
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 18 April 2024
Sec. Autism
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1381526
This article is part of the Research Topic Underlying Neurobiological, Genetic, and Behavioral Mechanisms in Schizophrenia and Autism Spectrum Disorder View all 10 articles
 Sofia Morais1,2
Sofia Morais1,2 Otília C. d’Almeida2,3,4Salomé Caldeira5Sofia Meneses5
Otília C. d’Almeida2,3,4Salomé Caldeira5Sofia Meneses5 Graça Areias5Vanessa Girão6
Graça Areias5Vanessa Girão6 Catarina Bettencourt6,7
Catarina Bettencourt6,7 Daniela Jardim Pereira2,3,8
Daniela Jardim Pereira2,3,8 António Macedo1,3,9
António Macedo1,3,9 Miguel Castelo-Branco2,3,4*
Miguel Castelo-Branco2,3,4*The profile of executive function (EF) in adults with Schizophrenia (SCZ) and autism spectrum disorder (ASD) remains unclear. This study aims to ascertain if distinct EF patterns can be identified between each clinical condition by comparing the neuropsychological profile of adults with SCZ and ASD, for whom the differential diagnosis is still highly challenging. Forty-five individuals (15 SCZ, 15 ASD, 15 controls) matched for age, sex, education level, and handedness underwent intelligence evaluation and neuropsychological testing for working memory, inhibition, planning and set-shifting, and verbal fluency subdomains. Principal component analysis (2D-PCA) using variables representing 4 domains was employed to identify patterns in neuropsychological profiles. The ASD group had lower scores on the Digits Forward subtest compared to the SCZ group (7.2 ± 2.1 vs. 9.3 ± 1.9, p = 0.003; Cohen’s d: 1.05). ASD also performed significantly worse on the Stroop Word Test compared to the control group (77.7± 17.9 vs. 98.0 ± 12.7, p = 0.009; Cohen’s d: 1.31). No significant differences were observed between ASD and SCZ on other EF measures. The larger contributors for the dimensions in 2D-PCA were the Digits Forward subtest and Stroop Word Test. Still, there was substantial overlap between the clinical groups. This study suggests a high degree of similarity of EF between SCZ and ASD. Through four EF measures, the discrimination of low and high-functioning EF groups spanning both diagnostic categories may help to identify the individuals who could better benefit from cognitive rehabilitation strategies.
• Schizophrenia (SCZ) and autism spectrum disorder (ASD) share functional features in executive function subdomains.
• ASD participants were differentially impaired on the Digits Forward subtest.
• ASD individuals showed slower response times on the Stroop Word-Color Test.
• PCA discriminates between low vs high-functioning groups, helping to stratify for rehabilitation.
The dichotomy of psychoses proposed by Kraepelin has dominated western psychiatry for over a century (1). More recently, in addition to this categorical perspective, in the field of psychoses and specifically in the context of neurodevelopmental disorders, a continuum perspective has also been favored, in which schizophrenia and autism spectrum disorders share some characteristics. There is growing evidence that focuses on the link between schizophrenia (SCZ) and autism spectrum disorder (ASD), with significant overlap in genetic studies (2), neuroimaging data (3), clinical signs and cognitive features (4). However, it is also important to investigate their differences, especially in the cognitive domain, to be able to design tailored cognitive remediation strategies across diagnostic groups.
ASD, typically diagnosed in childhood, is characterized by restricted or repetitive interests or behaviors and impaired social communication, and it tends to have a stable course. SCZ, typically diagnosed in adolescence or adulthood, is characterized by psychotic symptoms (e.g., hallucinations and delusions), but also with declining function. ASD without intellectual disability is often only diagnosed in early adulthood, and these patients can be hard to differentiate from SCZ due to the overlap of common presentations, especially when impaired in social interaction, inability to understand emotions, scarcity of psychotic symptoms, prominence of obsessive-compulsive symptoms, and overlap with SCZ usually diagnosed at this age.
Executive functions (EF) comprise cognitive abilities that enable and drive adaptive, goal-oriented behavior (5). These include: working memory, the ability to generate thought and think flexibly, and to update and monitor information mentally; inhibition, to inhibit what is irrelevant to current goals; set shifting, to modify attention and behavior in response to changing circumstances and demands; and, fluency, the ability to maximize the production of verbal or visual information in a specific time period while avoiding repeating responses (5). Besides, as in other neuropsychological tasks, there is a considerable overlap between the EF components measured within the individual subtests.
EF is known to be fundamental for learning, academic performance, mental health, adaptive and goal-directed behaviors (6). Although scarce, the existing literature suggests that while in SCZ there is a visible decline in EF after psychotic episodes and over time with increasing age (7), in ASD the EF difficulties tend to persist through adulthood (8).
Although an EF impairment was reported in each of these conditions, few studies compared EF in both SCZ and ASD (9–12). In the study of Eack (10), EF was assessed using the Wisconsin Card sorting Test and a cognitive battery (Measurement and Treatment to Improve Cognition in Schizophrenia – MATRICS) consisting of measures of processing speed, attention, working memory, verbal, and visual learning, and problem-solving. They reported that no significant differences were observed between SCZ and ASD in all cognitive domains, and the areas of larger impairment were similar across conditions. These included slowness in processing speed and inability to understand emotions. The main limitations of the study were the heterogeneity of the SCZ group, which included schizophrenia, schizoaffective disorders, and substance consumers, and the cognitive battery was not thoroughly evaluated in adults with ASD. Another study (9) assessed cognitive functions (verbal comprehension, perceptual organization, working memory, and processing speed) using the Wechsler adult intelligence scale-III (WAIS-III). SCZ patients scored significantly lower on processing speed than the ASD and the control group, but no other significant differences were found. However, few EF subdomains were assessed, as EF was only assessed by the subtests of WAIS-III, and there was no assessment of the psychosocial functioning in SCZ and ASD.
