 Zoe-Sofia Schöndorf1,2
Zoe-Sofia Schöndorf1,2 Valentin Terhoeven1
Valentin Terhoeven1 Anna Jaehn3
Anna Jaehn3 Daniela Roesch-Ely3
Daniela Roesch-Ely3 Hans-Christoph Friederich1,2
Hans-Christoph Friederich1,2 Christoph Nikendei1
Christoph Nikendei1 David Kindermann1,2*
David Kindermann1,2*- 1Department of General Internal Medicine and Psychosomatics, University Hospital Heidelberg, University of Heidelberg, Heidelberg, Germany
- 2DZPG (German Centre for Mental Health – Partner Site Heidelberg/Mannheim/Ulm), Heidelberg, Germany
- 3Department of General Psychiatry, University Hospital Heidelberg, University of Heidelberg, Heidelberg, Germany
Background: Previous research has indicated cognitive impairments in patients with post-traumatic stress disorder (PTSD), specifically in attention, memory, and executive functioning. However, there is limited knowledge about the cognitive profile of individuals with complex PTSD (cPTSD), a new diagnosis in ICD-11. Moreover, predictors of cognitive impairment remain unclear. The present study aims to enhance understanding of cognitive functioning and its predictors in cPTSD compared with non-complex PTSD (ncPTSD).
Methods: N = 64 participants (n = 34 cPTSD, n = 30 ncPTSD) completed psychometric questionnaires and the neuropsychological test set Cognitive Basic Assessment (COGBAT) assessing a general cognitive index, attention, visual memory, and executive functioning. First, the test results of both groups were compared to the COGBAT norm sample. Secondly, group differences in cognitive domains were analyzed using student t-tests with independent samples (cPTSD vs. ncPTSD). Thirdly, bivariate and multivariate regressions examined influencing factors of cognitive impairment.
Results: Both groups showed cognitive impairments in comparison to the COGBAT norm group. Significant differences between cPTSD and ncPTSD were found in visual memory (p = .003) and selective attention (p = .004). In multivariate regression, type of PTSD and age were found to significantly impact visual memory, while type of PTSD, age, and psychotropic medication showed significant effects on selective attention.
Conclusions: Given higher symptom severity and cognitive deficits in cPTSD, more intensive and diverse interventions should be considered in comprehensive treatment plans, for instance, cognitive training.
1 Introduction
Experiencing traumatic events can significantly impact mental well-being, potentially leading to mental disorders. In the 11th version of the International Classification of Diseases (ICD-11), the diagnosis of post-traumatic stress disorder (PTSD) is complemented by the new diagnosis of complex post-traumatic stress disorder (cPTSD), acknowledging the diverse symptomatology resulting from trauma (1, 2). In addition to the PTSD symptom triad of re-experience, avoidance, and hyperarousal, the diagnosis of cPTSD includes disturbances in self-organization (DSO): negative self-concept, interpersonal problems, and affective dysregulation. There is an ongoing debate on whether cPTSD is a distinct diagnosis from the “classic” PTSD, which will be referred to as “non-complex” PTSD (ncPTSD) in the following. In contrast to ICD-11, the new diagnosis of cPTSD was not included in the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; 3). However, in DSM-5, the diagnostic criteria for PTSD were expanded to include negative changes in mood and cognition as well as a dissociative subtype. The different symptom profiles resulting from this expansion of diagnostic criteria are criticized for complicating treatment planning based on the diagnosis (1). Overall, recent studies and clinical observations emphasize the need for both diagnostic entities (cPTSD and ncPTSD) (4–6). Moreover, cPTSD and ncPTSD result in different therapeutic strategies based on symptom profiles (1, 7). Current data from a representative German sample shows a one-month prevalence of 0.5% for cPTSD compared to 1.5% for ncPTSD (8). Given the relative novelty of this research field, further research is needed to enhance our understanding of cPTSD and improve therapeutic approaches.
Previous research indicates that trauma-related disorders are often associated with impairments in cognitive performance, even for emotionally neutral stimuli (9–11). In total, research on cognitive functioning in patients with trauma-related disorders identified cognitive impairments, primarily in the domains of memory, attention, and executive functioning (9, 10, 12–14), especially in tasks that require processing speed (11). From a clinical standpoint, these impairments may be highly relevant, as cognitive functioning was shown to play a role in coping with posttraumatic stress (10–12, 15). In previous research consisting of neuropsychological assessments, several factors have been identified to impair cognitive performance in patients with trauma-related disorders, including clinical variables such as higher posttraumatic symptom severity, dissociation, and comorbidities, such as depression and anxiety (9, 11, 16–18). Moreover, sociodemographic factors showed a significant influence on cognition in PTSD, with higher age and male gender being associated with lower cognitive performance (9, 10). In addition, social support was shown to be associated with better cognition, a factor known to buffer traumatic experiences and to protect against the development of posttraumatic stress (19, 20). However, most studies on cognition in trauma patients have not differentiated between cPTSD and ncPTSD, potentially resulting in heterogeneous populations varying in posttraumatic symptom profiles.
To our knowledge, only a few studies have investigated the differences between patients with cPTSD and ncPTSD regarding cognitive performance. Shin et al. (2021) investigated emotional perception, visual attention, and working memory in adolescents with cPTSD or ncPTSD (21). They found that the cPTSD group had more deficits in all cognitive functions when compared to the ncPTSD group. In addition, the cognitive test results in emotional perception, visual attention, and working memory correlated with the severity of cPTSD symptoms. Biscoe et al. (2024) examined executive functioning in veterans with cPTSD and ncPTSD (22). Their results showed an association between cognitive impairments and DSO symptoms. As these studies examined only a few, isolated cognitive functions in specific samples (i.e., adolescents and veterans), we aimed to explore a broad range of cognitive domains in patients with cPTSD compared to patients with ncPTSD. Further, we sought to examine potential influencing factors regarding cognitive functioning. We used a comprehensive and validated test set to assess cognitive functioning. This test set offers a standardized norm sample, allowing the comparison of the cognitive performance of patients with cPTSD and ncPTSD with a representative sample (23).
Considering previous research findings of cognitive functioning in trauma-exposed patients (9–14) as well as the studies on specific cognitive impairments in cPTSD (21, 22), we hypothesized that patients with cPTSD display more severe impairment in the cognitive domains of attention, memory, and executive function, compared to patients with ncPTSD. Regarding factors influencing cognitive impairments in trauma patients (cPTSD and ncPTSD), we hypothesized that symptom severity, age, gender, the presence of depression, anxiety, and dissociation are negatively associated with cognitive performance, whereas the presence of social support is positively associated with cognitive performance.
2 Methods
2.1 Participants and procedure
This study was conducted at the University Hospital in Heidelberg, Germany, from June 2021 to November 2023. German-speaking patients of the psychotraumatology outpatient clinic of at least 18 years of age with a clinical diagnosis of cPTSD or ncPTSD were informed about the study by telephone. In addition, patients were recruited via press coverage and flyers at psychotherapists’ practices. Exclusion criteria were severe psychiatric comorbidities, such as psychosis, bipolar disorder, or substance dependence as well as histories of neurological disorders or traumatic brain injury.
The recruitment process (Figure 1) involved a three-stage assessment to clinically confirm PTSD diagnosis and differentiate between cPTSD and ncPTSD. (1.) Individuals clinically diagnosed with cPTSD or ncPTSD (N = 226) were invited to participate. Of these, n = 117 accepted the invitation, resulting in a response rate of 52%. (2.) The PTSD section of the Structured Clinical Interview for DSM-IV for Axis 1 (SCID-I, 24) ensured the current presence of the diagnosis, and, (3.) using the International Trauma Questionnaire (ITQ, 25), group allocation was defined. N = 64 participants met diagnostic criteria for cPTSD (n = 34) or ncPTSD (n = 30) and were included in the analysis.
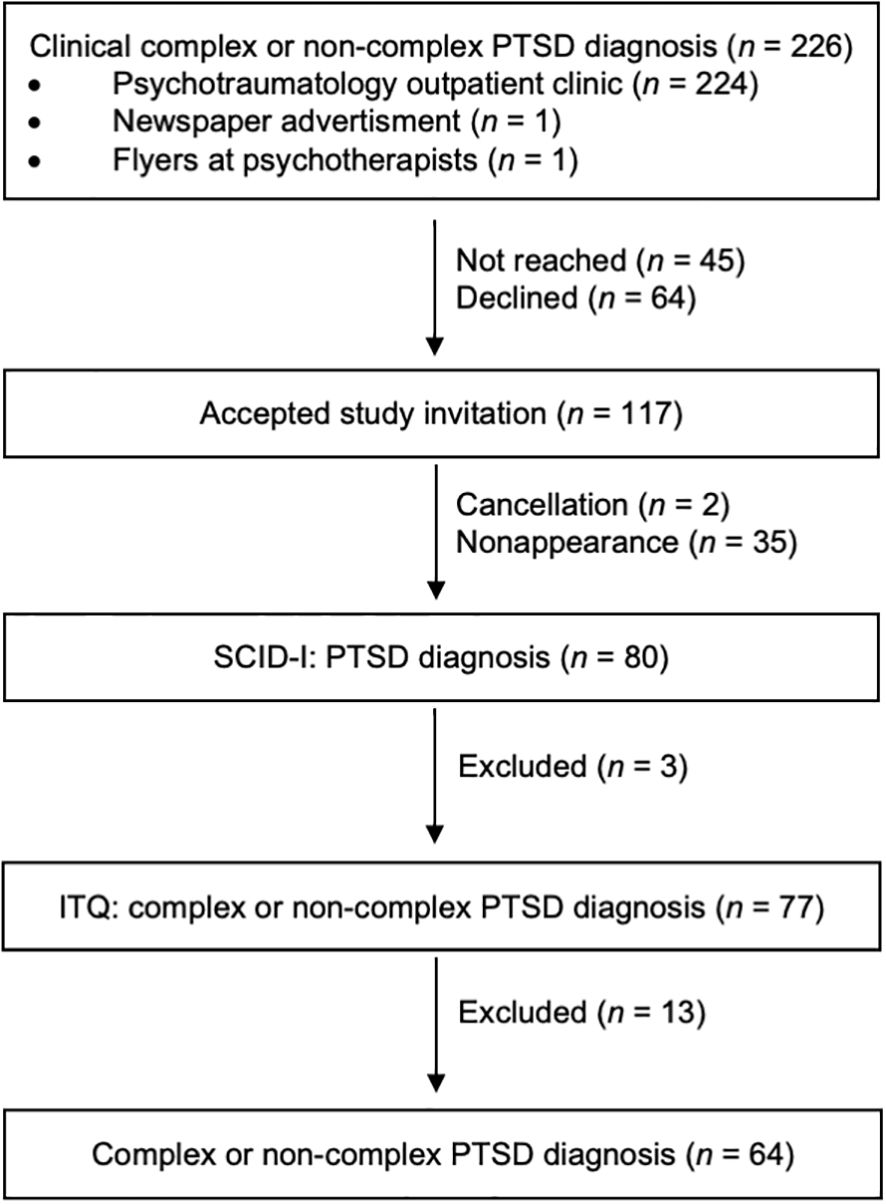
Figure 1. Flow diagram of recruitment and three stages of diagnostic process. PTSD, posttraumatic stress disorder, SCID-I, Structured Clinical Interview for DSM-IV (24), ITQ, International Trauma Questionnaire (25).
