 Fanfan Huang†
Fanfan Huang† Wenting Lu†Xiaochuan Zhao
Wenting Lu†Xiaochuan Zhao Na LiTianyu ZhaoShijie GuoBufan LiuRuojia RenLi Yang
Na LiTianyu ZhaoShijie GuoBufan LiuRuojia RenLi Yang Lan WangYuanyuan Gao
Lan WangYuanyuan Gao Ran WangMei SongQuan LinYuehang XuNa JinKuaikuai LiuMeina BaiXueyi Wang*
Ran WangMei SongQuan LinYuehang XuNa JinKuaikuai LiuMeina BaiXueyi Wang*- Mental Health Center, The First Hospital of Hebei Medical University, Hebei Clinical Medical Research Center for Mental Disorders, Shijiazhuang, China
Objectives: This study investigated the prevalence of suicidal ideation (SI) among Chinese medical students and its associated risk factors.
Methods: A total of 6643 medical students (2383 males/4260 females) were recruited from a medical college in Hebei Province, China. Demographic data were collected via a self-administered questionnaire. The Childhood Trauma Questionnaire Short Form (CTQ-SF) was used to evaluate childhood maltreatment (CM), and the Adolescent Self-Rating Life Events Checklist (ASLEC) was used to evaluate the stressful life events. Suicidal ideation was assessed using the Beck Scale for Suicide Ideation (BSSI). Univariate and multivariate logistic regression models were used to analyze the factors affecting SI.
Results: The prevalence of SI in medical students was 11.5% (763/6643). Multivariate logistic regression analysis revealed that SI was significantly associated with younger age, a female sex, being lovelorn, being introverted, experiencing CM during childhood, and experiencing stressful life events within the past 12 months. Of the five subtypes of CM, emotional abuse may have the strongest effect on SI (OR=2.76, 95% CI: 1.72–4.42). The joint effects of CM and stressful life events were significantly associated with an increased risk of SI (OR=5.39, 95% CI: 4.15–6.98).
Conclusion: The prevalence of SI among medical students is high, and medical students who have experienced CM and stressful life events have a higher tendency towards SI. Screening for both CM and stressful life events may be an effective way of identifying individuals at high risk of SI.
Introduction
Suicide is a critical public health concern and the foremost cause of death among people 15–24 years of age (1). The suicide model emphasizes the successive developmental stages of suicidal behavior: suicidal ideation (SI), suicidal plan, suicidal attempt and finally the completion of suicide (2, 3). Based on this theory, SI can be viewed as a sign of subsequent suicidal behavior; the risk of suicide gradually develops from being mild to being high. Suicidal ideation refers to an individual’s willingness to end his or her life by direct or indirect means (4). Although SI does not always lead to death, SI is a major link in the development of fatal suicidal behavior (5). It has been shown that roughly 10% of Chinese adolescents have SI (6); adolescents with SI exhibit a significantly higher risk of suicide (7). Therefore, it is critically important to explore the risk factors of SI with the goal of developing targeted suicide-prevention programs.
Suicidal ideation in adolescents is caused by a complex interaction of physiological and psychosocial factors. Previous studies have demonstrated a significant association between childhood maltreatment (CM) and suicide (8, 9). Childhood maltreatment is typically defined as a significant negative experience in early life. It generally encompasses five subtypes: emotional abuse (EA), emotional neglect (EN), physical abuse (PA), physical neglect (PN), and sexual abuse (SA) (10). The risk of suicide increases by anywhere from 2.7- to 6.1-fold with any type of CM (11). A study of a representative sample of adults (12) similarly found that CM was associated with a significant increase suicide risk in each developmental stage of a suicidal model. Furthermore, previous studies have focused more on the impact of CM on SI and ignored the impact of stressful life events on SI, which are more common and widespread than CM. Stressful life events—such as pressure to perform academically and stressors associated with interpersonal relationships—are associated with SI in college students (13, 14). Stressful life events are a major source of stress for SI, which can strongly predict SI (15) and play a triggering role in suicidal behavior (16). Both CM and stressful life events have a clear impact on SI, but the joint effects of CM and stressful life events on SI have not been explored.
The transition from adolescence to adulthood is an important period of psychological change. During this time, individuals explore their self-identity and values and increase their social responsibilities and expectations about their goals. The uncertainty that marks this period of time may cause adolescents to experience an uptick in mental health problems (17). Compared with non-medical students, medical students typically have a relatively heavy academic schedule, strict clinical work requirements, and they are furthermore exposed to stressors such as patient deaths. Medical students may accordingly have a higher risk of SI. According to previous research, the global prevalence of SI among medical students was 11.1% (18); the prevalence of SI among Chinese medical students was 17.9% (19). This can adversely affect the long-term health of medical students.
It is critical to explore the risk factors of SI in medical students. Although CM is widely recognized to be a strong predictor of SI, the impact of different subtypes of CM on SI remains controversial. In addition, there are no studies have investigated the impact of the joint effects of CM and stressful life events on SI in medical students. This study accordingly investigates the association between SI and different subtypes of CM in a large sample of Chinese medical students and explores the joint effects of CM and stressful life events on SI.
