
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 18 July 2024
Sec. Schizophrenia
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1436142
 Mubing Ding1,2†Shaotong Zhang2†Zaochen Zhu2†Renliang Cai2Jin Fang2
Mubing Ding1,2†Shaotong Zhang2†Zaochen Zhu2†Renliang Cai2Jin Fang2 Chao Zhou2
Chao Zhou2 Xiangrong Zhang2*
Xiangrong Zhang2* Xinyu Fang2*
Xinyu Fang2*Objective: The aim of this study was to explore the risk factors for different metabolic status in patients with schizophrenia.
Methods: A total of 968 hospitalized patients with schizophrenia were recruited. Fasting blood glucose (GLU) and lipid profile, including total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG) were measured. Schizophrenia patients were divided into four groups: normal metabolism and weight (NMNW), abnormal metabolism and normal weight (AMNW), normal metabolism and overweight/obesity (NMO), and abnormal metabolism and overweight/obesity (AMO).
Results: Our results showed that NMNW, AMNW, NMO, and AMO accounted for 25.3%, 12.7%, 25.4%, and 36.6%, respectively. There were significant differences in age, disease duration, body mass index (BMI), waist circumference, chronic disease, systolic blood pressure (SBP), diastolic blood pressure (DBP), GLU, TG, TC, HDL-C, and LDL-C among these four groups (all p < 0.05). With the NMNW group as the reference, the disordered multiple classification regression analysis showed that chronic disease was a significant risk factor for AMNW (OR = 5.271, 95% CI = 3.165 to 8.780, p < 0.001) and AMO (OR = 3.245, 95% CI = 2.004 to 5.254, p < 0.001), age was an important protective factor for NMO (OR = 0.968, 95% CI = 0.943 to 0.994, p = 0.015) and AMO (OR = 0.973, 95% CI = 0.948 to 0.999, p < 0.042), waist circumference was a significant risk factor for NMO (OR = 1.218, 95% CI = 1.180 to 1.257, p < 0.001) and AMO (OR = 1.252, 95% CI = 1.212 to 1.291, p < 0.001), and college education was an obvious protective factor for AMO (OR = 0.343, 95% CI = 0.123 to 0.953, p < 0.040) among patients with schizophrenia.
Conclusion: The findings of our study underscored the importance of factors such as age, education level, chronic disease, and waist circumference when exploring the influencing factors and biological mechanisms of obesity-related metabolic problems in schizophrenia patients.
Schizophrenia is a psychiatric disorder characterized by distorted thinking, perception, and emotional disharmony (1). It affects approximately 1% of the world population, with a heightened risk reaching 2.5 times for mortality compared to that in the general population (2), consequently leading to 10–20 years of life expectancy lost in patients with schizophrenia (3). Premature mortality is primarily attributed to preventable physical illness, especially cardiovascular disease (4). Large-scale epidemiological investigations have consistently shown that cardiovascular disease is the leading cause of death in individuals with schizophrenia, accounting for up to one-third of all cases (4, 5).
Patients diagnosed with schizophrenia are associated with a range of unfavorable cardiovascular traits, such as a higher risk of abdominal obesity, higher blood pressure, higher risk of hyperlipidemia, hyperglycemia, and insulin resistance (6). The occurrence of these metabolic disorders may be attributed to multiple factors, such as genetic liability, psychotropic drugs used, poor eating habits, and lifestyle (7, 8). A recent meta-analysis demonstrated that schizophrenia patients had an elevated risk of metabolic syndrome, even in first-episode drug-naïve patients, compared to the age- and gender-matched controls (9). Additionally, a Mendelian randomization study has indicated that schizophrenia was genetically associated with dyslipidemia (10). Moreover, a previous study has reported that schizophrenia patients receiving olanzapine monotherapy for over 2 years had a 44% risk of developing metabolic syndrome (11). Unhealthy habits such as poor diet, smoking, and lack of exercise are prevalent among schizophrenia patients, which were constantly shown to increase the risk of developing metabolic disorders (12). Taken together, patients with schizophrenia had an increased risk of metabolic disorders and cardiovascular disease due to various intrinsic and extrinsic factors, ultimately exacerbating the mortality outcome. Hence, knowing the risk factors for metabolic disorders in patients diagnosed with schizophrenia can help early cardiovascular disease screening and treatments and eventually improve their outcomes.
