 Lindsey Fisher-Fox
Lindsey Fisher-Fox MacKenzie Whitener
MacKenzie Whitener Wei Wu1
Wei Wu1 Melissa A. Cyders
Melissa A. Cyders Tamika C. B. Zapolski
Tamika C. B. Zapolski- 1Department of Psychology, Indiana University – Indianapolis, Indianapolis, IN, United States
- 2Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, United States
Introduction: Adolescence is a key developmental period characterized by increased maladaptive risky behaviors. Two related but distinct constructs, urgency (the tendency to act rashly in response to strong negative or positive emotions) and emotion dysregulation, are important risk factors for engaging in maladaptive risky behaviors. Thus far, research has largely agreed that these two risk factors are highly correlated. However, the causal direction between these constructs is less understood. The goal of the current study is to determine whether urgency predicts emotion dysregulation change among adolescents.
Method: This project is an analysis of 544 youth (49.8% female, Mage=14.22, SD=0.52). We tested whether urgency at baseline predicts change in emotion dysregulation over a nine-week period, and whether that relationship differs across boys and girls.
Results: Two multigroup latent change score path analyses found that negative, but not positive, urgency significantly predicted emotion dysregulation change (negative urgency: b= -0.57, p=0.001; positive urgency: b=0.22, p=0.06). There was no evidence of moderation by gender.
Discussion: This work provides initial evidence of a temporal relationship between higher negative urgency and increased emotion dysregulation. The next step is to determine whether negative urgency imparts risk for maladaptive behaviors through its effect on emotion dysregulation. The long-term goal of this program of research is to design and test interventions to reduce the impact of negative urgency for adolescent risk-taking.
1 Introduction
Adolescence is a key developmental period for the emergence and development of maladaptive risky behaviors (1–4) and is associated with increased emotional lability and risk-taking behaviors (5). Adolescents show marked increases in drinking alcohol, drinking and driving, using substances, engaging in risky sexual behaviors, and many other risk behaviors (2, 6–10). Two related but distinct constructs, urgency (the tendency to act rashly in response to strong negative or positive emotions) and emotion dysregulation, are important risk factors for engaging in maladaptive risky behaviors (11–13). Thus far, research has largely agreed that these two risk factors are related (14–17); however, the causal direction between these constructs is less understood. The goal of the current study is to determine whether urgency predicts emotion dysregulation change among adolescents.
Negative and positive urgency (18) reflect individual difference tendencies toward rash or maladaptive action during extreme emotional states. In adolescents, negative urgency relates to a wide range of maladaptive risk taking, including suicide attempts and non-suicidal self-injury, as well as the onset of binge eating and alcohol, marijuana, cigarette, and other drug use (19–29). Similarly, positive urgency relates to non-suicidal self-injury, and predicts the onset of cigarette, marijuana, and alcohol use (20, 22, 25, 28, 29). Despite these well-established relationships, the mechanism(s) by which negative and positive urgency impart risk are less well understood.
Emotion dysregulation, defined as engaging in a behavior to cope with emotions that is producing a dysfunctional, rather than an adaptive, outcome (30), may be a prime mechanism for how urgency increases maladaptive risk taking in adolescents. Emotion dysregulation is a hallmark symptom of and risk factor for psychopathology (13, 31–33). In youth, emotion dysregulation predicts aggressive behavior, deliberate self-harm, risky sexual behaviors, substance use, and eating pathology (13, 34–40). Interestingly, one study found that psychopathology does not, in turn, predict increases in emotion dysregulation (13), suggesting that emotion dysregulation may be a precursor of psychopathology and not the other way around.
Research has established that urgency and emotion dysregulation are related constructs, with moderate to strong bivariate correlations (r=0.32-0.70) (14–17, 41–47). Some work has conceptualized urgency as poor emotion regulation (48), with others supporting relationships between urgency and the use of fewer appropriate, and more inappropriate, emotion regulation strategies (49). Research has found that negative and positive urgency are significantly associated with emotion dysregulation (16), but that emotion dysregulation is not significantly associated with urgency (15). Importantly, these studies utilized cross-sectional data, so the temporal order of the relationship between urgency and emotion dysregulation cannot be inferred, leaving the causal direction between these constructs unknown.
Additionally, gender may impact the relationship between urgency and emotion dysregulation. First, boys more likely to engage in risky behavior than girls (50). Second, girls begin using emotion regulation strategies more quickly (51) and experience more emotion dysregulation (52, 53) and less emotional clarity, whereas boys have more difficulty with emotional awareness (52, 53). Third, there is some evidence that males may have higher levels of positive urgency (54), and females may have higher levels of negative urgency (55, 56), although some studies have failed to find gender differences in urgency (57, 58).
The current study
The goal of the current study is to determine whether negative and positive urgency predict emotion dysregulation change in adolescents. The underlying theoretical model for the current study proposes that trait urgency is an underlying predisposition that leads to the development of maladaptive risky behaviors, while emotion dysregulation is a set of skills (or lack thereof) that develops in part due to the underlying urgency predisposition, which then further reinforces maladaptive risk. Alternative conceptualizations exist, including conceptualizing urgency and emotion dysregulation as one and the same (14, 15, 48, 59–61). In the absence of experimental or longitudinal work establishing this pathway direction, we relied on theory (18) suggesting urgency as the precursor, as well as general evidence that personality develops temporally earlier (62–65) than emotion dysregulation (51, 66, 67).
Hypotheses
The hypotheses for the current study, supported by the reviewed literature, are as follows:
Hypothesis 1: Baseline negative urgency will significantly predict change in emotion dysregulation from baseline to the follow-up, such that negative urgency will be associated with increased emotion dysregulation. Gender will moderate the relationship, such that the relationship will be stronger in girls than in boys.
Hypothesis 2: Baseline positive urgency will significantly predict change in emotion dysregulation from baseline to the follow-up, such that positive urgency will be associated with increased emotion dysregulation. Gender will moderate the relationship, such that the relationship will be stronger in in girls than in boys.
Methods
This study is a secondary analysis of the Going 4 Goals project (PI: Zapolski), which seeks to determine the effectiveness of a brief adaptation of the skills group component of dialectical behavioral therapy for adolescents (DBT-A) to reduce risky behaviors among high school students who were engaging or at risk of engaging in high-risk behaviors, such as substance use, as identified by school staff (see protocol for full description of Going 4 Goals project, 68). The Going 4 Goals Project included a control sample of students who did not participate in the program but were included to compare changes in study outcomes to those students who did participate in the program. This study utilizes only the control sample from the parent study who did not receive any DBT-A skills training to eliminate systematic differences between the control and intervention groups due to the DBT-A intervention or pre-morbid risk profiles.
Participants
Participants were 544 ninth-grade high school students who ranged in age from 13 to 15 (49.8% female, MAge=14.22, SD=0.52) from a local public high school in Indianapolis recruited during the school’s health class at the beginning of either the Fall or Spring semester (between Fall of 2018 and Spring of 2020). Participants were offered the opportunity to participate while enrolled in a state-mandated health education class at their school.
Measures
Emotion dysregulation
The Emotion Dysregulation Scale short version (EDS-s) is a 12-item self-report measure that examines the construct of emotion dysregulation across three domains: emotional experience, cognition, and behavior (69). Items were scored on a 7-point Likert scale ranging from 1 (not true) to 7 (very true). Example items include “emotions overwhelm me” and “when I’m upset, I have trouble seeing or remembering anything good about myself.” This scale was found to have high internal consistency in the current sample (Cronbach’s alpha = 0.96), which is consistent with previous research [Cronbach’s alpha = 0.93 – 0.95; (69)]. This total score was calculated using a sum of the items. The EDS was completed at baseline and nine weeks later.
