 Nicolas A. Nuñez
Nicolas A. Nuñez Boney Joseph
Boney Joseph Gustavo H. Vazquez
Gustavo H. Vazquez- 1Department of Psychiatry, University of Utah, Salt Lake City, UT, United States
- 2Department of Psychiatry & Psychology, Mayo Clinic, Rochester, MN, United States
- 3Department of Neurology, Mayo Clinic, Rochester, MN, United States
- 4Department of Psychiatry, Queen's University, Kingston, ON, Canada
- 5International Consortium for Mood & Psychotic Disorder Research, McLean Hospital, Belmont, MA, United States
Editorial on the Research Topic
Old treatments new outcomes-augmentation treatments for depression
Introduction
Depression has become one of the most common and disabling mental disorders in the last years. Amongst adults, the literature has underscored a trend increase of depression (1) particularly with a worldwide prevalence increase of bipolar disorder (BD) reaching approximately 3% (2). Given that BD is a recurrent condition characterized by profound mood fluctuations spanning from mania/hypomania to severe depression, it is notable that the depressive phase of the illness contributes to a significant functional impairment and a diminished quality of life (3). In addition, established treatments have not modified drastically response and remission rates and in a few cases led to significant side effects that may contribute ultimately, to poor treatment adherence. Approximately one-third of patients do not respond and thus, may be considered treatment resistant (4). Different international guidelines have suggested multiple strategies such as a combination of different antidepressants or augmentation strategies with antipsychotics, mood stabilizers (lithium), or even different agents such as liothyronine and stimulants; however, the selection of these strategies still remains inconclusive with dearth of studies examining evidence base thoroughly (5). Augmentation strategies with compounds such as stimulants have been reported as early as the 1930s although concerns regarding substance abuse, risk for mood destabilization, and overall efficacy have been raised. Nevertheless, stimulant medications have been recognized in the literature as second and fourth-line therapy for patients specifically with BD. Specially of concern are how to select and personalize augmentation strategies in patients also with medical conditions. Additionally lifetime healthy behaviors such as exercise has shown its importance in reducing or alleviating depressive symptoms (6). Therefore, new ways of framing our clinical paradigms and integrating these strategies for depression and its management should be established. In this Research Topic we present selected studies that aim to highlight different augmentation strategies for patients with mood disorders, either with or without treatment resistance, with or without medical comorbidities or by improving residual symptoms such as daytime sleepiness and cognitive functions, all which could provide strategies to mitigate risk, personalize treatment and improve overall outcomes (see Table 1 for an overview of included studies).
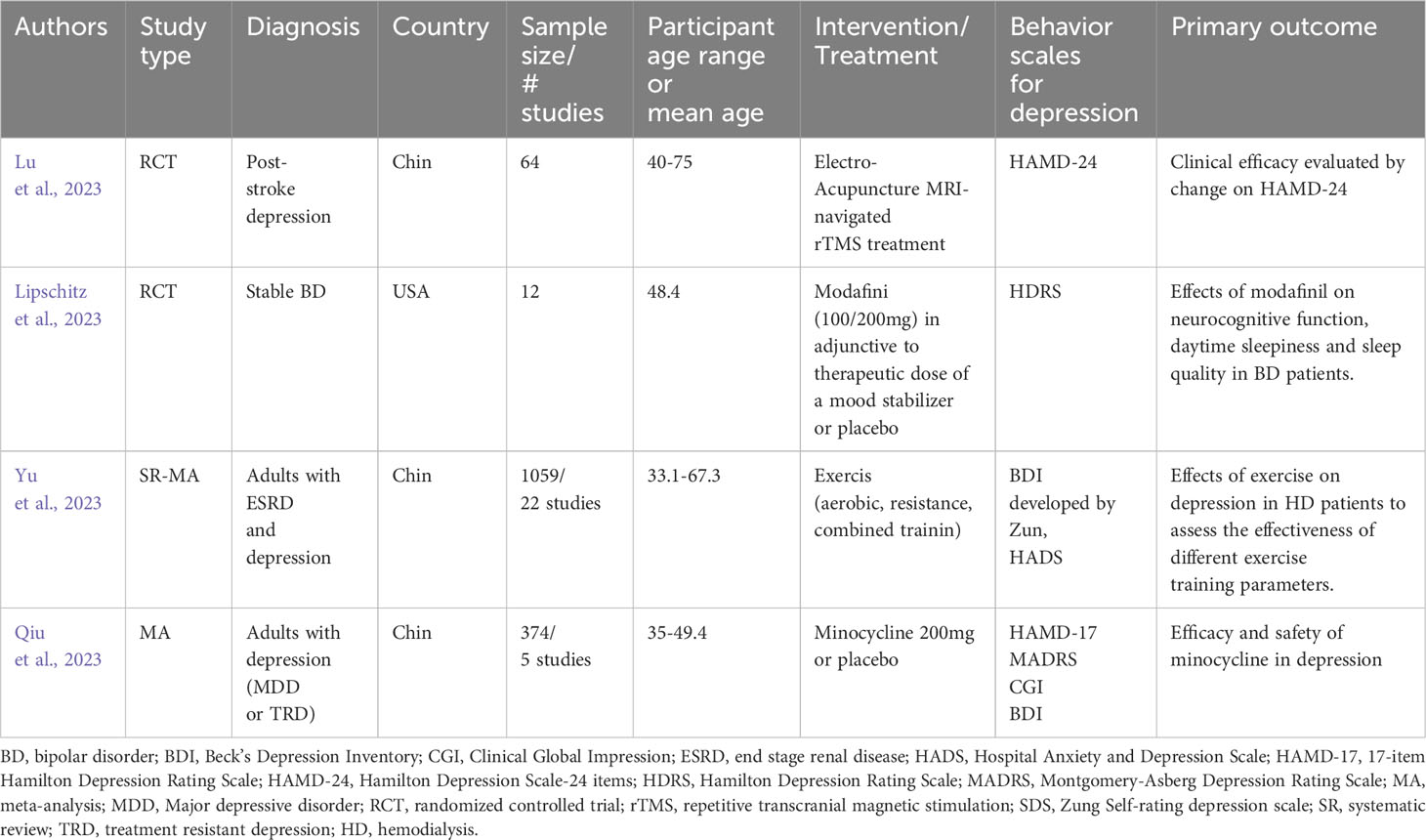
Table 1 Overview of edited primary studies.
