 Luigi Giuliani1*†
Luigi Giuliani1*† Paola Bucci1†
Paola Bucci1† Raffaele Bracalenti2*
Raffaele Bracalenti2* Giulia Maria Giordano1
Giulia Maria Giordano1 Matteo Conenna1
Matteo Conenna1 Giulio Corrivetti3*
Giulio Corrivetti3* Davide Palumbo1Andrea Dell’Acqua3
Davide Palumbo1Andrea Dell’Acqua3 Federica Piras4Giovanna Storti5Verdiana Abitudine1Roberta Di Lieto3Letizia Sandolo3Chiara Schiavitelli2Alice Mulè3Pierpaola D’Arista3
Federica Piras4Giovanna Storti5Verdiana Abitudine1Roberta Di Lieto3Letizia Sandolo3Chiara Schiavitelli2Alice Mulè3Pierpaola D’Arista3 Armida Mucci1
Armida Mucci1 Silvana Galderisi1
Silvana Galderisi1- 1Department of Mental and Physical Health and Preventive Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy
- 2Istituto Psicoanalitico per le Ricerche Sociali (IPRS), Rome, Italy
- 3Department of Mental Health of Salerno, Local Health Center of Salerno, Salerno, Italy
- 4Neuropsychiatry Laboratory, Department of Clinical Neuroscience and Neurorehabilitation, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Santa Lucia Foundation, Rome, Italy
- 5Integrated Area for Fragility, Local Health Center of Salerno, Salerno, Italy
Introduction: In recent years, the increasing presence of refugees and asylum seekers displaced from their country of origin, determined significant social, economic, humanitarian and public health implications in host countries, including Italy. These populations are exposed to several potential stressful experiences which make them vulnerable to psychological distress. In fact, the majority of studies addressing the topic found a higher prevalence of mental disorders, especially post-traumatic stress disorder and major depressive disorder, in refugees and asylum seekers with respect to the general population. However, heterogeneous prevalence rates have been reported among studies, due to methodological factor as well as to the impact of a variety of risk factors related to stressful experiences lived in the country of origin, during the migration journey and in the host country.
Objectives: The aim of the present study was to assess the prevalence of the main psychiatric diagnoses in a large group of adult refugees and asylum seekers (N=303) in the reception centers of two provinces of the Campania region, as well as to investigate the impact of potential risk factors on the occurrence of psychiatric disorders.
Methods: The diagnosis of psychiatric disorders and the identification of subjects at high risk to develop psychosis were carried out by means of structured diagnostic interviews. The following variables were explored as potential risk/protective factors to the occurrence of psychiatric disorders: socio-demographic variables, migration status (refugees/asylum seekers) and characteristics of the reception center,assessed by means of an ad hoc questionnaire; cognitive indices assessed by using standardized neuropsychological tests; traumatic experiences and level of political terror in the country of origin, assessed by means of reliable and valid self-report questionnaires.
Results: At least one mental disorder was found in 29.7% of the sample. Most prevalent diagnoses were depressive disorders, anxiety disorders and PTSD. Women showed, with respect to men, a higher prevalence of anxiety disorders, higher trauma levels, and came from more at-risk countries. Higher trauma levels, better cognitive abilities and unemployment and refugee status were associated to the presence of a current psychiatric disorder in the whole sample.
Conclusions: Our findings showed a higher prevalence of depressive disorders and PTSD in the sample of refugees and asylum seekers with respect to the general population and highlighted the role of potential risk factors whose identification may guide the implementation of preventive strategies and early treatments in these people.
Introduction
Migration is a persistent phenomenon since the 19th century (1). At the end of 2022, the United Nations estimated the number of international migrants worldwide at 295 million, corresponding to 3.6% of the world population (2). Out of these, 108.4 million are forced migrants and, in particular, 29.4 million are refugees, 5.4 asylum seekers, and 62.5 are internal displaced persons, while the remaining 11% are Palestinians refugees or Venezuelan displaced abroad. An even broader migration pattern has been reported in Italy, due to its geographical position. As a matter of fact, at the end of 2023, Italy registered the entrance of 157,652 people, with an increase of migration flows as compared to 2022 and 2021, when 105,131 and 67,477 migrants respectively arrived in the country (3).
Refugees and asylum seekers are exposed to several potential stressful and traumatic experiences which can occur before migration, during the migration journey, as well as after the arrival in the host nation, which make them vulnerable to psychological distress and to the occurrence of mental disorders (4). One review and one meta-analysis on the topic found that refugees and asylum seekers, with respect to the general population, have a higher overall lifetime prevalence of post-traumatic stress disorder (PTSD) and major depressive disorder but not of anxiety disorders and psychosis (5, 6). However, discrepant findings have also been reported, such as a higher prevalence reported also for anxiety disorders (7), lack of difference in the prevalence of depression (8) and higher prevalence of psychosis (9). A constant issue emerging from reviews and meta-analyses addressing this topic is the wide variability in the prevalence rate of mental disorders among studies (5–8, 10, 11). The same heterogeneous picture arises from studies carried out in samples of refugees and asylum seekers hosted in Italian regions, in which prevalence rates ranged from 17% to 40% for PTSD (12–16), from 7% to 15% for depressive disorders or depressive symptoms (13, 15–17), from 12% to 48% for anxiety disorders or anxiety symptoms (13, 16), and from 11.8% to 30.8% for psychosis (16, 18).
Factors responsible of such a variability can be grouped in two main categories: a) methodological differences among studies and b) heterogeneity among socio-demographic characteristics and experiences of refugees and asylum seekers, which represent risk factors or mediators in the development of certain mental disorders.
Methodological factors mainly impacting prevalence rates of mental disorders in refugees and asylum seekers include: 1) sample size, as studies including more than 200 subjects show lower rates of mental disorders and lower variability among results (19, 20), although the impact of the population dimension on prevalence rates seems limited to PTSD and depression and does not impact anxiety disorders (6); 2) sampling methods, with studies using nonrandom sampling showing higher rates of PTSD and depression (20); 3) type of assessment instruments, since lower rates of mental disorders are reported in studies using structured diagnostic interviews vs. those using self-report questionnaires or screening tools (6, 11, 19, 21); 4) lack of cross-cultural adaption and/or validation of diagnostic and assessment tools used in some studies, which may generate misunderstanding of the situations presented as exemplification of distress or to describe symptoms (7, 19); 5) lack of cultural mediators assistance in the diagnostic assessment, which is reported associated to a lower frequency of mental disorders (6); 6) lack of distinction in many studies between refugees and asylum seekers, although such differentiation has been recommended by the WHO (22), since the two groups do not receive the same level of protection and benefits in the host country and may have been exposed to different experiences of stressors in their country of origin (21, 23).
In addition to the above-mentioned potential methodological biases, a true heterogeneity in prevalence rates among different populations of refugees and asylum seekers may be related to differences on factors impacting the development of mental disorders, such as some socio-demographic characteristics and/or the experiences lived before, during and after the migration journey. Among-socio-demographic variables, female gender and higher levels of education have been found associated to higher risk to develop psychiatric disorders in these populations in some but not all studies; in particular, higher prevalence rates of PTSD (6) or anxiety (10) have been reported, as well as a lack of gender differences (24), while higher levels of education have been found to affect prevalence rate of depression (8) or psychiatric symptoms (25). Pre-migration factors related to the country of origin, and to the exposure to potential traumatic events, such as torture and violence, violation of human rights, presence of war conflicts and their duration, as well as separation from family or close friends, have been reported among factors increasing the risk to develop mental disorders in refugees and asylum seekers (4, 10, 14, 21, 26–29). Risk factors related to traumatic events occurring during the migration journey include physical harm, violence and extortion or having witnessed violent events perpetrated on others (4). Post-migration experiences may also represent important risk/protective factors for the development of mental disorders. They include: displacement duration, which has been found associated to lower rates of depression or PTSD in some studies (10, 11) but not in others (6); unemployment, financial difficulties, weak social network and weak social integration, discrimination and uncertainty regarding residence status, which all result associated to higher rates of mental disorders (19, 21, 30, 31). Post-migration factors are often different depending on the host country; this may be related to differences among host countries such as immigration policy strategies (32, 33), level of income – which may have an impact on some of the above-reported risk factors such as unemployment and financial difficulties, and public attitudes toward immigration among countries (34). In line with the latter hypothesis, in a sample of refugees and asylum seekers living in Genoa (Nort-West of Italy), community resilience was identified among protective factors against the effects of mental disorders on well-being (17).
