
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 18 April 2024
Sec. Public Mental Health
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1380401
This article is part of the Research Topic Medical Emergencies in Psychiatry View all 6 articles
 Claudia Aymerich1,2,3,4*
Claudia Aymerich1,2,3,4* Borja Pedruzo1,2,3,4
Borja Pedruzo1,2,3,4 Gonzalo Salazar de Pablo5,6,7,8Nora Olazabal1,2,4
Gonzalo Salazar de Pablo5,6,7,8Nora Olazabal1,2,4 Ana Catalan1,2,3,4,6,9†Miguel Ángel González-Torres1,2,3,4†
Ana Catalan1,2,3,4,6,9†Miguel Ángel González-Torres1,2,3,4†Introduction: The COVID-19 pandemic has significantly impacted mental health globally, leading to a deterioration in the overall mental health of the population and changes across all healthcare levels, including emergency departments (ED). However, the evolution of the quantity and nature of psychiatric ED visits in the post-pandemic period remains uncertain.
Aims: To examine changes in the number and nature of psychiatric emergencies at a general hospital before, during, and after the COVID-19 pandemic.
Materials and methods: Psychiatric ED visits from a tertiary hospital in the Basque Country (Spain) between January 2019 and November 2023 were investigated. Electronical health registers detailing the number and nature of psychiatric care consultations were analyzed for the study timeframe. Three periods were then compared: pre-pandemic (from January 2019 to February 2020), pandemic (from March 2020 to January 2022), and post-pandemic (from February 2022 onwards).
Results: 16,969 psychiatric ED visits were recorded for the study period. The number of psychiatric ED visits remained stable from pre-pandemic (269.93 visits/month) to pandemic (264.48 visits/month) periods but experienced a significant rise during the post-pandemic period (330.00 visits/month; t=-6.42; p<0.001), which was not reflected in medical and traumatological visits. The proportion of visits for anxiety (Z=-2.97; p=0.003), suicidal ideation (Z=-5.48; p<0.001), and administrative and social consultations (Z=-5.69; p<0.001) increased over the course of the pandemic. In contrast, visits for schizophrenia and other psychotic disorders (Z=4.85; p<0.001), as well as unspecified behavioral alterations (Z=2.51; p=0.012), significantly decreased.
Conclusion: The COVID-19 pandemic and its aftermath have altered the patterns of urgent psychiatric care, characterized by a sharp increase of average monthly number of consultations and a shift in their nature. Future efforts should focus on characterizing this surge in demand and enhancing both emergency services and outpatient settings.
The global pandemic caused by the appearance of SARS CoV-2 in early 2020 (1) presented a challenge for the health systems worldwide, pushing most governments towards adopting confinements and other restrictive measures to preserve public health. The pandemic and its consequences not only strained the physical health of the population but also exacerbated mental health issues (2, 3). This was fueled by a context of uncertainty and cumulative macroeconomic losses worldwide (4, 5), along with social isolation and its secondary impact on mental health and physical inactivity during this period (6). Over the months following the onset of the spread of COVID-19, an increased incidence of mental health symptoms were noted among both clinical (7) and general (8, 9) population. A substantial increase in the burden of major depressive disorder and anxiety disorders was noted in 2020, with an increase of their prevalence of around 0.4% worldwide for both disorders (10) and a prevalence of suicidal ideation among general population of 12.1% (11), substantially higher than in studies prior to the pandemic.
Furthermore, the pandemic entailed the shutdown of schools, public entities, and even medical services to minimize the risk of exposure, slow the spread of the virus, and concentrate most available resources on the treatment of the COVID-19 disease. This, in turn, resulted in reduced or difficulted access to mental health treatment delaying or avoiding medical care for many people (12–14). In this context, emergency services became the primary and, for many patients, the only point of contact with mental health services, with a potential impact on help-seeking behavior. Therefore, a shift in the number and nature of emergency department (ED) visits was also expected.
Indeed, a decline in patient visits of up to 60% occurring after the onset on the pandemic was noted in general emergencies, both for adults and pediatric patients (15, 16). As for the number of psychiatric ED visits, an initial reduction was noted worldwide. In Western Australia, a 43% decrease in the number of total psychiatric ED visits was recorded over the last weeks of April 2020 compared to previous years (17). In Europe, a Portuguese hospital reported a 52% overall decrease during the same period, mostly at the expense of female patients presenting with mood disorders (18), while in Ireland a 21% decrease was noted between March and May (19), due to the lockdowns and fear of infection. On the other hand, a later increase in the number of ED visits was also expected once the most severe restrictive measures were lifted, due to the general worsening of population’s mental health and the overwhelm of outpatient services. There is evidence that the pandemic differentially affected not only diverse demographic groups, but also individuals with certain specific mental disorders compared to others (20). For instance, a large increase in the number of hospitalizations and care seeking behavior was found during the pandemic in patients with eating disorders (21) or personality disorders (22), among others. On the other hand, patients with obsessive-compulsive disorder did not show significant symptom deterioration during the pandemic (23). Therefore, changes in both the quantity and the reason for psychiatric ED visits was expected.
