 Erik Ekbäck
Erik Ekbäck Lina Rådmark
Lina Rådmark Jenny Molin1,2
Jenny Molin1,2 Nick Midgley
Nick Midgley Eva Henje
Eva Henje
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 01 May 2024
Sec. Adolescent and Young Adult Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1393066
Introduction: Depression constitutes one of our largest global health concerns and current treatment strategies lack convincing evidence of effectiveness in youth. We suggest that this is partly due to inherent limitations of the present diagnostic paradigm that may group fundamentally different conditions together without sufficient consideration of etiology, developmental aspects, or context. Alternatives that complement the diagnostic system are available yet understudied. The Power Threat and Meaning Framework (PTMF) is one option, developed for explanatory and practical purposes. While based on scientific evidence, empirical research on the framework itself is still lacking. This qualitative study was performed to explore the experiences of adolescents and young adults with depression from the perspective of the PTMF.
Methods: We conducted semi-structured interviews with 11 Swedish individuals aged 15– 22 years, mainly female, currently enrolled in a clinical trial for major depressive disorder. Interviews were transcribed verbatim and analyzed with framework analysis informed by the PTMF.
Results: A complex multitude of adversities preceding the onset of depression was described, with a rich variety of effects, interpretations, and reactions. In total, 17 themes were identified in the four dimensions of the PTMF, highlighting the explanatory power of the framework in this context. Not all participants were able to formulate coherent narratives.
Discussion: The PTMF provides a framework for understanding the complexities, common themes, and lived experiences of young individuals with depression. This may be essential for the development of new interventions with increased precision and effectiveness in the young.
Depression has become the focus of a wealth of research in recent years (1). This is appropriate as major depressive disorder as defined by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) (2) is predicted to soon be the largest individual contributor to the global burden of disease (1, 3). In adolescence the prevalence of depression increases compared to childhood (4, 5), and an early onset predicts a threefold increase in the risk of adult depression (6) as well as a sixfold increase in all-cause mortality (7). Meta-analyses conclude that available interventions for adolescent depression show some promise but lack clear evidence of efficacy (8–13).
The DSM-5 is based on symptom criteria that largely discounts etiology and the subjective understanding of why one is depressed, which likely contributes to its low diagnostic validity for depressive disorders in this age-group (14–17). A shared understanding of the causes and contributing factors is essential for therapeutic alliance, and subjective causal beliefs seem to influence help-seeking (18). An integrated individual understanding also affects compliance with treatment and ability to handle symptoms (19).
Within the body of depression research there are relatively few qualitative studies that elicit the subjective understanding of the condition, and some previous studies have focused on the lived experience of depression among adolescents (20–25). Some investigators have touched upon the topic of potential causes of depression (23, 26–29) and its treatment (23, 30–37). In summary, the etiology is described as multidimensional, often with more than one cause (23, 26–29). Two studies have applied existing frameworks from psychology/social science (27) as well as physical health contexts (28) in the framing of depression. Still, no one has applied a comprehensive theoretical framework to the lived experience of depression in young people that accounts for both psychological, social, and biological factors without narrowly ascribing primacy to any single one of them.
One framework that could be used to do so is the Power Threat Meaning Framework (PTMF) (38). The PTMF is a complement/alternative to diagnosis-based practice that also aims at the identification of patterns in emotional distress, unusual experiences and troubled or troubling behavior. It is both an over-arching structure for identifying such patterns, and a meta-framework within which existing models and bodies of evidence is accommodated. The framework draws on several philosophical principles, theories, stakeholder perspectives, and scientific evidence. For example, it synthesizes the extensive literature pointing to a causal impact of relational and social adversities on human brain development and a range of emotional outcomes. The PTMF argues that distress, although enabled by and mediated by our bodies and biology, has not in any simplistic sense been shown to be caused by them. As experience is produced and perceived in contexts that are not separate from a range of socially constructed power-structures and social interactions, all imbued with personal narratives and meanings, the PTMF suggests that these aspects need to be integrated in our models to increase their explanatory power (38).
The PTMF may be relevant in the context of depression, which is often associated with profound feelings of powerlessness (22, 30). The PTMF postulates that power is a factor that needs to be considered both in turning current epidemiological trajectories around and to increase treatment effectiveness. An augmented threat-reactivity is furthermore characteristic of adolescent depression, with amygdala hyperreactivity to emotional stimuli (39) and an increased allostatic load (40). If the perceived problems, like e.g., power-imbalances in the affected individuals’ immediate and larger relationships and surroundings (23, 28) or subsequently activated/augmented threat reactions (23) are not addressed, it is likely that the affected individual will feel invalidated. If research is found to support the importance of including these factors, that may invite us to rethink the current interventions for depression in the young and inspire new personalized alternatives with better precision and effectiveness.
The aim of this study was to explore the experiences of adolescents and young adults with depression from the perspective of the PTMF.
The study was conducted with individuals who participated in a multi-center randomized controlled trial (RCT) (41) that investigates the effectiveness of interventions for depression at child and adolescent psychiatric outpatient clinics and youth clinics in two county councils in Northern Sweden. The trial has two phases; first, a one-armed clinical pilot (42) examining the experimental intervention called Training for Awareness Resilience and Action (TARA) (43) and second, an RCT in which participants are randomized to TARA or standard treatment, including but not limited to antidepressant medication and/or psychotherapy. The details of the RCT, including, e.g., eligibility criteria, are outlined in the openly available trial-protocol (41) and online pre-registration (clinicaltrials.gov, NCT-registration identifier: NCT04747340).