Within this framework, the management of the mental health of refugees and asylum seekers is an important issue for the mental health policies of the host countries, which needs to be considered in the development and organization of mental health interventions and treatment services. In addition, it is crucial to focus on the identification and management of potential risk factors in order to reduce the prevalence rate of mental disorders in refugees and asylum seekers by adopting early interventions and preventive strategies representing main goals to be implemented in psychiatry (35–41). Given the broad migration pattern in Italy and the potential impact of specific aspects of the host countries in the development of psychiatric disorders in refugees and asylum seekers, it could be of interest to assess frequency and correlates of psychiatric disorders in forced migrants hosted in an Italian catchment area. Findings reported in the specific context of Italy didn’t provide a clear and reliable picture so far as they were in part affected by the above-reported methodological limitations such as the inclusion of relatively small sample size (12, 14), the definition of diagnoses by means of self-report questionnaires (14, 16), the retrospective study design (15, 16), the assessment of prevalence rates only for some psychiatric disorders (12, 14) or only in subgroups of refugees and asylum seekers such as those with psychological distress as assessed by means of a self-report questionnaire (12). In the light of these research gaps, in the present study we investigated prevalence rates of main psychiatric disorders and their risk/protective factors in a sample of refugees and asylum seekers hosted in two Campania provinces, Salerno and Avellino. We also investigated the prevalence of psychotic disorders, to offer a contribution in clarifying this point – given the discrepant findings provided so far by the few studies exploring it in the Italian context (16, 18) – as well as the prevalence of subjects at high-risk for psychosis, to explore the need to implement prevention strategies for psychotic disorders. Main methodological biases reported in the literature were addressed, by including a large sample size, assessing psychiatric diagnoses by means of a structured diagnostic interview and distinguishing between refugees and asylum seekers. Variables investigated as potential protective/risk factors were chosen among those more frequently reported in association with psychiatric disorders in refugees and asylum seekers in the above-reported literature, and included socio-demographic indices, migration status (refugees/asylum seekers), characteristics of the reception center, trauma levels and political terror in the country of origin. In addition, the impact of cognitive functioning on the occurrence of psychiatric disorders was explored, particularly with regard to cognitive domains whose deficit may have an impact on psychosocial functioning (42, 43). We aimed at addressing the following questions: 1) Are the prevalence rates of psychiatric disorders in refugees and asylum seekers hosted in Italy higher with respect to the general population? If yes, is this true for all psychiatric diagnoses or just for some of them? We hypothesized to find higher prevalence rates at least for some of the explored diagnoses, such as depression and PTSD, as reported in the majority of papers (5, 6), but probably with lower percentages than those reported in studies biased by small sample size or by the use of self-report questionnaires to perform diagnoses. 2) Is the occurrence of psychiatric disorders in refugees and asylum seekers hosted in Italy influenced by risk factors such as socio-demographic characteristics, cognitive functioning or stressful events occurring in different stages of the migration process? We expected to confirm the associations of psychiatric diagnosis with the risk factors most frequently reported in the literature, such as female gender and levels of trauma, the latter especially in refugees vs. asylum seekers, since the formers may have been exposed to more stressful experiences in their country of origin.
Methods
Subjects
Study participants were recruited in second levels reception centers localized in two Campania provinces (Salerno and Avellino) hosting, altogether, about 1,200 refugees and asylum seekers. According to the Italian Law No. 173/2020, the reception centers are called “Reception and integration system” (SAI), which replaced the “Protection system for holders of international protection and for unaccompanied foreign minors” (SIPROIMI) which, in turn, replaced the “Protection system for asylum seekers and refugees” (SPRAR). Subjects were also recruited in “Extraordinary Reception Centers” (CAS), which are temporary facilities to be opened in case of “substantial and close arrivals of applicants that cannot be accommodated through the ordinary system” (Legislative Decree 142/2015, art. 11). The aforementioned legislation also applies to the reception centers of the two provinces involved in the present study. Therefore, the asylum situation in the region of investigation provides a good representation of that of the entire country.
Inclusion criteria were: at least 18 years of age; ability to provide an informed consent; and adequate language skills (Italian and/or English) for understanding informed consent and study interviews (or, in alternative, presence of a cultural mediator).
All patients signed a written informed consent to participate in the study after receiving a comprehensive explanation of its procedures and goals. Confidentiality was strictly maintained by anonymizing the data and storing it in encrypted files. Access to the data was limited to authorized research personnel, and participants were assured that their personal information would not be shared or linked to their responses. The study was approved by the Ethics Committee of the Integrated Area for Fragility of the Local Health Center of Salerno (approval number 233817 of the 03/10/2019).
Study procedures
Recruitment took place from February 1st, 2020, to October 11, 2021. The adequately trained staff of the reception centers involved in the study, provided to: a) select adults with adequate language skills (Italian and/or English) for understanding informed consent and study interviews questions and to answer them; b) explain the study protocol to the selected subjects; c) invite them to participate in the study. All patients who agreed to be included in the study signed a written informed consent after receiving a further comprehensive explanation of study procedures and goals by the researchers.
Enrolled subjects completed the assessments in two days following the schedule below: collection of socio-demographic and migration status information, psychopathological evaluation and cognitive assessment on day 1; diagnostic evaluation on day 2.
Clinical and psychopathological evaluations
An ad hoc questionnaire was developed in order to collect socio-demographic data (gender, age, education, employment), information on the migration status (refugee/asylum seeker) and type of reception center (less/more than 40 people hosted; placed in an urban center with less/more than 10.000 inhabitants).
The Mini-International Neuropsychiatric Interview (MINI) (44) was used for the diagnosis of mental disorders according to the criteria of DSM-IV and ICD-10. The MINI has shown good internal consistency, with Cronbach’s alpha values ranging between 0.79 and 0.90 across different diagnostic categories.
The identification of subjects at high-risk for psychosis was performed using the Comprehensive Assessment of At-Risk Mental States (CAARMS) (45), a semi-structured clinical interview designed to measure attenuated psychotic symptoms. It consists of 27 items (i.e. “Have you noticed any changes in your thoughts, such as thinking about things that don’t make sense?”) rated in terms of intensity and frequency/duration clustered in 7 subscales: positive symptoms, cognitive change, emotional disturbance, negative symptoms, behavioral change, motor/physical changes, general psychopathology. A CAARMS severity score (total-CAARMS) can be extracted by summing the product of the global rating scale score (0-6, where 0 is no symptoms) and the frequency score (0-6, where 0 = has never occurred) of the subscales. The CAARMS demonstrates excellent internal reliability, with Cronbach’s alpha reported at 0.93.
The Hopkins Symptom Checklist-25 (HSCL-25) (46) is a self-report questionnaire consisting of 25 items (i.e. “In the past week, how often have you felt suddenly scared for no reason?”) and exploring symptom severity with regard to anxiety and depression rated on a 4-point scale (from 1=not at all, to 4= extremely). The total score was used for the assessment of depressive and anxiety symptoms. The HSCL-25 has shown high internal consistency in various populations, with Cronbach’s alpha values ranging from 0.87 to 0.90.
Assessment of traumatic experiences
Traumatic experiences were evaluated with the Harvard Trauma Questionnaire post-traumatic stress checklist (HTQ-16) (47), a self-report questionnaire widely used in refugees and asylum seekers, assessing 16 post-traumatic symptoms (i.e. “Have you had recurrent thoughts or memories of the most hurtful or terrifying events?”) rated on a 4-point scale (from 1=not at all, to 4=extremely). Symptom severity was computed by averaging the 16 scores. The HTQ-16 demonstrates strong internal reliability, with Cronbach’s alpha ranging from 0.89 to 0.92 for the PTSD symptom checklist.
The state inflicted political terror in countries of origin was measured by the Political Terror Scale (PTS) (48), which is an annual measure of political terror in a nation based on a 5-level “terror scale”. A score > 4 indicates the presence of political terror in the country of origin.
Cognitive assessment
To assess global cognition, and to minimize the influence of linguistic, cultural and educational differences, we used 3 subtests of the Wechsler Adult Intelligence Scale fourth edition (WAIS-IV) (49), “block design”, “puzzles”, “matrix reasoning”. Combining together the scores of these three subtests, we obtained the perceptual reasoning index score, representing a measure of one of the main components of human intelligence. The WAIS-IV has demonstrated high internal consistency across its subtests, with Cronbach’s alpha values ranging between 0.88 and 0.97.
