 Marta Brás1,2,3*
Marta Brás1,2,3* Cátia Martins1,2,3
Cátia Martins1,2,3 Cristina Nunes1,2,3
Cristina Nunes1,2,3 Saul Neves Jesus1,3,4
Saul Neves Jesus1,3,4 Ana Rita Madeira1Cláudia Carmo1,2,3†
Ana Rita Madeira1Cláudia Carmo1,2,3†- 1Psychology and Education Sciences Department, University of Algarve, Faro, Portugal
- 2Psychology Research Centre (CIP), Lisboa, Portugal
- 3University Research Center in Psychology (CUIP), Faro, Portugal
- 4Research Centre for Tourism, Sustainability and Well-being (CinTurs), Faro, Portugal
Introduction: Suicide is a public health problem worldwide, being the fourth leading cause of death in young adult population (15-29 years). Therefore, it is important to identify its risk and protective factors, and how they interact to develop more effective interventions. The present study aims to analyze the relation between depressive symptoms, hopelessness (risk factors) with reasons for living (protective factors) and suicidal ideation in young adults with and without previous suicide attempts.
Methods: A sample of 845 Portuguese young adults answered an online form which assessed suicidal ideation, hopelessness, depressive symptoms, and reasons for living. Mean comparisons, correlations, and moderated mediation analysis were computed.
Results: Individuals with a history of suicide attempt showed higher mean levels in risk factors, compared to individuals without suicide attempt. When no history of suicide attempt was present, ideation was positively and significantly correlated to depression and hopelessness, and negatively correlated to the reasons for living. Higher levels of depressive symptomatology predict lower levels of reasons for living. Mediation and moderation relations were assessed in a model and the history of suicide attempts showed a relevant role.
Conclusions: The evidence found in this study reinforce that reasons for living may play a preponderant role in suicidal ideation, that is as a negative mediator and therefore it can act as a protective factor.
1 Introduction
Suicide is a public health problem worldwide, being the third leading cause of death in young adult population (aged 15-29 years) (1). In Portugal it is also one of the main causes of death among young adults, with a mortality rate of 9 per 100,000 inhabitants in 2020 (2).
Bagge et al. (3) report that approximately 20% of college students have considered committing suicide and more than 7% have attempted suicide. These rates are most likely underestimated because suicides are reported as other causes of death, such as traffic accidents (4–6).
Regarding the pandemic situation, several researchers identified a rise in loneliness and isolation in these age groups, increasing the likelihood of a scenario of suicidal ideation or suicidal behaviors in which to mobilize the necessary help can be difficult (7, 8). Depressive and anxious symptomatology have also increased with the passing of the pandemic, presenting a higher incidence in young adults, when compared to other age groups, which also can enhance the risk of suicide (7).
Suicide is a multifaceted and complex phenomenon that corresponds, most of the time, to the end of a process that range in a continuum from suicidal ideation to the completed suicide (9, 10). The General Health Coordination [GHC; (9)], in the National Suicide Prevention Plan, defines suicidal ideation as thoughts that aim to end one’s life, which may or may not be proceeded by a suicide attempt. Suicide attempt is understood as any act carried out by the self with the purpose of death, but which, for various reasons, results in the failure of its execution. In this process, self-injurious behaviors may coexist, which consist of behavioral acts against oneself, but without the intention to cause death (9).
Initiating the suicidal process seems to represent an increased risk for future suicide, especially if suicide attempts occur. It is estimated that 15% of individuals who commit one or more suicide attempts will perform the consummated suicide (11), and this being considered the main predictor (11, 12).
Given the importance of preventing these behaviors, research has been devoted to explore risk factors associated with suicide and more recently with protective factors; however, the need for robustness in this research topic is still imperative (13–15). Franklin et al. (16) in a meta-analysis conducted about risk factors for suicidal behaviors and thoughts reported a discrepancy between studies on risk factors, about more than three thousand studies, and studies on protective factors, less than five hundred studies. In addition, the observed decrease falls short of what is expected by 2030 by the World Health Organization, as a plan of action and prevention in reducing suicide (1).
Given the discrepancy between the number of studies on risk and protective factors, the focus is currently on protective factors and their possible mediating roles. Understanding the risk factors that increase the risk for suicidal ideation, suicide attempt, and completed suicide may not be sufficient to minimize the risk of these behaviors (10, 17). There is consistent empirical evidence on the role of psychological risk factors, such as depressive symptomatology and hopelessness (18, 19), but the role of protective factors, such as reasons for living is not fully clarified, especially regarding the interaction with other risk factors. Reasons for living (RFL) consist of the beliefs that an individual holds about his or her own life and expectations that seem to mitigate suicidal ideation (13, 20).
Individuals who present hopelessness regarding the future and/or have depressive symptomatology may have difficulty in identifying, enumerating, or connecting their RFL, which may result in suicidal ideation and/or an increased likelihood of a suicide attempt (3, 21). Furthermore, individuals with suicidal ideation reveal low levels of RFL compared to those without such ideation, and the ones with suicidal ideation generally lack cognitive beliefs that support the idea that they have reasons not to consummate suicide (22). The presence of more severe depressive symptoms and hopelessness, marked by high levels of mental pain, has been identified as a risk factor for suicide (4).