Negative urgency
Negative urgency was measured using the negative urgency subscale of the full UPPS-P modified for children [UPPS-PC; (70)]. Items were measured on a 4-point Likert scale from 1 (not at all like me) to 4 (very much like me), such that higher scores are indicative of more impulsive tendencies. One example item is, “When I feel bad, I often act without thinking.” The UPPS-PC uses eight items to assess negative urgency. This subscale was found to have good internal consistency in the current sample (Cronbach’s alpha = 0.85), which is consistent with previous research of the full UPPS-PC [Cronbach’s alpha = 0.81-0.90; (70)]. The total negative urgency score was calculated using a sum of items. Data from the baseline session was used for data analysis.
Positive urgency
Positive urgency, a component of impulsivity, was measured using the positive urgency subscale of the full UPPS-PC (UPPS-PC; 70). The items were measured on a 4-point Likert scale from 1 (not at all like me) to 4 (very much like me), such that higher scores are indicative of more impulsive tendencies with items such as “when I get really happy about something, I tend to do things that lead to trouble.” The UPPS-PC uses eight items to assess positive urgency. This subscale was found to have high internal consistency in the current sample (Cronbach’s alpha = 0.9), which is consistent with previous research with the UPPS-PC (Cronbach’s alpha = 0.81-0.90; 70). The total positive urgency score was calculated using a sum of items. Data from the baseline session was used for data analysis.
Procedure
The school staff sent all students an opt-out consent form letter for parent and/or guardian approval. The letter contained the study purpose, risks, benefits, and inclusion and exclusion criteria. Guardians were asked to sign and return the letter if they did not wish their student to participate and were given a period of two weeks to return the letter. After the two-week period passed, students who wished to participate signed assent forms and completed surveys assessing baseline measurements of the outcome variables. These measures were then collected again nine weeks later. Researchers provided snacks to study participants as incentives for completing the baseline and follow-up surveys.
Data analysis
All analyses were performed in R (71).
Data cleaning
Before beginning data analysis, participants were removed due to missing data at baseline, not providing a response to the gender item, or not identifying as cisgender male or female: Six participants were removed from the data set for not providing a response to the gender demographics item, and an additional five participants were removed for responding as transgender or “other” gender. While it is important to examine gender beyond the male and female binary, the sample of other genders was not large enough to be adequately powered to determine an effect; thus, the decision was to remove them for this analysis. There were 5 other participants removed from the data set due to missing the EDS-s or UPPS-PC at baseline. After removing those participants, there were 528 remaining participants for analysis.
Missing data analysis
The data set was then assessed for missingness. A test for missing completely at random (MCAR) was conducted on each of the variables of interest using Little’s test statistic (72). They were each non-significant, indicating that the data missing in the EDS-s and the UPPS-PC were MCAR. The EDS-s was found to have 0.4% missing data at baseline and 12% missing data at follow-up. The negative urgency subscale and positive urgency subscale each had 0.3% missing data at baseline. Upon a visual inspection of the data set, the missing data at the baseline time points were for individual items within the measures. Thus, given the small amount of missing data and MCAR mechanism, we calculated scale scores using the person mean imputation approach (73). Specifically, a total scale score was calculated for the EDS-s at baseline and follow-up, negative urgency at baseline, and positive urgency at baseline by taking a sum of the individual item scores for each participant. Note that those scale scores were only used in descriptive and preliminary analyses. For the confirmatory factor and latent change score models described below, the target constructs were included as latent variables with missing data on the individual items handled using the full information maximum likelihood estimation method (FIML).
Preliminary analyses
All variables were assessed for normal distribution skewness, kurtosis, and outliers. Previous research indicates that skewness between -2 and +2 and kurtosis between -7 and +7 are considered to be within a normal distribution range (74, 75). Bivariate correlations, t-tests, and an ANOVA were conducted to examine the associations between positive urgency, negative urgency, emotion dysregulation, and sample characteristics with the “psych” package in R (76).
Measurement invariance
Confirmatory factory analysis (CFA) was used to assess the factor structure of the EDS-s at baseline and follow-up and the negative and positive urgency items of the UPPS-PC using the “lavaan” package in R (77). A single-factor model was first fit to the data for each construct with the gender groups combined. Each latent construct was identified using the indicator approach (i.e., fix one of the item loadings to be 1). Model fit was assessed using the comparative fit index (CFI) and the root mean squared error or approximation (RMSEA): RMSEA<0.08 and CFI >0.90 were deemed adequate (78, 79). To ensure that the constructs were comparable across gender groups, measurement invariance of each latent construct between boys and girls was then evaluated using a series of multigroup CFA analyses (78) by sequentially adding equality constraints on parameters across groups: 1) configural (no parameter constraints), 2) weak invariance (factor loadings equated), and 3) strong invariance (factor loadings and intercepts equated). Configural invariance was established if the model fit the data. Weak and strong invariance were evaluated using chi-squared difference tests (Δχ2), as well as changes in CFI and RMSEA (ΔCFI and ΔRMSEA). While there are no set cut-off criteria, the current standard is to accept models that show ΔCFI and ΔRMSEA ≤.01 (80). Note that for the purpose of the current study (compare relationships among latent variables across groups), weak invariance would be sufficient.
Invariance of the EDS-s across time (baseline to follow-up assessments) was evaluated using the same process of adding equality constraints across the two assessment periods (81): 1) configural (no parameter constraints), 2) weak invariance (factor loadings equated), and 3) strong invariance (factor loadings and intercepts equated). The same fit indices as previously mentioned were used to evaluate model fit.
Hypothesis testing
After establishing weak invariance held for all the constructs, two multigroup latent change score models (see Figure 1 for the model specifications) were built to test whether baseline negative and positive urgency predicted change in emotion dysregulation from baseline to follow-up and if the associations differed by gender. All models were estimated using FIML for missing data with the “lavaan” package in R (77). The latent change score models modeled the change as a latent variable, removing the influence of measurement errors and facilitating the use of FIML in dealing with missing data on difference scores (82, 83). The first model allowed the associations to be different across boys and girls, and the second one equated them across groups. Note that for emotion dysregulation, since it was measured at two time points, the residuals on the same item were allowed to be correlated across time. The two models were nested and compared using Δχ2, with a significant result suggesting a moderation effect of gender (i.e., the associations significantly differed across group). As a sensitivity analysis, an additional equality constraint model was run on both positive and negative urgency, in separate models, such that the coefficients were constrained to be equal for negative, but not positive urgency, and vice versa, allowing to examine whether gender moderation occurred for one trait, but not the other. Cohen’s guidelines for coefficient β were used to determine the effect size of the relationships between negative and positive urgency and emotion dysregulation (84).