The Trail Making Test-A (TMT-A) (50), the Digit Symbol Coding (50) and the Verbal fluency (50) were used to assess speed of processing; the difference between Trail Making Test-B (TMT-B) (50) minus TMT-A score was used as an index of executive functions. The Trail Making Test, digit symbol coding and verbal fluency tasks showed moderate to good internal consistency, with Cronbach’s alpha values reported between 0.70 and 0.90, depending on the population.
Social cognition was assessed by means of the Facial Emotion Identification Test (FEIT) which has shown moderate to good internal consistency, with Cronbach’s alpha reported between 0.75 and 0.85 (51).
Training of the researchers
The training of all the researchers was conducted by expert psychologists and psychiatrists working at the Department of Mental and Physical Health and Preventive Medicine of the University of Campania “Luigi Vanvitelli”. Three psychologists were trained for the neurocognitive assessment, while eight trainees in psychiatry (attending the third or the fourth year of course) were trained for the structured diagnostic interviews (MINI and CAARMS).
The inter-rater reliability was formally evaluated by Cohen’s kappa for the MINI and the CAARMS. An excellent inter-rater agreement was found for both interviews: Cohen’s kappa was 0.92 for the former and 0.81 for the latter.
Statistical analysis
The minimum sample size was calculated setting the critical value associated with the confidence level (Z for 95%) at 1.96, the desired margin of error at 0.05 and the expected prevalence at 0.10–0.15, according to the WHO report on the global prevalence of mental disorders in general population.
The prevalence of mental disorders in the study sample as well as the frequency of each mental disorder were calculated.
All cognitive indices were transformed into z-scores. Composite scores were calculated for global cognition (mean of the 3 WAIS-IV subtests z-scores), for the cognitive domain “Speed of processing” (mean of TMT-A, Symbol Coding and Category fluency z-scores) and for executive functions (TMT-B minus TMT-A z-scores). Values of TMT-A and TMT-B were inverted, because a lower score at these tests correspond to a higher cognitive performance, differently from the other cognitive indices.
Analyses of variance (ANOVA) were performed to investigate group differences between subjects with vs. without at least one psychiatric disorder, between refugees vs. asylum seekers and between men vs. women for the following variables: speed of processing, executive functions, social and global cognition scores, traumatic events, anxious and depressive symptoms. Group differences in the frequency of psychiatric disorders were explored by means of χ² square test.
Pearson’s correlation analyses were conducted to investigate the relationship between HSCL-25 psychopathological index and the other study variables.
A logistic regression analysis was performed to identify factors associated to the presence of current mental disorder. The presence or the absence of a psychiatric diagnosis was selected as dependent variable. Gender, education, occupation status (employed/unemployed), migration status (refugees/asylum seekers), number of people hosted in the reception center (high/low), type of urban center (with high/low number of inhabitants), trauma levels (average score at the HTQ-16), social cognition (FEIT total number of correct answers), cognitive indices and political terror in the country of origin (score > 4 at the Political Terror Scale) were selected as independent variables. Multicollinearity among the independent variables was assessed using the Variance Inflation Factor (VIF). Variables with a VIF greater than 5 were considered to indicate potential multicollinearity. An a priori power analysis was conducted using Cohen’s f² to assess the adequacy of the sample size for detecting medium effect sizes in logistic regression models.
Statistical significance was fixed at p<.05 and SPSS v. 25 software was used for all the above-mentioned analyses.
Results
Characteristics of study sample
We estimated that the minimum sample size should be 139-196 subjects, setting the prevalence of mental disorders in general population respectively at 10 and 15%.
One thousand two hundred people hosted in the CAS or SPRAR/SIPROIMI structures sited in the and Avellino and Salerno provinces were screened. Three hundred and three subjects (241 males, 62 females) met inclusion criteria and were enrolled in the study. Their demographic and clinical characteristics are reported in Table 1. Mean age of the participants was 28 ± 6.58 years, mean education was 9.4 ± 4.11; 103 of them (34%) were employed at the time of the screening (72% of which did menial jobs, mainly farm hands); 246 subjects (81%) were asylum seekers, while 57 (19%) were refugees; 197 subjects (65%) came from countries with a high-risk for traumatic events (conflicts, war, political terror, etc.) as indicated by a score >4 at the Political Terror Scale.

Table 1. Characteristics of study sample (N=303).
Data on the nationality of study participants are provided in Table 2; the most frequent country of origin was Nigeria (41%), followed by Pakistan (28%), Bangladesh and Gambia (9%).
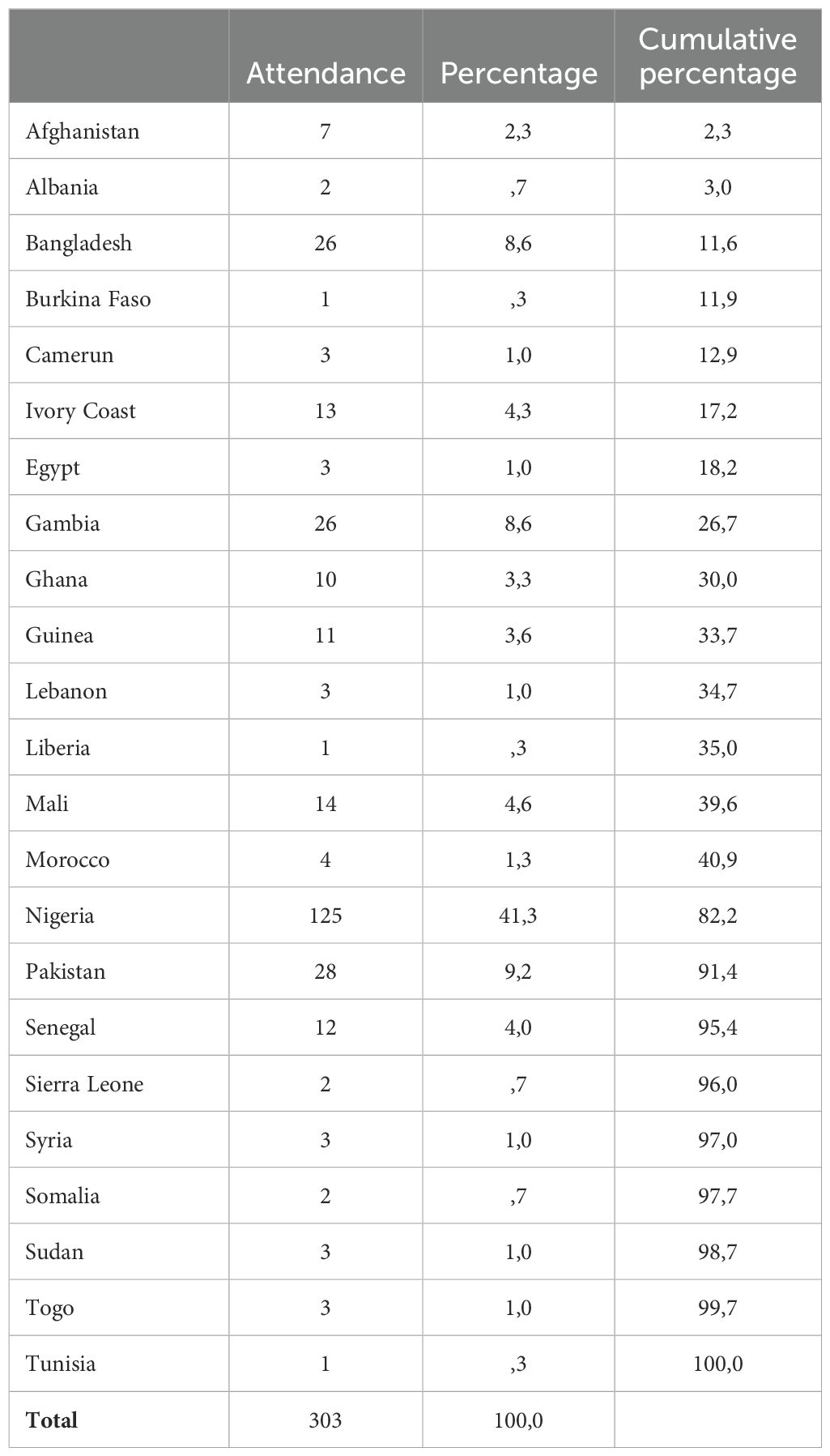
Table 2. Country of origin of study participants.
