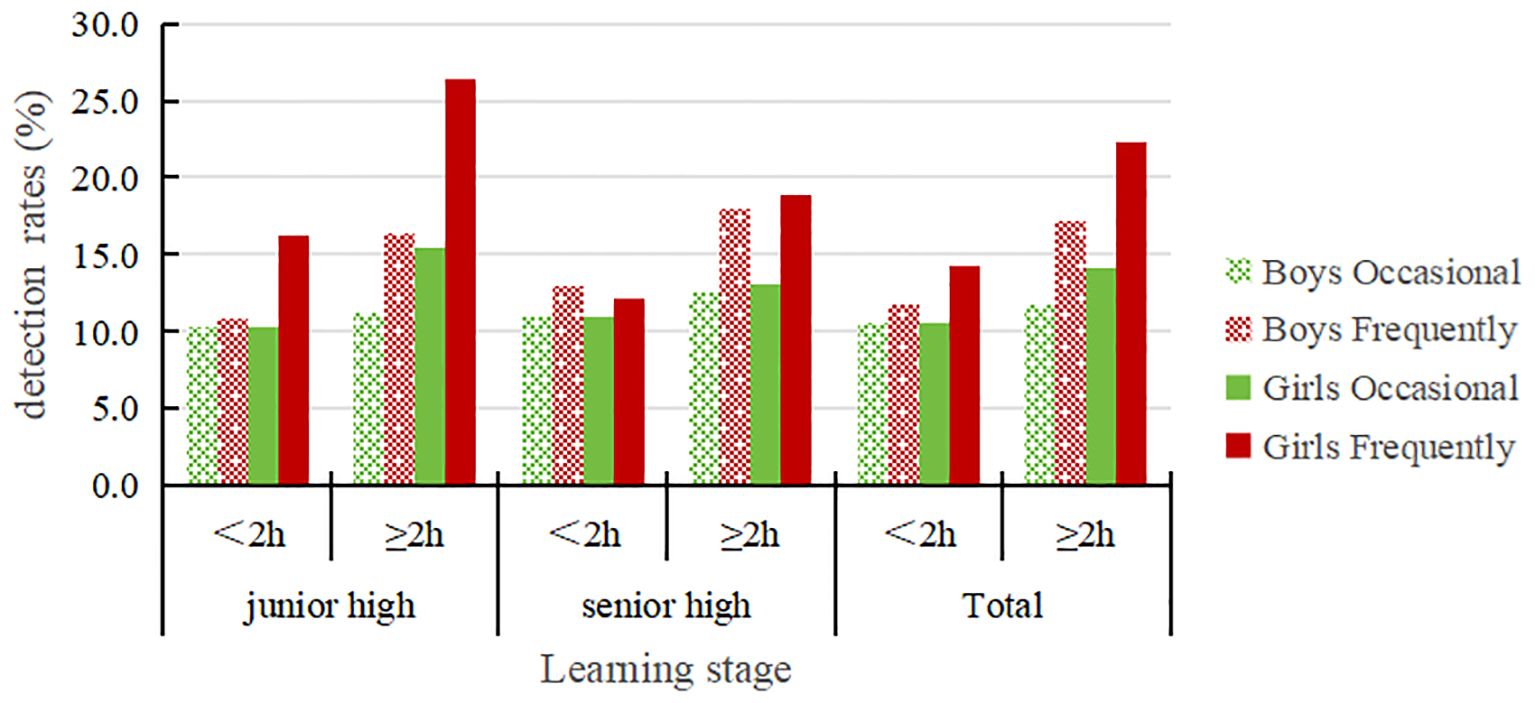
Figure 5. The detection of NSSI in adolescents with different screen time groups.