After agreeing to participate, patients received the study material by post, including an information letter about the study, the written consent form, and the psychometric questionnaires. After, the in-person assessment was conducted, using the SCID-I, the Multiple Choice Vocabulary Test (MWT-B, 26), and the Cognitive Basic Assessment test set (COGBAT, 27). An overview of the assessment material is shown in Table 1. The study duration was a maximum of three hours. For compensation, participants received 20 euros.
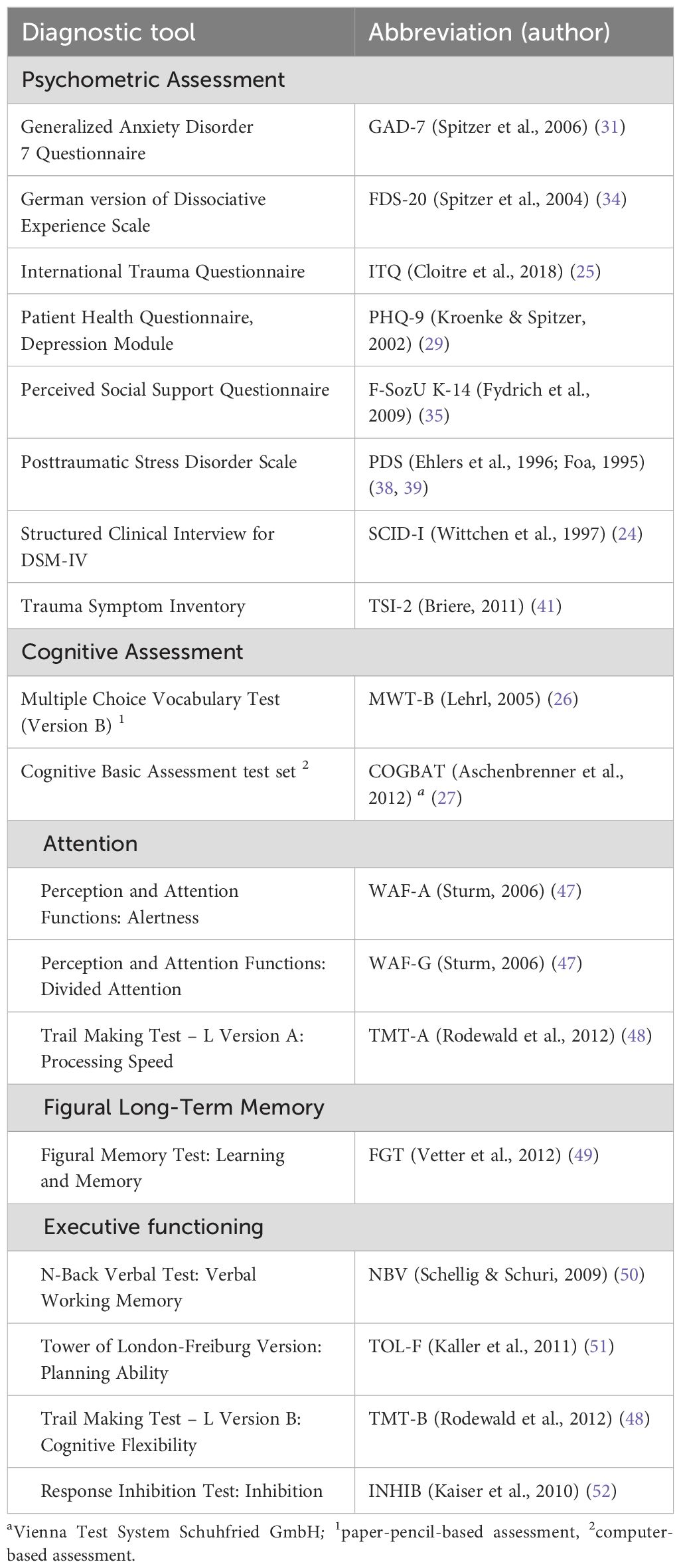
Table 1. Assessment material.
2.2 Ethics approval and consent to participate
The study protocol was developed according to the Helsinki II declaration (28). The Ethics Committee of the Medical Faculty of the University of Heidelberg approved the study under file number S-210/2020. Written informed consent was obtained from all study participants.
2.3 Measures
2.3.1 Psychometric assessment
Depression was assessed with the Patient Health Questionnaire, Depression Module (PHQ-9, 29) of the German version of the Patient Health Questionnaire (PHQ-D, 30). To measure anxiety, we used the German version of the anxiety module Generalized Anxiety Disorder 7 (GAD-7, 31) of the PHQ-D. German translations of the PHQ-9 and GAD-7 showed good internal consistency with Cronbach´s α = .85-.88 (32, 33). Dissociative symptoms were assessed using the FDS-20, the German translation and shortened screening version of the Dissociative Experience Scale, which showed good to excellent internal consistency with Cronbach´s α = .89-.93 (34). To evaluate perceived social support, we used the German questionnaire F-SozU K-14 with excellent internal consistency (Cronbach`s α = .94) (35).
As previously mentioned, we used the German version of the ITQ (25) for group assignment in order to differentiate between cPTSD and ncPTSD. The first section focuses on the three core symptoms of PTSD, with two items used to evaluate each symptom. Participants rate how severely they have been affected by the symptoms in the last month. The second section measures disturbances in self-organization (DSO) symptoms, consisting of three symptom domains (negative self-concept, interpersonal problems, and affective dysregulation). Participants answer the DSO items regarding how much these apply to them or their interactions with others in the past month. In addition, there are three questions on functional impairment in important areas of life for the PTSD and DSO sections. A diagnosis of ncPTSD requires a score of two or higher in at least one item of each PTSD symptom domain and functional impairment. A diagnosis of cPTSD requires fulfillment of the ncPTSD criteria and a score of two or higher on at least one item in each DSO symptom domain and functional impairment. The ITQ has satisfactory to excellent internal consistency (Cronbach’s α = .63 -.93) (6, 36, 37).
The Posttraumatic Stress Disorder Scale (PDS) is a screening instrument for the presence of PTSD according to the diagnostic criteria of the DSM-IV. We used the German translation (38, 39). In the present study, it was used to assess classic PTSD symptoms (re-experience, avoidance, and hyperarousal), in particular symptom severity. We used the list of traumatic events, or in cases of multiple traumas, the most distressing one, to determine the type of trauma. The PDS has excellent internal consistency with Cronbach’s α = .92 (40). In addition, the German version of the Trauma Symptom Inventory (TSI-2, 41) was administered to assess a broad range of posttraumatic symptoms with 136 items. Moreover, TSI-2 was applied to measure symptoms of the DSO cluster, using the following TSI-2 scales: inadequate self-reference to determine the negative self-image, insecure attachment to assess interpersonal problems, and the mean value of the scales depression, dissociation, anger, and tension reduction behavior to assess affect dysregulation (42). Most scales of the TSI-2 have an acceptable to excellent internal consistency (Cronbach’s α = .62 -.95) (43).
2.3.2 Cognitive testing
The MWT-B (26), a German questionnaire, was administered to control for premorbid intelligence deficits. It consists of 37 items, each containing five words, including four nonsense words. Participants are asked to cross out the word that exists in the German language for each item. The test results correlate strongly with the IQ of healthy adults (44). For a comprehensive evaluation of cognitive dimensions (i.e., attention, memory, and executive function), we used the German version COGBAT of the Vienna test system of Schuhfried GmbH (27). The COGBAT consists of six standardized tests administered on a computer using a mouse and a special keyboard lasting approximately 60 minutes. The norm sample consists of N = 419 people aged 16 to 80 years and allows a comparison with specific norms. The test battery has been validated in different populations (45, 46). The internal consistencies of Cronbach’s α >.70 are acceptable to excellent for all tests (23). The variables were selected based on the standard results protocol and COGBAT manual. The COGBAT tests employed in this study include the following:
Attention: Selective attention is measured using the test for Perception and Attention Functions - Alertness (WAF-A, 47). The task is to react as fast as possible to a presented stimulus. Divided attention is measured using the Perception and Attention Functions - Divided Attention (WAF-G, 47). The participants are presented with visual (squares) and auditory (sounds) stimuli simultaneously. They are asked to press a button if any type of stimulus changes twice in a row. Processing speed is measured using the Trail Making Test – Part A (TMT-A, 48) by connecting numbers as fast as possible in ascending order.
