 Mingyuan Jia
Mingyuan Jia Jia Zhang
Jia Zhang Jianhua Pan2
Jianhua Pan2 Zhipeng Zhu
Zhipeng Zhu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 07 October 2024
Sec. Autism
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1462601
Background: Numerous experimental studies have shown that exercise can serve as an intervention with beneficial effects on children and adolescents with autism. However, a systematic review on the specific areas affected has not been conducted.
Methods: Preliminary research sources were obtained by searching four databases, and two researchers independently screened the literature that met the study criteria. The study was conducted under the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions.
Results: 37 studies were included in the final analysis, of which 9 studies were quantitatively synthesized and 28 studies were qualitatively analyzed. Exercise interventions have positive effects on motor performance, cognitive function, individual and social relationships, behavioral problems, physical health, and brain function in children and adolescents with autism. The results of the meta-analysis indicate that exercise can effectively improve social skills [SMD=-0.53, 95%CI (-0.76, -0.3), P=0.000].
Conclusions: Long-term, regular, chronic exercise is beneficial for children and adolescents with autism, particularly in the area of social skills.
Systematic review registration: https://www.crd.york.ac.uk/prospero PROSPERO, identifier CRD42024554530.
Autism Spectrum Disorder (ASD) is an extremely complex and highly prevalent neurodevelopmental disorder (1). Children with autism exhibit delays in communication and social skills, and demonstrate repetitive behavior patterns (2). Currently, ASD affects approximately 1% of the global population (3). Moreover, individuals with ASD face additional medical and psychiatric risks (4), such as sleep disorders (5) and executive function deficits (6).
To date, no medication can cure ASD. Conventional treatment methods, including education, psychological support therapy, and medication (7), aim to stimulate cognitive and language development while attempting to mitigate maladaptive behaviors such as stereotypy (8). These treatments also address secondary symptoms like hyperactivity, emotional instability, and aggression. Research has shown that standard treatments can have positive effects on the core issues of ASD (9). Cognitive Behavioral Therapy (CBT) can alleviate anxiety in children with ASD (10). Selective Serotonin Reuptake Inhibitors (SSRIs), commonly used to treat mood and irritability issues in ASD patients, promote neurogenesis and neuroprotection, offering potential benefits (11). However, some atypical antipsychotics have side effects, including fatigue, gastrointestinal symptoms, and more severe issues like dyslipidemia and hyperglycemia (12). Exercise, as a non-pharmacological adjunct therapy, has gained increasing attention due to its low cost and ease of implementation.
It is well known that exercise is feasible and effective in improving or assisting in the treatment of many diseases. Studies have indicated that exercise benefits social interaction deficits (13) and can reduce stereotyped behaviors in children and adolescents with autism (14, 15). Additionally, research has shown that exercise positively impacts the cognitive function of typically developing children and adolescents and reduces the potential risk of cognitive decline (16). Meanwhile, a recent meta-analysis demonstrated that exercise interventions positively affect executive functions in children and adolescents with ASD (1). Furthermore, there is evidence that social skills in ASD are related to motor skill deficits (17, 18). However, it remains inconclusive whether exercise interventions can effectively improve communication skills.
Although previous studies have systematically reviewed the effects of exercise on ASD, there has been no systematic summary specific to the population of children and adolescents. Therefore, the primary aim of this study is to systematically review the benefits of exercise for children and adolescents with ASD and to conduct a meta-analysis on the impact of exercise on social skills, in order to provide evidence-based recommendations for patient treatment.
Our study was pre-registered with PROSPERO, registration number CRD42024554530.
As of April 1, 2024, a total of four databases were searched: PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Web of Science. The search strategy was designed around the study theme, combining professional terminology and keywords. The search strategy was constructed using PICO: Population: people with ASD; Intervention: exercise; Comparator: control group with usual care or no intervention; Outcomes: outcome measures for ASD. To retain all valuable studies, there were no restrictions on study time, language, or age. Detailed search strategies can be found in Supplementary Table 1.
Participants in the studies had to be diagnosed with autism either through autism scales or by a physician. Those with a potential for autism without a confirmed diagnosis were excluded. Our study focused solely on children and adolescents, thus the upper age was limited to 18 years. The intervention for the experimental group involved exercise; however, complex exercise interventions incorporating cognitive tasks were excluded.
All studies meeting the inclusion criteria were included in the qualitative synthesis. Additionally, quantitative synthesis was conducted for the included randomized controlled trials (RCTs) that reported sufficient experimental details and required data. Observational studies, review studies, conference papers, and animal studies were excluded.
Two researchers (MY and JZ) independently screened and excluded the retrieved literature using the reference manager EndNote. A third researcher (JH) reviewed and confirmed the results. The literature screening process involved excluding duplicate studies, reading titles and abstracts for further exclusion, and performing full-text reviews of the remaining articles. During the independent evaluation by the researchers, any discrepancies were resolved through discussion within the research team.
Two researchers (MY and JZ) extracted data from studies included in the quantitative synthesis. If the studies reported the required means and standard deviations, these were directly used for statistical analysis. If the required data were presented in graphical form, the data were extracted using digital science software (Engauge Digitizer). Some experiments included multiple or long-term follow-ups after the intervention and reported experimental data. To verify the intervention effects, only the data at the end of the experiment were extracted. The data extraction results were confirmed by a third researcher (JH), and any inconsistencies were resolved through team discussions. Additionally, we recorded the details of the included qualitative studies using standardized data tables.