3.4 Logistic regression analysis of sedentary behavior and non-suicidal self-injurious behavior
Table 6 shows that in Model 1, no variables were adjusted, and in Model 2, after controlling for factors such as school section, gender, family structure, sleep standard achievement, and study time, the NSSI detection rate for the group with daily sedentary behavior duration ≥8 hours was 1.393times that of the group with <8 hours (β= 0.332, P < 0.001). The NSSI detection rate for the group with daily screen time ≥2 hours was 1.569 times that of the group with <2 hours (β= 0.451, P < 0.01).
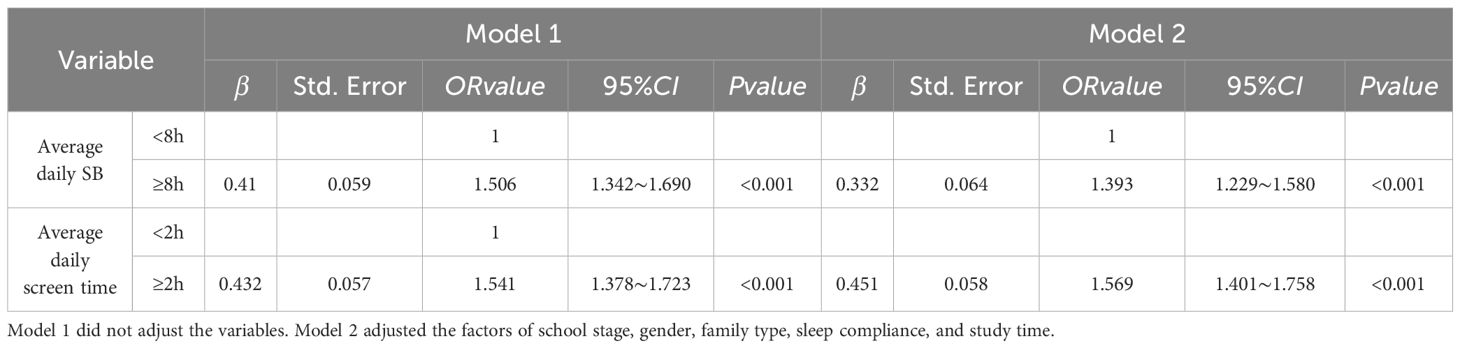
Table 6. Association of sedentary behavior duration and screen time with NSSI in adolescents.
4 Discussion
This study found that the duration of sedentary behavior and screen time showed an increasing trend with increasing age. Both domestic and foreign studies have shown that adolescents’ sedentary behavior duration is between 8 and 9.5 hours per day (11, 12, 17, 20). Our results are similar, indicating that the sedentary behavior duration of adolescents has not improved in recent years. In addition, our study also found a positive correlation between male sex, age/grade, and sedentary behavior; that is, the sedentary behavior duration of male students was longer than that of female students, and the sedentary behavior duration of senior students was longer than that of junior students (21). The duration of sedentary behavior is especially long in senior high school, which may be related to the curriculum setting in senior high school, including the number of class hours, the length of evening self-study, and the pressure of further education and schoolwork. In addition, studies have shown that with increasing age, adolescents tend to choose sedentary activities, and girls grow in this area faster than boys, which may be due to differences in the physical and mental development of the sexes (22).
Previous studies report that the screen time of children and adolescents in China is slightly higher than that found by this study (22). However, the present research did not differentiate between weekends and weekdays, and many studies have shown that teens spend significantly more time using screens on the weekend than midweek (23, 24). In general, this study shows that the average daily screen time of adolescents in China has declined and is lower than that of some developed countries. In recent years, China has attached great importance to the problems of increasing rates of myopia and a reduction In physical activity in children and adolescents and has taken corresponding measures to intervene; this may be one of the reasons for the decline of screen time in adolescents. However, with the popularity of various electronic devices, teenagers may increase their use of them, so it is necessary to continue to pay attention to and manage the sedentary behavior and screen time within a reasonable range.