Frequency of mental disorders in the study sample
Ninety subjects (29.7%) met criteria for a full-blown diagnosis of a mental disorder, as assessed by the MINI, 75 of them (25% of the sample) had a current psychiatric disorder, while the remaining 15 (17%) had only a psychiatric diagnosis in the medical history with no current disorder. Six subjects (2%) resulted at high-risk for developing psychosis.
The most frequent psychiatric diagnoses were major depressive episode (13.2%; 10.2% of which in the medical history and 3% current), followed by panic disorder (6.3%; 5.6% of which lifetime and 0.7% current), PTSD (6%) and generalized anxiety disorder (6%). The prevalence of any depressive disorder was 16.5% and that of any anxiety disorder was 16.2%. Further details on the frequency of psychiatric disorders in the study sample are reported in Table 3.
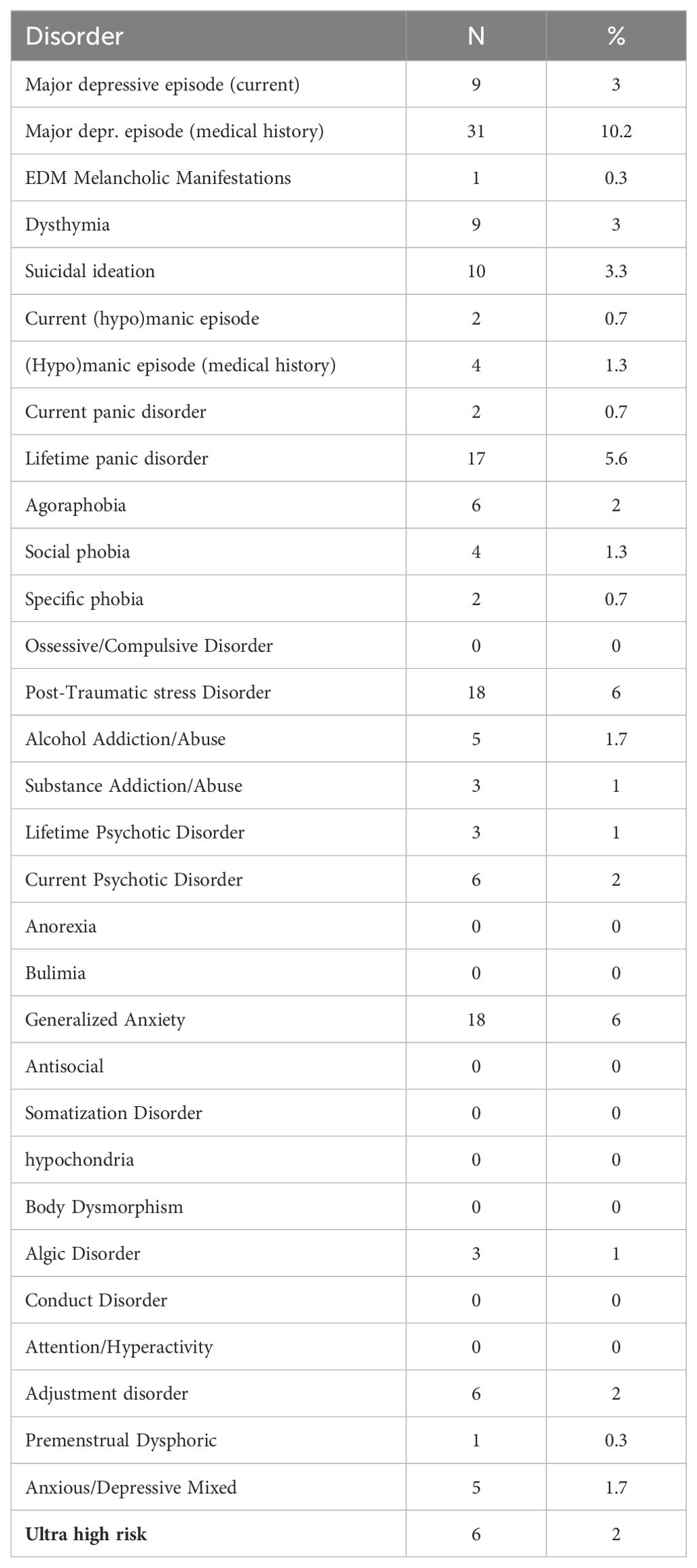
Table 3. Frequency of psychiatric disorders.
Group comparison between subjects with and without psychiatric disorders
Subjects with at least one psychiatric disorder with respect to those with no psychiatric disorders showed higher trauma levels (F=70.59; p<.0001), a better performance on global cognition (F=6.62; p=.011) and social cognition (F=8.22; p=.004), and greater severity of anxiety and depressive symptoms (F=61.84; p<.0001). No significant group difference was found for speed of processing (F=2.41; p=.122), executive functions (F=1.53; p=.192) and political terror scale (F=1.82; p=.178).
Group comparison between refugees and asylum seekers
No difference on the frequency of mental disorders was observed between refugees and asylum seekers (χ²=1.71; p=.19).
Asylum seekers with respect to refugees showed higher levels of trauma (F= 10.65; p=.001), more severe anxiety and depressive symptomatology (F=7.89, p=.005), higher speed of processing (F=5.61, p=.02) and better global cognition (F=4.12; p=.04).
Group comparison between male and female subjects
No gender difference was observed on the frequency of mental disorders (χ²=2.04; p=.153). When considering separately the diagnosis more frequently observed in the whole sample, anxiety disorders resulted significantly more frequent in women than in men (17.7% vs. 8.3%, χ²=4.79; p=.03), while no difference was observed in the prevalence rate of depressive disorders and PTSD (19% vs. 16%, χ²=0.46; p=.50 and 6.4% vs. 5.8%, χ²=0.04; p=.85, respectively). As for rate of employment, a significant difference was observed with less employed women compared to men (χ²=13.18; p<.0001). Moreover, women showed, with respect to men, higher levels of political terror in the country of origin (F=21.04; p<.0001), more severe anxiety and depressive symptoms (F=10.05; p=.002), higher trauma levels (F=4.92; p=.03) and better performance on the test exploring social cognition (F=5.79; p=.02).
Relationship of psychopathology and psychiatric diagnosis with sociodemographic variables, cognitive performance and risk factors for psychiatric disorders
Pearson’s correlation analyses showed that the severity of anxious and depressive symptoms assessed by the HSCL-25 was significantly associated only with the severity of trauma levels, measured with the HTQ-16. No significant associations were found with cognitive indices nor with the political terror scale.
A logistic regression analysis was performed to investigate factors associated with the presence of current mental disorders. Therefore, the 15 subjects who had a psychiatric disorder only in the medical history without any current psychiatric diagnosis were excluded from this analysis. The power analysis revealed that, given the sample size of 288 participants and a significance level of 0.05, the analysis indicated that the power to detect medium-sized effects (f² = 0.15) was sufficient (99.9%). The presence of a current psychiatric diagnosis resulted associated with higher levels of trauma (p<.001), unemployment (p<.008), refugee status (p=.04) and better global cognition (p<.03) (Table 4). Multicollinearity diagnostics using the Variance Inflation Factor (VIF) revealed that only two variables (global cognition and speed of processing) exceeded the critical threshold of 5, suggesting potential multicollinearity. This indicates that the relationship between these two variables could have inflated the association of global cognition with the presence of current mental disorders. Indeed, after having removed the processing speed from the predictors, the association between global cognition and the presence of a current psychiatric diagnosis became not significant.