Two researchers (MY and JZ) conducted a methodological quality assessment of the studies included in the quantitative synthesis. The assessment tool used was the Physiotherapy Evidence Database (PEDro) scale. The PEDro scale is considered an effective tool for assessing the quality of randomized controlled trials (19). Although this scale was developed for physical therapy, it may also be suitable for other fields (20). Furthermore, existing evidence suggests that the reliability of the total score of PEDro is acceptable (21).It includes 11 criteria, such as randomization and blinding (21). However, many exercise intervention trials cannot achieve blinding, so considering this limitation, the scoring system was categorized into three quality levels: high quality (≥6 points), moderate quality (4-5 points), and low quality (≤3 points) (22). Any discrepancies in scoring between the two assessors were resolved through team discussion.
Various tools were used to measure data across different studies; therefore, the effect size needed to be calculated using the standardized mean difference (SMD), with a 95% confidence interval (CI) between groups. The effect size was interpreted as small (≤0.2), medium (≤0.5), and large (≥0.8) (23). We used the Cochrane Q test to assess statistical heterogeneity, along with I² and P-value tests. The degree of heterogeneity was classified as low (≤25%), moderate (≤50%), and high (≥75%) (24). A fixed-effect model was used for low heterogeneity, and a random-effects model was used otherwise.
A total of 5359 articles were identified through the initial search. After excluding duplicate studies, screening for relevant topics, and reading abstracts and full texts, 37 articles were found to meet the study criteria. Among these, 28 studies were included in the qualitative analysis (7, 25–51), and 9 studies (52–60) were included in the meta-analysis. The detailed selection process is illustrated in Figure 1.
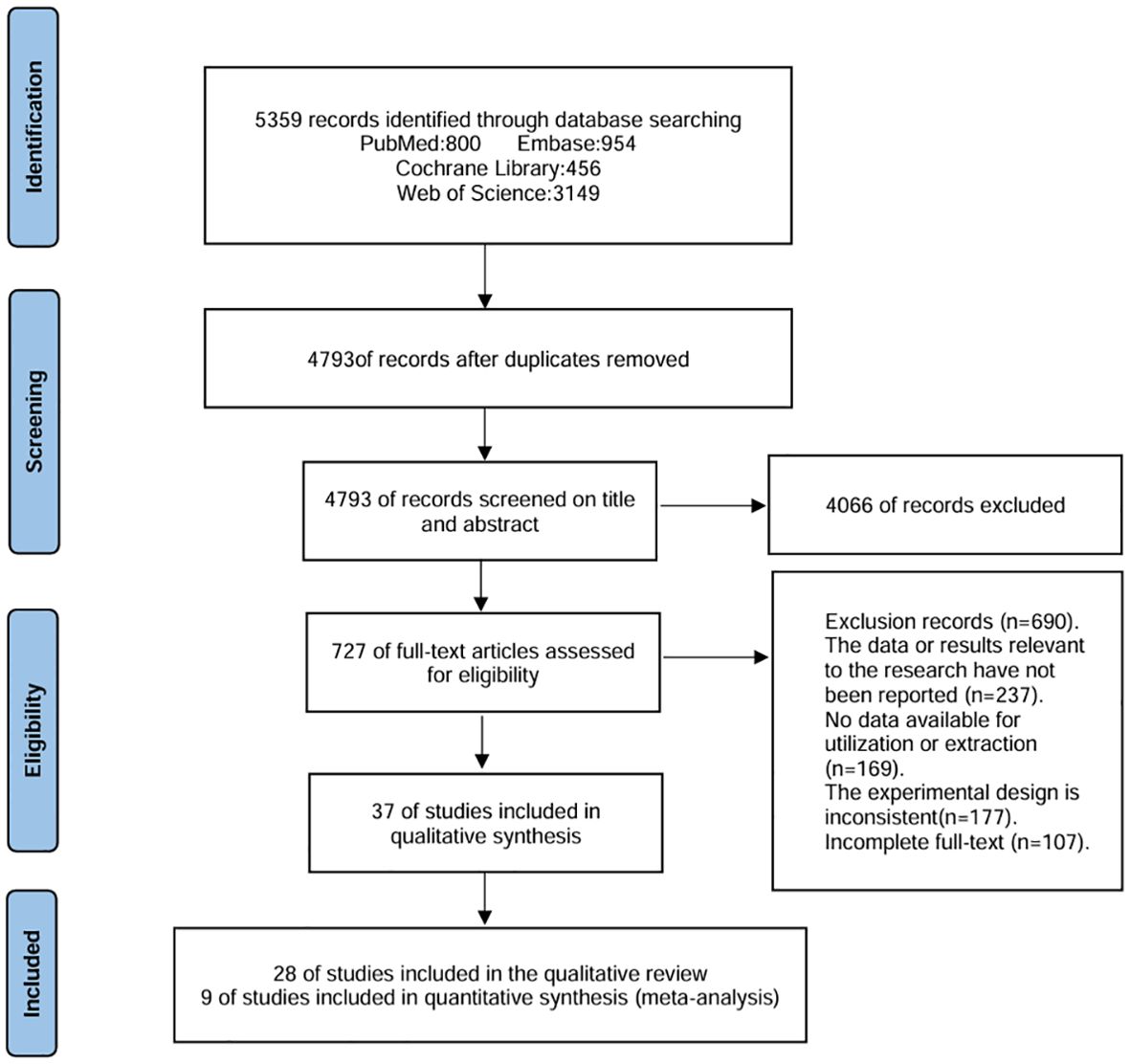
Figure 1. Search Flowchart.