All individuals that had been enrolled in the pilot or RCT at the end of October 2022 were asked to participate in interviews and all agreed to do so (N=66). From this group, nine individuals were randomly selected and interviewed. Two additional individuals were interviewed with purposive sampling to fill remaining knowledge-gaps, resulting in a sample of 10 females and one male, median age 19 years (range 15-23, IQR 4). This extended age range is motivated by neurobiological similarities between adolescents and young adults (44, 45) and recent calls for a new integrated youth mental health care service in this transitional age range (46). All participants had a clinical diagnosis of major depressive disorder, and the mean score on Reynolds adolescent depression self-rating scale 2nd edition (47) was 79.64 (SD 13.02). This scale has good validity and reliability in similar clinical samples and in the Swedish language (48). All participants were Swedish citizens, one was born in the U.S.A., and six had one parent born abroad (from England, Ghambia, India, Iran, Thailand, and the U.S.A.). None reported being part of any of the official national minorities in Sweden.
TARA participants were interviewed before TARA as the intervention has components that are related to the content of the interviews, and standard treatment participants were interviewed either before, during or after treatment.
Ethical approval was obtained from the national ethical review board, (Dnr 2020-05734 and 2021-06418-02) and all participants had provided written informed consent at the time of consenting for the clinical trial. Additional parental consent was not recommended as mandatory by the national ethical review board, and it was therefore not collected. Selected participants were contacted over the phone for more detailed information and oral consent for the interviews. Participation was voluntary and could be terminated at any time. Interviews were conducted in 2022-2023.
Three interviews were conducted by EE and two by a psychology student, all in person at the participants choice of location, most commonly in private rooms at the university or healthcare centers. Six interviews were conducted by LR through a secure online video platform. A semi-structured interview guide was used, with open-ended questions like, e.g., “I am interested in knowing more about what you think caused or contributed to your depression, what do you think?”. Follow-up questions informed by the PTMF-dimensions were asked to encourage participants to develop their narratives. For example, “Have you experienced anything that made you very scared or powerless?”, and “How did that affect you?”. More open follow-up questions, like “What other factors may have been important in your case?” were also included.
After six interviews the interview guide was modified to better probe different aspects of perceived causality and more details of treatment(s) received. Interviews lasted for 18-90 min (median 74 min) and the shortest one was ended prematurely by the participant due to an emerging painful reluctancy. All participants received a compensation equivalent to 20 Euro. Interviews were audio-recorded and transcribed verbatim.
Data was analyzed using framework analysis (49–52) to elicit the participants’ experiences of depression based on the dimensions of the PTMF. Framework analysis allows researchers to both bring a pre-defined set of issues and be responsive to emerging themes.
Transcripts were read by all five analysts for familiarization, and emergent issues were discussed to get an overall understanding of the data. The text was then divided and condensed into meaning units relevant to the aim of the study, and the meaning units were coded and sorted according to the dimensions of the PTMF (Power, Threat, Meaning, and Threat Response). These steps were performed individually by EE and LR who then compared their work and adjusted as necessary. All analysts then provided input on the sorting and agreed upon the format. The codes in each dimension were then grouped, abstracted, and interpreted into themes. All analysts met regularly in reflective dialogues to discuss interpretations and finally agreed on the structure and content of the results. Analysts were familiar with the PTMF prior to the analysis. The software MAXQDA 22.8.0 (2022, VERBI software GmbH, Berlin Germany) was used, and no AI tools were applied. The Consolidated Criteria for Reporting Qualitative Research (COREQ) (53) guided this report.
The results are presented as 17 themes, all incorporated into the four dimensions of the PTMF, to describe the participants experiences of their depression. An overview of the results is presented in Table 1. An elaboration of the results is presented in text and codes are compared within and across framework dimensions and themes. Quotations are included to illustrate themes and support analytical claims. The quotations have been translated from Swedish to English [translator’s clarifications are bracketed].
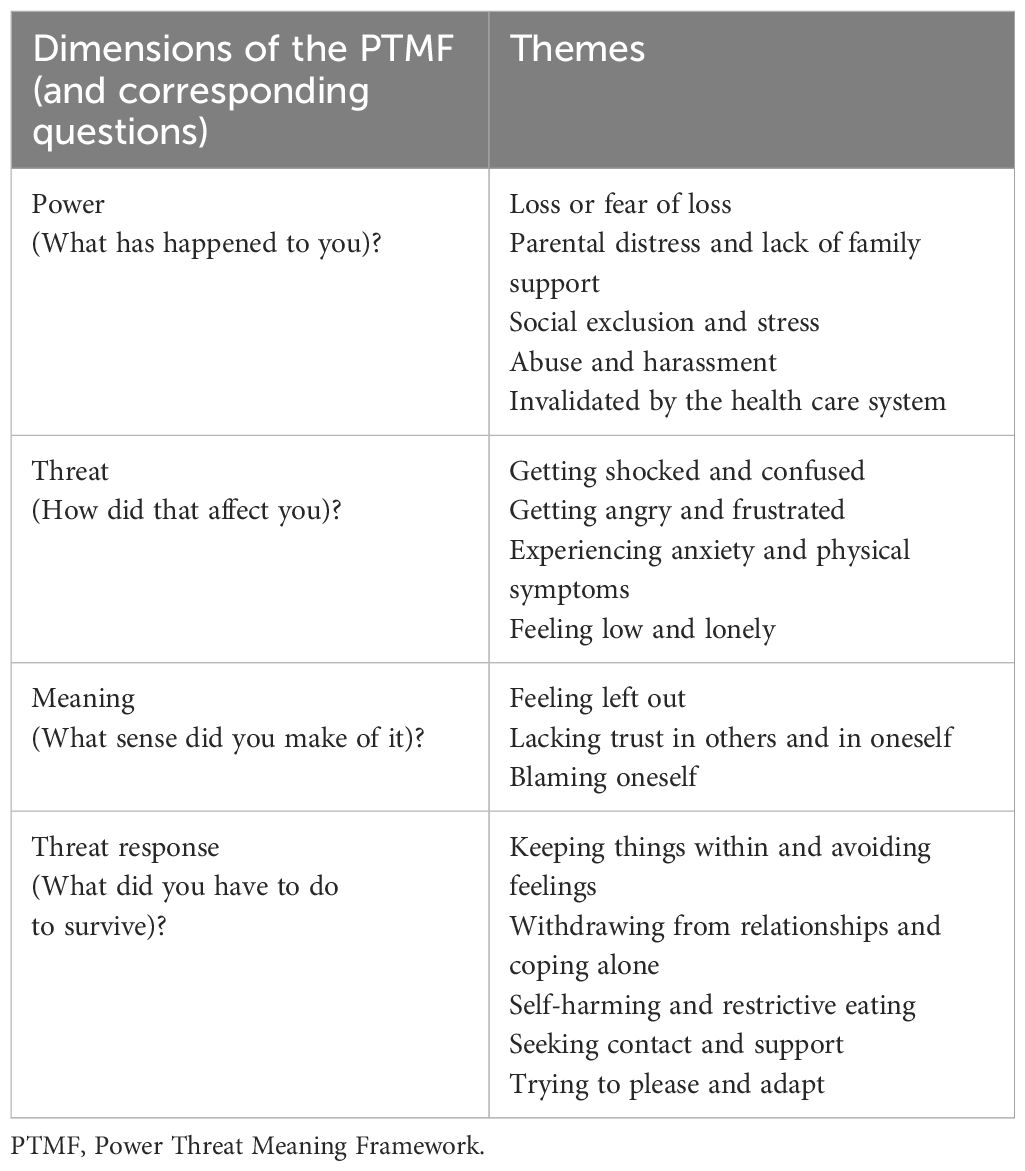
Table 1 Findings based on the PTMF-dimensions.