However, there is a shortage of research describing the evolution of psychiatric ED visits before, during and after the pandemic, not only in terms of numbers but also in the nature of consultations. To address this gap, we analyzed the electronic ED medical records from a tertiary hospital.
The primary objectives of this study were to (i) assess the evolution and presence of statistically significant variations in the monthly average number of visits to the psychiatric ED before, during, and after the COVID-19 pandemic; (ii) compare this evolution with that of medical and traumatological emergencies in the same periods; and (iii) assess the presence of changes in the nature of the psychiatric consultations before and after the pandemic. We hypothesized that ED visits for psychiatric care would decrease during the pandemic period, and then progressively increase in the following months and years to reach a higher number of ED visits compared to that prior to the COVID-19 pandemic. We also anticipated that this secondary increase in urgent care would be proportionally higher than that experienced by urgent care for other causes (medical and/or traumatological) in the same period.
This was a retrospective, observational study conducted at the Basurto University Hospital. This is a tertiary hospital located in the Basque Country in northern Spain, serving a population of 380,000 people. The Basurto University Hospital Research Ethics Committee gave ethical approval for the study (N.77.23 CEIHU). The present study followed the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines for cohort studies (Table S1) (24).
We used an electronic health register [EHR; Osabide Global 2.0 (25)] to retrospectively identify all visits to the Basurto University Hospital’s Emergency Department over the course of four years (from 1st of January 2019 to 30th November 2023). In this register, ED visits are divided in several groups (medical, psychiatric, traumatological) by the ED staff at the time of their admission, according to the main reason of consultation.
The number of monthly visits and the main diagnosis resulting from each visit were obtained through the EHR. In this database, all patients are assigned a relevant ICD-10 (26) code by ED doctors at the time of their discharge. The data were de-identified to protect privacy and confidentiality of patients. To simplify the analysis, the primary diagnoses were classified into the following categories: neurodevelopmental disorders, schizophrenia spectrum and other psychotic disorders, depressive disorders, bipolar disorders, anxiety, obsessive-compulsive and related disorders, trauma- and stressor-related disorders, dissociative disorders, somatic symptom and related disorders, feeding and eating disorders, sleep-wake disorders, substance-related and addictive disorders, personality disorders, administrative and social consultations, behavioral alterations not otherwise specified, medical and traumatological consultations (where patients coming for a mainly medical or traumatological reason, but required specific advise by a psychiatry specialist for any reason), other consultations, and suicide and self-harm related consultations. This last category was then divided into three subgroups: suicide ideation/suicide risk, non-suicidal self-injuries, and suicide attempts. A detailed list of all the codes included under each category is available in eMethods S1. Drugs were divided into several subgroups as well: alcohol, stimulants, benzodiazepines and other hypnosedatives, opioids, cannabinoids, and unspecified/multiple substances (eMethods S2).
Three periods were defined for the study timeframe: pre-pandemic (from January 1st, 2019, to February 28th, 2020, marking the detection of the first COVID-19 case in Northern Spain), pandemic (from March 1st, 2020, to January 31st, 2022, when all pandemic-restrictions were lifted in Spain, including mandatory mask-wearing), and post-pandemic (from February 1st, 2022, to November 30th, 2023).
Monthly averages of psychiatric ED visits (in order to account for stational variations in the ED affluence) for each study period and category were calculated. After verifying the normality of the samples using Shapiro-Wilk test, a two-sample t-test with Bonferroni correction was applied to assess whether there were any significant differences between each pair of periods. The same procedure was followed for ED visits for medical care (as opposed to psychiatric care) for each study period.
Then, the nature of the psychiatric consultations and its variations over the study periods were assessed. First, the percentage of visits per diagnostic category was calculated for each study period, and pie charts were created to depict the results. Then, we evaluated the presence of statistically significant differences in the percentage of consultations per diagnostic category between the pre-pandemic and post-pandemic periods. As percentages were used, Z-Test for Proportions was used for those categories including more than 30 consultations per study period (27). The same procedure was followed to assess the presence of statistically significant differences among diagnostic subgroups.
R software, version 1.4.1106 (28) was used for all analyses. The significance level was set at p <0.05, two-sided.
Throughout the study period, the hospital’s ED provided care for 16,969 individuals seeking psychiatric consultations and 450,105 individuals seeking medical or traumatological care. The number of monthly visit counts across the study period is available in Table S2 and Table S3.
During the pre-pandemic period (from January 2019 to February 2020), 269.93 psychiatric visits/month were registered in the ED. In April 2020, shortly after the onset of the pandemic, 350 visits were registered, but over the following months the visits/month went down to the previous figures, averaging at 264.48 visits/month for the pandemic period. However, in the post-pandemic period, the number of consultations increased significantly, reaching 330.00 average visits/month. The pre-pandemic and pandemic periods did not significantly differ in average monthly visits (t=0.53; p=0.60). However, during the post-pandemic period a significantly higher number of monthly visits were recorded, compared to both the pre-pandemic (t=-7.29; p<0.001) and pandemic (t=-6.42; p<0.001) periods.