Visual memory: Visual learning and memory are measured using the Figural Memory Test (FGT, 49). Figures are presented in a learning phase for five consecutive times. This is followed by a short-term delayed (5-minute interval) and long-term delayed (30-minute interval) recall. Lastly, a recognition phase follows, in which the previously learned figures need to be discriminated from similar, but unknown figures.
Executive functioning: Verbal working memory is assessed using the N-Back Verbal Test (NBV, 50), wherein letters are presented one after the other in a 2-back paradigm. Planning ability is measured using the Tower of London-Freiburg Version test (TOL-F, 51). Participants are asked to rearrange three different colored balls to match a presented target state using the fewest possible steps, adhering to predetermined rules. Points are given for the correct solution achieved with the minimum number of steps within a 60-second time frame. The Trail Making Test – Part B (TMT-B, 48) assesses cognitive flexibility by connecting numbers and letters in alternating ascending order as fast as possible. Response inhibition is assessed using the Response Inhibition Test (INHIB, 52) using a Go-NoGo-paradigm.
2.4 Statistical analysis
The data were analyzed using the “Statistical Package of Social Sciences” (SPSS; IBM SPSS Statistics for Macintosh, Version 29.0) (53). A power analysis was performed a priori with G*Power (version 3.1) (54) to estimate the sample size. In previous research, effect sizes on cognitive impairments in PTSD were dependent on the control group and the domain (10). No prior effect sizes were found for differences in cognition between cPTSD and ncPTSD. For a t‐test (one‐tailed) for two independent samples with an effect size of d = 0.70 (α = 0.05, power = 0.80, allocation ratio N2/N1 = 1), a total sample size of N = 52 was needed. Therefore, the current study has the power to detect large effect sizes.
The sociodemographic and psychometric parameters of the cPTSD and ncPTSD groups are presented using descriptive statistics. Group differences (cPTSD vs. ncPTSD) were tested for significance using student t-tests for independent samples or χ2-tests. For descriptive analyses, p-values of <.05 (one-tailed) were considered statistically significant.
To assess objective cognitive impairment of cPTSD and ncPTSD, we used percentile ranks comparing cognitive scores to a representative, healthy COGBAT norm sample based on age (16-30 years n = 127, 31-50 years n = 151, 51-80 years n = 141) (23). For the group comparison between cPTSD and ncPTSD concerning cognitive functioning, the raw scores of each individual were converted into standardized z-scores. If necessary, scores were inverted for higher scores describing better cognitive performance. A group comparison was performed using student t-tests for independent samples. First, we tested the composite scores for each domain (attention, visual memory, and executive functioning), with the subdomains also being analyzed if the domain scores were not significantly different. Bonferroni correction was applied on one-tailed p values to minimize Type I errors (11-test family, corrected p <.005). ANCOVAs were performed to control for the covariate medication. Additionally, we calculated bivariate regression analyses for cognitive functions with significant group differences between cPTSD and ncPTSD with all explanatory variables. Bonferroni correction was applied on one-tailed p values (12-test family, corrected p <.004). Lastly, we performed multivariate linear regressions to investigate predictors of cognitive impairment (i.e. PTSD type, age, cPTSD symptoms, PTSD symptoms, depression, anxiety, dissociation, and social support).
3 Results
3.1 Demographic and clinical assessment
Table 2 shows the participants’ sociodemographic and clinical characteristics. The age range in the cPTSD group was 20 - 65 years (median = 43.50, IQR = 25.25). In the ncPTSD group, age ranged from 20 to 67 years (median = 33.50, IQR = 32.50). In both groups, most participants were female. The groups did not differ significantly in age, gender distribution, or premorbid intelligence level. Individuals in the cPTSD group reported to have children (p = .041; cPTSD: M = 1.24 children (SD = 1.33) more often than the ncPTSD group: M = 0.70 children (SD = 1.06)). No significant differences were observed between groups in other sociodemographic or clinical variables. Regarding the type of trauma, in the cPTSD group, n = 4 had experienced an accident, n = 4 violence, n = 15 sexual assault, n = 1 war, and n = 1 a life-threatening illness; n = 9 reported other traumatic experiences. In the ncPTSD group, n = 6 individuals had experienced an accident, n = 1 a natural disaster, n = 10 violence, n = 2 sexual assault, n = 1 captivity, n = 1 a life-threatening illness, and n = 9 other traumatic events.
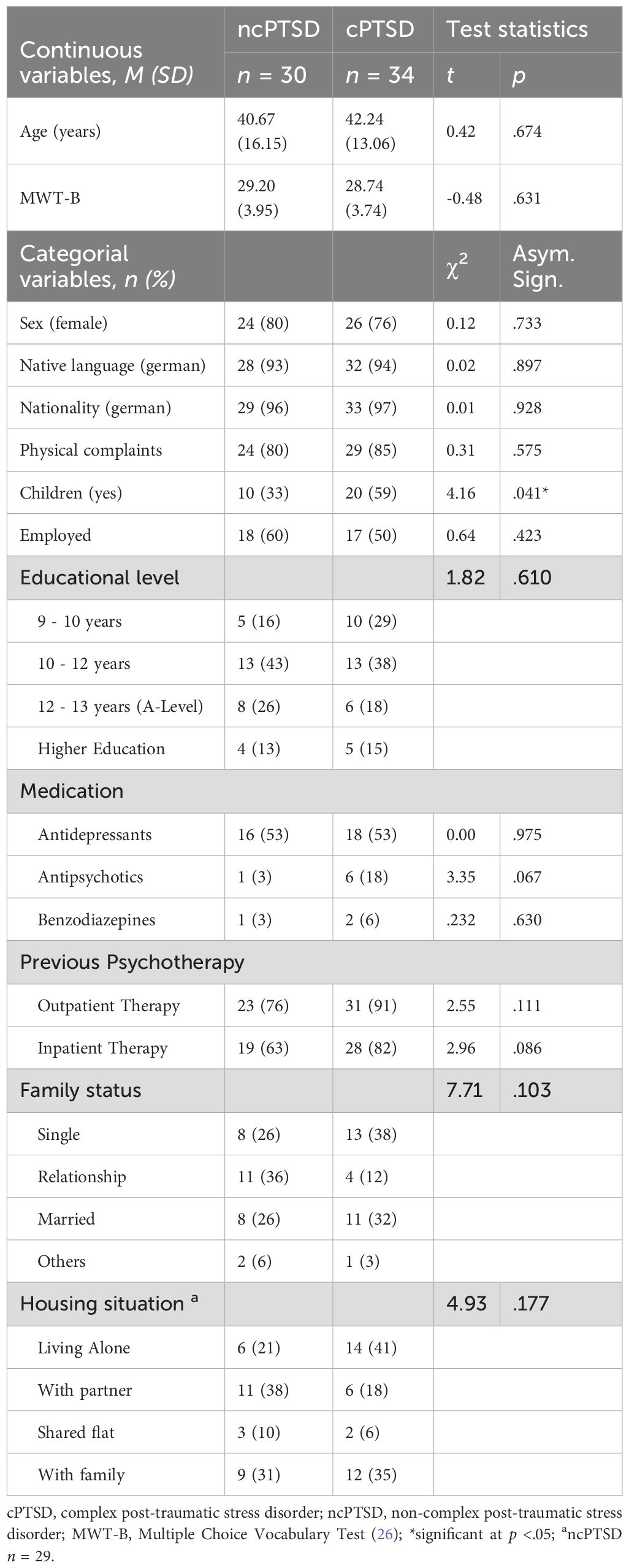
Table 2. Sociodemographic and clinical assessment of cPTSD and ncPTSD group.
3.2 Psychometric assessment
The mean and standard deviations of self-reported psychometric assessment are shown in Table 3. The severity of symptoms was significantly higher in cPTSD group than in the ncPTSD group regarding the following domains with medium to large effect sizes: PTSD symptom sum score (ITQ) (d = 0.58), DSO symptoms sum score (ITQ) (d = 2.05), PTSD symptom severity (PDS) (d = 0.90), cPTSD symptom severity (TSI) (d = 1.06), dissociation (FDS-20) (d = 0.87), depression (PHQ-9) (d = 1.29), anxiety (GAD-7) (d = 0.62), depression (TSI) (d = 1.02), dissociation (TSI) (d = 0.85), somatic preoccupations (TSI) (d = 0.66), sexual disturbances (TSI) (d = 0.69), suicidality (TSI) (d = 1.22), insecure attachment (TSI) (d = 0.82), impaired self-reference (TSI) (d = 0.94), tension reduction behavior (TSI) (d = 0.76), the factor somatization (d = 0.63), self-disturbance (d = 1.06), posttraumatic stress (d = 0.66), and externalization (TSI) (d = 0.95). A significant difference with a small effect size was found for anxious arousal (TSI) (d = 0.44), defensive avoidance (d = 0.44), with a higher score in the cPTSD group (all p <.05). Moreover, the cPTSD group showed significantly less social support (FSozU K-14) with a medium effect size (d = -0.76, p <.05). No significant group differences were found for PTSD symptoms sum score (ITQ), anxiety (GAD-7), somatic preoccupations (TSI), anxious arousal (TSI), anger (TSI), intrusive experiences (TSI), defensive avoidance (TSI), and factors of somatization and posttraumatic stress (TSI).