Methods
Study design and participants
The study was a cross-sectional design based on the Internet self-assessment questionnaire, and the research team members of this study served as investigators. The screening tool was an information network evaluation system developed by Saitron Information Co., Ltd., and the whole evaluation process took about 30 minutes. Participants had to be met the following inclusion criteria:(1)age ≥18 years;(2)willingness to sign the consent to participate form. All of the participants were in their sophomore, junior year or senior years of medical undergraduate study at a university in Hebei Province, China. Considering that the final exam may affect the mood of the participants, we recruited the subjects between June 15 and June 27, 2021. Prior to this time period, all participants had completed the final exam. At the same time, the damage caused to human beings by the COVID-19 is gradually decreasing under the natural law, and the reasonable epidemic prevention measures taken by the government have also put students’college life on the right track. Subsequently, the research team conducted a structured interview with all subjects using the Mini-International Neuropsychiatric Interview (MINI 5.0) between October 11 and November 7, 2021, to assess the prevalence of any mental disorders within 12 months.
We have harmonized survey methods and guidelines. First and foremost, all of the medical students who agreed to participate in the study were explained the purpose of the study and provided an official consent form. Second, all of the participants scanned the QR code and logged into the system using a virtual student number and their initials, in this way, the privacy of the participants is protected to the greatest extent. The participants filled in all the information in a quiet classroom, and the research team members of this study answered questions on site. Finally, all the data is sorted out by professional. Of the 7578 participants, 105 were excluded because they refused to participate or asked for leave; we additionally eliminated 297 questionnaires with incomplete data or logical contradictions; 533 were excluded because they had a history of mental disorders. The final sample size was 6643.
The study protocol was approved by the First Hospital of Hebei Medical University Ethics Committee (Code: 20210354).
Assessment of CM
The Childhood Trauma Questionnaire Short Form (CTQ-SF) (20) consists of 28 items and measures childhood abuse and neglect experiences that can be categorized as falling into five subtypes: EA, PA, SA, EN, and PN. The participants were asked about the CM they experienced before turning 16. Subjects with CM were defined as having at least one of following: EA ≥13 points, PA ≥10 points, SA ≥8 points, EN ≥15 points, or PN ≥10 points (21). The Chinese version of CTQ-SF has good validity and reliability (22).
Assessment of stressful life events
The Adolescent Self-Rating Life Events Checklist (ASLEC) was used to assess the negative life events within the past 12 months. The 27-item, Chinese version of the ASLEC developed by Liu (23) is a self-evaluation scale reflecting the physiological and psychological characteristics and social roles of adolescents. There are six dimensions: interpersonal relationships, learning stress, punishment, loss, health & adaptation, and others. Participants were asked if they had experienced any of these life events within the past 12 months. Responses to each item were coded as “yes” or “no” to indicate the presence or absence of the negative life events (no=0, yes=1). The validity and reliability of the ASLEC were proved to be good (24).
Assessment of SI
We used the 19-item Beck Scale for Suicide Ideation (BSSI) (25) to measure the SI of the participants. The first five questions of this scale were used to assess the participants’ SI. If a participants answered “Weak”/“Moderate to strong” to the question “Desire to make active suicide attempt” or answered “Weak”/“Moderate to strong” to the question “Passive suicidal desire”, they were defined as a suicidal ideator (SI). If not, they were defined as a non-suicidal ideator (NSI). For participants with SI, we took the necessary interventions. First of all, we told schools and guardians to strengthen care. Secondly, the research team provided a “green channel” for subjects with SI, that is, under the premise of the participants’ consent, they were provided with one-on-one psychological counseling services, provided psychological support. If necessary, participants are recommended for hospitalization, medication, physiotherapy, and psychotherapy. We also worked with the participants to develop a follow-up plan to prevent unexpected events.
Demographic characteristics
General demographic data—age (years), gender (male/female), only-child status (yes/no), grade (sophomore/junior/senior), parental marital status (both parents/single parent), relationship status (in love/single/lovelorn) and personality characteristics (between introversion and extroversion/introversion/extroversion) were collected from all of the participants.
Statistical analysis
Means (M) and standard deviations (SD) were used for continuous variables, and counts (n) and proportions (%) were used for the categorical variables. T-tests were used to compare the differences in the continuous variables across groups. Chi-square tests were used to analyze the differences in categorical variables across groups. Univariate and multivariate logistic regression analyses were used sequentially to explore associated factors of SI among all of the surveyed medical students. We also performed collinearity diagnostics between variables. Two-sided p-values <0.05 are statistically significant. Crude and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) were computed. All of the analyses were performed using SPSS (version 26.0).
Results
General characteristics of the study participants
The demographic characteristics of the participants are presented in Table 1. The average age of the participants was 21.0 (SD=1.0). Roughly two-thirds (64.1%) of the participants were female. The prevalence of SI was 11.5% among all of the participants. 22.0% of the participants reported at least one adverse childhood experience. Among the various subtypes of CM, 16.8% of the participants reported experiencing PN, 6.7% reported experiencing EN, 2.8% reported experiencing SA, 1.4% reported experiencing EA, and 1.3% reported experiencing PA. Participants with stressful life events accounted for 66.3% of the overall sample.