As we know, metabolic disorders encompass abnormalities in body mass, blood glucose, blood pressure, blood lipids, and other related indicators (13). Intriguingly, patients with schizophrenia do not usually have the above metabolic indicator abnormality simultaneity; some may only demonstrate alterations in one or two parameters of body mass, blood glucose, blood pressure, or blood lipids. However, most previous studies have only focused on one aspect of metabolic indicators and compared the differences between schizophrenia patients with and without obesity (14, 15), with and without diabetes (16), or with and without hyperlipidemia (17, 18). To better understand this topic, we divided schizophrenia patients into four groups: patients with normal metabolism and weight (NMNW), patients with abnormal metabolism and normal weight (AMNW), patients with normal metabolism and overweight/obesity (NMO), and patients with abnormal metabolism and overweight/obesity (AMO). We aimed to compare the basic data differences between groups, thus providing directions regarding more targeted supervision and intervention of these patients.
A total of 968 schizophrenia patients were recruited from the hospitalization department of Wuhu Fourth People’s Hospital, China. All patients met the following criteria: 1) diagnosed with schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), using modified sections of the Structured Clinical Interview for DSM-5 disorders (SCID) by at least two experienced psychiatrists; 2) age range from 18 to 65 years and Han Chinese ethnicity; and 3) body mass index (BMI) ≥18.5 kg/m2 (calculated by weight divided by the square of height). The exclusion criteria included the following: 1) any other major Axis disorder, 2) pregnant or breastfeeding, and 3) substance (except for tobacco) abuse/dependence.
The study was approved by the Institutional Review Board of Wuhu Fourth People’s Hospital, and all participants were recruited between January 2023 and August 2023. Written informed consent was provided by all patients and/or their guardians after the research process was fully explained.
A questionnaire was applied to collect the basic demographic and clinical data, including age, sex, height, weight, education level, marital status, smoking and drinking habits, chronic physical disease (excluding metabolic diseases directly related to blood pressure, blood glucose, and blood lipids, but including respiratory system diseases, digestive system diseases, etc.), and disease duration. Blood samples from the participants were obtained following an overnight fasting period. The serum was separated, aliquoted, and stored at −80°C until used for the assay. Fasting blood glucose (GLU) and lipid profile, including total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG), were measured using an automatic Biochemical Analyzer (HITACHI 7170A, Hitachi, Ltd., Tokyo, Japan). Blood pressure including systolic blood pressure (SBP) and diastolic blood pressure (DBP) was measured using an automated blood pressure machine before the blood was obtained. The waist circumference of patients was measured between the lower rib margin and the iliac crest after a normal expiratory breath (13).
In the present study, four groups: normal metabolism and weight (NMNW), abnormal metabolism and normal weight (AMNM), normal metabolism and overweight/obesity (NMO), and abnormal metabolism and overweight/obesity (AMO), according to their BMI and metabolic parameters. Overweight/obesity was defined as BMI ≥ 24 kg/m2, and normal weight was defined as a BMI between 18.5 and 24 kg/m2 (14). According to the definition by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), abnormal metabolism was diagnosed using any two of the following criteria: 1) blood pressure ≥130/85 mmHg, a history of hypertension, or received antihypertensive treatment; 2) fasting triglyceride level ≥1.7 mmol/L; 3) HDL-C level <1.03 mmol/L for men and <1.30 mmol/L for women; or 4) a fasting plasma glucose (FPG) level ≥5.6 mmol/L or has reported previously physician-diagnosed diabetes (19).
The data analysis was performed using IBM SPSS software (version 23.0, Chicago, IL, USA). The analysis of variance (ANOVA) or the chi-squared tests were used to compare the differences between groups, as appropriate. The Bonferroni correction was further used for multiple tests. Then, the disordered multiple classification regression analysis was conducted to identify risk factors related to abnormal metabolism and overweight/obesity, with all observed factors as independent variables and the four groups set as dependent variables (with normal metabolism and weight as the reference). All statistical tests were two-tailed, and statistical significance was set at alpha ≤ 0.05.