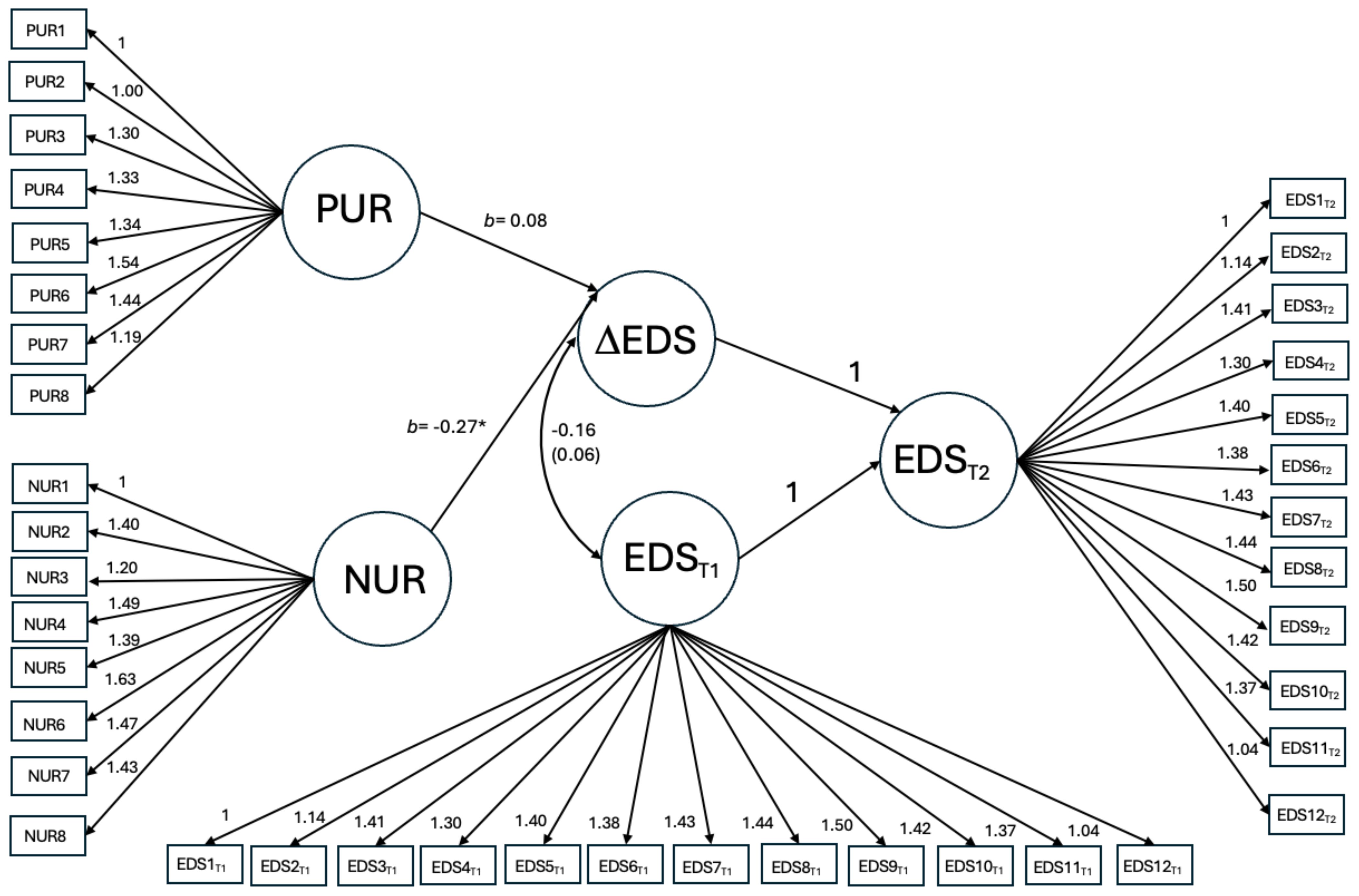
Figure 1. Path diagram for the multiple group latent change score model with regression coefficients associated with negative and positive urgency freely estimated across gender. For emotion dysregulation, since it was measured at two time points, the residuals on the same item were allowed to covary across time. For simplicity, these covariances were included in the model but omitted from the graph. Results were similar comparing unconstrained to models with only negative urgency or only positive urgency constrained, although they trended towards having worse fit. NUR=negative urgency, PUR=positive urgency, EDST1= EDS-s at baseline, EDST2= EDS-s at follow-up, ΔEDS = change in EDS-s from baseline to follow-up. *p<0.05.
Results
Sample characteristics
Participants were between the ages of 13-16 and, on average, 14 years old (M=14.21, SD=0.52); 74% of the participants were 14 years old. Because of this, age was not included as a covariate in hypothesis testing. The sample was mostly Black or White (31.3% African American/Black, 27.4% White, 0.4% Asian American/Pacific Islander, 1.9% Native American/American Indian/Alaskan Native, 6.3% Other race, and 18.7% more than one race, 24.2% did not respond to race demographic item), mostly not Hispanic/Latino (25.1% Hispanic/Latino), and in ninth grade (100%).
Preliminary analyses
Skewness and kurtosis were within normal limits for each study variable. Means, standard deviations, and correlations of study variables can be found in Table 1. As expected, negative urgency, positive urgency, and emotion dysregulation (both baseline and follow-up), showed positive, significant correlations (all p’s<0.001). Boys demonstrated lower negative urgency [t(526)=-3.23, p=0.001; boys: M=18.21, SD=5.13 and girls: M=19.76, SD=5.82)] and emotion dysregulation at both baseline [t(526)= -6.39, p<0.001; boys: M1 = 36.72, SD1 = 16.41; girls: M1 = 46.55, SD1 = 18.88] and follow-up [t(458)= -6.02, p<0.001; boys: M2 = 35.92, SD2 = 17.26; girls M2 = 46.06, SD2 = 18.84) than girls. There was no difference in positive urgency across gender [t(526)= -0.20, p=0.84].
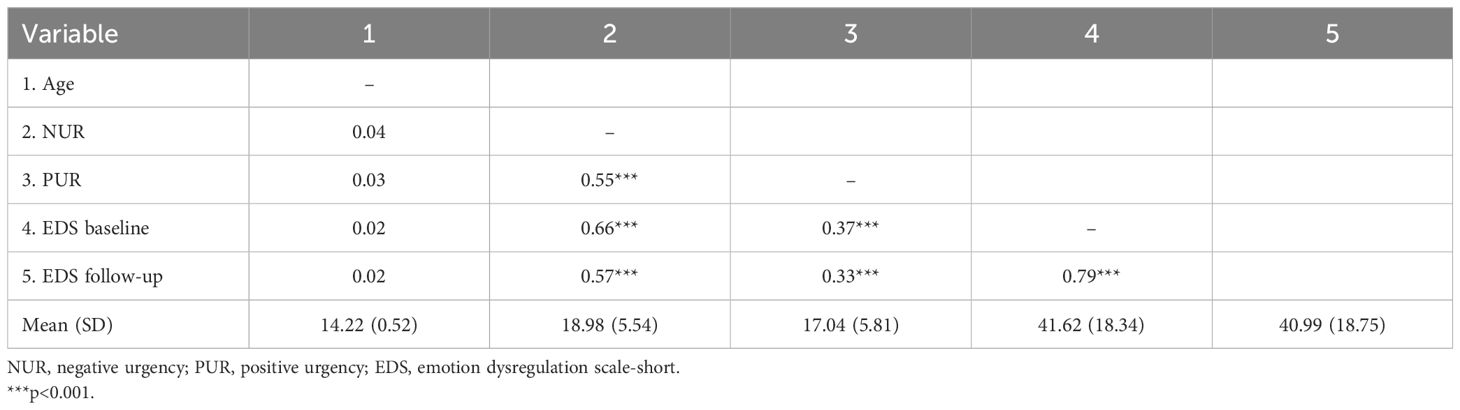
Table 1. Means, standard deviations, and correlations of key study variables.
Measurement invariance
First, the factor structure for the EDS-s at baseline and at follow-up supported a single factor fit the data with the two groups combined (baseline: RMSEA = 0.073, 90% CI = [0.063, 0.084], CFI = 0.96; follow-up: RMSEA = 0.058, 90% CI [0.046, 0.070], CFI = 0.98). Three residual covariances were included across six items (items five and nine, items 11 and 12, and items one and nine). For negative negative urgency, two residual covariances were included (items 17 and 26 and items 20 and 30) and a single factor fit the data with the two groups combined (RMSEA = 0.067, 90% CI [0.049, 0.086], CFI = 0.97). For positive urgency, six residual covariances were included (items 38 and 39, items 36 and 40, items 33 and 34, items 35 and 38, items 34 and 36, and items 33 and 36) and a single factor fit the data with the two groups combined (RMSEA = 0.080, 90% CI [0.060, 0.101], CFI = 0.98).
