 Wenrong Ge
Wenrong Ge Cancan Zhang2
Cancan Zhang2 Guang Yang
Guang Yang Bo Zhang
Bo Zhang- 1Department of Pediatrics, Beijing Friendship Hospital, Capital Medical University, Beijing, China
- 2Division of General Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States
- 3Department of Pediatrics, the First Medical Center of Chinese PLA General Hospital, Beijing, China
- 4Senior Department of Pediatrics, the Seventh Medical Center of Chinese PLA General Hospital, Beijing, China
- 5Medical School of Chinese PLA, Beijing, China
- 6Department of Neurology, Boston Children’s Hospital, Harvard Medical School, Boston, MA, United States
- 7Biostatistics and Research Design Center, Institutional Centers for Clinical and Translational Research, Boston Children’s Hospital, Harvard Medical School, Boston, MA, United States
Background: The National Health Interview Survey (NHIS) is a comprehensive health survey conducted by the National Center for Health Statistics (NCHS) in the U.S., providing valuable insights into the health status of the population. This study focuses on the NHIS child survey between 2019 and 2021, exploring developmental disabilities in U.S. children, including autism spectrum disorder (ASD), attention deficit/hyperactivity disorder or attention-deficit disorder (ADHD/ADD), intellectual disability (ID), other developmental delay (other DD), and learning disability (LD).
Objective: Leveraging NHIS data, our primary objective is to investigate the latest trends and disparities in the prevalence of developmental disabilities among various racial-ethnic groups.
Methods: Employing a repeated cross-sectional design, we analyzed NHIS data from 2019 to 2021, focusing on children aged 3-17. The survey employed a meticulous stratified multi-stage sampling design. We utilized SAS version 9.4 for data analysis, calculating race-ethnicity-specific prevalence rates and employing weighted linear regression and the Rao-Scott chi-square test for trend analysis.
Results: Among 19,490 children, prevalence rates varied: ASD (3.11%), ADHD/ADD (9.50%), ID (1.85%), other DD (5.66%), and LD (7.49%). Non-Hispanic black children exhibited higher rates of ID and LD, while non-Hispanic white children had the highest ADHD/ADD prevalence. Disparities persisted across sociodemographic subgroups, with variations in prevalence rates.
Conclusion: Our study reveals an increase in ASD prevalence and persistent disparities among racial-ethnic groups. Non-Hispanic black children face elevated risks of ID and LD, while non-Hispanic white children exhibit higher rates of ADHD/ADD.
1 Introduction
The National Health Interview Survey (NHIS) is an extensive and ongoing survey conducted by the National Center for Health Statistics (NCHS), a part of the Centers for Disease Control and Prevention (CDC) in the United States (U.S.) (1, 2). The primary objective of the NHIS is to gather data on a broad spectrum of health-related topics, encompassing health status, healthcare access, health behaviors, and healthcare usage. It yields valuable insights into health trends and the challenges faced by the American population. The NHIS comprises both adult and child surveys and stands as one of the most vital sources of information regarding the health and well-being of the U.S. populace (2). The child survey within the NHIS between 2019 and 2021 encompassed various sections dedicated to developmental disabilities in U.S. children and adolescents. It addressed conditions including autism spectrum disorder (ASD), attention deficit/hyperactivity disorder or attention-deficit disorder (ADHD/ADD), intellectual disability (ID), any other developmental delay (other DD), and learning disability (LD) (3). These conditions typically manifest early in the developmental stages and can lead to personal, social, learning, language, and behavioral challenges.