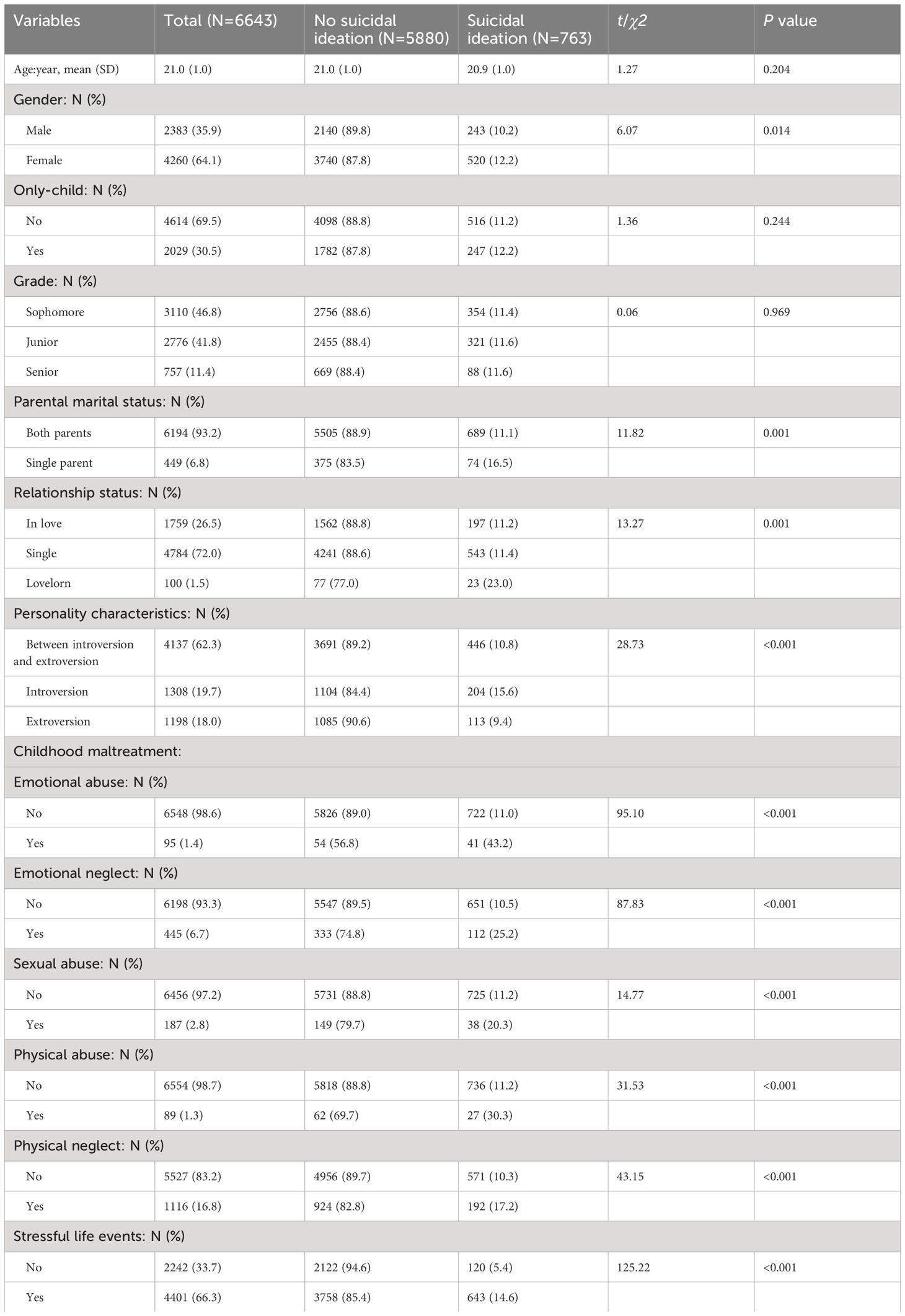
Table 1 Demographic and clinical variables of medical students (N=6,643).
We found statistically significant differences between the SI group and the NSI group in terms of gender (χ2 = 6.07, p=0.014), parental marital status (χ2 = 11.82, p=0.001), relationship status (χ2 = 13.27, p=0.001), personality characteristics (χ2 = 28.73, p<0.001), EA (χ2 = 95.10, p<0.001), EN (χ2 = 87.83, p<0.001),SA (χ2 = 14.77, p<0.001), PA (χ2 = 31.53, p<0.001), PN (χ2 = 43.15, p<0.001) and stressful life events (χ2 = 125.22, p<0.001). There was no significant difference of age, only-child status and grade between the SI group and the NSI group (p >0.05).
Associated factors of SI in medical students
Data from the logistic regression analyses are listed in Table 2. The Hosmer-Lemeshow test revealed that the model fit the data well (χ2 = 15.25, p=0.055). A female sex (OR=1.28, 95% CI: 1.08–1.52), a lovelorn status (OR=2.17, 95% CI: 1.31–3.61), being introversion (OR=1.48, 95% CI: 1.23–1.78), EA (OR=2.76, 95% CI: 1.72–4.42), EN (OR=1.81, 95% CI: 1.39–2.37), PN (OR=1.37, 95% CI: 1.12–1.66) and the occurrence of stressful life events (OR=2.76, 95% CI: 2.25–3.39) were all significantly associated with an increased risk of SI. However, among all five subtypes of CM, we did not find a correlation between PA (p=0.400), SA (p=0.161) and SI. In addition, the age (OR=0.89, 95% CI: 0.80–0.98) was inversely correlated with the risk of SI.