Among 968 schizophrenia patients we included in the present study, 245 were NMNW (25.3%), 123 were AMNW (12.7%), 246 were NMO (25.4%), and 354 were AMO (36.6%). As shown in Table 1, there were significant differences in age, disease duration, BMI, waist circumference, chronic disease, SBP, DBP, GLU, TG, TC, HDL-C, and LDL-C among these four groups (all p < 0.05). After the Bonferroni correction was conducted, we found that schizophrenia patients with AMNW and AMO were older than patients with NMNW and NMO (Bonferroni-corrected p < 0.05), while there was no significant difference in age between patients with AMNW and AMO (Bonferroni-corrected p > 0.05) and between patients with NMNW and NMO (Bonferroni-corrected p > 0.05). Patients with AMNW had a longer disease duration compared to patients with NMO after the Bonferroni correction was conducted (Bonferroni-corrected p = 0.044), but no difference among other groups remained (Bonferroni-corrected p > 0.05). After the Bonferroni correction was conducted, there were significant differences in BMI and waist circumference among groups (Bonferroni-corrected p < 0.001) except for the two groups of NMNW and AMNW (Bonferroni-corrected p > 0.05). For SBP, DBP, and GLU, our results showed that patients with AMNW and AMO had a higher level of these three indicators than patients with NMNW and NMO (Bonferroni-corrected p < 0.001), while there was no significant difference between patients with AMNW and AMO (Bonferroni-corrected p > 0.05) and between patients with NMNW and NMO (Bonferroni-corrected p > 0.05). The difference in TG among the four groups still remained after the Bonferroni correction was conducted (Bonferroni-corrected p < 0.05), with NMNW having the lowest TG level, followed by NMO and then AMNW, and AMO having the highest level. After the Bonferroni correction was conducted, the difference in HDL-C levels between groups (Bonferroni-corrected p < 0.001) was still significant except for the two groups of AMNW and AMO (Bonferroni-corrected p > 0.05), and the differences in LDL-C and TC levels between the NMNW and NMO groups, between the NMNW and AMO groups, between the AMNW and AMO groups, and between the NMO and AMO groups still remained after the Bonferroni correction was conducted (Bonferroni-corrected p < 0.05), but there were no differences in LDL-C and TC levels between the NMNW and AMNW groups and between the AMNW and NMO groups after the Bonferroni correction was conducted (Bonferroni-corrected p > 0.05). Additionally, we found that schizophrenia patients with AMNW and AMO had a higher rate of chronic disease compared to the patients with NMNW and NMO (Bonferroni-corrected p < 0.05), while there was no significant difference in age between patients with AMNW and AMO (Bonferroni-corrected p > 0.05) and between patients with NMNW and NMO (Bonferroni-corrected p > 0.05) after the Bonferroni correction was conducted.
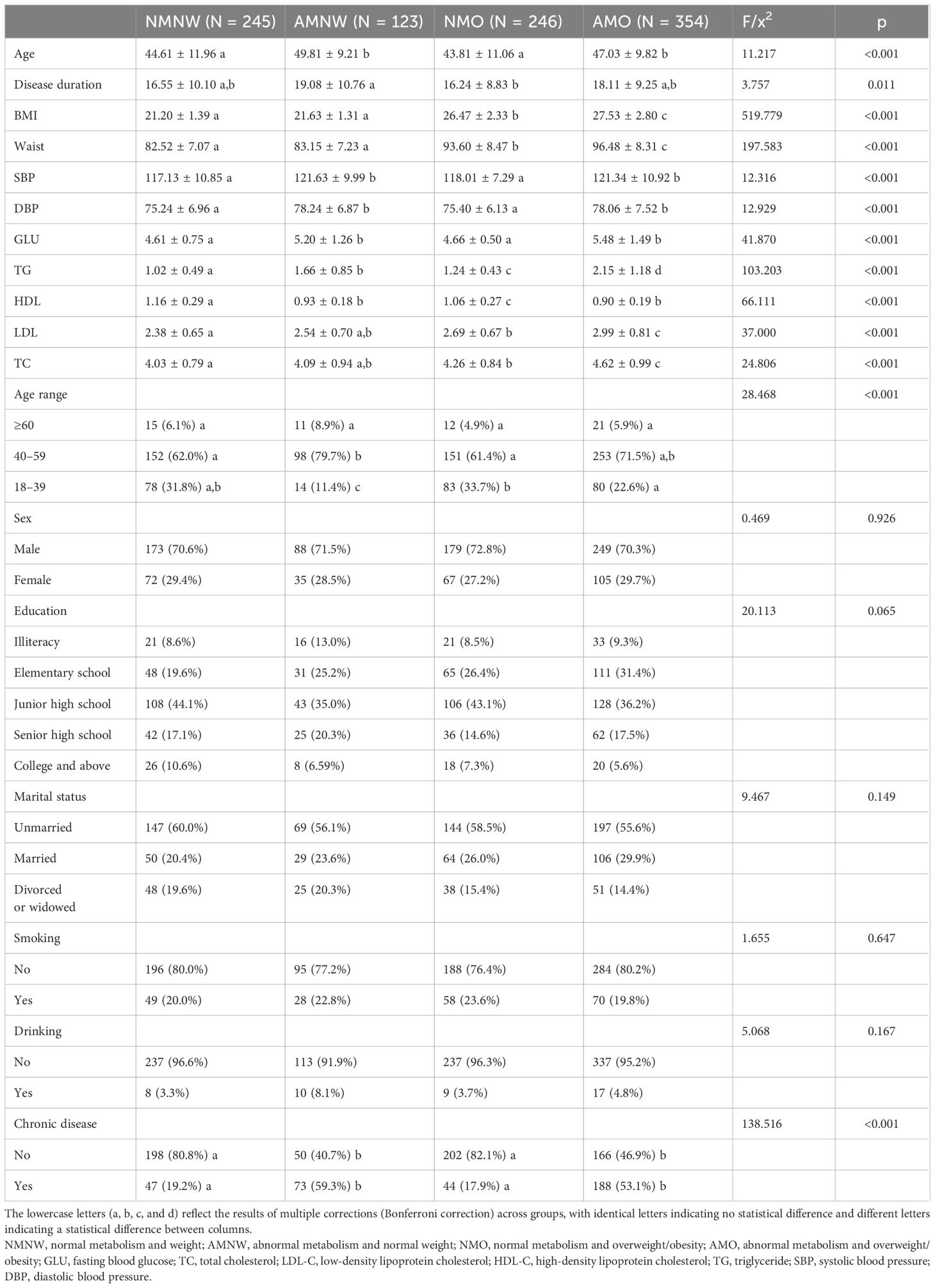
Table 1 Comparisons among four different patient groups.