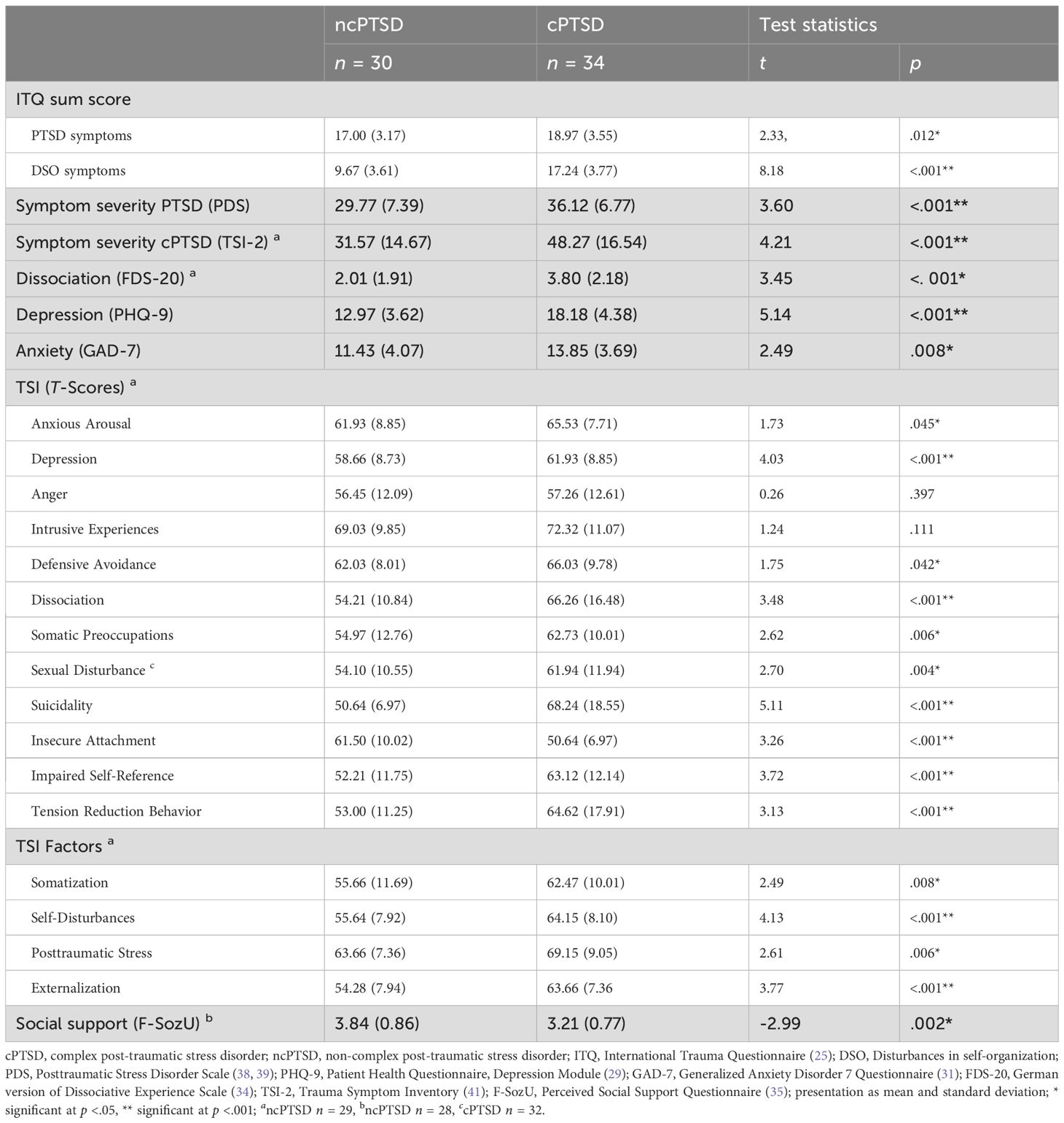
Table 3. Psychometric assessment of cPTSD and ncPTSD group.
3.3 Cognitive assessment
Table 4 presents percentile ranks of cognitive performance on a dimensional level for the cPTSD and ncPTSD groups compared to an age-matched comparison group derived from the representative norm sample of the COGBAT. Across all domains, the cPTSD group remained below the 16th percentile in 21 – 44% of the test scores, whereas the ncPTSD group remained below the 16th percentile in 7 – 14% of the test scores, indicating significant cognitive impairment in both patient groups compared to the norm sample.
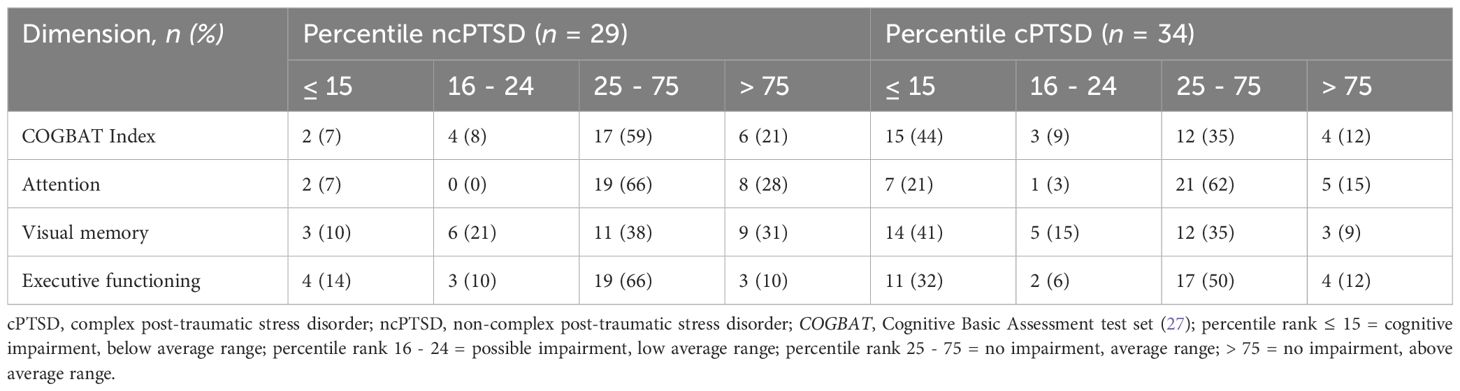
Table 4. Neuropsychological assessment: Percentile ranks of cPTSD and ncPTSD group compared to an age-matched COGBAT norm sample.
Table 5 shows the comparison of COGBAT scores for the cPTSD and the ncPTSD group. Significant differences with medium effect sizes were found for visual memory (d = -0.73) on a cognitive domain level, showing lower cognitive performance in the cPTSD group. The groups did not significantly differ in executive functioning or attention domains. On a subdomain level, a significant difference between groups with medium effect sizes was found in selective attention (reaction time) (d = -0.70), with lower cognitive performance of cPTSD group. No significant group differences were found for working memory, planning ability, cognitive flexibility, inhibition, and divided attention (mean reaction time). After adjusting for medication, results on visual memory and selective attention remained significant.
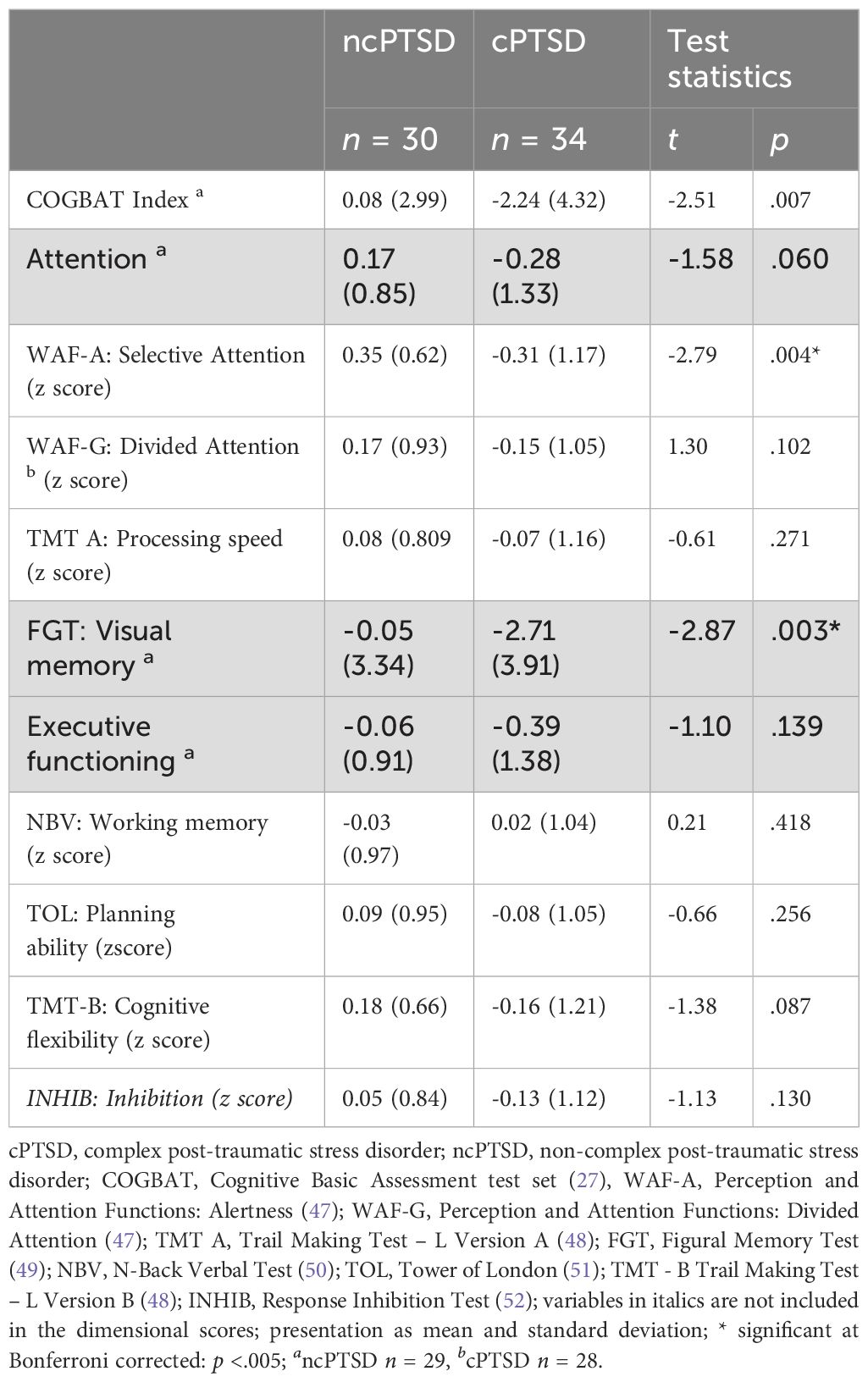
Table 5. Neuropsychological assessment: Dimensional scores and test scores of complex post-traumatic stress disorder (cPTSD) and non-complex post-traumatic stress disorder (ncPTSD) group.