In contrast, medical and traumatological emergency visits displayed a distinct pattern, exhibiting a clinically and statistically significant decrease from the pre-pandemic period to the pandemic period (from 8155.71 visits/month to 6777.48 visits/month; t=4.92; p<0.001). In the post-pandemic period, the number of average monthly visits rose back to numbers similar to the pre-pandemic period (8183.77 visits/month). There were no statistically significant differences between the pre-pandemic and post-pandemic periods ED affluence (t=-0.20; p=0.84).
In Figure 1, the evolution of the average monthly visits for psychiatric and medical/traumatological ED is detailed.
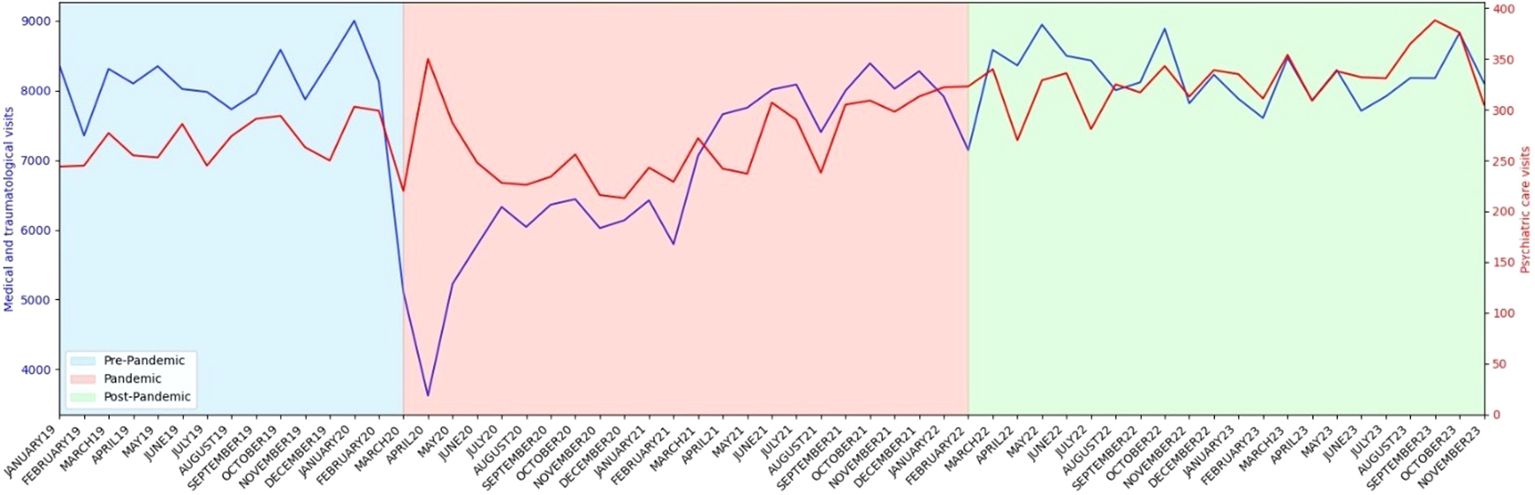
Figure 1 Absolute number of psychiatric care (in red) and medical and traumatological care (in blue) ED visits over the course of the study period.
In the pre-pandemic period, the main reason for psychiatric ED visits were anxiety-related consultations (30.2%), followed by schizophrenia spectrum and other psychotic disorders (14.0%), substance-related and addictive disorders (9.7%), behavior alterations not otherwise specified in the discharge report (9.3%), and suicide and self-harm related consultations (8.1%). At that time, administrative and social consultations only represented 5.2% of the total.
During the post-pandemic period, however, some statistically significant changes in the characteristics of psychiatric ED visits were noted. Although the absolute number of visits for almost all the diagnostic categories grew (Table 1), anxiety-related consultations rose to 33.0% of the total (Z=-2.97; p=0.003). Suicide and self-harm related consultations also experienced a notable growth (10.3%; Z=-3.83; p<0.001), along with administrative and social consultations (8.1%; Z=-5.69; p<0.001). On the other hand, a statistically significant reduction was detected in the percentages of consultations for schizophrenia spectrum and other psychotic disorders (10.9%; Z=4.85; p<0.001), trauma- and stressor-related disorders (from 4.8% to 4.0%; Z=1.99; p=0.047), behavior alterations not otherwise specified (7.9%; Z=2.51; p=0.012), and liaison psychiatry consultations in patients with a primary medical and/or traumatological diagnosis (from 3.94% to 2.95%; Z=2.76; p=0.006). The percentage of visits for depressive disorders and bipolar affective disorders, sleep-wake disorders, substance-related and addictive disorders, and personality disorders, did not show significant changes between the two periods (Figure 2, Table 2).