This dimension of the PTMF corresponds to questions like “What has happened to you?” and “How has power operated in your life?”. Participants described a range of conditions as potentially related to their depression, and our interpretation of the findings in this dimension is elaborated in the five following themes.
Loss was described as a cause for depressive symptoms, e.g., losing community or friends due to moving. Participants also expressed a loss of safety, routines and contact with close ones, e.g., due to parental divorce or the birth of a sibling. Natural changes to the body due to puberty, and diseases or injuries with sometimes permanent sequelae were said to make it hard to exercise or hang out with friends in ways that participants were used to. Participants further mentioned disappearances and deaths, sometimes violently, of family members, close friends and/or pets, and expressed fear that other loved ones would also die.
“I had five rough years where I just lost friend after friend, suicide, diseases, and even a heart attack.” (Participant 5)
Participants described stressful and unsafe home environments with parents who were busy and preoccupied with their own problems and who did not have the time to help them, engage with them, or even listen to them. Some parents were said to not understand participants’ feelings or the severity of their condition, and some had argued that there was no need for the participant to see a psychologist or seek help in other ways.
“Home was never really a safe place. Mom was super sick, very depressed, drank a lot, and took a lot of pills. And dad was super stressed from just taking care of her.” (Participant 2)
Some said their parents struggled with addictions, mental disorders, poverty, and physical disorders. Authoritarian parents were also described, with rigid rules that restricted the families’ and participants’ lives. Some parents were said to be angry with them for being inactive/low, and one participant was kicked out of home. Some participants assumed much responsibility at home, e.g., for siblings or even their parents when they could not cope.
Social exclusion and stress were common topics, and these were often described as persisting common parts of the participants everyday lives. The participants were often bullied in school both by students, teachers, and other school staff. Social media was also described as a stressful platform for social comparison and competition.
“And when they said all those mean things, I started to realize it myself too. I started to think that I was the problem.” (Participant 7)
Some said it was difficult to make new friends even if they wanted to, and therefore they hung out with people despite knowing they were being used by them. There were descriptions of being misunderstood and let down, and not having adults in school that could be trusted. Participants who got in conflict with teachers expressed a lack of support from their peers. Some were struggling with dyslexia, and both before and after receiving this diagnosis participants reported unfair treatment. Additionally, a pressure related to the achievement of high grades was said to come from both teachers, parents, and/or themselves. Outside school hours participants described being left behind as family members took part in social activities without them.
“I had to stay at home and the whole family went away, so I was all alone in the weekends too.” (Participant 9)
Previous and ongoing domestic violence was described, including parental assaults directed to the participants themselves, other adults, siblings and/or pets. Participants described parents and/or stepparents who were aggressive and unpredictable in subjecting the participants and/or others to physical and verbal violence, silencing, withholding of information, and who made uninvited intrusive contact. Destructive romantic relationships and sexual abuse was also described, with examples of being forced to do things without consent and being physically hindered to scream for help.
“If I said no, I knew he would get angry with me, because he got angry a lot. Then it was just like if I said no, and he wanted to have sex, then it was like he just pulled my legs anyway as if I had no choice.” (Participant 5)
Participants also mentioned sexual harassment by strangers on the street, as well as close relationships in which partners and parents had made them feel stupid.
Participants described long waiting times in health care, which contributed to feelings of being insignificant and neglected. Participants also expressed that they were not seen, diminished, and even betrayed by professionals, especially in a child- and adolescent psychiatry. Some described that when trying to explain their problems and feelings, professionals did not seem to understand the nature or severity of their condition, and at times they did not even seem interested in their story.
“Being treated by someone supposed to help you, who doesn’t even know what they’re doing or why they are there, in the end I just sat there in silence.” (Participant 4)
Participants also expressed experiences of not getting better by previous treatments, including antidepressant medication and psychotherapy, which led to feelings of invalidation and a lack of solutions or hope. Antidepressants were said to be prescribed without a treatment plan or follow-up, and participants described a shortage of information as to e.g., for how long they would continue the medication.
This dimension of the PTMF corresponds to questions like “How did that affect you?”. Participants described a variety of ways in which they were affected by being subjected to the different forms of power dynamics described in the previous section, and our interpretation of the findings in this dimension is elaborated in the four following themes.
Participants described being shocked by things that had happened to them, and this was often accompanied by a struggle to understand their situation and their feelings. Unexpected events were said to trigger disbelief and denial. Situations where participants were lacking an understanding of how they got to a particular place or situation were also described, and so was derealization and movie-like experiences. All this was said to raise more questions that mostly ended up leaving participants confused.