Second, measurement invariance analyses were conducted for each construct (see Table 2). The configural invariance models with the multiple group CFA also showed an adequate fit. The models with factor loadings equated did not have a significantly different model fit from the corresponding configural models, supporting weak invariance. The strong invariance models showed significantly worse χ2 for all constructs except for positive urgency. Although ΔCFIs from weak to strong invariance were less than.01 for most of the constructs, ΔRMSEAs were all greater than the threshold, indicating that strong invariance was not established. Based on the result, weak invariance was assumed. Correspondingly, in subsequent hypothesis testing models, item loadings were constrained to be equal across boys and girls, but intercepts were not.
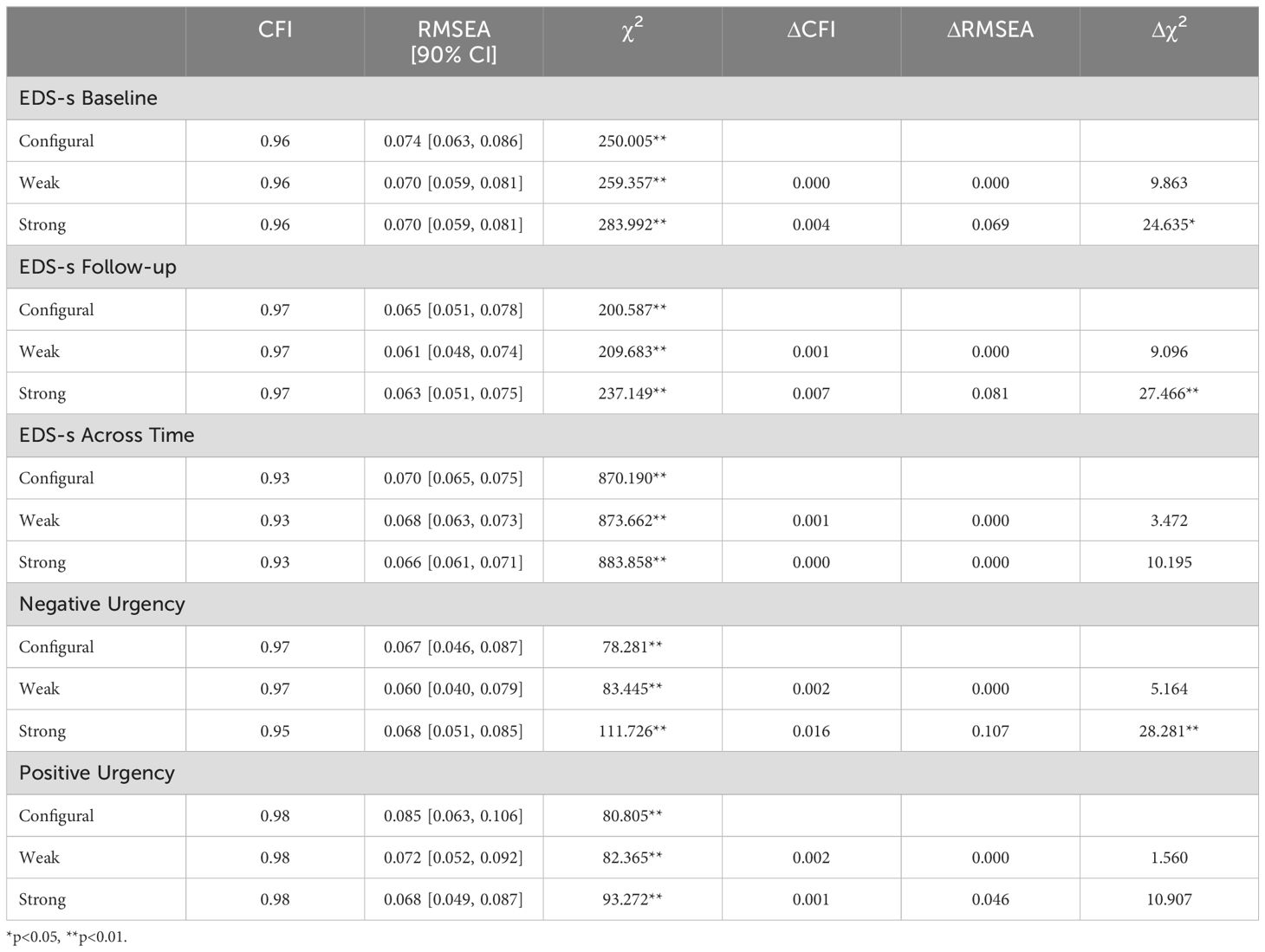
Table 2. Measurement Invariance for Sex (dummy coded against Male).
Third, configural invariance of the EDS-s across time showed an adequate fit (see Table 2). The model with the factor loadings equated did not have a significantly different model fit from the corresponding configural model, supporting weak invariance. The strong invariance model did not have a significantly different model fit from the configural model, supporting strong invariance. Thus, strong invariance was established for the EDS-s across time, allowing to the examination of change over time.
Hypothesis testing
The multigroup latent change score analyses found no significant moderation effect of gender. Between the models with the regression coefficients associated with negative and positive urgency equated vs. relaxed across boys and girls, there was no significant change in model fit (Δχ2 = 3.785, Δdf = 2, p=0.15). The constrained model (RMSEA = 0.062, 90% CI [0.059, 0.065], CFI = 0.89) revealed that negative urgency (b= -0.27, p=0.02) was significantly associated with change in emotion dysregulation, while the relationship with positive urgency was not significant (b=0.22, p=0.06; see Figure 1). There was also no significant change in model fit when only negative or positive urgency had their coefficients constrained to be equal, although it did trend towards significance (positive urgency coefficients constrained model to unconstrained model: Δχ2 = 3.219, Δdf = 1, p=0.07; negative urgency coefficients constrained model to unconstrained model: Δχ2 = 3.070, Δdf = 1, p=0.08).
Discussion
This study was the first to examine a temporal, predictive relationship between urgency and emotion dysregulation change. Results indicated that baseline negative, but not positive, urgency predicted change in emotion dysregulation across a 9-week period among our sample of 9th grade adolescents. Girls had higher emotion dysregulation scores than boys at both timepoints; however, there was not a main effect of gender in either model, and gender did not significantly moderate the relationship between urgency and emotion dysregulation change.
The negative, significant relationship between baseline negative urgency and change in emotion dysregulation extends previous cross-sectional relationships between negative urgency and emotion dysregulation (14, 16, 17, 42, 44, 46), suggesting that higher negative urgency is associated with increased emotion dysregulation over time. This study provides initial evidence of a temporal relationship, supporting the idea that negative urgency influences the development of emotion dysregulation over time, as suggested by previous theory (18, 64, 65). If this is true, negative urgency may impact how one learns to regulate their emotions through personality-environment translation effects and may serve as one mechanism for how negative urgency impacts risk [e.g., (18)].
The relationship between baseline positive urgency and change in emotion dysregulation was not significant, which is consistent with previous research that indicates that positive and negative urgency relate to some risky behaviors in different ways (15, 47, 85–87). This finding contradicts previous work that suggests that both negative and positive urgency relate to emotion dysregulation (e.g., 42, 44) and have similar risk patterns (11, 88, 89). The effect of positive urgency on emotion dysregulation change fell just short of significance, and was in the opposite direction than hypothesized and than the effect of negative urgency. This may mean that positive urgency has a unique, and as of yet unstudied and not understood, negative impact on emotion dysregulation. However, given the trend-like nature of this effect and the unexpected direction, this should be examined more fully before reaching this conclusion. The use of the EDS-s, which primarily includes items concerning negative emotional states, may have contributed to significant association of negative urgency and null effects of positive urgency in the current study. Future research regarding the relationship between emotion dysregulation and positive urgency may consider assessing emotion dysregulation with positive emotions, such as the DERS-positive (90). Alternatively, since both negative and positive urgency were placed into one model, the residual variance trend with positive urgency, after removing the effect of negative urgency, may be spurious, especially given the high intercorrelation between the two traits.
