 Bixi Yang
Bixi Yang Chenxi Liao
Chenxi Liao Yuqing Yang
Yuqing Yang Binbin Shi1
Binbin Shi1 Caidi Zhang
Caidi Zhang Chunbo Li
Chunbo Li- 1Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 2Shanghai Yangpu District Mental Health Center, Shanghai University of Medicine and Health Sciences, Shanghai, China
- 3Shanghai Key Laboratory of Psychotic Disorders, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 4Institute of Psychology and Behavioral Science, Shanghai Jiao Tong University, Shanghai, China
Background: Cognitive restructuring (CR) is an evidence-based psychological technique for depression. However, face-to-face CR is not easily accessible. Digital CR interventions often overlook the difficulties individuals experiencing depression encounter in identifying their negative automatic thoughts (NAT), leading to suboptimal outcomes. Virtual Reality (VR) has potential advantages in assisting the identification of NAT in CR intervention.
Objective: The aim of this preliminary feasibility study is to assess the efficacy, acceptability and safety of a VR-based self-guided training on the identification of negative automatic thoughts (VR-STINAT) for depression, as well as to evaluate the user experience.
Methods: In a mixed methods study, 20 healthy participants underwent VR-STINAT and completed a semi-structured interview, followed by post-training homework. The VR-STINAT includes three modules: psychological education, NAT identification training in VR scenarios, and practice in personally experienced scenarios. Effectiveness was measured via Thought Record Skills Assessment (TRSA) of homework and Cognitive Therapy Awareness Scale (CTAS). Acceptability was measured using an adapted Technology Acceptance Model and duration of training. Safety was measured via Simulator Sickness Questionnaire and self-reported negative emotions. Qualitative material was analyzed using thematic analysis.
Results: The VR-STINAT was acceptable, with an average rating of 80.68%. The accuracy of NAT identification in TRSA reached 84.55%, and CTAS correctness reached 76.67%. The majority of participants experienced minimal or no side effects, although a few (10%, 2/20) reported relatively severe fatigue and craniofacial pain. Thematic analysis reviewed four themes: effectiveness, acceptability, advantages of VR, difficulties in use and suggestions for improvement. Most participants indicated that they’ve learned how to identify their NAT through VR-STINAT (85%, 17/20), which was engaging (90%, 18/20) and easy to use (60%, 12/20).
Conclusion: This study provides preliminary evidence that self-guided training for the identification of negative automatic thoughts related to depression using VR is feasible. Future studies are needed to compare the efficacy of VR with other intervention modalities in people with depression.
1 Introduction
Cognitive restructuring (CR) is an evidence-based psychological technique for depression (1). Automatic thoughts (AT), the most accessible levels of cognition and generally the first to be targeted in CR, refer to individuals’ immediate interpretations of specific situations, which occur spontaneously in consciousness. AT can occur so quickly that individuals may not always be fully aware of them, yet they can significantly impact their emotions (2). Identification of negative automatic thoughts (NAT) that trigger intense emotions is the initial step of CR, followed by evaluation for veracity and functionality before modification.
However, individuals experiencing depression may encounter challenges in identifying their own NAT due to their cognitive and psychological characteristics. First, individuals experiencing depression often experience alexithymia (3), making it difficult for them to adequately identify and describe their emotions and thoughts. Secondly, depression has been associated with over general autobiographical memory, manifested by a reduction in the quantity of specific memories (4). This impedes the ability of individuals experiencing depression to identify previous NAT through recollection. Moreover, experiential avoidance, including behavioral and cognitive avoidance, serves as a coping mechanism among individuals experiencing depression to avoid negative emotions, but this can negatively impact NAT identification (5, 6).
In face-to-face CR therapy, to help individuals experiencing depression to identify their NAT, therapists often employ techniques such as role playing and guided imagery (6). However, individuals experiencing depression may withhold their genuine NAT due to concerns about the therapist’s response. In addition, the current accessibility of professional psychotherapy is limited (7). In China, only 9.5% of individuals experiencing depression have received mental health services, and the proportion of those considered to have received adequate treatment (antidepressants and outpatient psychotherapy from mental health institutions) for depression is as low as 0.5% (8).
The effectiveness and acceptability of digital CR interventions have been preliminarily verified in recent years (9). However, there is a lack of attention to the challenge faced by individuals experiencing depression in identifying NAT. Existing digital CR interventions elicit emotional arousal mainly through imagination and recollection, a process influenced by factors such as users’ autobiographical memory and imaginative ability. Consequently, evaluating and ensuring the activation of cognitive schema becomes challenging (10), which plays a crucial role in acquisition of CR skills and subsequent efficacy of interventions (11, 12). Current digital CR interventions primarily focus on the evaluation and modification of NAT. The intervention promptly proceeds to the subsequent stage once the user reports the initial NAT they identify, which may unintentionally lead to the omission of other important NAT (13), potentially compromising effectiveness (14).
Virtual Reality (VR) broadly refers to computer-generated interactive environments, providing safe, controllable, and repeatable scenarios (15). Numerous studies have integrated VR with various psychotherapies, and their effectiveness and safety have been preliminarily validated (16–18). VR holds potential advantages in assisting with the identification of NAT in CR for depression. First, VR can trigger more emotional arousal than imaginative approach (10, 19). VR scenarios enable users to acquire perceptual and emotional experiences similar to those in the real world, thereby minimizing the influence of memory, imagination, and experiential avoidance. Also, VR has the potential to create a non-judgmental environment, facilitating the reduction of defense mechanisms in individuals with secondary (or state) alexithymia (3), therefore enhancing their ability to identify and articulate their thoughts and emotions. Moreover, VR is the most concrete form of multimedia, requiring minimal cognitive effort from users, making it suitable for individuals experiencing depression with impaired learning capacity (20). VR also enables activation of visual, auditory, and kinesthetic encoding modes, enhancing the retention of psychological techniques (21). In addition, VR interaction enhances the enjoyment of learning, thereby promoting user engagement and proactivity (22, 23).
However, VR-assisted CR for depression is yet to be explored (24, 25). In 2008, Botella et al. initially employed the EMMA’s World VR system as a sandbox-like tool, to help an individual with complicated grief to express thoughts and emotions (26). In 2021, the study conducted by Kocur et al. developed CAT-DB, an auxiliary tool for CR, in which participants are faced with a virtual avatar expressing their personal dysfunctional beliefs to implement role playing technique (19). That same year, Bolinski et al. developed Zondag Virtual Restaurant as a VR scenario to elicit negative emotions (10). However, in this study, VR was only used as a tool for emotional induction, still requiring the full participation of a psychotherapist to implement CR.
The aim of this study is to evaluate the feasibility of a VR-based self-guided training on identification of NAT (VR-STINAT) for depression, including its efficacy, acceptability and safety, using a mixed methods design primarily within the healthy population. The study posits that the VR-STINAT is effective, safe and acceptable in healthy adults.