“Then when he passed away it was like a piece of me followed him. A piece of me that I knew, disappeared completely. Then there I was, I felt a bit empty, but then also so unreal.” (Participant 4)
Based on being fed up with how things were, participants expressed that irritation and anger were common in their lives. Participants described quarrels, a lot of fighting and screaming, both with parents and friends. Often all persons involved were said to be irritated, which led to misunderstandings and further problems. Both overt hatred and a quieter disappointment was described.
“Everyone said I just got more and more angry, and I had to start seeing a therapist because they said I was having problems with aggression, for taking it out on other things I mean.” (Participant 7)
Negative events were said to trigger fears and expectations that more negative events would occur. This led to worry, fear, social anxiety, and panic attacks that caused avoidance of triggering places and situations. A tendency to overthink and over-analyze was also described, and this was said to make it difficult to sleep or get other important things done.
“I just can’t relax; I must analyze how the person reacted. And I have trouble sleeping from having to go through the entire day before I go to sleep.” (Participant 2)
Physical symptoms like muscular tension and pain were common, and nausea, palpitations, a heaviness in the chest, shortness of breath, lumps in the throat or sense of being strangulated, hair loss, headaches, and stomachaches were described. Previous experiences were also said to have made participants more alert, sensitive, and easily triggered by things, even small insignificant sounds. One participant got really scared if someone sneezed. Participants reported that they vigilantly observed previous perpetrators, often in their home, for indicators of their current mood. If the person raised their voice, touched them, or even stayed silent it was said to indicate that more negative things were coming.
As a result of negative operations of power, participants described getting tired and low, with little or no energy to engage in their everyday lives. Things they used to enjoy were said not to feel as enjoyable. Some said it was hard to start new projects when feeling sick, leading to procrastination. Further descriptions included apathy, depression, and a deep sadness. A sense of loneliness was also common and moreover a “stuck-ness” with oneself and an inability to reach out to others.
“In the beginning I didn’t notice it much, it was more like I just didn’t have any energy to do stuff, it was no longer fun to do things I used to like.” (Participant 8)
This dimension of the PTMF corresponds to questions like “What sense did you make of it?”. Participants described different ways of understanding their situation, and a few participants expressed that they were still struggling to make sense of the meaning of some events. Our interpretation of the findings in this dimension is elaborated in the three following themes.
Participants sometimes interpreted their situation as if they did not belong anywhere. They described that they had nothing in common with the people around them, and therefore had a sense of not fitting in. By not understanding the social codes or themselves in relation to others, and perceiving themselves as embarrassing and in the way, participants expressed that they lost their groups and sense of community and belonging.
“I have nothing in common with them, they laugh at things I don’t understand. I mean it is like I’ve been living underneath a stone my entire life.” (Participant 11)
Participants described insecurities, doubt, and mistrust in others and in themselves. They expressed feeling such as no one could help them and therefore found it hard to rely on others. Others were said not to care. This, and the experience of losing others - which was often interpreted to mean that “goodbye means bye forever” - made some participants draw the conclusion that they were meant to be alone with their problems.
“It becomes a defense mechanism or whatever you call it. I mean the trust you have, in my case to my mom particularly. The thing is now, I can’t trust her the way I did before.” (Participant 1)
On top of that an insecurity regarding their own capability to handle things was expressed. Based on a sense of being wrong, an inability to understand and improve their situation, and not feeling good enough, some were left with a mistrust in their own feelings and thoughts. One said she could not be herself, and others said it was hard to do anything at times of uncertainty.
The participants expressed that they assumed responsibility for many things that had happened to them and/or their friends and family.
“I felt like a failure, inadequate. When I couldn’t fix my parents relationship, and the divorce, like, how was I gonna handle the rest of my life?” (Participant 8)
After situations of abuse a sense of self-disgust was described, and participants blamed themselves for letting perpetrators do things with them. This was also true with bullying. Seeing faults in oneself was said to result in a bad conscience and seeing oneself as a burden, and failures were described, like e.g., not being able to prevent the death of others, and not being able to explain their situation in a way that health care could understand. Others reported that they created problems out of nothing, that they just exaggerated the problem and overreacted. One said it was like they had “a ghost in the brain”, and others said that if it wasn’t for them problems wouldn’t have happened.
This dimension of the PTMF corresponds to questions like “What did you have to do to survive?”. Participants reflected on a variety of coping strategies that they used to handle their situation, and our interpretation is elaborated in the five following themes.
Participants described that they often handled their situation by not talking about problems, sometimes to spare their friends and family from trouble. It was also said that feelings were kept inside, often in attempts to be carefree and “happy-go-lucky “– which sometimes annoyed people around them. Some said they avoided thinking about the situation altogether, pushing things away or denying them. One said she told her parents the truth all at once and that this was not common for her.
“When I got to see a child psychiatrist, that’s when my mom really got to understand that I actually had been feeling really bad. I had not let her know about that until then.” (Participant 5)
Participants described isolating themselves, as sometimes it was said to be easier to be alone. Refusing to go to school, sometimes for several years, was said to negatively affect their grades. A fear of leaving home was expressed, as home was sometimes the only place where they could feel safe and in control. For some, the isolation was said to be an escape, as getting away was sometimes the only possible thing to do. Some said they hung out with others only on the internet as a way of hiding and protecting themselves.
“I stopped having contact with my friends in school. I didn’t want to talk to them, I was so ashamed, so I have stopped talking to them completely.” (Participant 6)
Participants also described things they did on their own to try to accept or improve their situation. Some reflected and made plans, others expressed a need to withdraw to spend time with their thoughts and feelings here and now. Some said they used music, movies, or physical exercise to relax and avoid rumination.