Our study found that the total detection rate of NSSI behavior among adolescents in Chinese four cities was 25.1 %, which was slightly lower than the results of a domestic meta-analysis (28.2 %) (25), but similar to the detection rate of developed countries such as Italy and the Netherlands (26, 27). These findings suggest that while there are global trends in NSSI behavior, the cultural context of China, with its unique social and familial expectations, may influence the expression and reporting of NSSI behaviors. The lower detection rate compared to the meta-analysis might reflect cultural stigma or differences in behavioral reporting within Chinese adolescents. We also found that the incidence of NSSI behaviors among adolescents varies significantly with age, with 12–15 years being the high-incidence age group. Previous research indicates that the detection rate of NSSI behaviors in adolescence shows an inverted trend, peaking at 15 years of age before beginning to decline (28). In this study, the detection rate peaked at ages 14–15 and was significantly higher than in the other age groups. Overall, the NSSI behavior of adolescents showed a trend of first increasing and then decreasing with age, which is similar to the results of the aforementioned studies. This may be related to the fact that adolescents in the 14–15 age group are more likely to experience negative psychological emotions due to facing sensitive issues such as academic pressure, sexual maturity, and the rebellious period (29). Combined with the traits of irritability and impulsivity common in adolescents, this age group is more likely to resort to self-injurious behavior as a means to vent negative emotions. Preventing and intervening in NSSI behavior among adolescents during this high-incidence period will be crucial in reducing the current high occurrence of NSSI behavior.
In addition, we found that the NSSI behavior detection rate in girls was significantly higher than that in boys, consistent with previous research results (3, 30). However, sex differences in NSSI behavior among adolescents have not yet been established, and results are conflicting. Some studies have shown that the detection rate of NSSI behavior in boys is higher than that in girls (31), while others have pointed out that there is no significant difference between the sexes (32). These contradictory results may be related to the various studies’ evaluation methods and the age characteristics of the participants. The results of our study show that NSSI behavior is more common among girls in early adolescence, while in later adolescence, boys are more likely to engage in such behavior. This suggests that age-characteristic differences between participants in different studies may be a reason for the sex differences in the incidence of NSSI among adolescents. In terms of the types of self-injurious behavior exhibited by boys and girls, Hu Ya’s study (33) shows that boys are more inclined to engage in behaviors such as hitting, striking hard objects, and injuring themselves, while girls tend to adopt behaviors such as pinching, scratching, biting, piercing, and abrasions. The sex differences found in NSSI behavior among adolescents may also be related to the differences in the physical and mental development of boys and girls. Some studies have pointed out that NSSI behavior in girls is closely related to attempted suicide, while boys are more likely to engage in NSSI behavior to externalize their inner emotions (34). These results suggest that subsequent research should further refine their sample based on different sexes and ages, to conduct relevant explorations targeting different high-risk groups with distinct characteristics. This will provide a reference and a basis for developing more targeted prevention and control measures and intervention programs.
This study also found that longer sedentary behavior duration and screen time significantly increased the risk of NSSI behavior in adolescents. Other research suggests potential physiological and psychological mechanisms, such as the impact of sedentary behavior on mood regulation and the psychological effects of increased isolation and depressive symptoms, which are associated with NSSI (35). Foreign studies have found that health risk behavior is related to an increase in the detection rate of self-injury behavior and self-injury intention, including longer leisure-time sedentary behavior, which is consistent with the results of this study (36). However, there are few studies on the relationship between sedentary behavior and adolescent NSSI behavior at home and abroad. The present stud’s results indicate that even after controlling for related factors, a positive correlation between the total duration of sedentary behavior and adolescent NSSI behavior remains. Considering demographic factors, family structure, nutritional status, and sleep patterns, the total duration of sedentary behavior still has a significant relationship with adolescent NSSI behavior. This suggests that sedentary behavior may have an independent negative effect on adolescent NSSI behavior, but it may also be influenced by other related factors. Therefore, further research is needed to strengthen the understanding of the relationship between sedentary behavior and adolescent NSSI behavior.