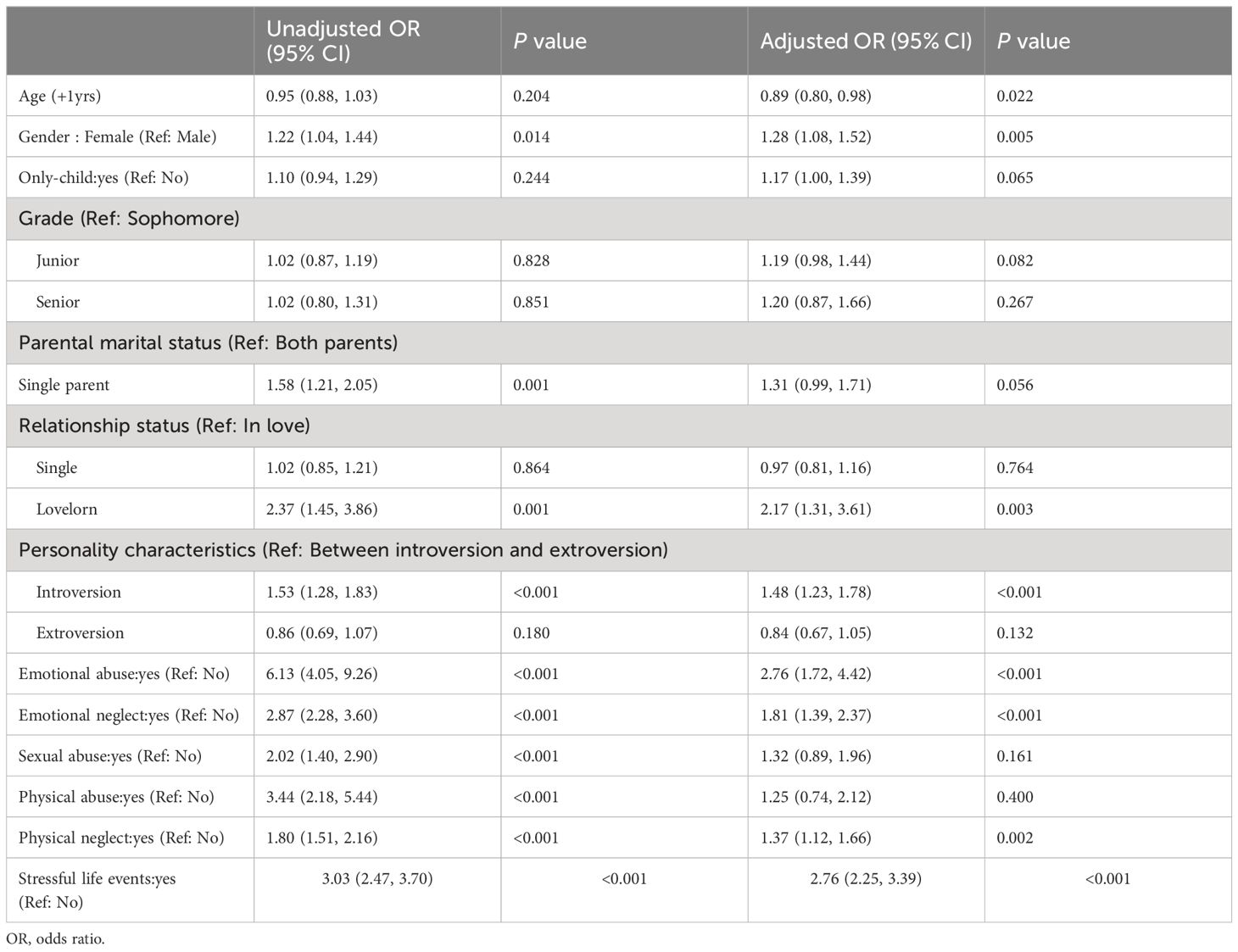
Table 2 Logistic regression analysis of suicidal ideation (N=6,643).
CM, stressful life events, and SI
Table 3 presents data about the impact of the joint effects of CM and stressful life events on SI in our medical-student cohort. The impact of CM and stressful life events on SI were divided into the following four types: (1) Without CM, without stressful life events; (2) Without CM, with stressful life events; (3) With CM, without stressful life events; (4) With CM, with stressful life events. Compared with medical students who experienced neither CM nor stressful life events, students with stressful life events and without CM had a 2.81-fold higher risk of SI (OR=2.81, 95% CI: 2.22–3.57); medical students with CM and without stressful life events had a 2.04-fold higher risk of SI (OR=2.04, 95% CI: 1.33–3.14). We also found that the risk of SI was 5.39-fold higher among medical students with CM and stressful life events (OR=5.39, 95% CI: 4.15–6.98).