With the NMNW group as the reference, our disordered multiple classification regression analysis showed that the chronic disease was a significant risk factor for AMNW (OR = 5.271, 95% CI = 3.165 to 8.780, p < 0.001) and AMO (OR = 3.245, 95% CI = 2.004 to 5.254, p < 0.001), age was an important protective factor for NMO (OR = 0.968, 95% CI = 0.943 to 0.994, p = 0.015) and AMO (OR = 0.973, 95% CI = 0.948 to 0.999, p < 0.042), waist circumference was a significant risk factor for NMO (OR = 1.218, 95% CI = 1.180 to 1.257, p < 0.001) and AMO (OR = 1.252, 95% CI = 1.212 to 1.291, p < 0.001), and college education was an obvious protective factor for AMO (OR = 0.343, 95% CI = 0.123 to 0.953, p < 0.040) among patients with schizophrenia (see Table 2).
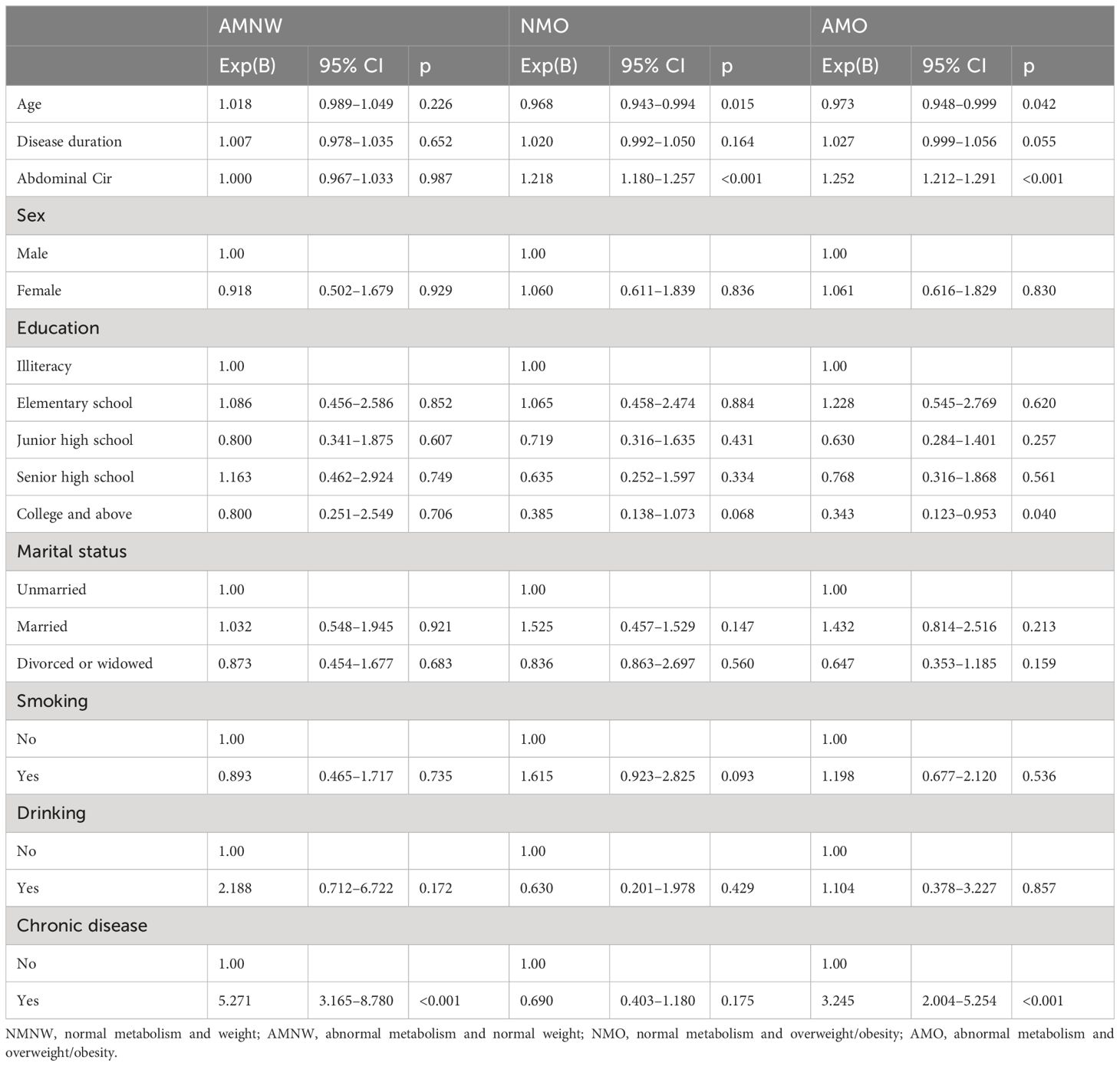
Table 2 The results of disordered multiple classification regression analysis.