In addition, several studies have found that screen time has an impact on the risk of self-injury behavior in adolescents, and too much screen time is associated with a high NSSI detection rate (1). This is consistent with the findings of this study, which show that spending more than two hours per day in front of a screen significantly increases the risk of NSSI behavior among adolescents. Watching videos related to self-injury behavior may induce children and adolescents to follow suit, and screen time can also lead to insufficient sleep and various related adverse psychological symptoms, increasing the risk of NSSI behavior (37). Overseas studies (38) have found that online chatting and sending instant messages are associated with NSSI behaviors among children and adolescents. Similarly, Liu et al.’s study of middle school students in 10 cities in China (39) found that excessive screen time is related to a higher NSSI detection rate. Hawto’s research also found that excessive screen time not only has a serious negative impact on the mental health of adolescents (1) but is also a risk factor for repeated self-injury and suicide. The present study also found that the detection rate of self-injurious behavior among adolescents engaging in excessive screen use is 10% higher than that of those with less than 2 hours of screen time per day. Research has found that up to 90% of videos with high viewership on YouTube contain non-character videos engaging in self-injurious behavior, and 28% of character-based videos also contain this type of behavior (37). Watching videos related to self-injurious behavior may lead children and adolescents to imitate, which is one of the reasons for the increased risk of NSSI associated with excessive screen time. Excessive screen time will also cause sleep deprivation and the emergence of various poor psychological symptoms such as depression and anxiety, which will further increase the risk of NSSI. Internet addiction will greatly increase the screen time of middle school students, and studies have shown that there is a close relationship between NSSI behavior and internet addiction among middle school students (40, 41). Internet addiction and suspected internet addiction are both risk factors for NSSI behavior among middle school students, suggesting that NSSI and internet addiction behavior may have a common development pattern and interact with one another. The internet provides an information source about adolescent NSSI behavior, and students who engage in NSSI behavior use the internet to alleviate negative emotions. Adolescents have a strong curiosity and desire to imitate new things, cannot view things scientifically, and are prone to psychological and behavioral problems. If the internet provides improper guidance, it will lead to a high incidence of NSSI among adolescents, resulting in a significant positive correlation between screen time and NSSI behavior.
While this study reveals a significant positive correlation between adolescent's sedentary behavior, particularly screen time, and NSSI, it is not without limitations. The cross-sectional nature of our data limits our ability to infer causality, and the reliance on self-reported measures of sedentary behavior and NSSI may introduce reporting biases. Our results may have broad generalizability; however, we acknowledge the need for further validation of these findings in different cultural, socioeconomic, and geographical contexts to enhance the external validity of our conclusions.
Recognizing the limitations of our study, future research should incorporate a wider range of potential confounding factors, including mental health status, social support networks, and family environment, to better understand the relationship between sedentary behavior and NSSI. A multicenter, multi-population approach would also strengthen the assessment of the generalizability and applicability of intervention measures, addressing the limitations of our single-setting study.
Despite the limitations, our findings support the development of clinical interventions targeting sedentary behavior to prevent NSSI. Future research should evaluate the effectiveness of interventions such as school-based physical activity promotion, parent education, and digital health applications in reducing screen time and promoting physical activity among adolescents. It is crucial to explore the applicability of these interventions across different populations and settings to maximize their impact.
In summary, this study provides a new perspective on the prevention of NSSI behavior among adolescents and points the way for future intervention research and clinical practice.
5 Conclusions
The results of this study confirm that sedentary behavior, especially screen time, is closely related to the occurrence of non-suicidal self-injury behavior in adolescents, indicating that it is feasible to intervene in and prevent NSSI behavior in adolescents by encouraging physical activity.
Based on the study’s findings, we propose the following specific recommendations:
Schools and families should restrict adolescent’ sedentary behavior and screen time, encouraging more physical activity.
Public health policies should promote physical activities among adolescents to prevent NSSI behavior.
Future research should further explore interventions to reduce sedentary behavior and their effectiveness in preventing NSSI behavior.