2 Methods
2.1 Research design
A convergent mixed-method design was adopted to investigate the feasibility of the VR-STINAT among healthy individuals (27, 28). Quantitative and qualitative data were collected and analyzed concurrently from the same group of participants to obtain an overview of the user experience, as well as to reveal personal experiences, thereby enhancing understanding and reflection of the training process. The integration of quantitative and qualitative findings was conducted during the interpretation stage. Considering the potential emotional fluctuations that NAT identification training might cause and to avoid potential harm to patients with depression (29), this preliminary exploratory feasibility study targeted only healthy individuals who also experience NAT. This study has been approved by the Ethics Committee of the Shanghai Mental Health Center (2019-51C2), and completed clinical research registration (ChiCTR2000040894). All participants have signed informed consent.
2.2 Participants and recruitment
Inclusion criteria for the study included being aged between 18 and 60 years old, being able to read and understand Chinese, scoring below 10 at the Patient Health Questionnaire-9 (PHQ-9) (30). We excluded individuals who suffered from severe physical or mental disorder as assessed with the Mini International Neuropsychiatric Interview Version 4.0.0 (MINI) (31), such as alcohol and/or substance dependence disorder, bipolar disorder, psychotic disorder, suicidal ideation, and those who had received psychological therapy within the past 3 months. The sample size was determined by data saturation, using a saturation table (32). Enrollment stopped when no new themes emerged in the qualitative data.
Participants were recruited online in January 2022. A maximum variation purposive sampling was used to ensure diversity in the sample across gender, age, education level, and experience in VR use. A total of 688 online screening questionnaires were collected initially, out of which 43 samples were obtained. A total of 24 participants completed the offline enrollment screening, out of whom 4 participants were excluded due to bipolar disorder (n=2), post-traumatic stress disorder (n=1), suicidal ideation (n=1), resulting in a final inclusion of 20 participants.
2.3 Study procedure
The study was conducted in Shanghai Mental Health Center. After completing baseline assessments, the enrolled participants registered for training accounts and imported their personalized information. Subsequently, they underwent VR-STINAT, followed by post-intervention assessment and semi-structured interview. The entire training process was closely monitored by researchers, who promptly documented any issues that arise during the training. At the training site, recliner chairs and eye patches are provided to alleviate symptoms such as dizziness, nausea, dry eye. The participants were instructed to submit daily homework on NAT identification for 7 days after the training and subsequently complete follow-up questionnaires. The offline study required approximately 2.5 hours, and the online homework took about 15 minutes per day.
2.4 VR-based training
The VR-STINAT was iteratively developed with the involvement of end-users (CBT therapists, psychiatrists, patients with depression, and healthy individuals), based on cognitive load theory -learning from worked example (33), and Mayer’s cognitive theory of multimedia learning (34). Gamification elements such as feedback and achievements were incorporated to enhance enjoyment, and engagement (35).
The VR-STINAT includes three modules: ① psychological education, ② NAT identification training in VR scenarios, and ③ practice in personally experienced scenarios (see Figure 1). The initial module helped users understand the training process and learn about Beck’s cognitive model through worked-out examples (2). The second module consists of six VR scenarios, including various interactive elements such as mobile phones, during which users were required to complete several tasks of NAT identification. In the third module, the virtual psychotherapist guided users to describe their personal experiences and to identify their NAT and emotions that arose in those particular situations. A fading procedure was implemented in which problem-solving elements are progressively incorporated into example study until the users could solve problems on their own. Identification of AT and emotions was facilitated through an operable panel suspended in virtual space, enabling interaction via controllers and voice input. The first and third modules were implemented within a virtual psychotherapy room, which was modeled based on actual psychotherapy rooms. Participants were given the option to choose the gender of their virtual therapist, whose voices were provided by experienced psychotherapists, and physical appearance resembling that of real psychotherapists. Personalized information of participants (e.g. work experience) was preloaded in the VR scenarios to enhance involvement and emotional arousal.
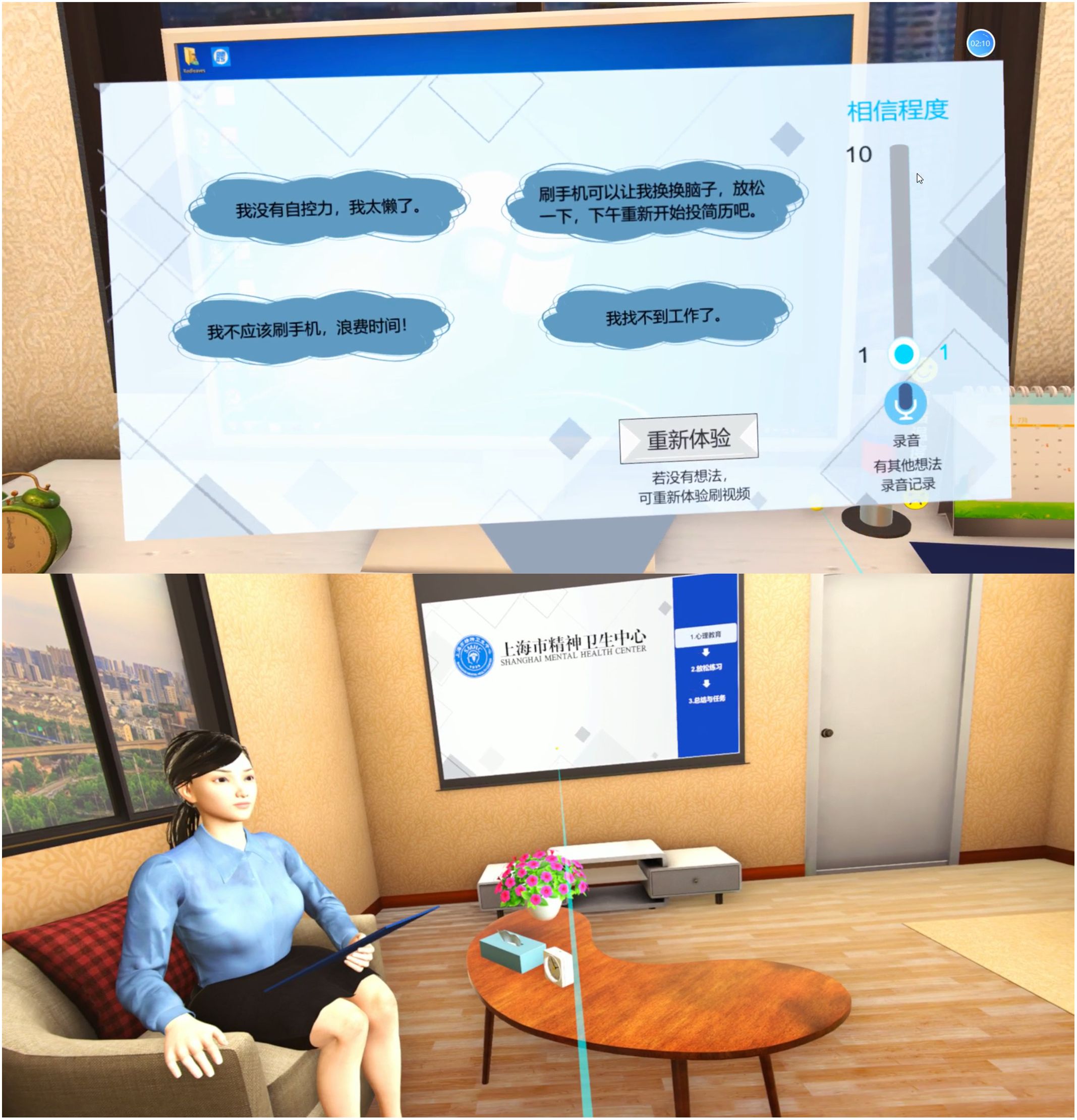
Figure 1. Screenshots of VR-STINAT.