Although negative urgency had a significant association on emotion dysregulation change, the effect size was small (84) and the study period was brief. Although statistically significant, the small effect may not translate to clinically-significant effects. On the other hand, small effects can be important when they occur with minimal manipulation or when they impact a difficult-to-change outcome (91). Thus, although the effect in this study was small, the fact that it occurred over such a short period of time and without intervention suggests that this effect could be meaningful in broader prospective or interventional studies. A longer follow-up period could provide additional insight into the true impact of urgency on emotion dysregulation across the adolescent period. First, emotion dysregulation develops in early and middle adolescence (51, 52, 67), but the time over which measurable, natural change in emotion dysregulation takes place is less well understood. The brief nine-week period used in the current study may have resulted in smaller effects as there was less change in emotion dysregulation to predict. Second, we chose the direction from urgency to emotion dysregulation based on theory that personality develops temporally before emotion dysregulation, which suggests that urgency may be the precursor (51, 62–67). However, this does not rule out a feedback loop from emotion dysregulation back to changes in urgency, which could then further impact changes in emotion dysregulation over time. Alternatively, others conceptualize negative urgency as being part of emotion dysregulation (14, 48, 61). These additional models should be studied further in future work.
Girls had higher emotion dysregulation scores compared to boys. This finding contradicts prior work that suggests there are no gender differences in emotion dysregulation (92, 93), but supports other findings that girls experience more emotion dysregulation compared to boys (52, 53). This is thought to be due to adolescent boys being less aware of their emotional experience than girls (52, 53). There is extensive work establishing that boys have elevated levels of risk-taking compared to girls (50). For example, adolescent boys are more likely to use drugs (94) and to gamble (95) than adolescent girls. These higher levels of negative urgency and emotion dysregulation in girls found in the present study could lead to higher risk for girls in other domains, such as anxiety and depression (49, 96).
Findings did not support the hypothesis that gender would moderate the relationship between urgency and emotion dysregulation, suggesting that negative urgency relates to emotion dysregulation in the same way across boys and girls. It is unlikely that the null result in the current study was driven by statistical concerns because the large sample allowed for adequate power to test for a small effect and because there was an equal proportion of boys and girls in the sample. However, and importantly, there was a significant relationship between negative urgency and gender, which could mask interaction effects.
The long-term goal of this line of research is to determine how to reduce risk-taking in adolescents. Given the high rate of risk-taking and emotional lability among adolescents (5), this goal addresses an important intervention endpoint. Negative and positive urgency may not be directly intervenable and may even impede treatment response (97–100). Emotion dysregulation could be targeted as a modifiable risk factor (45) to reduce the impact of negative urgency on emotion dysregulation development. One study has sought to do this: Weiss et al. (17) found success in reducing both emotion dysregulation and urgency through an emotion modulation skills training. This study, along with the current findings, suggest that future research should test whether or not existing effective emotion regulation treatments [see (101)] can also successfully reduce urgency and its impact of risk-taking. A more immediate and practical application of the current study is that clinicians may want to measure negative urgency and emotion dysregulation constructs in youth to better understand why, and under what conditions, youth engage in risk-taking. Both the UPPS-PC and the EDS-s appear to be adequate measures of these constructs in youth that are freely available and require very little time to implement, thus maximizing the benefits and minimizing the costs of additional assessments.
This study is not without limitations. First, we relied on self-report measures, which are limited by how aware, open, and willing participants were to disclose. Emotional awareness is less developed in adolescence (52), which could lead to under-reporting of both urgency and emotion dysregulation. Under-reporting could have reduced the effect size between these constructs detected in the current study. Using caregiver and/or teacher reports and behavioral measures, such as respiratory sinus arrhythmia (33), would provide complementary and potentially more robust relationship effects. Second, this sample was primarily composed of cisgender youth, which may limit generalizability to other gender identities. Third, strong measurement invariance was not fully supported for negative urgency and the EDS-s, suggesting that although comparisons can be made comparing strengths of relationships across boys and girls, boys and girls show mean level differences in these traits and comparisons should only be made with this in mind. Fourth, there could be a third variable responsible for the changes seen in emotion dysregulation across time, such as neuroticism or negative affectivity, which was not examined in the current study. One study found that neuroticism is typically higher in adolescent females than males starting around age 14 (102). Fifth, although participants in this study likely had a wide range of risk behavior engagement, this work should be replicated in clinical samples to ensure generalizability to high-risk adolescents.
In conclusion, this study is the first to establish a predictive temporal relationship between negative urgency and increased emotion dysregulation in adolescents, albeit in a brief timeframe. This work extends previous cross-sectional research and suggests the viability of further prospective work examining this relationship over a longer period of time, incorporating a measurement of risk-taking as the endpoint outcome. Positive urgency may relate to emotion dysregulation differently and should be studied further. Understanding how these constructs are related, and in turn, relate to the development of risky behaviors in adolescents, paves the way for the design and testing of interventions to reduce the impact of negative urgency for adolescent risk-taking.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Identifiable data on participants under the age of 18. Requests to access these datasets should be directed to Tamika Zapolski, dHphcG9sc2tAaXUuZWR1.
Ethics statement
The studies involving humans were approved by Indiana University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because of the use of a passive parental opt-out and active participant assent process.
Author contributions
LF-F: Writing – review & editing, Writing – original draft, Investigation, Formal analysis, Conceptualization. MW: Writing – review & editing, Project administration, Investigation, Data curation. WW: Formal analysis, Writing – review & editing. MC: Writing – review & editing, Writing – original draft, Supervision, Conceptualization. TZ: Writing – review & editing, Supervision, Resources, Methodology, Investigation, Funding acquisition, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by an IUPUI Diversity Fellowship awarded to LF-F, a National Science Foundation Graduate Research Fellowship to LF-F, internal funding by Indiana University via the Addictions Grand Challenge program, and NIH award K01DA043654 (PI: Zapolski).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Arnett J. Reckless behavior in adolescence: A developmental perspective. Dev Rev. (1992) 12:339–73. doi: 10.1016/0273-2297(92)90013-R
2. Eaton DK, Kann L, Kinchen S, Shanklin S, Flint K, Hawkins J, et al. Youth risk behavior surveillance–United State. MMWR Surveillance Summaries. (2012) 61:1–162.