Ren et al. (23) found that RFL in adolescents is negatively related to low self-esteem, perceived inability to escape from aversive situations, and suicidal ideation. The association between perceived inability to escape from aversive situations and suicidal ideation is moderated by RFL. This study thus suggests that RFL may weaken the relationship between risk factors for suicide and suicidal ideation.
The prevalence and increasing rates of suicidal behavior and ideation in college students remains significant and leads to the emergence for mental health professionals. Given the negative impact and often unalterable consequences that suicide can cause, it is essential to understand the reasons why young-adults consider life worth living (13).
Wang and colleagues (25) showed that severe depression has a mediating effect on the relationship between hopelessness and suicidal ideation, that is, hopelessness does not seem to be a direct cause of suicidal ideation, but if individuals with hopelessness are in depressive states, they are more likely to have more thoughts related to suicide. Hope provides a perception of control over one’s life, making it easier to find alternative solutions when faced with problematic situations. Additionally, because they have high levels of hopelessness, individuals at risk of suicide usually have difficulty solving problems (24). They also compared the levels of hopelessness in individuals with and without suicidal ideation and concluded that the former showed higher levels of hopelessness (25).
However, divergent results on the role of RFL in suicide emerge in the literature (17). In fact, several factors have been identified that, when interacting with each other, they can contribute to the development of suicidal behaviors. A history of prior suicide attempt, especially in the past 6 months, is such a factor, that it is considered more important than any psychiatric disorder (11, 12). Even so, Klonsky and May (10) refer the existence of contradictory results, with differences between clinical and non-clinical populations, but without statistically significant differences in RFL between individuals with suicidal ideation alone and with depressive symptomatology.
Since suicide attempts are considered the best predictor of future suicidal acts, it is important to clarify whether they have a differential effect on the relationship between other risk and protective factors for suicidal ideation. That is, if the relationship between depressive symptoms, reasons for living and suicidal ideation varies according to the existence of previous suicide attempts.
The present study aims to analyze the relation between depressive symptoms, hopelessness (risk factors for suicide) with reasons for living (protective factors) and suicidal ideation in young adults with and without previous suicide attempts (Figure 1).

Figure 1. Suicidal Ideation conceptual model to be tested.
2 Methods
2.1 Participants
The study was conducted with a national sample of 845 young adults, from different regions of Portugal and islands, where 189 were males (22.4%) and 656 females (77.6%). 33 participants (3.9%) had previously attempted suicide and 812 participants had not (96.1%). Age ranked from 18 to 30 years old (M = 21.79; DP = 2.87).
2.2 Instruments
2.2.1 Sociodemographic questionnaire
The sociodemographic and clinical information questionnaire was developed to gathered information regarding (a) personal information (age, gender, education level); (b) history of psychopathology; (c) history of suicidal behavior including previous suicide attempts; and (d) history of suicide attempts in family members or close ones.
2.2.2 Suicidal Ideation Questionnaire (SIQ)
The SIQ (26, 27) main objective is to assess the severity of suicidal thoughts in adolescents. It is composed of 30 items (e.g., “I thought about killing myself”), and each one can be punctuated from 0 (Never had this thought) to 6 (Almost every day). The final score can range from 0 to 180 points; and the higher the score, the more frequent are the suicidal thoughts. The Portuguese version of this questionnaire has good psychometrics values (α = .96) (26).
2.2.3 Beck Hopelessness Scale (BHS)
BHS (28, 29) is a 20 items-scale that assesses hopelessness or negative attitudes about future related events answered with single choice option, true or false (e.g., “I look forward to the future with hope and enthusiasm”; “My future seems dark to me”). The total score ranges from 0 to 20, and higher scores are associated with more negative attitudes toward the future (28). The Portuguese version was used, and the original study reveal good internal consistency (KR_20 = .90) (29).
2.2.4 Beck Depression Inventory – II (BDI-II)
BDI-II (30, 31) is a 21 items-inventory that assesses the severity of depressive symptoms. Each item is rated on a 4-point scale ranging from 0 to 3, with a maximum total score of 63 points (e.g., “I do not feel sad”). The higher the total score is, the severe the symptoms are (30). The Portuguese version of BDI-II has good internal reliability (α = .91), identical factorial structure to the original study and adequate convergent validity (31).
2.2.5 Reasons for Living Inventory for Young Adults (RFL-YA-II)
The inventory RFL-YA-II (6, 13, 32) has 28 items organized in four subscales: (1) Faith-Related Support (FRS; e.g., “I believe that I can find a solution to most problems because of my faith”); (2) Family Sources of Support (FSS; e.g., “I have a close relationship with my family”); (3) Perceived Personal Strength (PPS; e.g., “I feel satisfied with myself”); and (4) Peer Acceptance and Support (PAS; e.g., “believe that I can count on my friends when I have a problem”). Each item is answered from 1 (Not at all important) to 6 (Extremely important). The Cronbach’s alpha of the Portuguese version indicated values similar with the original study, suggesting good consistency (between.93 and.98) (6, 13, 32).