“Getting back from the walk, I have had the time to think and can handle my emotions better, like is this really my fight? No, then I don’t have to get as offended when they are the ones with problems. I can put it to the side a little.” (Participant 1)
Participants expressed an urge to harm themselves in different ways, often as other strategies or means of expression were lacking. Knives, blunt objects, and tools were used to injure oneself. Some smoked large amounts of cigarettes and used alcohol and other drugs for this purpose. Participants also described being preoccupied with food and their weight, sometimes restricting their eating, and sometimes also binging as vengeance to parents who had said they ate too much.
“That [restricted eating] is something I can control, I guess the other things become less in your face when there is at least something you can control.” (Participant 10)
Help seeking was described by some participants, including seeing psychologists to discuss the situation and find support. Some also described close relationships as important, and family members, teachers and friends who were described as invaluable support. To actively seek out and protect such supportive individuals was a strategy for some. Romantic relationships were sometimes also described as helpful. While some enjoyed opportunities to share their story with other young people in similar situations, others expressed a value in being surrounded by animals.
“To hear someone else [here at the youth clinic] explain that it is not all that strange that I think along these lines, it makes things easier somehow.” (Participant 3)
Participants described that they avoided conflicts in every possible way and did their best to understand others’ feelings, thoughts and needs in order to please them. Some said they tried to compensate for perceived shortcomings by making others happy and satisfied, no matter the cost, and friends were sometimes bought with money or favors. Additionally, participants said they tried to be normal and inconspicuous to fit in.
“Something that I have had to learn is to analyze everything that happens around me. To always sense what someone needs or if something is wrong, maybe even before they say they need something.” (Participant 10)
This study explored the experiences of adolescents and young adults with depression from the perspective of the PTMF (38). While the PTMF is based on research, few studies have investigated it empirically in a clinical context. This is perhaps because it has a high level of complexity, with implications that challenge us to rethink key aspects of current psychiatric care and treatment.
In the present study it was feasible to apply the PTMF in the collection and analysis of data, and the dimension of “power” was clearly identified in the interviews. Data contained readily appearing and clearly traumatizing experiences that have all been previously implicated in depression in young people (54–58). We replicate previous findings of interpersonal problems (23, 26, 27, 29) pressure (23, 29), and loss (28) as central to adolescent depression, their common power-related denominator has however previously been largely unrecognized.
The second dimension of “threat” originally refers to what core human needs are threatened by the described negative operations of power. In our sample participants did not spontaneously identify core human needs as threatened in their responses to questions on how they were affected. Themes in this dimension reflect more autonomic stress and threat reactions. This may be due to the questions which were openly formulated. Participants were also relatively young for an analysis of their situation on this level, and potentially the current depression limited their metacognitive capacity. However, in the dimension of “meaning”, the need to belong was prominent, indicating that the ability to identify needs was present. Perhaps some experiences do cut across framework dimensions and therefore fit in more than one. It was expected that the framework would have areas of better and worse fit, as this has been described in previous framework analyses (49, 52).
Subsequent “threat responses” or coping strategies varied in quality and some participants described self-perpetuating negative spirals, e.g., the threat reaction of isolation led to poor school performance, which in turn led to new spirals of school stress and fear of losing other things. In the analysis it was sometimes challenging to see where one chain of events ended and a new one started, and this is acknowledged by the original authors (38). Also, some participants appeared to suffer from dissociation, and some were unable to form a coherent narrative which complicated the matter. To analyze meaning, form a coherent narrative, and regulate emotions are processes that require a coordination of several high-level processes (59), and in young people with depression the fronto-limbic maturation process is delayed in comparison to healthy individuals (60). This, and the inclusions of participants that had not achieved full integration of previous traumatic experiences, can potentially explain the described difficulties. Furthermore, only negative interpretations/meanings were voiced, which may reflect the participants depressed state. The same may be true for negative views on previous therapists and interventions.
Importantly, we identified different meanings ascribed to apparently similar situations and diagnostic labels, indicating the value of personalized approaches to understand, describe, validate, and treat depression successfully. We foresee that contextual, diagnostic, and biomedical approaches to understand, describe and manage depression will complement each other and lead to improved outcomes over time.
Even within the current diagnostic paradigm, trauma informed approaches to depression treatment may be motivated in young people. In this context the PTMF may be helpful in eliciting adverse experiences that were previously obscured. As there is a growing body of evidence that suggests that difficult lives explain depression better than broken brains (61, 62), treatment approaches that acknowledge this can potentially be more effective than interventions that primarily deal with downstream symptoms. One implication of our findings on the relevance of negative operations of power in the context of depression is that intersectional analyses of these mechanisms may be useful, both to enable individual empowerment, restored self-confidence and better life navigation skills as part of depression treatment. Policy reforms aimed to prevent depression in young people may also benefit from such analyses.
Limitations: The interviews might be considered as brief and few when trying to understand the complex phenomena behind depression. We determined the information density to be high, and the material was rich enough for analysis. Only one participant was male however, which may affect transferability. By bringing the PTFM both to the interview design and data analysis, there an almost inevitable risk of “finding” what was simply assumed a priori. To minimize this risk, we carefully searched for meaning units, codes and themes that did not fit within the PTMF, without any such findings. Also, methodological and epistemological triangulation was used by performing framework analysis (51). This allowed us to draw upon existing knowledge and yet not be limited by it, as both realist and constructionist epistemologies were applied. To our knowledge this is the first time that this approach is applied within clinical psychiatry.
Strengths include that that the study gives voice to young people with depression, a group with limited abilities and opportunities to express themselves and be fully heard. The study constitutes a real-world application of the PTMF in a diverse ethnical sample and may contribute to a paradigm shift in the way we conceptualize and address mental disorders at large.
In the last decades there has hardly been any pragmatic or clinically useful alternative available to DSM diagnosis-based practice, and the biomedical and pharmaceutical approach that follows from it may obscure individual needs and lead to missed opportunities for interventions to meet those needs. The PTMF provides an alternative understanding of depression in young people. It is internally coherent and compatible both with the present qualitative data and with previous studies and models of youth depression. As the negative operation of various forms of power appears to be related to the onset of depression in young people, we echo the United Nations special rapporteur: “Mental health policies should begin to address power imbalances rather than chemical imbalances” (63). This approach may improve our understanding of depression and inspire the development of new interventions with increased precision and effectiveness.