In the present study, a preliminary comparison was made among schizophrenia patients with different BMI and metabolic status, and the influencing factors of different metabolic status in those patients were further explored. Our results showed that NMNW, AMNW, NMO, and AMO accounted for 25.3%, 12.7%, 25.4%, and 36.6% respectively. In addition to BMI, SBP, DBP, GLU, TG, TC, HDL-C, and LDL-C, there were also significant differences in age, disease duration, waist circumference, and chronic disease among four patient groups. Further disordered multiple classification regression analysis demonstrated that chronic disease was a significant risk factor for AMNW and AMO, waist circumference was a significant risk factor for NMO and AMO, age was an important protective factor for NMO and AMO, and college education was an obvious protect factor for AMO in patients with schizophrenia.
A newly published meta-analysis revealed a combined pooled prevalence of overweight and obesity at 58.6% among patients with schizophrenia (20), a finding consistent with our current study (25.4% + 36.6%). Furthermore, an earlier meta-analysis comprising 77 publications with a sample size of 25,692 schizophrenia patients indicated a prevalence of metabolic syndrome in this population at 32.5% (21). Previous research has also shown that the incidence of metabolic syndrome varies in first-episode drug-naïve schizophrenia patients and those undergoing long-term atypical antipsychotic-treated schizophrenia patients ranging from 19% to 44% (11, 22). In the current study, the prevalence of metabolic syndrome ranged from at least 36.6% to a maximum of 49.3% among chronic hospitalized schizophrenia. Collectively, this body of evidence supports that schizophrenia patients have a heightened prevalence of overweight/obesity and metabolic abnormalities. However, not all schizophrenia patients with metabolic syndrome have overweight/obesity, and not all obese patients have metabolic syndrome, so the heterogeneity of metabolic abnormalities should be considered when exploring the association between metabolic status and demographic, clinical, or even neurobiological parameters in schizophrenia patients. Hence, we carried out this preliminary investigation.
There was a significant difference in age among the four patient groups; furthermore, regression analysis revealed that age was a protective factor for overweight/obesity (regardless of metabolism) in schizophrenia patients. This was different from a recent study conducted in China, which found that age was a risk factor for AMNW and NMO when compared to NMNW in schizophrenia (23). This discrepancy may be caused by the age distribution of the patients recruited in the different studies. In the present study, schizophrenia patients aged 18–39 years, 40–59 years, and over 60 years accounted for 26.3%, 67.6%, and 6.1%, respectively, but in that recent study, patients in the corresponding age groups accounted for 45.2%, 41.5%, and 13.3%, respectively. As we know, many functions of the body are degraded as age slowly increases; for example, digestive ability is not as good as before, thus leading to weight loss in older patients. Additionally, it should be pointed out that age may also reflect the length of the disease course, which together affects metabolic status in patients with schizophrenia; although our regression analysis did not find a direct effect of disease duration on metabolic status, the protective effect of age needs to be interpreted with caution. Therefore, future studies should enlarge the sample size and recruit schizophrenia patients of different ages in balance to further rigorously explore the effects of age and disease duration on body weight and metabolism.