2.3 Data collection procedure
The data collection protocol was disseminated through an online form by several higher education institutions in Portugal. Participation was anonymous, confidential, and voluntary, without any counterpart and preceded by informed consent. To avoid more than one answer by the same participants to the survey, emails were collected. According to WHO information (1) regarding the age of young people at which the highest number of suicides occurs, inclusion criteria were age from 18 to 30 years and Portuguese nationality. Scientific and ethical approvals were sought from the Faculty of Human and Social Sciences of the University of Algarve.
2.4 Data analyses procedure
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 28.0 for Windows. Descriptive statistics (i.e., frequency, percentage, mean and standard deviation) were performed for the sociodemographic variables. Student’s t test for independent samples was used to compare individuals with and without a history of suicide attempt on the variables of interest: suicidal ideation, depressive symptoms, hopelessness, and reasons for living. After the confirming the assumptions of normality and homogeneity, results were interpreted regarding 5% significance level and Cohen’s d was used to analyze the magnitude of the differences (0.25 indicating a low effect, 0.50 a moderate effect, and 0.80 a high effect). Pearson’s correlation coefficient was computed to analyze the relationship between the variables of interest, and significance (5%), magnitude and sign were explored (33).
Lastly, moderated mediation analysis was carried out with model 58 of Hayes PROCESS macro for SPSS (34). In this model, suicidal ideation (total score) was entered as the outcome variable, depressive symptomatology as independent variable, and the reasons for living (total score) as mediator. History of suicidal attempt was included as the moderator on the dependent variables’ reasons for living and suicidal ideation. See Figure 1 for a representation of the conceptual and statistic model.
3 Results
The mean values of suicidal ideation, depressive symptomatology, hopelessness, and reasons for living were compared between individuals with and without a history of suicide attempt (Table 1).
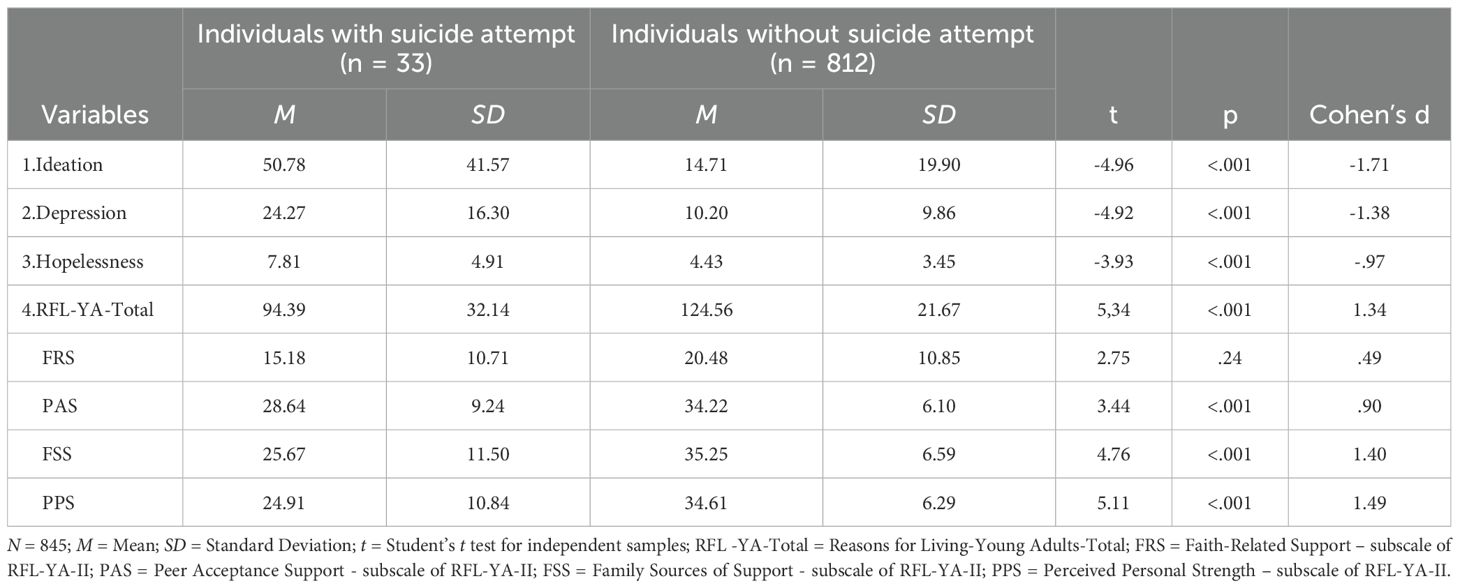
Table 1. Means, Standard Deviations, Cohen’s d and Student’s t-test of the variables according to the history of suicide attempts.