Previous studies by Boyles et al. (4) and Zaboltsky et al. (5) investigated the prevalence and trends of these developmental disabilities among U.S. children and adolescents, spanning from 1997 to 2008 and from 2009 to 2017, respectively. Both studies reported an increase in prevalence during their respective periods. Additionally, Kogan et al. (6) and Xu et al. (7) conducted an analysis of the 2016 National Survey of Children’s Health (NSCH), concluding that the prevalence of ASD in the U.S. in 2016 was 2.50%, indicating 1 in 40 U.S. children was autistic in 2016. Magaña et al. (8) utilized data from the 2005-2006 wave of the National Survey of Children with Special Health Care Needs to investigate racial-ethnic disparities in the quality of healthcare among children with ASD, Down syndrome, cerebral palsy, and Intellectual Disability. They compared black and Latino children with white children and identified racial-ethnic disparities in five out of six healthcare quality outcomes (8). Magaña et al. repeated this investigation for the 2009-2010 wave of the survey and found that these disparities remained unchanged (9).
This study leveraged data released by the NHIS from 2019 to 2021. Our primary objective was to investigate the latest trends and disparities in the prevalence of developmental disabilities among various racial-ethnic groups.
2 Methods
This study adopted a repeated cross-sectional design by consolidating data gathered through the NHIS surveys conducted between 2019 and 2021. The NHIS employed a meticulously structured stratified multi-stage sampling design and conducted interviews with either adults or parents and guardians of children, with the aim of collecting comprehensive information regarding the health conditions of U.S. residents (10, 11). The NHIS’s sampling plan was thoughtfully crafted by the Division of Health Interview Statistics within the National Center for Health Statistics at the Centers for Disease Control and Prevention. The NHIS waves from 2019 to 2021 and from previous years were conducted independently from one another, following the stratified multi-stage sampling design each year. As a result, the data collected from these individual years can be combined for analysis while maintaining the independence of each wave. For a more in-depth understanding of the sampling design and its implementation, the Survey Design document of the NHIS provides detailed information (10).
In our study, we focused on children and adolescents between the ages of 3 and 17, drawing data from the 2019, 2020, and 2021 waves of the NHIS. Our analysis revolved around the responses to the NHIS survey questions related to developmental disabilities. These questions are as follows. Parents or guardians were asked, “Does [sample child’s name] currently have Autism, Asperger’s disorder, pervasive developmental disorder, or autism spectrum disorder?” for ASD. They were also asked, “Does [sample child’s name] currently have Attention-Deficit/Hyperactivity Disorder or ADHD, or Attention-Deficit Disorder or ADD?” for ADHD/ADD. For ID, the question was, “Does [sample child’s name] currently have an intellectual disability, also known as Intellectual Disability?” Additionally, there was a subsequent question, “Does [sample child’s name] still have any other developmental delay?” for other DD. Lastly, the survey included a question, “Does [sample child’s name] currently have a learning disability?” to assess LD. Our analysis sought to examine the outcomes of these survey questions in conjunction with sociodemographic characteristics. Furthermore, our objective was to investigate the most recent trends and disparities in the prevalence of these developmental disabilities among various racial-ethnic groups. The dataset for our study also encompassed sociodemographic characteristics of the sample children, including age, sex, racial-ethnic groups (non-Hispanic white, non-Hispanic black, Hispanic, non-Hispanic others; these categories were designed by the NHIS survey and adopted here), the highest level of education attained by all adults in the sample children’s family, and the income-to-poverty ratio of the sample children’s family.
Following NHIS guidelines (10, 11), we executed the survey procedure using SAS version 9.4 (SAS Institute Inc.) to calculate race-ethnicity-specific prevalence rates of developmental disabilities, along with 95% confidence intervals (CIs). We provided stratified estimates considering age, gender, highest family education level, and family income-to-poverty ratio. To assess the association between race/ethnicity and prevalence, we conducted the Rao-Scott chi-square test to examine independence. Additionally, we employed weighted linear regression analysis to identify trends, with statistical significance defined as a p-value less than 0.05. Our study did not involve research on human subjects and animals, and thus, it was exempt from the requirement for ethical approval.
