 Franziska Langner1*
Franziska Langner1* Anna Katharina Börke1Patric Muschner1Maria Muther2Andreas Reichelt3
Anna Katharina Börke1Patric Muschner1Maria Muther2Andreas Reichelt3 Gerd-Dieter Willmund1
Gerd-Dieter Willmund1 Ulrich Wesemann1Peter Lutz Zimmermann1Isabel Schönsee1
Ulrich Wesemann1Peter Lutz Zimmermann1Isabel Schönsee1- 1Bundeswehr Center for Military Mental Health, Military Hospital Berlin, Berlin, Germany
- 2Department of Marriage, Family And Life Councelling, Diocese Augsburg, Augsburg, Germany
- 3Department of Occupational Medicine, Sanitätsunterstützungszentrum Berlin, Berlin, Germany
Introduction: Given a high amount of workplace stressors, burnout syndrome, as a depression-related syndrome, is highly relevant for medical service soldiers. This study aims to examine their effects with regard to moral injuries and personal values following foreign deployment.
Materials and methods: This longitudinal study included 91 soldiers of the German Armed Forces Medical Service. Participants completed the Maslach Burnout Inventory (MBI) and the Portrait-Value-Questionnaire (PVQ) before and after a foreign deployment as well as the Moral Injury Scale (SMBE) after deployment. Analysis has been conducted using t-tests to assess potential changes in MBI and PVQ scales between pre-test - t1 (2-4 weeks before deployment) and post-test – t2 (up to 6 months after deployment). In addition, correlations were examined between moral injuries (MI) after deployment and MBI scores at t1 and t2 as well as between personal values (PVQ t1) and MBI scores at t1 and t2.
Results: The MBI subscales showed mild to moderate burnout symptoms at both pre- and post-tests, with a slight deterioration during the study period, albeit not significant. There were no significant mean differences in PVQ between measurement points. Nevertheless, PVQ self-direction and tradition at t1 correlated negatively with MBI INV at t2 (PVQ SD r = -.21, p = .043) and MBI PA at t2 (PVQ TR r = -.23, p = .027). Furthermore, the subscale PVQ power at t1 correlated positively with MBI PA at t2 (PVQ PO r = .28, p = .006), meanwhile PVQ universalism at t1 correlated positively with MBI INV at t1 (PVQ UN r = .25, p = .018). Furthermore, positive correlations were found between moral injuries at t2 (SMBE total score, SMBE_Sub1, SMBE_Sub2) and MBI subscales Emotional Exhaustion (EE; r = -.54, p = .001), Depersonalization (DP; r = .38, p = .001), and Involvement (INV; r = .30, p = .004) before and after the deployment period. No correlation was found between MI and MBI subscale Personal Accomplishment (PA).
Conclusion: The results indicate that medical service soldiers exhibit mild to moderate burnout symptoms even before deployment. Significant associations between moral injuries and burnout were found in 3 out of 4 MBI subscales (EE, DP, INV). There was a significant association with a stronger moral injury and higher burnout levels, persisting both before and after the study period. Furthermore, our results suggest that personal value orientations might be meaningful predictors of burnout. Hence, causal questions regarding general work stress among medical service soldiers should be further explored in more detailed studies. Further research could lay the foundation for future approaches in psychotherapy as well as primary and secondary prevention in this field.
Introduction
For over 20 years, Germany has witnessed an increase in burnout cases (1, 2). A meta-analysis (3) on the burnout syndrome revealed a reciprocal relationship between work-related stress and burnout. Burnout syndrome is characterized by three dimensions: feelings of energy depletion or exhaustion, increased mental distance from one’s job or work-related feelings of negativism or cynicism, as well as reduced professional efficacy. While commonly associated with mental disorders, burnout syndrome is not recognized as a distinct mental illness in the ICD classification of mental disorders. However, it can be coded as a comorbid feature in relation in coping with life’s challenges (4, 5). Due to heterogeneous definition criteria for burnout syndrome, quantifying the overall prevalence and delineating it in terms of differential diagnosis is difficult (6, 7). Meta-analyses have shown significant associations between exhaustion components of burnout syndrome (8) and depression (r = 0.520, SE = 0.012, 95% CI = 0.492, 0.547) as well as between burnout syndrome and anxiety (9) (r = 0.460, SE = 0.014, 95% CI = 0.421, 0.497). In contrast to the solely work-related genesis of burnout syndrome, studies such as those by Khammissa (10) suggest that both exogenous work-related and endogenous personal factors determine the extent and severity of symptoms.
Various studies on the prevalence of burnout syndrome in specific occupational groups revealed that professions with helping and counseling attitudes, such as healthcare, nursing or in the pedagogical field, are often affected more than other professional groups (11–13). Medical personnel play a distinct role, as workload and burnout syndrome as well as burnout syndrome and medical error rates (14) correlate positively among physicians in general (15) and emergency physicians in particular (14, 16–18).
In civilian cohorts of this occupational group, the emergence of psychological distress has been associated with workplace conditions such as experienced violence (19), the characteristics of critical events (20, 21), including ethical considerations (22), psychosocial factors (23), and the presence of resources (24). Military medical personnel may face additional stressors, such as experiencing personal threat or combat exposure during overseas deployment, which in turn may increase the risk for ill health (25, 26) and burnout (13). Consequently, studying burnout and mental health within military contexts becomes increasingly relevant.
Burnout syndrome and mental disorders in the military
The prevalence of burnout syndrome among military personnel seems slightly lower than in society at large (11). Nevertheless, in line with findings from civilian studies (27, 28), certain military specializations show an increased likelihood of burnout syndrome (29), including personnel in operational roles, flight crews, and medical personnel, particularly in intensive care. Already in 2011, Eisenlohr et al. (6) highlighted the significance of burnout syndrome within the general medical care setting of the German Armed Forces, pointing out specific challenges in the military work environment. Differences are also reflected in specialties of military health care workers, with emergency physicians exhibiting higher levels of burnout than orthopedic surgeons (30).
Other studies have emphasized overseas deployment as a specific risk factor regarding burnout symptomatology. For instance, a study of US military personnel reported a positive correlation between the number of completed overseas deployments and an increased risk of burnout syndrome (31). Adler et al. (13) demonstrated a correlation between the perception of occupational stress among military medical personnel deployed overseas and burnout levels.
Overseas deployments put physical and psychological strains on soldiers. Comparing German soldiers with and without deployments abroad in 2012, the 12-month prevalence of PTSD increased from 0.3% to nearly 3%, with an estimated number of unreported cases of about 50% (32). The prevalence of mental disorders among deployed participants in a study of the German Armed Forces was 21.4% (33, 34). Previous studies have shown that the 12-month prevalence of mental disorders in German soldiers without deployment history is comparable to that of the general population (35). Research indicates that it is not the deployment itself, but instead high combat exposure with threats to life and physical integrity that is linked with increased prevalence rates of anxiety disorders and PTSD (35, 36). An international study demonstrated varying prevalence rates depending on the sending country and the deployment region (36). The stressors faced by soldiers during overseas deployments are likely to favor the phenomenon of burnout syndrome. Further insights could be provided by studies examining emotional stress (37) and the development of depressive disorders and anxiety disorders (20, 38) during deployment, as these show similarities with the symptoms of burnout syndrome (39, 40).
Moral injury in the context of foreign deployment
In addition, soldiers on deployment may face traumatic experiences that challenge their individualized psychological value systems. These conflicts often arise from the disparity between internalized Western-liberal values and prevailing views in the country of deployment. Litz et al. (41) have introduced the concept of “moral injury” (MI), in which soldiers are morally burdened by experiences during deployment, either by their own offenses (e.g. exercising or witnessing disproportionate violence), or when they themselves do not act or are not allowed to act (“leadership decisions that were life-ending”, “neglect”). Depending on the type (42) of PMIES (stemming from the actions of self and other), Dale et al. (43) showed an increased risk of specific mental illnesses (self MI: more burnout syndromes/depression, other MI: more anxiety).
Other authors define moral injury as betrayal by authority figures in extreme situations (44), actions that contradict one’s own moral convictions (45) or as breaks in the moral self-concept that cause intense emotional reactions such as guilt and shame (46). Such experiences can have a profound impact on psychological well-being and the integrity of moral character (47). Moral character is seen as dynamic and malleable, influenced by personal experiences, cultural norms and social interactions (48). Moral dissonances, which arises when a person performs actions or witnesses’ events that contradict their moral beliefs (47), can undermine confidence in one’s own moral judgment and sow doubt in one’s own moral integrity.
The consequences of MI are negative feelings and cognitive dissonance. If these cannot be reduced, they can lead to secondary mental illnesses, accompanied by feelings of guilt and shame (41, 49). Studies (48, 50–52) show that MI, like the confrontation with adversity and the killing of opponents, increase the frequency of mental illness after deployment. The moral fragmentation that those affected experience when their actions and beliefs do not coincide also leads to an incoherent perception of their own moral principles (48). In addition, MI represents a differentially mediating variable between the stressor “confrontation with hardship, suffering, violence in the population” and the psychological syndromes “PTSD” and “depression” on the one hand and “burnout syndrome” and alcohol abuse on the other (53, 54).
Moral injury and burnout are two different but often co-occurring phenomena that occur in the context of occupational stress (41). Both can have serious psychological and physical consequences for those affected, but their causes, manifestations and effects differ considerably. In the military context, moral injury results from acts of violence or witnessing civilian casualties, leading to moral dilemmas (42, 48) or from situations in which medical personnel have to deal with end-of-life decisions or medical errors (55, 56). Burnout, on the other hand, is caused by chronic professional overload and emotional stress, e.g. intense physical and psychological demands as well as traumatic events lead to burnout (57) or the emotional strain of dealing with seriously ill patients by medical staff (58, 59). So far it is unknown, whether moral injury leads to higher or lower levels of burnout. For the first time, this research paper addresses this question in order to provide some preliminary results on this topic.