As shown in Table 1, results reveal significative differences in all dimensions, except in faith-related support (t = 2.75, p = .240, d = .49), but with a moderate effect. So, individuals with a history of suicide attempt show higher mean levels of suicidal ideation (MWith = 50.78, SDWith = 41.57; MWithout = 14.71, SDWithout = 19.90), depressive symptoms (MWith = 24.27, SDWith = 16.30; MWithout = 10.20, SDWithout = 9.86), hopelessness (MWith = 7.81, SDWith = 4.91; MWithout = 4.43, SDWithout = 3.45), and reasons for living (MWith = 94.39, SDWith = 32.14; MWithout = 124.56, SDWithout = 21.67) compared to individuals without suicide attempt, in the risk factors. Thus, those who have history of suicide attempt may be more susceptible to suicidal thoughts/behaviors, depressive symptoms, and hopelessness, which leads to a higher risk of suicide. In relation to reasons for living, individuals with history of suicide attempt present a lower mean value than individuals without history of suicide attempt. The group of people with a history of suicide attempt scored higher on the PAS (MWith = 28.64, SDWith = 9.24; MWithout = 34.22, SDWithout = 6.10) and FSS (MWith = 25.67, SDWith = 11.50) subscales of the RFL-YA-II, while individuals without a history of suicide attempt had higher levels on the FSS (MWithout = 35.25, SDWithout = 6.59) and PPS subscales (MWith = 24.91, SDWith = 10.84; MWithout = 34.61, SDWithout = 6.29).
As for the effect size, it is moderate only in the FRS (d = -.97), and the rest of the analyzed dimensions, its score is very large (d = .90 - 1.71).
For the individuals without history of suicide attempt (Table 2, left triangle), ideation was highly and positively correlated to depression (rwithout = .71, p <.001) and moderately to hopelessness (rwithout = .57, p <.001), and low and negative correlated to the total RFL (rwithout = -.33, p <.001), and respective sub-scales (rWhithoutFRS = -.16, p <.001; rFRS = -.16, p <.001). Depression was positively moderately correlated to ideation (rwithout = .64, p <.001) and hopelessness (rwithout = .67, p <.001), and negatively with RFL (rwithout = -.36, p <.001). Hopelessness displays low negative correlations to the total score of RFL (rwithout = -.35, p <.001), and its sub-scales (Range rwithout = -.21 - -.36, p <.001).