3 Results
A total of 19,490 children and adolescents, aged 3 to 17 years, participated in the NHIS survey conducted between 2019 and 2021. Among the participants across the three years, the results indicated the following prevalence rates: 3.11% (CI: [2.80%, 3.41%]) reported being diagnosed with ASD; 9.50% (8.95%, 10.04%) had ADHD/ADD; 1.85% (1.61%, 2.09%) had ID; 5.66% (5.23%, 6.08%) had other DD; 7.49% (6.99%, 7.99%) had LD (Table 1, top section). Non-Hispanic black children exhibited the highest prevalence rates of ID (2.82%, CI: [1.84%, 3.80%]) and LD (9.40%, CI: [7.67%, 11.13%]) in comparison to other racial/ethnic groups (p=0.0117 and 0.0006, respectively). Non-Hispanic white children had the highest prevalence of ADHD/ADD (11.18%, CI: [10.41%, 11.95%], p<0.0001). No significant differences were observed in the prevalence of ASD and other DD among various racial-ethnic groups (Table 1, top section).
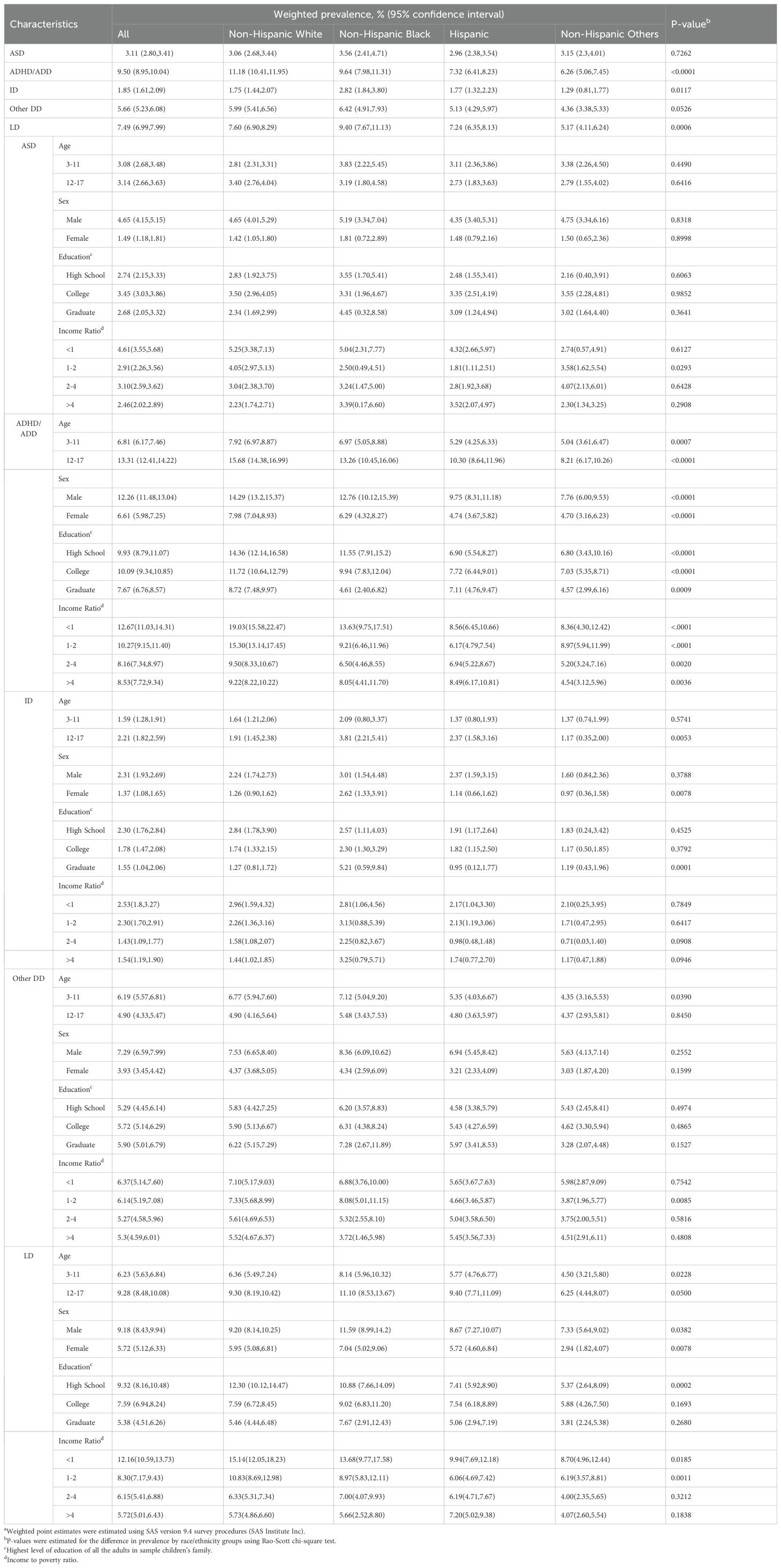
Table 1. Weighted prevalence of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder or attention deficit disorder (ADHD/ADD), intellectual disability (ID), any other developmental disabilities (Other DD), and learning disabilities (LD) in the US children and adolescents aged 3 to 17 by race/ethnicity in the National Health Interview Survey, 2019-2021.