VR scenarios simulate first-person experiences, capable of evoking a notable level of emotional arousal and providing opportunities for practicing the identification of NAT. In contrast to specific phobias and other mental disorders, the negative cognitive induction scenarios associated with depression lack specificity. The VR scenarios in the VR-STINAT were generated through qualitative research on psychotherapy documentation and homework from our previous CBT intervention studies for depression.
Combining VR with NAT identification may give rise to potential risks, including mood fluctuations, self-harm, or even suicide. To address this, the VR-STINAT has an early warning mechanism that promptly alerts the user’s doctor or psychotherapist when the level of negative emotional arousal exceeds a predetermined threshold. The doctor or psychotherapist then evaluates the user’s risk of suicide and provides preventive measures, including psychological education, contacting family members, and making referrals. Besides, relaxation techniques such as abdominal breathing and progressive muscle relaxation were provided in virtual natural environments following the training to mitigate emotional distress.
Participants entered the VR environment by means of a commercially available head-mounted display (HTC VIVE COSMOS 2Q2R100), connected to a laptop (ALIENWARE x17 R1 17.3-inch 8-core i7 32G 1T RTX3070 165Hz) on which the application was run. The Steam VR platform was used as the intermediary between hardware input and the intervention software (36). Participants interacted with the VR environment using two wireless hand-controllers.
2.5 Outcome measures
2.5.1 Quantitative outcomes
2.5.1.1 Effectiveness
The Thought Record Skills Assessment (TRSA) (37, 38) was used to evaluate participants’ mastery of AT identification by rating their homework based on the content of situational events, emotions, and AT. Two researchers (YBX and SBB) independently assessed the scores and engaged in discussions to achieve consensus in case of any discrepancies.
An adapted version of Cognitive Therapy Awareness Scale (CTAS) was used to assess the participants’ knowledge of CR theory and application. The original CTAS consists of 40 true or false questions (Cronbach α=0.58). We selected 12 items related to automatic thoughts (37).
2.5.1.2 Safety
The Chinese version of Simulator Sickness Questionnaire (SSQ) was used to evaluate physiological safety (39). In terms of psychological safety, emotional arousal was assessed via self-report through the operable panel in VR scenarios, and emotional intensity was assessed via the Visual Analogue Scale (40) (1=almost none, 10=extremely). VR scenarios where the intensity of negative emotions reached 8 were marked.
2.5.1.3 Acceptability
The acceptability of the VR-STINAT was assessed according to the Virtual Reality Hardware Acceptance Model (VR-HAM) (41), including four dimensions: perceived usefulness, perceived ease of use, attitude towards use, and intention to use. The duration of VR training was recorded.
2.5.1.4 Engagement and adherence
Engagement was measured by the number of exercises participants voluntarily performed in the third module of VR-STINAT. Adherence was measured by the participants’ completion of assigned homework.
2.5.1.5 Depressive symptoms
Depressive symptoms were assessed using the Chinese version of Patient Health Questionnaire Depression Scale (PHQ-9), a self-report questionnaire for the assessment of depressive symptoms (30).
2.5.1.6 Presence
Immersion was assessed using the Chinese version of the Igroup Presence Questionnaire (IPQ), a 13-item self-reported questionnaire rated on a 7-point scale. The items are categorized into three dimensions: spatial presence, involvement, and realness (42).
2.5.2 Qualitative outcomes
A semi-structured interview questionnaire was developed to understand the participants’ experience with the VR-STINAT (43, 44). The interview included a series of open-ended questions, covering the following topics: expectations, experience, opinions and suggestions (Supplementary Material 1). Before the interview, we obtained participants’ informed consent to record audio. The interview was conducted in a quiet and private environment, ranged between 8 and 35 minutes (Mean=14 minutes). Each interview was fully recorded on a voice recorder and transcribed verbatim. Furthermore, feedback on the overall experience of VR and homework was collected 7 days after the VR intervention to ensure thorough gathering of participants’ feedback.
2.6 Data Analysis
Quantitative data analysis was conducted using SPSS V.28.0. Descriptive statistics for categorical variables and safety data were reported as frequencies and percentages. Depending on the data distribution, continuous variables were reported as mean ± standard deviation (M ± SD) (for normal distribution), and as median (interquartile range) (for abnormal distribution). Pearson correlation with Bonferroni correction was used for correlation analysis. T-tests or non-parametric tests were used for continuous data, while chi-square tests were used for categorical data. When the minimum expected value is below 5, Fisher’s exact test was applied. When analyzing the pre-post differences of PHQ-9, a repeated measures analysis of variance was used. The significance level was set at α = 0.05.
Qualitative material was analyzed through the six-step approach (45) to thematic analysis using nVivo (V.12). The thematic analysis was conducted with guidance from the Technology Acceptance Model (TAM) and the Theory of Planned Behavior (TPB) (46, 47). All transcripts were read and coded individually by two researchers (YBX and SBB). They then discussed their codes and generated themes in an iterative process, referring back to the transcripts and the original codes to ensure that the analysis was representative of the data.
3 Results
For sociodemographic characteristics of participants, see Table 1.

Table 1. Sociodemographic and baseline characteristics.
3.1 Quantitative results
All participants (n=20) completed the training and post-training assessment. Table 2 summarizes the quantitative results.