3. Gardner M, Steinberg L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: an experimental study. Dev Psychol. (2005) 41:625–35. doi: 10.1037/0012-1649.41.4.625
4. Steinberg L. A social neuroscience perspective on adolescent risk-taking. Dev Rev. (2008) 28:78–106. doi: 10.1016/j.dr.2007.08.002
5. Steinberg L. Risk taking in adolescence: what changes, and why? Ann New York Acad Sci. (2004) 1021:51–8. doi: 10.1196/annals.1308.005
6. Biolcati R, Mancini G, Trombini E. Proneness to boredom and risk behaviors during adolescents’ Free time. Psychol Rep. (2018) 121:303–23. doi: 10.1177/0033294117724447
7. Duell N, Steinberg L, Icenogle G, Chein J, Chaudhary N, Di Giunta L, et al. Age patterns in risk taking across the world. J Youth Adolescence. (2018) 47:1052–72. doi: 10.1007/s10964-017-0752-y
8. Jones CM, Clayton HB, Deputy NP, Roehler DR, Ko JY, Esser MB, et al. Prescription opioid misuse and use of alcohol and other substances among high school students – Youth Risk Behavior Survey, United States 2019. Morbidity Mortality Weekly Rep MMWR. (2020) Suppl 69:38–46. doi: 10.15585/mmwr.su6901a5
9. Lowry R, Kann L, Collins JL, Kolbe LJ. The effect of socioeconomic status on chronic disease risk behaviors among US adolescents. Jama. (1996) 276:792–7. doi: 10.1001/jama.1996.03540100036025
10. Yellman MA, Bryan L, Sauber-Schatz EK, Brener N. Transportation risk behaviors among high school students – youth risk behavior survey, United States 2019. MMWR. (2020) Supplements 60:77–83. doi: 10.15585/mmwr.su6901a9
11. Berg JM, Latzman RD, Bliwise NG, Lilienfeld SO. Parsing the heterogeneity of impulsivity: A meta-analytic review of the behavioral implications of the UPPS for psychopathology. psychol Assess. (2015) 27:1129. doi: 10.1037/pas0000111
12. Cyders MA, Coskunpinar A, VanderVeen JD. “Urgency: A common transdiagnostic endophenotype for maladaptive risk taking”. In Zeigler-Hill V, Marcus DK editors. The dark side of personality: Science and practice in social, personality, and clinical psychology. American Psychological Association (2016). pp. 157–88. doi: 10.1037/14854-009
13. McLaughlin KA, Hatzenbuehler ML, Mennin DS, Nolen-Hoeksema S. Emotion dysregulation and adolescent psychopathology: A prospective study. Behav Res Ther. (2011) 49:544–54. doi: 10.1016/j.brat.2011.06.003
14. Anestis MD, Kleiman EM, Lavender JM, Tull MT, Gratz KL. The pursuit of death versus escape from negative affect: An examination of the nature of the relationship between emotion dysregulation and both suicidal behavior and non-suicidal self-injury. Compr Psychiatry. (2014) 55:1820–30. doi: 10.1016/j.comppsych.2014.07.007
15. Espeleta HC, Brett EI, Ridings LE, Leavens ELS, Mullins LL. Childhood adversity and adult health-risk behaviors: Examining the roles of emotion dysregulation and urgency. Child Abuse Negl. (2018) 82:92–101. doi: 10.1016/j.chiabu.2018.05.027
16. Jebraeili H, Moradi A, Habibi M. Investigating the role of dimensions of UPPS-P model of impulsivity and age increasing in men’s emotion dysregulation. J Fundamentals Ment Health. (2018) 20:228–35. doi: 10.22038/JFMH.2018.10737
17. Weiss NH, Tull MT, Davis LT, Searcy J, Williams I, Gratz KL. A preliminary experimental investigation of emotion dysregulation and impulsivity in risky behaviours. Behav Change. (2015) 32:127–42. doi: 10.1017/bec.2015.5
18. Cyders MA, Smith GT. Emotion-based dispositions to rash action: positive and negative urgency. psychol Bulletin. (2008) 134:807–28. doi: 10.1037/a0013341
19. Auerbach RP, Stewart JG, Johnson SL. Impulsivity and suicidality in adolescent inpatients. J Abnormal Child Psychol. (2017) 45:91–103. doi: 10.1007/s10802-016-0146-8
20. Bos J, Hayden MJ, Lum JAG, Staiger PK. UPPS-P impulsive personality traits and adolescent cigarette smoking: A meta-analysis. Drug Alcohol Depend. (2019) 197:335–43. doi: 10.1016/j.drugalcdep.2019.01.018
21. Burris JL, Riley E, Puleo GE, Smith GT. A longitudinal study of the reciprocal relationship between ever smoking and urgency in early adolescence. Drug Alcohol Depend. (2017) 178:519–26. doi: 10.1016/j.drugalcdep.2017.06.007
22. Claes L, Muehlenkamp J. The relationship between the UPPS-P impulsivity dimensions and nonsuicidal self-injury characteristics in male and female high-school students. Psychiatry J. (2013) 2013:654847. doi: 10.1155/2013/654847
23. Davis HA, Smith GT. An integrative model of risk for high school disordered eating. J Abnormal Psychol. (2018) 127:559–70. doi: 10.1037/abn0000365
24. Davis HA, Ortiz AML, Smith GT. Transactions between early binge eating and personality predict transdiagnostic risk. Eur Eating Disord Rev. (2019) 27:614–27. doi: 10.1002/erv.2682
25. Lopez-Vergara HI, Spillane NS, Merrill JE, Jackson KM. Developmental trends in alcohol use initiation and escalation from early to middle adolescence: Prediction by urgency and trait affect. Psychol Addictive Behav. (2016) 30:578–87. doi: 10.1037/adb0000173
26. Pang RD, Farrahi L, Glazier S, Sussman S, Leventhal AM. Depressive symptoms, negative urgency and substance use initiation in adolescents. Drug Alcohol Depend. (2014) 144:225–30. doi: 10.1016/j.drugalcdep.2014.09.771
27. Phillips WJ, Hine DW, Marks ADG. Individual differences in trait urgency moderate the role of the affect heuristic in adolescent binge drinking. Pers Individ Dif. (2009) 47:829–34. doi: 10.1016/j.paid.2009.06.028
28. Rawlings J, Shevlin M, Corcoran R, Morriss R, Taylor PJ. Out of the blue: Untangling the association between impulsivity and planning in self-harm. J Affect Disord. (2015) 184:29–35. doi: 10.1016/j.jad.2015.05.042
29. VanderVeen JD, Plawecki MH, Millward JB, Hays J, Kareken DA, O’Connor S, et al. Negative urgency, mood induction, and alcohol seeking behaviors. Drug Alcohol Depend. (2016) 165:151–8. doi: 10.1016/j.drugalcdep.2016.05.026
30. Cole PM, Michel MK, Teti LOD. The development of emotion regulation and dysregulation: A clinical perspective. Monogr Soc Res Child Dev. (1994) 59:73–100. doi: 10.2307/1166139
31. Cole PM, Hall SE. Emotion dysregulation as a risk factor for psychopathology. In: Beauchaine TP, Hinshaw SP, editors. Child and Adolescent Psychopathology. Hoboken, New Jersey: John Wiley & Sons Inc (2008). p. 265–98.