Marinopoulou and colleagues (11) studied EF subdomains using the Delis–Kaplan Executive Function System, after the applying WAIS-III. As in De Boer (9), SCZ and ASD scored similarly on EF assessment, except on processing speed, in which SCZ patients scored significantly lower than the ASD group. As a limitation, no neurotypical group was considered. Moreover, ASD group had higher Full-scale Intelligence Quotient (IQ) than SCZ, that was also a significant predictor of the variance of five EF measures in which the clinical groups showed statistically significant differences (11).
More recently, Yon-Hernández (12) found no differences between SCZ and ASD in inhibition performance. SCZ performed poorer than ASD and controls in Updating and Shifting, but their performance improved when there were no time constraints. The results of this study have a few limitations because age was not matched between groups. Overall, the heterogeneity of the neuropsychological tests applied, and the EF subdomains studied, with possible underrepresentation of some cognitive domains, can be strong contributors to the heterogeneity and consistency of results. Principal component analysis (PCA) is a method that allows to identify major cognitive functions by reducing the neuropsychological variables dimensionality to major functional axes. Here we asked if there are distinct executive dysfunction patterns within and between SCZ and ASD, to study their potential application in differential diagnosis and most importantly to help tailor rehabilitation approaches.
In the present study, we applied a battery of neuropsychological tests to evaluate four subdomains of EF: working memory, inhibition, planning and set-shifting, and verbal fluency, in adults with SCZ, ASD, and controls. Our main goal is to compare the functioning of these three groups, matched for age, sex, level of education and handedness. The principal component analysis will allow identifying patterns in neuropsychological profiles by providing additional data reduction while extracting the 2 main functional axes across these disorders.
This study followed a descriptive cross-sectional design with a non-probabilistic sampling approach for participants selection. We included outpatients with schizophrenia (SCZ) and autism spectrum disorder (ASD) from a major university hospital, besides controls, matched for age, sex, education level, and handedness. Intelligence was evaluated using Wechsler Adult Intelligence Scale III (WAIS-III). Inclusion criteria were: (1) DSM-5 criteria for SCZ or ASD (13); (2) age between 18–40; (3) capacity to give consent; (4) handedness through evaluation with the Edinburgh Handedness Inventory (14, 15); (5) clinical stability in the last 6 months prior to enrollment, for the clinical groups. General exclusion criteria were: (1) medical or neurological comorbidity (e.g., epilepsy, head trauma, intellectual disability defined for IQ<80); (2) substance abuse/dependence; (3) contra-indications to magnetic resonance imaging, needed for an MRI protocol outside the scope of this study.
All participants were assessed, by an expert psychologist blinded to the diagnosis, with WAIS-III, Portuguese version (16).
Patients’ clinical assessment included instruments such as the Positive and Negative Syndrome Scale (PANSS) (17) in SCZ group to measure symptoms of SCZ; Autism Diagnostic Observation Schedule Second Edition (ADOS-2) Module 4 (18) in ASD group to confirm the diagnosis, and the Personal and Social Performance Scale (PSP) (19, 20) addressing functioning.
In clinical groups, SCZ and ASD, pharmacological exposure was calculated through defined daily dose – DDD (21), and current antipsychotic exposure was calculated through chlorpromazine equivalents – CPZE (22, 23).
Control individuals were volunteers recruited from the community. A brief interview was performed to exclude personal or family history of psychiatric disorders, in addition to general exclusion criteria. All participants provided written informed consent. The study was approved by the local Ethics Committees of the Faculty of Medicine of the University of Coimbra (ref. CE-043/2020) and Coimbra Hospital and University Centre (ref. CHUC-109-18) in accordance with the Declaration of Helsinki.
A second expert psychologist, blinded to the performance on the IQ evaluation, assessed four subdomains of EF: working memory, inhibition, planning and set-shifting, verbal fluency. The same battery was administered to all participants in a fixed order.
Working memory was examined with the Portuguese versions of Digit Span task and Letter-number sequencing (16). In the Digit Span Forward subtest, the participant must repeat the sequence of numbers stated by the examiner in the same order. It includes eight increasing levels of difficulty from two up to nine-digit sequences. In the Digit Span Backward subtest, the participant is asked to repeat the same numbers but in reverse order, i.e., from last to first digit stated. It has seven increasing levels of difficulty from two up to eight-digit sequences. In both Forward and Backward tasks, each level includes two trials of the same length. Participants must correctly reproduce at least one trial at each level to proceed. The task is discontinued when both trials are recalled incorrectly. The accurate responses are calculated by scoring 1 point for each number sequence recalled correctly (forward and backward). In Letter-number sequencing, the examinee is presented with 7 triads of a sequence of numbers and letters. After hearing each sequence, the participant is instructed to first recall the numbers in ascending order, and later the letters in alphabetical order. The task is discontinued after the 3 sequences of each triad are recalled incorrectly. The accurate responses are calculated by scoring 1 point for each letter-number sequence recalled correctly.
Inhibition was examined with Stroop Color and Word Test, Portuguese version (24, 25). The test includes three conditions (Word, Color, and Word-Color). In each condition, examinees are presented with a printed sheet with five columns of 20 stimuli that they must read or name as quickly as possible within 45 seconds. In the first trial (Stroop Word), the participant must read the names of the colors that are all written in black on the card (“red”, “green”, or “blue”). In the second trial (Stroop Color), the participant is instructed to name the color in which sequences of the letter “X” are printed. In the third trial (Stroop Word-Color), the participant must name the color in which the words are written (e.g., the correct response to the word “green” written in red ink would be “red”). The score is the number of correct answers in 45 seconds.
Planning and set-shifting was assessed with the Wisconsin Card Sorting Test-64, Portuguese version (26, 27) and with the Trail Making Test – A and B, Portuguese version (28, 29). The Wisconsin Card Sorting Test-64 consists of a deck of 64 cards that need to be matched to one of four target cards through trial and error. The participant must match the cards one by one according to a criterion that can be color (red, yellow, blue, or green), shape, or number. After each response, the examiner signals whether the participant matched the card correctly or incorrectly. The matching criterion changes without a warning after 10 consecutive correct matches, i.e., after one successfully completed category. The total number of correct responses, errors, completed categories, and the perseverative responses are considered. Perseverative responses were defined as responses that matched the established perseverated-to principle, i.e., the previous sorting principle that the participant is persisting in. In Trail Making Test-A the participant is asked to connect continuously 25 numbers placed randomly on a page in ascending order as fast as possible. Trail Making Test-B includes connecting 13 numbers and 12 letters alternately and as quickly as possible without lifting the pencil. If an error is made, it is pointed out by the examiner for correction. The score used was the time, in seconds, required to complete each part.