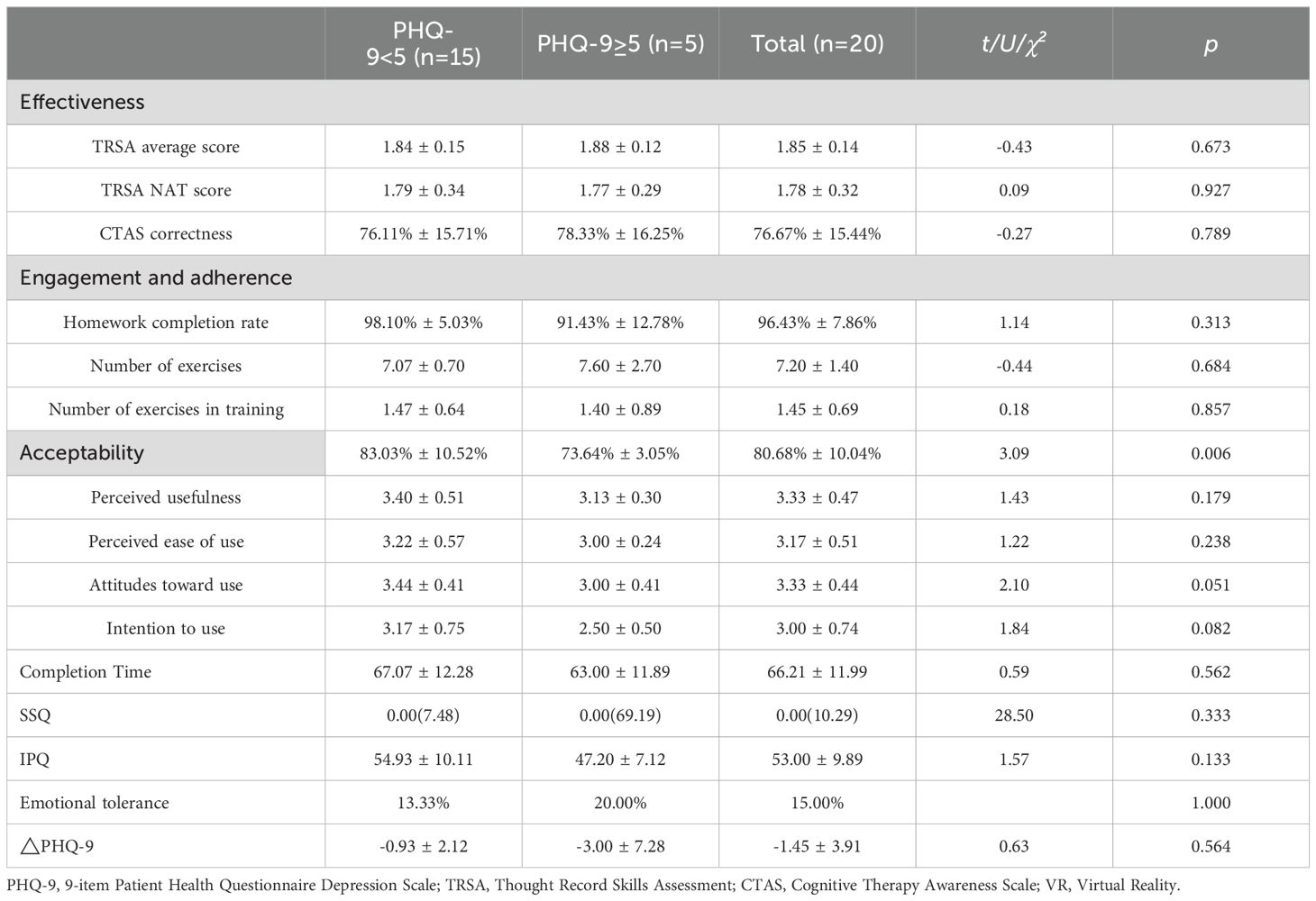
Table 2. Outcome measures.
The TRSA scores for homework showed a high inter-rater reliability of 82.64% (357/432). According to SSQ, the majority of participants (n=18, 90%) experienced negligible symptoms (SSQ score <5), while two participants (10%) reported problematic symptoms (SSQ score >20) of moderate general discomfort, eyestrain, difficulty focusing, fullness of head, nausea, dizzy (eyes open), and moderate-to-severe fatigue, blurred vision. The most common adverse event was fatigue (n=5), and the most frequently observed adverse event of moderate to severe intensity was craniofacial pain induced by VR glasses (n=3, 15%). Three participants (15%) experienced relatively intense negative emotions.
Subgroup analysis was conducted between the participants with baseline PHQ-9 scores above and below 5. The VR-STINAT was significantly more acceptable for the PHQ-9<5 group (t = 3.09, p = 0.006). The mean scores of attitudes toward use and intention to use between two groups were to the edge of significantly different.
Correlation analysis showed that pre- and post-training change in PHQ-9 score (△PHQ9) was positively correlated with age (r = 0.493, p = 0.032), indicating that improvement in depressive symptoms decreases with increasing age. Repeated-measures ANOVA with PHQ-9 score as dependent variable and age as covariate revealed a significant decrease in depressive symptoms after controlling for the effects of age (F = 7.135, p = 0.016).
3.2 Qualitative results
Four core themes emerged through thematic analysis: effectiveness, acceptability, advantages of VR, difficulties and suggestions for improvement (see Figure 2). Any themes mentioned by at least two participants (10% of the sample) are depicted.
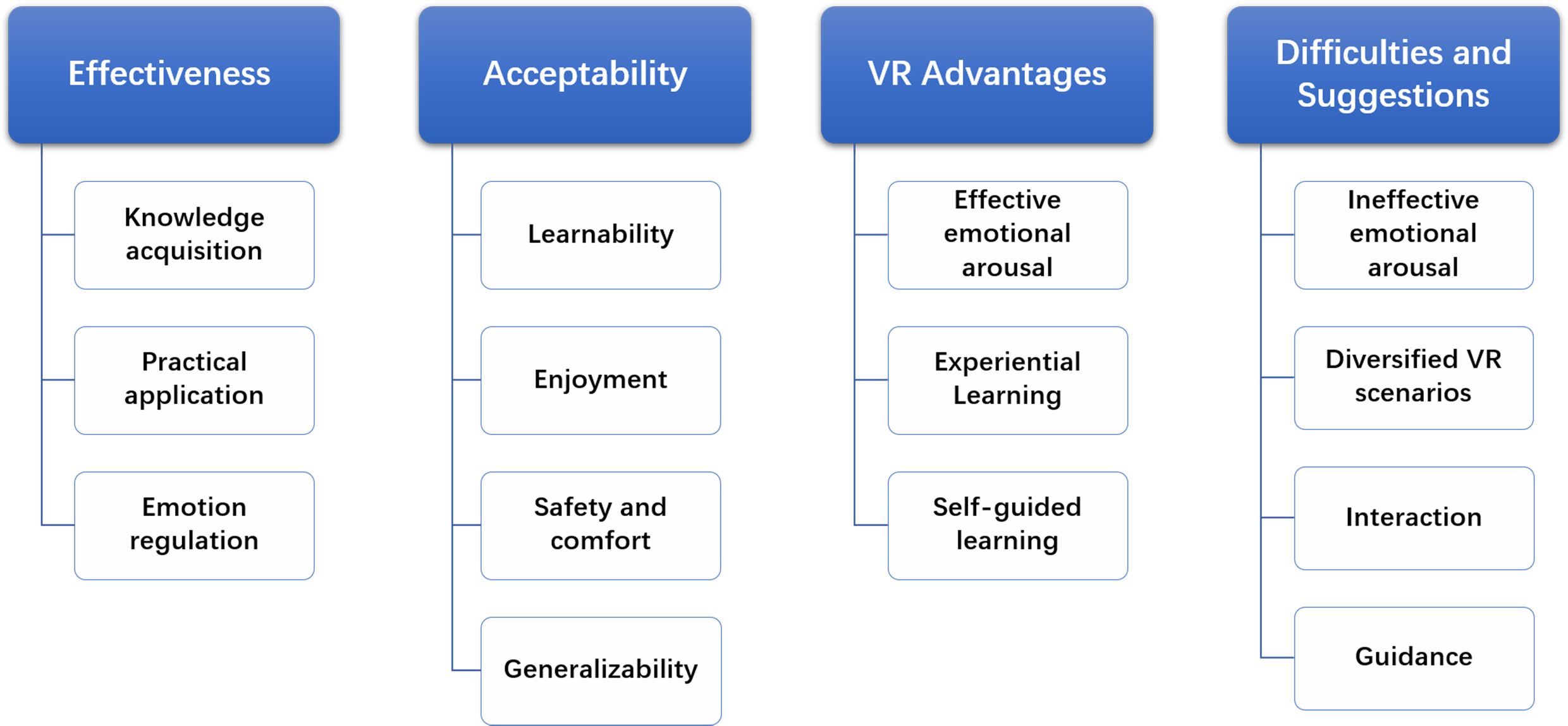
Figure 2. Structure of the thematic analysis.