Through these measures, we can anticipate significant progress in reducing NSSI among adolescents, creating a more positive and healthier environment for their growth.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by the Human Subject Protection Committee of East China Normal University (approval number: HR319-2021). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
YG: Formal analysis, Software, Validation, Writing – original draft, Writing – review & editing. XY: Conceptualization, Project administration, Resources, Writing – review & editing. JX: Formal analysis, Methodology, Writing – original draft. FC: Conceptualization, Project administration, Supervision, Writing – review & editing. FZ: Data curation, Software, Validation, Writing – review & editing. YL: Investigation, Validation, Writing – review & editing. PS: Investigation, Validation, Writing – review & editing. JH: Investigation, Validation, Writing – review & editing. YH: Conceptualization, Investigation, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the National Natural Science Foundation of China (granted number: 82373595), and the Key Laboratory Construction Project of Adolescent Health Assessment and Exercise Intervention of the Ministry of Education (granted number: 40500-22203-542500/001/007/002).
Acknowledgments
Thank you to all participants and school personnel who participated in the data collection of this study, and to all collaborators for their contributions to the publication of the paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1489707/full#supplementary-material
References
1. Ali A, Azam M, Mattiullah J. Physical exercise as medicine for self-injurious behavior. Psychiatr Ann. (2020) 50:167–77. doi: 10.3928/00485713-20200302-02
2. Swannell SV, Martin GE, Page A, Hasking P, St JN. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life Threat Behav. (2014) 44:273–303. doi: 10.1111/sltb.12070
3. Cheung Y, Wong P, Lee AM, Lam TH, Fan Y, Yip P. Non-suicidal self-injury and suicidal behavior: prevalence, co-occurrence, and correlates of suicide among adolescents in Hong Kong. Soc Psychiatry Psychiatr Epidemiol. (2013) 48:1133–44. doi: 10.1007/s00127-012-0640-4
4. Hawton K, Saunders KE, O'Connor RC. Self-harm and suicide in adolescents. Lancet. (2012) 379:2373–82. doi: 10.1016/S0140-6736(12)60322-5
5. Wilson E, Crudgington H, Morgan C, Hirsch C, Prina M, Gayer-Anderson C. The longitudinal course of childhood bullying victimization and associations with self-injurious thoughts and behaviors in children and young people: a systematic review of the literature. J Adolesc. (2023) 95:5–33. doi: 10.1002/jad.12097
6. Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Pers Disord Emot Dysregul. (2015) 2:2. doi: 10.1186/s40479-014-0024-3
7. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41:S240–65. doi: 10.1139/apnm-2015-0630
8. Cruza AG, Suárez JF, Ciro JO, Chavarro NR, Villegas JG. Association between nutritional status and physical abilities in children aged 6 to 18 years in Medellin (Colombia). Pediatr (Barc). (2014) 81:343–51. doi: 10.1016/j.anpedi.2013.10.040
9. Jianyi X. Research on the relationship between Sedentary Behavior and Non-Suicidal Self-Injury Behavior in adolescents. Shanghai: East China Normal Univ. (2022).
10. Ruiz J, Ortega F, Martínez-Gómez D, Labayen I, Moreno L, De Bourdeaudhuij I, et al. Objectively measured physical activity and sedentary time in European adolescents: the HELENA study. Am J Epidemiol. (2011) 174:173–184. doi: 10.1093/aje/kwr068
11. Yang L, Cao C, Kantor ED, Nguyen LH, Zheng XB, Park Y, et al. Trends in sedentary behavior among the US population, 2001-2016. JAMA. (2019) 321:1587–97. doi: 10.1001/jama.2019.3636
12. Jian Y, Ming W, Fu-Bing Q, An-Qiao L, Jing-Yuan J, Ting Z. Research on health-related sedentary behaviors of children and adolescents aged twelve to 17. Chin J Rehabil Theory Pract. (2020) 26:1365–72.