Personal values as influencing factors of mental health
In the medical context (medical service), unresolvable feelings of guilt, shame and self-blame (e.g. due to limited medical resources for the further treatment of locals in the war zone), the experience of potentially morally injurious events (PMIE) and resulting conflicts between personal and professional values may increase the risk for mental illness (53, 60). Furthermore, initial research suggests that values may also play an important role in predicting levels of burnout and engagement (61) as well as mental health (62). From a theoretical perspective, values have also been integrated into the areas of worklife model of burnout as one of six key areas in which a person-job imbalance might affect an individual’s level of experienced burnout (7, 61, 63). It therefore seems necessary to examine personal value orientations in relation to mental health and burnout more closely.
Values, as central beliefs that guide behavior and attitudes, have been identified in several studies (50, 64–66) as personality-related influencing factors in the development and progress of mental health (65). Long-term studies and cognitive consistency theories demonstrate the relative stability (Bardi 2003) of values in adulthood. Biological and developmental psychology perspectives (67, 68) complement this view by examining the role of socialization and genetic factors in the formation of values. Schwartz (69, 70). identified ten types of values (see Table 1), which represent different motivational goals deriving from overarching universal human needs. An extensive overview of the relationship between value orientations and mental health is given by Heim et al. (71).
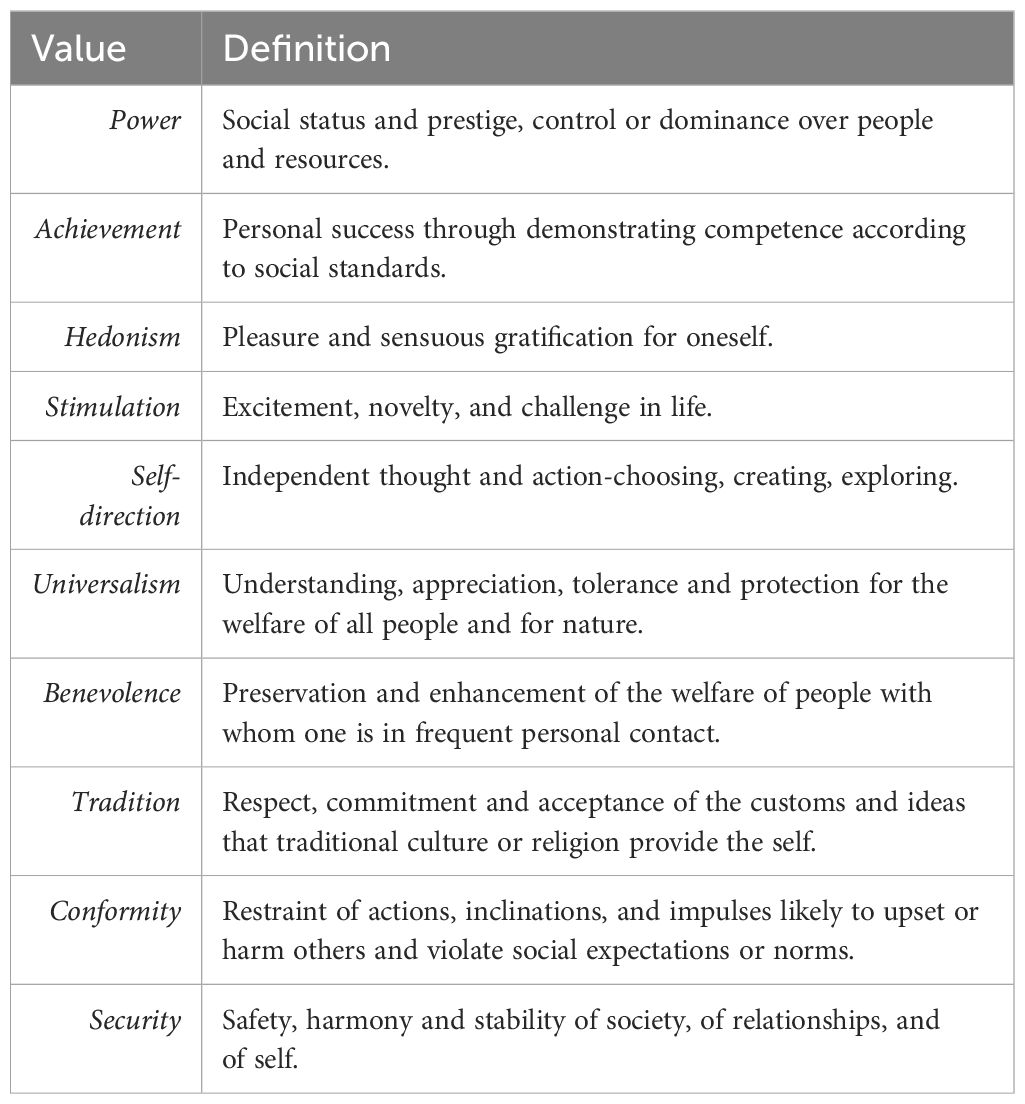
Table 1. Definitions of ten value constructs in terms of their goals (70).
Meanwhile the majority of previous research demonstrates the stability of personal value orientations (72–75), more recent research, such as that by Bardi et al. (73), challenges the theory of value stability and shows that specific events such as the COVID-19 pandemic or terroristic attacks can cause temporary changes in values. The studies by Bojanowska et al. (76) and Daniel et al. (77) suggest that exceptional circumstances such as a pandemic can lead to temporary adjustments in values that do not necessarily reflect long-term changes.
The distinction between temporary and stable changes in values requires a differentiated view of time perspectives and contexts. In the context of foreign assignments, stressful experiences can trigger temporary changes in values by stimulating a reflection or reassessment of life goals and convictions (78, 79) or by raising existential questions. In addition, it seems that people under stress can temporarily adapt their values in order to cope better with challenges (80). Nevertheless, studies show that fundamental values remain stable over longer periods of time and can serve as orientation systems and sources of resilience in stressful situations (81, 82).
So far, we only identified one study reporting on personal values and mental health in the military context (83). Here, certain value types have been identified as commonly held by soldiers, such as benevolence and universalism. These seem to support moral professional conduct but also make individuals more susceptible to moral conflicts. Conversely, individuals who are more materially oriented and less compassionate (high hedonism) may be protected from such stressors. Further evidence in this field of research is missing. Hence, in order to address this research gap, we examine personal values in the military context looking more closely at their association with burnout and their stability over time.
Objectives and hypotheses
To date, studies on the development of burnout syndrome among medical personnel in the German Armed Forces considering personal value orientations and moral injuries in overseas deployments are missing. It seems that value orientations and moral injuries influence the pathogenesis of mental illnesses and are influenced by participation in military deployments (50, 66). Overall, our study underscores the importance of understanding burnout syndrome, particularly in military contexts, and highlights the need to examine how value change and how MI contribute to soldiers’ burnout symptoms after deployment.
This project provides initial results on the relationship between burnout symptoms, value orientations, and moral injury among medical personnel of the German Armed Forces deployed in overseas missions. We hypothesize that 1) there will be an increase in burnout symptomatology after the deployment period, 2) personal values are associated with burnout and remain stable even after a six months period after deployment and 3) a stronger experience of moral injury is associated with significantly higher levels of burnout.
Materials and methods
Sample
In this quantitative study, 91 medical soldiers were surveyed via structured questionnaires between December 2014 and November 2016. The study population represents the official proportion of female soldiers in the German medical service of 44.6% and was not specifically selected.
Participants were recruited during a routine health examination (BA90/5) preceding their deployment to various missions abroad (e.g., Afghanistan, Mali, Kosovo). Participation in the study was optional, with interested individuals being briefed about the research project during individual consultations with study personnel. Participants were required to have a minimum deployment duration of 30 days and meet the age criteria of 20-60 years. Exclusion and discontinuation criteria included acute mental illness, suicidality, or concurrent participation in another study.
Research procedure
The study was conducted in accordance with the Declaration of Helsinki guidelines. A positive ethics vote from the Humboldt University of Berlin (Charité) was obtained (No. EA1/203/13). All patients gave informed written consent for an examination and voluntarily participated in the study. The study was registered by the Bundeswehr Medical Academy under a special research number 07-K4-S321315. There was no third-party funding.
The participants were examined at two times of measurement. The pretest (t1) was conducted 2-4 weeks before deployment (Maslach Burnout Inventory + Portrait Value Questionnaire). The posttest (t2) was conducted up to 6 months after the end of the deployment (Maslach Burnout Inventory + Portrait Value Questionnaire + Moral Injury Event Scale). Immediate post-measurement was omitted due to difficult scheduling of out-of-mission dates, frequent subsequent vacation and rest days, and other personal reasons of the participants.
Measures
Maslach burnout inventory
The Maslach Burnout Inventory (MBI) in its German version (84) consists of 25 items comprising four subscales: emotional exhaustion (EE; 9 items), depersonalization (DP; 5 items), personal accomplishment (PA; 8 items), and involvement (INV; 3 items). Participants rated themselves on a seven-point intensity scale ranging from 0 (= never) to 6 (= daily). Whereas the subscales EE, DP and PA showed acceptable inter-item correlations of α = .88, α = .82 and α = .72, respectively, the inter-item correlation of the subscale INV was α = .53. Despite the low inter-item correlation, INV was also surveyed in order to check whether it is particularly important for military medical personnel. For example, a high level of involvement could indicate a lower capacity for self-detachment and thus represent a stressor that has a negative effect on the individual’s energy balance and a positive effect on increasing burnout. Means and standard deviation for MBI-HSS scales can differ among different occupational groups. Maslach (85), for example, reports on a group of medical personnel (N = 1104, MBI EE M = 22.19, SD = 9.53; MBI DP M = 7.12, SD = 5.22, MBI PA M = 36.53, SD = 7.34) whose standard values differ from Mental health personal (N = 730, MBI EE M = 16.89, SD = 8.90; MBI DP M = 5.72, SD = 4.62, MBI PA M = 30.87, SD = 6.37).