Table 2. Intercorrelations of study variables separated by history of suicidal attempt (with and without).
For the individuals with suicide attempt (Table 2, right triangle), ideation was highly positively correlated with depression (rwith = .64, p <.001) and moderately with hopelessness (rwith = .51, p <.001), and negatively with perceived personal strength subscale (rwith = -.49, p <.001). Depression was only significantly correlated with ideation, highly with hopelessness (rwith = .89, p <.001), and moderately negatively with perceived personal strength scale (rwith = -.60, p <.001). Hopelessness reveals a significantly correlation with ideation and depression, and a negative moderate correlation with perceived personal strength scale (rwith = -.65, p <.001).
Regarding the testing of the model (Figure 2), as shown in Table 3, higher levels of depressive symptomatology predict lower levels of reasons for living (b = -0.79, SE = 0.07, p = .001, CI = -.93, -.64). Previous suicide attempts did not moderate the association between depressive symptomatology and reasons for living, as the interaction was not significant (b = 0.13, SE = 0.24, p = .587, CI = -.34, -.59). Predictors explained 18.5% of reasons for living (R2=.19; F(3,84) = 63.41, p <.001).
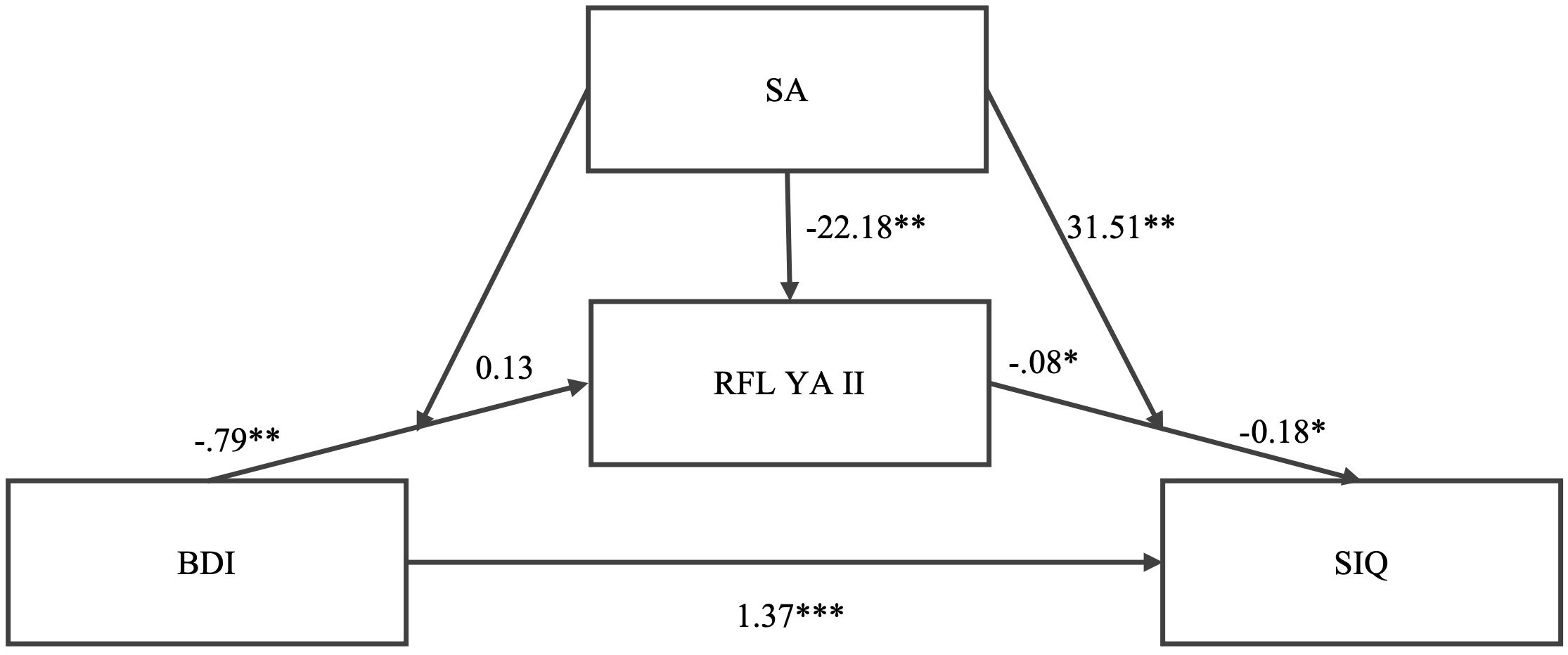
Figure 2. Tested model and no standardized coefficients.
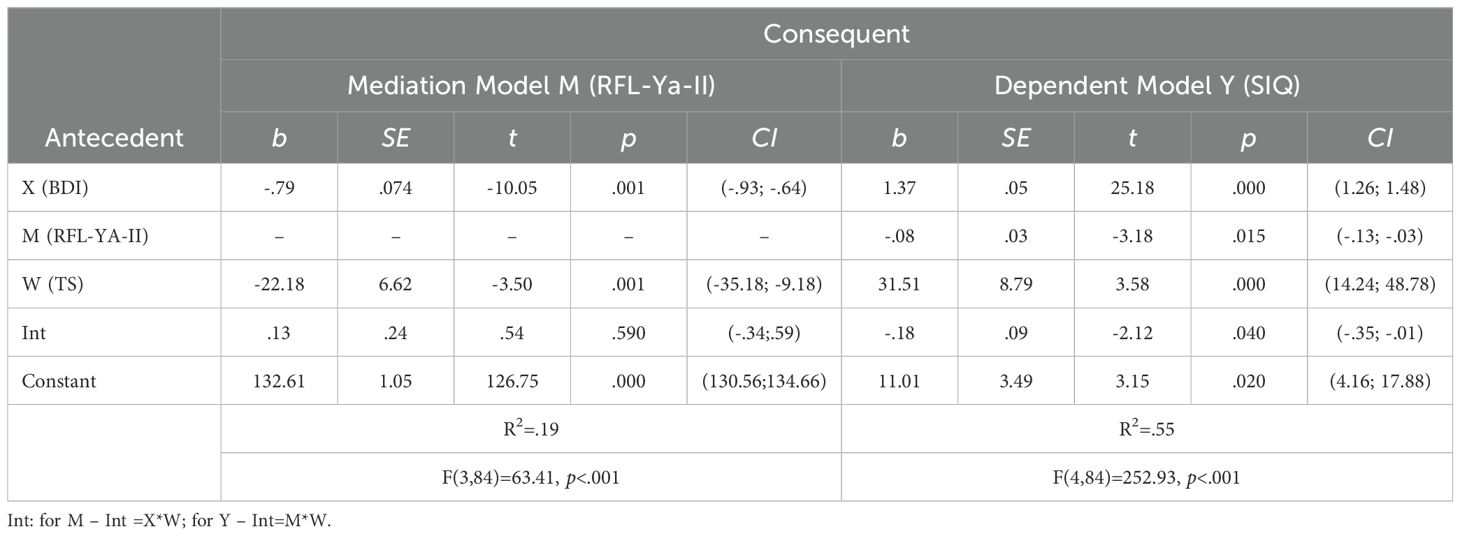
Table 3. Moderated mediation results for the link between depressive symptomatology and suicidal ideation. .
Higher levels of reasons for living predict lower levels of suicidal ideation (b = -0.08, SE = 0.03, p = .015, CI = -.13, -.03). History of suicide attempts moderates the association between reasons for living and suicidal ideation (b = -0.18, SE = 0.09, p = .035, CI = -.35, -.01), as the interaction is significant.