Verbal fluency was assessed with Production of words under restricted conditions, which includes Phonemic Verbal fluency task P-R-M, Portuguese version (30, 31); and Semantic Verbal fluency task, Portuguese version (31, 32). The Phonemic Verbal fluency task entails saying as many words, as quickly as possible, beginning with P, R, and M in 60 seconds. Participants cannot use proper nouns or use a stem word with different endings. The Semantic Verbal fluency task entails saying as many words within 5 categories (animals, fruits, food, people names, and clothes), as quickly as possible, in 60 seconds, with no restrictions on the first letter or any other characteristics. We calculated the number of correct items generated in 60 seconds.
For all participants clinical and demographic data were collected: age, sex, education level, and handedness. Intelligence was evaluated with WAIS-III Portuguese version (16), by an expert psychologist blinded to the diagnose. The four subdomains of EF: working memory, inhibition, planning and set-shifting, verbal fluency, was evaluated by a second expert psychologist, blinded to the performance on the IQ evaluation. The same battery was administered to all participants in a fixed order.
In SCZ group the PANSS (17) was used to measure symptoms of SCZ, by an expert psychiatrist. In ASD group the ADOS-2 Module 4 (18) was used to confirm the diagnosis, by a third expert psychologist blinded to the performance on the IQ evaluation.
In clinical groups SCZ and ASD, PSP (19, 20) was used to address functioning, and pharmacological exposure was calculated, both by an expert psychiatrist.
For controls, medical history was obtained by an interview preceding assessment by an expert psychiatrist.
Demographic and clinical data analyses were performed with IBM SPSS Statistics 28.0 (IBM Corporation, New York, EUA). Normality of the data was tested using the Shapiro–Wilk test. When data were normally distributed, parametric tests were used to test differences between groups. If the assumption of normality was not met, non-parametric Kruskal–Wallis H or Mann–Whitney U tests were used to assess between-group differences. Fisher-Freeman-Halton’s exact test was used to assess between-group differences in categorical variables. Comparisons of neuropsychological tests metrics between groups were evaluated with ANCOVA using Performance-IQ as covariate. When appropriate, multiple comparison post-hoc tests were conducted with Bonferroni correction. Effect sizes of group comparisons were calculated according to Cohen’s d formula.