The MBI manual (63) defined burnout (BO) cutoff values for each item with “low”, “medium” and “high” levels of burnout (MBI EE low <16, med = 18-29, high >30; MBI DP low <5, med 6-7-, high >12; MBI PA low <33, med 34-39, high >40) by dividing the normative sample into three equally-sized groups of 33.3%. A differentiation is made between the normative data of medical personnel (N = 1104, MBI EE M = 22.19, SD = 9.53; MBI DP M = 7.12, SD = 5.22, MBI PA M = 36.53, SD = 7.34) and mental health personnel (N = 730, MBI EE M = 16.89, SD = 8.90; MBI DP M = 5.72, SD = 4.62, MBI PA M = 30.87, SD = 6.37). The lack of external validation and the rather arbitrary test construction prevent these cutoff values and severity classifications from constituting diagnostically valid instruments for medical practice. Therefor the cut-off scores were removed in the latest version of MBI-HSS MP. For research purposes, the values of the individual scales continue to be used to assess the BO level: higher values of the EE, DP and INV scales indicate a higher degree of burnout, lower values of the PA scale indicate a higher degree of BO (86, 87).
Portrait value questionnaire
The Portrait Value Questionnaire (PVQ) comprises 40 items (69, 88) and assesses the expression of ten value types (e.g., power, achievement, security). Participants rate themselves on a 6-point Likert scale (1 = very dissimilar; 6 = very similar). Internal consistency ranges from α = .35–.83, and test-retest reliability (82) ranges from.62 to.82.
Moral injury event scale
The Moral Injury Event Scale (SMBE) includes 9 items and assesses the burden on participants caused by events that violate moral beliefs and values via a 6-point Likert scale (1 = strongly disagree, 6 = strongly agree). Item responses were averaged, such that higher scores on the SMBE correspond to a greater intensity of exposure and distress (49). In the German version, internal consistencies for moral injury caused by others (SUB1, 5 items) and for betrayal of moral standards (50) due to one’s own misconduct (SUB 2, 4 items) ranged from α = .82 to α = .78, respectively.
Statistics
Data analysis was conducted using IBM Statistics SPSS 25. Initially, a descriptive analysis of the sample was performed based on sociodemographic information and the assessment of burnout symptoms. To examine whether differences occurred over time, a paired sample t-test was used. The requirements for the t-test were met. A test for normal distribution was omitted, as simulation studies show that the t-test is robust to this violation (89). Furthermore, changes in value orientations over time were examined using a t-test for related samples.
Additionally, Pearson correlation analyses were conducted to see if there was a correlation between Moral Injury (SMBE total score, SUB 1, and SUB 2) and Burnout (EE, PA, DP, IV) subscales. The prerequisites for a correlation (interval scaled variables, linearity) were met. Outliers were left in the data set. The sample size was determined using G-Power. Method used: Correlation, Bivariate normal model. In a power analysis conducted based on a conservatively estimated Pearson correlation of r = 0.3 (mean effect), alpha error =.05 and power (1-beta err. prob.) = 0.80 the minimum sample size (total sample size) is N = 67.
Results
Sample description
In total, 91 medical soldiers, including male (N=48; 52.7%) and female (N=43; 47.3%) soldiers with an average age of 33.55 years (SD = 6.07) took part in this study. Of these, 80.3% reported being in a relationship, while 19.8% reported being single. Overall, 75.8% belonged directly to the Medical Service section of the armed service, while the remaining participants were soldiers from other military services such as the Land Forces (8.8%), the Air Force (4.4%), and the Navy (2.2%). No information regarding the specific area of service was provided by 8.8% of the participants. The various ranks, which reflect the hierarchy within the German Armed Forces, are broken down as follows, from the lowest (enlisted ranks), through the middle (non-commissioned officers) to the highest ranks (officers): 6.6% NATO rank OR-1 to OR-4, 48.4% NATO rank OR-5 to OR-9, 44% NATO rank OF-1 to OF-5 and 1.1% provided no information.
The deployment was the first overseas assignment for 45.1% of the participants. The other participants had previously participated in an average of 4.60 deployments (SD = 12.82; Mode = 1), the average duration was 238.83 days (SD = 204.89). In the current deployment, participants were deployed to various operational areas of the German Armed Forces (45.1% Kosovo; 36.3% Afghanistan; 9.9% Mali; 5.5% other areas; 3.3% no information provided.
MBI
The initial mean values of the MBI (see Table 2) in our study sample showed deviating values in individual subscales compared to the normative samples, depending on the occupational subgroup. For example, medical personnel show lower levels in EE and DP as well as a higher level in PA than our study sample. In comparison to the subgroup of mental health personnel the reported means of EE, DP and PA are higher. Using the burnout cutoff values the MBI subscales Depersonalization (MBI_DP Mt1 = 6.93) and Personal Accomplishment (MBI_PA Mt1 = 36.76) indicated a moderate level of burnout at t1. The scales Emotional Exhaustion (MBI_EE Mt1 = 17.0) and Involvement (MBI_INV Mt1 = 3.72) reflected a low level of burnout.
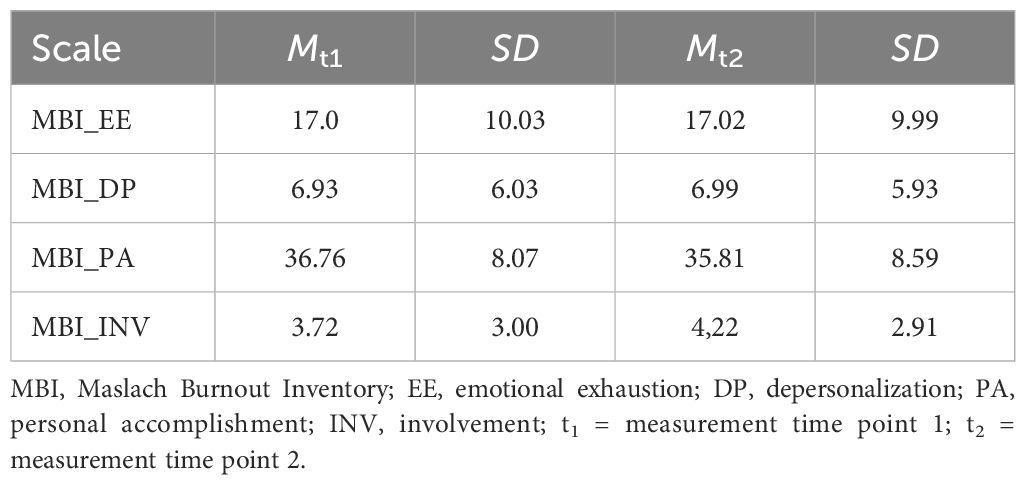
Table 2. t-test for dependent samples of the MBI including means and standard deviations for MBI-HSS Scales.
During the study period, a slight deterioration was observed, but paired t-test analysis showed no significant changes over time in the MBI subscales: MBI_EE t (90) = - 0.030, p = .976, dz = 0; MBI_DP t(90) = - 0.127, p = .899, dz = 0; MBI_PA t(90) = 1.46, p = .147, dz = 0.153; MBI_INV t(86) = -1.75, p = .083, dz = - 0.188.
PVQ
Furthermore, paired t-tests were conducted to examine whether the values of the PVQ changed from t1 to t2 (see Table 3). There were no significant changes in the subscales between the two times of measurement.
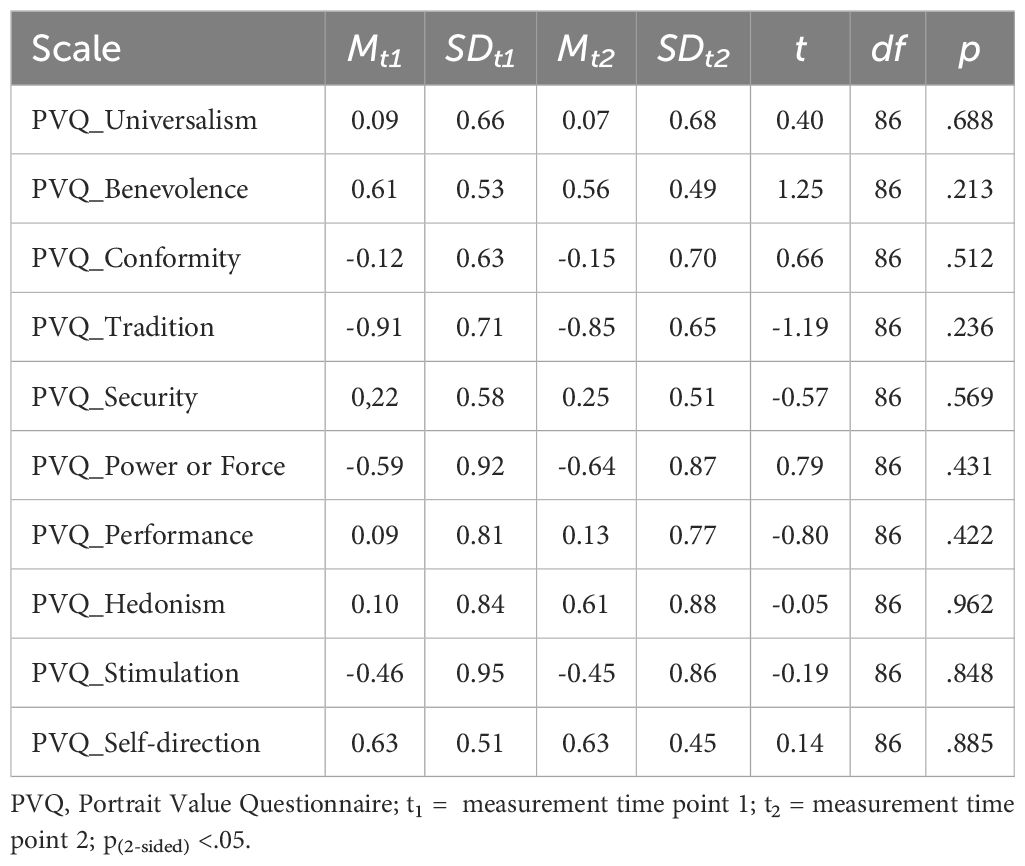
Table 3. t-test for dependent samples of the centered values PVQ.
