 Minseok Hong1
Minseok Hong1 Hyesoo Kim1
Hyesoo Kim1 C. Hyung Keun Park2
C. Hyung Keun Park2 Hyunju Lee3,4
Hyunju Lee3,4 Sang Jin Rhee3
Sang Jin Rhee3 Sooyeon Min3
Sooyeon Min3 Min Ji Kim1
Min Ji Kim1 Jeong Hun Yang3Yoojin Song1,3
Jeong Hun Yang3Yoojin Song1,3 Kyunghoon Son3
Kyunghoon Son3 Yong Min Ahn1,3,5*
Yong Min Ahn1,3,5*- 1Department of Psychiatry, Seoul National University College of Medicine, Seoul, Republic of Korea
- 2Department of Psychiatry, Asan Medical Center, Seoul, Republic of Korea
- 3Department of Neuropsychiatry, Seoul National University Hospital, Seoul, Republic of Korea
- 4Department of Clinical Medical Sciences, Seoul National University College of Medicine, Seoul, Republic of Korea
- 5Seoul National University Medical Research Center, Institute of Human Behavioral Medicine, Seoul, Republic of Korea
Background: Attitudes toward suicide are essential in suicide prevention, as suicide is socio-culturally nuanced. Although the relationship between individual attitudes and suicidal behavior has been extensively studied, the effect of community attitudes—aggregated by region—on suicide mortality remains ambiguous. This study explored the association between community attitudes and real-world suicide mortality.
Methods: Data on attitudes toward suicide from the 2018 Korea National Suicide Survey (N = 1500) and individual mortality data from the MicroData Integrated System were obtained. Confirmatory factor analysis supported a factor structure with three factors: “Permissiveness,” “Unjustified behavior,” and “Readiness to help/Preventability.” Thirty regional units in South Korea aggregated the data for ecological analysis. We used negative binomial models to examine the association at the regional level, and stratified analysis by gender and age group was conducted.
Results: “Permissiveness” was associated with reduced suicide rates in a univariate model (P < 0.001). Adjusting for gender, age, and additional sociodemographics did not alter the association. Additionally, this relationship was observed in males and individuals under 60 years of age after stratification. However, “Unjustified Behavior” and “Readiness to help/Preventability” exhibited no significant association with suicide in any model or stratum.
Conclusion: The observed inverse association between permissive community attitudes and suicide contradicts the findings of previous research that links permissive individual attitudes to increased suicidal behavior. Our findings suggest that attitudes may operate differently at the individual and group levels. Although the cross-sectional design and single-country focus of this study warrant further investigation, our findings indicate that attitudes are significant contextual factors in the process of suicide, which could lead to novel approaches in suicide prevention.
1 Introduction
Annually, more than 700,000 people die by suicide (1). South Korea has the highest suicide rate among the Organisation for Economic Co-operation and Development (2). Moreover, suicide is the leading cause of death in Korea for individuals in their teens to thirties (3). Given its prominence as a national issue, Korea has made strenuous efforts over the last decade to reduce the suicide rate. These initiatives included reducing exposure to known means of suicide (4), implementing nationwide suicide prevention education (5), and creating guidelines for suicide reporting in the media (6). Consequently, the suicide rate declined from 2010 to 2016 (7). However, despite ongoing efforts, the suicide rate has not continued to decrease, and alarmingly, youth suicide has risen since then (8). A fresh perspective and approach are required to enhance our understanding and prevention of suicide.
Although mental health issues are a main risk factor for suicide (9–11), suicide is a multifaceted phenomenon that also occurs within a socio-cultural context. Since Durkheim’s classic work on suicidology (12), even contemporary influential theories such as the interpersonal theory (13, 14), the integrated motivational-volitional model (IMV) (15), and the three-step theory (3ST) (16) have highlighted the social dimensions of suicide. Attitudes play a critical role in integrating individual and social perspectives on one’s behavior (17), particularly regarding suicide (18). Evidence indicates that attitudes toward suicide are involved in the social interplay surrounding suicide. Attitude toward suicide is affected by the suicide of a close person and the suicidal intensity (19); it may be involved in suicide clustering among adolescents (20). Therefore, investigating community attitudes, which are aggregated at the regional or group level, is theoretically significant and could offer new insights into suicide prevention.
In recent years, numerous studies have explored the relationship between attitudes toward suicide and suicidal behavior, such as suicidal ideation and attempts. Research from various socio-cultural backgrounds consistently demonstrates that permissive or pro-suicidal attitudes are associated with increased suicidal behavior at the individual level (21–31). A study conducted in Korea, Japan and US found that permissive attitudes were the most significant predictor of the intensity of suicidal ideation across all three countries (18). However, most of these studies have focused on how suicidal behavior changes according to attitudes at the individual level. The potential effect of community attitudes on suicide has been overlooked despite its recognized necessity (25).
Furthermore, the relationship between attitudes toward suicide and actual suicide remains unclear, likely because of difficulties measuring an inner attitude through psychological autopsies. Suicide is a distinguished phenomenon from a suicide attempt. Suicide attempts had an estimated incidence at least 20 times higher than suicides (32), whereas psychological autopsy studies show that more than half of suicides result in death at the first attempt (33). Differences in the method have been observed between suicides and suicide attempts (34), emphasizing the necessity to examine the characteristics of suicide mortality separately.
Despite the pressing need for further investigation, the limited literature on this topic has yielded inconsistent results. Specifically, while Neeleman et al. found that pro-suicidal attitudes toward suicide are associated with increased suicide rates (35), Reynder et al. reported a non-significant association (36). In Sweden, the suicide rate has decreased since the 1980s, whereas permissive attitude ratings have increased (25). Some studies have merely compared two regions (21, 37), resulting in a low level of evidence. Moreover, most of these studies were primarily based in European and North American countries, and research in different socio-cultural contexts is required.
This exploratory study examined the association between attitudes toward suicide and the suicide rate through an ecological analysis, a research methodology investigating relationships between variables at an aggregated level (38). We combined a nationwide survey and statistics, ensuring representativeness, and presented several regression models with varying covariate inputs to accomplish this. To the best of our knowledge, this study is the first to explore the relationship between attitudes and suicide mortality using a nationwide survey and mortality microdata. This group-level investigation will contribute to a deeper understanding of suicide as a biopsychosocial phenomenon. Enhancing our comprehension of the multifaceted nature of suicide may strengthen suicide prevention efforts (39, 40) and provide insight into the stagnant suicide rate in Korea.
2 Materials and methods
2.1 Participants
The 2018 Korea National Survey on Suicide (KNSS) (41), sponsored by the Ministry of Health and Welfare of Korea, served as the basis for this study. This survey was conducted based on a complex sample design to ensure representativeness. Structured face-to-face interviews were conducted with 1,500 adults aged 19 to 75 between November 21 and December 17, 2018. The interviewers were trained by experts and supported during the survey. Ten households were randomly selected for each district, and an interviewer visited each household and conducted the survey. Following the interview, 30% of the participants underwent phone follow-up for quality control.
The Seoul National University Hospital Institutional Review Board approved and monitored this study (IRB No. 1810-062-979). Interviewers obtained informed consent from participants before commencing the interviews. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines (42) and was conducted in compliance with the Declaration of Helsinki.
2.2 Measurements
Demographic characteristics of participants, including age, gender, education, employment, and religion, were collected. Participants were also asked about any previous experience with suicidal ideation.
The Questionnaire on Attitudes Toward Suicide (ATTS) was employed to assess the normative attitudes of participants toward suicide. Developed and validated by Renberg and Jacobsson (25), the ATTS is suitable for large-scale studies and widely used in various countries (43). The Korean version, created through the 2013 KNSS (44), was utilized in the 2018 KNSS. Each item of the ATTS was scored on a Likert scale of 1-5 points, where 1 indicated “disagreement” and 5 indicated “agreement.”