Table 1 presents the detailed information of the included studies. The country with the most studies was Iran, with a total of 9 studies. China conducted 8 studies, the United States had 6 studies, India had 3 studies, Brazil, Turkey, and Australia each had 2 studies, and the UK, Tunisia, Switzerland, Italy, and Portugal each had 1 study. The age range of the 1553 participants was 2.3-17.3 years, with a higher number of male children and adolescents compared to females. The methods of symptom diagnosis included physician diagnosis, ICD-10, ADOS-2, DSM-4, DSM-5, and GARS2 scale, but 4 studies did not report specific diagnostic methods.
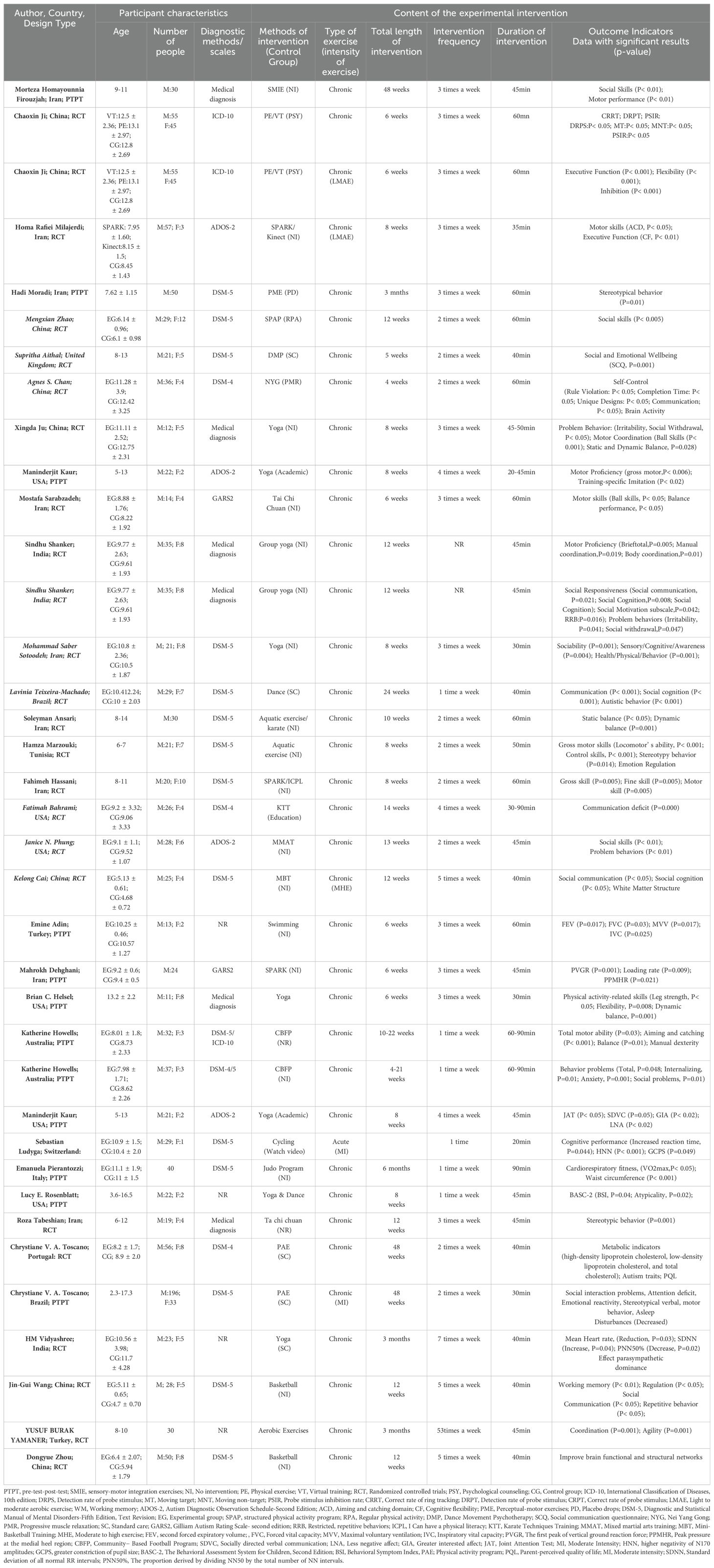
Table 1. Detailed information on qualitative analysis.
Five studies reported the specific intensity of exercise, with only one study focusing on acute exercise interventions, while the others focused on long-term exercise interventions. Regarding the frequency and duration of interventions, interventions were conducted at least once a week, with a maximum of 7 times per week, and the duration of each session ranged from 20 minutes to 90 minutes. Most studies reported positive effects of exercise, whereas the acute exercise intervention reported negative effects. In the assessment of social skills, the test content focuses on language, communication, and overall social skills evaluation. The judgment of experimental results mainly centers on the scores of the relevant scales, as these scores can specifically reflect whether the intervention has had a tangible impact on the patient, be it positive or negative.
Table 2 presents the quality assessment of the studies included in the quantitative analysis. Overall, the quality of the studies included in the meta-analysis was above average, with an overall mean score of 6.33. All studies reported the eligibility criteria for participants and achieved random allocation in the grouping. However, due to the nature of the control group not engaging in exercise, blinding of participants and therapists was not feasible.