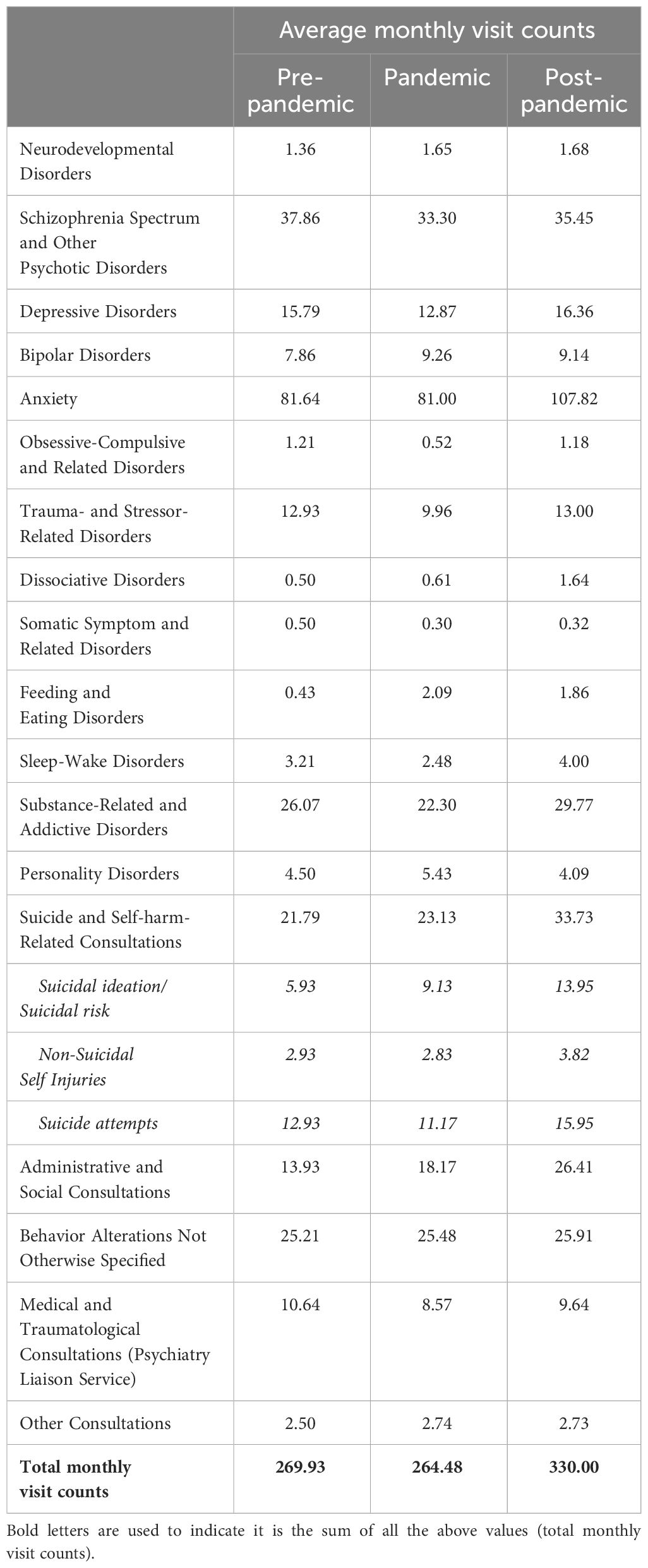
Table 1 Average monthly visit counts by diagnostic category for psychiatric care patients across different study periods.
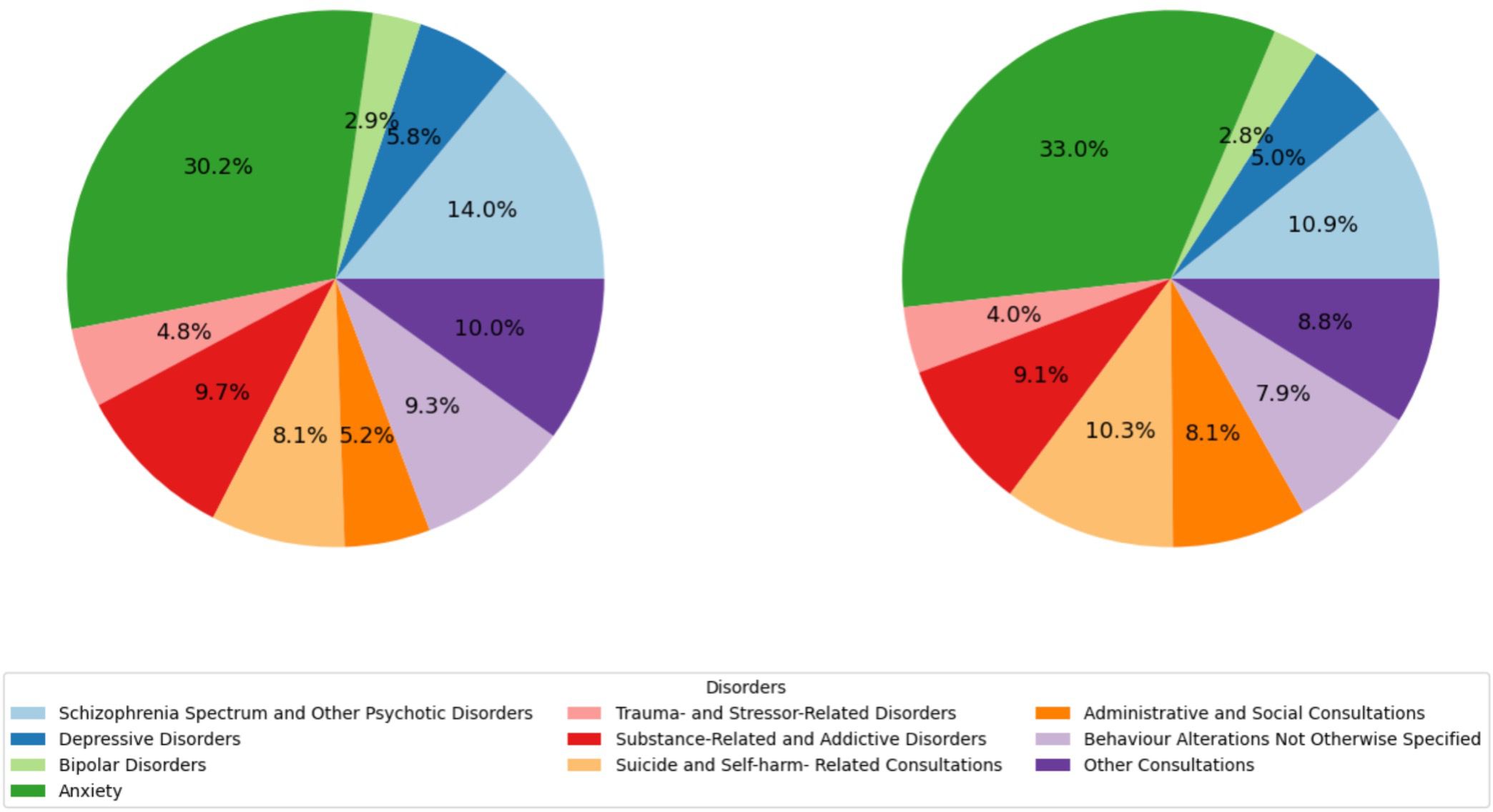
Figure 2 Reason for consultation of visits to the ED for psychiatric care in the pre-pandemic period (left) and the post-pandemic period (right).
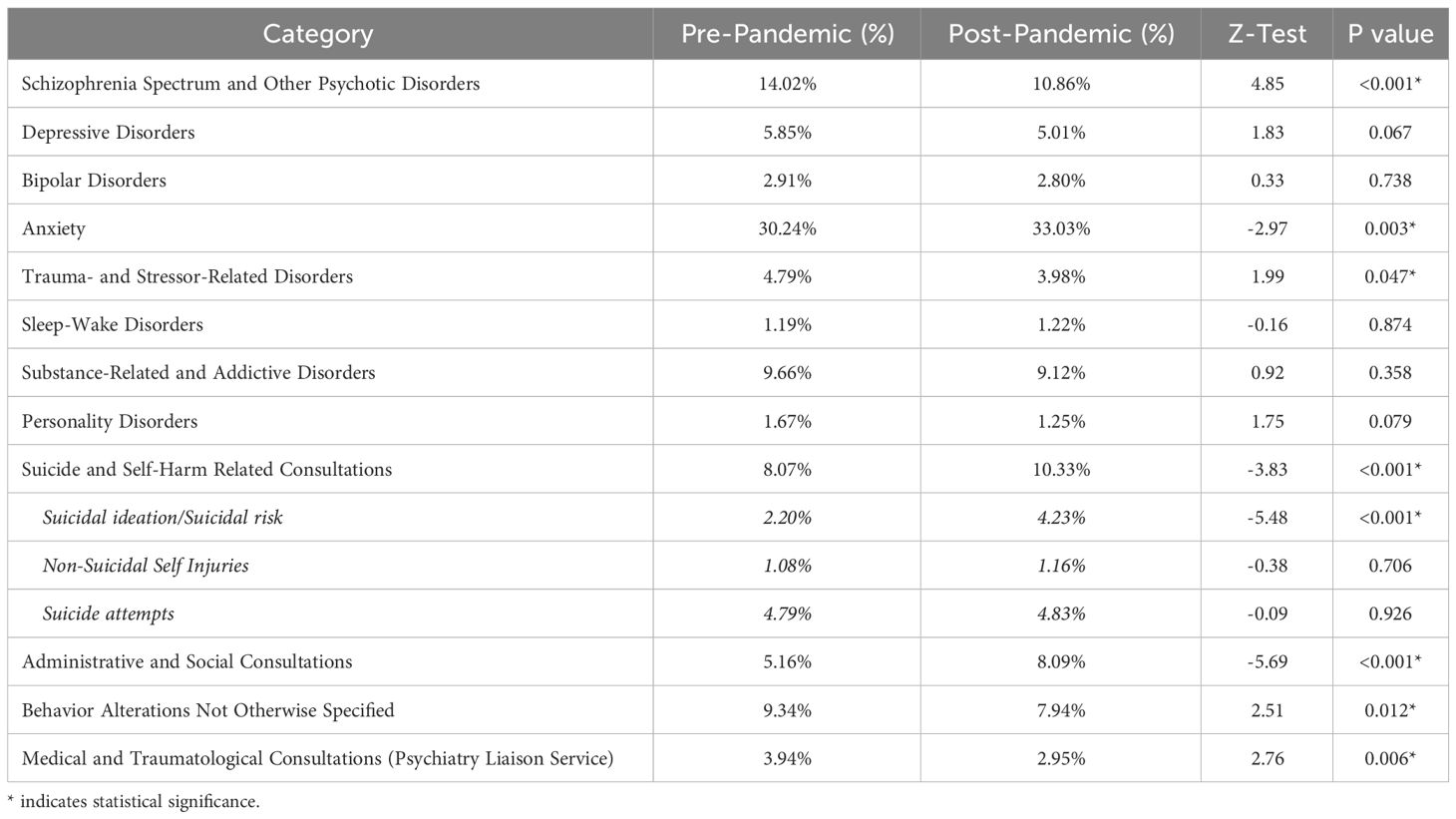
Table 2 Consultation reason distribution in psychiatric emergency department visits pre-pandemic period (left) vs. post-pandemic period (right).
Subgroup analysis also revealed important findings. When suicide and self-harm related consultations were divided into three subgroups, no statistically significant changes were appreciated in the percentage of consultations for non-suicidal self-injuries (from 1.08% to 1.16%; Z=-0.38; p=0.706) nor suicide attempts (from 4.79% to 4.83%; Z=-0.09; p=0.926). However, visits for suicidal ideation or suicidal risk significantly increased from 2.20% to 4.23% (Z=-5.48; p<0.001*), which suggests that the relative increase of the whole category is at the expense of this subgroup of visits.
On the other hand, no significant changes were noted between the two periods in terms of the substance that caused the substance-related and addictive disorders consultations, with alcohol representing well over 50% of those visits for both periods (Table S3).
To the best of the authors’ knowledge, this is the first study to comprehensively investigate the evolution in the number and nature of psychiatric emergencies at a general hospital before, during, and after the coronavirus pandemic.