2.2.1 Factor structure of ATTS
Kim et al. previously reported a factor structure of ATTS based on the 2013 and 2018 KNSS (45). In this study, we reevaluated the previous factor structure, as multiple methods for determining the number of factors indicated that a three-factor structure best fits the 2018 KNSS data alone (Supplementary Figure 1). Unreliable and semantically redundant factors were removed or combined to create a more parsimonious structure while maintaining the basic framework of the original factor structure. The revised factor structure encompassed 3 factors and 15 items (Table 1). Through confirmatory factor analysis (Supplementary Figure 2), we assessed the goodness of fit and acquired factor score. The revised factor structure had a good absolute fit and parsimony correction, and the comparative fit was within an acceptable or satisfactory range (46). Acquisition of factor score used Barlett’s method.
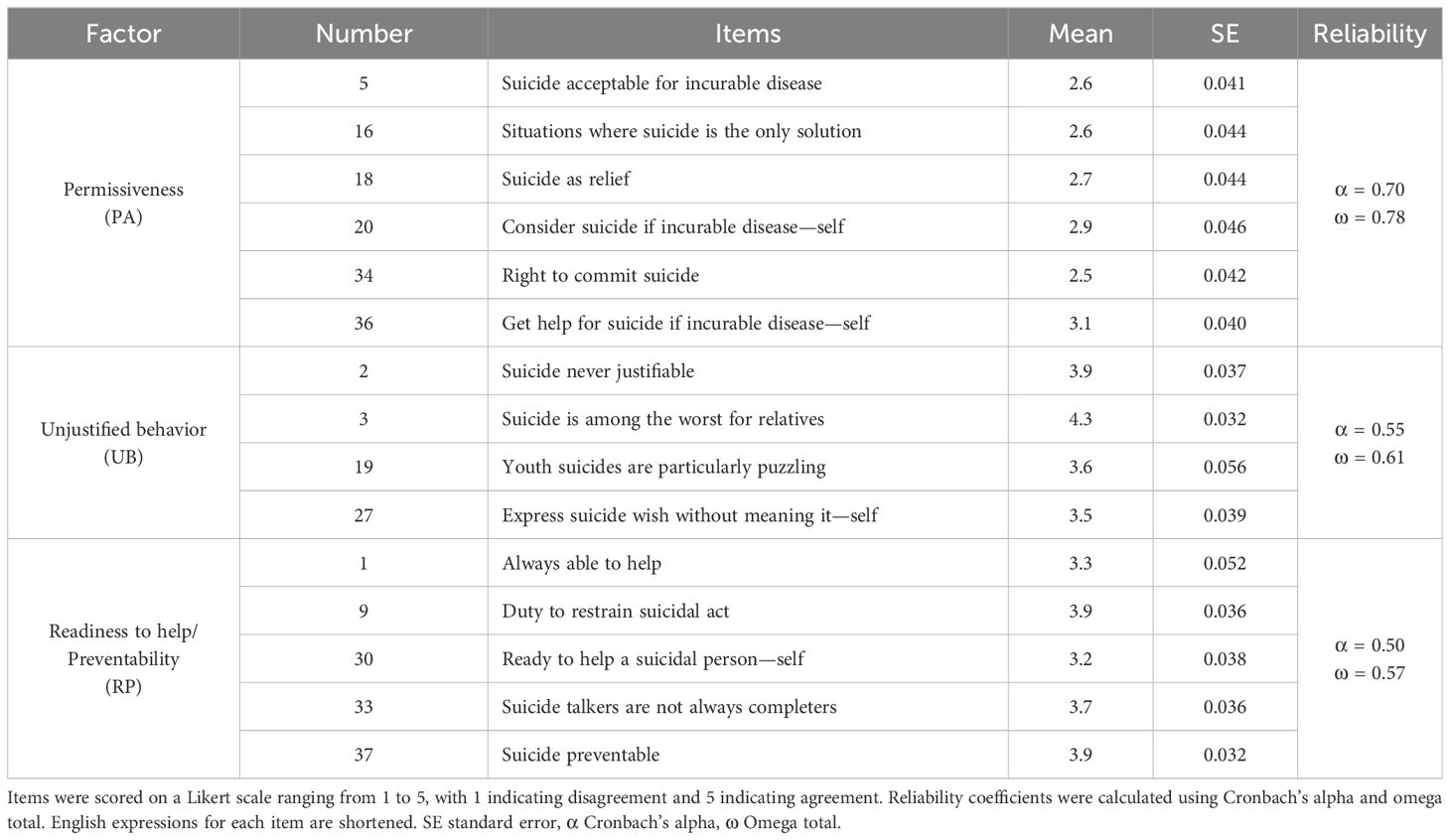
Table 1. Revised factor structure for the Questionnaire on Attitudes Toward Suicide.
The factors names, “Permissiveness (PA),” “Unjustified behavior (UB)” and “Readiness to help/Preventability (RP),” were derived from the original factor structure. PA semantically represents permissive and acceptable attitudes toward suicide, considering it a right or option in certain circumstances, such as incurable diseases. UB represents opposition to justifying suicide and regards it as morally reprehensible behavior that should be restrained. Intriguingly, this factor also included items that perceive suicide as puzzling or deceptive. RP represents proactive attitudes toward suicide prevention, characterized by a readiness to help and taking an active role in preventing suicide. Compared to PA, participants in the 2018 KNSS generally demonstrated greater agreement with items in UB and RP, and their standard errors were narrower for most items. The reliability of UB and RP, evaluated using Cronbach’s alpha, is low; however, it surpasses the requisite value of 0.5 for preliminary or exploratory research, as proposed by Nunnally (47).
2.2.2 Suicide mortality
Microdata on suicide mortality were obtained through the MicroData Integrated System (MDIS) provided by Statistics Korea (48). The MDIS provides individual information, including the deceased’s gender, age, address, and cause of death, as registered in the Causes of Death Statistics. Researchers remotely accessed and processed the data stored on the MDIS server, and Statistics Korea examined and approved the anonymization of the processed data when exported. This study included individuals who died between January 1 and December 31, 2018, and whose causes of death corresponded to the X60-X84 (intentional self-harm) codes of the Korean Standard Classification of Diseases 7th edition (49). Consistent with the participants in the KNSS, only death cases involving individuals aged 19 to 75 were included in the analysis.
2.3 Statistical analysis
The country was divided into 30 regional units for ecological analysis. Survey strata comprising 80 or more participants were reorganized into clusters of 40 to 70 participants based on geographical proximity, forming regional units (Supplementary Table 1). Basic characteristics, ATTS, and microdata on suicide mortality were aggregated by these regional units, utilizing survey weights based on a complex sample design. Comparisons were conducted between regions with high and low suicide rates to demonstrate differences in regional characteristics according to suicide rates. If the Shapiro-Wilk test rejected the normal distribution, Wilcoxon’s test was employed for comparison; otherwise, Welch’s t-test was utilized.
In the preliminary analysis, regional suicide counts exhibited overdispersion, with a mean substantially lower than the variance (386.2 vs. 15924.5). As the negative binomial regression model can be generalized to overdispersed count data in place of Poisson models (50), this model was employed to predict suicide mortality. A univariate model (Modeluniv) and four multivariate models (Model 1 to Model 4) were constructed. In Model 1, adjustments were made for the proportions of females and adults over 60 years. Using the proportion of older adults as a covariate rather than the mean age allowed for consideration of South Korea’s unique characteristics, where elderly suicide is notably prevalent, and its etiology appears to be differentiated (51, 52). In Models 2 and 3, one additional covariate from Model 1 was further adjusted by adding lifetime experience of suicidal ideation (Model 2) and college education (Model 3). In Model 4, a quadratic term of the factor score was added to the adjustments made in Model 1. The dependent variable was the incidence of suicide in each region, with the regional population set as an offset variable. The result of each model was presented as an incidence rate ratio (IRR), and model performance was assessed by Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC). Additionally, because of differences in the mechanisms resulting in suicide based on gender and age (53–56), stratified analyses were performed. Stratification was based on gender (male, female) and age group (-39, 40–59, 60- years).