The moderated mediation model showed that the indirect effect was only significant for reasons for living and the interaction between reasons for living and suicide attempts (path b), but not for depression and reasons for living (path a); that is, the moderator has mediation influence on the dependent variable, but not of the independent variable on the mediator.
The moderated mediation effect is supported by the significant indirect effect of depressive symptomatology on suicidal ideation through reasons for living only in the group of individuals without a history of suicide attempts. The moderated mediation is significant when 95% CI did not encompass zero as occurs in the no suicide attempt group. The predictors explain 55% of the variance in suicidal ideation.
4 Discussion and conclusion
Suicide is usually the culmination of a continuous process that includes other phenomena, such as self-injurious behaviors, suicidal ideation, or suicide attempts (3, 9, 13).
Within the study of suicidal behaviors, empirical studies include both risk and protective factors in understanding suicidal behavior, highlighting the role of the protective factors (35). This study aimed to assess the relationship between protective factors (i.e., reasons for living) and risk factors (i.e., depressive symptoms and hopelessness) for suicidal ideation and verify whether reasons for living mediate the relationship between risk factors and suicidal ideation in young adults with and without a history of suicide attempt.
The comparison between individuals with history of suicide attempt, our results showed that there are significative differences between them. The group with suicide attempt reveals predominance of suicidal ideation, depressive symptoms and feelings of hopelessness, and lower scores of the reasons for living. These results are accordingly to previous studies (3, 4, 8, 36, 37). The Christensen et al. (37) study, for example, also with young adults, found that individuals with a history of suicide attempts and suicidal ideation reported significantly lower reasons for living than individuals with no history of suicide attempts, even if they had a history of suicidal ideation. Only in the sub-scale Faith-Related Support of the Reasons for Living measure no significative differences were reported, but a moderate effect size was described. Although faith is frequently pointed as a protective factor, we did not find it in the present study. This could be due to the sample size or to the fact that the sample is composed of young adults, maybe with less consolidate beliefs.
The correlations’ analysis corroborates the previous research (3–5) since the group with suicide attempt showed positive associations with the risk factors (e.g., depression, hopelessness) and negative with the protective factors (e.g., reasons for living). Regarding the group without suicide attempt, the results reveal positive and moderate to strong relations with the protective factors, which could act as a subjacent cause to mitigate potential risks toward suicide behaviors (4, 16). Moreover, the tested model also showed that the reasons for living can be a negative mediator of the relation between the depressive symptoms and suicidal ideation, that is, it can act as a protective factor. Another relevant relation tested in the model was that a history of suicide attempt can be a moderator between Reasons for Living and suicidal ideation, intensifying this connection.
These results indicate that coping and survival beliefs and responsibility with family may be considered protective factors for high-risk people (38). Individuals with high levels of reasons to live may exhibit high levels of fear of suicide, fear of social disapproval, moral objections to suicide, coping and survival beliefs, and responsibilities to family. These people may therefore have negative attitudes toward suicide and positive attitudes toward themselves and life. Thus, even individuals who have higher levels of reasons for living may believe that they cannot escape a particular situation, yet they may choose more constructive ways, rather than suicide, as solutions for coping with aversive situations (23). It is therefore understood that reasons for living are a relevant domain that should be addressed earlier in interventions to prevent and cope with suicidal ideation and to reduce the risk of suicide (6, 13, 20, 23, 35, 39).
The results obtained in Bruns and Letcher’s (35) research support the hypothesis that higher levels of protective factors may be associated with lower levels of suicide risk. The study of Shi et al. (36) also highlights the role of reasons for living as protective factors, having simultaneously assessed depressive symptoms and hopelessness, among others, as risk factors for suicide. Thus, it is important that prevention of suicidal behaviors aim to promote the development or enhancement of protective factors and reduction or minimization of risk factors (40), such as at the level of clinical intervention.
Young adults are vulnerable to suicide, which seems to be strongly related to family conditions and the sociocultural context. This vulnerability is mainly the result of the interaction of multiple factors and, therefore, intervention strategies for these behaviors should consider transdisciplinary approaches (41) and considered the development of internal assets as resilience (42).
In the present study, all methodological procedures required in a research study were followed, however there are some limitations, mainly regarding the used samples. There was a big difference between the “clinical” and non-clinical sample size, and the representation of young adults with a history of suicide attempt may be underestimated in this study, although these population are not very easy to have access and to participate.
Despite the limitations, the evidence found in this study allows us to verify that reasons for living may play a preponderant role in suicidal ideation. An intervention focused on promoting these beliefs and developing strategies to face adversity and deal with life situations that may cause psychological pain and suffering may work as a protective measure for individuals with a history of suicide attempt, or who may be more susceptible to suicidal ideation. Thus, it is important that professionals who intervene with these mental health situations are aware of the protective factors and recognize the role of reasons for living in the prevention and clinical intervention of suicidal behaviors.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Scientific Commission of the Psychology and Sciences Education Department of the University of Algarve. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. CM: Writing – original draft, Writing – review & editing. CN: Conceptualization, Formal analysis, Funding acquisition, Writing – review & editing. SJ: Conceptualization, Formal analysis, Writing – review & editing. AM: Formal analysis, Investigation, Methodology, Writing – original draft. CC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was partially funded by the FCT—Fundação para a Ciência e a Tecnologia, grant number UIDB/PSI/04345/2020.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Suicide (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/suicide (Accessed August 29, 2024).