Our findings show that the frequency of psychiatric emergencies in the ED remained consistent during the pandemic, not deviating significantly from the affluency observed in the previous year. This finding stands in contrast to other research, which has reported both and increase (29) and decrease (30–32) in such emergencies. The variance seen in these studies could be attributed to differences in the pandemic’s impact across various countries and in healthcare management practices (33, 34). For instance, previous studies in this area report a differential impact of the pandemic on primary care utilization for mental disorders across European countries, highly correlating with containment strategies used in each of them (35). Furthermore, it’s worth noting that most studies focused solely on the year 2020, not accounting for the continued pandemic-related restrictions like lockdowns, social distancing, and the reduction in outpatient medical services that persisted beyond this year.
However, in the period following the lifting of SARS-COV-2 related restrictions (post-pandemic period in our study), our research detected a notable rise in the number of psychiatric emergencies, that has persisted without any indication of diminishing. This surge was not mirrored in the total number of ED consultations for medical care, which decreased during 2020 and subsequently reverted to pre-pandemic figures.
There are several possible explanations for this increase in psychiatric ED visits after the initial waves of the pandemic. There is consistent evidence indicating changes in the levels of psychological distress in the population during the pandemic, characterized by cyclical periods of deterioration (often coinciding with new COVID-19 waves and the implementation of new restrictive measures) followed by recovery. However, data suggest that this recovery did not reach pre-pandemic levels, with a slow, steady deterioration of the overall mental health of the population as the pandemic progressed (36, 37), often referred to as the ‘second pandemic’ (38, 39). The health crisis and subsequent lockdowns have been characterized by unpredictability and uncertainty, with numerous restrictions, an increase in unemployment rates, and changes in living standards. These factors have posed sustained stress for many individuals, including those with pre-existing mental health diagnoses and others who had not previously required psychiatric care. Economic recession and social isolation are known factors that exacerbate rates of psychopathology, suicidal behaviors, and substance use, among others, as has previously been reported in other major health crisis (40). Furthermore, these changes have hindered access to mental health services, which were already precarious and overwhelmed in many communities (41, 42). Numerous countries implemented alternatives to address these issues, prominently telemedicine and hotline services. However, the preference of patients is still face to face therapy, and these measures have often proven insufficient (43). Almost two thirds of mental health professionals expressed negative thoughts on the efficacy of telemental health, prominently technology problems and concerns on its safety in certain settings and disorders (44).