To check for an association between the PVQ and MBI subscales at t1 and t2 Pearson correlations were calculated. Only a few significant correlations were found.
PVQ Self-direction at t1 correlates negatively with MBI INV (see Table 4) at t2 (PVQ SD r = -.21, p = .043). The higher self-direction at t1, the lower the involvement in MBI scale at t2. Furthermore, the subscale PVQ Power at t1 correlates positively with MBI PA at t2 (PVQ PO r = .28, p = .006). Lower scores in the MBI INV and higher values in the MBI PA can indicate a lower level of burnout. Thus, higher values in the PVQ Self-direction and lower scores in PVQ PA at t1 can be associated with an increased occurrence of burnout symptoms after deployment at t2.
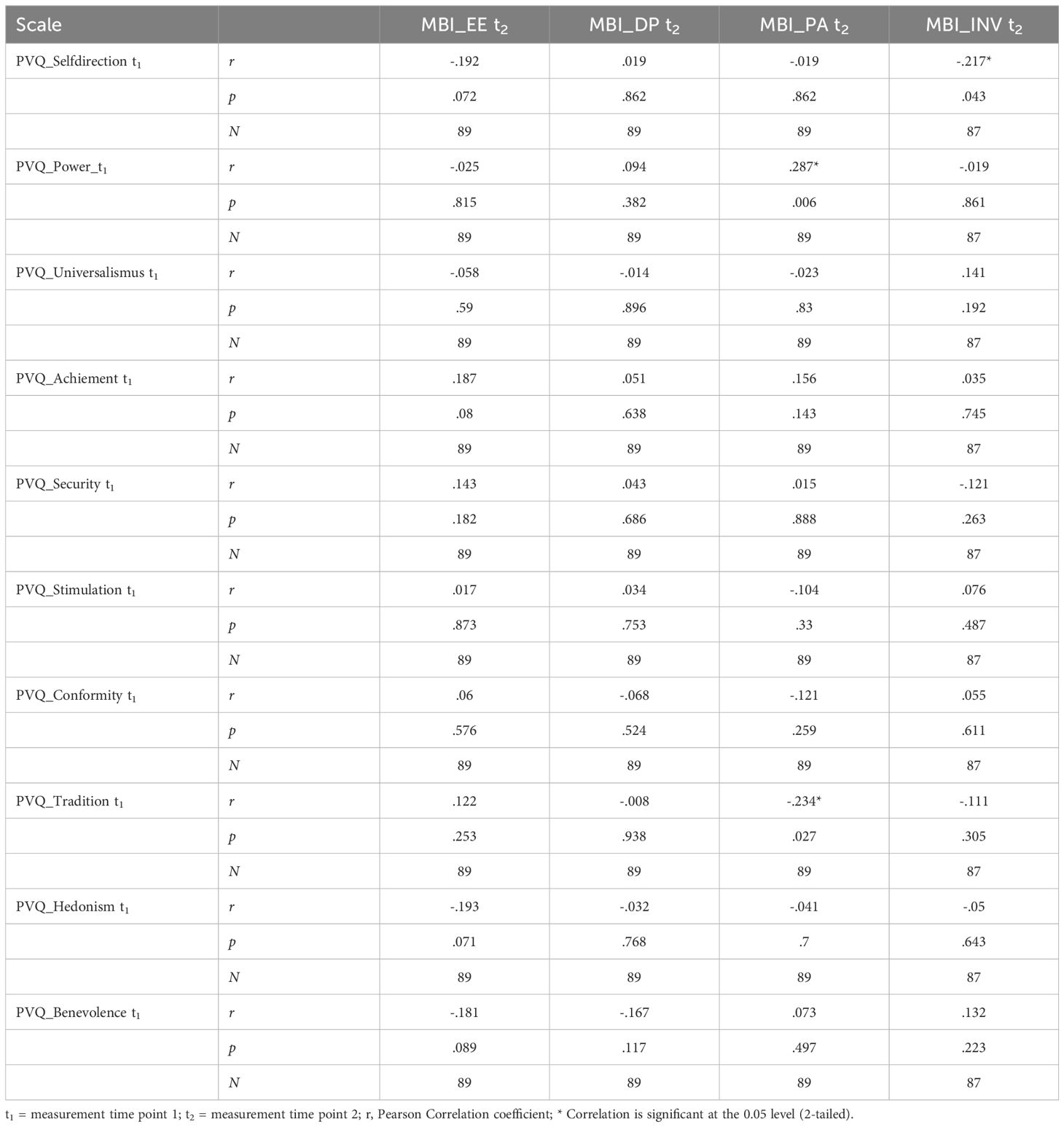
Table 4. Corellation matrix with scales PVQ subscales at t1 and MBI subscales at t2.
PVQ Tradition at t1 correlates negatively with MBI PA at t2 (PVQ TR r = -.23, p = .027) The higher tradition at t1, the lower the MBI PA at t2. There was a positive correlation found between PVQ Universalism at t1 and MBI INV (see Table 5) at t1 (PVQ UN r = .25, p = .018). PVQ Hedonism at t1 correlates negatively with MBI EE at t1 (PVQ HE r = -.26, p = .012). The higher hedonism at t1, the lower the emotional exhaustion in MBI at t1. In addition, PVQ Benevolence at t1 correlates negatively with MBI DP at t1 (PVQ BE r = -.25, p = .016), indicating that the higher benevolence at t1, the lower depersonalization in MBI at t1. According to Cohen (90, 91), all correlations represent a small effect size. The detailed tabular view can be viewed in the appendix.
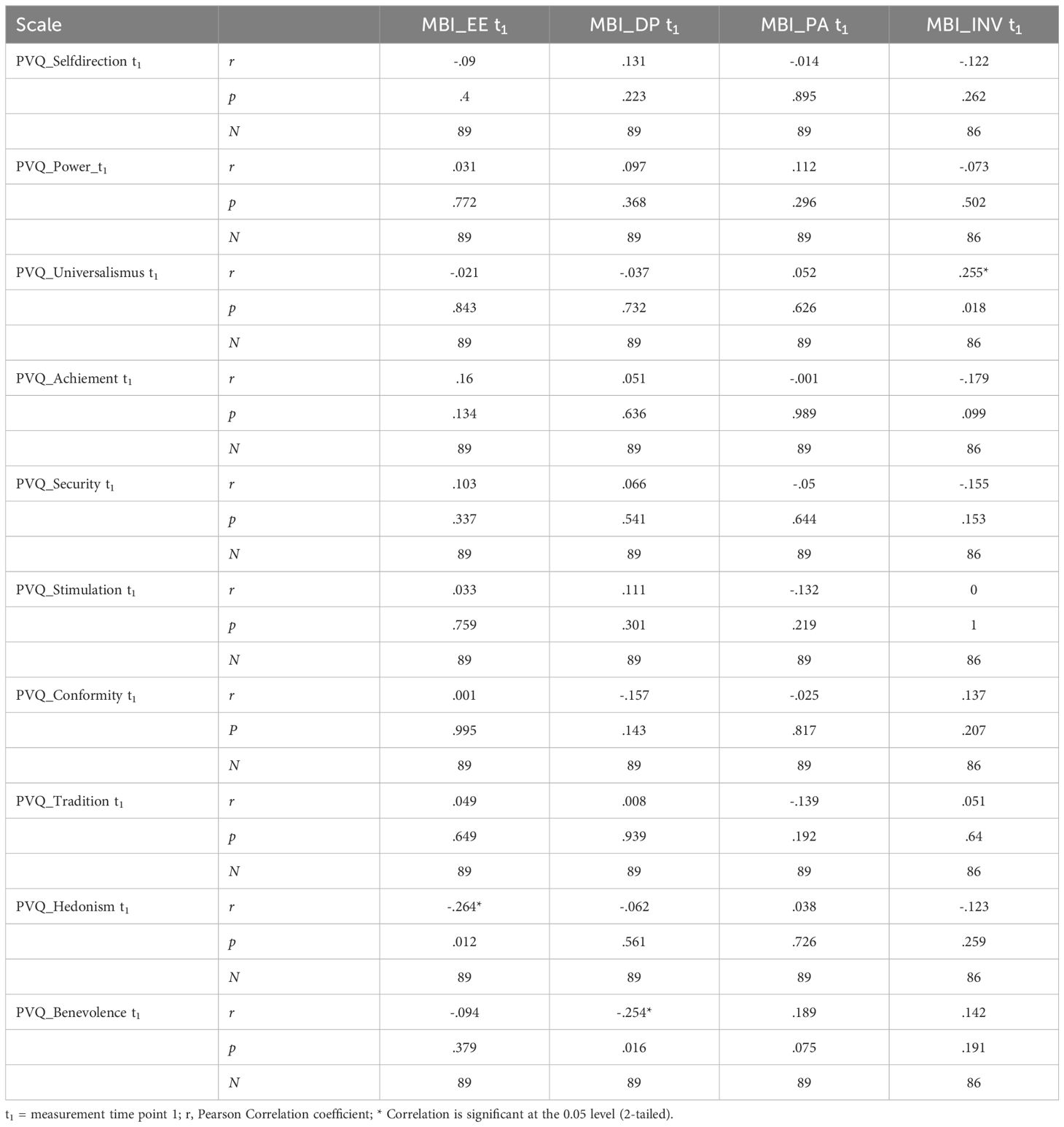
Table 5. Corellation matrix with scales PVQ subscales at t1 and MBI subscales at t1.
SMBE
Table 6 shows the moral injuries experienced by soldiers after deployment (t2). Compared to a possible total score of 54 points, the overall mean score of SMBE (SMBE in total) indicates a rather low score (Mt2 = 21.79), suggesting a lower level of distress in general. Examining the individual subscales, it can be highlighted that soldiers experienced lower moral injury from their own actions (SMBE_Sub2 Mt2 = 7.49) compared to the actions of others (SMBE_Sub1 Mt2 = 14.29).