To profile the participants based on their EF neuropsychological test performance a two-dimensional unsupervised PCA was conducted using the ‘FactoMineR’ and ‘factoextra’ packages in the R Studio software (version 4.2.1). First, a data reduction procedure was applied by directly comparing each neuropsychological test metric between the three groups (ANOVA). Within each EF subdomain, the metric presenting the largest effect size (partial η2) was selected. Finally, four variables were included in the 2D-PCA: Digits Forward subtest, Stroop Word Test, Trail Making Test A (time), and Semantic Verbal fluency task. To ensure equal importance of each variable, data were standardized before the PCA. The amount of variation retained by each principal component was based on the eigenvalues.
Study design and data analysis were aligned with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) consensus (33).
Demographic and clinical data are summarized in Table 1. All patients with SCZ were on stable antipsychotic medication, predominantly atypical antipsychotics: single second-generation (n = 7), single third-generation (n = 3), a combination of two second-generation (n = 2), or a combination of second and third-generation (n = 3) antipsychotic medication. Within the ASD group, 11 patients were stable without any medication, 1 with a single second-generation antipsychotic medication, and 3 under a combination of antidepressant and second-generation antipsychotics. In the SCZ group, the mean disease duration was 5.6 ± 4.1 years.
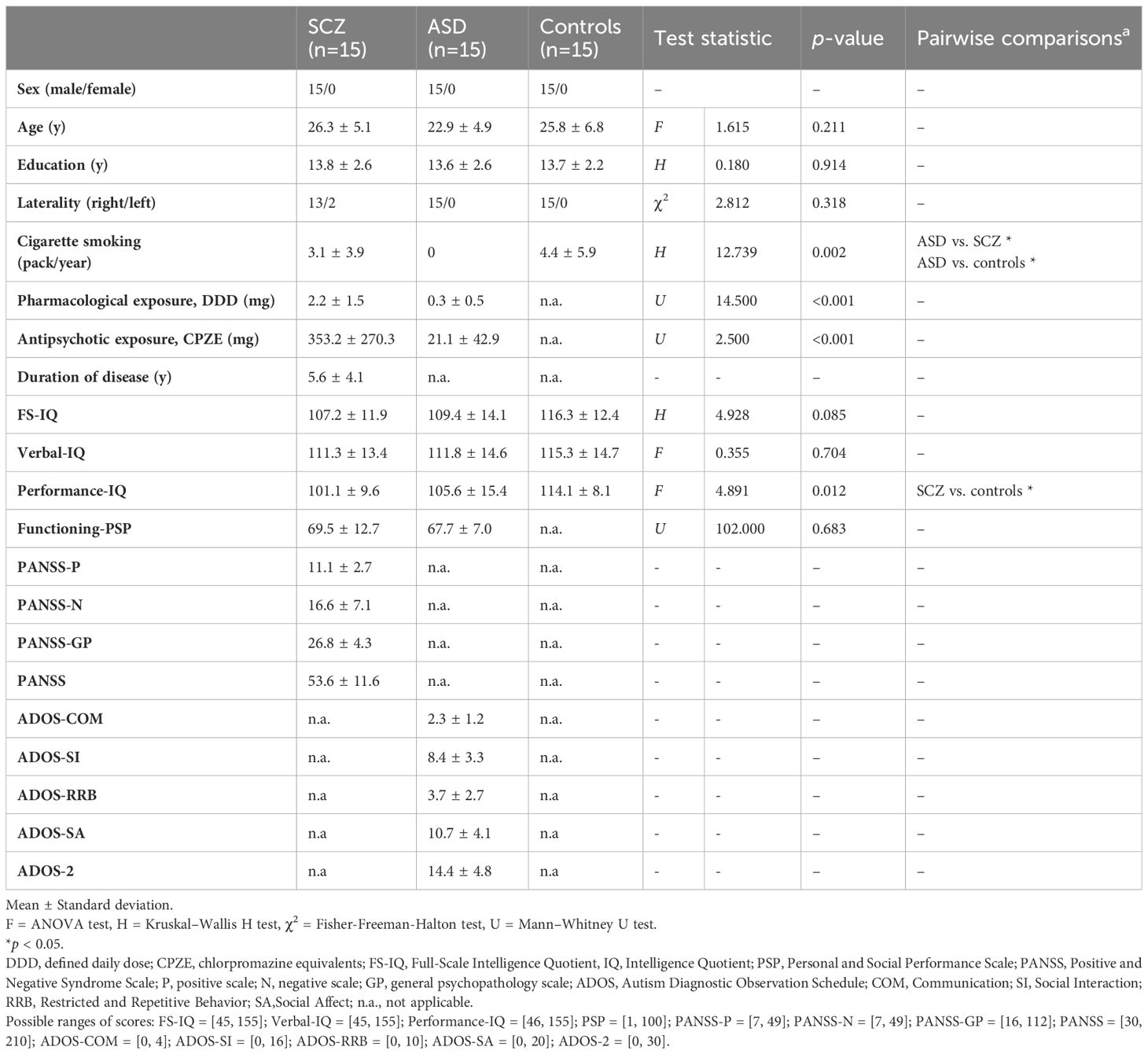
Table 1 Demographic and clinical data of study groups: schizophrenia (SCZ), autism spectrum disorder (ASD) and controls.
Clinical groups (SCZ and ASD) had no relevant demographic differences. The psychopharmacology and antipsychotics exposure, was greater in SCZ patients (p <0.001).
Regarding Full-scale Intelligence Quotient evaluation, there were no statistically significant differences between the three groups. However, there was a statistically significant difference in Performance-IQ, greater in controls compared to the SCZ group (p = 0.012).
As expected, three patients (n = 2, SCZ; n = 1, ASD) had discrepancies between Verbal-IQ and Performance-IQ, related to the discrepancy in verbal and performance skills that are often described in SCZ (34) and in ASD (35).
Individuals in the ASD group had no exposure to cigarettes. No statistically significant differences were found between SCZ and the control groups in smoking.
The statistics of group performance in executive functions measures and the test statistics corrected for Performance-IQ are summarized in Table 2.
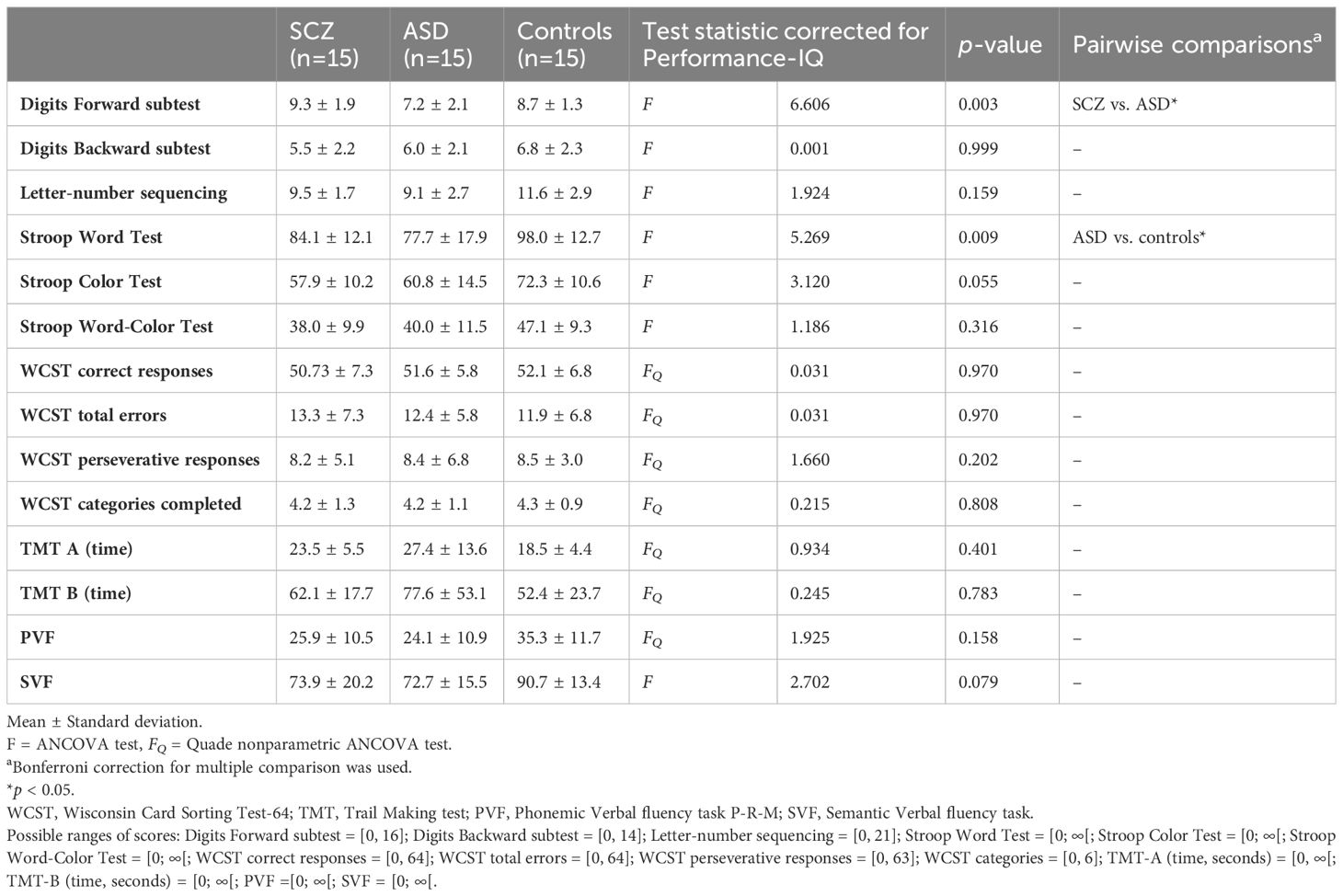
Table 2 Executive functions measures of study groups: schizophrenia (SCZ), autism spectrum disorder (ASD), and controls.