When we examined the prevalence of ASD among various sociodemographic subgroups, we observed that, for these subgroups, there was generally no significant association between ASD and race/ethnicity (Table 1, ASD section). However, a further analysis of our data revealed noteworthy disparities in the prevalence of ADHD/ADD across different racial-ethnic groups within all sociodemographic subgroups. Specifically, among children who were non-Hispanic white and black, we found significantly higher prevalence rates compared to Hispanic children and non-Hispanic others. These differences were consistent across all four sociodemographic factors, with a p-value ranged from less than 0.0001 to 0.0036 (Table 1, ADHD/ADD section). These disparities remained in prevalence of LD across different racial-ethnic groups within most sociodemographic subgroups, except four subgroups in highest family education level and income-to-poverty ratio (Table 1, LD section). Furthermore, we discovered that non-Hispanic black children aged 12-17 had a significantly higher prevalence rate (p=0.0053) of ID compared to other racial-ethnic groups. Among female children (p=0.0078) and among those whose highest family education level was graduate school (p=0.0001), the non-Hispanic black subgroup exhibited significantly higher prevalence rates of ID (Table 1, ID section). Non-Hispanic black children aged 3-11 and whose highest family education level was graduate school (p=0.0001) had a significantly higher prevalence rate (p=0.0390) of other DD compared to other racial-ethnic groups (Table 1, other DD section).
4 Discussion
Our study provides the latest update on prevalence rates and racial-ethnic disparities for various developmental disabilities, offering a valuable comparison to earlier findings. Yuan, Li, and Lu (12) conducted an analysis of the 2014-2018 waves of the NHIS, reporting an overall ASD prevalence of 2.49%. In a similar vein, Xu et al. (7) examined the prevalence of ASD in the U.S. in 2016, reporting a rate of 2.50% based on their analysis of the NSCH data. However, our analysis revealed a noteworthy change in the prevalence rate of ASD from 2019 to 2021. During this period, the prevalence of ASD in the U.S. increased to 3.11%, signifying a notable rise in ASD prevalence within the country.
Our study also revealed variations in the prevalence of ADHD/ADD, ID, other DD, and LD among different racial-ethnic groups. Notably, non-Hispanic black children exhibited the highest prevalence of ID and LD, while non-Hispanic white children had the highest prevalence of ADHD/ADD. While we observed significant disparities in the prevalence of ADHD/ADD and LD among different racial-ethnic groups, such disparities were not evident in the case of ASD. This suggested a more consistent prevalence of ASD across diverse racial-ethnic backgrounds as reported by Yuan, Li, and Lu (12). Past research has indicated that learning difficulties can be linked to parental involvement in children’s education (13). When parents have lower levels of education or income, their involvement in their children’s education may be reduced, potentially exacerbating disparities in LD (14).