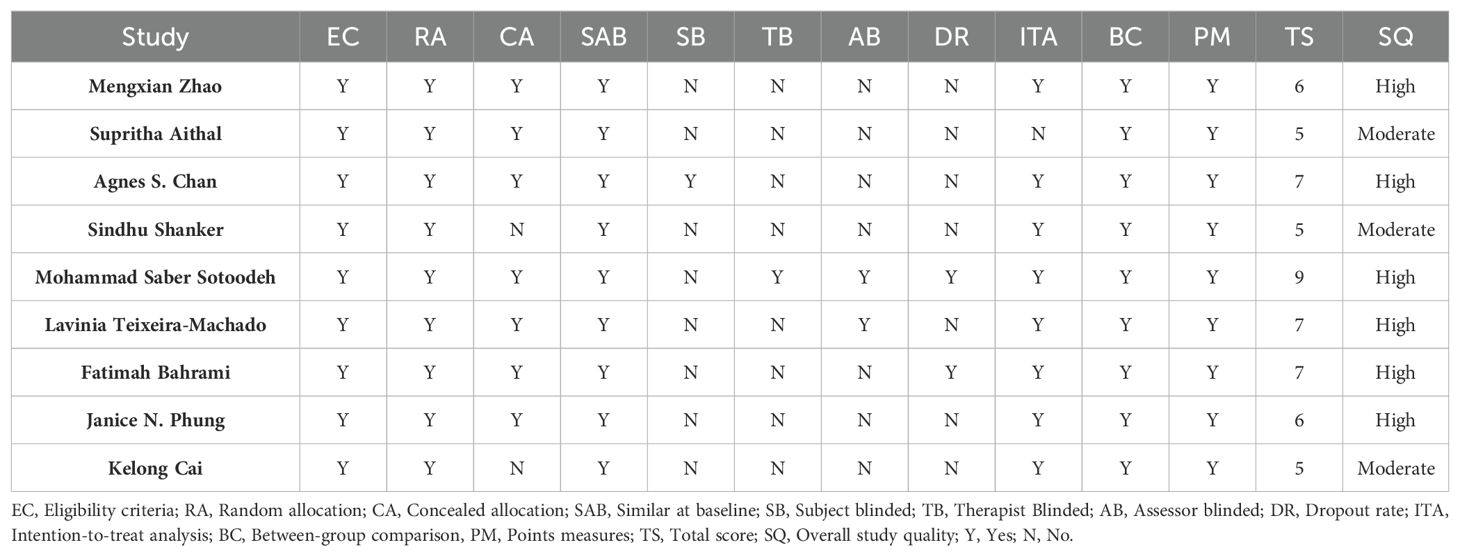
Table 2. Quality assessment results.
Nine studies reported the impact of exercise on the social function of children and adolescents with autism, as shown in Figure 2. Compared to the control group, exercise effectively improved social skills, demonstrating a moderate effect size [SMD=-0.53, 95% CI (-0.76, -0.3), P=0.000]. The statistical heterogeneity results indicated low heterogeneity among the included studies (I²=0.0%, P=0.612).
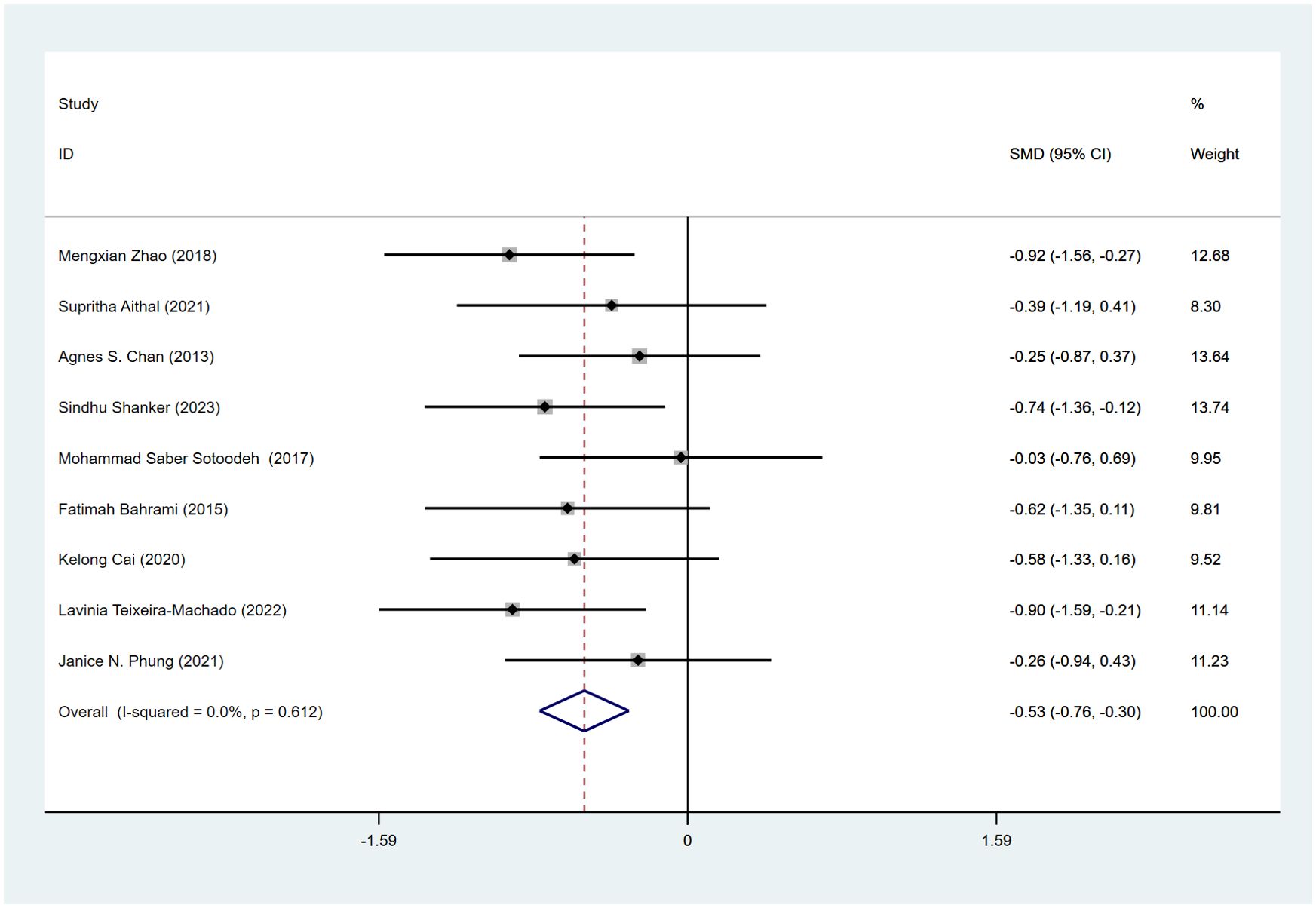
Figure 2. Meta-analysis forest plot on the effects of exercise on social skills.