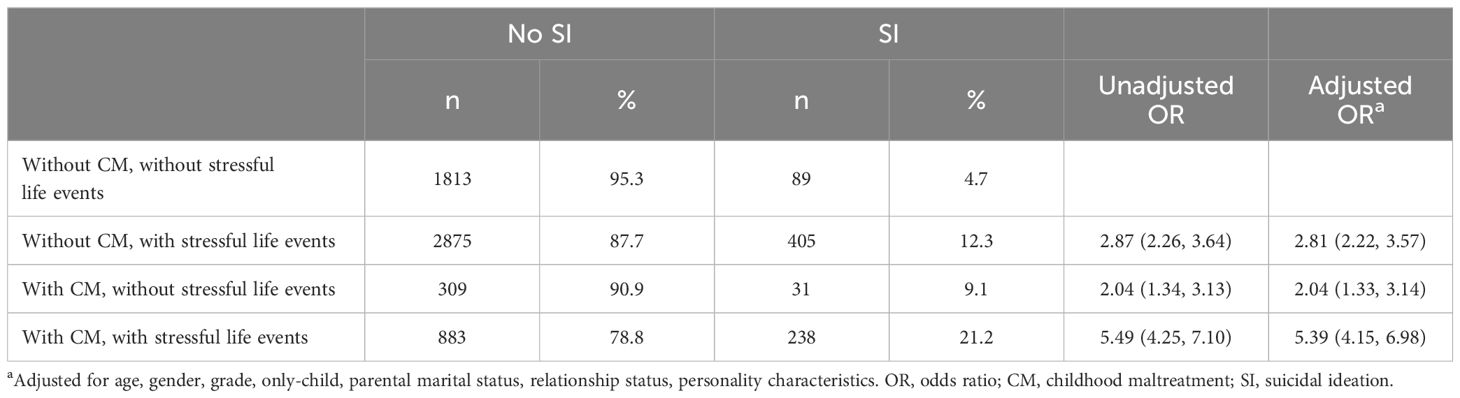
Table 3 Associations between childhood maltreatment, stressful life events, and suicidal ideation (N=6,643).
Discussion
This study investigated the prevalence of SI and its associated risk factors at a medical college in Hebei Province, China. There are several major findings. First, the prevalence of SI among medical students is high. Second, both CM and stressful life events are independently associated with the risk of SI. Third, the joint effects of CM and stressful life events are significantly associated with an increased risk of SI. Our findings highlight that screening for both CM and stressful life events may be an effective way of identifying individuals at high risk of SI.
High prevalence of SI in medical students
We found that the prevalence of SI in medical students was 11.5%, which was higher than the rate reported among other college students in China (7.5%) (26). As mentioned above, the unique nature of medical majors may cause medical students to have more mental stress than non-medical students. Other studies have reported that roughly 10% of medical students experience SI in their lifetime (18, 27), which is similar to our findings. However, some studies (19, 28) have found that the prevalence of SI in medical students is higher than the results that we found. Possible reasons for the difference include study sample size, measurement methods, and cultural differences. For example, some studies only relied on the question “Have you ever had thoughts of committing suicide?”to indicate SI. In our study we used the BSSI scale; this scale has high reliability and validity, and it can more accurately assess the SI of an individual (29).
Associated factors of SI
The significant clinical correlates of SI in our study included younger age, a female sex, being lovelorn, and being introverted. Some studies have shown that females report significantly higher intensity of SI compared to males (30–32). Our study further proves that female students are more likely to have SI than the male. This finding may be related to the fact that the differences in Chinese parenting styles, Chinese families generally believe that more care should be given to the upbringing of girls, and there will be stricter discipline and requirements for boys, so girls’ psychological endurance and resilience will be lower than boys, and girls are more likely to have SI when they encounter adverse events in life (33). Furthermore, neuroendocrine changes that occur in different genders during adolescence may be at play (34). We also found that being lovelorn was at a greater risk of SI. One possible explanation for this finding is when they lack the experience to deal with emotional events, once they have a painful emotional experience, it often brings them psychological wounds that are difficult to heal and promotes SI. Our study found that introversion was a factor that increased the risk of SI, which also aligns with the previous finding that an American study demonstrated that individuals with lower levels of extroversion were more likely to experience SI (35). Introverted personality traits tend to manifest as poorer social interactions, higher levels of feeling loneliness, and lower social connections (36). This may be due to their more sensitive nature, which makes them more susceptible to interpersonal or other problems.
Our study found that all forms of CM, with the exception of PA and SA, had an effect on SI. EA was the strongest predictor of an increased risk of SI among five subtypes of CM. Negative values may be one of the cognitive outcomes of CM (37, 38), and negative values can motivate individuals to react negatively when they experience stress. Previous findings have supported links between CM and suicidal behavior (39, 40). Study has also shown that exposure to traumatic situations during childhood can affect an individual’s proper neurobiological and affective development. EA was the strongest predictor of emotion deregulation (41). CM can lead to negative coping styles and pessimistic worldviews, and indirectly increase the likelihood of suicidal behavior by increasing the risk of impulsivity and hopelessness (42, 43). However, we did not find an association between PA and SI. This result may be related to changes in traditional Chinese parenting styles, which today often replaces corporal punishment with vocal admonishment. No significant association between SA and SI were observed in this study. It was distinctive to the study by Bruffaerts et al., in which SA was the strongest risk factor for the onset of suicidal behaviour, especially during adolescence (44). Differences in study subjects, degree of exposure to the SA experience, or sample size may also contribute to the different results.
The joint effects of CM and stressful life events
We also analyzed the joint effects of CM and stressful life events in relation to SI. Our study found that the joint effects of CM and stressful life events are significantly associated with an increased risk of SI; this finding still remained true after adjusting for confounders. Our finding supports the “cumulative stress hypothesis”, which suggests that neuropsychiatric disorders are largely triggered by the accumulation of multiple major adverse events (45). The continued accumulation of adverse experiences in childhood and adulthood is even more damaging (46). As our research found, the joint effects of CM and stressful life events significantly increase the risk of SI in individuals. The possible reason for this is that early exposure to CM increases an individual’s vulnerability to the effects of later stressful life events. Specifically, the experiences of CM in childhood can reduce an individual’s tolerance to relatively minor stressors, making the individual “sensitive”, which is called stress sensitization effects (47). Findings from our study highlight the need to continually evaluate the mental health status of medical students over time and provide them with appropriate mental health support and mental health services.