32. Bradley B, DeFife JA, Guarnaccia C, Phifer J, Fani N, Ressler KJ, et al. Emotion dysregulation and negative affect: association with psychiatric symptoms. J Clin Psychiatry. (2011) 72:685–91. doi: 10.4088/JCP.10m06409blu
33. Beauchaine TP, Gatzke-Kopp L, Mead HK. Polyvagal Theory and developmental psychopathology: emotion dysregulation and conduct problems from preschool to adolescence. Biol Psychol. (2007) 74:174–84. doi: 10.1016/j.biopsycho.2005.08.008
34. Althoff RR, Verhulst FC, Rettew DC, Hudziak JJ, van der Ende J. Adult outcomes of childhood dysregulation: a 14-year follow-up study. J Am Acad Child Adolesc Psychiatry. (2010) 49:1105–16. doi: 10.1016/j.jaac.2010.08.006
35. Bohnert AM, Crnic KA, Lim KG. Emotional competence and aggressive behavior in school-age children. J Abnormal Child Psychol. (2003) 31:79–91. doi: 10.1023/A:1021725400321
36. Bonn-Miller MO, Vujanovic AA, Zvolensky MJ. Emotional dysregulation: association with coping-oriented marijuana use motives among current marijuana users. Subst Use Misuse. (2008) 43:1653–65. doi: 10.1080/10826080802241292
37. Gratz KL, Roemer L. The relationship between emotion dysregulation and deliberate self-harm among female undergraduate students at an urban commuter university. Cogn Behav Ther. (2008) 37:14–25. doi: 10.1080/16506070701819524
38. Gratz KL, Tull MT. The relationship between emotion dysregulation and deliberate self-harm among inpatients with substance use disorders. Cogn Ther Res. (2010) 34:544–53. doi: 10.1007/s10608-009-9268-4
39. Messman-Moore TL, Walsh KL, DiLillo D. Emotion dysregulation and risky sexual behavior in revictimization. Child Abuse Negl. (2010) 34:967–76. doi: 10.1016/j.chiabu.2010.06.004
40. Peh CX, Shahwan S, Fauziana R, Mahesh MV, Sambasivam R, Zhang Y, et al. Emotion dysregulation as a mechanism linking child maltreatment exposure and self-harm behaviors in adolescents. Child Abuse Negl. (2017) 67:383–90. doi: 10.1016/j.chiabu.2017.03.013
41. Dir AL, Banks DE, Zapolski TC, McIntyre E, Hulvershorn LA. Negative urgency and emotion regulation predict positive smoking expectancies in non-smoking youth. Addictive Behav. (2016) 58:47–52. doi: 10.1016/j.addbeh.2016.02.014
42. Fossati A, Gratz KL, Maffei C, Borroni S. Impulsivity dimensions, emotion dysregulation, and borderline personality disorder features among Italian nonclinical adolescents. Borderline Pers Disord Emotion Dysregulation. (2014) 1:5. doi: 10.1186/2051-6673-1-5
43. Hasking P, Claes L. Transdiagnostic mechanisms involved in nonsuicidal self-injury, risky drinking and disordered eating: Impulsivity, emotion regulation and alexithymia. J Am Coll Health. (2020) 68:603–9. doi: 10.1080/07448481.2019.1583661
44. Lavender JM, King WC, Kalarchian MA, Devlin MJ, Hinerman A, Gunstad J, et al. Examining emotion-, personality-, and reward-related dispositional tendencies in relation to eating pathology and weight change over seven years in the Longitudinal Assessment of Bariatric Surgery (LABS) study. J Psychiatr Res. (2020) 120:124–30. doi: 10.1016/j.jpsychires.2019.10.014
45. MacPherson HA, Cheavens JS, Fristad MA. Dialectical behavior therapy for adolescents: theory, treatment adaptations, and empirical outcomes. Clinal Child Family Psychol Rev. (2013) 16:59–80. doi: 10.1007/s10567-012-0126-7
46. Pivarunas B, Conner BT. Impulsivity and emotion dysregulation as predictors of food addiction. Eating Behav. (2015) 19:9–14. doi: 10.1016/j.eatbeh.2015.06.007
47. Reff J, Baschnagel JS. The role of affective urgency and emotion regulation in vaping susceptibility. Addictive Behav Rep. (2021) 14:100355. doi: 10.1016/j.abrep.2021.100355
48. Jara-Rizzo MF, Navas JF, Catena A, Perales JC. Types of emotion regulation and their associations with gambling: cross-sectional study with disordered and non-problem Ecuadorian gamblers. J Gambling Stud. (2019) 35:997–1013. doi: 10.1007/s10899-019-09868-7
49. d’Acremont M, Van der Linden M. How is impulsivity related to depression in adolescence? Evidence from a French validation of the cognitive emotion regulation questionnaire. J Adolescence. (2007) 30:271–82. doi: 10.1016/j.adolescence.2006.02.007
50. Ajisuksmo CR. Why some adolescents engage in risk-taking behavior. Int J Educ Psychol. (2021) 10:143–71. doi: 10.17583/ijep.2021.4258
51. Gullone E, Hughes EK, King NJ, Tonge B. The normative development of emotion regulation strategy use in children and adolescents: a 2-year follow-up study. J Child Psychol Psychiatry. (2010) 51:567–74. doi: 10.1111/j.1469-7610.2009.02183.x
52. Bender PK, Reinholdt-Dunne ML, Esbjørn BH, Pons F. Emotion dysregulation and anxiety in children and adolescents: Gender differences. Pers Individ Dif. (2012) 53:284–8. doi: 10.1016/j.paid.2012.03.027
53. Zafar H, Debowska A, Boduszek D. Emotion regulation difficulties and psychopathology among Pakistani adolescents. Clin Child Psychol Psychiatry. (2021) 26:121–39. doi: 10.1177/1359104520969765
54. Cyders MA. Impulsivity and the sexes: Measurement and structural invariance of the UPPS-P Impulsive Behavior Scale. Assessment. (2013) 20:86–97. doi: 10.1177/1073191111428762
55. d’Acremont M, Van der Linden M. Adolescent impulsivity: Findings from a community sample. J Youth Adolescence. (2005) 34:427–35. doi: 10.1007/s10964-005-7260-1
56. Santano-Mogena E, Franco-Antonio C, Cordovilla-Guardia S. Gender differences in susceptibility to smoking among high school students. J Advanced Nurs. (2023) 79:1912–25. doi: 10.1111/jan.15382
57. Kotbagi G, Morvan Y, Romo L, Kern L. Which dimensions of impulsivity are related to problematic practice of physical exercise? J Behav Addict. (2017) 6:221–8. doi: 10.1556/2006.6.2017.024
58. Settles RE, Fischer S, Cyders MA, Combs JL, Gunn RL, Smith GT. Negative urgency: a personality predictor of externalizing behavior characterized by neuroticism, low conscientiousness, and disagreeableness. J Abnormal Psychol. (2012) 121:160–72. doi: 10.1037/a0024948
59. Hahn AM, Hahn CK, Simons RM, Simons JS. History of rape moderates the pathways from emotion dysregulation to alcohol and risky sex outcomes among college women. psychol Trauma: Theory Res Practice Policy. (2022) 14:786–94. doi: 10.1037/tra0001101
60. Torrado M, Bacelar-Nicolau L, Skryabin V, Teixeira M, Eusébio S, Ouakinin S. Emotional dysregulation features and problem gambling in university students: a pilot study. J Addictive Dis. (2020) 38:550–66. doi: 10.1080/10550887.2020.1800889
61. Velotti P, Garofalo C, Petrocchi C, Cavallo F, Popolo R, Dimaggio G. Alexithymia, emotion dysregulation, impulsivity and aggression: A multiple mediation model. Psychiatry Res. (2016) 237:296–303. doi: 10.1016/j.psychres.2016.01.025
62. Caspi A, Roberts BW, Shiner RL. Personality development: stability and change. Annu Rev Psychol. (2005) 56:453–84. doi: 10.1146/annurev.psych.55.090902.141913
63. Costa PT, McCrae RR. A theoretical context for adult temperament. In: Temperament in context. Mahwah, New Jersey: Lawrence Erlbaum Associates Publishers (2001). p. 1–21.