3.4 Influencing factors of cognitive impairments
Table 6 shows bivariate regressions for selective attention and visual memory with type of PTSD (cPTSD vs. ncPTSD), age, gender, cPTSD symptoms, PTSD symptoms, depression, anxiety, dissociation, and social support. In the bivariate regressions, after Bonferroni correction, higher age (β = -548, p <.001) was the only factor to remain significant, being associated with lower performance in visual memory.
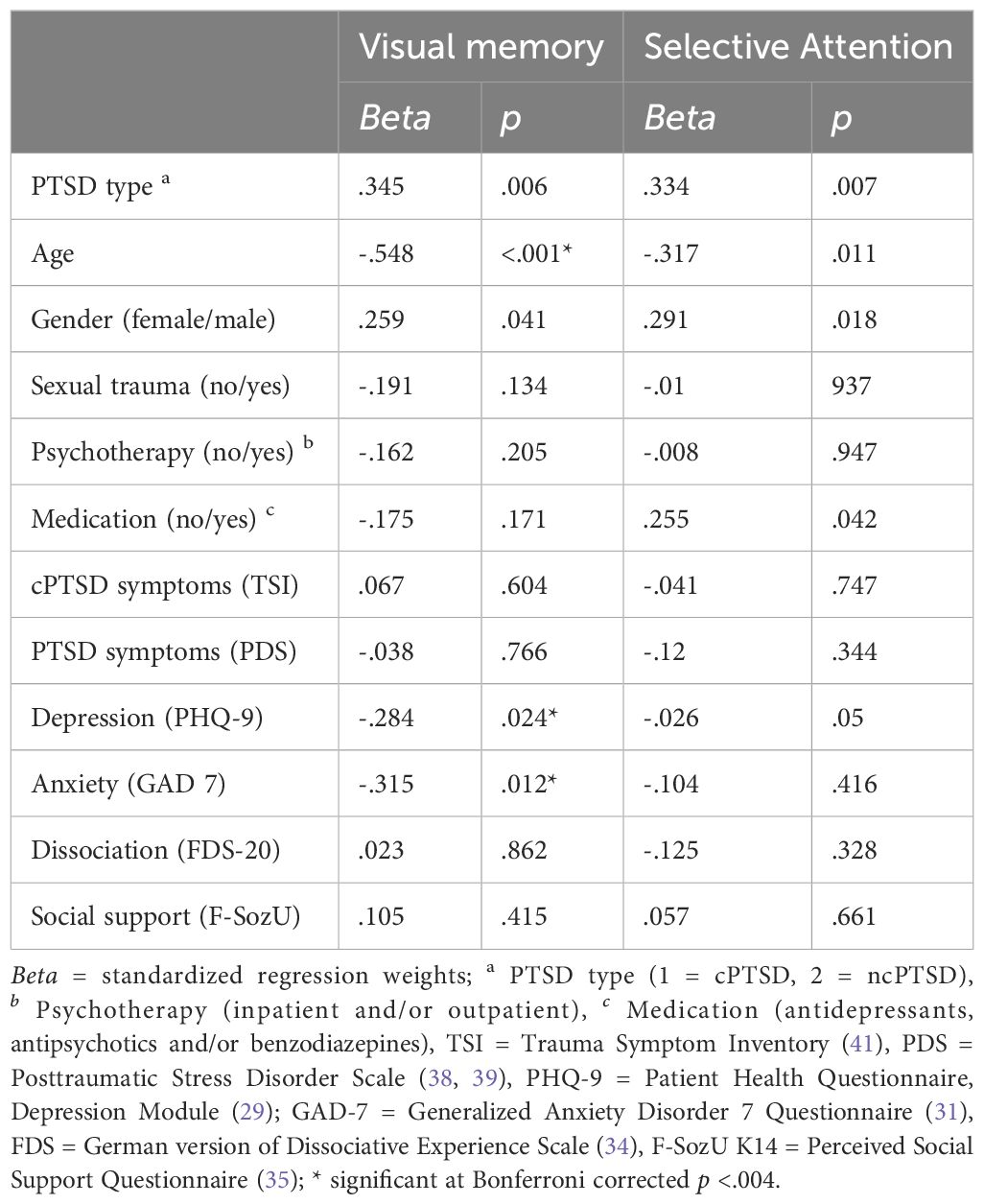
Table 6. Bivariate regressions of cognitive impairments.
Table 7 shows the results of multivariable omnibus regression. For the visual memory, the model explains 54.1% of the variance (R2 = 54.1, adj. R2 = 42.9, F (8, 53) = 4.82, p <.001), with cPTSD group (β = .313, p = .021) and age (β = -.459, p <.001) negatively influencing cognitive performance. For selective attention, the model explains 40.5% (R2 = 40.5, adj. R2 = 25.9, F (8, 53) = 2.78, p = .006) of the variance, with cPTSD group (β = .302, p = .049), age (β = -.321, p =.022) negatively influencing cognitive performance and psychotropic medication (β = .298, p = .018) positively influencing selective attention.
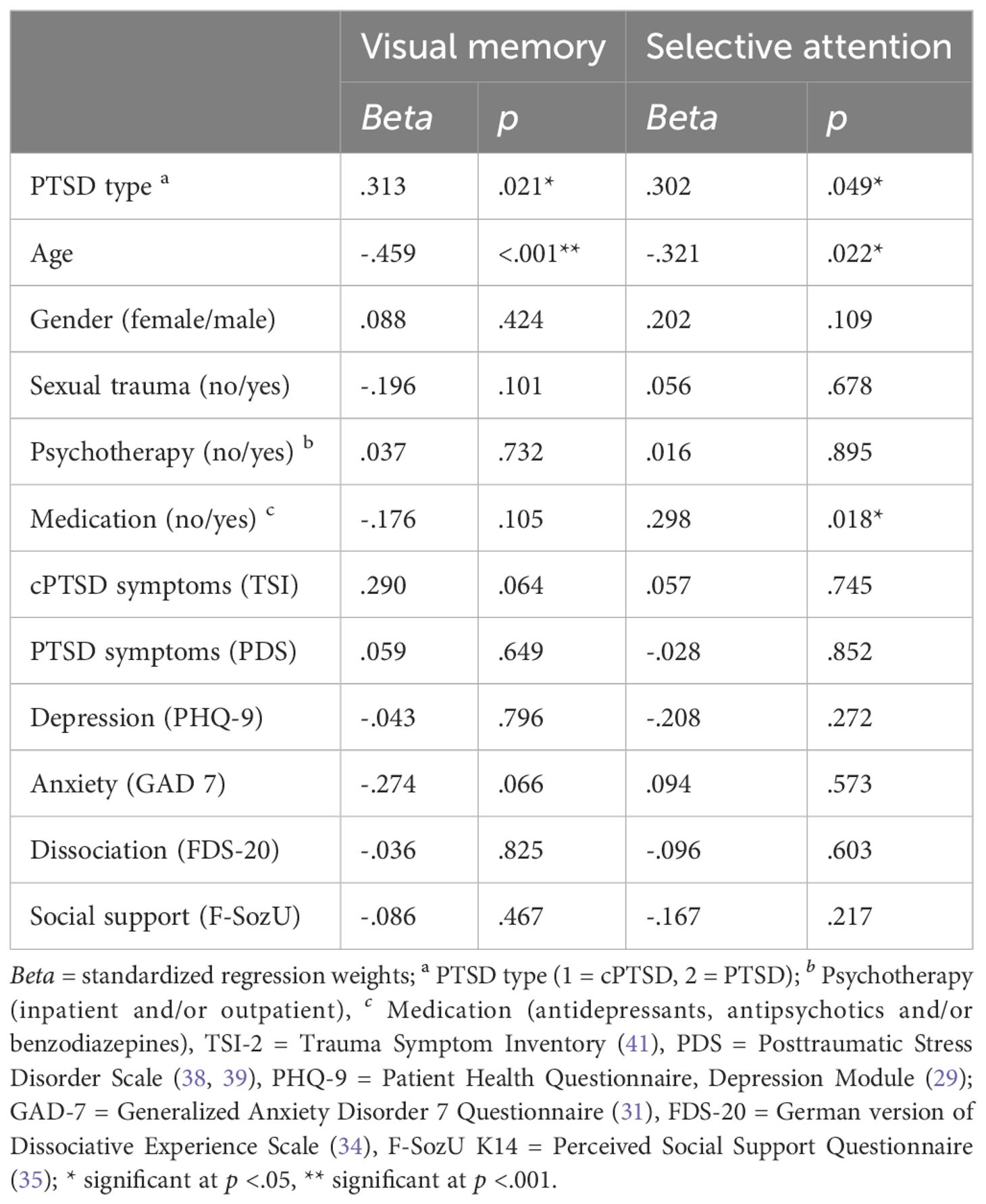
Table 7. Multiple regressions of cognitive impairments.
4 Discussion
The present study examined cognitive functioning in patients with cPTSD and ncPTSD using a three-stage diagnostic process and a standardized neuropsychological test set. In general, both patient groups showed objective cognitive impairment compared to a healthy norm sample. The cPTSD group performed significantly worse in the cognitive testing than the ncPTSD group, particularly in selective attention and visual memory. Moreover, age and type of PTSD (cPTSD vs. ncPTSD) were identified to be associated with cognitive performance in patients suffering from posttraumatic stress.