The increase in the prevalence of autism in this study may be due to a variety of factors. One key factor is the improvement in diagnostic criteria and greater awareness among healthcare providers and the public. The definitions of ASD have broadened over time, encompassing a wider range of behaviors and developmental issues, leading to more children being diagnosed (15). Additionally, healthcare access has improved, allowing more families to seek and obtain diagnoses for developmental conditions (16). Another contributing factor could be an increase in early screening initiatives and better access to educational resources, which have improved early identification of children with ASD (17). Changes in parental reporting, as well as sociocultural factors such as the reduced stigma surrounding autism, may also play a role in the upward trend in prevalence rates. The difference in autism prevalence between males and females, with boys being diagnosed more frequently than girls, is a well-documented phenomenon in the previous studies (12–14). One reason for this discrepancy may be that autism presents differently in girls, often with less overt or stereotypical behaviors, which can lead to underdiagnosis or misdiagnosis. Girls with autism may also be better at masking or compensating for their symptoms, making it harder for parents and clinicians to recognize their challenges early on.
Differences in the prevalence of developmental disabilities by race, as reported in this study, can be attributed to several factors. Socioeconomic disparities, healthcare access, and cultural attitudes toward disabilities may all contribute to these differences. For instance, non-Hispanic black children exhibited higher prevalence rates for certain developmental disabilities such as ID and LD. This could be due to differences in access to diagnostic and support services (18), particularly in lower-income communities (19), which tend to have a higher proportion of minority populations. Additionally, racial-ethnic minorities often experience systemic barriers in healthcare, such as implicit bias in diagnosis and treatment, which could result in under- or over-diagnosis of certain conditions in different racial groups.
The primary limitation of this study pertains to the assessment of these developmental disabilities including ASD. The data in the NHIS were reported by parents or guardians, and as such, the prevalences were reliant on their reports.
5 Conclusions
Our study reveals an increase in ASD prevalence and persistent disparities among racial-ethnic groups. Non-Hispanic black children face elevated risks of ID and LD, while non-Hispanic white children exhibit higher rates of ADHD/ADD. Targeted interventions are essential to address these disparities, emphasizing the importance of inclusive strategies to mitigate the impact of developmental disabilities.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
This is a reanalysis of the publicly available data set, so no ethical approval is required. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because this is a reanalysis of the publicly available data set.
Author contributions
WG: Formal analysis, Software, Writing – original draft, Writing – review & editing. CZ: Formal analysis, Software, Writing – review & editing. GY: Conceptualization, Supervision, Validation, Writing – review & editing. BZ: Conceptualization, Formal analysis, Software, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
NHIS, National Health Interview Survey; ASD, autism spectrum disorder; ADHD/ADD, attention deficit/hyperactivity disorder or attention-deficit disorder; ID, intellectual disability; DD, developmental delay; LD, learning disability.
References
1. The Centers for Disease Control and Prevention. National health interview survey . Available online at: https://www.cdc.gov/nchs/nhis/index.htm (Accessed January 2023).
2. National Centers for Health Statistics, the Centers for Disease Control and Prevention. National Health Interview Survey (NHIS) sample questionnaire brochure . Available online at: https://www.cdc.gov/nchs/data/nhis/Sample-Questionnaire-Brochure.pdf (Accessed January 2023).
3. The Centers for Disease Control and Prevention. 2019-2021 National Health Interview Survey (NHIS) codebook for sample child file . Available online at: https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm (Accessed January 2023).
4. Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, et al. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics. (2011) 127:1034–42. doi: 10.1542/peds.2010-2989
5. Zablotsky B, Black LI, Maenner MJ, Schieve LA, Danielson ML, Bitsko RH, et al. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics. (2019) 144:e20190811. doi: 10.1542/peds.2019-0811
6. Kogan MD, Vladutiu CJ, Schieve LA, Ghandour RM, Blumberg SJ, Zablotsky B, et al. The prevalence of parent-reported autism spectrum disorder among US children. Pediatrics. (2018) 142:e20174161. doi: 10.1542/peds.2017-4161
7. Xu G, Strathearn L, Liu B, O’Brien M, Kopelman TG, Zhu J, et al. Prevalence and treatment patterns of autism spectrum disorder in the United States, 2016. JAMA pediatrics. (2019) 173:153–9. doi: 10.1001/jamapediatrics.2018.4208
8. Magaña S, Parish SL, Rose RA, Timberlake M, Swaine JG. Racial and ethnic disparities in quality of health care among children with autism and other developmental disabilities. Intellectual Dev disabilities. (2012) 50:287–99. doi: 10.1352/1934-9556-50.4.287
9. Magaña S, Parish S, Morales MA, Li H, Fujiura G. Racial and ethnic health disparities among people with intellectual and developmental disabilities. Intellectual Dev disabilities. (2016) 54:161–72. doi: 10.1352/1934-9556-54.3.161
10. Division of Health Interview Statistics, National Centers for Health Statistics, the Centers for Disease Control and Prevention. 2019 National Health Interview Survey (NHIS) survey description . Available online at: https://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2019/srvydesc-508.pdf (Accessed January 2023).
11. Moriarity C, Parsons VL, Jonas K, Schar BG, Bose J, Bramlett MD. Sample design and estimation structures for the National Health interview survey, 2016-2025. Vital Health Stat 1. (2022) 191:1–30. doi: 10.15620/cdc:115394
12. Yuan J, Li M, Lu ZK. Racial/ethnic disparities in the prevalence and trends of autism spectrum disorder in US children and adolescents. JAMA Network Open. (2021) 4:e210771. doi: 10.1001/jamanetworkopen.2021.0771
13. Yotyodying S, Wild E. Predictors of the quantity and different qualities of home-based parental involvement: Evidence from parents of children with learning disabilities. Learn Individ Differences. (2016) 49:74–84. doi: 10.1016/j.lindif.2016.05.003
14. O’Connor SC, Spreen O. The relationship between parents’ socioeconomic status and education level, and adult occupational and educational achievement of children with learning disabilities. J Learn disabilities. (1988) 21:148–53. doi: 10.1177/00222194880210030
15. Maye MP, Kiss IG, Carter AS. Definitions and classification of autism spectrum disorders. In: Autism Spectrum Disorders. New York: Routledge (2022). p. 3–26.
16. Andersen RM, Davidson PL, Baumeister SE. Improving access to care in America. Changing the US health care system: key issues in health services policy and management. 3a. edición. San Francisco: Jossey-Bass (2007) p. 3–1.
17. Choueiri R, Garrison WT, Tokatli V, Daneshvar N, Belgrad J, Zhu G, et al. The RITA-T (Rapid interactive screening test for autism in toddlers) community model to improve access and early identification of autism in young children. Child Neurol Open. (2023) 10:2329048X231203817. doi: 10.1177/2329048X231203817
18. Zeleke WA, Hughes TL, Drozda N. Disparities in diagnosis and service access for minority children with ASD in the United States. J Autism Dev Disord. (2019) 49:4320–31. doi: 10.1007/s10803-019-04131-9
Keywords: neurodevelopmental disorders, learning disability, National Health Interview Survey (NHIS) data, racial disparities, prevalence of autism spectrum disorder
Citation: Ge W, Zhang C, Yang G and Zhang B (2024) Prevalence and trends of autism spectrum disorder and other developmental disabilities among children and adolescents in the United States from 2019 to 2021. Front. Psychiatry 15:1471969. doi: 10.3389/fpsyt.2024.1471969
Received: 28 July 2024; Accepted: 09 September 2024;
Published: 26 September 2024.
Edited by:
Antonio Narzisi, Stella Maris Foundation (IRCCS), ItalyReviewed by:
Paulina Sofia Arango, University of the Andes, ChileRenata Rizzo, University of Catania, Italy
Copyright © 2024 Ge, Zhang, Yang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guang Yang, eWFuZ2czMDFAMTI2LmNvbQ==