R Statistical Software v4.2.2 (57) was used for all statistical analyses. Furthermore, package lavaan v0.6-13 (58) was utilized for confirmatory factor analysis, package survey v4.1-1 (59) for analysis based on the complex sample design, and package MASS v7.3-58.2 (60) for the negative binomial regression model. All statistical tests were two-tailed, and a P-value of 0.05 was considered the threshold for significance. Asterisks were used to indicate the significance level for enhanced readability: * for P < 0.05, ** for P < 0.01, and *** for P < 0.001.
3 Results
3.1 Group comparison of regional characteristics
Demographic information and ATTS responses were collected from 1,500 participants through the 2018 KNSS. Moreover, the inclusion criteria yielded data on suicide mortality for 11,587 cases obtained via MDIS. No missing values were observed in the data.
Group comparisons were conducted by categorizing the 30 regions into those with high and low suicide rates (Table 2). Regions with high suicide rates exhibited older mean ages (P = 0.029*) and greater proportions of older adults (P = 0.041*). Conversely, no statistically significant differences were observed in gender or participant count. Seoul, Korea’s largest city and capital, and its metropolitan areas predominantly fell within the low suicide rate regions (Supplementary Table 1). Nevertheless, the regional population did not exhibit any significant group differences.
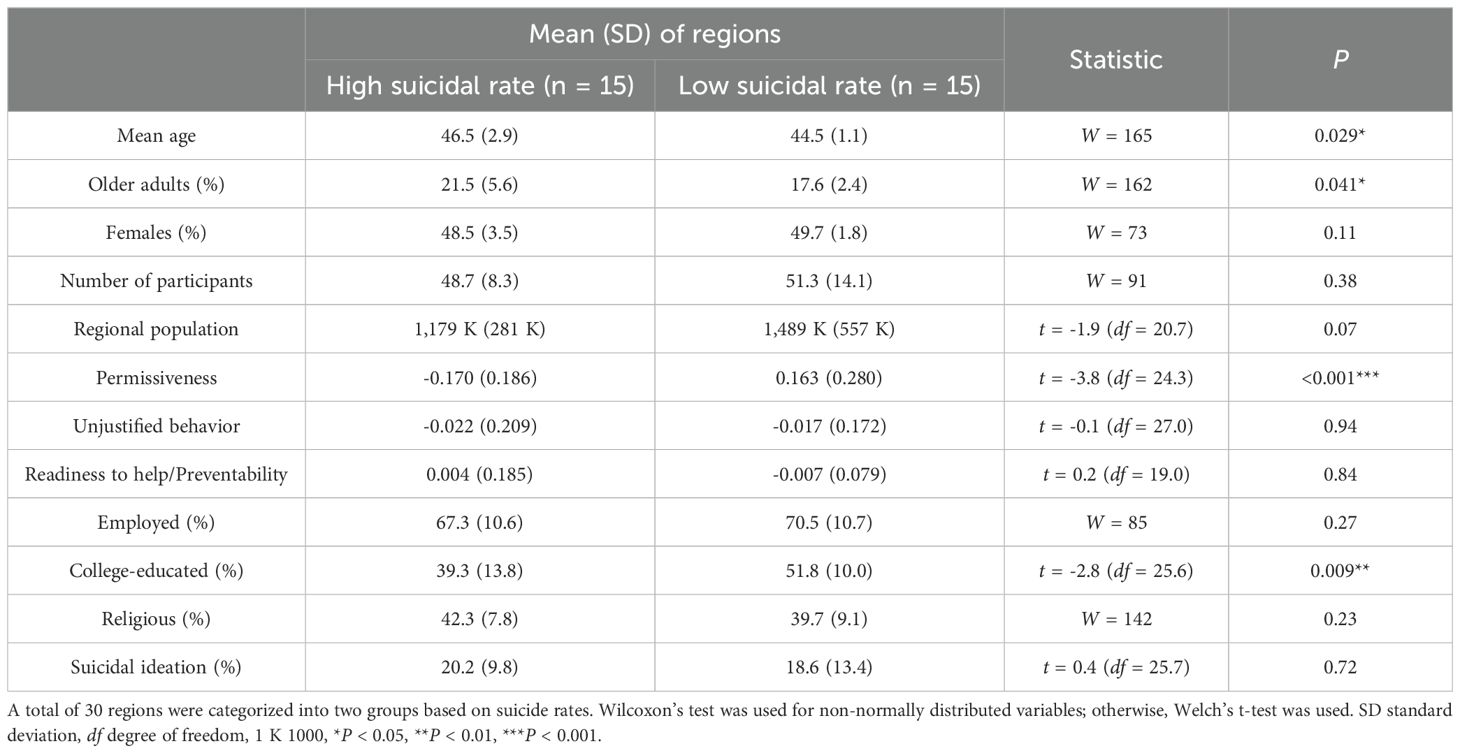
Table 2. Group comparison of basic regional characteristics.
Regarding factor scores, PA was higher in regions with low suicide rates (P < 0.001***), while UB and RP showed no group difference. Participants in regions with low suicide rates were more likely to have completed college-level education (P = 0.009**), but no significant differences were observed in employment and religiousness rates. The lifetime prevalence of suicidal ideation was found to be approximately 20%, with no observed group difference.
3.2 Regression models
A scatter plot of factor scores and suicide rates for each region is illustrated along with a regression line based on Modeluniv (Figure 1). A significant decrease in suicide mortality was observed as the PA score increased (P < 0.001***). Comparing the 20th to 80th percentile of the “Permissiveness” score, predicted suicide rates decreased by 11.2%, equating to a difference of 34.9 cases per year in a virtual region with a population of a million. However, no significant association was identified for UB and RP.
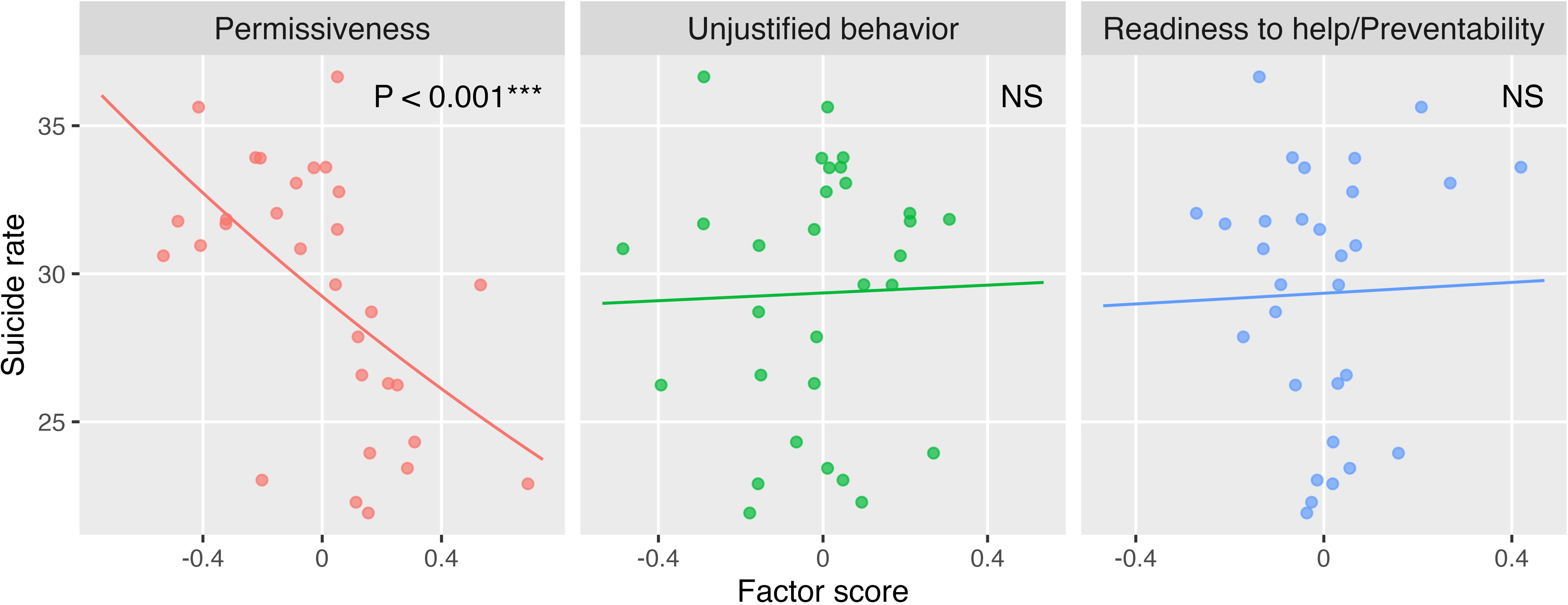
Figure 1. Factor scores and suicide mortality rates. Regression lines from a univariate negative binomial regression model are displayed together. Each point represents one region. A zero score indicates an average level, while positive and negative scores indicate above-average agreement and disagreement, respectively. Suicide rates were calculated per 100,000 people. NS not significant, *P < 0.05, **P < 0.01, ***P < 0.001.