3.2.1 Effectiveness
The majority of participants (n=17) reported that through VR-STINAT they have learned how to identify their NAT and emotions, with awareness of the impact of thoughts on emotions, and have realized the need to distinguish between subjective perceptions and objective facts. Some participants (n=13) made further associations that emotions can be regulated by adjusting cognitions and started to summarize and reflect on the identified NAT.
“I’ve learned a method. When you want to analyze something, the thought record can help you calmly analyze your thoughts at that moment. You can see some mood swings and score your mood.” (P01)
Participants also found that VR-STINAT positively influenced their application of the skills (n=16), by enhancing their self-efficacy and an awareness of continuous practice. Several participants (n=8) proactively planned to continuously practice the learned psychological skill in their daily lives.
“I truly learned the skill to regulate emotions through cognition … When encountering situations in the future, I can slow down a bit, think about which of my thoughts caused the emotion, and further evaluate whether my thoughts are objective and accurate. This can reduce some unnecessary emotional consumption.” (P05)
After one week of practice, participants (n=9) reported that identifying NAT helped regulate their emotions and fostered greater acceptance and compassion towards their emotions, providing an enhanced understanding of their internal experiences. Participants reported that when they experienced negative emotions, they learned not to dwell on the negativity but instead to start using the psychological techniques to analyze (n=3).
“Trying to adjust my automatic thoughts is helpful for problem-solving and mood adjustment.” (P11)
“This VR experience made me realize that all thoughts are actually normal. Everyone has their automatic thoughts, which then generate various emotions, good and bad.” (P13)
“I will not indulge in negative emotions; instead, I can step back and analyze the situation.” (P15)
3.2.2 Acceptability
Most participants found VR-STINAT easy to understand and use (n=12), as well as engaging (n=18). Participants perceived the main source of enjoyment in VR-STINAT to be its immersive and gamified experience, role-playing and human-computer interaction. They also believed that it had the potential for broader application (n=6), serving not only healthy individuals but also patients with depression who feel ashamed due to illness or have difficulty accessing treatment.
“I had no prior experience in VR, so overall this experience was very good. The operation was quite convenient, and even though I’m not very good with electronic devices, I found it completely manageable.” (P05)
“It was quite interesting and somewhat immersive … I even reached out with the controller to see if there was a real table in front of me, and I wanted to give a thumbs-up on my social media in VR. It was quite fun.” (P10)
“It felt as if I were playing a game or something. It’s very interesting.” (P19)
“I know that psychological therapy is not that accessible right now, and people with mental conditions are often reluctant to seek help. If this could be used at home, it would be helpful.” (P09)
Some participants reported feeling fatigued and uncomfortable after using the head-mounted virtual glasses for extended periods (n=4).
The thing with VR glasses is that they’re not very user-friendly. They can get pretty heavy and start to feel uncomfortable if you wear them for a long time. ( P02)
3.2.3 VR advantages
Most participants stated that VR-STINAT allowed them to immerse themselves in a first-person perspective, effectively evoking their emotional experiences, which helped them practice identifying their AT (n=10). They reported that certain components within the system could help them alleviate the negative emotions aroused (n=3).
“It really evoked my emotions. At that moment, I felt depressed … This sense of frustration was very clear to me. So, the overall environment, including the scenarios’ immersion, was quite strong. I didn’t like the negative emotions, but I think this method worked very well. Although it induced negative emotions, it made the learning experience more impactful because my emotions were triggered.” (P07)
Participants mentioned that, after theoretical learning, immediate practice of the learned psychological skill in VR scenarios was a concrete and step-by-step way to help them apply these techniques in real life (n=7). The participants reported that compared to computer-based systems, this VR-based system is more engaging, and the use of head-mounted virtual goggles effectively isolates distractions from the environment, enhancing their focus during training (n=2).
“It allowed me to better understand how to analyze or use this skill in an immersive way. Simply having the knowledge and immediately analyzing it on my own might not be that effective.” (P10)
With computer, there are many external interferences that make it difficult to concentrate. However, these VR glasses provided a fully immersive experience, you can truly immerse yourself and focus on your own feelings in that moment. (P06)
Some participants mentioned that the self-guided format of VR-STINAT, which does not require the actual presence of a psychotherapist, allowed them to feel more relaxed and at ease, and to experience self-directed learning (n=2).
“VR is more comfortable and freer because it doesn’t involve facing a real person. It allows for more freedom and relaxation.” (P19)
3.2.4 Difficulties and suggestions for improvement
Participants encountered several difficulties while using VR-STINAT, including experiencing multiple virtual training scenarios in a short time, which made it difficult for their emotional responses to keep up (n=2), and finding that the VR scenarios did not match their current mood, thus failing to evoke emotional responses effectively (n=2).
“My emotions couldn’t keep up because I experienced a few days of life in just a few minutes.” (P01)
“It felt like watching a story … I found that it didn’t match my current mood very well.” (P20)
Participants also provided suggestions for improving the system, including enriching the existing VR scenarios and providing more options (n=7), increasing the quantity, sensitivity, accuracy, and variety of human-computer interactions (n=5), and offering more personalized design in the training process and guidance (n=5).
“The scenes and storylines could be more diverse.” (P02)
“There could be more interaction, such as interaction with the virtual therapist.” (P18)
“The interaction was a bit slow sometimes, and the operation needs to be more responsive.” (P03)
“It would be way easier if I could control it just by speaking.” (P06)
“It would be better if the first part were more detailed, with more examples and analyses. People with stronger comprehension skills might be fine, but those with weaker comprehension might find it difficult to understand.” (P17)
4 Discussion
To the best of our knowledge, this preliminary mixed-methods study represents the first attempt to investigate the feasibility of a VR-based self-guided training on the identification of NAT for depression. The effectiveness, safety, and acceptability of VR-STINAT were found to be favorable among the healthy population. This study addresses the limitations of NAT identification training in existing digital CR interventions, expanding the scope of VR-assisted psychotherapy for depression.
4.1 Effectiveness
Our quantitative and qualitative data both indicate the effectiveness of VR-STINAT in training participants to identify their NAT. After training, participants demonstrated a higher level of proficiency in identifying NAT in their homework and a better understanding of cognitive theory, surpassing previous research on APP intervention conducted in non-clinical populations (13). Participants reported that VR-STINAT facilitated their acquisition and utilization of NAT identification technique, as well as enhanced their awareness of the impact of AT on emotions following an event. To date, no other studies have employed VR for self-guided training aimed at identification of NAT associated with depression. Our research fills this gap in the literature.