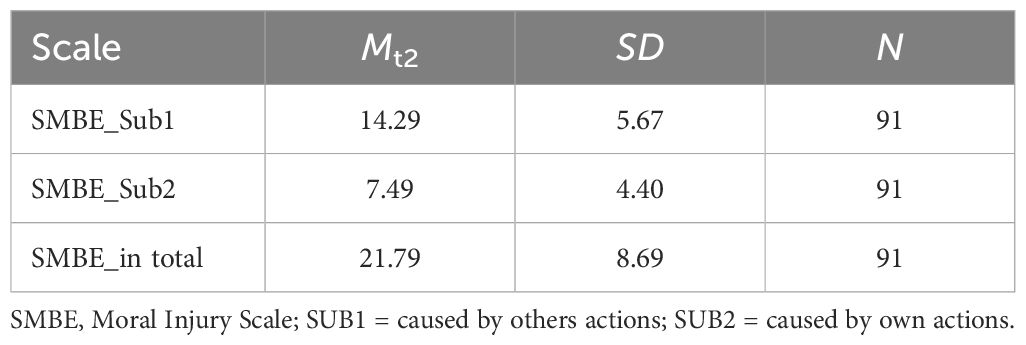
Table 6. Descriptive statistic.
Table 7 demonstrates that moral injuries resulting from the actions of others as well as from one’s own actions positively correlate with the Emotional Exhaustion (EE) scale of the MBI at t1 (SMBE_Sub1 r = .48, p = .001, SMBE_Sub2 r = .45, p = .001, SMBE_Sub in total r = -.54, p = .001) and t2 (SMBE_Sub1 r = .46, p = .001, SMBE_Sub2 r = .38, p = .001, SMBE_Sub in total r = .49, = .001). According to Cohen (92), this represents a medium effect size. The higher the experienced number of moral injuries caused by the actions of others or by one’s own actions, the higher the emotional exhaustion. These findings are reflected in conjunction with the Depersonalization (DP) scale. There is also a medium positive correlation with moral injuries caused by others (SMBE_Sub 1 r = .33, p = .001) as well as moral injuries caused by one’s own actions (SMBE_Sub 2 r = .32, p = .002) and total moral injuries (SMBE_Sub in total r = .38, p = .001) at t1. At t2, the correlation changes to weakly positive for moral injuries caused by others and by one’s own actions (SMBE_Sub1 r = .26, p = .011, SMBE_Sub2 r = .28, p = .007), while the total score of SMBE_Sub in total continues to show a medium positive correlation (SMBE_Sub in total r = .31, p = .002). Overall, this means that the more moral injuries a soldier experiences, the stronger the experience of depersonalization.
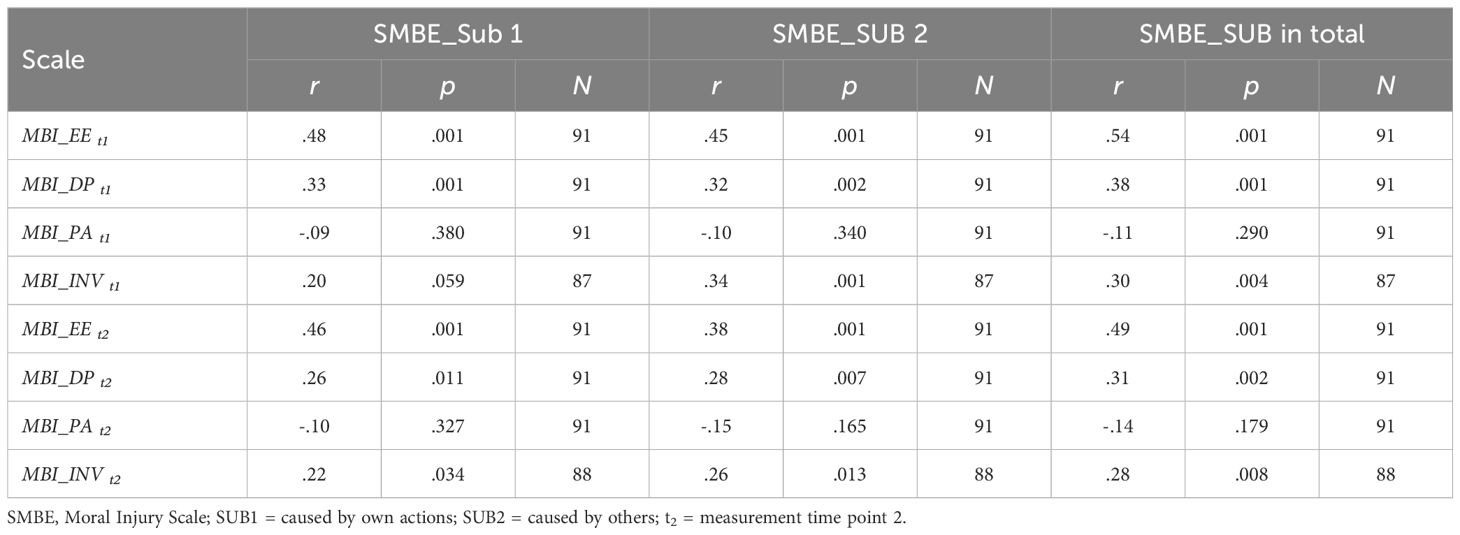
Table 7. Correlation matrix with scales MBI and SMBE.
Furthermore, the subscale Involvement (INV) of the MBI at t1 shows a medium positive correlation with moral injuries caused by one’s own actions as well as with the total score of SMBE (SMBE_Sub 2 r = 0.34, p = .001, SMBE_Sub in total r = .30, p = .004). No significant relationship could be found for moral injuries caused by others and INV. At t2, both subscales of SMBE show a low positive correlation with INV (SMBE_Sub1 r = .22, p = .034, SMBE_Sub2 r = .26, p = .013). The total score of SMBE shows a medium positive correlation (Sub in total r = .28, p = .008) with INV. Again, it is evident that the higher the experienced moral injuries caused by one’s own actions or by the actions of others, the higher the experience of involvement in the MBI. No significant relationships could be found between moral injuries and the Personal Accomplishment scale of the MBI.
Discussion
For the first time, this study examined the relationship between burnout syndrome, value orientations, and moral injuries among medical service soldiers after participating in a foreign mission.
The psychological strain and the increased incidence of mental illnesses among soldiers participating in overseas deployments have been demonstrated in various studies (33, 75). Additionally, Adler (13) demonstrated significant positive correlations between the perception of occupational stressors and the degree of burnout among medical personnel in the US military. Zimmermann et al. also found a significant increase in depression over the course of deployment among soldiers without a medical background (64). In line with these findings and taking into account the similar symptom expression between burnout syndrome and depression (5, 8), we expected to see an increase in burnout symptomatology among medical service soldiers after foreign deployment.
Comparing the results of the MBI from t1 to t2, it became evident that medical soldiers already showed mild to moderate burnout symptoms in the subscales of depersonalization and personal accomplishment before deployment. These slightly worsened during the deployment, but contrary to our expectations this change wasn’t significant. Thus, we reject our first hypothesis. In interpreting this finding, one must consider the chosen normative sample. Based on normative samples with medical personnel, we saw a comparatively low burnout burden among the medical soldiers in our study. However, compared to the normative sample group of mental health professionals, higher values were observed in EE and DP (85). However, the normative samples did not account for adjusted values such as age and gender, which might explain some of the differences between the amount of burnout symptoms in our study sample and that of the normative sample group.
Furthermore, in contrast to Houkes and Watson (15), our study did not exclusively survey medical personnel, so not all medical soldiers may have been exposed to the same stressors. Overall, 75% of the participants were members of the medical service, the remaining participants belonged to other branches of the armed forces (Navy, Army, Air Force). Nevertheless, this doesn’t prevent them from working in the medical service. Further inferences about medical duties can be made by looking at the rank groups, with the group of officers, comprising 44%, most likely being deployed as medical officers. Our study replicates the results of an American study, which also found no increase in burnout syndrome among soldiers deployed in Iraq (93). Overall, this indicates that further research is needed in this area, as also described by Chambel et al. (94).
As personal values might be involved in the development of burnout symptomatology, we looked closer at the concept of personal values and their possible association with burnout. Firstly, we hypothesized that personal values remain stable over time. By assessing the changes in the PVQ from t1 to t2, no significant differences could be found. This confirmed our hypothesis and seems to support the idea that values are similar to personality factors in influencing behavior over long periods of time (95). Nevertheless, because of the high variability in measuring time points after deployment (t2) value changes might not have been detected. On the one hand, these could result from contextual factors, such as potential stressors following repatriation (relationship issues, reintegration into domestic service, and challenges in finding meaning in domestic activities). On the other hand, the process of value adaptation might follow a reflection process, which hasn’t occurred yet when the data collection, as in our study, happens relatively early post-deployment. Addressing these contextual and timely factors would be a valuable addition to future studies.
Regarding the association between values and burnout, this paper can only provide some initial results. Since very few studies have addressed this research topic, no specific hypothesis about the direction of the association nor the most relevant type of values could be defined beforehand. Nevertheless, our findings suggest that a higher expression in the values of self-direction and power before deployment is associated with a lower value in the burnout subscale of involvement and a higher value in the subscale of personal accomplishment after deployment, respectively. Cautiously said, the more one is able to establish and develop one’s own life path (value of self-direction) and the more power one feels over other people and resources (value of power) before deployment, the lower the level of burnout after deployment.
In contrast, a higher expression in the value of tradition seems to be associated with a lower value in the burnout subscale of personal accomplishment. This finding suggests that the more one holds on to traditional customs or norms of behavior (value of tradition) before deployment, the higher the level of burnout after deployment.
Interestingly, certain values at t1 were correlated with some of the burnout subscales before deployment only. For example, the value of universalism (being interested in protecting the well-being of people or the environment) was positively correlated with a higher score in the subscale of involvement (pointing towards a higher level of burnout) prior to being deployed. Meanwhile, enjoying life’s goals and events (value of hedonism) and aiding people with whom one is in close contact (value of benevolence) seems to be correlated negatively with the subscale of emotional exhaustion and depersonalization, respectively.