Although the number of studies included in the meta-analysis did not exceed ten, a funnel plot was drawn to identify potential publication bias (see Supplementary Table 2). A visual inspection of the funnel plot showed no obvious asymmetry, and the Egger test results (P=0.328) also indicated no significant publication bias, suggesting that the study results are reasonably robust.
We utilized a standardized literature search and screening process and determined the effect size of the meta-analysis based on the existing data. The current evidence indicates that most long-term chronic exercise interventions have positive effects on children and adolescents with autism, particularly in the area of social skills.
Overall, the positive effects of exercise primarily encompass improvements in motor performance, cognitive function, individual and social relationships, behavioral problems, physical health, and brain function. This suggests that exercise can serve as an effective intervention method. The types of interventions mainly included aerobic exercises, aquatic exercises, mind-body exercises, and ball sports. However, the variations in exercise intervention types, intensities, and doses make it difficult to determine which specific methods and intervention frequencies yield the maximum benefits. The findings highlight the importance of exercise as a beneficial intervention for children and adolescents with autism. Yet, further research is needed to identify the optimal types, intensities, and frequencies of exercise interventions to maximize the benefits for this population.
In terms of motor performance, chronic exercise has been shown to improve gross motor abilities such as motor coordination, dynamic and static balance, as well as fine motor skills. Existing research indicates that exercises like walking and strength training are effective alternative therapies for improving motor skills in children with ASD (61, 62). Similarly, there is evidence supporting the enhancement of cognitive abilities through exercise, particularly in executive functions of ASD. A meta-analysis of randomized controlled trials demonstrated significant training effects of exercise interventions on overall executive functions in children with ASD and Attention Deficit Hyperactivity Disorder (ADHD) (63). Positive effects of exercise on cognitive abilities have also been observed in other neurodevelopmental disorder populations, such as children with intellectual disabilities (64). Regarding improvements in social relationships, we speculate that these may be linked to enhancements in communication skills. Improvements in indicators such as social responsibility and reduced social withdrawal are closely associated with improved communication with others. Exercise is known to enhance physical health by improving cardiovascular function, a well-established finding (65), which holds true for individuals with ASD as well.
Furthermore, through meta-analysis, we found significant improvements in social functioning among children and adolescents with ASD following regular exercise interventions. Previous studies have reported an association between motor skills and communication abilities. There is evidence of a correlation between motor skills and adaptive social skills or adaptive communication (18). However, the potential reasons for the correlation between motor skills and social skills in patients with autism remain unclear. Thus, the underlying mechanisms may involve multiple aspects, such as neurophysiological mechanisms, behavioral and psychological mechanisms. Exercise influences levels of neurotransmitters such as dopamine (66), which play important roles in emotional regulation and behavior. Enhancing these neurotransmitter levels through exercise may improve emotional states, reduce anxiety, and thereby facilitate social interactions. In terms of behavioral and psychological mechanisms, the sense of achievement that exercise brings to children and adolescents with ASD may increase their confidence and willingness to engage in social interactions. Through interactions and correlations among these potential influencing mechanisms, overall improvements in social capabilities are promoted. Of course, there are likely many other mechanisms influencing the relationship between exercise and social skills.
This study has both strengths and limitations. Firstly, we conducted the first meta-analysis examining the effects of exercise interventions on social skills in children and adolescents with ASD. Secondly, the quantitative analysis focused exclusively on randomized controlled trials, excluding observational studies, thereby enhancing the reliability and accuracy of the study outcomes. We targeted a precise intervention for children and adolescents in developmental stages, which is advantageous. However, this study also has limitations. Firstly, the number of studies included in the quantitative analysis was limited, potentially compromising the reliability of the effects of exercise interventions and making it difficult to draw definitive conclusions. Moreover, the limited number of studies suggests that other potential moderating factors may have influenced the results. Thirdly, due to differences in variables such as the severity of ASD and intervention dosages among the included studies, subgroup comparisons were not feasible.
Based on the analysis of existing literature, chronic exercise interventions are beneficial for children and adolescents with ASD, particularly in improving social skills.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
MJ: Writing – review & editing, Writing – original draft, Software, Funding acquisition, Conceptualization. JZ: Writing – review & editing, Software, Funding acquisition, Formal analysis, Data curation, Conceptualization. JP: Writing – review & editing, Supervision, Investigation, Formal analysis. FH: Writing – review & editing, Validation, Investigation, Data curation. ZZ: Writing – review & editing, Validation, Investigation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research was supported by a grant from Fundamental Research Funds for the Central Universities (2024CDJSKXYTY03).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1462601/full#supplementary-material
1. Liang X, Li R, Wong SHS, Sum RKW, Wang P, Yang B, et al. The effects of exercise interventions on executive functions in children and adolescents with autism spectrum disorder: A systematic review and meta-analysis. Sports Med. (2022) 52:75–88. doi: 10.1007/s40279-021-01545-3
2. Tarr CW, Rineer-Hershey A, Larwin K. The effects of physical exercise on stereotypic behaviors in autism: small-n meta-analyses. In: Focus on Autism and Other Developmental Disabilities, vol. 35. (2019). p. 26–35.