Aligned with the theory of situated learning (48), participants perceived this system as facilitating contextualized learning and experiential practice, making abstract theoretical knowledge more concrete, thereby enhancing the practical application of the technology. Secondly, participants mentioned that the VR scenarios in this training effectively elicit their emotional responses. Emotional arousal indicates the activation of cognitive schemas, which is a prerequisite for identification of AT and plays a pivotal role in facilitating the acquisition of CR techniques and reaching the desired outcomes (11, 12). In addition, the completely self-guided training format offers participants a non-judgmental and secure environment conducive to the expression of their authentic NAT rather than processed ones (6).
The homework compliance of this study was higher compared to previous studies that implemented CBT interventions digitally, face-to-face, or via telephone (49–52). Several participants proactively planned to continue practicing the NAT identification skill in real-life scenarios even before the homework was assigned. The challenge of identifying scenarios that necessitate the use of CR techniques is a prevalent factor contributing to clients’ discontinuation of utilization (53). VR-STINAT provides a range of typical scenarios that can induce NAT, thereby facilitating the participants’ acquisition of knowledge on when and how to employ this technique. Following the training, several participants summarized the potential application scenarios for this technique. Furthermore, the training necessitated active participation from the participants, thereby fostering an enhanced self-efficacy and sense of accomplishment, consequently resulting in increased skill use quantity and frequency (54).
4.2 Acceptability and safety
The VR-STINAT demonstrated high acceptance rates among the healthy population. The findings of this study align with previous studies combining VR with psychotherapies (55, 56). Most participants reported the interface of VR-STINAT to be clear, concise, user-friendly, and easy to learn, demonstrating a high level of usability. Most participants showed a positive attitude towards the use of VR-STINAT, considering it novel and interesting, as well as beneficial for mental health. They also perceived VR-STINAT as a professionally designed and scientifically grounded approach, suitable for both healthy individuals and those at high risk, thereby indicating a certain level of intention to recommend.
Subgroup analysis revealed that participants with depressive symptoms exhibited significantly lower acceptability of this system compared to those without depressive symptoms. The discrepancy may reside in attitude toward using and intention to use, while no subgroup disparity was observed in perceived usefulness and perceived ease of use. Qualitative interviews revealed that participants with depressive symptoms may potentially experience heightened negative emotions within the VR scenarios, or they may encounter difficulties in fully immersing themselves in the VR scenarios due to an excess of negative thoughts of themselves, leading to a relatively unfavorable disposition towards the VR-STINAT.
The physiological safety of the VR-STINAT was comparable to that observed in previous studies on VR (57). The most common adverse reactions were fatigue and tenderness in the head and face, which can be attributed to the VR headset and prolonged training duration. No participant discontinued the use of VR-STINAT due to adverse reactions, and reported discomforts were effectively alleviated following a 15-20 minute session using a recliner chair and eye patches for relieving eye fatigue. Among the two participants who reported problematic symptoms, one had recently completed a full day of work, suggesting that their discomfort might not be unrelated to their pre-intervention state. Therefore, future training sessions should be scheduled to avoid times when participants may be experiencing discomfort. Additionally, it is recommended to record SSQ scores as a baseline measure prior to the intervention.
A few participants reported intense experience of emotional distress. Previous studies have suggested that activation of negative cognition may result in a transient exacerbation of depressive symptoms, and this temporary deterioration is positively associated with treatment outcomes upon completion (29). Additional psychological techniques are still necessary to address the negative emotions experienced by participants post-training. Therefore, VR-STINAT may serve as a supplementary tool for CR intervention.
4.3 Suggestions for improvement
The VR-STINAT still has potential for further improvement. First, participants proposed an increase in the availability of diverse VR scenarios for their selection. The current VR scenarios primarily emphasize achievement-related events, rendering them particularly suitable for autonomous individuals. Conversely, sociotropic individuals may exhibit a greater propensity to experience emotional reactions and NAT triggered by negative interpersonal events (58).
Furthermore, the participants proposed that the richness and comfort of human-computer interaction can be further enhanced, for instance, through voice command. In addition, regarding training process and guidance, some participants exhibited a preference for more comprehensive instructions, while others leaned towards a more succinct approach. Therefore, it may be worth considering the division and refinement of modules within the training to offer a personalized training experience.
Moreover, participants mentioned the challenge of synchronizing emotional reactions when exposed to multiple VR scenarios within a limited timeframe, stemming from the temporal inconsistency between the VR environment and the real world. The factor of time should be taken into account when constructing VR scenarios in the future.
4.4 Symptoms of depression
The results of our quantitative analysis suggest that, after controlling for age, the VR-STINAT effectively mitigates depressive symptoms. Participants reported that the training and post-training homework facilitated their comprehension of emotions and NAT, promoted cognitive reflection, and fostered greater self-acceptance of both themselves and their emotions.
Previous studies have shown that self-monitoring of emotions and thoughts can foster adaptive self-attention and self-awareness, augment self-efficacy, subsequently contributing to the amelioration of depression (59). Previous studies that employed VR to alleviate depression were predominantly based on Erikson’s psychological theory, mindfulness, exercise, and behavioral activation [24]. However, no research has yet explored the potential of integrating NAT identification technique within VR for depression (25).
4.5 Limitations and future research
Several limitations should be considered when interpreting the results. First, this study is a small exploratory feasibility study. In consideration of ethical concerns pertaining to the safety of emerging technologies, this study specifically targeted a sample of healthy individuals who also experience NAT, thereby constraining the generalizability of the findings to clinical population. The feasibility and effectiveness of VR-STINAT in patients with depression have been assessed through a subsequent randomized controlled trial conducted in a larger sample, and the findings will be independently published in another article (Yang YQ, et al. Self-Service Virtual Reality-Based Psychotherapy for the Treatment of Mild to Moderate Depressive Disorders: A Randomized Controlled Trial). Secondly, the construction of VR scenarios in this system was based on the NAT-evoking scenarios reported by patients with depression in our previous studies. However, the representativeness of these scenarios in the depressed population remains unverified and necessitates further studies to establish their reliability and validity. Finally, future research should integrate VR-STINAT as an auxiliary tool into CR interventions to evaluate its effectiveness and cost-efficiency among individuals with depression.
This study represents the first attempt to employ VR for delivering self-guided training on identification of NAT, and to explore its feasibility through a mixed-methods approach. The findings indicate that the VR-STINAT demonstrated high effectiveness, acceptability, and safety among healthy individuals, showing potential as an auxiliary tool for CR interventions. This study enriches the research on VR-assisted CR interventions for depression and offers valuable insights for exploring novel models of CR interventions for depression. CR is one of the key psychological techniques for depression, and future research on VR-based CR interventions holds potential for enhancing the efficacy and accessibility of mental health services for depression.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Shanghai Mental Health Center (2019-51C2). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BY: Writing – original draft, Conceptualization, Data curation, Formal analysis. CxL: Formal analysis, Writing – original draft. YY: Data curation, Writing – review & editing. BS: Formal analysis, Writing – review & editing, Conceptualization. CZ: Supervision, Writing – review & editing. CbL: Funding acquisition, Project administration, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the National Key Research and Development Program of China (Grant No. 2018YFC2001605) and the long term efficacy evaluation of psychotherapy intervention in schizophrenia(2021-QH-01).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1479207/full#supplementary-material
References
1. Ciharova M, Furukawa TA, Efthimiou O, Karyotaki E, Miguel C, Noma H, et al. Cognitive restructuring, behavioral activation and cognitive-behavioral therapy in the treatment of adult depression: A network meta-analysis. J Consulting Clin Psychol. (2021) 89:563–74. doi: 10.1037/ccp0000654