Working memory. ANCOVA analysis showed statistically significant differences in the performance of Digits Forward subtest, with worse working memory performance in ASD group than the SCZ group (7.2 ± 2.1 vs. 9.3 ± 1.9, p = 0.003; Cohen’s d: 1.05). On Digits Backward subtest and Letter-number sequencing, there were no significant differences between groups.
Inhibitory control. For this EF component, we found a significant group difference in the Stroop Word Test, and statistical analysis showed that the ASD group was slower than the control group (77.7± 17.9 vs. 98.0 ± 12.7, p = .009; Cohen’s d: 1.31).
Planning and Set-shifting ability. ANCOVA analysis showed that the three groups performed similarly in the Wisconsin Card Sorting Test, and in the Trail Making Test A and B.
Verbal fluency. Results did not indicate significant group differences in the performance of Phonemic Verbal fluency task P-R-M, and Semantic Verbal fluency task.
In PCA, two principal components were extracted from four initial variables, together explaining nearly 77.6% of the total variation. On average, the first and second components explained 55% ± 1.48 and 22.6% ± 0.95 of the variance. The variables that contributed most to these two components altogether were the Digits Forward subtest and the Stroop Word Test whereas the Semantic Verbal fluency task was the lowest contributor (Figure 1A). The PCA of the standardized metrics of the EF neuropsychological tests displayed a substantial overlap between the three groups (Figure 1B), especially between the two clinical groups, SCZ and ASD (Figure 1C).
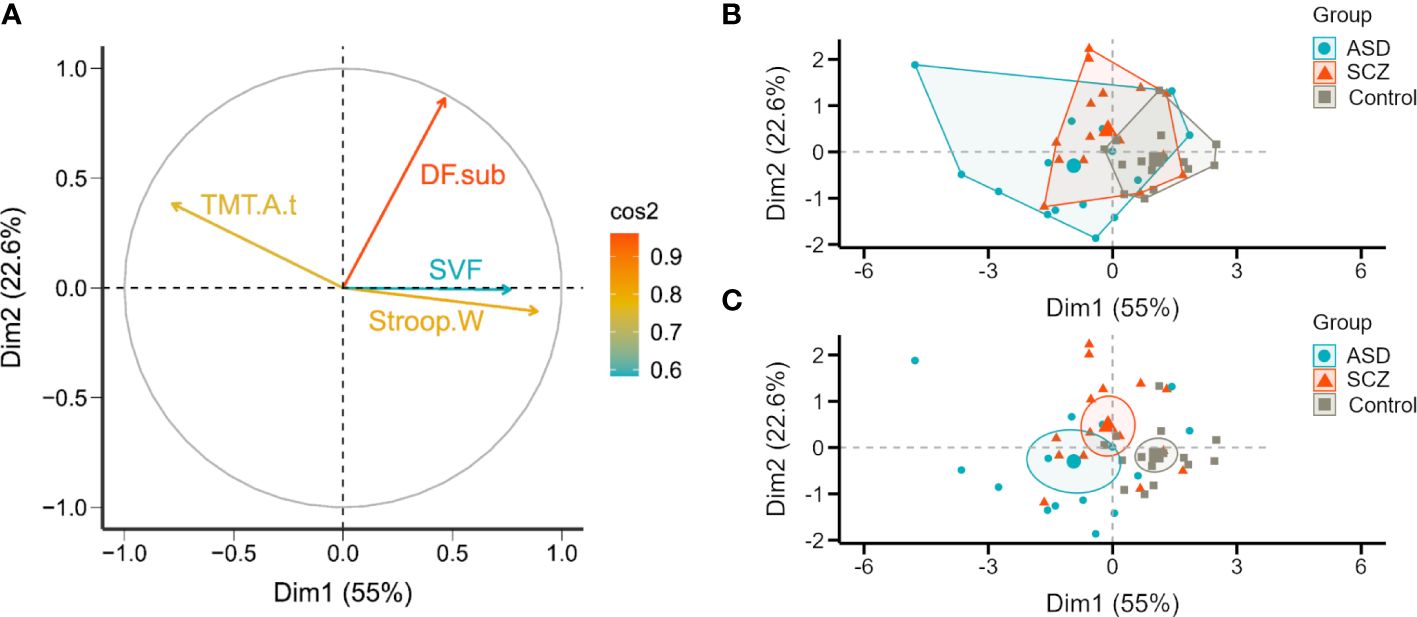
Figure 1 2D Principal component analysis (2D-PCA) of all 45 participants from the three cohorts, schizophrenia (SCZ), autism spectrum disorder (ASD) and controls based on normalized neuropsychological tests’ scores for executive function. (A) The variables under analysis are represented in a correlation circle over the space formed by the two principal components. The length of the vector reflects the strength of the correlation with each dimension and the color, the overall contribution of the variable (based on the cosine squared). (B, C) Participants are represented in the biplots and marked according to the group, SCZ (orange triangles), ASD (blue circles), and control (grey squares). The boundaries overlaid around group means (larger markers) represent in (B) a convex hull of the set of points of each group and in (C) the 95% confidence ellipses. DF.sub, Digits Forward subtest; Stroop.W, Stroop Word Test; TMT.A.t, Trail Making Test A (time); SVF, Semantic Verbal fluency task.
We compared four subdomains of EF: working memory, inhibition, planning and set-shifting, and verbal fluency, in adults with SCZ, ASD, and controls matched for age, sex, education level, and handedness. More specifically, we asked if distinct executive dysfunction patterns could be found between SCZ and ASD.