Moreover, our findings revealed variations in waist circumference among schizophrenia patients with different metabolic status, with waist circumference proving to be a significant risk for overweight/obesity (NMO and AMO) in this population. This was also supported by a recent study that indicated that waist circumference was a prominent risk factor for obesity in schizophrenia patients (24). Interestingly, a longitudinal study demonstrated a significant increase in waist circumference following 6 months of antipsychotic treatment (25), suggesting its potential utility in the early monitoring of drug-induced weight and associated metabolic disorders among schizophrenia patients. In addition, waist circumference is widely regarded as a reliable indicator of abdominal adiposity and a valuable predictor of cardiovascular disease risk, particularly in situations where the use of radiological imaging is not feasible (26, 27).
We have also discovered that college education is an important protective factor for AMO, although it has no significant effect on AMNW and NMO in patients with schizophrenia. This means that high educational attainment has some protective effect against concurrent overweight/obesity and metabolic abnormalities in schizophrenia patients. The possible explanation is that highly educated individuals tend to show higher self-discipline and pay more attention to weight control, diet control, and physical exercise, especially when the body experiences weight changes or metabolic abnormalities, and these individuals are more alert to avoid developing a more serious metabolic state. This explanation needs to be further verified by future studies (28).
As we know, obesity and metabolic abnormalities are common chronic diseases in humans. In this study, we further analyzed the effects of chronic diseases other than obesity and glycolipid metabolism on obesity-related metabolic status in schizophrenia patients. Our findings revealed that the prevalence of chronic disease in schizophrenia patients with abnormal metabolism (AMNW or AMO) was significantly higher than that in patients with normal metabolism (NMNW or NMO). Regression analysis further indicated that chronic diseases were a risk factor for abnormal metabolism in patients with schizophrenia. A recent observational multicohort study also demonstrated that obesity is highly correlated with 21 diseases, and the interconnectedness of multiple diseases accelerates the development of obesity-related morbidity (29). Research from China additionally supported the link between obesity and the risk of chronic diseases (30). Overall, the aforementioned evidence supports the notion that obesity and other chronic diseases are interconnected, underscoring the need for future studies to consider and address the influence of other chronic diseases when investigating the influencing factors and biological mechanisms behind obesity-related metabolic issues in patients with schizophrenia patients. Furthermore, knowing what drives these associations is crucial to increasing the quality and duration of life for those patients.
Several limitations should be mentioned here. First, with a cross-sectional study design, we were unable to make a causal relationship between different metabolic status and factors in patients with schizophrenia. Second, only a few factors were investigated in the present study, while other information related to metabolic syndrome, such as physical activity and dietary habits, was not recorded. In addition, it is well known that antipsychotic drugs can have serious metabolic side effects but vary between drugs (31, 32). However, the present study did not consider and calculate the effects of the duration, types, and dosage of antipsychotic drugs on the metabolic status of schizophrenia patients. Third, all patients were of chronically hospitalized types and with long-term medications treated in one hospital, which limits the generalizability of our findings. Therefore, future studies based on longitudinal design and incorporating more relevant factors are warranted to explore the influence factors and even biological mechanism of different BMI and metabolic status in schizophrenia patients.
In summary, our study demonstrated that age, disease duration, waist circumference, and chronic disease are important influencing factors in overweight/obesity and metabolic abnormalities in schizophrenia, thus underscoring the importance of strict monitoring and management of these factors to reduce the risk of obesity-related metabolic problems. Additionally, future neurobiological studies on this topic should also consider the influence of these fundamental factors.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Fourth People’s Hospital of Wuhu. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MD: Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Resources, Visualization. SZ: Data curation, Formal analysis, Methodology, Software, Writing – original draft, Visualization. ZZ: Data curation, Formal analysis, Methodology, Software, Writing – original draft, Investigation, Resources, Visualization. RC: Data curation, Formal analysis, Methodology, Writing – original draft. JF: Data curation, Formal analysis, Methodology, Writing – original draft. CZ: Data curation, Formal analysis, Methodology, Writing – original draft. XZ: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Writing – review & editing. XF: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Key Research and Development Program of China (No. 2018YFC1314300 and 2016YFC1307002), the National Natural Science Foundation of China (82371510, 81971255, 81571314 and 82101572), Social Development Foundation of Jiangsu Province, China (No. BE2023668 and No. BE2019610), Jiangsu Provincial Medical Talent project (ZDRCA2016075), Nanjing Major Science and Technology Project (Life and Health, No 202305035), the Key Project supported by Medical Science and Technology Development Foundation, Nanjing Department of Health (YKK20090), and the Science and Technology Development Program of Nanjing Medical University (NMUB2019107).