3. Elsabbagh M, Divan G, Koh YJ, Kim YS, Kauchali S, Marcín C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. (2012) 5:160–79. doi: 10.1002/aur.239
4. Healy S, Nacario A, Braithwaite RE, Hopper C. The effect of physical activity interventions on youth with autism spectrum disorder: A meta-analysis. Autism Res. (2018) 11:818–33. doi: 10.1002/aur.1955
5. Calhoun SL, Pearl AM, Fernandez-Mendoza J, Durica KC, Mayes SD, Murray MJ. Sleep disturbances increase the impact of working memory deficits on learning problems in adolescents with high-functioning autism spectrum disorder. J Autism Dev Disord. (2020) 50:1701–13. doi: 10.1007/s10803-019-03928-y
6. Sachse M, Schlitt S, Hainz D, Ciaramidaro A, Schirman S, Walter H, et al. Executive and visuo-motor function in adolescents and adults with autism spectrum disorder. J Autism Dev Disord. (2013) 43:1222–35. doi: 10.1007/s10803-012-1668-8
7. Toscano CVA, Ferreira JP, Quinaud RT, Silva KMN, Carvalho HM, Gaspar JM. Exercise improves the social and behavioral skills of children and adolescent with autism spectrum disorders. Front Psychiatry. (2022) 13:1027799. doi: 10.3389/fpsyt.2022.1027799
8. Sowa M, Meulenbroek R. Effects of physical exercise on Autism Spectrum Disorders: A meta-analysis. Res Autism Spectr Disord. (2012) 6:46–57. doi: 10.1016/j.rasd.2011.09.001
9. Vismara LA, Rogers SJ. Behavioral treatments in autism spectrum disorder: what do we know? Annu Rev Clin Psychol. (2010) 6:447–68. doi: 10.1146/annurev.clinpsy.121208.131151
10. Wichers RH, van der Wouw LC, Brouwer ME, Lok A, Bockting CLH. Psychotherapy for co-occurring symptoms of depression, anxiety and obsessive-compulsive disorder in children and adults with autism spectrum disorder: a systematic review and meta-analysis. Psychol Med. (2023) 53:17–33. doi: 10.1017/s0033291722003415
11. Jansson LC, Louhivuori L, Wigren HK, Nordström T, Louhivuori V, Castrén ML, et al. Brain-derived neurotrophic factor increases the motility of a particular N-methyl-D-aspartate/GABA-responsive subset of neural progenitor cells. Neuroscience. (2012) 224:223–34. doi: 10.1016/j.neuroscience.2012.08.038
12. Aishworiya R, Valica T, Hagerman R, Restrepo B. An update on psychopharmacological treatment of autism spectrum disorder. Neurotherapeutics. (2022) 19:248–62. doi: 10.1007/s13311-022-01183-1
13. Bremer E, Crozier M, Lloyd M. A systematic review of the behavioural outcomes following exercise interventions for children and youth with autism spectrum disorder. Autism. (2016) 20:899–915. doi: 10.1177/1362361315616002
14. Petrus C, Adamson SR, Block L, Einarson SJ, Sharifnejad M, Harris SR. Effects of exercise interventions on stereotypic behaviours in children with autism spectrum disorder. Physiother Can. (2008) 60:134–45. doi: 10.3138/physio.60.2.134
15. Ferreira JP, Ghiarone T, Júnior CRC, Furtado GE, Carvalho HM, Rodrigues AM, et al. Effects of physical exercise on the stereotyped behavior of children with autism spectrum disorders. Medicina (Kaunas). (2019) 55. doi: 10.3390/medicina55100685
16. Erickson KI, Hillman C, Stillman CM, Ballard RM, Bloodgood B, Conroy DE, et al. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med Sci Sports Exerc. (2019) 51:1242–51. doi: 10.1249/mss.0000000000001936
17. Bhat AN, Galloway JC, Landa RJ. Relation between early motor delay and later communication delay in infants at risk for autism. Infant Behav Dev. (2012) 35:838–46. doi: 10.1016/j.infbeh.2012.07.019
18. MacDonald M, Lord C, Ulrich D. The relationship of motor skills and adaptive behavior skills in young children with autism spectrum disorders. Res Autism Spectr Disord. (2013) 7:1383–90. doi: 10.1016/j.rasd.2013.07.020
19. Fang Q, Aiken CA, Fang C, Pan Z. Effects of exergaming on physical and cognitive functions in individuals with autism spectrum disorder: A systematic review. Games Health J. (2019) 8:74–84. doi: 10.1089/g4h.2018.0032
20. Macedo LG, Elkins MR, Maher CG, Moseley AM, Herbert RD, Sherrington C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J Clin Epidemiol. (2010) 63:920–5. doi: 10.1016/j.jclinepi.2009.10.005
21. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) 83:713–21. doi: 10.1093/ptj/83.8.713
22. Armijo-Olivo S, da Costa BR, Cummings GG, Ha C, Fuentes J, Saltaji H, et al. PEDro or cochrane to assess the quality of clinical trials? A meta-epidemiological study. PloS One. (2015) 10:e0132634. doi: 10.1371/journal.pone.0132634
23. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
24. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
25. Homayounnia Firouzjah M, Majidi Yaeichi N, Hematinia R. The effectiveness of sensory-motor integration exercises on social skills and motor performance in children with autism. J Autism Dev Disord. (2024).