The results of univariate and four multiple regression models were acquired (Table 3). PA was significantly associated with decreased suicide mortality in all the regression models. Conversely, UB was not associated with suicide in any model. RP showed no significant association with suicide in any model, except in Model 4, where the quadratic term was significantly associated. This association indicated that suicide mortality increased as the factor score deviated further from the mean. The lowest values of both AIC and BIC were observed in Modeluniv with PA, followed by Model 3 with PA.
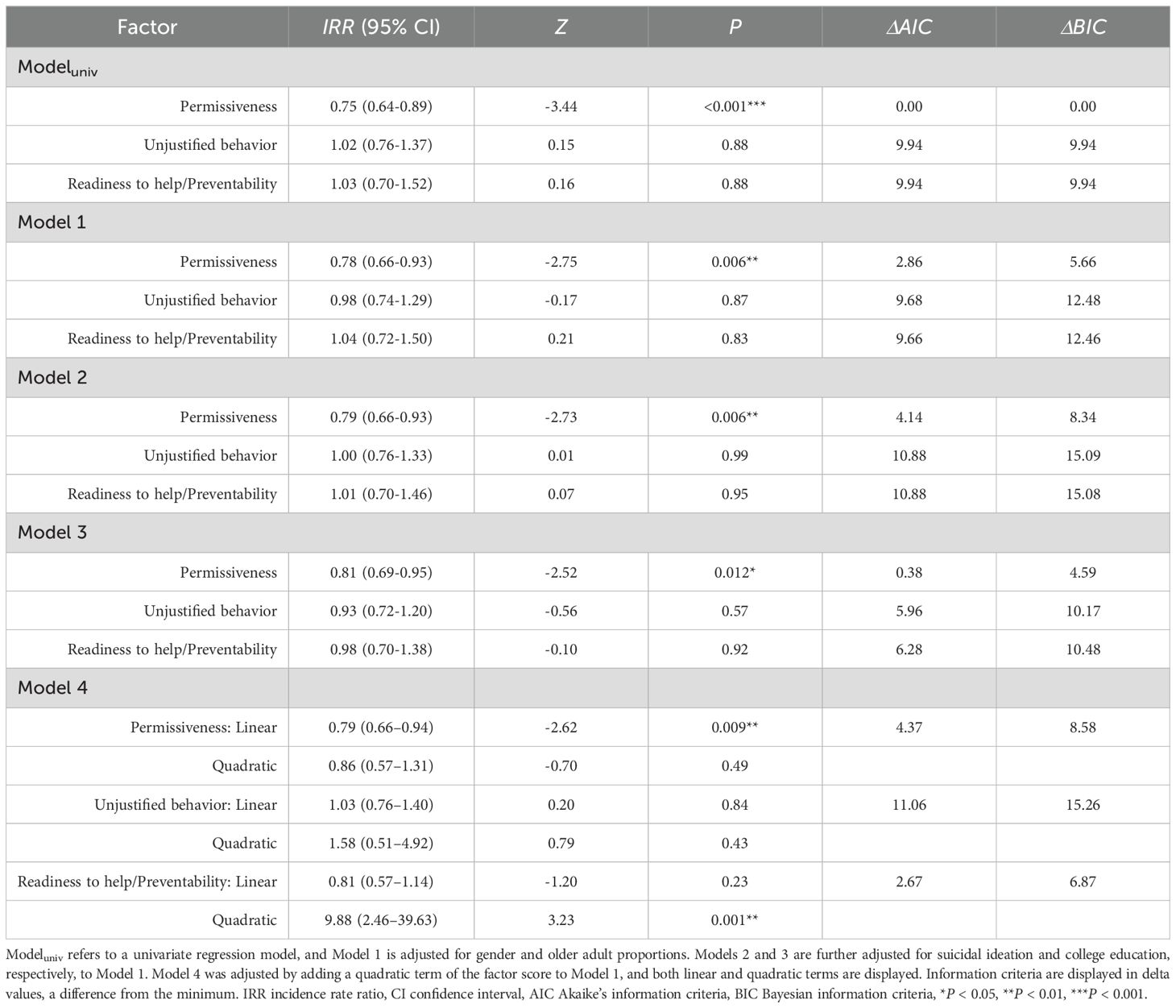
Table 3. Results of negative binomial regression models.
3.3 Stratified analysis
Stratified analysis was conducted in Model 1 to examine the impact of gender and age (Figure 2). Results showed that PA was associated with decreased IRR of suicide in males and ages under 60 years. UB and RP did not exhibit significant associations in any strata, and no factor significantly impacted the IRR for females and older adults. Findings from other models were consistent, except for the female stratum in Modeluniv (Supplementary Figure 2).
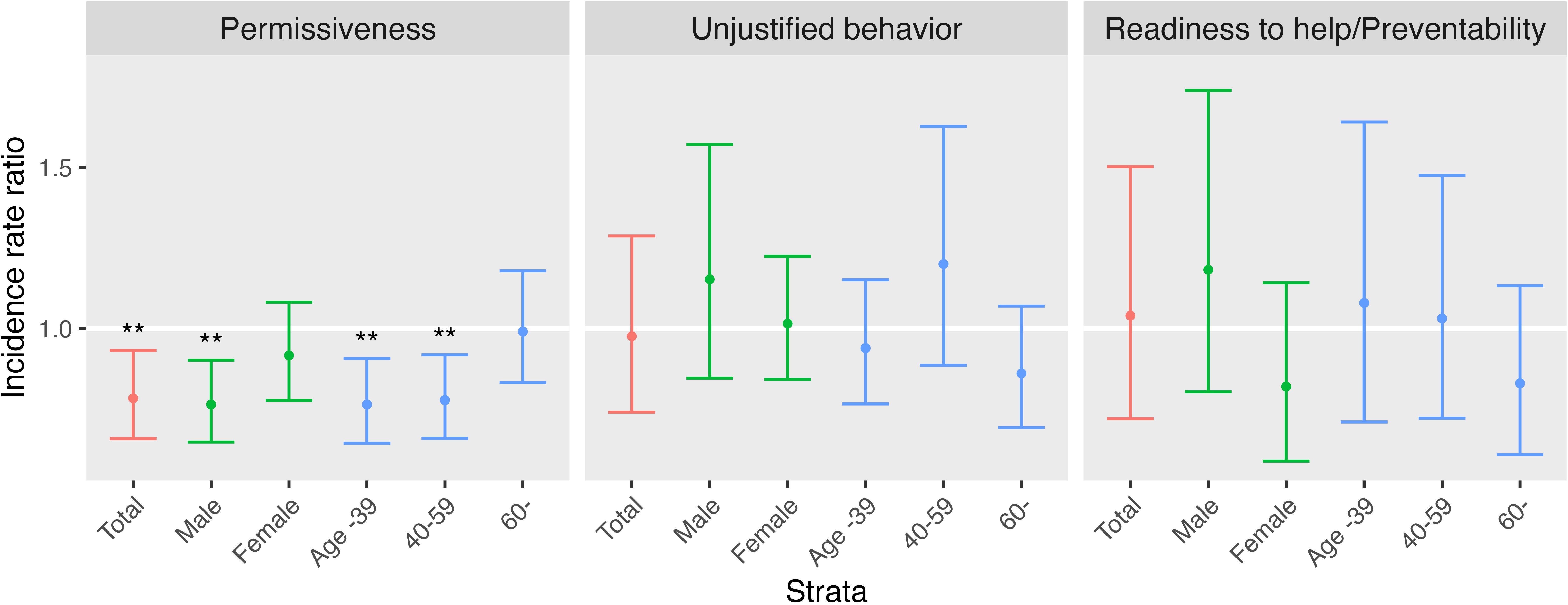
Figure 2. Gender and age group stratified analysis in Model 1. It displays the incidence rate ratios of suicide mortality with 95% confidence intervals indicated by error bars. *P < 0.05, **P < 0.01, ***P < 0.001.