We thank all clinical psychiatrists, nurses, and schizophrenia patients who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Grywińska WB, Głowacka A. Combining samidorphan with olanzapine to mitigate weight gain as a side effect in schizophrenia treatment. Postepy psychiatrii neurologii. (2023) 32:128–37. doi: 10.5114/ppn.2023.132493
2. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiologic Rev. (2008) 30:67–76. doi: 10.1093/epirev/mxn001
3. Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. (2014) 13:153–60. doi: 10.1002/wps.v13.2
4. Chang CK, Chesney E, Teng WN, Hollandt S, Pritchard M, Shetty H, et al. Life expectancy, mortality risks and cause of death in patients with serious mental illness in South East London: a comparison between 2008-2012 and 2013-2017. psychol Med. (2023) 53:887–96. doi: 10.1017/S0033291721002257
5. Olfson M, Gerhard T, Huang C, Crystal S, Stroup TS. Premature mortality among adults with schizophrenia in the United States. JAMA Psychiatry. (2015) 72:1172–81. doi: 10.1001/jamapsychiatry.2015.1737
6. Papanastasiou E. The prevalence and mechanisms of metabolic syndrome in schizophrenia: a review. Ther Adv Psychopharmacol. (2013) 3:33–51. doi: 10.1177/2045125312464385
7. Polcwiartek C, O'Gallagher K, Friedman DJ, Correll CU, Solmi M, Jensen SE, et al. Severe mental illness: cardiovascular risk assessment and management. Eur Heart J. (2024) 45:987–97. doi: 10.1093/eurheartj/ehae054
8. Veeneman RR, Vermeulen JM, Bialas M, Bhamidipati AK, Abdellaoui A, Munafò MR, et al. Mental illness and cardiovascular health: observational and polygenic score analyses in a population-based cohort study. psychol Med. (2024) 54:931–9. doi: 10.1017/S0033291723002635
9. Garrido-Torres N, Rocha-Gonzalez I, Alameda L, Rodriguez-Gangoso A, Vilches A, Canal-Rivero M, et al. Metabolic syndrome in antipsychotic-naïve patients with first-episode psychosis: a systematic review and meta-analysis. psychol Med. (2021) 51:2307–20. doi: 10.1017/S0033291721002853
10. Saadullah Khani N, Cotic M, Wang B, Abidoph R, Mills G, Richards-Belle A, et al. Schizophrenia and cardiometabolic abnormalities: A Mendelian randomization study. Front Genet. (2023) 14:1150458. doi: 10.3389/fgene.2023.1150458
11. Zhang C, Fang X, Yao P, Mao Y, Cai J, Zhang Y, et al. Metabolic adverse effects of olanzapine on cognitive dysfunction: A possible relationship between BDNF and TNF-alpha. Psychoneuroendocrinology. (2017) 81:138–43. doi: 10.1016/j.psyneuen.2017.04.014
12. Heald A, Pendlebury J, Anderson S, Narayan V, Guy M, Gibson M, et al. Lifestyle factors and the metabolic syndrome in schizophrenia: a cross-sectional study. Ann Gen Psychiatry. (2017) 16:12. doi: 10.1186/s12991-017-0134-6
13. Fang X, Yu L, Wang D, Chen Y, Wang Y, Wu Z, et al. Association between SIRT1, cytokines, and metabolic syndrome in schizophrenia patients with olanzapine or clozapine monotherapy. Front Psychiatry. (2020) 11:602121. doi: 10.3389/fpsyt.2020.602121
14. Zhang Y, Tang W, Tang B, Fan K, Zhao K, Fang X, et al. Altered mitochondrial lymphocyte in overweight schizophrenia patients treated with atypical antipsychotics and its association with cognitive function. Front Immunol. (2023) 14:1325495. doi: 10.3389/fimmu.2023.1325495
15. Deng X, Lu S, Li Y, Fang X, Zhang R, Shen X, et al. Association between increased BMI and cognitive function in first-episode drug-naïve male schizophrenia. Front Psychiatry. (2024) 15:1362674. doi: 10.3389/fpsyt.2024.1362674
16. Huo L, Zhang G, Du XD, Jia Q, Qian ZK, Chen D, et al. The prevalence, risk factors and clinical correlates of diabetes mellitus in Chinese patients with schizophrenia. Schizophr Res. (2020) 218:262–6. doi: 10.1016/j.schres.2019.12.029
17. Yu Y, Zhao J, Jin YL, Xie Q, Yao DF, Yao M. [Prevalence rate and risk factor analysis of nonalcoholic fatty liver disease in 115 female patients with schizophrenia]. Zhonghua gan zang bing za zhi = Zhonghua ganzangbing zazhi = Chin J Hepatol. (2023) 31:947–53. doi: 10.3760/cma.j.cn501113-20230407-00148