EE is a male resident in family medicine and doctoral student in child and adolescent psychiatry. LR is a female pharmacist with a PhD in clinical neuroscience. JM is a female mental health nurse and associate professor in nursing. MS is a female specialist physiotherapist and associate professor in physiotherapy. NM is a male child psychotherapist and a professor of psychological therapies with children and young people. EH is a female specialist and professor in Child and adolescent psychiatry, she developed the TARA intervention. None of the authors had any therapeutic or other relationship to any of the participants and participants were not given any specific information about the researchers. All authors had experience of qualitative research in this area.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was approved by the Swedish national ethical review board, (Dnr 2020-05734 and 2021-06418-02). The study was conducted in accordance with the local legislation and institutional requirements. All participants provided written informed consent. Additional parental consent for participants below 18 years of age was not recommended as mandatory by the national ethical review board.
EE: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. LR: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology. JM: Writing – review & editing, Conceptualization, Formal analysis, Investigation, Methodology. MS: Writing – review & editing, Formal analysis. NM: Methodology, Writing – review & editing. EH: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the County Council of the Region Västerbotten; the County Council of the Region Västernorrland, municipality of Örnsköldsvik and the Kempe foundation under grant nr. LVNFOU933598; the Swedish Society of Medicine under grant nr. SLS-935854; Lars Jacob Boëthius foundation; Fredrik and Ingrid Thurings foundation; and the Oskar-foundation. The funders had no role in the study design, data collection, analysis, interpretation, writing the report or decision to submit the article for publication.
The authors would like to thank the participants for their individual contributions to this study, Mio Negga for conducting two interviews, and Elisabeth Loisel for transcribing the recordings.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Santomauro DF, Herrera AMM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. (2021) 398:1700–12. doi: 10.1016/S0140-6736(21)02143-7
2. APA. Diagnostic and statistical manual of mental disorders. 5th edition. Arlington, VA, USA: American psychiatric publishing (2013).
3. Lepine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat. (2011) 7:3–7. doi: 10.2147/NDT
4. Avenevoli S, Swendsen J, He JP, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psychiatry. (2015) 54:37–44.e2. doi: 10.1016/j.jaac.2014.10.010
5. Lebrun-Harris LA, Ghandour RM, Kogan MD, Warren MD. Five-year trends in US children’s health and well-being, 2016-2020. JAMA Pediatr. (2022) 176:e220056. doi: 10.1001/jamapediatrics.2022.0056
6. Johnson D, Dupuis G, Piche J, Clayborne Z, Colman I. Adult mental health outcomes of adolescent depression: A systematic review. Depress Anxiety. (2018) 35:700–16. doi: 10.1002/da.2018.35.issue-8
7. Leone M, Kuja-Halkola R, Leval A, D’Onofrio BM, Larsson H, Lichtenstein P, et al. Association of youth depression with subsequent somatic diseases and premature death. JAMA Psychiatry. (2020) 78(3):302–10. doi: 10.1001/jamapsychiatry.2020.3786
8. Cox GR, Callahan P, Churchill R, Hunot V, Merry SN, Parker AG, et al. Psychological therapies versus antidepressant medication, alone and in combination for depression in children and adolescents. Cochrane Database Syst Rev. (2014) 11:Cd008324. doi: 10.1002/14651858.CD008324.pub3
9. Cipriani A, Zhou X, Del Giovane C, Hetrick SE, Qin B, Whittington C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet. (2016) 388:881–90. doi: 10.1016/S0140-6736(16)30385-3
10. Zhou X, Hetrick SE, Cuijpers P, Qin B, Barth J, Whittington CJ, et al. Comparative efficacy and acceptability of psychotherapies for depression in children and adolescents: A systematic review and network meta-analysis. World Psychiatry. (2015) 14:207–22. doi: 10.1002/wps.v14.2
11. Yang L, Zhou X, Zhou C, Zhang Y, Pu J, Liu L, et al. Efficacy and acceptability of cognitive behavioral therapy for depression in children: A systematic review and meta-analysis. Acad Pediatr. (2017) 17:9–16. doi: 10.1016/j.acap.2016.08.002
12. Zhou X, Teng T, Zhang Y, Del Giovane C, Furukawa TA, Weisz JR, et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: a systematic review and network meta-analysis. Lancet Psychiatry. (2020) 7:581–601. doi: 10.1016/S2215-0366(20)30137-1
13. Weisz JR, Venturo-Conerly KE, Fitzpatrick OM, Frederick JA, Ng MY. What four decades of meta-analysis have taught us about youth psychotherapy and the science of research synthesis. Annu Rev Clin Psychol. (2023) 19:79–105. doi: 10.1146/annurev-clinpsy-080921-082920
14. Alexandrino-Silva C, Wang YP, Carmen Viana M, Bulhões RS, Martins SS, Andrade LH. Gender differences in symptomatic profiles of depression: results from the São Paulo Megacity Mental Health Survey. J Affect Disord. (2013) 147:355–64. doi: 10.1016/j.jad.2012.11.041
15. Blom EH, Forsman M, Yang TT, Serlachius E, Larsson JO. Latent classes of symptoms related to clinically depressed mood in adolescents. Scand J Child Adolesc Psychiatr Psychol. (2014) 2:19–28. doi: 10.21307/sjcapp-2014-004
16. BPS. Classification of behaviour and experience in relation to functional psychiatricdiagnoses: Time for a paradigm shift. In: DCP Position Statement. The British Psychological Society, Leichester (2013).