4.1 Symptom profiles in cPTSD and ncPTSD
With regard to the classic PTSD symptoms of re-experience, avoidance, and hyperarousal, the results of the group comparison showed a significant difference, with a higher symptom load in the cPTSD group. Further analysis of posttraumatic symptoms applying the TSI showed that cPTSD patients displayed significantly higher levels of defensive avoidance, somatic preoccupations, sexual disturbance, suicidality, insecure attachment, greater impairments in self-reference, and more frequent use of tension reduction behavior. These results are in line with previous findings, indicating that patients with cPTSD exhibit a generally higher symptom load compared to ncPTSD (1, 5, 55, 56). Furthermore, our findings were consistent with previous studies, demonstrating that patients with cPTSD suffer from higher depressive symptom severity (36, 57), more severe dissociation (58, 59), and report less social support (60). We did find a significant group difference in anxiety symptoms. Even though cPTSD was associated with higher levels of anxiety in a large sample of a study by Karatzias et al. (2019) (57), recent studies with comparable sample sizes to our study did not find significant differences in anxiety between cPTSD and ncPTSD (21, 61). Concerning our finding of higher symptom severity in cPTSD, it can be assumed that cPTSD may generally be associated with disruptions in essential psychological capacities, e.g. coping strategies, some of which manifest in DSO symptoms (1). These disruptions, in turn, may complicate the processing of comorbid symptomatology like depression or dissociation, resulting in higher symptom severity for patients with cPTSD. Regarding type of trauma, the majority of cPTSD patients (44%) reported sexual assault as their most distressing trauma, compared to only 0.6% in the ncPTSD group. This is in line with previous research that showed that interpersonal trauma, especially sexual assault, is strongly associated with psychological dysfunction in general and with a higher risk to result in PTSD than non-interpersonal trauma (62–64).
4.2 Cognitive impairments in cPTSD and ncPTSD
In our study, norm group comparison indicated that both patient groups showed cognitive impairments in all cognitive domains. Specifically, in the domain of visual memory, we observed significant group differences, indicating lower cognitive performance of the cPTSD group compared to the ncPTSD group. In addition to studies showing verbal memory deficits in patients with PTSD (13, 14), further studies found impaired non-verbal memory to be linked with PTSD (65–67). Our findings align with prior research, demonstrating that higher PTSD symptom load is associated with worse performance in visual memory (66). Previous studies discussed reduced hippocampal volume as a possible reason for these impairments in memory (65). The underlying assumption is that stress induces changes in the hippocampus, which results in a reduced volume. Consequently, the severe traumatic experiences and higher symptom burden linked to cPTSD could lead to greater stress levels, thereby contributing to more pronounced reductions in hippocampal volume and, subsequently, more significant impairments in memory functions. In addition, previous studies found that early life stress in particular is associated with lower hippocampal volume (68). As cPTSD is often associated with trauma in early childhood (1, 55, 61), cognitive impairments in learning and memory in cPTSD may be the result of reduced hippocampal volume due to trauma experienced during childhood. Regarding this assumption, a previous study already highlighted the need to empirically compare cognitive profiles of cPTSD patients with and without childhood trauma for future research (69). These more severe memory impairments in patients with cPTSD are highly relevant, as previous studies were able to demonstrate that learning and memory deficits in patients with PTSD are associated with problems in everyday life and therapy (70). For example, memory deficits in PTSD were a predictor for problems in social and occupational functioning (65). Moreover, pre-treatment learning and memory performance can predict treatment outcomes in PTSD, which was particularly important for verbal memory (71–73). Haaland et al. (2016) suggest interventions to improve learning and memory before therapy (72).
Concerning the cognitive domain of attention, we found significant group differences in selective attention, with slower reaction times in the cPTSD group. This is in line with previous research that revealed greater impairments of attention in cPTSD compared to ncPTSD with an association with symptom severity (21). Based on previous cognitive models of PTSD, these attentional deficits may be the consequence of a “shift” in information processing capacities toward the search and recognition of potentially threat-related stimuli, causing a focus on the traumatic experience and a reinforcement of PTSD symptoms (15, 74, 75). The heightened attentional focus on threat-related stimuli is assumed to be established at the expense of attention on other stimuli and the expense of other cognitive domains (11, 15). Thus, greater impaired attention in cPTSD may be associated with greater impairments in other domains of cognition, such as memory. Moreover, addressing the attentional bias toward threat stimuli, e.g. by applying attention control training, was shown to reduce PTSD symptoms (76).
Contrary to our expectations and prior studies, no significant group differences in cognitive functioning were observed between patients with cPTSD and ncPTSD with regard to executive functioning and the attentional subdomains of divided attention and processing speed. In particular, complex trauma, often involving repeated interpersonal threats in the early stages of life, was previously associated with impaired executive functioning and processing speed (77). A study investigating patients with a history of parental abuse revealed that the patients with cPTSD performed significantly worse in working memory, a subdomain of executive functioning, than those with ncPTSD (21). However, a recent study investigating a sample of veterans also showed more deficits in executive functioning in cPTSD compared to ncPTSD (22). Previous research demonstrated that the duration and type of trauma may influence the manifestation of posttraumatic symptoms, impacting cognitive functioning as well (11, 15). Considering these findings, the type of trauma might have differential effects on cognitive functioning in cPTSD patients, which, however, has not yet been explicitly investigated. To gain a deeper understanding of cognitive functioning in patients with cPTSD, future research should therefore consider the type of trauma as a potentially relevant variable.
4.3 Factors influencing cognitive impairment
We identified a higher age to be significantly associated with impairments in visual memory and selective attention of trauma patients. Previous research in trauma patients has already identified the variable age to be negatively associated with cognitive performance (9, 78). This may be attributed to age in general being accompanied by cognitive decline (79) or to the duration of PTSD symptoms (9). In a longitudinal study on cognitive performance in older patients with PTSD, Yehuda et al. (2006) found that aging, trauma exposure, and PTSD symptom severity may have differential effects on memory performance (78).
Analyzing the variables in one model, the type of PTSD (cPTSD vs. ncPTSD) was identified to be a predictor of cognitive performance in visual memory and selective attention. This outcome is not surprising, given that we selected variables for regression analysis based on the presence of significant group differences. However, the lack of significant influence from comorbidities in this model suggests that it is not the individual variables but rather the interplay of different factors being associated with cognitive impairment in patients suffering from posttraumatic stress. Additionally, psychotropic medication was found to be associated with better performance in selective attention in our model. Previous research has shown mixed results regarding the impact of psychotropic medication on cognition. While antidepressants may positively influence certain cognitive domains, such as psychomotor speed and delayed recall (80), other studies found a negative effect of psychotropic medication on cognitive functioning. For instance, psychotropic medication has been associated with lower overall cognitive function and working memory (81), and benzodiazepine use has been linked to cognitive deficits (82). To get a better understanding of these effects, future research on cognition in PTSD should further consider specific types of medication, including dosage and duration of intake.
5 Limitations
An important limitation of the study is that its statistical power is sufficient to detect large effect sizes. However, based on previous research, medium effect sizes may also be hypothesized in comparing cognitive functioning in trauma patients (10). Another limitation is that the study population was homogenous in terms of gender, nationality, and type of trauma limiting the generalizability of the study results. The participants were mainly female and of German nationality, with various other forms of trauma, such as war-related trauma, remaining underrepresented. Furthermore, a limitation can be considered in the study’s cross-sectional design limiting the generalizability of our findings regarding possible longitudinal variable changes. Moreover, this research shares limitations with other studies on cognitive functioning in trauma patients concerning the possibility of earlier alcohol, drug, or medication abuse that was not reported by the participants and may have affected cognitive performance (65, 67, 83). Moreover, studies indicate that PTSD treatment might affect cognition. For example psychotherapy such as cognitive behavioral therapy has been associated with improvement in memory function (71). The majority of our participants had received psychotherapy (cPTSD 94%, ncPTSD 83%), resulting in a relatively homogeneous group in terms of treatment exposure. It would be interesting in future studies to compare groups with and without prior psychotherapy to explore differences in cognitive outcomes. Another limitation of the present study is that the regression analysis only considered a selection of possible variables. Our choice was made based on existing literature, but other factors may also influence cognitive impairment in trauma patients.
6 Conclusion
The finding of differences in cognitive functioning between cPTSD and ncPTSD diversifies our understanding of the multifaceted symptomatology that may result from trauma. Based on the result that cPTSD patients displayed a higher symptom burden and more pronounced cognitive deficits, especially in visual memory and selective attention, more intense and comprehensive interventions may prove to be beneficial for treatment. As cognitive functioning plays an important role in processing traumatic memories and engaging in therapeutic processes, cognitive training should be implemented as part of a comprehensive treatment plan.
Data availability statement
The datasets presented in this study can be found in heiDATA, https://doi.org/10.11588/data/B3HNSQ.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Medical Faculty of the University of Heidelberg. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Z-SS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. VT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. AJ: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. DR-E: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. H-CF: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. CN: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. DK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Open Access funding enabled and organized by “Projekt DEAL”. For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten” as well as by Heidelberg University.
Acknowledgments
We thank Molly Sutcliffe for English language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Maercker A, Cloitre M, Bachem R, Schlumpf YR, Khoury B, Hitchcock C, et al. Complex post-traumatic stress disorder. Lancet. (2022) 400:60–72. doi: 10.1016/S0140-6736(22)00821-2
2. World Health Organization. International Statistical Classification of Diseases and Related Health Problems. 11th ed. Geneva: World Health Organization (2018). Available at: https://icd.who.int/en.