18. Li X, Gao Y, Wang Y, Wang Y, Wu Q. Prevalence and influence factors for non-alcoholic fatty liver disease in long-term hospitalized patients with schizophrenia: A cross-sectional retrospective study. Neuropsychiatr Dis Treat. (2023) 19:379–89. doi: 10.2147/NDT.S398385
19. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement: Executive Summary. Crit pathways Cardiol. (2005) 4:198–203. doi: 10.1097/00132577-200512000-00018
20. Afzal M, Siddiqi N, Ahmad B, Afsheen N, Aslam F, Ali A, et al. Prevalence of overweight and obesity in people with severe mental illness: systematic review and meta-analysis. Front Endocrinol. (2021) 12:769309. doi: 10.3389/fendo.2021.769309
21. Mitchell AJ, Vancampfort D, Sweers K, van Winkel R, Yu W, De Hert M. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders–a systematic review and meta-analysis. Schizophr Bull. (2013) 39:306–18. doi: 10.1093/schbul/sbr148
22. Lang X, Liu Q, Fang H, Zhou Y, Forster MT, Li Z, et al. The prevalence and clinical correlates of metabolic syndrome and cardiometabolic alterations in 430 drug-naive patients in their first episode of schizophrenia. Psychopharmacology. (2021) 238:3643–52. doi: 10.1007/s00213-021-05983-9
23. Yu W, Liu Z, Xu Y, Yuan Q, Guo Y, Zhao R, et al. The current prevalence situation and influencing factors of normal weight,overweight or obesity in different metabolic types of Bao'an district in Shenzhen. Chin J Prev Control Chronic Dis. (2022) 30:597–601,5.
24. Yong N, Pan J, Li X, Yu L, Hou X. Influencing factors of obesity in community patients with deficit schizophrenia: a cross-sectional study. Eur J Med Res. (2022) 27:90. doi: 10.1186/s40001-022-00706-y
25. Jaberi N, Faramarzi E, Farahbakhsh M, Ostadarahimi A, Asghari Jafarabadi M, Fakhari A. Prevalence of metabolic syndrome in schizophrenia patients treated with antipsychotic medications. Caspian J Internal Med. (2020) 11:310–4. doi: 10.22088/cjim.11.3.310
26. Barber J, Palmese L, Chwastiak LA, Ratliff JC, Reutenauer EL, Jean-Baptiste M, et al. Reliability and practicality of measuring waist circumference to monitor cardiovascular risk among community mental health center patients. Community Ment Health J. (2014) 50:68–74. doi: 10.1007/s10597-012-9590-2
27. de Vegt F, Dekker JM, Jager A, Hienkens E, Kostense PJ, Stehouwer CD, et al. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: The Hoorn Study. Jama. (2001) 285:2109–13. doi: 10.1001/jama.285.16.2109
28. Wang L, Zhou B, Zhao Z, Yang L, Zhang M, Jiang Y, et al. Body-mass index and obesity in urban and rural China: findings from consecutive nationally representative surveys during 2004-18. Lancet (London England). (2021) 398:53–63. doi: 10.1016/S0140-6736(21)00798-4
29. Kivimäki M, Strandberg T, Pentti J, Nyberg ST, Frank P, Jokela M, et al. Body-mass index and risk of obesity-related complex multimorbidity: an observational multicohort study. Lancet Diabetes Endocrinol. (2022) 10:253–63. doi: 10.1016/S2213-8587(22)00033-X
30. Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. (2021) 9:446–61. doi: 10.1016/S2213-8587(21)00118-2
31. Vancampfort D, Stubbs B, Mitchell AJ, De Hert M, Wampers M, Ward PB, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry. (2015) 14:339–47. doi: 10.1002/wps.20252
32. Pillinger T, McCutcheon RA, Vano L, Mizuno Y, Arumuham A, Hindley G, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. (2020) 7:64–77. doi: 10.1016/S2215-0366(19)30416-X
Keywords: schizophrenia, obesity, metabolism, risk factors, glucose, lipid
Citation: Ding M, Zhang S, Zhu Z, Cai R, Fang J, Zhou C, Zhang X and Fang X (2024) Influencing factors of different metabolic status in hospitalized patients with schizophrenia. Front. Psychiatry 15:1436142. doi: 10.3389/fpsyt.2024.1436142
Received: 21 May 2024; Accepted: 02 July 2024;
Published: 18 July 2024.
Edited by:
Tianhong Zhang, Shanghai Jiao Tong University, ChinaReviewed by:
Chao Deng, University of Wollongong, AustraliaCopyright © 2024 Ding, Zhang, Zhu, Cai, Fang, Zhou, Zhang and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinyu Fang, Znh5d2lsYnVyQDE2My5jb20=; Xiangrong Zhang, ZHJ4cnpAaG90bWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.