To our knowledge, the only study reporting on personal value orientations and psychiatric symptoms within the military has been conducted by Zimmermann et al. (72). The authors found the values of power and hedonism to be negatively correlated with the probability of PTSD, meanwhile the values of universalism and tradition increased the probability of developing PTSD after foreign deployment. Furthermore, Maercker et al. (62) identified the value of self-direction as a predictor of resilience, suggesting that personal value orientations are meaningful predictors of mental health.
Our findings seem to point into a similar direction. However, as they are only based on simple correlations and were not hypothesis-driven, the interpretation of the results must be viewed with caution. Nevertheless, we believe that these initial findings should be further investigated in follow-up studies in order to better understand the predictive potential of personal values on mental health.
In our third hypothesis, we expected that increased experiences of moral injuries during deployments would be significantly associated with elevated burnout levels. This hypothesis was partly confirmed as significant correlations were found between moral injuries and three of the four burnout subscales (Emotional Exhaustion, Depersonalization, and Involvement).
Interestingly, these correlations were found before and after deployment, suggesting two different interpretations. First, one could argue that early burnout levels pre deployment influence the experience of moral injuries during deployment. For instance, burnout symptoms such as emotional exhaustion might make soldiers more susceptible to morally questionable behavior. Second, experiencing moral injuries seems to be associated with elevated burnout levels after deployment. This interpretation could be seen in line with the theoretical model of the areas of worklife model of burnout which proposes that the greater the perceived incongruity between one’s own ideals and motivations the greater the likelihood of burnout (61).
Overall, since simple correlations are unable to allow for causality, further research is necessary to better understand the association between moral injury and burnout.
Furthermore, medical soldiers in our study sample reported a low incidence of moral injuries in the SMBE total score. The frequency of moral injuries caused by others was higher than that by their own actions. A similar distribution was observed in a non-military study of medical personnel during the COVID-19 pandemic (43), emphasizing the influence of self-induced moral injuries (Self MI) on burnout syndrome. The overall low symptom burden can be seen in line with previous findings by Wittchen et al. (32). Here, the frequency of stressful events during overseas deployments was significantly lower for medical soldiers compared to combat troops. The nature of the deployment (combat mission, security detail, and associated treatment of civilians in medical facilities with available resources) could also influence the confrontation with potentially stressful and morally significant events. In addition, the German Armed Forces have various regulations within deployment contingents. For instance, the surgical treatment of civilians being transferred to local facilities post-treatment, varies greatly, potentially leading to various moral burdens across different deployment contingents (96). These detailed correlations warrant further investigation in subsequent studies. The association between moral injury at the end of deployment and burnout was observed both before and after the examined deployment interval. Since in this study moral injuries were measured only at the end (t2) of the deployment, a specific attribution to the deployment experiences is therefore only partially feasible.
For the first time, our results demonstrate an association between moral injuries and the level of burnout symptoms in medical soldiers. Additionally, a high pre-existing burden might be considered a risk factor for developing burnout syndrome post-deployment. Moreover, personal value types might be meaningful predictors of burnout. These preliminary findings should be further investigated in future controlled studies to identify additional influencing factors. Although soldiers undergo medical pre-screening before deployment to determine their fitness for duty, replicating our results could prompt consideration of screening measures for psychological symptoms to aid evaluating physicians. Moreover, leadership support for medical personnel during extremely stressful work experiences, such as the COVID-19 pandemic, was identified as a protective factor by Dale (43). Therefore, strengthening personal resilience and robustness (97) and destigmatizing mental health issues through education on moral injuries and burnout syndrome (98) could be beneficial topics in leadership training within the German Armed Forces.
Limitations of the study
This study has several limitations, including the lack of randomization and the absence of a control group, which limits the comparability of burnout development and value changes with non-deployed soldiers. Additionally, changes over time cannot be ruled out.
In a participant group comprised solely of medical service soldiers, it is not possible to clearly distinguish general soldier burdens from those specific to the medical service. Thus, the effects found should only be considered in the context of medical soldiers deployed on overseas missions. The sample size is relatively small, which might explain the lack of significant results due to underpowering and overestimated effect sizes. The sample also exhibits high heterogeneity; while the gender distribution is balanced within the medical service of the German armed forces, women are significantly underrepresented in the entire Bundeswehr (13% in 2022).
Another limitation arises from the unclear causal mechanisms and the fact that the majority of deployment participants (54.9%) had multiple overseas deployments, thus accumulating deployment experiences. The chosen test method, which generally inquires about the burden of past moral injuries without specifying a particular time frame, makes the observed relationship with burnout symptoms non-specific. Furthermore, moral injuries acquired domestically during general service as medical soldiers are also to be expected, as demonstrated in studies on military (30) and non-military medical personnel (27, 28).
It is plausible that the delayed timing of the surveys at t2 might also reflect general burdens such as family environment or reorientation to domestic life for the soldiers. Future studies should either separately inquire about these factors or conduct the second measurement immediately after return from deployment. Potential alternative causes for the altered response behavior could also be attributable to other unobserved factors, such as age, rank, responsibility, occupational role, type of event, and prior experiences (99, 100).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Humboldt University of Berlin (Charité). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FL: Writing – original draft. AB: Writing – original draft. PM: Writing – review & editing, Formal analysis, Data curation. MM: Writing – review & editing, Investigation, Data curation. AR: Writing – review & editing, Conceptualization. G-DW: Writing – review & editing, Supervision. UW: Writing – review & editing, Supervision, Formal analysis. PZ: Writing – review & editing, Supervision, Methodology, Conceptualization. IS: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank Braun and Wetzel.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Meyer M, Wing L, Schenkel A. Krankheitsbedingte Fehlzeiten in der deutschen Wirtschaft im Jahr 2021. In: Badura B, Ducki A, Meyer M, Schröder H, editors. Fehlzeiten-Report 2022. Springer Berlin Heidelberg, Berlin, Heidelberg (2022). p. 287–368. Herausgeber(Fehlzeiten-Report; Bd. 2022). Verfügbar unter. doi: 10.1007/978-3-662-65598-6_19
2. Badura B, Ducki A, Baumgardt J, Meyer M, Schröder H. Zeitenwende - Arbeit gesund gestalten. Berlin: Springer (2023). p. 815 S. Herausgeber(Fehlzeiten-Report).
3. Guthier C, Dormann C, Voelkle MC. Reciprocal effects between job stressors and burnout: A continuous time meta-analysis of longitudinal studies. psychol Bull. (2020) 146:1146–73. doi: 10.1037/bul0000304
4. Ahola K, Hakanen J, Perhoniemi R, Mutanen P. Relationship between burnout and depressive symptoms: A study using the person-centred approach. Burnout Res. (2014) 1:29–37. doi: 10.1016/j.burn.2014.03.003
5. Bianchi R, Schonfeld IS, Vandel P, Laurent E. On the depressive nature of the “burnout syndrome”: A clarification. Eur Psychiatr. (2017) 41:109–10. doi: 10.1016/j.eurpsy.2016.10.008
6. Eisenlohr V, Zimmermann P, Kowalski J. Burnout – ein bedeutendes Symptombild in der truppenärztlichen Praxis. WMM. (2011) 55):224–8.
7. Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. (2016) 15:103–11. doi: 10.1002/wps.20311
8. Bianchi R, Verkuilen J, Schonfeld IS, Hakanen JJ, Jansson-Fröjmark M, Manzano-García G. Is burnout a depressive condition? A 14-sample meta-analytic and bifactor analytic study. Clin psychol Sci. (2021) 9:579–97. doi: 10.1177/2167702620979597
9. Koutsimani P, Montgomery A, Georganta K. The relationship between burnout, depression, and anxiety: A systematic review and meta-analysis. Front Psychol. (2019) 10:284. doi: 10.3389/fpsyg.2019.00284
10. Khammissa RAG, Nemutandani S, Feller G, Lemmer J, Feller L. Burnout phenomenon: neurophysiological factors, clinical features, and aspects of management. J Int Med Res. (2022) 50:030006052211064. doi: 10.1177/03000605221106428
11. Hosseini SM, Hesam S, Hosseini SA. Burnout among Military Personnel: A systematic Review. IJPS. (2023) 184:e522–30. doi: 10.18502/ijps.v18i2.12371
12. Ryan E, Hore K, Power J, Jackson T. The relationship between physician burnout and depression, anxiety, suicidality and substance abuse: A mixed methods systematic review. Front Public Health. (2023) 11:1133484. doi: 10.3389/fpubh.2023.1133484
13. Adler AB, Adrian AL, Hemphill M, Scaro NH, Sipos ML, Thomas JL. Professional stress and burnout in U.S. Military medical personnel deployed to Afghanistan. Military Med. (2017) 182:e1669–76. doi: 10.7205/MILMED-D-16-00154
14. Kamaloo A, Ahmadipour A, Labbaf A, Hesari E, Valadkhani S, Zebardast J. Why Do Emergency Medicine Residents Experience Burn Out? A qualitative study. Iran J Psychiatry. (2017) 12:214–8.