3. American Psychiatric Association. Diagnostic and statistical Manual of Mental Disorders. Fifth Edition. American Psychiatric Association (2013).
4. Brewin CR, Cloitre M, Hyland P, Shevlin M, Maercker A, Bryant RA, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clin Psychol Rev. (2017) 58:1–15. doi: 10.1016/j.cpr.2017.09.001
5. Perkonigg A, Höfler M, Cloitre M, Wittchen HU, Trautmann S, Maercker A. Evidence for two different ICD-11 posttraumatic stress disorders in a community sample of adolescents and young adults. Eur Arch Psychiatry Clin Neurosci. (2016) 266:317–28. doi: 10.1007/s00406-015-0639-4
6. Karatzias T, Cloitre M, Maercker A, Kazlauskas E, Shevlin M, Hyland P, et al. PTSD and Complex PTSD: ICD-11 updates on concept and measurement in the UK, USA, Germany and Lithuania. Eur J Psychotraumatol. (2017) 8:1418103. doi: 10.1080/20008198.2017.1418103
7. Kindermann D, Nikendei C. Traumafolgestörungen und psychosoziale Versorgung bei Geflüchteten in der frühen postmigratorischen Phase. In: Sack M, Sachsse U, Schellong J, editors. Komplexe Traumafolgestörungen, 2 Auflage: Diagnostik und Behandlung von Folgen schwerer Gewalt und Vernachlässigung. Schattauer, Stuttgart (2022). p. 511–7.
8. Maercker A, Hecker T, Augsburger M, Kliem S. ICD-11 prevalence rates of posttraumatic stress disorder and complex posttraumatic stress disorder in a german nationwide sample. J Nerv Ment Dis. (2018) 206:270–6. doi: 10.1097/NMD.0000000000000790
9. Polak AR, Witteveen AB, Reitsma JB, Olff M. The role of executive function in posttraumatic stress disorder: a systematic review. J Affect Disord. (2012) 141:11–21. doi: 10.1016/j.jad.2012.01.001
10. Scott JC, Matt GE, Wrocklage KM, Crnich C, Jordan J, Southwick SM, et al. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol Bull. (2015) 141:105–40. doi: 10.1037/a0038039
11. Twamley EW, Allard CB, Thorp SR, Norman SB, Cissell SH, Berardi KH, et al. Cognitive impairment and functioning in PTSD related to intimate partner violence. J Int Neuropsychol Society. (2009) 15:879–87. doi: 10.1017/S135561770999049X
12. Aupperle RL, Melrose AJ, Stein MB, Paulus MP. Executive function and PTSD: disengaging from trauma. Neuropharmacology. (2012) 62:686–94. doi: 10.1016/j.neuropharm.2011.02.008
13. Brewin CR, Kleiner JS, Vasterling JJ, Field AP. Memory for emotionally neutral information in posttraumatic stress disorder: A meta-analytic investigation. J Abnorm Psychol. (2007) 116:448–63. doi: 10.1037/0021-843X.116.3.448
14. Johnsen GE, Asbjørnsen AE. Consistent impaired verbal memory in PTSD: a meta-analysis. J Affect Disord. (2008) 111:74–82. doi: 10.1016/j.jad.2008.02.007
15. Block SR, Liberzon I. Attentional processes in posttraumatic stress disorder and the associated changes in neural functioning. Exp Neurology. (2016) 284:153–67. doi: 10.1016/j.expneurol.2016.05.009
16. Olff M, Polak AR, Witteveen AB, Denys D. Executive function in posttraumatic stress disorder (PTSD) and the influence of comorbid depression. Neurobiol Learn Memory. (2014) 112:114–21. doi: 10.1016/j.nlm.2014.01.003
17. Nijdam MJ, Gersons BP, Olff M. The role of major depression in neurocognitive functioning in patients with posttraumatic stress disorder. Eur J Psychotraumatology. (2013) 4:19979. doi: 10.3402/ejpt.v4i0.19979
18. Gkintoni E, Ortiz PS. Neuropsychology of generalized anxiety disorder in clinical setting: A systematic evaluation. Healthcare. (2023) 11:2446. doi: 10.3390/healthcare11172446
19. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol. (2000) 68:748–66. doi: 10.1037/0022-006X.68.5.748
20. Costa-Cordella S, Arevalo-Romero C, Parada FJ, Rossi A. Social support and cognition: a systematic review. Front Psychol. (2021) 12:637060. doi: 10.3389/fpsyg.2021.637060
21. Shin YJ, Kim SM, Hong JS, Han DH. Correlations between cognitive functions and clinical symptoms in adolescents with complex post-traumatic stress disorder. Front Public Health. (2021) 9:586389. doi: 10.3389/fpubh.2021.586389
22. Biscoe N, New E, Murphy D. Complex PTSD symptom clusters and executive function in UK Armed Forces veterans: a cross-sectional study. BMC Psychol. (2024) 12:209. doi: 10.1186/s40359-024-01713-w
23. Aschenbrenner S, Kaiser S, Pfüller D, Roesch-Ely D, Weisbrod M. Manual Kognitive Basistestung - Kurzbezeichnung COGBAT. Mödlingen: Schuhfried (2021). 58 p.
24. Wittchen H-U, Zaudig M, Fydrich T. Skid. In: Strukturiertes klinisches Interview für DSM-IV. Hogrefe-Verlag, Göttingen (1997).
25. Cloitre M, Shevlin M, Brewin CR, Bisson JI, Roberts NP, Maercker A, et al. The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica. (2018) 138:536–46. doi: 10.1111/acps.12956
26. Lehrl S. Mehrfachwahl-Wortschatz-Intelligenztest: MWT-B [Multiple Choice Vocabulary Test, version B]. Balingen, Germany: Spitta Verlag GmbH & Co. KG (2005).
27. Aschenbrenner S, Kaiser S, Pfüller U, Roesch-Ely D, Weisbrod M. Wiener Testsystem: Testset Kognitive Basistestung COGBAT Mödling. Schuhfried (2012).
28. Williams JR. The Declaration of Helsinki and public health. Bull World Health Organ. (2008) 86:650–2. doi: 10.2471/BLT.08.050955
29. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr annals. (2002) 32:509–15. doi: 10.3928/0048-5713-20020901-06
30. Löwe B, Spritzer RL, Zipfel S, Herzog W. PHQ-D: Gesundheitsfragebogen für Patienten (2. Auflage). Manual. Karlsruhe: Pfitzer (2002).
31. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
32. Gräfe K, Zipfel S, Herzog W, Löwe B. Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ-D). Diagnostica. (2004) 50:171–81. doi: 10.1026/0012-1924.50.4.171
33. Hinz A, Klein AM, Brähler E, Glaesmer H, Luck T, Riedel-Heller SG, et al. Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J Affect Disord. (2017) 210:338–44. doi: 10.1016/j.jad.2016.12.012
34. Spitzer C, Mestel R, Klingelhöfer J, Gänsicke M, Freyberger HJ. Screening und Veränderungsmessung dissoziativer psychopathologie: psychometrische charakteristika der Kurzform des Fragebogens zu dissoziativen Symptomen (FDS-20). Psychother Psychosom Med Psychol. (2004) 54:165–72. doi: 10.1055/s-2003-814783
35. Fydrich T, Sommer G, Tydecks S, Brähler E. Fragebogen zur sozialen unterstützung (F-SozU): Normierung der Kurzform (K-14). Z für Medizinische Psychologie. (2009) 18:43–8.
36. Hyland P, Shevlin M, Fyvie C, Karatzias T. Posttraumatic stress disorder and complex posttraumatic stress disorder in DSM-5 and ICD-11: Clinical and behavioral correlates. J Traumatic Stress. (2018) 31:174–80. doi: 10.1002/jts.2018.31.issue-2
37. Hyland P, Vallières F, Cloitre M, Ben-Ezra M, Karatzias T, Olff M, et al. Trauma, PTSD, and complex PTSD in the Republic of Ireland: prevalence, service use, comorbidity, and risk factors. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:649–58. doi: 10.1007/s00127-020-01912-x
38. Foa EB. PDS: Posttraumatic stress diagnostic scale: Manual. Minneapolis: Natl Comput Syst. (1995).
39. Ehlers A, Steil R, Winter H, Foa E. Deutsche Übersetzung der Posttraumatic Stress Diagnostic Scale (PDS) [German translation of the Posttraumatic Stress Diagnostic Scale]. Oxford: Department of Psychiatry, Warnford Hospital, University of Oxford (1996).
40. McCarthy S. Post-traumatic stress diagnostic scale (PDS). Occup Med. (2008) 58:379–. doi: 10.1093/occmed/kqn062
41. Briere J. Trauma symptom inventory-2 (TSI-2). Odessa, FL: Psychological Assessment Resources (2011).
42. Krammer S, Grosse Holtforth M, Soyka M, Liebrenz M. Assessment of complex posttraumatic stress disorder with the revised Trauma Symptom Inventory (TSI-2). Fortschr Neurol Psychiatr. (2019) 87:364–71. doi: 10.1055/s-0044-101034
43. Krammer S, Grossenbacher H, Goldstein N, Kaufmann C, Schwenzel A, Soyka M. Validierung der deutschen Übersetzung des revidierten Trauma Symptom Inventory (TSI-2) zur Erfassung komplexer posttraumatischer Belastungssymptomatik. PPmP-Psychotherapie· Psychosomatik· Medizinische Psychologie. (2017) 67:212–20. doi: 10.1055/s-0042-120839
44. Lehrl S, Triebig G, Fischer B. Multiple choice vocabulary test MWT as a valid and short test to estimate premorbid intelligence. Acta Neurologica Scandinavica. (1995) 91:335–45.