4 Discussion
This study investigated the effect of community attitudes on real-world suicide through an ecological methodology. Attitudes, which were aggregated by region, demonstrated various relationships with suicide mortality, also aggregated by region. Regions where suicide was permissible (as measured by PA) had a lower suicide rate. This association remained significant even after adjusting for gender, the proportion of older adults, suicidal ideation, and college education. After stratification, significant associations were still present in males, younger adults, and middle-aged adults. Oppositional attitudes toward suicide (as measured by UB) showed no significant connection to suicide rates in any stratum or model. Proactive attitudes toward suicide prevention (as measured by RP) demonstrated a significant quadratic association with suicide rates.
It is worth noting that regional variations in the proportion of individuals who have experienced suicidal behavior, although a minority, may influence the association. Additionally, Seoul and its metropolitan area, which have a high socioeconomic and education level (61), showed low suicide rates, which may confound the association. Nevertheless, the association between permissive attitudes and low suicide mortality was still significant after adjusting for either suicidal ideation or college education. Furthermore, the performance of the univariate model, as measured by AIC and BIC, was superior to that of the other multivariate models. This implies that permissive attitudes effectively and independently predict regional suicide rates, though overinterpretation should be avoided.
As mentioned earlier, previous studies have established a positive association between pro-suicidal attitudes and suicidal behavior at the individual level (21–30), including a study of the 2013 and 2018 KNSS data (45). However, this study reports a negative association between suicide rates and permissive attitudes, where permissive regions had lower suicide rates despite permissive individuals being more likely to engage in suicidal behavior. A more comprehensive perspective must consider individuals at risk of suicide and their surrounding communities to reconcile these conflicting results. In a region or community, suicide is uncommon, and most people do not intend to or attempt it (62). Therefore, attitudes aggregated through ecological analysis are more likely to reflect non-suicidal individuals’ views. Our findings, based on this context, show that if a community has permissive attitudes toward suicide, individuals at risk of suicide are less likely to die by suicide.
Reverse causality is one possible explanation, whereby if suicide is more frequent, the community may become less permissive. However, this explanation is less likely, as previous studies consistently report that losing a close person by suicide can result in a more permissive or normalizing attitude toward suicide (19, 63). Another possible explanation is that high levels of permissive attitudes may prevent suicide. Individuals’ attitudes and stigma significantly affect their behavior in disclosing their struggles, seeking help, and utilizing mental health services (64–66). As suicide occurs within socio-cultural contexts, community attitudes toward suicide may affect the behavior of suicidal individuals.
Taking community attitudes as a variable that operates in a socio-cultural context, diverse possibilities exist regarding their role in contemporary suicide theories. The theoretical explanations of 3ST and IMV on the point where social factors affect the progression of suicidal behavior differ slightly. From the perspective of 3ST (16), community attitudes can be seen as related to connectedness, which is defined as a broad construct encompassing various social elements that prevent individuals’ suicidal ideation from escalating into a strong desire. In this sense, individuals surrounded by permissive neighbors may be more likely to seek and receive help when at risk of suicide, leading to a lower suicide rate in the community. Conversely, the perspective of IMV (15) considers social interaction variables as motivational moderators that govern the eventual occurrence of suicidal ideation in vulnerable individuals. Permissive attitudes in a community may prevent defeated, humiliated, and entrapped individuals from developing suicidal ideation. Besides, the influence of contextual variables among social factors is not explicitly organized within these theoretical systems (67, 68). Therefore, an elaboration on the role of community attitudes can aid in integrating the influence of socio-cultural context into modern suicide theory, contributing to its advancement.
The stratified analysis revealed that male suicide is more strongly associated with attitudes than that in females. Previous studies have established that while male suicide is more common than female suicide, females are more likely to attempt suicide and seek help (69, 70). The effect of permissive attitudes on male suicide may be more powerful as male suicidal behavior is often silent and stealthy. In addition, older adults, who have the highest suicide rate among the Korean population, were least affected by attitudes when stratified by age group. In Korea, socioeconomic status, such as poverty, might be a more significant risk factor for suicide in older adults (51, 52), outweighing the effect of attitudes. Therefore, suicide prevention strategies for females and elderly individuals should consider other factors beyond attitudes. Attitudinal approaches to suicide prevention may be most effective in males and younger individuals.
No significant associations between oppositional attitudes toward suicide and suicide mortality were observed across models or strata. Participants in the 2018 KNSS uniformly agreed with items in the UB (Table 1), which may have resulted in an insignificant association due to the narrow distribution. The cognitive-emotional elements of public stigma, namely stereotypes and prejudice (71), are semantically related to oppositional attitudes. Previous research has revealed high levels of public stigma among Korean policymakers (72), with this elevated stigma closely linked to various cultural factors within the country (73). It is plausible that the distribution of oppositional attitudes serves as a manifestation of public stigma. Moreover, inconsistencies in associations between community attitudes and suicide observed in previous studies may be attributable to the heterogeneity of public stigma across time and regions. As a result, it would be inappropriate to conclude that public stigma is not a significant issue in Korean suicide merely because oppositional attitudes toward suicide have not exhibited an association with suicide mortality.
The significant quadratic association between proactive attitudes toward suicide prevention and suicide mortality suggests that proactive attitudes may have a bidirectional relationship with suicide. Regions with average levels of proactive attitudes showed lower suicide rates, while regions with either high or low attitude scores exhibited higher suicide rates. It is plausible that in regions with low proactive attitudes, weaker suicide prevention efforts lead to higher suicide mortality. However, this does not explain why regions with high proactive attitudes also have high suicide rates. Thus, it is possible that high suicide rates may, in turn, elevate proactive attitudes. In fact, since 2011, a nationwide suicide prevention education program has been implemented, and by 2019, 1.2 million people had completed the program (5). Promoting proactive attitudes is one of the primary objectives of these programs, and it is possible that the program’s implementation or efficacy was particularly strong in some regions where suicide is more prevalent.
The reliability of UB and RP warrants discussion. No consensus exists on a definitive threshold for reliability, as this depends on the study’s purpose (74). ATTS encompasses a broad spectrum of human attitudes, which are inherently non-clear-cut and ambivalent. The ATTS features a limited number of items because of the need for feasibility in large-scale surveys (25). Furthermore, KNSS, with its goal of nationwide information gathering and wide age range coverage, inevitably introduces heterogeneity into the sample. Considering these circumstances and the objectives of this study, it is reasonable for attitude factors to carry some degree of heterogeneity; thus, the reliability levels of these factors are deemed acceptable. Other studies measuring attitudes toward suicide have also reported similar levels of reliability (24–26).