13. Composing and Editorial Board of Physical Activity Guidelines for Chinese. Physical activity guidelines for Chinese (2021). Chin J Epidemiol. (2022) 43:5–6.
14. Wu HP. Study on Physical Fitness and Influencing Factors of Mental Sub-health Adolescents. Shanghai: East China Normal University (2019). Doctor.
15. Bosquet EM, Englund MM, Egeland B. Maternal childhood maltreatment history and child mental health: mechanisms in intergenerational effects. J Clin Child Adolesc Psychol. (2018) 47:S47–62. doi: 10.1080/15374416.2016.1144189
16. National Disease Control and Prevention Administration. Physical activity level evaluation for children and adolescents aged 7–18 years. In: National Health Commission Of China editor WS/T 10008-2023. National Disease Control and Prevention Administration, Beijing (2023).
17. Zhaohua Z, Liu Z, Hongjuan L. A Meta-analysis of physical activity among Chinese children and adolescents with accelerometer data. Chin J School Health. (2020) 41:173–8.
18. Inoue M, Yamamoto S, Kurahashi N, Iwasaki M, Sasazuki S, Tsugane S. Daily total physical activity level and total cancer risk in men and women: results from a large-scale population-based cohort study in Japan. Am J Epidemiol. (2008) 168:391–403. doi: 10.1093/aje/kwn146
19. Yuhui W, Wan L, Jiahu H, Fangbiao T. Development and evaluation on reliability and validity of Adolescent Non-suicidal Self-injury Assessment Questionnaire. Chin J School Health. (2018) 39:170–3.
20. Choi H, Kim C, Ko H, Park CG. Relationship between sedentary time and sleep duration among Korean adolescents. J Sch Nurs. (2020) 36:423–9. doi: 10.1177/1059840519842230
21. Salmon J, Tremblay MS, Marshall SJ, Hume C. Health risks, correlates, and interventions to reduce sedentary behavior in young people. Am J Prev Med. (2011) 41:197–206. doi: 10.1016/j.amepre.2011.05.001
22. Zhu Z, Tang Y, Zhuang J, Liu Y, Wu XP, Cai YJ, et al. Physical activity, screen viewing time, and overweight/obesity among Chinese children and adolescents: an update from the 2017 physical activity and fitness in China the youth study. BMC Public Health. (2019) 19:197. doi: 10.1186/s12889-019-6515-9
23. Liang Y-J, Hu Y-H, Tan X. Patterns of leisure time sedentary behaviors and physical activities among children. Acta Academiae Medicinae CPAF. (2011) 20:437–40.
24. Xiaoyan W, Shuman T, Shichen Z, Yukun Z, Kun H, Fangbiao T. Analysis of screen time and influencing factors among primary and secondary school students in 12 provinces in China. Chin J Prev Med. (2016) 50:508–13.
25. Shuangyu G, Meijie D, Xiaorong L, Xiangzi S, Chan P, Wanzhu Z. Meta-analysis of the detection rate of non-suicidal self-injury among Chinese adolescents. Modern Prev Med. (2023) 50:263–71.
26. Fleming TM, Clark T, Denny S, Bullen P, Crengle S, Peiris-John R, et al. Stability and change in the mental health of New Zealand secondary school students 2007-2012: Results from the national adolescent health surveys. Aust N Z J Psychiatry. (2014) 48:472–80. doi: 10.1177/0004867413514489
27. Giletta M, Scholte R, Engels R, Ciairano S, Prinstein MJ. Adolescent non-suicidal self-injury: a cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res. (2012) 197:66–72. doi: 10.1016/j.psychres.2012.02.009
28. Vancampfort D, Stubbs B, Mugisha J, Firth J, Van Damme T, Smith L, et al. Leisure-time sedentary behavior and suicide attempt among 126,392 adolescents in 43 countries. J Affect Disord. (2019) 250:346–53. doi: 10.1016/j.jad.2019.03.053
29. Blakemore SJ. The social brain in adolescence. Nat Rev Neurosci. (2008) 9:267–77. doi: 10.1038/nrn2353
30. Ting Z. Study on the Relationship Between Health-Related Physical Fitness and Mental behavior problems and Exercise Intervention of Adolescents. East China Normal University, Shanghai (2023).