15. Houkes I, Winants Y, Twellaar M, Verdonk P. Development of burnout over time and the causal order of the three dimensions of burnout among male and female GPs. A three-wave panel study. BMC Public Health. (2011) 11:240. doi: 10.1186/1471-2458-11-240
16. Arora M, Asha S, Chinnappa J, Diwan AD. Review article: Burnout in emergency medicine physicians. Emerg Med Australasia. (2013) 25:491–5. doi: 10.1111/1742-6723.12135
17. Kansoun Z, Boyer L, Hodgkinson M, Villes V, Lançon C, Fond G. Burnout in French physicians: A systematic review and meta-analysis. J Affect Disord. (2019) 246:132–47. doi: 10.1016/j.jad.2018.12.056
18. Watson AG, McCoy JV, Mathew J, Gundersen DA, Eisenstein RM. Impact of physician workload on burnout in the emergency department. Psychology Health Med. (2019) 24:414–28. doi: 10.1080/13548506.2018.1539236
19. Sahebi A, Golitaleb M, Moayedi S, Torres M, Sheikhbardsiri H. Prevalence of workplace violence against health care workers in hospital and pre-hospital settings: An umbrella review of meta-analyses. Front Public Health. (2022) 10:895818. doi: 10.3389/fpubh.2022.895818
20. Sahebi A, Nejati-Zarnaqi B, Moayedi S, Yousefi K, Torres M, Golitaleb M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog Neuropsychopharmacol Biol Psychiatry. (2021) 107:110247. doi: 10.1016/j.pnpbp.2021.110247
21. Wesemann U, Applewhite B, Himmerich H. Investigating the impact of terrorist attacks on the mental health of emergency responders: systematic review. BJPsych Open. (2022) 8:e107. doi: 10.1192/bjo.2022.69
22. Sahebi A, Moayedi S, Golitaleb M. COVID-19 pandemic and the ethical challenges in patient care. jmehm. (2020) 18 (2): 213–36. doi: 10.18502/jmehm.v13i24.4955
23. Stene LE, Fernandez A, Gindt M, Nachon O, Askenazy F. Editorial: Recovering after terrorist attacks, large-scale accidents and other disasters: Psychosocial care responses across countries. Front Psychol. (2023) 14:1168679. doi: 10.3389/fpsyg.2023.1168679
24. Nejati-Zarnaqi B, Sahebi A, Jahangiri K. Factors affecting management of corpses of the confirmed COVID-19 patients during pandemic: A systematic review. J Forensic Legal Med. (2021) 84:102273. doi: 10.1016/j.jflm.2021.102273
25. Jones M, Fear NT, Greenberg N, Jones N, Hull L, Hotopf M. Do medical services personnel who deployed to the Iraq war have worse mental health than other deployed personnel? Eur J Public Health. (2008) 18:422–7. doi: 10.1093/eurpub/ckn031
26. McCauley M, Hughes JH, Liebling-Kalifani H. Wellbeing of military mental health staff: Mathew McCauley and colleagues explore the psychosocial effects of operational deployment during the Iraq war on nurses and psychiatrists in the armed forces. Ment Health Practice. (2010) 14:14–9. doi: 10.7748/mhp2010.12.14.4.14.c8106
27. Chuang CH, Tseng PC, Lin CY, Lin KH, Chen YY. Burnout in the intensive care unit professionals: A systematic review. Medicine. (2016) 95:e5629. doi: 10.1097/MD.0000000000005629
28. van Mol MMC, Kompanje EJO, Benoit DD, Bakker J, Nijkamp MD. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: A systematic review. PloS One. (2015) 10:e0136955. doi: 10.1371/journal.pone.0136955
30. Williams BJ, Rudinsky SL, Matteucci MJ. Burnout in military emergency medicine resident physicians: A cross-sectional study with comparisons to other physician groups. Military Med. (2020) 185:e331–4. doi: 10.1093/milmed/usz236
31. Summers SM, Nagy CJ, April MD, Kuiper BW, Rodriguez RG, Jones WS. The prevalence of faculty physician burnout in military graduate medical education training programs: A cross-sectional study of academic physicians in the United States department of defense. Military Med. (2019) 184:e522–30. doi: 10.1093/milmed/usz055
32. Wittchen HU, Gloster A, Beesdo K, Schönfeld S, Perkonigg A. Posttraumatic stress disorder: diagnostic and epidemiological perspectives. CNS Spectr. (2009) 14:5–12.
33. Wittchen HU, Schönfeld S, Kirschbaum C, Thurau C, Trautmann S, Steudte S. Traumatic experiences and posttraumatic stress disorder in soldiers following deployment abroad. Deutsches Ärzteblatt Int. (2012) 109 (35-36): 559–68. doi: 10.3238/arztebl.2012.0559
34. Wittchen HU, Schönfeld S, Kirschbaum C, Trautmann S, Thurau C, Siegert J. Rates of mental disorders among german soldiers deployed to Afghanistan: increased risk of PTSD or of mental disorders in general? J Depress Anxiety. (2013) 02:200–7. doi: 10.4172/2167-1044
35. Trautmann S, Goodwin L, Höfler M, Jacobi F, Strehle J, Zimmermann P. Prevalence and severity of mental disorders in military personnel: a standardised comparison with civilians. Epidemiol Psychiatr Sci. (2017) 26:199–208. doi: 10.1017/S204579601600024X
36. Sundin J, Herrell RK, Hoge CW, Fear NT, Adler AB, Greenberg N. Mental health outcomes in US and UK military personnel returning from Iraq. Br J Psychiatry. (2014) 204:200–7. doi: 10.1192/bjp.bp.113.129569
37. Ferrier-Auerbach AG, Erbes CR, Polusny MA, Rath CM, Sponheim SR. Predictors of emotional distress reported by soldiers in the combat zone. J Psychiatr Res. (2010) 44:470–6. doi: 10.1016/j.jpsychires.2009.10.010
38. Matthäus E, Schanze S, Helms C, Willmund GD, Zimmermann P, Wesemann U. Prädiktoren der Entwicklung von Angst- und depressiven Störungen bei Einsatzsoldaten der Bundeswehr – eine explorative Pilotstudie. WMM. (2021) 65:419–23.
39. Bakker AB, Schaufeli WB, Demerouti E, Janssen PPM, van der Hulst R, Brouwer J. Using equity theory to examine the difference between burnout and depression. Anxiety Stress Coping. (2000) 13:247–68. doi: 10.1080/10615800008549265
40. Demerouti E, Bakker AB, Peeters MCW, Breevaart K. New directions in burnout research. Eur J Work Organizational Psychol. (2021) 30:686–91. doi: 10.1080/1359432X.2021.1979962
41. Litz BT, Stein N, Delaney E, Lebowitz L, Nash WP, Silva C. Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clin Psychol Rev. (2009) 29:695–706. doi: 10.1016/j.cpr.2009.07.003
42. Zerach G, Levi-Belz Y, Griffin BJ, Maguen S. Patterns of exposure to potentially morally injurious events among Israeli combat veterans: A latent class analysis approach. J Anxiety Disord. (2021) 79:102378. doi: 10.1016/j.janxdis.2021.102378
43. Dale LP, Cuffe SP, Sambuco N, Guastello AD, Leon KG, Nunez LV. Morally distressing experiences, moral injury, and burnout in Florida healthcare providers during the COVID-19 pandemic. IJERPH. (2021) 18:12319. doi: 10.3390/ijerph182312319
44. Shay J. Achilles in Vietnam: combat trauma and the undoing of character. New York: Scribner (2003). p. 246. 1. Scribner trade paperback edS.
45. Molendijk T, Verkoren W, Drogendijk A, Elands M, Kramer EH, Smit A. Contextual dimensions of moral injury: An interdisciplinary review Military Psychol. (2022) 34:742–53. doi: 10.1080/08995605.2022.2035643
46. Cappuccio ML, Peeters A, McDonald W. Sympathy for dolores: moral consideration for robots based on virtue and recognition. Philos Technol. (2020) 33:9–31. doi: 10.1007/s13347-019-0341-y
47. Griffin BJ, Purcell N, Burkman K, Litz BT, Bryan CJ, Schmitz M. Moral injury: an integrative review. J Traumatic Stress. (2019) 32:350–62. doi: 10.1002/jts.22362
48. Currier JM, Holland JM, Drescher KD. Spirituality factors in the prediction of outcomes of PTSD treatment for US military veterans. J Traumatic Stress. (2015) 28:57–64. doi: 10.1002/jts.21978
49. Nash WP, Marino Carper TL, Mills MA, Au T, Goldsmith A, Litz BT. Psychometric evaluation of the moral injury events scale. Military Med. (2013) 178:646–52. doi: 10.7205/MILMED-D-13-00017
50. Hellenthal A, Zimmermann P, Willmund G, Lovinusz A, Fiebig R, Bozoyan C. Einsatzerlebnisse, moralische Verletzungen, Werte und psychische Erkrankungen bei Einsatzsoldaten der Bundeswehr. Verhaltenstherapie. (2017) 27:244–52. doi: 10.1159/000470848
51. Zimmermann P, Fischer C, Lorenz S, Alliger-Horn C. Changes of personal values in deployed German Armed Forces Soldiers with psychiatric disorders. Wehrmedizinische Monatsschrift. (2016) 60:7–14.
52. Ames D, Erickson Z, Youssef NA, Arnold I, Adamson CS, Sones AC. Moral injury, religiosity, and suicide risk in U.S. Veterans and active duty military with PTSD symptoms. Military Med. (2019) 184:e271–8.
53. Wilson MA, Shay A, Harris JI, Faller N, Usset TJ, Simmons A. Moral distress and moral injury in military healthcare clinicians: A scoping review. AJPM Focus. (2024) 3:100173. doi: 10.1016/j.focus.2023.100173
54. Norman SB, Feingold JH, Kaye-Kauderer H, Kaplan CA, Hurtado A, KaChadourian L. Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: Relationship to PTSD symptoms, burnout, and psychosocial functioning. Depression Anxiety. (2021) 38:1007–17. doi: 10.1002/da.23205
55. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. (2019) 36:400–2.