17. Manfro PH, Pereira RB, Rosa M, Cogo-Moreira H, Fisher HL, Kohrt BA, et al. Adolescent depression beyond DSM definition: a network analysis. Eur Child Adolesc Psychiatry. (2021) 32(5):881–92. doi: 10.1007/s00787-021-01908-1
18. O’Neill A, Humphrey N, Stapley E. A systematic review of qualitative research focusing on emotional distress among adolescents: perceived cause and help-seeking. Adolesc Res Review. (2023) 8:387–402. doi: 10.1007/s40894-022-00203-7
19. Nunstedt H, Nilsson K, Skärsäter I, Kylén S. Experiences of major depression: individuals’ Perspectives on the ability to understand and handle the illness. Issues Ment Health Nursing. (2012) 33:272–9. doi: 10.3109/01612840.2011.653038
20. Wisdom JP, Green CA. “Being in a funk”: teens’ efforts to understand their depressive experiences. Qual Health Res. (2004) 14:1227–38. doi: 10.1177/1049732304268657
21. Woodgate RL. Living in the shadow of fear: adolescents’ lived experience of depression. J Adv Nurs. (2006) 56:261–9. doi: 10.1111/j.1365-2648.2006.04020.x
22. Farmer TJ. The experience of major depression: adolescents’ perspectives. Issues Ment Health Nurs. (2002) 23:567–85. doi: 10.1080/01612840290052776
23. Ross E, Ali A, Toner B. Investigating issues surrounding depression in adolescent girls across Ontario: a participatory action research project. Can J Commun Ment Health. (2003) 22:55–68. doi: 10.7870/cjcmh-2003-0004
24. Midgley N, Parkinson S, Holmes J, Stapley E, Eatough V, Target M. Beyond a diagnosis: The experience of depression among clinically-referred adolescents. J Adolesc. (2015) 44:269–79. doi: 10.1016/j.adolescence.2015.08.007
25. De Mol J, D’Alcantara A, Cresti B. Agency of depressed adolescents: embodiment and social representations. Int J Qual Stud Health Well-being. (2018) 13:1564516. doi: 10.1080/17482631.2018.1564516
26. Radovic A, Gmelin T, Stein BD, Miller E. Depressed adolescents’ positive and negative use of social media. J Adolesc. (2017) 55:5–15. doi: 10.1016/j.adolescence.2016.12.002
27. Rose-Clarke K, Hassan E, Bk P, Magar J, Devakumar D, Luitel NP, et al. A cross-cultural interpersonal model of adolescent depression: A qualitative study in rural Nepal. Soc Sci Med. (1982) 2021:270. doi: 10.1016/j.socscimed.2020.113623
28. Bear HA, Krause KR, Edbrooke-Childs J, Wolpert M. Understanding the illness representations of young people with anxiety and depression: A qualitative study. Psychol Psychother. (2021) 94:1036–58. doi: 10.1111/papt.12345
29. Midgley N, Parkinson S, Holmes J, Stapley E, Eatough V, Target M. “Did I bring it on myself?” An exploratory study of the beliefs that adolescents referred to mental health services have about the causes of their depression. Eur Child Adolesc Psychiatry. (2017) 26:25–34. doi: 10.1007/s00787-016-0868-8
30. Maroun RA, Thackeray LA, Midgley N. Meaning and medication: a thematic analysis of depressed adolescents’ views and experiences of SSRI antidepressants alongside psychological therapies. BMC Psychiatry. (2018) 18:374. doi: 10.1186/s12888-018-1961-y
31. Weitkamp K, Klein E, Midgley N. The experience of depression: A qualitative study of adolescents with depression entering psychotherapy. Glob Qual Nurs Res. (2016) 3:2333393616649548. doi: 10.1177/2333393616649548
32. O’Keeffe S, Martin P, Target M, Midgley N. ‘I just stopped going’: A mixed methods investigation into types of therapy dropout in adolescents with depression. Front Psychol. (2019) 10:75. doi: 10.3389/fpsyg.2019.00075
33. Midgley N, Holmes J, Parkinson S, Stapley E, Eatough V, Target M. “Just like talking to someone about like shit in your life and stuff, and they help you”: Hopes and expectations for therapy among depressed adolescents. Psychother Res. (2016) 26:11–21. doi: 10.1080/10503307.2014.973922
34. Housby H, Thackeray L, Midgley N. What contributes to good outcomes? The perspective of young people on short-term psychoanalytic psychotherapy for depressed adolescents. PloS One. (2021) 16:e0257334. doi: 10.1371/journal.pone.0257334
35. Wilmots E, Midgley N, Thackeray L, Reynolds S, Loades M. The therapeutic relationship in Cognitive Behaviour Therapy with depressed adolescents: A qualitative study of good-outcome cases. Psychol Psychother. (2020) 93:276–91. doi: 10.1111/papt.12232
36. Herring GT, Loades ME, Higson-Sweeney N, Hards E, Reynolds S, Midgley N. The experience of cognitive behavioural therapy in depressed adolescents who are fatigued. Psychol Psychother. (2022) 95:234–55. doi: 10.1111/papt.12365
37. Reinodt S, Haglund E, Bremander A, Jarbin H, Larsson I. Adolescents’ Long-term experiences of manageability, comprehensibility, and meaningfulness of a group-based exercise intervention for depression. Int J Environ Res Public Health. (2022) 19(5):2894. doi: 10.3390/ijerph19052894
38. Johnstone LB M, Cromby J, Dillon J, Harper D, Kinderman P, Longden E, et al. The Power Threat Meaning Framework: Towards the identification of patterns in emotional distress, unusual experiences and troubled or troubling behaviour, as an alternative to functional psychiatric diagnosis. Leichester: British Psychological Society (2018).
39. Yang TT, Simmons AN, Matthews SC, Tapert SF, Frank GK, Max JE, et al. Adolescents with major depression demonstrate increased amygdala activation. J Am Acad Child Adolesc Psychiatry. (2010) 49:42–51. doi: 10.1097/00004583-201001000-00008
40. National, Scientific, Council, on, the, Developing, Child. Connecting the brain to the rest of the body: early childhood development and lifelong health are deeply intertwined: working paper no. 15 (2020)Available online at: www.developingchild.harvard.edu.