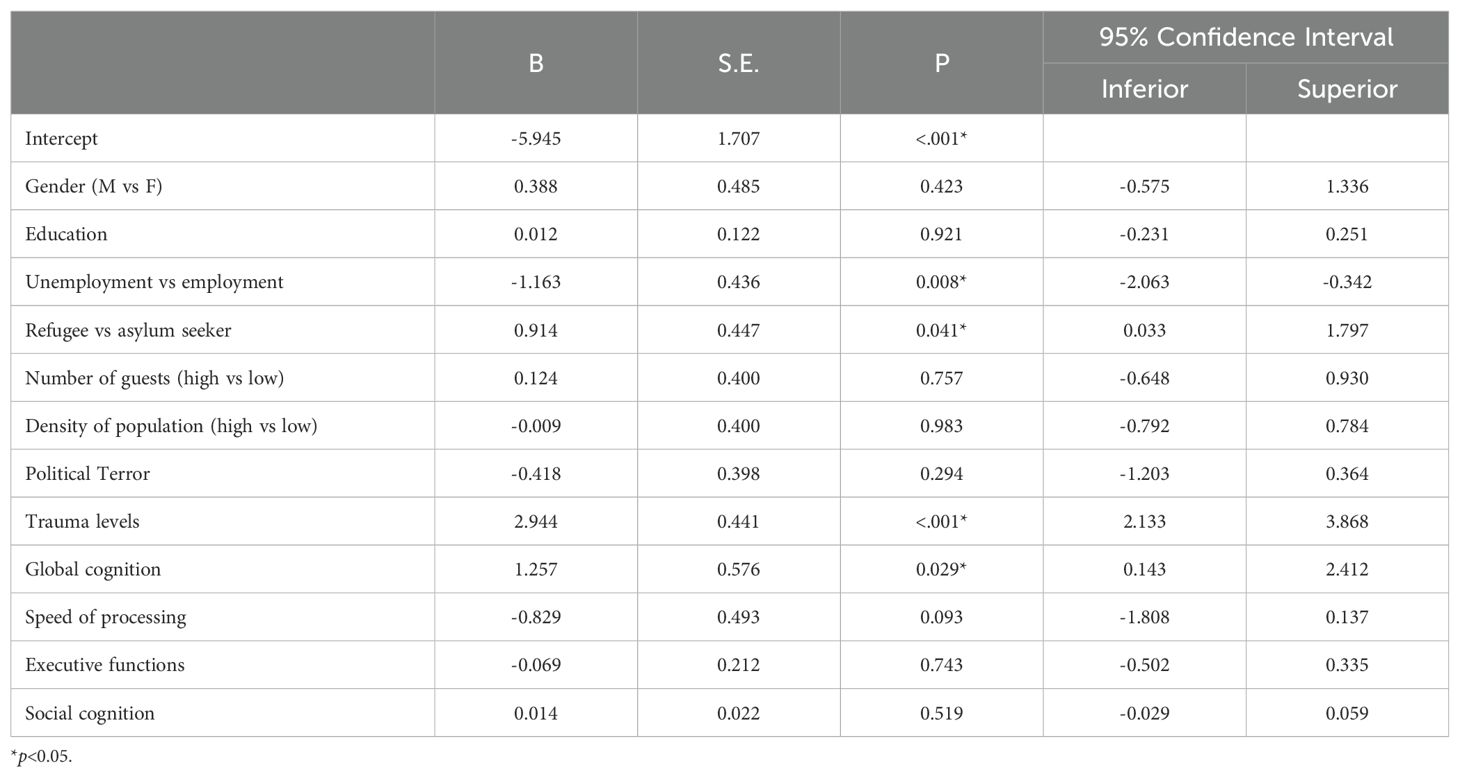
Table 4. Factors associated with the presence of a current psychiatric disorder (N=288).
Discussion
According to our findings, 29.7% of the people hosted in refugee centers in the Campania provinces of Avellino and Salerno suffered from at least one lifetime full-blown mental disorder and 25% of them had a current mental disorder. In line with other studies (5, 6, 19, 21, 52), we found that the most frequent psychiatric diagnoses were any depressive disorder, any anxiety disorder and PTSD. A higher prevalence with respect to the general population (53–58) was observed in our sample only for depressive disorders (16.5% vs. 12%) and PTSD (6% vs. 3.9%), while a prevalence comparable to that of the general population was observed for the other psychiatric disorders.
The prevalence of PTSD and depressive disorders observed in our sample, although higher with respect to that of the general population, was lower with respect to that reported in other studies (6, 12, 15, 21, 24). This is probably related to methodological factors. In fact, higher prevalence of PTSD and depressive disorders were reported in reviews and meta-analysis including data from studies conducted also in middle- and low-income countries, and/or with heterogeneous methodological quality (6, 21), as well as in studies with sample sizes < 200 (12) or in which diagnosis was not performed by means of diagnostic tools (15). As a matter of fact, prevalence rates similar to those found in our sample were reported in studies including only research conducted in high-income countries and of high methodological quality (i.e., sample size > 200 and assessment by means of diagnostic instruments) (5, 10, 59, 60).
We found a prevalence of psychotic disorders comparable to that of the general population. The literature in this regard is quite heterogeneous as some studies report a comparable or even reduced prevalence in refugees and asylum seekers vs. the general population (5) while others found an increased prevalence (16, 61–64). However, it must be noticed that studies reporting a greater prevalence of psychosis found that this was limited to some ethnic groups or to refugees and asylum seekers in some host countries, or to the migration status of refugees, thus suggesting that the development of a psychotic disorder is related to several factors, including the characteristics of the host countries, which may affect the quantity and quality of social interaction of refugees and asylum seekers. The low number of subjects with lifetime or current psychotic disorder in our sample (N=9) does not allow to further clarify this point.
Six individuals (2%) in our sample resulted at high risk for developing psychosis, a prevalence comparable to that reported in the general population (65–69). So far, this condition was explored in refugees and asylum seekers in a very few numbers of studies reporting no higher prevalence with respect to the general population (70).
In our sample, women showed more severe anxiety and depressive symptoms and a higher prevalence of anxiety disorders with respect to men, while the prevalence of depressive disorder, PTSD and any psychiatric disorder did not show any gender differences. Literature findings in this respect are very heterogeneous, as no gender differences in prevalence have been reported, as well as an increased prevalence in women of anxiety disorders, or depressive disorders, or PTSD (10, 24). These discrepancies may be related to the fact that female gender may not represent per se a risk factor to develop psychiatric disorders in refugees and asylum seekers but be a further element of vulnerability in people exposed to other risk factors, such as traumatic events. As a matter of fact, women in our sample were from more at-risk countries and had higher trauma levels. These factors, in addition to the finding of a better performance on social cognition, which may cause higher levels of frustration related to the difficulty of resettlement, could underlie the greater severity of anxiety and depressive symptoms and the higher frequency of anxiety disorders found in women.
Our findings highlighted the impact of traumatic events on mental health in refugees and asylum seekers. First, we found significantly higher trauma levels in subjects with at least one psychiatric disorder vs. those with no psychiatric disorder. Second, we observed a strong association between levels of trauma and severity of depressive and anxious symptoms as assessed by the HSCL-5. Third, trauma level was the most statistically significant independent variable, among those explored in the logistic regression, resulting associated with the presence of a current psychiatric disorder. These findings are widely supported by the literature, which has shown that trauma plays a central role in the development of psychological distress in the forced migrant populations (4, 12, 52). Refugees and asylum seekers may undergo traumatic experiences both in their country of origin, in the context of the migration process, and in the host country. The role of political terror level in the country of origin has been explored to understand the extent to which it affects the development of psychiatric disorders. Unlike Steel et al. (20), who found a strong association between high levels of PTS and PTSD diagnosis, and a weaker association with depressive disorders, in our sample there was no such positive correlation of PTS with anxiety and depressive symptomatology assessed by means of the HSCL-25 and no significant difference in the PTS scale between subjects with psychiatric disorder and those without. This finding supports the view that traumatic events experienced in the country of origin are not the only stressful factors related to the occurrence of psychiatric disorders, as many other stressful and traumatic events occurring during the migration journey, as well as after the arrival in the host country, can make refugees and asylum seekers vulnerable to psychological distress and to the occurrence of mental disorders. This finding highlights the importance to implement preventive strategies in host countries to manage potential risk factors.
To the best of our knowledge, no study explored so far, the impact of cognitive functioning in the occurrence of psychiatric disorders in a population of recently settled asylum seekers and refugees. Since cognitive functioning and psychopathology are independent but related dimensions, which interact in a transdiagnostic manner (71), we investigated the issue and found that the group of subjects with at least one psychiatric disorder had a better performance in global and social cognition with respect to subjects with no psychiatric disorders. In addition, a better performance on global cognition resulted associated in the linear regression analysis to the presence of a current psychiatric disorder. These findings may sound unexpected, given the well-known presence of cognitive deficit in some psychiatric disorders, mainly schizophrenia and bipolar disorders (72–75). However, it must be noticed that these disorders were poorly represented in our sample, while the most frequent psychiatric diagnoses were depressive disorders, anxiety disorders and PTSD. Additionally, studies exploring whether the association between cognitive ability and mental health (depression, anxiety, and psychological wellbeing) could be accounted for by different categories of risk factors such as socioeconomic status, coping/appraisal and social relationships demonstrated that such association can be partly explained by cognitive-behavioral mechanisms also highlighting the protective influence of socioeconomic status (76). The association of a better cognitive performance in subjects with these psychiatric diagnoses in our sample may be explained by the higher degree of frustration and disappointment of expectations experienced by subjects with better cognitive abilities. This would lead them to be more affected by the stressful events associated with the migratory journey and settlement, thus being more exposed to the development of anxiety and depressive syndromes. This hypothesis is in line with the finding reported in some studies of a higher risk to develop depressive and anxious symptoms in refugees with higher degrees of education, as they might suffer from the downgrading of social status in the host country compared to their qualifications (25, 77), however it may sound quite speculative. As a matter of fact, it must be noticed that the association between cognitive performance and the presence of current mental disorders seems to be influenced by multicollinearity among cognitive variables, in particular global cognition and speed of processing, and that the observed association between global cognition and the presence of a current psychiatric diagnosis became not statistically significant after removing the processing speed from the predictors. Further research exploring the impact of cognitive functioning on the occurrence of psychiatric disorders in these populations is needed to clarify this uncertain point.