56. Epstein EG, Hamric AB. Moral distress, moral residue, and the crescendo effect. J Clin Ethics. (2009) 20:330–42. doi: 10.1086/JCE200920406
57. Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. AJP. (2007) 164:150–3. doi: 10.1176/ajp.2007.164.1.150
58. Shanafelt TD, Hasan O, Dyrbye LN, Sinsky C, Satele D, Sloan J. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proc. (2015) 90:1600–13. doi: 10.1016/j.mayocp.2015.08.023
59. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. (2018) 283:516–29. doi: 10.1111/joim.12752
60. King EL, Hawkins LE. Identifying and mitigating moral injury risks in military behavioral health providers. Military Psychol. (2023) 35:169–79. doi: 10.1080/08995605.2022.2093599
61. Leiter MP, Maslach C. AREAS OF WORKLIFE: A STRUCTURED APPROACH TO ORGANIZATIONAL PREDICTORS OF JOB BURNOUT. In: Research in Occupational Stress and Well-Being. Emerald (MCB UP, Bingley (2003). p. 91–134. doi: 10.1016/S1479-3555(03)03003-8/full/html
62. Maercker A, Chi Zhang X, Gao Z, Kochetkov Y, Lu S, Sang Z. Personal value orientations as mediated predictors of mental health: A three-culture study of Chinese, Russian, and German university students. Int J Clin Health Psychol. (2015) 15:8–17. doi: 10.1016/j.ijchp.2014.06.001
63. Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory. In: Evaluating stress: A book of resources, 3rd ed. Scarecrow Press Lanham MD, USA: Scarecrow Education (1996). p. 191–218.
64. Zimmermann P, Alliger-Horn C, Köhler K, Varn A, Zollo M, Reichelt A. Depressivität und Wertorientierungen im Verlauf von militärischen Auslandseinsätzen. Trauma Gewalt. (2018) 12:134–50. doi: 10.21706/tg-12-2-134
65. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consulting Clin Psychol. (2000) 68:748. doi: 10.1037/0022-006X.68.5.748
66. Zimmermann P, Firnkes S, Kowalski J, Backus J, Alliger-Horn C, Willmund G. Zusammenhänge zwischen Psychischer Symptomatik und Persönlichen Werten bei Bundeswehrsoldaten nach einem Auslandseinsatz. Psychiatrische Praxis. (2015) 42:436–42.
67. Knafo A, Schwartz SH. Value socialization in families of Israeli-born and soviet-born adolescents in Israel. J Cross-Cultural Psychol. (2001) 32:213–28. doi: 10.1177/0022022101032002008
68. Hitlin S, Piliavin JA. Values: reviving a dormant concept. Annu Rev Sociol. (2004) 30:359–93. doi: 10.1146/annurev.soc.30.012703.110640
69. Schwartz SH, Melech G, Lehmann A, Burgess S, Harris M, Owens V. Extending the cross-cultural validity of the theory of basic human values with a different method of measurement. J Cross-Cultural Psychol. (2001) 32:519–42. doi: 10.1177/0022022101032005001
70. Sagiv L, Schwartz SH. Value priorities and subjective well-being: direct relations and congruity effects. Eur J Soc Psychol. (2000) 30:177–98. doi: 10.1002/(ISSN)1099-0992
71. Heim E, Maercker A, Boer D. Value orientations and mental health: A theoretical review. Transcult Psychiatry. (2019) 56:449–70. doi: 10.1177/1363461519832472
72. Schuster C, Pinkowski L, Fischer D. Intra-individual value change in adulthood: A systematic literature review of longitudinal studies assessing Schwartz’s value orientations. Z für Psychol. (2019) 227:42–52. doi: 10.1027/2151-2604/a000355
73. Bardi A, Buchanan KE, Goodwin R, Slabu L, Robinson M. Value stability and change during self-chosen life transitions: Self-selection versus socialization effects. J Pers Soc Psychol. (2014) 106:131–47. doi: 10.1037/a0034818
74. Vecchione M, Schwartz S, Alessandri G, Döring AK, Castellani V, Caprara MG. Stability and change of basic personal values in early adulthood: An 8-year longitudinal study. J Res Pers. (2016) 63:111–22. doi: 10.1016/j.jrp.2016.06.002
75. Sundberg R. Value stability and change in an ISAF contingent. J Pers. (2016) 84:91–101. doi: 10.1111/jopy.12142
76. Bojanowska A, Kaczmarek ŁD, Koscielniak M, Urbańska B. Changes in values and well-being amidst the COVID-19 pandemic in Poland. Devleesschauwer B, Herausgeber. PloS One. (2021) 16:e0255491. doi: 10.1371/journal.pone.0255491
77. Daniel E, Bardi A, Fischer R, Benish-Weisman M, Lee JA. Changes in personal values in pandemic times. Soc psychol Pers Sci. (2022) 13:572–82. doi: 10.1177/19485506211024026
78. Schaie KW. Developmental Influences on Adult Intelligence: The Seattle Longitudinal Study. Oxford University Press, Oxford, GB: Oxford University Press (2012). Available at: https://academic.oup.com/book/3681.
79. Jost JT, Andrews R. System justification theory. In: Christie DJ, editor. The Encyclopedia of Peace Psychology (2011). Herausgeber. doi: 10.1002/9780470672532.wbepp273
80. Kobasa SC. Stressful life events, personality, and health: An inquiry into hardiness. J Pers Soc Psychol. (1979) 37:1–11. doi: 10.1037/0022-3514.37.1.1
81. Myers DG, Diener E. The scientific pursuit of happiness. Perspect Psychol Sci. (2018) 13:218–25. doi: 10.1177/1745691618765171
82. Cieciuch J, Schwartz SH. The number of distinct basic values and their structure assessed by PVQ–40. J Pers Assess. (2012) 94:321–8. doi: 10.1080/00223891.2012.655817
83. Zimmermann P, Firnkes S, Kowalski JT, Backus J, Siegel S, Willmund G. Personal values in soldiers after military deployment: associations with mental health and resilience. Eur J Psychotraumatol. (2014) 5:22939. doi: 10.3402/ejpt.v5.22939
84. Büssing A, Perrar KM. Die Messung von Burnout. Untersuchung einer deutschen Fassung des Maslach Burnout Inventory (MBI-D). Diagnostica. (1992) 38:328–53.
85. Maslach C, Jackson SE, Leiter MP, Schaufeli WB, Schwab R. Maslach Burnout Inventory Manual. 4th ed. Mindgarden, Menlo Park, CA: Mind Garden, Inc. (1996). Available at: www.mindgarden.com. 707 Menlo Avenue, Suite 120, Menlo Park, CA 94025; Telephone: 650-322-6300; FAX: 650-322-6398; E-mail:aW5mb0BtaW5kZ2FyZGVuLmNvbQ==.
86. Rotenstein LS, Torre M, Ramos MA, Rosales RC, Guille C, Sen S. Prevalence of burnout among physicians: A systematic review. JAMA. (2018) 320:1131. doi: 10.1001/jama.2018.12777
87. Elsayed H, Aljohani E, Jeddo Z, Alraheili R, Alsisi G, Alkayyal A. Burnout rate among healthcare workers during COVID19 pandemic in Medina, Saudi Arabia. Med Sci. (2022) 26 (127): 1–11. doi: 10.13140/RG.2.2.36057.39526
88. Schmidt P, Bamberg S, Davidov E, Herrmann J, Schwartz SH. Die Messung von Werten mit dem “Portraits Value Questionnaire. Z für Sozialpsychologie. (2007) 38:261–75. doi: 10.1024/0044-3514.38.4.261
89. Salkind N. Encyclopedia of Research Design. 2455 Teller Road, Thousand Oaks California 91320 United States: SAGE Publications, Inc (2010). Available at: https://methods.sagepub.com/reference/encyc-of-research-design.
90. Gignac GE, Szodorai ET. Effect size guidelines for individual differences researchers. Pers Individ Dif. (2016) 102:74–8. doi: 10.1016/j.paid.2016.06.069
91. Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. (2013) 4:863. doi: 10.3389/fpsyg.2013.00863
92. Faller H. Signifikanz, effektstärke und konfidenzintervall. Rehabilitation. (2004) 43:174–8. doi: 10.1055/s-2003-814934
93. Cragun JN, April MD, Thaxton RE. The impact of combat deployment on health care provider burnout in a military emergency department: A cross-sectional professional quality of life scale V survey study. Military Med. (2016) 181:730–4. doi: 10.7205/MILMED-D-15-00420
94. Chambel M, Lopes S, Castanheira F, Silveira C. Militaries’ Burnout and work engagement: A qualitative systematic literature review. In: The Routledge International Handbook of Military Psychology and Mental Health, 1st ed.Routledge, London. (2019) pp 1–47.
95. Schwartz SH. Are there universal aspects in the structure and contents of human values? J Soc Issues. (1994) 50:19–45.
96. Ryu MY, Martin MJ, Jin AH, Tabor HK, Wren SM. Characterizing moral injury and distress in US military surgeons deployed to far-forward combat environments in Afghanistan and Iraq. JAMA Netw Open. (2023) 6:e230484. doi: 10.1001/jamanetworkopen.2023.0484
97. Litam SDA, Balkin RS. Moral injury in health-care workers during COVID-19 pandemic. Traumatology. (2021) 27:14–9. doi: 10.1037/trm0000290
98. Kopacz MS, Ames D, Koenig HG. It’s time to talk about physician burnout and moral injury. Lancet Psychiatry. (2019) 6:e28. doi: 10.1016/S2215-0366(19)30385-2
99. Kowalski JT, Hauffa R, Jacobs H, Höllmer H, Gerber WD, Zimmermann P. Deployment-related stress disorder in German soldiers. Deutsches Ärzteblatt Int. (2012) 109 (35-36):569–75. doi: 10.3238/arztebl.2012.0569
Keywords: burnout, values, soldiers, military, moral injury, deployment, medical service
Citation: Langner F, Börke AK, Muschner P, Muther M, Reichelt A, Willmund G-D, Wesemann U, Zimmermann PL and Schönsee I (2024) Burnout and moral injuries after foreign deployment among medical personnel of the German armed forces: a pre-post study. Front. Psychiatry 15:1408849. doi: 10.3389/fpsyt.2024.1408849
Received: 28 March 2024; Accepted: 15 July 2024;
Published: 10 September 2024.
Edited by:
Su Lu, De Montfort University, United KingdomReviewed by:
Li Lin, Lingnan University, Hong Kong SAR, ChinaMassimiliano Lorenzo Cappuccio, United Arab Emirates University, United Arab Emirates
Copyright © 2024 Langner, Börke, Muschner, Muther, Reichelt, Willmund, Wesemann, Zimmermann and Schönsee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franziska Langner, ZmxAcHR6Yncub3Jn