45. Schwert C, Stohrer M, Aschenbrenner S, Weisbrod M, Schröder A. Biased neurocognitive self-perception in depressive and in healthy persons. J Affect Disord. (2018) 232:96–102. doi: 10.1016/j.jad.2018.02.031
46. Sharma A, Schray A, Bartolovic M, Roesch-Ely D, Aschenbrenner S, Weisbrod M. Relationship between serum calcium and neuropsychological performance might indicate etiological heterogeneity underlying cognitive deficits in schizophrenia and depression. Psychiatry Res. (2017) 252:80–6. doi: 10.1016/j.psychres.2017.01.101
47. Sturm W. Wahrnehmungs- und Aufmerksamkeitsfunktionen - Batterie (WAF). Mödling: Schuhfried (2006).
48. Rodewald K, Weisbrod M, Aschenbrenner S. Wiener Testsystem: Trail Making Test-Langensteinbacher Version (TMT-L). Mödling: Schuhfried (2012).
49. Vetter J, Aschenbrenner S, Weisbrod M. Figuraler Gedächtnistest (FGT). Mödling: Schuhfried (2012).
51. Kaller CP, Uterrainer JM, Kaiser S, Weisbrod M, Aschenbrenner S. Tower of London - Freiburger Version (TOL-F). Mödling: Schuhfried (2011).
52. Kaiser S, Aschenbrenner S, Pfüller U, Roesch-Ely D, Weisbrod M. INHIB Response Inhibition mödling. Schuhfried (2010).
54. Faul F, Erdfelder EL A-G, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
55. Cloitre M, Hyland P, Bisson JI, Brewin CR, Roberts NP, Karatzias T, et al. ICD-11 posttraumatic stress disorder and complex posttraumatic stress disorder in the United States: A population-based study. J traumatic stress. (2019) 32:833–42. doi: 10.1002/jts.22454
56. Stopyra MA, Simon JJ, Rheude C, Nikendei C. Pathophysiological aspects of complex PTSD – a neurobiological account in comparison to classic posttraumatic stress disorder and borderline personality disorder. Rev Neurosciences. (2023) 34:103–28. doi: 10.1515/revneuro-2022-0014
57. Karatzias T, Hyland P, Bradley A, Cloitre M, Roberts NP, Bisson JI, et al. Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: Findings from a trauma-exposed population based sample of adults in the United Kingdom. Depress Anxiety. (2019) 36:887–94. doi: 10.1002/da.2019.36.issue-9
58. Hyland P, Shevlin M, Fyvie C, Cloitre M, Karatzias T. The relationship between ICD-11 PTSD, complex PTSD and dissociative experiences. J Trauma Dissociation. (2020) 21:62–72. doi: 10.1080/15299732.2019.1675113
59. Fung HW, Chien WT, Lam SKK, Ross CA. The relationship between dissociation and complex post-traumatic stress disorder: A scoping review. Trauma Violence Abuse. (2023) 24:2966–82. doi: 10.1177/15248380221120835
60. Simon N, Roberts NP, Lewis CE, van Gelderen MJ, Bisson JI. Associations between perceived social support, posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD): implications for treatment. Eur J Psychotraumatol. (2019) 10:1573129. doi: 10.1080/20008198.2019.1573129
61. Guzman Torres E, Krause-Utz A, Sack M. Predictors of complex PTSD: the role of trauma characteristics, dissociation, and comorbid psychopathology. Borderline Pers Disord Emot Dysregul. (2023) 10:1. doi: 10.1186/s40479-022-00208-7
62. Dworkin ER, Jaffe AE, Bedard-Gilligan M, Fitzpatrick S. PTSD in the year following sexual assault: A meta-analysis of prospective studies. Trauma Violence Abuse. (2023) 24:497–514. doi: 10.1177/15248380211032213
63. Dworkin ER, Menon SV, Bystrynski J, Allen NE. Sexual assault victimization and psychopathology: A review and meta-analysis. Clin Psychol Rev. (2017) 56:65–81. doi: 10.1016/j.cpr.2017.06.002
64. Kilpatrick DG, Ruggiero KJ, Acierno R, Saunders BE, Resnick HS, Best CL. Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: results from the National Survey of Adolescents. J consulting Clin Psychol. (2003) 71:692. doi: 10.1037/0022-006X.71.4.692
65. Geuze E, Vermetten E, de Kloet CS, Hijman R, Westenberg HG. Neuropsychological performance is related to current social and occupational functioning in veterans with posttraumatic stress disorder. Depression anxiety. (2009) 26:7–15. doi: 10.1002/da.20476
66. Brandes D, Ben-Schachar G, Gilboa A, Bonne O, Freedman S, Shalev AY. PTSD symptoms and cognitive performance in recent trauma survivors. Psychiatry Res. (2002) 110:231–8. doi: 10.1016/S0165-1781(02)00125-7
67. Jelinek L, Jacobsen D, Kellner M, Larbig F, Biesold K-H, Barre K, et al. Verbal and nonverbal memory functioning in posttraumatic stress disorder (PTSD). J Clin Exp neuropsychology. (2006) 28:940–8. doi: 10.1080/13803390591004347
68. Hanson JL, Nacewicz BM, Sutterer MJ, Cayo AA, Schaefer SM, Rudolph KD, et al. Behavioral problems after early life stress: contributions of the hippocampus and amygdala. Biol Psychiatry. (2015) 77:314–23. doi: 10.1016/j.biopsych.2014.04.020
69. Bryant RA, Felmingham KL, Malhi G, Andrew E, Korgaonkar MS. The distinctive neural circuitry of complex posttraumatic stress disorder during threat processing. Psychol Med. (2021) 51:1121–8. doi: 10.1017/S0033291719003921
70. Samuelson KW. Post-traumatic stress disorder and declarative memory functioning: a review. Dialogues Clin Neurosci. (2011) 13:346–51. doi: 10.31887/DCNS.2011.13.2/ksamuelson
71. Wild J, Gur RC. Verbal memory and treatment response in post-traumatic stress disorder. Br J Psychiatry. (2008) 193:254–5. doi: 10.1192/bjp.bp.107.045922
72. Haaland KY, Sadek JR, Keller JE, Castillo DT. Neurocognitive correlates of successful treatment of PTSD in female veterans. J Int Neuropsychol Society. (2016) 22:643–51. doi: 10.1017/S1355617716000424
73. Nijdam MJ, de Vries G-J, Gersons BP, Olff M. Response to psychotherapy for posttraumatic stress disorder: The role of pretreatment verbal memory performance. J Clin Psychiatry. (2015) 76:18178. doi: 10.4088/JCP.14m09438
74. Zinchenko A, Al-Amin MM, Alam MM, Mahmud W, Kabir N, Reza HM, et al. Content specificity of attentional bias to threat in post-traumatic stress disorder. J Anxiety Disord. (2017) 50:33–9. doi: 10.1016/j.janxdis.2017.05.006
75. Hayes JP, VanElzakker MB, Shin LM. Emotion and cognition interactions in PTSD: a review of neurocognitive and neuroimaging studies. Front Integr Neurosci. (2012) 6:89. doi: 10.3389/fnint.2012.00089
76. Badura-Brack AS, Naim R, Ryan TJ, Levy O, Abend R, Khanna MM, et al. Effect of attention training on attention bias variability and PTSD symptoms: Randomized controlled trials in Israeli and US combat veterans. Am J Psychiatry. (2015) 172:1233–41. doi: 10.1176/appi.ajp.2015.14121578
77. Lewis SJ, Koenen KC, Ambler A, Arseneault L, Caspi A, Fisher HL, et al. Unravelling the contribution of complex trauma to psychopathology and cognitive deficits: a cohort study. Br J Psychiatry. (2021) 219:448–55. doi: 10.1192/bjp.2021.57
78. Yehuda R, Tischler L, Golier JA, Grossman R, Brand SR, Kaufman S, et al. Longitudinal assessment of cognitive performance in holocaust survivors with and without PTSD. Biol Psychiatry. (2006) 60:714–21. doi: 10.1016/j.biopsych.2006.03.069
79. Cohen RA, Marsiske MM, Smith GE. Neuropsychology of aging. Handbook of Clinical Neurology. (2019) 167:149–80.
80. Rosenblat JD, Kakar R, McIntyre RS. The cognitive effects of antidepressants in major depressive disorder: a systematic review and meta-analysis of randomized clinical trials. Int J Neuropsychopharmacol. (2016) 19:pyv082. doi: 10.1093/ijnp/pyv082
81. Corney KB, Stuart AL, Pasco JA, Mohebbi M, Kavanagh BE, Sui SX, et al. Psychiatric symptoms, associated pharmacological treatments and cognitive function: A population-based study of men. J Affect Disord. (2024) 356:657–63. doi: 10.1016/j.jad.2024.04.076
82. Gregory E, Torres IJ, Ge R, Blumberger DM, Downar JH, Daskalakis ZJ, et al. Predictors of cognitive impairment in treatment-resistant depression. J Affect Disord. (2020) 274:593–601. doi: 10.1016/j.jad.2020.05.101
Keywords: complex PTSD, cognitive functioning, visual memory, executive functioning, attention
Citation: Schöndorf Z-S, Terhoeven V, Jaehn A, Roesch-Ely D, Friederich H-C, Nikendei C and Kindermann D (2025) Characterization of cognitive functioning in complex PTSD compared to non-complex PTSD. Front. Psychiatry 15:1433614. doi: 10.3389/fpsyt.2024.1433614
Received: 16 May 2024; Accepted: 25 November 2024;
Published: 15 January 2025.
Edited by:
Marco Grados, Johns Hopkins University, United StatesReviewed by:
Thomas Wenzel, Medical University of Vienna, AustriaBradley Grant, Kennedy Krieger Institute, United States
Copyright © 2025 Schöndorf, Terhoeven, Jaehn, Roesch-Ely, Friederich, Nikendei and Kindermann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Kindermann, ZGF2aWQua2luZGVybWFubkBtZWQudW5pLWhlaWRlbGJlcmcuZGU=