In addition to trauma levels and cognitive abilities, the other variables resulting associated in the linear regression to the presence of a current psychiatric disorder, were unemployment and refugee status. Unemployment in itself has been identified as a risk factor for mental disorders and can be an obstacle to a full integration into the new social context (4, 52, 78). As to the refugee status, it may represent a further risk factor probably in relation to the higher risks present in their country of origin, as reported in other studies (6). On the other hand, in line with the findings of some reviews (21, 79) we found that asylum seekers with respect to refugees showed more severe anxiety and depressive symptomatology, which may be related to post-migration factors, such as the uncertainty of their condition, as by definition asylum seeker is a person who hasn’t yet been legally recognized as a refugee and is waiting to receive a decision on their asylum claim, and is not allowed to work in the country until is granted refugee status.
The main strengths of our study are: a) sample size > 200 subjects; b) the assessment of psychiatric diagnosis carried out by means of structured diagnostic interviews; c) the novelty of assessing the risk for developing psychosis and the impact of cognitive performance. The following study limitation have to be acknowledged: a) lack of information on specific traumatic events and displacement duration, which may represent a further risk factor to develop psychiatric disorders; b)lack of information about the length of stay in Italy of study participants; c) although in the study design the presence of cultural mediators was planned when needed, it was not possible to recruit them, especially due to the pandemic, therefore only Italian and English speaking subjects could be included in the study with a possible bias to a lower frequency of mental disorders. In addition, it cannot be excluded that the absence of cultural mediators have impacted the validity of collected data among subjects with limited linguistic skills in Italian or English, although it must be noticed that inclusion criteria required adequate language skills (Italian and/or English) for understanding informed consent and study interviews; d) the recruitment of participants only from specific reception centers in two provinces of the Campania region limits generalizability of our findings.
Overall, our findings suggest the identification of risk factors for the development of psychiatric disorders in a large ample of refugees and asylum seekers, namely higher levels of trauma – related not only to pre-migration stressful events, but also to stressful experiences lived in the host country – better global cognition and unemployment. The identification of such risk factors can be of help in the implementation of preventive strategies and early treatments in forced migrant populations. In particular, our findings suggest the following recommendations: for health policymakers, to invest in interventions targeting the increase of screening for psychiatric disorders during the asylum procedure and the reduction of barriers to mental health care in refugees and asylum seekers living in the community; for mental health professionals, recommendations include a careful assessment of stressful events to which each individual is exposed during all the phases of the migration process in order to work with the patient in focusing on the relationships between current problems and his/her traumatic events and vulnerabilities.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of University of Campania Luigi Vanvitelli. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LG: Data curation, Formal analysis, Methodology, Writing – original draft. PB: Supervision, Writing – original draft, Writing – review & editing. RB: Conceptualization, Funding acquisition, Resources, Writing – review & editing. GG: Writing – review & editing. MC: Writing – original draft. GC: Conceptualization, Funding acquisition, Resources, Writing – review & editing. DP: Conceptualization, Investigation, Methodology, Writing – original draft. AD: Data curation, Methodology, Writing – review & editing. FP: Investigation, Methodology, Writing – review & editing. GS: Methodology, Writing – review & editing. VA: Methodology, Writing – review & editing. RD: Methodology, Writing – review & editing. LS: Methodology, Writing – review & editing. CS: Data curation, Writing – review & editing. AlM: Methodology, Writing – review & editing. PD: Methodology, Writing – review & editing. ArM: Data curation, Resources, Supervision, Writing – review & editing. SG: Conceptualization, Funding acquisition, Investigation, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PENDING Project (Promotion of Well-being in Mental Health through a Cognitive Rehabilitation Model for the Early Treatment of Severe Mental Disorders) has been funded by the Asylum, Migration and Integration Fund 2014 – 2020 established by EU Regulation No. 516/2014. The funder had no role in the study design, data collection and analysis, interpretation of results, decision to publish, or preparation of the manuscript.
Conflict of interest
GG has been a consultant for Angelini. AM has been a consultant and/or advisor to or has received honoraria from Angelini, Gedeon. Richter Bulgaria, Janssen Pharmaceuticals, Lundbeck, Otsuka Pharmaceutical, Pfizer, Pierre Fabre, Rovi. Pharma and Boehringer Ingelheim. SG has been a consultant and/or advisor to or has received honoraria from Angelini, Boehringer Ingelheim, Gedeon Richter-Recordati, Janssen, Lundbeck, Otsuka, ROVI.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. United Nations, Department of Economic and Social Affairs, Population Division. International Migration Report 2017. Population Division (2017).
2. Centro Studi e Ricerche IDOS. Dossier statistico immigrazione 2023. Rome, Italy: Edizioni IDOS (2023).
4. Giacco D, Laxhman N, Priebe S. Prevalence of and risk factors for mental disorders in refugees. Semin Cell Dev Biol. (2018) 77:144–52. doi: 10.1016/j.semcdb.2017.11.030
5. Fazel M, Wheeler J, Danesh J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet. (2005) 365:1309–14. doi: 10.1016/S0140-6736(05)61027-6
6. Blackmore R, Boyle JA, Fazel M, Ranasinha S, Gray KM, Fitzgerald G, et al. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PloS Med. (2020) 17:e1003337. doi: 10.1371/journal.pmed.1003337
7. Turrini G, Purgato M, Ballette F, Nose M, Ostuzzi G, Barbui C. Common mental disorders in asylum seekers and refugees: umbrella review of prevalence and intervention studies. Int J Ment Health Syst. (2017) 11:51. doi: 10.1186/s13033-017-0156-0
8. Foo SQ, Tam WW, Ho CS, Tran BX, Nguyen LH, McIntyre RS, et al. Prevalence of depression among migrants: A systematic review and meta-analysis. Int J Environ Res Public Health. (2018) 15:1986. doi: 10.3390/ijerph15091986
9. Kirkbride JB, Anglin DM, Colman I, Dykxhoorn J, Jones PB, Patalay P, et al. The social determinants of mental health and disorder: evidence, prevention and recommendations. World Psychiatry. (2024) 23:58–90. doi: 10.1002/wps.21160
10. Bogic M, Njoku A, Priebe S. Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights. (2015) 15:29. doi: 10.1186/s12914-015-0064-9
11. Hoell A, Kourmpeli E, Salize HJ, Heinz A, Padberg F, Habel U, et al. Prevalence of depressive symptoms and symptoms of post-traumatic stress disorder among newly arrived refugees and asylum seekers in Germany: systematic review and meta-analysis. BJPsych Open. (2021) 7:e93. doi: 10.1192/bjo.2021.54
12. Nose M, Turrini G, Imoli M, Ballette F, Ostuzzi G, Cucchi F, et al. Prevalence and correlates of psychological distress and psychiatric disorders in asylum seekers and refugees resettled in an Italian catchment area. J Immigr Minor Health. (2018) 20:263–70. doi: 10.1007/s10903-017-0629-x
13. Voglino G, Gualano MR, Lo Moro G, Forghieri P, Caprioli M, Elhadidy H, et al. Mental health and discrimination among migrants from Africa: An Italian cross-sectional study. J Community Psychol. (2022) 50:601–19. doi: 10.1002/jcop.22685
14. Caroppo E, Calabrese C, Mazza M, Rinaldi A, Coluzzi D, Napoli P, et al. Migrants’ mental health recovery in Italian reception facilities. Commun Med (Lond). (2023) 3:162. doi: 10.1038/s43856-023-00385-8
15. Firenze A, Aleo N, Ferrara C, Maranto M, LAC C, Restivo V. The occurrence of diseases and related factors in a center for asylum seekers in Italy. Zdr Varst. (2016) 55:21–8. doi: 10.1515/sjph-2016-0003
16. Cristofalo D, Bonetto C, Ballarin M, Amaddeo F, Ruggeri M, Nose M, et al. Access to and use of psychiatric services by migrants resettled in northern Italy. J Immigr Minor Health. (2018) 20:1309–16. doi: 10.1007/s10903-018-0703-z
17. Olcese M, Madera F, Cardinali P, Serafini G, Migliorini L. The role of community resilience as a protective factor in coping with mental disorders in a sample of psychiatric migrants. Front Psychiatry. (2024) 15:1430688. doi: 10.3389/fpsyt.2024.1430688
18. Ventriglio A, Bellomo A, Petito A, Pascucci M, Cuozzo E, Vitrani G, et al. Factors associated to the onset of mental illness among hospitalized migrants to Italy: A chart review. J Immigr Minor Health. (2021) 23:425–33. doi: 10.1007/s10903-020-01105-3
19. Slewa-Younan S, Uribe Guajardo MG, Heriseanu A, Hasan T. A systematic review of post-traumatic stress disorder and depression amongst Iraqi refugees located in western countries. J Immigr Minor Health. (2015) 17:1231–9. doi: 10.1007/s10903-014-0046-3
20. Steel Z, Chey T, Silove D, Marnane C, Bryant RA, van Ommeren M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA. (2009) 302:537–49. doi: 10.1001/jama.2009.1132
21. James PB, Renzaho AMN, Mwanri L, Miller I, Wardle J, Gatwiri K, et al. The prevalence of anxiety, depression, and post-traumatic stress disorder among African migrants: A systematic review and meta-analysis. Psychiatry Res. (2022) 317:114899. doi: 10.1016/j.psychres.2022.114899
23. Tessitore F, Margherita G. Land of care seeking: Pre- and post-migratory experiences in asylum seekers’ narratives. Community Psychol Global Perspective. (2020) 6:74–91.