26. Ji C, Yang J. Effects of physical exercise and virtual training on visual attention levels in children with autism spectrum disorders. Brain Sci. (2021) 12. doi: 10.3390/brainsci12010041
27. Ji C, Yang J, Lin L, Chen S. Executive function improvement for children with autism spectrum disorder: A comparative study between virtual training and physical exercise methods. Children (Basel). (2022) 9. doi: 10.3390/children9040507
28. Rafiei Milajerdi H, Sheikh M, Najafabadi MG, Saghaei B, Naghdi N, Dewey D. The effects of physical activity and exergaming on motor skills and executive functions in children with autism spectrum disorder. Games Health J. (2021) 10:33–42. doi: 10.1089/g4h.2019.0180
29. Moradi H, Sohrabi M, Taheri H, Khodashenas E, Movahedi A. Comparison of the effects of perceptual-motor exercises, vitamin D supplementation and the combination of these interventions on decreasing stereotypical behavior in children with autism disorder. Int J Dev Disabil. (2018) 66:122–32. doi: 10.1080/20473869.2018.1502068
30. Ju X, Liu H, Xu J, Hu B, Jin Y, Lu C. Effect of yoga intervention on problem behavior and motor coordination in children with autism. Behav Sci (Basel). (2024) 14. doi: 10.3390/bs14020116
31. Kaur M, Bhat A. Creative yoga intervention improves motor and imitation skills of children with autism spectrum disorder. Phys Ther. (2019) 99:1520–34. doi: 10.1093/ptj/pzz115
32. Sarabzadeh M, Azari BB, Helalizadeh M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. J Bodyw Mov Ther. (2019) 23:284–90. doi: 10.1016/j.jbmt.2019.01.007
33. Shanker S, Pradhan B. Effect of yoga on the motor proficiency of children with autism spectrum disorder and the feasibility of its inclusion in special school environments. Adapt Phys Activ Q. (2022) 39:247–67. doi: 10.1123/apaq.2021-0108
34. Ansari S, Elmieh A, Hojjati Z. Effects of aquatic exercise training on pain, symptoms, motor performance, and quality of life of older males with knee osteoarthritis. Ann-Appl-Sport-Sci. (2014) 2:29–38. doi: 10.18869/acadpub.aassjournal.2.2.29
35. Marzouki H, Soussi B, Selmi O, Hajji Y, Marsigliante S, Bouhlel E, et al. Effects of aquatic training in children with autism spectrum disorder. Biol (Basel). (2022) 11. doi: 10.3390/biology11050657
36. Hassani F, Shahrbanian S, Shahidi SH, Sheikh M. Playing games can improve physical performance in children with autism. Int J Dev Disabil. (2022) 68:219–26. doi: 10.1080/20473869.2020.1752995
37. Adin E, Pancar Z. Effect of swimming exercise on respiratory muscle strength and respiratory functions in children with autism. Eurasian J Med. (2023) 55:135–9. doi: 10.5152/eajm.2023.0118
38. Dehghani M, Jafarnezhadgero AA, Darvishani MA, Aali S, Granacher U. Effects of an 8-week multimodal exercise program on ground reaction forces and plantar pressure during walking in boys with autism spectrum disorder. Trials. (2023) 24:170. doi: 10.1186/s13063-023-07158-7
39. Helsel BC, Foster RNS, Sherman J, Ptomey LT, Montgomery RN, Washburn RA, et al. A remotely delivered yoga intervention for adolescents with autism spectrum disorder: feasibility and effectiveness for improving skills related to physical activity. J Autism Dev Disord. (2023) 53:3958–67. doi: 10.1007/s10803-022-05702-z
40. Howells K, Sivaratnam C, Lindor E, He J, Hyde C, McGillivray J, et al. Can a community-based football program benefit motor ability in children with autism spectrum disorder? A pilot evaluation considering the role of social impairments. J Autism Dev Disord. (2022) 52:402–13. doi: 10.1007/s10803-021-04933-w
41. Howells K, Sivaratnam C, Lindor E, Hyde C, McGillivray J, Whitehouse A, et al. Can participation in a community organized football program improve social, behavioural functioning and communication in children with autism spectrum disorder? A pilot study. J Autism Dev Disord. (2020) 50:3714–27. doi: 10.1007/s10803-020-04423-5
42. Kaur M, Eigsti IM, Bhat A. Effects of a creative yoga intervention on the joint attention and social communication skills, as well as affective states of children with Autism Spectrum Disorder. Res Autism Spectr Disord. (2021) 88. doi: 10.1016/j.rasd.2021.101860
43. Ludyga S, Gerber M, Bruggisser F, Leuenberger R, Brotzmann M, Trescher S, et al. A randomized cross-over trial investigating the neurocognitive effects of acute exercise on face recognition in children with autism spectrum disorder. Autism Res. (2023) 16:1630–9. doi: 10.1002/aur.2977
44. Pierantozzi E, Morales J, Fukuda DH, Garcia V, Gómez AM, Guerra-Balic M, et al. Effects of a long-term adapted judo program on the health-related physical fitness of children with ASD. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph192416731
45. Rosenblatt LE, Gorantla S, Torres JA, Yarmush RS, Rao S, Park ER, et al. Relaxation response-based yoga improves functioning in young children with autism: a pilot study. J Altern Complement Med. (2011) 17:1029–35. doi: 10.1089/acm.2010.0834
46. Tabeshian R, Nezakat-Alhosseini M, Movahedi A, Zehr EP, Faramarzi S. The effect of tai chi chuan training on stereotypic behavior of children with autism spectrum disorder. J Autism Dev Disord. (2022) 52:2180–6. doi: 10.1007/s10803-021-05090-w
47. Toscano CVA, Carvalho HM, Ferreira JP. Exercise effects for children with autism spectrum disorder: metabolic health, autistic traits, and quality of life. Percept Mot Skills. (2018) 125:126–46. doi: 10.1177/0031512517743823
48. Vidyashree HM, Maheshkumar K, Sundareswaran L, Sakthivel G, Partheeban PK, Rajan R. Effect of yoga intervention on short-term heart rate variability in children with autism spectrum disorder. Int J Yoga. (2019) 12:73–7. doi: 10.4103/ijoy.ijoy_66_17
49. Wang JG, Cai KL, Liu ZM, Herold F, Zou L, Zhu LN, et al. Effects of mini-basketball training program on executive functions and core symptoms among preschool children with autism spectrum disorders. Brain Sci. (2020) 10. doi: 10.3390/brainsci10050263
50. Yamaner YB, Demirli A, Moghanlou AE, Gökçelik E. The effect of aerobic exercises on skill behaviour of autestic children. Pakistan J Med Health Sci. (2022) 16:713–. doi: 10.53350/pjmhs22163713
51. Zhou D, Liu Z, Gong G, Zhang Y, Lin L, Cai K, et al. Decreased functional and structural connectivity is associated with core symptom improvement in children with autism spectrum disorder after mini-basketball training program. J Autism Dev Disord. (2023).