There is mounting interest in investigating the EF profile of adults with SCZ and ASD, to answer core questions about the unique aspects of both disorders. Noteworthy, SCZ and ASD are neurodevelopmental disorders, in which several studies have documented a high genetic, neuroimaging, and clinical overlap. Differential diagnosis is often challenging, namely because ASD without intellectual disability is often only diagnosed in early adulthood, which can be hard to differentiate from SCZ due to common clinical presentations, especially when manifestations include impairments in social interaction, inability to understand emotions, scarcity of psychotic symptoms or prominence of obsessive-compulsive symptoms. Also, SCZ is usually diagnosed at early stages of life.
Overall, we found no major differences in EF tests’ performance, particularly between the clinical groups, as assessed by a comprehensive battery of neuropsychological tests, where Performance-IQ was considered as covariate. It is important to note that distinct sampling strategies, with significant homogeneity in our case, may have particular impact in neuropsychological evaluation studies, which might influence the detection of EF differences. Nevertheless, in our cohort, the ASD group was significantly impaired on the Digits Forward subtest compared to the SCZ group, suggesting a particular deficit in working memory in ASD. The ASD group also showed slower response times on the Stroop Word-Color Test than the control group, reflecting an impairment in inhibitory control, and these results are in line with a recent meta-analysis (36).
Two separate (not allowing for direct comparison) meta-analyses of EF in SCZ (37) and in ASD (36) have shown impaired performance in EF in both conditions. In SCZ, the meta-analysis showed significantly impaired performance in all subtests of the EF neuropsychological battery (Behavioural Assessment of Dysexecutive Syndrome – BADS), with a very large effect size in complex forward planning, inhibition, cognitive flexibility, and novel problem solving (37). In ASD, the other meta-analysis showed significantly reduced performance in a set of neuropsychological tests (Behavior Rating Inventory Task – BRIEF, Luria hand game, Stroop Test, Card Sorting Task, and multiple others) in subdomains of EF: planning, working memory, inhibition, and flexibility (36). Also, other studies (38) found executive dysfunction which persisted across development in the ASD group, in comparison with neurotypical controls. However, no differential changes were found across EF subdomains (working memory, response inhibition, planning, fluency, mental flexibility, and concept formation), reflecting an overall and not fractionated impairment in EF performance. The still unclear scenario regarding differential dysfunction in EF subdomains in ASD is in accordance with previous research focusing on aberrant brain connectivity in predicting cognitive deficits and symptom severity in ASD (39) and is due to the scarcity of direct comparison studies.
We found no differences between SCZ and ASD groups regarding three EF subdomains: inhibitory control, planning and set-shifting ability, and verbal fluency suggesting a similar performance in these subdomains. The available literature addressing explicit comparisons shows heterogeneous findings. While some studies (9, 11) reported that patients with SCZ performed worse than ASD in processing speed or in updating and shifting (12); another study did not find any significant differences in EF subdomains between SCZ and ASD (10).
Importantly, as a potential explanation for existing discrepancies, in SCZ adults EF performance depends on moderator variables such as medication, symptoms level, duration of disease, age, sex, education, or general cognition (37). In our SCZ cohort, symptoms level was measured with PANSS, namely negative symptoms with PANSS-N (16.6 ± 7.1, range score 7 - 49) that can influence EF performance. Moreover, we focused on young, all male for sample homogeneity, with education level similar to other groups, while intelligence was evaluated and taken into account. Antipsychotic medication was at the minimum dose and measured with CPZE, although a meta-analysis on cognitive performance in drug-naïve SCZ reported that significant cognitive impairments are evident even at an early stage of SCZ in unmedicated patients (40).
In ASD it is harder to have an accurate clinical identification, due to the inherently difficult diagnostic approach, as a result of being part of a spectrum, which may lead to greater cognitive variability (9). Individuals with ASD continue to develop skills throughout their life, which may help to compensate for their impairments (41). Also, ASD individuals self-report more difficulties than SCZ individuals related to EF and adaptive behaviors in everyday life situations (42). Future research should focus more on combination types of assessment such as neuropsychological, and more ecologically valid evaluations of EF.
Two principal components were able to explain nearly 77.6% of the variance in the data. The larger contributors were Digits Forward subtest and Stroop Word Test, evaluating working memory and inhibitory control subdimensions, respectively. Semantic Verbal fluency task was the least important variable.
These dimensions are relevant as set-shifting, and inhibition are considered “higher-order” EF whereby an individual needs to rely on multiple executive capacities to successfully simulate and evaluate a sequence of events prior to their execution (43).
There are some limitations of this study to be considered. First, the relatively small-sized sample which was traded-off with the search for homogeneity. However, some possible confounders such as age, sex, laterality, and educational level were considered, increasing sample homogeneity. Second, we assessed and controlled current medication use, namely antipsychotics, but its possible effect on EF measures in SCZ group cannot be entirely ruled out. Third, we have not included females in our sample that may have different EF performances, because significant sex differences in EF, explained by different strategies employed, supported by different circuit and/or neurochemical mechanisms are utilized by males and females to solve the same cognitive problems (44). Fourth, we only analyzed EF performance, therefore, future studies should explore the relationship between EF performance and functioning using PSP. Our results cannot be generalized to non-verbal individuals with ASD and with comorbid intellectual disability, and it is not clear whether the same conclusions can be drawn for SCZ group with florid symptoms and treatment resistant SCZ.
To sum up, adults with SCZ and ASD matched for age, sex, education level, and handedness share executive dysfunction patterns, as assessed by neuropsychological testing, while dimensional analysis suggested differences in level of functioning that may help select patients for tailored cognitive interventions.
Future research should directly study the relationship between executive (dys)function and behavioral manifestations. Clinicians should be aware that individuals in this situation try to compensate in daily life executive dysfunction but may suffer its social consequences. The EF measures that mostly explained the variance in the sample were related to working memory and inhibition. This suggests the need for patient stratification across conditions for cognitive intervention.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the local Ethics Committees of the Faculty of Medicine of the University of Coimbra (ref. CE-043/2020) and Coimbra Hospital and University Centre (ref. CHUC-109-18) in accordance with the Declaration of Helsinki. The participants provided their written informed consent to participate in this study.