Limitations
Several possible limitations to this study should be acknowledged. First, since CM was recalled, there is the potential for recall bias. Second, given that this investigation was a cross-sectional study we could not directly explain the causal relationship between SI and risk factors based on our results. Third, the study, which investigated SI among medical students in Hebei Province, China, has not yet been generalized nationwide, it should be prudent when interpretation and extrapolating our findings. Fourth, other potential contributing factors to SI were not taken into consideration, such as socioeconomic level and family history of mental disorders. Lastly, we did not know exactly when the CM occurred, the impact of CM on SI may vary according to the age at which the maltreatment occurred. Therefore, we need more research to validate our results.
Conclusion
Suicide is the result of an accumulation of risk factors over a lifetime. Suicidal ideation can be considered to be an early warning sign of suicidal behavior, exploring the risk factors for SI is essential for early and effective interventions. This study found that the prevalence of SI was 11.5% among Chinese medical students. Higher rates of SI were associated with younger age, being female, being lovelorn, being introverted, experiencing maltreatment during childhood and stressful life events within the past 12 months. In addition, our findings highlight the potential joint effects of CM and stressful life events on an increased risk of SI. It is critical to screen individuals for CM and stressful life events to identify people at a high risk of SI. Suicide interventions could include reducing adverse childhood experiences and strengthening adaptive coping to stressful life events.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the First Hospital of Hebei Medical University Ethics Committee (Code: 20210354). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. WL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. XZ: Data curation, Investigation, Validation, Writing – original draft. NL: Data curation, Investigation, Validation, Writing – original draft. TZ: Data curation, Investigation, Validation, Writing – original draft. SG: Data curation, Investigation, Validation, Writing – original draft. BL: Data curation, Investigation, Validation, Writing – original draft. RR: Data curation, Investigation, Validation, Writing – original draft. LY: Data curation, Investigation, Validation, Writing – original draft. LW: Data curation, Investigation, Methodology, Validation, Writing – original draft. YG: Data curation, Investigation, Methodology, Validation, Writing – original draft. RW: Data curation, Investigation, Methodology, Validation, Writing – original draft. MS: Data curation, Investigation, Methodology, Validation, Writing – original draft. QL: Data curation, Formal analysis, Investigation, Writing – original draft. YX: Data curation, Formal analysis, Investigation, Writing – original draft. NJ: Data curation, Formal analysis, Investigation, Writing – original draft. KL: Data curation, Formal analysis, Investigation, Writing – original draft. MB: Data curation, Formal analysis, Investigation, Writing – original draft. XW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Key R&D projects in Hebei Province (Grant number: 21377711D); Hebei Provincial science and technology program funding (Grant number: 199776245D); Hebei Province has introduced foreign intellectual projects (Grant number: YZ202306).
Acknowledgments
The authors thank all the participants for their time and efforts.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Neeleman J, Wessely S, Wadsworth M. Predictors of suicide, accidental death, and premature natural death in a general-population birth cohort. Lancet. (1998) 351:93–7. doi: 10.1016/S0140-6736(97)06364-2
3. Sveticic J, De Leo D. The hypothesis of a continuum in suicidality: a discussion on its validity and practical implications. Ment Illn. (2012) 4:e15. doi: 10.4081/mi.2012.e15
4. Posner K, Oquendo MA, Gould M, Stanley B, Davies M. Columbia Classification Algorithm of Suicide Assessment (C-CASA): classification of suicidal events in the FDA’s pediatric suicidal risk analysis of antidepressants. Am J Psychiatry. (2007) 164:1035–43. doi: 10.1176/ajp.2007.164.7.1035
5. Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol Bull. (2016) 143:187–232. doi: 10.1037/bul0000084
6. Peng C, Cheng J, Rong F, Wang Y, Tan Y, Yu Y. Specific effects of five subtypes of childhood maltreatment on suicide behaviours in Chinese adolescents: the moderating effect of sex and residence. Epidemiol Psychiatr Sci. (2023) 32:e45. doi: 10.1017/S2045796023000604
7. Reinherz HZ, Tanner JL, Berger SR, Beardslee WR, Fitzmaurice GM. Adolescent suicidal ideation as predictive of psychopathology, suicidal behavior, and compromised functioning at age 30. Am J Psychiatry. (2006) 163:1226–32. doi: 10.1176/ajp.2006.163.7.1226