24. Peconga EK, Hogh Thogersen M. Post-traumatic stress disorder, depression, and anxiety in adult Syrian refugees: What do we know? Scand J Public Health. (2020) 48:677–87. doi: 10.1177/1403494819882137
25. Hermansson AC, Timpka T, Thyberg M. The mental health of war-wounded refugees: an 8-year follow-up. J Nerv Ment Dis. (2002) 190:374–80. doi: 10.1097/00005053-200206000-00005
26. Barbui C, Tedeschi F, Acarturk C, Anttila M, Au T, Baumgartner J, et al. Risk factors for mental disorder development in asylum seekers and refugees resettled in Western Europe and Turkey: Participant-level analysis of two large prevention studies. Int J Soc Psychiatry. (2023) 69:664–74. doi: 10.1177/00207640221132430
27. Silove D, Ventevogel P. Living through interminable adversity: the mental health of the Afghan people. World Psychiatry. (2022) 21:55–6. doi: 10.1002/wps.20955
28. Steel JL, Dunlavy AC, Harding CE, Theorell T. The psychological consequences of pre-emigration trauma and post-migration stress in refugees and immigrants from Africa. J Immigr Minor Health. (2017) 19:523–32. doi: 10.1007/s10903-016-0478-z
29. Tinghog P, Malm A, Arwidson C, Sigvardsdotter E, Lundin A, Saboonchi F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: a population-based survey. BMJ Open. (2017) 7:e018899. doi: 10.1136/bmjopen-2017-018899
30. Lecerof SS, Stafstrom M, Westerling R, Ostergren PO. Does social capital protect mental health among migrants in Sweden? Health Promot Int. (2016) 31:644–52. doi: 10.1093/heapro/dav048
31. Teodorescu DS, Heir T, Hauff E, Wentzel-Larsen T, Lien L. Mental health problems and post-migration stress among multi-traumatized refugees attending outpatient clinics upon resettlement to Norway. Scand J Psychol. (2012) 53:316–32. doi: 10.1111/j.1467-9450.2012.00954.x
32. FitzGerald DS, Arar R. The sociology of refugee migration. Annu Rev Sociol. (2018) 44:387–406. doi: 10.1146/annurev-soc-073117-041204
33. Williams DR, Etkins OS. Racism and mental health. World Psychiatry. (2021) 20:194–5. doi: 10.1002/wps.20845
34. Verkuyten M. Public attitudes towards migrants: understanding cross-national and individual differences. World Psychiatry. (2021) 20:132–3. doi: 10.1002/wps.20819
35. Acarturk C, Uygun E, Ilkkursun Z, Carswell K, Tedeschi F, Batu M, et al. Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: a randomized controlled trial. World Psychiatry. (2022) 21:88–95. doi: 10.1002/wps.20939
36. Atwoli L, Muhia J, Wanja Gitau C. From diversity to individualized care: Africa’s contribution to psychiatry. World Psychiatry. (2022) 21:424–6. doi: 10.1002/wps.21007
37. Colizzi M, Cullen AE, Martland N, Di Forti M, Murray R, Schoeler T, et al. Association between stressful life events and psychosis relapse: a 2-year prospective study in first-episode psychosis. World Psychiatry. (2023) 22:159–60. doi: 10.1002/wps.21046
38. Killaspy H, Harvey C, Brasier C, Brophy L, Ennals P, Fletcher J, et al. Community-based social interventions for people with severe mental illness: a systematic review and narrative synthesis of recent evidence. World Psychiatry. (2022) 21:96–123. doi: 10.1002/wps.20940
39. Malla A, Boksa P, Joober R. Meeting the challenges of the new frontier of youth mental health care. World Psychiatry. (2022) 21:78–9. doi: 10.1002/wps.20927
40. Schafer SK, Thomas LM, Lindner S, Lieb K. World Health Organization’s low-intensity psychosocial interventions: a systematic review and meta-analysis of the effects of Problem Management Plus and Step-by-Step. World Psychiatry. (2023) 22:449–62. doi: 10.1002/wps.21129
41. Sharan P. Implementation strategies for the new World Mental Health Report in low-resource settings. World Psychiatry. (2022) 21:466–7. doi: 10.1002/wps.21032
42. Harvey PD, Strassnig M. Predicting the severity of everyday functional disability in people with schizophrenia: cognitive deficits, functional capacity, symptoms, and health status. World Psychiatry. (2012) 11:73–9. doi: 10.1016/j.wpsyc.2012.05.004
43. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry. (2014) 13:275–87. doi: 10.1002/wps.20167
44. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59 Suppl 20:22–33;quiz 4-57.
45. Yung AR, Yuen HP, McGorry PD, Phillips LJ, Kelly D, Dell’Olio M, et al. Mapping the onset of psychosis: the Comprehensive Assessment of At-Risk Mental States. Aust N Z J Psychiatry. (2005) 39:964–71. doi: 10.1080/j.1440-1614.2005.01714.x
46. Ventevogel P, De Vries G, Scholte WF, Shinwari NR, Faiz H, Nassery R, et al. Properties of the Hopkins Symptom Checklist-25 (HSCL-25) and the Self-Reporting Questionnaire (SRQ-20) as screening instruments used in primary care in Afghanistan. Soc Psychiatry Psychiatr Epidemiol. (2007) 42:328–35. doi: 10.1007/s00127-007-0161-8
47. Wind TR, van der Aa N, Knipscheer J, de la Rie S. The assessment of psychopathology among traumatized refugees: measurement invariance of the Harvard Trauma Questionnaire and the Hopkins Symptom Checklist-25 across five linguistic groups. Eur J Psychotraumatol. (2017) 8:1321357. doi: 10.1080/20008198.2017.1321357
49. Weiss LG, Saklofske DH, Coalson DL, Engi Raiford S. WAIS-IV Clinical Use and Interpretation - A volume in Practical Resources for the Mental Health Professional: Elsevier Inc. (2010).
50. Nuechterlein KH, Green MF, Kern RS, Baade LE, Barch DM, Cohen JD, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry. (2008) 165:203–13. doi: 10.1176/appi.ajp.2007.07010042
51. Kerr SL, Neale JM. Emotion perception in schizophrenia: specific deficit or further evidence of generalized poor performance? J Abnorm Psychol. (1993) 102:312–8. doi: 10.1037/0021-843X.102.2.312
52. Priebe S, Giacco D, El-Nagib R. Public health aspects of mental health among migrants and refugees: A review of the evidence on mental health care for refugees, asylum seekers and irregular migrants in the WHO european region. In: WHO Health Evidence Network Synthesis Reports. Copenhagen: WHO Regional Office for Europe (2016).