64. McCrae RR, Costa PT Jr., Ostendorf F, Angleitner A, Hrebícková M, Avia MD, et al. Nature over nurture: temperament, personality, and life span development. J Pers Soc Psychol. (2000) 78:173–86. doi: 10.1037//0022-3514.78.1.173
65. Shiner R, Caspi A. Personality differences in childhood and adolescence: measurement, development, and consequences. J Child Psychol Psychiatry. (2003) 44:2–32. doi: 10.1111/1469-7610.00101
66. Crowell SE, Puzia ME, Yaptangco M. The ontogeny of chronic distress: emotion dysregulation across the life span and its implications for psychological and physical health. Curr Opin Psychol. (2015) 3:91–9. doi: 10.1016/j.copsyc.2015.03.023
67. Zimmermann P, Iwanski A. Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. Int J Behav Dev. (2014) 38:182–94. doi: 10.1177/0165025413515405
68. Zapolski T, Whitener M, Khazvand S, Crichlow Q, Revilla R, Salgado EF, et al. Implementation of a brief dialectical behavioral therapy skills group in high schools for at-risk youth: protocol for a mixed methods study. JMIR Res Protoc. (2022) 11:e32490. doi: 10.2196/32490
69. Powers A, Stevens J, Fani N, Bradley B. Construct validity of a short, self-report instrument assessing emotional dysregulation. Psychiatry Res. (2015) 225:85–92. doi: 10.1016/j.psychres.2014.10.020
70. Zapolski TCB, Stairs AM, Settles RF, Combs JL, Smith GT. The measurement of dispositions to rash action in children. Assessment. (2010) 46:220–31. doi: 10.1177/1073191109351372
71. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2023). Available at: https://www.R-project.org/.
72. Little RJA. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. (1988) 83:1198–202. doi: 10.1080/01621459.1988.10478722
73. Wu W, Gu F, Fukui S. Combining proration and full information maximum likelihood in handling missing data in Likert scale items: A hybrid approach. Behav Res Methods. (2022) 54:922–40. doi: 10.3758/s13428-021-01671-w
74. Hair J, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. 7th ed. Upper Saddle River, New Jersey: Pearson Educational International (2010).
75. Byrne BM. Structural equation modeling with AMOS: Basic concepts, applications, and programming. New York: Routledge (2010).
76. Revelle W. psych: procedures for psychological, psychometric, and personality research. Northwestern University, Evanston, Illinois: R package version 2.3.6 (2023). Available at: https://CRAN.R-project.org/package=psych.
77. Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Software. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
78. van de Schoot R, Lugtig P, Hox J. A checklist for testing measurement invariance. Eur J Dev Psychol. (2012) 9:486–92. doi: 10.1080/17405629.2012.686740
79. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equation Modeling: A Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
80. Fischer R, Karl JA. A primer to (cross-cultural) multi-group invariance testing possibilities in R. Front Psychol. (2019) 10. doi: 10.3389/fpsyg.2019.01507
81. Kim E, Wang Y, Liu S. The impact of measurement noninvariance on latent change score modeling: a Monte Carlo simulation study. Struct Equation Modeling: A Multidiscip J. (2020) 27:918–30. doi: 10.1080/10705511.2020.1711759
82. Castro-Schilo L, Grimm KJ. Using residualized change versus difference scores for longitudinal research. J Soc Pers Relat. (2018) 35:32–58. doi: 10.1177/0265407517718387
83. Ghisletta P, McArdle JJ. Latent curve models and latent change score models estimated in R. Struct Equation Modeling: A Multidiscip J. (2012) 19:651–82. doi: 10.1080/10705511.2012.713275
84. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers (1988).
85. Cyders MA, Flory K, Rainer S, Smith GT. The role of personality dispositions to risky behavior in predicting first-year college drinking. Addiction. (2009) 104:193–202. doi: 10.1111/j.1360-0443.2008.02434.x
86. Fischer S, Smith GT. Binge eating, problem drinking, and pathological gambling: Linking behavior to shared traits and social learning. Pers Individ Dif. (2008) 44:789–800. doi: 10.1016/j.paid.2007.10.008
87. Zapolski TC, Cyders MA, Smith GT. Positive urgency predicts illegal drug use and risky sexual behavior. Psychol Addictive Behav. (2009) 23:348. doi: 10.1037/a0014684
88. Berg JM. The heterogeneous roles of the UPPS-P impulsivity pathways across features of psychopathology. Emory University, Atlanta (GA (2016).
89. Sperry SH, Lynam DR, Kwapil TR. The convergence and divergence of impulsivity facets in daily life. J Pers. (2018) 86:841–52. doi: 10.1111/jopy.12359
90. Weiss NH, Gratz KL, Lavender JM. Factor structure and initial validation of a multidimensional measure of difficulties in the regulation of positive emotions: the DERS-positive. Behav modification. (2015) 39:431–53. doi: 10.1177/0145445514566504
91. Prentice DA, Miller DT. When small effects are impressive. psychol Bull. (1992) 112:160–4. doi: 10.1037/0033-2909.112.1.160
92. Mancinelli E, Sharka O, Lai T, Sgaravatti E, Salcuni S. Self-injury and Smartphone Addiction: Age and gender differences in a community sample of adolescents presenting self-injurious behavior. Health Psychol Open. (2021) 8:20551029211038811. doi: 10.1177/20551029211038811
93. Weinberg A, Klonsky ED. Measurement of emotion dysregulation in adolescents. Psychol Assess. (2009) 21(4):616–21. doi: 10.1037/a0016669
94. Cotto JH, Davis E, Dowling GJ, Elcano JC, Staton AB, Weiss SR. Gender effects on drug use, abuse, and dependence: a special analysis of results from the National Survey on Drug Use and Health. Gender Med. (2010) 7:402–13. doi: 10.1016/j.genm.2010.09.004
95. Stefanovics EA, Gueorguieva R, Zhai ZW, Potenza MN. Gambling participation among Connecticut adolescents from 2007 to 2019: Potential risk and protective factors. J Behav Addict. (2023) 12:490–9. doi: 10.1556/2006.2023.00027
96. Marmorstein NR. Associations between dispositions to rash action and internalizing and externalizing symptoms in children. J Clin Child Adolesc Psychol. (2013) 42(1):131–8. doi: 10.1080/15374416.2012.734021
98. Hershberger AR, Um M, Cyders MA. The relationship between the UPPS-P impulsive personality traits and substance use psychotherapy outcomes: A meta-analysis. Drug Alcohol Depend. (2017) 178:408–16. doi: 10.1016/j.drugalcdep.2017.05.032
99. Peckham AD, Forgeard M, Hsu KJ, Beard C, Björgvinsson T. Turning the UPPS down: Urgency predicts treatment outcome in a partial hospitalization program. Compr Psychiatry. (2019) 88:70–6. doi: 10.1016/j.comppsych.2018.11.005
100. Whitt ZT, Bernstein M, Spillane N, Stein LAR, Suffoletto B, Neighbors C, et al. Positive urgency worsens the impact of normative feedback on 21st birthday drinking. Drug Alcohol Depend. (2019) 204:107559. doi: 10.1016/j.drugalcdep.2019.107559
101. Waxmonsky JG, Baweja R, Bansal PS, Waschbusch DA. A review of the evidence base for psychosocial interventions for the treatment of emotion dysregulation in children and adolescents. Child Adolesc Psychiatr Clinics North America. (2021) 30:573–94. doi: 10.1016/j.chc.2021.04.008
Keywords: negative urgency, positive urgency, emotion dysregulation, adolescents, risk-taking
Citation: Fisher-Fox L, Whitener M, Wu W, Cyders MA and Zapolski TCB (2024) Urgency as a predictor of change in emotion dysregulation in adolescents. Front. Psychiatry 15:1451192. doi: 10.3389/fpsyt.2024.1451192
Received: 18 June 2024; Accepted: 02 September 2024;
Published: 03 October 2024.
Edited by:
Henry W. Chase, University of Pittsburgh, United StatesReviewed by:
Phillip Karl Wood, University of Missouri, United StatesAshok Kumar Paudel, Pokhara University, Nepal
Şafak Eray Çamli, Bursa Uludağ University, Türkiye
Casey R. Guillot, University of North Texas, United States
Copyright © 2024 Fisher-Fox, Whitener, Wu, Cyders and Zapolski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lindsey Fisher-Fox, bGluZmlzaGVAaXUuZWR1