8. Chen H, Li W, Cao X, Liu P, Liu J, Chen X, et al. The association between suicide attempts, anxiety, and childhood maltreatment among adolescents and young adults with first depressive episodes. Front Psychiatry. (2021) 12:745470. doi: 10.3389/fpsyt.2021.745470
9. Grillault Laroche D, Godin O, Dansou Y, Belzeaux R, Aouizerate B, Burté T, et al. Influence of childhood maltreatment on prevalence, onset, and persistence of psychiatric comorbidities and suicide attempts in bipolar disorders. Eur Psychiatry. (2022) 65:e15. doi: 10.1192/j.eurpsy.2022.7
10. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. (2003) 27:169–90. doi: 10.1016/S0145-2134(02)00541-0
11. Duke NN, Pettingell SL, McMorris BJ, Borowsky IW. Adolescent violence perpetration: associations with multiple types of adverse childhood experiences. PEDIATRICS. (2010) 125:e778–86. doi: 10.1542/peds.2009-0597
12. Stickley A, Waldman K, Ueda M, Koyanagi A, Sumiyoshi T, Narita Z, et al. Childhood neglect and suicidal behavior: Findings from the National Comorbidity Survey Replication. Child Abuse Negl. (2020) 103:104400. doi: 10.1016/j.chiabu.2020.104400
13. Kang C, Zheng Y, Yang L, Wang X, Zhao N, Guan TF, et al. Prevalence, risk factors and clinical correlates of suicidal ideation in adolescent patients with depression in a large sample of Chinese. J Affect Disord. (2021) 290:272–8. doi: 10.1016/j.jad.2021.04.073
14. Wang C, Mo J, Niu X, Jia X, Lin L. The role of interpersonal problems and family environment in the association between impulsivity and suicidal ideation: A moderate mediation model. J Nerv Ment Dis. (2019) 207:22–8. doi: 10.1097/NMD.0000000000000916
15. Laglaoui Bakhiyi C, Jaussent I, Beziat S, Cohen R, Genty C, Kahn JP, et al. Positive and negative life events and reasons for living modulate suicidal ideation in a sample of patients with history of suicide attempts. J Psychiatr Res. (2017) 88:64–71. doi: 10.1016/j.jpsychires.2016.12.022
16. O’Connor RC, Kirtley OJ. The integrated motivational-volitional model of suicidal behaviour. Philos Trans R Soc Lond B Biol Sci. (2018) 373:20170268. doi: 10.1098/rstb.2017.0268
17. Arnett JJ. Emerging adulthood: the winding road from the late teens through the twenties. 2nd edn. New York: Oxford University Press (2015). doi: 10.1093/acprof:oso/9780199929382.001.0001
18. Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: A systematic review and meta-analysis. JAMA. (2016) 316:2214–36. doi: 10.1001/jama.2016.17324
19. Sun L, Zhou C, Xu L, Li S, Kong F, Chu J. Suicidal ideation, plans and attempts among medical college students in China: The effect of their parental characteristics. Psychiatry Res. (2017) 247:139–43. doi: 10.1016/j.psychres.2016.11.024
20. He J, Zhong X, Gao Y, Xiong G, Yao S. Psychometric properties of the Chinese version of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) among undergraduates and depressive patients. Child Abuse Negl. (2019) 91:102–8. doi: 10.1016/j.chiabu.2019.03.009
21. Walker EA, Unutzer J, Rutter C, Gelfand A, Saunders K, VonKorff M, et al. Costs of health care use by women HMO members with a history of childhood abuse and neglect. Arch Gen Psychiatry. (1999) 56:609–13. doi: 10.1001/archpsyc.56.7.609
22. Fu W, Yao S, Yu H, Zhao X, Li R, Li Y, et al. Initial reliability and validity of childhood trauma questionnaire (CTQ-SF) apllied in Chinese college students. Chin J Clin Psychol. (2005) 13:40–2. doi: 10.16128/j.cnki.1005–3611.2005.01.012
23. Liu X, Liu L, Yang J, Zhao G. Reliability and validity of the adolescents self-rating life events checklist. Chin J Clin Psychol. (1997) 5:34–6. doi: 10.16128/j.cnki.1005-3611.1997.01.01134
24. Xin XH, Yao SQ. Validity and reliability of the adolescent self-rating life events checklist in middle school students. Chin Ment Health J. (2015) 29:355–60. doi: 10.3969/j.issn.1000–6729.2015.05.010
25. Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the Scale for Suicide Ideation. J Consult Clin Psychol. (1979) 47:343–52. doi: 10.1037//0022-006X.47.2.343
26. Huang Q, Lin S, Li Y, Huang S, Liao Z, Chen X, et al. Suicidal ideation is associated with excessive smartphone use among Chinese college students. Front Public Health. (2022) 9:809463. doi: 10.3389/fpubh.2021.809463
27. Li ZZ, Li YM, Lei XY, Zhang D, Liu L, Tang SY, et al. Prevalence of suicidal ideation in Chinese college students: a meta-analysis. PloS One. (2014) 9:e104368. doi: 10.1371/journal.pone.0104368
28. Chen JM, Ai M, Kuang L, Wang MJ, Shen Y, Li DQ, et al. Suicide ideation among college students in Chongqing. Chin J Epidemiol. (2010) 31:290–3. doi: 10.3760/cma.j.isn.0254—6450.2010.03.012
29. Zhang J, Brown GK. Psychometric properties of the scale for suicide ideation in China. Arch Suicide Res. (2007) 11:203–10. doi: 10.1080/13811110600894652