53. Dragioti E, Radua J, Solmi M, Gosling CJ, Oliver D, Lascialfari F, et al. Impact of mental disorders on clinical outcomes of physical diseases: an umbrella review assessing population attributable fraction and generalized impact fraction. World Psychiatry. (2023) 22:86–104. doi: 10.1002/wps.21068
54. Kessler RC, Aguilar-Gaxiola S, Alonso J, Chatterji S, Lee S, Ormel J, et al. The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiol Psichiatr Soc. (2009) 18:23–33. doi: 10.1017/S1121189X00001421
55. Koenen KC, Ratanatharathorn A, Ng L, McLaughlin KA, Bromet EJ, Stein DJ, et al. Posttraumatic stress disorder in the World Mental Health Surveys. Psychol Med. (2017) 47:2260–74. doi: 10.1017/S0033291717000708
56. Leichsenring F, Steinert C, Rabung S, Ioannidis JPA. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry. (2022) 21:133–45. doi: 10.1002/wps.20941
57. McIntyre RS, Alsuwaidan M, Baune BT, Berk M, Demyttenaere K, Goldberg JF, et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. (2023) 22:394–412. doi: 10.1002/wps.21120
58. Stein DJ, Shoptaw SJ, Vigo DV, Lund C, Cuijpers P, Bantjes J, et al. Psychiatric diagnosis and treatment in the 21st century: paradigm shifts versus incremental integration. World Psychiatry. (2022) 21:393–414. doi: 10.1002/wps.20998
59. Richter K, Peter L, Lehfeld H, Zaske H, Brar-Reissinger S, Niklewski G. Prevalence of psychiatric diagnoses in asylum seekers with follow-up. BMC Psychiatry. (2018) 18:206. doi: 10.1186/s12888-018-1783-y
60. Tekin A, Karadag H, Suleymanoglu M, Tekin M, Kayran Y, Alpak G, et al. Prevalence and gender differences in symptomatology of posttraumatic stress disorder and depression among Iraqi Yazidis displaced into Turkey. Eur J Psychotraumatol. (2016) 7:28556. doi: 10.3402/ejpt.v7.28556
61. Brandt L, Henssler J, Muller M, Wall S, Gabel D, Heinz A. Risk of psychosis among refugees: A systematic review and meta-analysis. JAMA Psychiatry. (2019) 76:1133–40. doi: 10.1001/jamapsychiatry.2019.1937
62. Dapunt J, Kluge U, Heinz A. Risk of psychosis in refugees: a literature review. Transl Psychiatry. (2017) 7:e1149. doi: 10.1038/tp.2017.119
63. Halvorsrud K, Nazroo J, Otis M, Brown Hajdukova E, Bhui K. Ethnic inequalities in the incidence of diagnosis of severe mental illness in England: a systematic review and new meta-analyses for non-affective and affective psychoses. Soc Psychiatry Psychiatr Epidemiol. (2019) 54:1311–23. doi: 10.1007/s00127-019-01758-y
64. Selten JP, van der Ven E, Termorshuizen F. Migration and psychosis: a meta-analysis of incidence studies. Psychol Med. (2020) 50:303–13. doi: 10.1017/S0033291719000035
65. Brady LS, Larrauri CA, Committee ASS. Accelerating Medicines Partnership((R)) Schizophrenia (AMP((R)) SCZ): developing tools to enable early intervention in the psychosis high risk state. World Psychiatry. (2023) 22:42–3. doi: 10.1002/wps.21038
66. Danese A. Bridging between youth psychiatry and child and adolescent psychiatry. World Psychiatry. (2022) 21:83–5. doi: 10.1002/wps.20931
67. Lang U, Ramsay H, Yates K, Veijola J, Gyllenberg D, Clarke MC, et al. Potential for prediction of psychosis and bipolar disorder in Child and Adolescent Mental Health Services: a longitudinal register study of all people born in Finland in 1987. World Psychiatry. (2022) 21:436–43. doi: 10.1002/wps.21009
68. Salazar de Pablo G, Radua J, Pereira J, Bonoldi I, Arienti V, Besana F, et al. Probability of transition to psychosis in individuals at clinical high risk: an updated meta-analysis. JAMA Psychiatry. (2021) 78:970–8. doi: 10.1001/jamapsychiatry.2021.0830
69. Uher R, Pavlova B, Radua J, Provenzani U, Najafi S, Fortea L, et al. Transdiagnostic risk of mental disorders in offspring of affected parents: a meta-analysis of family high-risk and registry studies. World Psychiatry. (2023) 22:433–48. doi: 10.1002/wps.21147
70. Moore D, Castagnini E, Mifsud N, Geros H, Sizer H, Addington J, et al. The associations between migrant status and ethnicity and the identification of individuals at ultra-high risk for psychosis and transition to psychosis: a systematic review. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:1923–41. doi: 10.1007/s00127-021-02047-3
71. Chavez-Baldini U, Nieman DH, Keestra A, Lok A, Mocking RJT, de Koning P, et al. The relationship between cognitive functioning and psychopathology in patients with psychiatric disorders: a transdiagnostic network analysis. Psychol Med. (2023) 53:476–85. doi: 10.1017/S0033291721001781
72. Keshavan MS, Eack SM. Cognitive enhancement interventions are effective for schizophrenia: why not provide them early? World Psychiatry. (2023) 22:326–7. doi: 10.1002/wps.21091
73. McIntyre RS, Alda M, Baldessarini RJ, Bauer M, Berk M, Correll CU, et al. The clinical characterization of the adult patient with bipolar disorder aimed at personalization of management. World Psychiatry. (2022) 21:364–87. doi: 10.1002/wps.20997
74. Watson D, Levin-Aspenson HF, Waszczuk MA, Conway CC, Dalgleish T, Dretsch MN, et al. Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry. (2022) 21:26–54. doi: 10.1002/wps.20943
75. Giordano GM, Pezzella P, Quarantelli M, Bucci P, Prinster A, Soricelli A, et al. Investigating the Relationship between White Matter Connectivity and Motivational Circuits in Subjects with Deficit Schizophrenia: A Diffusion Tensor Imaging (DTI) Study. Journal of clinical medicine (2021) 11(1):61. doi: 10.3390/jcm11010061
76. Jokela M. Why is cognitive ability associated with psychological distress and wellbeing? Exploring psychological, biological, and social mechanisms. Pers Individ Differ. (2022) 192:111592. doi: 10.1016/j.paid.2022.111592
77. Sonne C, Carlsson J, Bech P, Vindbjerg E, Mortensen EL, Elklit A. Psychosocial predictors of treatment outcome for trauma-affected refugees. Eur J Psychotraumatol. (2016) 7:30907. doi: 10.3402/ejpt.v7.30907
78. Montgomery E, Foldspang A. Discrimination, mental problems and social adaptation in young refugees. Eur J Public Health. (2008) 18:156–61. doi: 10.1093/eurpub/ckm073
Keywords: refugees, asylum seekers, mental health, health policy, prevention, early intervention
Citation: Giuliani L, Bucci P, Bracalenti R, Giordano GM, Conenna M, Corrivetti G, Palumbo D, Dell’Acqua A, Piras F, Storti G, Abitudine V, Di Lieto R, Sandolo L, Schiavitelli C, Mulè A, D’Arista P, Mucci A and Galderisi S (2024) Prevalence of mental disorders and related risk factors in refugees and asylum seekers in Campania. Front. Psychiatry 15:1478383. doi: 10.3389/fpsyt.2024.1478383
Received: 09 August 2024; Accepted: 15 October 2024;
Published: 12 November 2024.
Edited by:
Antonio Vita, University of Brescia, ItalyCopyright © 2024 Giuliani, Bucci, Bracalenti, Giordano, Conenna, Corrivetti, Palumbo, Dell’Acqua, Piras, Storti, Abitudine, Di Lieto, Sandolo, Schiavitelli, Mulè, D’Arista, Mucci and Galderisi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luigi Giuliani, bHVpZ2kuZ2l1bGlhbmlAdW5pY2FtcGFuaWEuaXQ=; Raffaele Bracalenti, ci5icmFjYWxlbnRpQGlwcnMuaXQ=; Giulio Corrivetti, Zy5jb3JyaXZldHRpQGFzbHNhbGVybm8uaXQ=
†These authors have contributed equally to this work