SMo: Conceptualization, Formal analysis, Investigation, Visualization, Data curation, Writing – original draft. OCd'A: Formal analysis, Investigation, Methodology, Writing – review & editing. SC: Investigation, Methodology, Visualization, Validation, Writing – review & editing. SMe: Investigation, Methodology, Validation, Writing – review & editing. GA: Investigation, Methodology, Validation, Writing – review & editing. VG: Investigation, Methodology, Validation, Writing – review & editing. CB: Investigation, Methodology, Validation, Writing – review & editing. DP: Investigation, Validation, Writing – review & editing. AM: Conceptualization, Supervision, Validation, Writing – review & editing. MC-B: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the BRAINTRAIN grant, a Collaborative Project supported by the European Commission, under the Health Cooperation Work Programme of the 7th Framework Programme [Grant Agreement 602186 (www.braintrainproject.eu); and the Fundação para Ciência e Tecnologia (FCT) – FCT/UIDB/4950, FCT/UIDP/4950, PTDC/PSI-GER/1326/2020 and DSAIPA/DS/0041/2020.
We would like to thank the participants for their involvement in this study. We are also very grateful to Margarida Marques for descriptive statistical analysis. Finally, we acknowledge the reviewers’ insightful comments and improvement suggestions, adding quality to this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1381526/full#supplementary-material
1. Rybakowski JK. 120th anniversary of the kraepelinian dichotomy of psychiatric disorders. Curr Psychiatry Rep. (2019) 21:65. doi: 10.1007/s11920-019-1048-6
2. Grove J, Ripke S, Als TD, Mattheisen M, Walters RK, Won H, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. (2019) 51:431–44. doi: 10.1038/s41588-019-0344-8
3. Du Y, Fu Z, Xing Y, Lin D, Pearlson G, Kochunov P, et al. Evidence of shared and distinct functional and structural brain signatures in schizophrenia and autism spectrum disorder. Commun Biol. (2021) 4:1073. doi: 10.1038/s42003-021-02592-2
4. Jutla A, Foss-Feig J, Veenstra-VanderWeele J. Autism spectrum disorder and schizophrenia: An updated conceptual review. Autism Res. (2022) 15:384–412. doi: 10.1002/aur.2659
5. Rabinovici GD, Stephens ML, Possin KL. Executive dysfunction. Contin (Minneap Minn). (2015) 21:646–59. doi: 10.1212/01.con.0000466658.05156.54
6. Hartung J, Engelhardt LE, Thibodeaux ML, Harden KP, Tucker-Drob EM. Developmental transformations in the structure of executive functions. J Exp Child Psychol. (2020) 189:104681. doi: 10.1016/j.jecp.2019.104681
7. Muralidharan A, Finch A, Bowie CR, Harvey PD. Older versus middle-aged adults with schizophrenia: Executive functioning and community outcomes. Schizophr Res. (2020) 216:547–9. doi: 10.1016/j.schres.2019.11.001
8. Di Sarro R, Di Santantonio A, Desideri L, Varrucciu N. Profiling planning skills and cognitive flexibility of adults with autism spectrum disorders: Preliminary results from an exploratory service-based study. Int J Dev Disabil. (2022) 68:651–7. doi: 10.1080/20473869.2020.1871311
9. de Boer M, Spek AA, Lobbestael J. Comparing cognitive functioning in schizophrenia and autism using WAIS-III. Res Autism Spectr Disord. (2014) 8:737–45. doi: 10.1016/j.rasd.2014.03.001
10. Eack SM, Bahorik AL, McKnight SA, Hogarty SS, Greenwald DP, Newhill CE, et al. Commonalities in social and non-social cognitive impairments in adults with autism spectrum disorder and schizophrenia. Schizophr Res. (2013) 148:24–8. doi: 10.1016/j.schres.2013.05.013
11. Marinopoulou M, Lugnegård T, Hallerbäck MU, Gillberg C, Billstedt E. Asperger syndrome and schizophrenia: A comparative neuropsychological study. J Autism Dev Disord. (2016) 46:2292–304. doi: 10.1007/s10803-016-2758-9
12. Yon-Hernández JA, Wojcik DZ, García-García L, Magán-Maganto M, Franco-Martín M, Canal-Bedia R. Neuropsychological profile of executive functions in autism spectrum disorder and schizophrenia spectrum disorders: a comparative group study in adults. Eur Arch Psychiatry Clin Neurosci. (2023) 273:719–30. doi: 10.1007/s00406-022-01466-w
13. American Psychiatric Association. Manual de diagnóstico e estatística das Perturbações Mentais, (5a ed.). Lisboa: Climepsi Editores (2014).
14. Espírito-Santo H, Pires CF, Garcia IQ, Daniel F, Silva AG, Fazio RL. Preliminary validation of the Portuguese Edinburgh Handedness Inventory in an adult sample. Appl Neuropsychol Adult. (2017) 24:275–87. doi: 10.1080/23279095.2017.1290636
15. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. (1971) 9:97–113. doi: 10.1016/0028-3932(71)90067-4
16. Wechsler D. Escala de Inteligência de Wechsler para Adultos (3a ed) versão Portuguesa de C. Ferreira, M. Machado, & A. M. Rocha). Lisboa: Cegoc. (2008).
17. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
18. Lord C, Rutter M, DiLavore PC, Risi S, Gotham K, Bishop S. Autism diagnostic observation schedule-2nd edition (ADOS-2). Torrance, CA: Western Psychological Services (2012).
19. Brissos S, Palhavã F, Marques JG, Mexia S, Carmo AL, Carvalho M, et al. The Portuguese version of the Personal and Social Performance Scale (PSP): reliability, validity, and relationship with cognitive measures in hospitalized and community schizophrenia patients. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1077–86. doi: 10.1007/s00127-011-0412-6
20. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. (2000) 101:323–9. doi: 10.1034/j.1600-0447.2000.101004323.x
21. WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2023. Oslo, Norway: WHO Collaborating Centre for Drug Statistics Methodology (2022).