Randomized controlled trials
Lu and colleagues presented a protocol study in which 64 patients (age 40-75 years) with post stroke depression will be randomized to electro-acupuncture/MRI-navigated rTMS or only MRI-navigated rTMS for 12 to 20 sessions (4 weeks) assessing primarily changes on the Hamilton Depression Scale-24 item scores from baseline to 4 weeks. Additionally, the authors will measure behavioral scales assessing quality of life as well as acceptability and a cost-effectiveness analysis. Exploring the effectiveness of electroacupuncture, which has shown promise in treating depression, in conjunction with rTMS, could present a novel therapeutic strategy for individuals in this population (Lu et al.).
Lipschitz et al. aimed to better understand the effects of a stimulant like agent, modafinil on neurocognitive and sleep disturbances in patients with bipolar disorder. The authors randomized 12 stable BD patients to modafinil (100-200mg/day) or placebo adjunctive to mood stabilizers for a duration of 8 weeks. The authors underscored a cognitive benefit and overall improvement in daytime sleepiness in the experimental group. However, the authors did not find a significant difference in terms of sleep quality. In terms of emergent side effects, there were no significant differences with placebo, but the authors highlighted symptoms such as palpitations, itching, fatigue and decreased energy as new emergent side effects in the experimental group. This pilot study further enriches the existing literature by highlighting the potential enhancement and the role of stimulant-like agents in improving cognition, episodic memory, and working memory performance, thereby offering promise in alleviating cognitive challenges among patients with mood disorders (8).
Systematic reviews
The first systematic review included in this series summarized evidence from 5 studies examining the utilization of minocycline—an antibiotic recognized for its anti-inflammatory, antioxidant, and neuroprotective attributes—in the treatment of psychiatric disorders. Qiu et al. suggested that minocycline in the included studies (minocycline, n=178; placebo, n=186) improved depressive symptoms and may augment response rates as well as it showed no statistically significant differences in all cause discontinuation rates when compared to placebo. This study provides more data of an affordable and readily available molecule which could potentially be effectively and safely utilized in TRD patients (9).
Considering the importance and the interplay between depressive symptoms and overall treatment outcomes in many medical conditions, Yu and colleagues conducted a systematic review in which they evaluated the effect of exercise on depressive symptoms in patients with comorbid end stage renal disease undergoing hemodialysis. By including 22 studies, they suggested that patients had better outcomes with intradialytic exercise and low depression following aerobic exercise; specially this was more notorious with activities with a duration greater than 1 hour. Moreover, those patients who engaged in exercise activities for more than 6 months had lower depression scores (Yu et al.).
The studies presented in this Research Topic provide an insight and overview of potential strategies for patients experiencing treatment resistance, residual symptoms with or without medical comorbidities. Moreover, the use of personalized interventions either by the use of these augmentation strategies, neuromodulation and lifestyle changes may provide an additional intervention to mitigate risk for relapse as well as to improve overall outcomes for individuals struggling with depression.
Author contributions
NN: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BJ: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GV: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Weinberger AH, Gbedemah M, Martinez AM, Nash D, Galea S, Goodwin RD. Trends in depression prevalence in the USA from 2005 to 2015: widening disparities in vulnerable groups. Psychol Med. (2018) 48:1308–15. doi: 10.1017/S0033291717002781
2. Vieta E, Berk M, Schulze TG, Carvalho AF, Suppes T, Calabrese JR, et al. Bipolar disorders. Nat Rev Dis Primers. (2018) 4:1–16. doi: 10.1038/nrdp.2018.8
3. Frye MA. Bipolar disorder—A focus on depression. New Engl J Med. (2011) 364:51–9. doi: 10.1056/NEJMcp1000402
4. Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clinics North America. (1996) 19:179–200. doi: 10.1016/S0193-953X(05)70283-5
5. Yatham LN, Kennedy SH, Parikh SV, Schaffer A, Bond DJ, Frey BN, et al. Canadian network for mood and anxiety treatments (Canmat) and international society for bipolar disorders (Isbd) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. (2018) 20:97–170. doi: 10.1111/bdi.12609
Keywords: bipolar disorder, depression, augmentation strategies, systematic reviews, randomized controlled trials
Citation: Nuñez NA, Joseph B and Vazquez GH (2024) Editorial: Old treatments new outcomes-augmentation treatments for depression. Front. Psychiatry 15:1384641. doi: 10.3389/fpsyt.2024.1384641
Received: 10 February 2024; Accepted: 15 February 2024;
Published: 29 February 2024.
Edited and Reviewed by:
Marcin Siwek, Jagiellonian University, PolandCopyright © 2024 Nuñez, Joseph and Vazquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gustavo H. Vazquez, Zy52YXpxdWV6QHF1ZWVuc3UuY2E=