30. Lu L, Xu L, Luan X, Sun L, Li J, Qin W, et al. Gender difference in suicidal ideation and related factors among rural elderly: a cross-sectional study in Shandong, China. Ann Gen Psychiatry. (2020) 19:2. doi: 10.1186/s12991-019-0256-0
31. Otten D, Ernst M, Tibubos AN, Brähler E, Fleischer T, Schomerus G, et al. Does social support prevent suicidal ideation in women and men? Gender-sensitive analyses of an important protective factor within prospective community cohorts. J Affect Disord. (2022) 306:157–66. doi: 10.1016/j.jad.2022.03.031
32. Yang X, Xin M, Liu K, Böke BN. The impact of internet use frequency on non-suicidal self injurious behavior and suicidal ideation among Chinese adolescents: an empirical study based on gender perspective. BMC Public Health. (2020) 20:1727. doi: 10.1186/s12889-020-09866-0
33. Che Y, Fang D, Cai L, Ran H, Chen L, Wang S, et al. Mediation of resilience in the association between personality traits and suicidal ideation among Chinese adolescents. Front Psychol. (2022) 13:898318. doi: 10.3389/fpsyg.2022.898318
34. Rhodes AE, Boyle MH, Bridge JA, Sinyor M, Links PS, Tonmyr L, et al. Antecedents and sex/gender differences in youth suicidal behavior. World J Psychiatry. (2014) 4:120–32. doi: 10.5498/wjp.v4.i4.120
35. Szücs A, Szanto K, Wright AGC, Dombrovski AY. Personality of late- and early-onset elderly suicide attempters. Int J Geriatr Psychiatry. (2020) 35:384–95. doi: 10.1002/gps.5254
36. Su MH, Chen HC, Lu ML, Feng J, Chen IM, Wu CS, et al. Risk profiles of personality traits for suicidality among mood disorder patients and community controls. Acta Psychiat Scand. (2017) 137:30–8. doi: 10.1111/acps.12834
37. Smetana JG, Kelly M, Twentyman CT. Abused, neglected, and nonmaltreated children’s conceptions of moral and social-conventional transgressions. Child Dev. (1984) 55:277–87. doi: 10.2307/1129852
38. Smetana JG, Toth SL, Cicchetti D, Bruce J, Kane P, Daddis C. Maltreated and nonmaltreated preschoolers’ conceptions of hypothetical and actual moral transgressions. Dev Psychol. (1999) 35:269–81. doi: 10.1037//0012-1649.35.1.269
39. Angelakis I, Austin JL, Gooding P. Association of childhood maltreatment with suicide behaviors among young people: A systematic review and meta-analysis. JAMA Netw Open. (2020) 3:e201256. doi: 10.1001/jamanetworkopen.2020.12563
40. Naughton AM, Cowley LE, Tempest V, Maguire SA, Mann MK, Kemp AM. Ask Me! self-reported features of adolescents experiencing neglect or emotional maltreatment: a rapid systematic review. Child Care Health Dev. (2017) 43:348–60. doi: 10.1111/cch.12440
41. Burns E, Jackson J, Harding H. Child maltreatment, emotion regulation, and posttraumatic stress: the impact of emotional abuse. J Aggress Maltreat T. (2010) 19:801–19. doi: 10.1080/10926771.2010.522947
42. Pérez-Balaguer A, Peñuelas-Calvo I, Alacreu-Crespo A, Baca-García E, Porras-Segovia A. Impulsivity as a mediator between childhood maltreatment and suicidal behavior: A systematic review and meta-analysis. J Psychiatr Res. (2022) 151:95–107. doi: 10.1016/j.jpsychires.2022.04.021
43. Li ET, Luyten P, Midgley N. Psychological mediators of the association between childhood emotional abuse and depression: A systematic review. Front Psychiatry. (2020) 11:559213. doi: 10.3389/fpsyt.2020.559213
44. Bruffaerts R, Demyttenaere K, Borges G, Haro JM, Chiu WT, Hwang I, et al. Childhood adversities as risk factors for onset and persistence of suicidal behaviour. Brit J Psychiat. (2010) 197:20–7. doi: 10.1192/bjp.bp.109.074716
45. Rincel M, Aubert P, Chevalier J, Grohard PA, Basso L, Monchaux de Oliveira C, et al. Multi-hit early life adversity affects gut microbiota, brain and behavior in a sex-dependent manner. Brain Behav Immun. (2019) 80:179–92. doi: 10.1016/j.bbi.2019.03.006
46. Holzman C, Eyster J, Tiedje LB, Roman LA, Seagull E, Rahbar MH. A life course perspective on depressive symptoms in mid-pregnancy. Matern Child Health J. (2006) 10:127–38. doi: 10.1007/s10995–005-0044–0
Keywords: suicidal ideation, medical students, prevalence, risk factors, childhood maltreatment, stressful life events
Citation: Huang F, Lu W, Zhao X, Li N, Zhao T, Guo S, Liu B, Ren R, Yang L, Wang L, Gao Y, Wang R, Song M, Lin Q, Xu Y, Jin N, Liu K, Bai M and Wang X (2024) Suicidal ideation in medical students of Hebei province: prevalence and associated factors. Front. Psychiatry 15:1398668. doi: 10.3389/fpsyt.2024.1398668
Received: 10 March 2024; Accepted: 08 July 2024;
Published: 30 July 2024.
Edited by:
Tushar Singh, Banaras Hindu University, IndiaReviewed by:
Gellan Ahmed, Assiut University, EgyptSaurabh Raj, Babasaheb Bhimrao Ambedkar Bihar University, India
Copyright © 2024 Huang, Lu, Zhao, Li, Zhao, Guo, Liu, Ren, Yang, Wang, Gao, Wang, Song, Lin, Xu, Jin, Liu, Bai and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xueyi Wang, MDcwQGhlYm11LmVkdS5jbg==
†These authors have contributed equally to this work