22. Atkins M, Burgess A, Bottomley C, Riccio M. Chlorpromazine equivalents: a consensus of opinion for both clinical and research applications. Psychiatr Bull. (1997) 21:224–6. doi: 10.1192/pb.21.4.224
23. Patel MX, Arista IA, Taylor M, Barnes TR. How to compare doses of different antipsychotics: a systematic review of methods. Schizophr Res. (2013) 149:141–8. doi: 10.1016/j.schres.2013.06.030
25. Golden CJ. Stroop Color and Word Test: Manual for Clinical and Experimental Uses. Stoetling, Chicago (1978).
26. Faustino B, Oliveira J, Lopes P. Normative scores of the Wisconsin Card Sorting Test in a sample of the adult Portuguese population. Appl Neuropsychol Adult. (2022) 29:767–74. doi: 10.1080/23279095.2020.1810040
27. Kongs SK, Thompson LL, Iverson GL, Heaton RK. Wisconsin Card Sorting Test-64 cards version professional manual. Odessa, FL: Psychological Assessment Resources (2000).
28. Cavaco S, Gonçalves A, Pinto C, Almeida E, Gomes F, Moreira I, et al. Trail Making Test: regression-based norms for the Portuguese population. Arch Clin Neuropsychol. (2013) 28:189–98. doi: 10.1093/arclin/acs115
29. Reitan RM. Validity of the trail making test as an indicator of organic brain damage. Percept Mot Skills. (1958) 8:271–6. doi: 10.2466/pms.1958.8.3.271
30. Borkowski JG, Benton AL, Spreen O. Word fluency and brain damage. Neuropsychologia. (1967) 5:135–40. doi: 10.1016/0028-3932(67)90015-2
31. Cavaco S, Gonçalves A, Pinto C, Almeida E, Gomes F, Moreira I, et al. Semantic fluency and phonemic fluency: regression-based norms for the Portuguese population. Arch Clin Neuropsychol. (2013) 28:262–71. doi: 10.1093/arclin/act001
32. Robert P, Migneco V, Marmod D, Chaix I, Thauby S, Benoit M, et al. Verbal fluency in schizophrenia: the role of semantic clustering in category instance generation. Eur Psychiatry J Assoc Eur Psychiatr. (1997) 12:124–9. doi: 10.1016/s0924-9338(97)80200-3
33. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med. (2007) 147:W163–94. doi: 10.7326/0003-4819-147-8-200710160-00010-w1
34. Sørensen HJ, Mortensen EL, Schiffman J, Ekstrøm M, Denenney D, Mednick SA. Premorbid IQ and adult schizophrenia spectrum disorder: verbal Performance subtests. Psychiatry Res. (2010) 178:23–6. doi: 10.1016/j.psychres.2010.03.016
35. Kanai C, Tani M, Hashimoto R, Yamada T. Cognitive profiles of adults with Asperger’s disorder, high-functioning autism, and pervasive developmental disorder not otherwise specified based on the WAIS-III. Res Autism Spectr Disord. (2012) 6:58–64. doi: 10.1016/j.rasd.2011.09.004
36. Hemmers J, Baethge C, Vogeley K, Falter-Wagner CM. Are executive dysfunctions relevant for the autism-specific cognitive profile? Front Psychiatry. (2022) 13:886588. doi: 10.3389/fpsyt.2022.886588
37. Thai ML, Andreassen AK, Bliksted V. A meta-analysis of executive dysfunction in patients with schizophrenia: Different degree of impairment in the ecological subdomains of the Behavioural Assessment of the Dysexecutive Syndrome. Psychiatry Res. (2019) 272:230–6. doi: 10.1016/j.psychres.2018.12.088
38. Demetriou EA, Lampit A, Quintana DS, Naismith SL, Song YJC, Pye JE, et al. Autism spectrum disorders: A meta-analysis of executive function. Mol Psychiatry. (2018) 23:1198–204. doi: 10.1038/mp.2017.75
39. Aoki Y, Abe O, Nippashi Y, Yamasue H. Comparison of white matter integrity between autism spectrum disorder subjects and typically developing individuals: a meta-analysis of diffusion tensor imaging tractography studies. Mol Autism. (2013) 4:25. doi: 10.1186/2040-2392-4-25
40. Fatouros-Bergman H, Cervenka S, Flyckt L, Edman G, Farde L. Meta-analysis of cognitive performance in drug-naïve patients with schizophrenia. Schizophr Res. (2014) 158:156–62. doi: 10.1016/j.schres.2014.06.034
41. Happé F, Charlton RA. Aging in autism spectrum disorders: a mini-review. Gerontology. (2012) 58:70–8. doi: 10.1159/000329720
42. Yon-Hernández JA, Wojcik DZ, García-García L, Franco-Martín MA, Canal-Bedia R. Differences in daily life executive functioning between people with autism and people with schizophrenia. J Autism Dev Disord. (2023) 53:2773–85. doi: 10.1007/s10803-022-05547-6
43. Diamond A. Executive functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
Keywords: executive function, schizophrenia, autism spectrum disorder, neuropsychology, stroop
Citation: Morais S, d’Almeida OC, Caldeira S, Meneses S, Areias G, Girão V, Bettencourt C, Pereira DJ, Macedo A and Castelo-Branco M (2024) Executive function in schizophrenia and autism in adults shares common components separating high and low performance groups. Front. Psychiatry 15:1381526. doi: 10.3389/fpsyt.2024.1381526
Received: 03 February 2024; Accepted: 27 March 2024;
Published: 18 April 2024.
Edited by:
Rafael Penadés, Hospital Clinic of Barcelona, SpainReviewed by:
Stefano Barlati, University of Brescia, ItalyCopyright © 2024 Morais, d’Almeida, Caldeira, Meneses, Areias, Girão, Bettencourt, Pereira, Macedo and Castelo-Branco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Castelo-Branco, bWNicmFuY29AZm1lZC51Yy5wdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.