2. Beck J. Cognitive Behavior Therapy: Basics and Beyond. 2nd ed. Beijing: China Light Industry Press Ltd (2013).
3. Hemming L, Haddock G, Shaw J, Pratt D. Alexithymia and its associations with depression, suicidality, and aggression: an overview of the literature. Front Psychiatry. (2019) 10:203. doi: 10.3389/fpsyt.2019.00203
4. Liu Y, Zhang F, Wang Z, Cao L, Wang J, Na A, et al. Overgeneral autobiographical memory at baseline predicts depressive symptoms at follow-up in patients with first-episode depression. Psychiatry Res. (2016) 243:123–7. doi: 10.1016/j.psychres.2016.06.029
5. A-Tjak JGL, Davis ML, Morina N, Powers MB, Smits JAJ, Emmelkamp PMG. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother Psychosomatics. (2015) 84:30–6. doi: 10.1159/000365764
6. Beck J. Cognitive Theraoy for Challenging Problems: What to Do When the Basics Don't Work. Beijing: China Light Industry Press Ltd (2014).
7. Mohr DC, Ho J, Duffecy J, Baron KG, Lehman KA, Jin L, et al. Perceived barriers to psychological treatments and their relationship to depression. J Clin Psychol. (2010) 66:394–409. doi: 10.1002/jclp.20659
8. Lu J, Xu X, Huang Y, Li T, Ma C, Xu G, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2021) 8:981–90. doi: 10.1016/S2215-0366(21)00251-0
9. Cuijpers P, Noma H, Karyotaki E, Cipriani A, Furukawa TA. Effectiveness and acceptability of cognitive behavior therapy delivery formats in adults with depression: A network meta-analysis. JAMA Psychiatry. (2019) 76:700–7. doi: 10.1001/jamapsychiatry.2019.0268
10. Bolinski F, Etzelmüller A, De Witte NAJ, Beurden C, Debard G, Bonroy B, et al. Physiological and self-reported arousal in virtual reality versus face-to-face emotional activation and cognitive restructuring in university students: A crossover experimental study using wearable monitoring. Behav Res Ther. (2021) 142:103877. doi: 10.1016/j.brat.2021.103877
11. Hofmann SG, Asmundson GJG, Beck AT. The science of cognitive therapy. Behav Ther. (2013) 44:199–212. doi: 10.1016/j.beth.2009.01.007
12. Samoilov A, Goldfried MR. Role of emotion in cognitive-behavior therapy. Clin Psychology-science Practice. (2006) 7:373–85. doi: 10.1093/clipsy.7.4.373
13. Stiles-Shields C, Montague E, Lattie EG, Schueller SM, Kwasny MJ, Mohr DC. Exploring user learnability and learning performance in an app for depression: usability study. JMIR Hum Factors. (2017) 4:e18. doi: 10.2196/humanfactors.7951
14. Domhardt M, Steubl L, Boettcher J, Buntrock C, Karyotaki E, Ebert DD, et al. Mediators and mechanisms of change in internet- and mobile-based interventions for depression: A systematic review. Clin Psychol Review. (2021) 83:101953. doi: 10.1016/j.cpr.2020.101953
15. Li L, Yu F, Shi D, Shi J, Tian Z, Yang J, et al. Application of virtual reality technology in clinical medicine. Am J Transl Res. (2017) 9:3867–80.
16. Dellazizzo L, Potvin S, Luigi M, Dumais A. Evidence on virtual reality-based therapies for psychiatric disorders: meta-review of meta-analyses. J Med Internet Res. (2020) 22:e20889. doi: 10.2196/20889
17. Kim S, Kim E. The use of virtual reality in psychiatry: A review. Soa Chongsonyon Chongsin Uihak. (2020) 31:26–32. doi: 10.5765/jkacap.190037
18. Mishkind MC, Norr AM, Katz AC, Reger GM. Review of virtual reality treatment in psychiatry: evidence versus current diffusion and use. Curr Psychiatry Rep. (2017) 19:80. doi: 10.1007/s11920-017-0836-0
19. Kocur M, Dechant M, Wolff C, Nothdurfter CWetter TC, Rupprecht R, et al. Computer-assisted avatar-based treatment for dysfunctional beliefs in depressive inpatients: A pilot study. Front Psychiatry. (2021) 12:608997. doi: 10.3389/fpsyt.2021.608997
20. Baukal CE, Ausburn FB, Ausburn LJ. A proposed multimedia cone of abstraction: updating a classic instructional design theory. J Educ Technology. (2013) 9:15–24. doi: 10.26634/jet.9.4.2129
21. Abich JI, Parker J, Murphy JS, Eudy M. A review of the evidence for training effectiveness with virtual reality technology. Virtual Reality. (2021) 25:919–33. doi: 10.1007/s10055-020-00498-8
22. Zitzmann NU, Matthisson L, Ohla H, Joda T. Digital undergraduate education in dentistry: A systematic review. Int J Environ Res Public Health. (2020) 17:3269. doi: 10.3390/ijerph17093269
23. Doo YM. A problem in online interpersonal skills training: do learners practice skills? Open Learning: J Open Distance e-Learning. (2006) 21:263–72. doi: 10.1080/02680510600953252
24. Baghaei N, Chitale V, Hlasnik A, Stemmet L, Liang H, Porter R. Virtual reality for supporting the treatment of depression and anxiety: scoping review. JMIR Ment Health. (2021) 8:e29681. doi: 10.2196/29681
25. Reategui-Rivera CM, Villarreal-Zegarra D, de la Cruz-Torralva K, Díaz-Sánchez P, Finkelstein J. Immersive technologies for depression care: scoping review. JMIR Ment Health. (2024) 11:e56056. doi: 10.2196/56056
26. Botella C, Osma J, Palacios AG, Guillén V, Baños R. Treatment of complicated grief using virtual reality: a case report. Death Stud. (2008) 32:674–92. doi: 10.1080/07481180802231319
27. Levitt HM, Bamberg M, Creswell JW, Frost DM, Josselson R, Suárez-Orozco C. Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report. Am Psychol. (2018) 73:26–46. doi: 10.1037/amp0000151
28. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. (2013) 48:2134–56. doi: 10.1111/1475-6773.12117
29. Hayes AM, Feldman GC, Beevers CG, Laurenceau JP, Cardaciotto LA, Lewis-Smith J. Discontinuities and cognitive changes in an exposure-based cognitive therapy for depression. J Consulting Clin Psychol. (2007) 75:409–21. doi: 10.1037/0022-006X.75.3.409
30. Bian CD, He XY, Qian J, Wu WY, Li CB. The reliability and validitu of a modified patient health questionnnaire for screening depressice syndrome in general hospital outpaitients (in Chinese). J Tongji Univ (Medical Science). (2009) 30:5.
31. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59 Suppl 20:22–33.