4.1 Implications and future directions
The findings of this study bear significant implications for both the research field and practical application. First, our investigation provides theoretical evidence that the effects of community attitudes and individual attitudes toward suicide may differ. Individuals with permissive attitudes may be more likely to engage in suicidal behavior (18). Extrapolating this relationship to the group level or other contexts, however, may result in oversimplification. Future studies on attitudes toward suicide should differentiate between the attitudes of at-risk individuals and those of the surroundings.
Second, the results imply that addressing community attitudes could serve as a practical approach to suicide prevention. However, modifying attitude is a complex process, and short-term suicide prevention education has not shown a significant association with permissive attitudes toward suicide (75, 76). Furthermore, proactive attitudes toward suicide prevention are already prevalent in Korea and appear to have limited effect on suicide mortality. Consequently, alternative strategies beyond temporary measures are required, as well as short-term educational efforts focusing on public stigma and technical aspects. Community attitudes may function as surrogate markers for sociological variables that influence the phenomenon of suicide, such as individualism-collectivism (77) and social integration (12). This study might provide evidence that Korean society necessitates an extended, long-term discourse encompassing diverse values surrounding suicide and life.
To corroborate and actualize these implications, further elaboration on how community attitudes function as contextual variables is essential. Multilevel analysis suits this inquiry (78). It enables us to distinguish between group-level effects and cross-level interactions and the identification of the impact of community attitudes on the development of suicidal behavior. Unfortunately, the sample size of 1,500 participants and 30 regions included in this study was insufficient to conduct a multilevel analysis because of the low base rate of suicidal behavior in the general population, which would necessitate a larger sample size (79). Future studies with larger sample sizes, measuring help-seeking variables, and utilizing longitudinal design may aid in elucidating the relationship between attitudes and suicidal behavior more comprehensively. A better understanding of the socio-cultural context through community attitudes is required to address the stagnant suicide rates in Korea.
4.2 Limitations
While this study has several strengths, such as utilizing MDIS to categorize real-world suicide into specific populations and employing a factor structure supported by confirmatory factor analysis, it also presents some limitations. First, the study’s cross-sectional design precludes any meaningful discussions about causality. Causal inferences drawn from this study should be cautiously approached and require additional evidence. Second, an ecological study is subject to the ecological bias or fallacy, where the observed associations at the group level may differ from the actual associations at the individual level (80, 81). Thus, the regional-level associations observed in this study cannot be equated with individual-level associations, and we discussed the possibility that the associations between permissive attitudes and suicide mortality may differ at different levels. Third, the regression models remained simplistic because of the limited number of observations across 30 regions (82). A greater number of regional units would allow for considering various covariates and their interactions in a single model. Fourth, the factor scores from the ATTS were derived from an average of 50 participants per region, which is relatively small to ensure representativeness. This could introduce measurement errors in regional attitudes and potentially affect the study’s findings. Finally, while maintaining a relatively uniform cultural context within a single nation may be considered a strength from certain perspectives (83), it could also limit generalizability. It would be necessary to examine whether these associations can be replicated in different population and cultural contexts outside of South Korea.
5 Conclusion
In this study, we explored the relationship between suicide-related community attitudes and suicide mortality based on a nationwide survey and real-world suicide data in South Korea. Permissive attitudes were associated with reduced suicide mortality at the group level, with this relationship affecting males and individuals younger than 60 years more than their counterparts. It is imperative to note that attitudes may behave differently at the individual and group levels, and exercising caution when oversimplifying permissive attitudes as a risk factor is essential. Moreover, our findings show that community attitudes could play a vital role in shaping future strategies to address the gaps in Korean suicide prevention efforts. Although further studies are required, our findings might contribute to a deeper understanding of the modifiable social determinants of suicide and enhance early detection and intervention for individuals on the verge of suicide.
Data availability statement
Publicly available datasets were analyzed in this study. The 2018 Korea National Survey on Suicide data can be found at: Korean Statistical Information Service (https://kosis.kr/). Microdata on suicide mortality is available upon appropriate request from: MicroData Integrated System (https://mdis.kostat.go.kr/)
Ethics statement
The studies involving humans were approved by Institutional Review Board of Seoul National University Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MH: Conceptualization, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. HK: Methodology, Writing – review & editing. CP: Conceptualization, Project administration, Writing – review & editing. HL: Methodology, Writing – review & editing. SR: Formal analysis, Methodology, Writing – review & editing. SM: Writing – review & editing. MK: Writing – review & editing. JY: Writing – review & editing. YS: Writing – review & editing. KS: Writing – review & editing. YA: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was conducted in agreement in accordance with a research service agreement (grant number: 25183177900) with the Ministry of Health and Welfare, Republic of Korea. The funders of this study had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Acknowledgments
The authors acknowledge Professor E. S. Renberg for providing the original ATTS text and advice. We also thank the staff of Hankook Research, who conducted the survey’s field practice. During the preparation of this work the authors used chatGPT 4 (Open AI, California, United States) to enhance English language style. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1423609/full#supplementary-material
Abbreviations
IMV, integrated motivational-volitional model; 3ST, three-step theory; KNSS, Korea National Survey on Suicide; ATTS, Questionnaire on Attitudes Toward Suicide; PA, factor “Permissiveness”; UB, factor “Unjustified behavior”; RP, factor “Readiness to help/Preventability”; MDIS, MicroData Integrated System; IRR, incidence rate ratio; AIC, Akaike Information Criteria; BIC, Bayesian Information Criteria.
References
1. World Health Organization. Suicide Worldwide in 2019: Global Health Estimates. Geneva, World Health Organization (2021).
2. Organization for Economic Cooperation and Development. Suicide Rates (Indicator) (2022). Available online at: https://data.oecd.org/healthstat/suicide-rates.htm (Accessed 21 August, 2024).
3. Statistics Korea. 2021 Cause of Death Statistics (2022). Available online at: http://kosis.kr/ (Accessed 21 August, 2024).
4. Kim H, Kwon SW, Ahn YM, Jeon HJ, Park S, Hong JP. Implementation and outcomes of suicide-prevention strategies by restricting access to lethal suicide methods in Korea. J Public Health Policy. (2019) 40:91–102. doi: 10.1057/s41271-018-0152-x
5. Park SC, Na KS, Kwon SJ, Kim M, Kim HJ, Baik M, et al. Suicide care" (Standardized suicide prevention program for gatekeeper intervention in Korea): an update. Psychiatry Investig. (2020) 17:911–24. doi: 10.30773/pi.2020.0166
6. Jang J, Myung W, Kim S, Han M, Yook V, Kim EJ, et al. Effect of suicide prevention law and media guidelines on copycat suicide of general population following celebrity suicides in South Korea, 2005-2017. Aust N Z J Psychiatry. (2022) 56:542–50. doi: 10.1177/00048674211025701
7. Lee S-U, Park J-I, Lee S, Oh I-H, Choi J-M, Oh C-M. Changing trends in suicide rates in South Korea from 1993 to 2016: A descriptive study. BMJ Open. (2018) 8:e023144. doi: 10.1136/bmjopen-2018-023144
8. Korea Foundation for Suicide Prevention. 2022 White Paper on Suicide Prevention (2022). Available online at: https://www.kfsp.or.kr/ (Accessed 21 August, 2024).