Another important finding of our research is that a significant shift has been found in the nature of ED visits after the pandemic. When compared to the pre-pandemic period, there is a substantial increase in consultations related to anxiety, suicidal attempts, and self-harm behaviors. The rising suicide attempt rates during this period is as concerning as consistent with reports from other settings, such as inpatient units (45). As of now, suicide ranks as the leading cause of non-natural death in Spain among those aged 15 to 29 (46), and in 2020, it led to a greater loss of potential life years than the coronavirus itself (47). The results of our study suggest that this trend likely persisted in the years after the pandemic, in line with initial predictions made at the start of the pandemic (48) and similar findings in other countries (49, 50). Recent reports suggest this increase in suicidality to be mainly driven by suicides in older adults, potentially impacted by the isolation, the loss, and bereavement they have faced in the context of particularly high mortality rates in Spain (51). There is an urgent need for the implementation of strategies targeted to particularly vulnerable populations to address and alleviate this critical global health issue. It’s also noteworthy the rise in administrative and social consultations in recent years. These consultations encompass a range of issues, including requests for overnight stays, medical reports or prescriptions, and other administrative matters. The pandemic and its consequences have significantly impacted Spain and its population’s economic conditions (5), with a national health system that was not prepared for the burden of the pandemic due to insufficient funding after budget cuts in the previous economic crisis, that left the country with lower social and health expenditure per capita than the European Union average (52). This, added to the overburdening of primary overburdening of primary care services (53) and a decrease and delay of face-to-face assessments, resulted in patients having increasingly directed these types of non-urgent inquiries and procedures to the ED.
Conversely, there has been a notable decrease in the percentage of urgent care visits for schizophrenia and other psychotic disorders. Additionally, there’s been a reduction in the proportion of urgent consultations related to behavioral alterations not otherwise specified in discharge summaries, many of which are associated with psychotic disorders. This might be reflecting two opposite (but possibly complementing) realities. On the one hand, a prior study in the same population suggested that, compared to individuals with other severe mental disorders, patients with schizophrenia did not experience a significant decline in mental health during and after the COVID-19 pandemic (20). Moreover, patients with schizophrenia maintained adherence to their treatment throughout this period (54). On the other hand, this decrease in the urgent care visits could reflect a loss of follow-up of this group of patients, an especially vulnerable subpopulation that were also at increased risk of COVID-19 hospitalization and mortality risk (55).
This observed shift in urgent care demand patterns post-pandemic likely mirrors a sustained worsening in the mental health of the population, a challenge that outpatient settings may be struggling to meet due to overwhelming demand. This trend, far from moderating, seems to be escalating, as evidenced by historically high levels of urgent psychiatric care at the time of writing this article. This situation urgently calls for not only strengthening emergency services but also enhancing outpatient settings, which are ideally suited for managing most of these demands (56). Resources allocation is highly challenging in a pandemic, where emergency relief resources are needed simultaneously at multiple affected areas (57). However, this pandemic poses an opportunity to prepare for future health crisis and disasters. Additionally, there is a need for developing preventive and social strategies to mitigate the socio-economic impacts of the pandemic. It’s also crucial to acknowledge the potential impact of this increased care demand on healthcare workers, a group significantly affected by the SARS-COV-2 pandemic (58), and to provide additional training to primary care professionals to help them deal with psychological crisis outside the ED (59). Finally, basic self-care strategies can be taught to population to help them recognize and deal with signs of distress, along with education on the use of urgent care settings.
The findings of this study should be interpreted within the context of several limitations. First, the study is subject to the inherent limitations of observational, retrospective designs, where establishing causality between the examined factors is challenging. Nonetheless, the multifaceted impact (health-related (60, 61), social (62, 63), and economic (5), among others) of the COVID-19 pandemic on the mental health of the population has been extensively demonstrated. Second, the limited range of study variables, restricting the investigation to important factors such as the patients’ sex or age. Third, the coding of discharge diagnoses in an emergency department is primarily intended for clinical purposes and is often made under time-sensitive circumstances. Therefore, syndromic diagnoses (such as anxiety) coexist with more specific ones like schizophrenia. And fourth, only the primary coding of each consultation was considered in the analysis. Consequently, it is possible that secondary diagnoses may have been overlooked.
On the other hand, while demand patterns for psychiatric assistance encompass economic and cultural factors (64), Spain’s provision of free and universal healthcare indicates that the data collected in this study likely offers a realistic perspective, unaffected by economic constraints. Furthermore, this study was conducted in a hospital where the psychiatry department serves as a primary point of contact for urgent care, and all patients included were assessed by trained psychiatrists. This contrasts with other centers where general physicians initially manage all urgent consultations, escalating to specialists only in certain cases. Consequently, a vast majority of psychiatric consultations, irrespective of their level of complexity or severity, have been included in this study. This approach significantly enhances the internal validity of the data.
Our findings revealed that COVID-19 pandemic and its aftermath have profoundly altered urgent psychiatric care. Future research should aim to characterize how these past few years have impacted particularly vulnerable subpopulations such as adolescents (65), women (66), and those economically hard-hit by the pandemic (67, 68), who seem more susceptible to psychopathological decline, while other populations might have maintained adequate mental health levels throughout the pandemic. What remains unanswered, however, is whether this has led to an increased demand in any of these subgroups, or if, on the contrary, they remain unable to even access urgent care services.