41. Ekbäck E, Granåsen G, Svärling R, Blomqvist I, Henje E. Clinical effectiveness of training for awareness resilience and action online compared to standard treatment for adolescents and young adults with depression: study protocol and analysis plan for a pragmatic, multi-center randomized controlled superiority trial. Front Psychiatry. (2021) 12:674583. doi: 10.3389/fpsyt.2021.674583
42. Ekbäck E, Rådmark L, Granåsen G, Svärling R, Sörlin M, Schönbeck C, et al. Clinical effectiveness of training for awareness, resilience, and action for adolescents and young adults with depression: The pilot phase of a multicenter randomized controlled trial. Front Psychiatry. (2023) 14. doi: 10.3389/fpsyt.2023.1130035
43. Henje Blom E, Duncan LG, Ho TC, Connolly CG, LeWinn KZ, Chesney M, et al. The development of an RDoC-based treatment program for adolescent depression: “Training for Awareness, Resilience, and Action” (TARA). Front Hum Neurosci. (2014) 8:630. doi: 10.3389/fnhum.2014.00630
44. Bethlehem RAI, Seidlitz J, White SR, Vogel JW, Anderson KM, Adamson C, et al. Brain charts for the human lifespan. Nature. (2022) 604:525–33. doi: 10.1038/s41586-022-04554-y
45. Shaw P, Kabani NJ, Lerch JP, Eckstrand K, Lenroot R, Gogtay N, et al. Neurodevelopmental trajectories of the human cerebral cortex. J Neurosci. (2008) 28:3586–94. doi: 10.1523/JNEUROSCI.5309-07.2008
46. McGorry PD, Mei C, Chanen A, Hodges C, Alvarez-Jimenez M, Killackey E. Designing and scaling up integrated youth mental health care. World Psychiatry. (2022) 21:61–76. doi: 10.1002/wps.20938
47. Reynolds WM. Reynolds adolescent depression scale. In: Professional manual, 2nd edition. Psychological Assessment Resources, Odessa (FL (2002).
48. Ekbäck E, Blomqvist I, Dennhag I, Henje E. Psychometric properties of the Swedish version of the Reynolds Adolescent Depression Scale second edition (RADS-2) in a clinical sample. Nord J Psychiatry. (2022) 77(4):383–92. doi: 10.1080/08039488.2022.2128409
49. Parkinson S, Eatough V, Holmes J, Stapley E, Midgley N. Framework analysis: a worked example of a study exploring young people’s experiences of depression. Qual Res Psychol. (2016) 13:109–29. doi: 10.1080/14780887.2015.1119228
50. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. (2013) 13:117–. doi: 10.1186/1471-2288-13-117
51. Ritchie J SL. Analyzing qualitative data, Chapter 9: Qualitative data analysis for applied policy research. Bryman BBR, editor. London and New York: Routledge (1994).
52. Goldsmith L. Using framework analysis in applied qualitative research. In: Qualitative report. (2021) 26(6):2061–76. doi: 10.46743/2160-3715/2021.5011
53. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
54. Kendler KS, Karkowski LM, Prescott CA. Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry. (1999) 156:837–41. doi: 10.1176/ajp.156.6.837
55. Friis RH, Wittchen HU, Pfister H, Lieb R. Life events and changes in the course of depression in young adults. Eur Psychiatry. (2002) 17:241–53. doi: 10.1016/S0924-9338(02)00682-X
56. Pine DS, Cohen P, Johnson JG, Brook JS. Adolescent life events as predictors of adult depression. J Affect Disord. (2002) 68:49–57. doi: 10.1016/S0165-0327(00)00331-1
57. Kendler KS, Hettema JM, Butera F, Gardner CO, Prescott CA. Life event dimensions of loss, humiliation, entrapment, and danger in the prediction of onsets of major depression and generalized anxiety. Arch Gen Psychiatry. (2003) 60:789–96. doi: 10.1001/archpsyc.60.8.789
58. Andersen SL, Teicher MH. Stress, sensitive periods and maturational events in adolescent depression. Trends Neurosci. (2008) 31:183–91. doi: 10.1016/j.tins.2008.01.004
59. Ahmed SP, Bittencourt-Hewitt A, Sebastian CL. Neurocognitive bases of emotion regulation development in adolescence. Dev Cognit Neurosci. (2015) 15:11–25. doi: 10.1016/j.dcn.2015.07.006
60. Yang TT, Simmons AN, Matthews SC, Tapert SF, Frank GK, Bischoff-Grethe A, et al. Depressed adolescents demonstrate greater subgenual anterior cingulate activity. Neuroreport. (2009) 20:440–4. doi: 10.1097/WNR.0b013e3283262e10
61. Moncrieff J, Cooper RE, Stockmann T, Amendola S, Hengartner MP, Horowitz MA. Difficult lives explain depression better than broken brains. Mol Psychiatry. (2024). doi: 10.1038/s41380-024-02462-3
62. de Lacy N, Ramshaw MJ, McCauley E, Kerr KF, Kaufman J, Nathan Kutz J. Predicting individual cases of major adolescent psychiatric conditions with artificial intelligence. Transl Psychiatry. (2023) 13:314. doi: 10.1038/s41398-023-02599-9
Keywords: depression, adolescents, young adults, qualitative research, framework analysis
Citation: Ekbäck E, Rådmark L, Molin J, Strömbäck M, Midgley N and Henje E (2024) The Power Threat Meaning Framework: a qualitative study of depression in adolescents and young adults. Front. Psychiatry 15:1393066. doi: 10.3389/fpsyt.2024.1393066
Received: 28 February 2024; Accepted: 15 April 2024;
Published: 01 May 2024.
Edited by:
Francesco Monaco, Azienda Sanitaria Locale Salerno, ItalyReviewed by:
Pasquale Scognamiglio, ASL Napoli 3 Sud, ItalyCopyright © 2024 Ekbäck, Rådmark, Molin, Strömbäck, Midgley and Henje. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Erik Ekbäck, ZXJpay5la2JhY2tAdW11LnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.