32. Xie AL, Chen JY. Determining sample size in qualitative research: saturation, its conceptualization, operationalization and relevant debates. J East China Normal Univ (Educational Sciences). (2021) 39:15–27. doi: 10.16382/j.cnki.1000-5560.2021.12.002
33. Paas F, van Gog T. Optimising worked example instruction: Different ways to increase germane cognitive load. Learn Instruction. (2006) 16:87–91. doi: 10.1016/j.learninstruc.2006.02.004
35. Lindner P, Rozental A, Jurell A, Reuterskiöld L, Andersson G, Hamilton W, et al. Experiences of gamified and automated virtual reality exposure therapy for spider phobia: qualitative study. JMIR Serious Games. (2020) 8:e17807. doi: 10.2196/17807
36. Corporation V, Steam VR. (2020). Available online at: https://steamvr.com/en/ (Accessed Octobor 05,2024).
37. Hundt NE, Mignogna J, Underhill C, Cully JA. The relationship between use of CBT skills and depression treatment outcome: a theoretical and methodological review of the literature. Behav Ther. (2013) 44:12–26. doi: 10.1016/j.beth.2012.10.001
38. Neimeyer RA, Feixas G. The role of homework and skill acquisition in the outcome of group cognitive therapy for depression - Republished article. Behav Ther. (1990) 47:747–54. doi: 10.1016/j.beth.2016.08.013
39. Zhang XX, Ke XX, Zhang LR, Jiang JH, Wang YM. Validity and reliability of the Chinese version of the Simulator Sickness Queationnnaire in college students. Chin Ment Health J. (2022) 36:5.
40. Tanner BA. Validity of global physical and emotional SUDS. Appl Psychophysiol Biofeedback. (2012) 37:31–4. doi: 10.1007/s10484-011-9174-x
41. Manis KT, Choi D. The virtual reality hardware acceptance model (VR-HAM): Extending and individuating the technology acceptance model (TAM) for virtual reality hardware. J Business Res. (2019) 100:503–13. doi: 10.1016/j.jbusres.2018.10.021
42. Wang X, Zhang QQ, Yan BY, Ni SH, Peng KP. The reliability and validity of Chinese version of igroup presense questionnaire. Chin J Clin Psychol. (2019) 2):4. doi: 10.16128/j.cnki.1005-3611.2019.02.016
43. Migoya-Borja M, Delgado-Gómez D, Carmona-Camacho R, Porras-Segovia A, López-Moriñigo JD, Sánchez-Alonso M, et al. Feasibility of a virtual reality-based psychoeducational tool (VRight) for depressive patients. Cyberpsychol Behav Soc Netw. (2020) 23:246–52. doi: 10.1089/cyber.2019.0497
44. Falconer CJ, Cutting P, Bethan Davies E, Hollis C, Stallard P, Moran P. Adjunctive avatar therapy for mentalization-based treatment of borderline personality disorder: a mixed-methods feasibility study. Evid Based Ment Health. (2017) 20:123–7. doi: 10.1136/eb-2017-102761
45. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:101 – 77. doi: 10.1191/1478088706qp063oa
46. Ajzen I. The theory of planned behavior. Organizational Behav Hum Decision Processes. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-T
47. Davis FD. A technology acceptance model for empirically testing new end-user information systems: Theory and results. USA: Massachusetts Institute of Technology (1986).
48. Cui YH, Wang ZN. How does learning happen:interpritation of situated learning (in Chinese). Educ Sci Res. (2012) 7):5. doi: 10.3969/j.issn.1009-718X.2012.07.005
49. Yang BX, CB LI. Progression in smartphone applications in the psychotherapy of depression (in Chinese). Chin J Psychiatry. (2020) 53:4. doi: 10.3760/cma.j.cn113661-20200428-00201
50. Kazantzis N, Whittington C, Zelencich L, Kyrios M, Norton PJ, Hofmann SG. Quantity and quality of homework compliance: A meta-analysis of relations with outcome in cognitive behavior therapy. Behav Ther. (2016) 47:755–72. doi: 10.1016/j.beth.2016.05.002
51. de Graaf LE, Huibers MJH, Riper H, Gerhards SAH, Arntz A. Use and acceptability of unsupported online computerized cognitive behavioral therapy for depression and associations with clinical outcome. J Affect Disord. (2009) 116:227–31. doi: 10.1016/j.jad.2008.12.009
52. Aguilera A, Ramos Z, Sistiva D, Wang Y, Alegria M. Homework completion via telephone and in-person Cognitive Behavioral Therapy among Latinos. Cogn Ther Res. (2018) 42:340–7. doi: 10.1007/s10608-017-9884-3
53. Eilert N, Timulak L, Duffy D, Earley C, Enrique A, Kennedy P, et al. Following up internet-delivered cognitive behaviour therapy (CBT): A longitudinal qualitative investigation of clients' usage of CBT skills. Clin Psychol Psychotherapy. (2022) 29:200–21. doi: 10.1002/cpp.2619
54. Simons PRJ. Transfer of learning: paradoxes for learners. Int J Educ Res. (1999) 31:577–89. doi: 10.1016/S0883-0355(99)00025-7
55. Paul M, Bullock K, Bailenson J. Virtual reality behavioral activation for adults with major depressive disorder: feasibility randomized controlled trial. JMIR Ment Health. (2022) 9:e35526. doi: 10.2196/35526
56. Stamou G, Garcia-Palacios A, Woodford BJ, Suso-Ribera C, Botella C. The combination of cognitive-behavioural therapy with virtual reality for the treatment of postnatal depression in a brief intervention context: A single-case study trial. J Healthc Eng. (2021) 2021:5514770. doi: 10.1155/2021/5514770
57. Kim J, Jung YH, Shin YB, Kim MK, Eom H, Kim E, et al. Feasibility of a virtual reality-based interactive feedback program for modifying dysfunctional communication: a preliminary study. BMC Psychol. (2020) 8:50. doi: 10.1186/s40359-020-00418-0
58. Zettle RD, Herring EL. Treatment utility of the sociotropy/autonomy distinction: Implications for cognitive therapy. J Clin Psychol. (1995) 51:280. doi: 10.1002/1097-4679(199503)51:2<280::AID-JCLP2270510219>3.0.CO;2-J
Keywords: virtual reality, cognitive behavioral therapy, cognitive restructuring, negative automatic thoughts, feasibility
Citation: Yang B, Liao C, Yang Y, Shi B, Zhang C and Li C (2024) A virtual reality-based self-guided training on identification of negative automatic thoughts in healthy adults: a mixed-methods feasibility study. Front. Psychiatry 15:1479207. doi: 10.3389/fpsyt.2024.1479207
Received: 11 August 2024; Accepted: 31 October 2024;
Published: 27 November 2024.
Edited by:
Khaldoon Dhou, Texas A&M University Central Texas, United StatesReviewed by:
Michele Procacci, Terzo Centro di Psicoterapia, ItalyRaquel Simões de Almeida, Polytechnic of Porto, Portugal
Copyright © 2024 Yang, Liao, Yang, Shi, Zhang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caidi Zhang, Y2FpZGlfemhhbmcyMDIzQDE2My5jb20=; Chunbo Li, Y2h1bmJvX2xpQDE2My5jb20=
†These authors have contributed equally to this work and share first authorship