9. Dai J, Zhong BL, Xiang YT, Chiu HF, Chan SS, Yu X, et al. Internal migration, mental health, and suicidal behaviors in young rural Chinese. Soc Psychiatry Psychiatr Epidemiol. (2015) 50:621–31. doi: 10.1007/s00127-014-0985-y
10. Gili M, Castellví P, Vives M, de la Torre-Luque A, Almenara J, Blasco MJ, et al. Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. J Affect Disord. (2019) 245:152–62. doi: 10.1016/j.jad.2018.10.115
11. Zhong BL, Xie WX, Zhu JH, Lu J, Chen H. Prevalence and correlates of suicide attempt among Chinese individuals receiving methadone maintenance treatment for heroin dependence. Sci Rep. (2019) 9:15859. doi: 10.1038/s41598-019-52440-x
13. Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE Jr. The interpersonal theory of suicide. Psychol Rev. (2010) 117:575–600. doi: 10.1037/a0018697
14. Joiner TE. Why People Die by Suicide. Cambridge, MA: Harvard University Press (2005). doi: 10.2307/j.ctvjghv2f
15. O'Connor RC. Towards an integrated motivational-volitional model of suicidal behaviour. In: International Handbook of Suicide Prevention: Research, Policy and Practice. Wiley Blackwell, Hoboken, NJ, US (2011). p. 181–98. doi: 10.1002/9781119998556.ch11
16. Klonsky ED, May AM. The three-step theory (3st): A new theory of suicide rooted in the “Ideation-to-action” Framework. Int J Cognit Ther. (2015) 8:114–29. doi: 10.1521/ijct.2015.8.2.114
18. Lee H, Park CHK, Rhee SJ, Kim J, Kim B, Lee SS, et al. An integrated model for the relationship between socio-cultural factors, attitudes toward suicide, and intensity of suicidal ideation in Korean, Japanese, and American populations. J Affect Disord. New York, NY (2021) 280:203–10. doi: 10.1016/j.jad.2020.10.042
19. Lee H, Kim MJ, Hong M, Rhee SJ, Shin D, Park J-I, et al. Effect of suicidal loss on bereaved individuals' Suicidal ideation: structural equation model using attitudes towards suicide scale and moderation effect of interest in news media. J Affect Disord. (2022) 298:51–7. doi: 10.1016/j.jad.2021.10.085
20. Kleiman EM. Suicide acceptability as a mechanism of suicide clustering in a nationally representative sample of adolescents. Compr Psychiatry. (2015) 59:17–20. doi: 10.1016/j.comppsych.2015.02.002
21. Kerkhof A, Natawat S, World Health Organization. Suicidal behavior and attitudes towards suicide among students in India and the Netherlands. In: Diekstra RF, editor. Suicide and Its Prevention: The Role of Attitude and Imitation. Brill, Leiden (1989). p. 144–59.
22. Limbacher M, Domino G. Attitudes toward Suicide among Attempters, Contemplators, and Nonattempters. Omega. (1986) 16:325–34. doi: 10.2190/XG9Y-1H7L-JHD7-VU86
23. Stein D, Brom D, Elizur A, Witztum E. The association between attitudes toward suicide and suicidal ideation in adolescents. Acta Psychiatr Scand. (1998) 97:195–201. doi: 10.1111/j.1600-0447.1998.tb09987.x
24. Arnautovska U, Grad OT. Attitudes toward suicide in the adolescent population. Crisis. (2010) 31:22–9. doi: 10.1027/0227-5910/a000009
25. Renberg ES, Jacobsson L. Development of a questionnaire on attitudes towards suicide (Atts) and its application in a swedish population. Suicide Life Threat Behav. (2003) 33:52–64. doi: 10.1521/suli.33.1.52.22784
26. Kodaka M, Inagaki M, Poštuvan V, Yamada M. Exploration of factors associated with social worker attitudes toward suicide. Int J Soc Psychiatry. (2013) 59:452–9. doi: 10.1177/0020764012440674
27. Zemaitiene N, Zaborskis A. Suicidal tendencies and attitude towards freedom to choose suicide among Lithuanian schoolchildren: results from three cross-sectional studies in 1994, 1998, and 2002. BMC Public Health. (2005) 5:83. doi: 10.1186/1471-2458-5-83
28. McAuliffe C, Corcoran P, Keeley HS, Perry IJ. Risk of suicide ideation associated with problem-solving ability and attitudes toward suicidal behavior in university students. Crisis. (2003) 24:160–7. doi: 10.1027//0227-5910.24.4.160
29. Hong M, Park J-I, Lee S-U, Shin M-S, Ahn Y. Factor structure of attitudes toward suicide (Atts) of adults: based on a nationwide survey in South Korea. Korean J Biol Psychiatry. (2019) 26:71–8. doi: 10.22857/kjbp.2019.26.2.006
30. Hom MA, Stanley IH, Duffy ME, Davis L, Joiner TE. Examining the relationship between attitudes toward suicide and suicide attempt history. Crisis. (2019) 40:265–72. doi: 10.1027/0227-5910/a000564
31. Cwik JC, Till B, Bieda A, Blackwell SE, Walter C, Teismann T. Measuring attitudes towards suicide: preliminary evaluation of an attitude towards suicide scale. Compr Psychiatry. (2017) 72:56–65. doi: 10.1016/j.comppsych.2016.09.008
32. Centers for Disease Control and Prevention. Suicide Prevention Resource for Action: A Compilation of the Best Available Evidence. Atlanta, GA: National Center for Injury Prevention and Control (2022).
33. Korea Foundation for Suicide Prevention. 2021 Report of Psychological Autopsy Interview (2022). Available online at: https://www.kfsp.or.kr/ (Accessed 21 August, 2024).
34. Lim M, Lee SU, Park J-I. Difference in suicide methods used between suicide attempters and suicide completers. Int J Ment Health Syst. (2014) 8:54. doi: 10.1186/1752-4458-8-54
35. Neeleman J, Halpern D, Leon D, Lewis G. Tolerance of suicide, religion and suicide rates: an ecological and individual study in 19 western countries. Psychol Med. (1997) 27:1165–71. doi: 10.1017/s0033291797005357
36. Reynders A, Kerkhof AJFM, Molenberghs G, Van Audenhove C. Stigma, attitudes, and help-seeking intentions for psychological problems in relation to regional suicide rates. Suicide Life Threat Behav. (2016) 46:67–78. doi: 10.1111/sltb.12179
37. Sale I, Williams CL, Clark J, Mills J. Suicide behavior: community attitudes and beliefs. Suicide. (1975) 5:158–68. doi: 10.1111/j.1943-278X.1975.tb00324.x
38. Lash TL, Rothman KJ, VanderWeele TJ, Haneuse S. Modern Epidemiology. Philadelphia: Wolters Kluwer (2020).
39. Cramer RJ, Kapusta ND. A social-ecological framework of theory, assessment, and prevention of suicide. Front Psychol. (2017) 8:1756. doi: 10.3389/fpsyg.2017.01756
40. Rodríguez-Otero JE, Campos-Mouriño X, Meilán-Fernández D, Pintos-Bailón S, Cabo-Escribano G. Where is the social in the biopsychosocial model of suicide prevention? Int J Soc Psychiatry. (2022) 68:1403–10. doi: 10.1177/00207640211027210
41. Seoul National University College of Medicine. 2018 Korea National Survey on Suicide. Ahn YM, editor. Sejong: Ministry of Health and Welfare (2019).
42. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (Strobe) statement: guidelines for reporting observational studies. Prev Med. (2007) 45:247–51. doi: 10.1016/j.ypmed.2007.08.012
43. Kodaka M, Postuvan V, Inagaki M, Yamada M. A systematic review of scales that measure attitudes toward suicide. Int J Soc Psychiatry. (2011) 57:338–61. doi: 10.1177/0020764009357399
44. Seoul National University College of Medicine. 2013 Korea National Survey on Suicide. Ahn YM, editor. Sejong: Ministry of Health and Welfare (2014).
45. Kim MJ, Lee H, Shin D, Hong M, Rhee SJ, Park J-I, et al. Effect of attitude toward suicide on suicidal behavior: based on the korea national suicide survey. Psychiatry Investig. (2022) 19:427–34. doi: 10.30773/pi.2021.0361
46. Brown TA. Specification and interpretation of cfa models. In: Confirmatory Factor Analysis for Applied Research, 3rd ed. Guilford Publications, New York, NY (2015). p. 88–138.
48. Statistics Korea. Microdata Integrated Service (2022). Available online at: https://mdis.kostat.go.kr/ (Accessed 21 August, 2024).
49. Statistics Korea. Korean Standard Classification of Diseases 7th ed. (2015). Available online at: https://www.koicd.kr/kcd/kcd.do (Accessed 21 August, 2024).