2. National Institute of Statistics. Portal do INE (2024). Available online at: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0003736&contexto=bd&selTab=tab2 (Accessed May 16, 2024).
3. Bagge CL, Lamis DA, Nadorff M, Osman A. Relations between hopelessness, depressive symptoms and suicidality: Mediation by reasons for living. J Clin Psychol. (2014) 70:18–31. doi: 10.1002/jclp.2014.70.issue-1
4. Gvion Y, Levi-Belz Y. Serious suicide attempts: Systematic review of psychological risk factors. Front Psychiatry. (2018) 9:1–17. doi: 10.3389/fpsyt.2018.00056
5. Lamis DA, Lester D. Risk and protective factors for reasons for living in college men. Int J Mens Health. (2012) 11:189–201. doi: 10.3149/jmh.1103.189
6. Madeira A, Janeiro L, Carmo C, Brás M. Reasons for living inventory for young adults: psychometric properties among portuguese sample. Omega (United States). (2022) 85:887–903. doi: 10.1177/0030222820959940
7. O’Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br J Psychiatry. (2021) 218:326–33. doi: 10.1192/bjp.2020.212
8. Yi S, Chang EC, Chang OD, Seward NJ, McAvoy LB, Krause ER, et al. Coping and suicide in college students: Does being optimistic matter? Cris J Cris Interv Suicide Prev. (2021) 42:5–12. doi: 10.1027/0227-5910/a000662
9. General Health Coordination (Direção Geral da Saúde). National Plan for Suicide Prevention (Plano Nacional de Prevenção do Suicídio). Lisboa: Direção-Geral da Saúde (2013).
10. Klonsky ED, May AM. Differentiating suicide attempters from suicide ideators: A critical frontier for suicidology research. Suicide Life-Threatening Behav. (2014) 44:1–5. doi: 10.1111/sltb.2014.44.issue-1
11. Suominem K, Isometsä E, Suokas J, Haukka J, Achte K, Lönnqvist J. Completed suicide after a suicide attempt. Am J Psychiatry. (2004) 161:562–3. doi: 10.1176/appi.ajp.161.3.562
12. Bilsen J. Suicide and youth: risk factors. Front Psychiatry. (2018) 9:1–5. doi: 10.3389/fpsyt.2018.00540
13. Pirani S, Kulhanek C, Wainwright K, Osman A. The reasons for living inventory for young adults (RFL-YA-II). Assessment. (2021) 28:942–54. doi: 10.1177/1073191119900242
14. Sheldon E, Simmonds-buckley M, Bone C, Mascarenhas T, Chan N, Wincott M, et al. Prevalence and risk factors for mental health problems in university undergraduate students: A systematic review with meta-analysis. J Affect Disord. (2021) 287:282–92. doi: 10.1016/j.jad.2021.03.054
15. Ahern S, Burke L-A, McElroy B, Corcoran P, McMahon EM, Keeley H, et al. A cost-effectiveness analysis of school-based suicide prevention programmes. Eur Child Adolesc Psychiatry. (2018) 27:1295–304. doi: 10.1007/s00787-018-1120-5
16. Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
17. Bakhiyi CL, Calati R, Guillaume S, Courtet P. Do reasons for living protect against suicidal thoughts and behaviors A systematic review of the literature. J Psychiatr Res. (2016) 77:92–108. doi: 10.1016/j.jpsychires.2016.02.019
18. Testoni I, Piol S, De Leo D. Suicide prevention: university students’ Narratives on their reasons for living and for dying. J Environ Res Public Heal. (2021) 18:8029. doi: 10.3390/ijerph18158029
19. Amit N, Ibrahim N, Jaladin RAM, Din NC. The predicting roles of reasons for living and social support on depression, anxiety and stress among young people in Malaysia. Med J Malaysia. (2017) 72:291–7.