52. Zhao M, Chen S. The effects of structured physical activity program on social interaction and communication for children with autism. BioMed Res Int. (2018) 2018:1825046. doi: 10.1155/2018/1825046
53. Aithal S, Karkou V, Makris S, Karaminis T, Powell J. A dance movement psychotherapy intervention for the wellbeing of children with an autism spectrum disorder: A pilot intervention study. Front Psychol. (2021) 12:588418. doi: 10.3389/fpsyg.2021.588418
54. Chan AS, Sze SL, Siu NY, Lau EM, Cheung MC. A chinese mind-body exercise improves self-control of children with autism: a randomized controlled trial. PloS One. (2013) 8:e68184. doi: 10.1371/journal.pone.0068184
55. Shanker S, Pradhan B. Effect of yoga on the social responsiveness and problem behaviors of children with ASD in special schools: A randomized controlled trial. Explore (NY). (2023) 19:594–9. doi: 10.1016/j.explore.2022.12.004
56. Sotoodeh MS, Arabameri E, Panahibakhsh M, Kheiroddin F, Mirdoozandeh H, Ghanizadeh A. Effectiveness of yoga training program on the severity of autism. Complement Ther Clin Pract. (2017) 28:47–53. doi: 10.1016/j.ctcp.2017.05.001
57. Teixeira-MaChado L, Arida RM, Ziebold C, Barboza AB, Ribeiro L, Teles MC, et al. A pilot randomized controlled clinical trial of dance practice for functionality in autistic children and adolescent with all levels of need support. Complement Ther Clin Pract. (2022) 49:101650. doi: 10.1016/j.ctcp.2022.101650
58. Bahrami F, Movahedi A, Marandi SM, Sorensen C. The effect of karate techniques training on communication deficit of children with autism spectrum disorders. J Autism Dev Disord. (2016) 46:978–86. doi: 10.1007/s10803-015-2643-y
59. Phung JN, Goldberg WA. Mixed martial arts training improves social skills and lessens problem behaviors in boys with Autism Spectrum Disorder. Res Autism Spectr Disord. (2021) 83:101758. doi: 10.1016/j.rasd.2021.101758
60. Cai K, Yu Q, Herold F, Liu Z, Wang J, Zhu L, et al. Mini-basketball training program improves social communication and white matter integrity in children with autism. Brain Sci. (2020) 10. doi: 10.3390/brainsci10110803
61. Dong L, Shen B, Pang Y, Zhang M, Xiang Y, Xing Y, et al. FMS effects of a motor program for children with autism spectrum disorders. Percept Mot Skills. (2021) 128:1421–42. doi: 10.1177/00315125211010053
62. Fessia G, Manni D, Contini L, Astorino F. Strategies of planned physical activity in autism: systematic review. Rev Salud Publica (Bogota). (2018) 20:390–5.
63. Zhang M, Liu Z, Ma H, Smith DM. Chronic physical activity for attention deficit hyperactivity disorder and/or autism spectrum disorder in children: A meta-analysis of randomized controlled trials. Front Behav Neurosci. (2020) 14:564886. doi: 10.3389/fnbeh.2020.564886
64. Sibley B, Etnier J. The relationship between physical activity and cognition in children: A meta-analysis. Pediatr Exercise Sci. (2003) 15:243–56. doi: 10.1123/pes.15.3.243
65. Fentem PH. ABC of sports medicine. Benefits of exercise in health and disease. Bmj. (1994) 308:1291–5. doi: 10.1136/bmj.308.6939.1291
Keywords: exercise, autism, positive effect, social skills, long-term approach
Citation: Jia M, Zhang J, Pan J, Hu F and Zhu Z (2024) Benefits of exercise for children and adolescents with autism spectrum disorder: a systematic review and meta-analysis. Front. Psychiatry 15:1462601. doi: 10.3389/fpsyt.2024.1462601
Received: 12 July 2024; Accepted: 19 September 2024;
Published: 07 October 2024.
Edited by:
Joana M Gaspar, Federal University of Santa Catarina, BrazilReviewed by:
Deborah Ann Pearson, University of Texas Health Science Center at Houston, United StatesCopyright © 2024 Jia, Zhang, Pan, Hu and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jia Zhang, emhhbmdqaWFhYUBjcXUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.