50. Ver Hoef JM, Boveng PL. Quasi-poisson vs. Negative binomial regression: how should we model overdispersed count data? Ecology. (2007) 88:2766–72. doi: 10.1890/07-0043.1
51. Choi JW, Kim TH, Shin J, Han E. Poverty and suicide risk in older adults: A retrospective longitudinal cohort study. Int J Geriatr Psychiatry. (2019) 34:1565–71. doi: 10.1002/gps.5166
52. Kim JW, Jung HY, Won DY, Shin YS, Noh JH, Kang TI. Landscape of elderly suicide in South Korea: its trend according to age, gender, and educational attainment. Omega. (2020) 82:214–29. doi: 10.1177/0030222818807845
53. Callanan VJ, Davis MS. Gender differences in suicide methods. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:857–69. doi: 10.1007/s00127-011-0393-5
54. McGirr A, Séguin M, Renaud J, Benkelfat C, Alda M, Turecki G. Gender and risk factors for suicide: evidence for heterogeneity in predisposing mechanisms in a psychological autopsy study. J Clin Psychiatry. (2006) 67:1612–7. doi: 10.4088/jcp.v67n1018
55. Conwell Y, Van Orden K, Caine ED. Suicide in older adults. Psychiatr Clin North Am. (2011) 34:451–68. doi: 10.1016/j.psc.2011.02.002
56. Stanley IH, Hom MA, Rogers ML, Hagan CR, Joiner TE Jr. Understanding suicide among older adults: A review of psychological and sociological theories of suicide. Aging Ment Health. (2016) 20:113–22. doi: 10.1080/13607863.2015.1012045
57. R Core Team. R: A Language and Environment for Statistical Computing V4.2.2 (2022). Vienna. Available online at: https://www.r-project.org/ (Accessed 21 August, 2024).
58. Rosseel Y. Lavaan: an R package for structural equation modeling. J Stat Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
59. Lumley T. Analysis of complex survey samples. J Stat Softw. (2004) 9:1–19. doi: 10.18637/jss.v009.i08
60. Venables WN, Ripley BD. Modern Applied Statistics with S. 4th ed. New York, NY: Springer (2002).
61. Burt ME, Park N. Education inequality in the Republic of Korea: measurement and causes. In: Holsinger DB, Jacob WJ, editors. Inequality in Education: Comparative and International Perspectives. Springer Netherlands, Dordrecht (2009). p. 261–89. doi: 10.1007/978-90-481-2652-1_11
62. Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. (2016) 12:307–30. doi: 10.1146/annurev-clinpsy-021815-093204
63. Pitman A, Nesse H, Morant N, Azorina V, Stevenson F, King M, et al. Attitudes to suicide following the suicide of a friend or relative: A qualitative study of the views of 429 young bereaved adults in the UK. BMC Psychiatry. (2017) 17:400. doi: 10.1186/s12888-017-1560-3
64. Ammerman BA, Piccirillo ML, O'Loughlin CM, Carter SP, Matarazzo B, May AM. The role of suicide stigma in self-disclosure among civilian and veteran populations. Psychiatry Res. (2022) 309:114408. doi: 10.1016/j.psychres.2022.114408
65. Abo-Rass F, Abu-Kaf S, Matzri D, Braun-Lewensohn O. Mental health underutilization by palestinian-arabs in Israel: stigma-related, attitudinal, and instrumental barriers. Int J Soc Psychiatry. (2023) 69:1015–23. doi: 10.1177/00207640231152213
66. Sharp M-L, Fear NT, Rona RJ, Wessely S, Greenberg N, Jones N, et al. Stigma as a barrier to seeking health care among military personnel with mental health problems. Epidemiol Rev. (2015) 37:144–62. doi: 10.1093/epirev/mxu012
67. Klonsky ED, Pachkowski MC, Shahnaz A, May AM. The three-step theory of suicide: description, evidence, and some useful points of clarification. Prev Med. (2021) 152:106549. doi: 10.1016/j.ypmed.2021.106549
68. O'Connor RC, Kirtley OJ. The integrated motivational-volitional model of suicidal behaviour. Philos Trans R Soc Lond B Biol Sci. (2018) 373:20170268. doi: 10.1098/rstb.2017.0268
69. Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. (1998) 28:1–23. doi: 10.1111/j.1943-278X.1998.tb00622.x
70. Hur JW, Lee BH, Lee SW, Shim SH, Han SW, Kim YK. Gender differences in suicidal behavior in Korea. Psychiatry Investig. (2008) 5:28–35. doi: 10.4306/pi.2008.5.1.28
71. Rüsch N, Angermeyer MC, Corrigan PW. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma. Eur Psychiatry. (2005) 20:529–39. doi: 10.1016/j.eurpsy.2005.04.004
72. Chung Ang University. Suicide Perception Survey. Seoul: Korea Health Promotion Institute (2013).
73. An S, Lee H, Lee J, Kang S. Social stigma of suicide in South Korea: A cultural perspective. Death Stud. (2023) 47:259–67. doi: 10.1080/07481187.2022.2051096
74. McNeish D. Thanks coefficient alpha, we'll take it from here. Psychol Methods. (2018) 23:412–33. doi: 10.1037/met0000144
75. Kodaka M, Inagaki M, Yamada M. Factors associated with attitudes toward suicide: among Japanese pharmacists participating in the board certified psychiatric pharmacy specialist seminar. Crisis. (2013) 34:420–7. doi: 10.1027/0227-5910/a000219
76. Ko Y, Youn H, Lee SI, Lee J, Lee A, Kim SG. The effect of suicide prevention education on attitudes toward suicide in police officers. Psychiatry Investig. (2021) 18:1076–81. doi: 10.30773/pi.2021.0176
77. Eskin M. The effects of individualistic-collectivistic value orientations on non-fatal suicidal behavior and attitudes in Turkish adolescents and young adults. Scand J Psychol. (2013) 54:493–501. doi: 10.1111/sjop.12072
78. Haneuse S, Bartell S. Designs for the combination of group- and individual-level data. Epidemiology. (2011) 22:382–9. doi: 10.1097/EDE.0b013e3182125cff
79. Hox J, Moerbeek M, van de Schoot R. Sample sizes and power analysis in multilevel regression. In: Multilevel Analysis: Techniques and Applications, 3rd ed. Routledge (2017). doi: 10.4324/9781315650982
80. Wakefield J. Ecologic studies revisited. Annu Rev Public Health. (2008) 29:75–90. doi: 10.1146/annurev.publhealth.29.020907.090821
81. Morgenstern H, Wakefield J. Ecologic studies and analysis. In: Lash TL, Rothman KJ, VanderWeele TJ, Haneuse S, editors. Modern Epidemiology, 4th ed. Wolters Kluwer, Philadelphia (2020).
82. Dufault B, Klar N. The quality of modern cross-sectional ecologic studies: A bibliometric review. Am J Epidemiol. (2011) 174:1101–7. doi: 10.1093/aje/kwr241
Keywords: suicidal ideation, completed suicide, attitudes toward suicide, suicide rate, social stigma, risk factors, general population survey, suicide prevention
Citation: Hong M, Kim H, Park CHK, Lee H, Rhee SJ, Min S, Kim MJ, Yang JH, Song Y, Son K and Ahn YM (2024) Effect of community attitudes on suicide mortality in South Korea: a nationwide ecological study. Front. Psychiatry 15:1423609. doi: 10.3389/fpsyt.2024.1423609
Received: 26 April 2024; Accepted: 26 August 2024;
Published: 16 September 2024.
Edited by:
Ricardo Gusmão, University of Porto, PortugalReviewed by:
Matias E. Rodriguez-Rivas, Universidad de Desarrollo, ChileYan-Min Xu, Wuhan Mental Health Center, China
Copyright © 2024 Hong, Kim, Park, Lee, Rhee, Min, Kim, Yang, Song, Son and Ahn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Min Ahn, YXltQHNudS5hYy5rcg==