20. Cassaretto M, Martínez P. Razones para vivir en jóvenes adultos: validación del RFL-YA. Rev Psicol. (2012) 30:169–88. doi: 10.18800/psico.201201.007
21. Gutierrez PM, Osman A, Barrios FX, Kopper BA, Baker MT, Haraburda CM. Development of the reasons for living inventory for young adults. J Clin Psychol. (2002) 58:339–57. doi: 10.1002/jclp.v58:4
22. Ellis TE, Rufino KA, Allen JG. A controlled comparison trial of the Collaborative Assessment and Management of Suicidality (CAMS) in an inpatient setting: Outcomes at discharge and six-month follow-up. Psychiatry Res. (2017) 249:252–60. doi: 10.1016/j.psychres.2017.01.032
23. Ren Y, You J, Zhang X, Huang J, Conner BT, Sun R, et al. Differentiating suicide attempters from suicide ideators: the role of capability for suicide. Arch Suicide Res. (2019) 23:64–81. doi: 10.1080/13811118.2018.1426507
24. Vicent M, Rubio-Aparicio M, Sánchez-Meca J, Gonzálvez C. A reliability generalization meta-analysis of the child and adolescent perfectionism scale. J Affect Disord. (2019) 245:533–44. doi: 10.1016/j.jad.2018.11.049
25. Wang YY, Jiang NZ, Cheung EFC, Sun HW, Chan RCK. Role of depression severity and impulsivity in the relationship between hopelessness and suicidal ideation in patients with major depressive disorder. J Affect Disord. (2015) 183:83–9. doi: 10.1016/j.jad.2015.05.001
26. Ferreira JA, Castela MC. Questionário de ideação suicida (QIS). In: Testes e Provas Psicológicas em Portugal. APPORT/SHO, Braga (1999). p. 123–30.
27. Reynolds WM. Psychometric characteristics of the Adult Suicidal Ideation Questionnaire in college students. J Pers Assess. (1991) 56:289–307. doi: 10.1207/s15327752jpa5602_9
28. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: The Hopelessness Scale. J Consult Clin Psychol. (1974) 42:861–5. doi: 10.1037/h0037562
29. Cruz JP. Terapia Cognitiva de los intentos de suicidio: Cambiando historias de muerte por historias de vida. (Doctoral thesis). University of Sevilla, Sevilla, ES. (2000).
30. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological Corporation (1996).
31. Campos RC, Gonçalves B. The portuguese version of the beck depression inventory-II (BDI-II). Eur J Psychol Assess. (2011) 27:258–64. doi: 10.1027/1015-5759/a000072
32. Pirani S, Acosta M, Hoyos J, Gonzalez K, Osman A. Structure and validity of the reasons for living inventory for young adults-II (RFL-YA-II): A measure for assessing reasons for living. San Antonio: The University of Texas. (2016).
33. Field A. Discovering statistics using IBM SPSS Statistics. London: SAGE Publications Limited (2024).
34. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: The Guilford Press (2022).
35. Bruns KL, Letcher A. Protective factors as predictors of suicide risk among graduate students. J Coll Couns. (2018) 21:111–24. doi: 10.1002/jocc.2018.21.issue-2
36. Shi XL, Jiang L, Chen X, Zhu Y. Distinct trajectories of suicidal behaviors throughout the university stage and associated risk and protective factors: A large-scale prospective study. J Affect Disord. (2022) 319:407–15. doi: 10.1016/j.jad.2022.09.107
37. Christensen K, Hom MA, Stanley IH, Joiner TE. Reasons for living and suicide attempts among young adults with lifetime suicide ideation. Crises. (2021) 42:179–85. doi: 10.1027/0227-5910/a000705
38. Bryan CJ, Oakey DN, Harris JA. Reasons for living among U.S. Army personnel thinking about suicide. Cognit Ther Res. (2018) 42:758–68. doi: 10.1007/s10608-018-9932-7
39. Osman A, Barrios FX, Gutierrez PM, Wrangham JJ, Kopper BA, Truelove RS, et al. The Positive and Negative Suicide Ideation (PANSI) Inventory: Psychometric evaluation with adolescent psychiatric inpatient samples. J Pers Assess. (2002) 79:512–30. doi: 10.1207/S15327752JPA7903_07
40. Pechorro P, Revilla R, Palma VH, Nunes C, Martins C, Cyders MA. Examination of the SUPPS-P impulsive behavior scale among male and female youth: psychometrics and invariance. Children. (2021) 8:283. doi: 10.3390/children8040283
41. Junior ARC, Fletes JC, Lemos T, Teixeira EP, de Souza M de L. Risk factors for suicide: Systematic review. Saudi J Heal Sci. (2020) 9:183–93. doi: 10.4103/sjhs.sjhs_83_20
Keywords: suicide, depressive symptoms, reasons for living, hopelessness, young adults
Citation: Brás M, Martins C, Nunes C, Jesus SN, Madeira AR and Carmo C (2025) Reasons for living and depressive symptomatology in young adults with and without suicide attempts: a moderated mediation approach. Front. Psychiatry 15:1443894. doi: 10.3389/fpsyt.2024.1443894
Received: 04 June 2024; Accepted: 23 December 2024;
Published: 23 January 2025.
Edited by:
Jean Marc Guile, University of Picardie Jules Verne, FranceReviewed by:
Joël Djatche Miafo, Joël Miafo DJATCHE, CameroonMerve Bat Tonkus, Istanbul Yeni Yüzyıl University, Türkiye
Daniel Nzebou, UNIPSY Yaoundé, Cameroon, in collaboration with reviewer JDM
Copyright © 2025 Brás, Martins, Nunes, Jesus, Madeira and Carmo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Brás, bWJyYXNAdWFsZy5wdA==
†ORCID: Cláudia Carmo, orcid.org/0000-0002-7301-349X