31. Yuhui W. The Role of Pain Processing in the Relationship between Childhood Physical Abuse and Non-Suicidal Self-Injury Behaviors among Middle School Students. Anhui: Anhui Medical University (2015). Doctor.
32. Arensman E, Larkin C, Corcoran P, Reulbach U, Perry IJ. Factors associated with self-cutting as a method of self-harm: findings from the Irish National Registry of Deliberate Self-Harm. Eur J Public Health. (2014) 24:292–7. doi: 10.1093/eurpub/ckt087
33. Yan H, Hui-Giong X, Yu-Hui W, Pu-Yu S, Yin-Guang F, Dong-Ging Y. The status and influencing factors of non-suicidal self-injury among middle school students in Anhui Province. Chin J Dis Control Prev. (2020) 24:923–8.
34. Yates TM. The developmental psychopathology of self-injurious behavior: compensatory regulation in posttraumatic adaptation. Clin Psychol Rev. (2004) 24:35–74. doi: 10.1016/j.cpr.2003.10.001
35. Armijos Briones FM, Cortez Vega PS, Quishpe Achote KD. Negative impact of the excessive use of electronic devices in children and youth: a scientific approach. J Advanced Zool. (2023) 44:788–93. doi: 10.53555/jaz.v44iS1.511
36. Asante KO, Quarshie E, Onyeaka HK. Epidemiology of suicidal behaviours amongst school-going adolescents in post-conflict Sierra Leone. J Affect Disord. (2021) 295:989–96. doi: 10.1016/j.jad.2021.08.147
37. Lewis SP, Heath NL, St Denis JM, Noble R. The scope of nonsuicidal self-injury on YouTube. Pediatrics. (2011) 127:E552–7. doi: 10.1542/peds.2010-2317
38. Mitchell KJ, Ybarra ML. Online behavior of youth who engage in self-harm provides clues for preventive intervention. Prev Med. (2007) 45:392–6. doi: 10.1016/j.ypmed.2007.05.008
39. Liu M, Ming Q, Yi J, Wang X, Yao S. Screen time on school days and risks for psychiatric symptoms and self-harm in mainland Chinese adolescents. Front Psychol. (2016) 7:574. doi: 10.3389/fpsyg.2016.00574
40. Ying M, Yanru C, Man Z, Hongda G, Yanni Y, Jie T. Association of non-suicidal self-injury with Internet addictive behavior among adolescents. Chin J School Health. (2019) 40:972–6.
Keywords: adolescents, non-suicidal self-injury, sedentary behavior, screen time, mental health
Citation: Guo Y, Yin X, Xu J, Chen F, Zhang F, Liu Y, Sun P, Hong J and Hu Y (2024) The relationship between sedentary behavior and non-suicidal self-injury behavior among adolescents in China. Front. Psychiatry 15:1489707. doi: 10.3389/fpsyt.2024.1489707
Received: 12 September 2024; Accepted: 18 November 2024;
Published: 04 December 2024.
Edited by:
Yan Cai, Fujian Energy General Hospital, ChinaReviewed by:
Zhengxiao Wei, Chengdu Public Health Clinical Medical Center & Public Health Clinical Center of Chengdu University of Traditional Chinese Medicine, ChinaTianjiao Li, Chinese PLA General Hospital, China
Xiaoshuai Ning, Fuyang Third People's Hospital, China
Copyright © 2024 Guo, Yin, Xu, Chen, Zhang, Liu, Sun, Hong and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fule Chen, Mzk1NzEwMTQzQHFxLmNvbQ==; Feng Zhang, ZnpoYW5nMTk4OEAxMjYuY29t