Our study revealed a disproportionate rise in the number of psychiatric consultations in the emergency department during the post-pandemic period, relative to both the pre-pandemic and pandemic periods, with a notable increase in consultations related to anxiety, suicidal ideation, and self-harm, as well as those linked to administrative and social issues, possibly in relation to the negative impact of the pandemic on Spain’s economy. Conversely, there was a relative decrease in the number of patients presenting with schizophrenia and other psychotic disorders during the same timeframe, which could reflect both a better adaptation to confinement and isolation measures and a loss of follow-up of particularly vulnerable patients. Health systems and particularly urgent care settings should prepare for potential upcoming health crisis, with sufficient budget, resource allocation, and preventive measures. Health systems and particularly urgent care settings should prepare for potential upcoming health crisis, with sufficient budget, resource allocation, and preventive measures.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The Basurto University Hospital Research Ethics Committee gave ethical approval for the 106 study (N.77.23 CEIHU).
CA: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. BP: Data curation, Validation, Writing – original draft, Writing – review & editing. GS: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. NO: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. AC: Supervision, Validation, Writing – original draft, Writing – review & editing. MG: Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research received funding from the OSI Bilbao Basurto Research Commission for publication fees.
The authors would also like to thank Joan Aymerich-Nicolas for his help in the development of the figures.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1380401/full#supplementary-material
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. Novel coronavirus from patients with pneumonia in China, 2019. New Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
2. Cénat JM, Farahi SMMM, Dalexis RD, Darius WP, Bekarkhanechi FM, Poisson H, et al. The global evolution of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis of longitudinal studies. J Affect Disord. (2022) 315:70–95. doi: 10.1016/j.jad.2022.07.011
3. Dragioti E, Li H, Tsitsas G, Lee KH, Choi J, Kim J, et al. large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J Med Virol. (2022) 94:1935–49. doi: 10.1002/jmv.27549
4. Chen J, Vullikanti A, Santos J, Venkatramanan S, Hoops S, Mortveit H, et al. Epidemiological and economic impact of COVID-19 in the US. Sci Rep. (2021) 11:20451. doi: 10.1038/s41598-021-99712-z
5. Pinilla J, Barber P, Vallejo-Torres L, Rodríguez-Mireles S, López-Valcárcel BG, Serra-Majem L. The economic impact of the SARS-COV-2 (COVID-19) pandemic in Spain. Int J Environ Res Public Health. (2021) 18:4708. doi: 10.3390/ijerph18094708
6. Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, Ganz F, Torralba R, Oliveira DV, et al. Impact of social isolation due to COVID-19 on health in older people: mental and physical effects and recommendations. J Nutr Health Aging. (2020) 24:938–47. doi: 10.1007/s12603-020-1500-7
7. van Reekum EA, Woo JJ, Petropoulos J, Samaan Z, Mbuagbaw L. Association between the COVID -19 pandemic and psychiatric symptoms in people with preexisting obsessive-compulsive, eating, anxiety, and mood disorders: a systematic review and meta-analysis of before-after studies. Psychiatry Clin Neurosci. (2023) 77:583–91. doi: 10.1111/pcn.13582
8. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Globalization Health. (2020) 16:57. doi: 10.1186/s12992-020-00589-w
9. Anonymous. The impact of the COVID-19 pandemic and associated control measures on the mental health of the general population. Ann Internal Med. (2022) 175:1560–71. doi: 10.7326/M22-1507
10. Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. (2021) 398:1700–12. doi: 10.1016/S0140-6736(21)02143-7
11. Farooq S, Tunmore J, Wajid Ali M, Ayub M. Suicide, self-harm and suicidal ideation during COVID-19: A systematic review. Psychiatry Res. (2021) 306:114228. doi: 10.1016/j.psychres.2021.114228
12. Yonemoto N, Kawashima Y. Help-seeking behaviors for mental health problems during the COVID-19 pandemic: A systematic review. J Affect Disord. (2023) 323:85–100. doi: 10.1016/j.jad.2022.11.043
13. Rameez S, Nasir A. Barriers to mental health treatment in primary care practice in low- and middle-income countries in a post-covid era: A systematic review. J Family Med primary Care. (2023) 12:1485–504. doi: 10.4103/jfmpc.jfmpc_391_22
14. Gao CX, McDonald LP, Hamilton MP, Simons K, Menssink JM, Filia K, et al. Inequalities in access to mental health treatment by Australian youths during the COVID-19 pandemic. Psychiatr Serv (Washington D.C.). (2023) 74:581–8. doi: 10.1176/appi.ps.20220345
15. Heppner Z, Shreffler J, Polites A, Ross A, Thomas JJ, Huecker M. COVID-19 and emergency department volume: The patients return but have different characteristics. Am J Emergency Med. (2021) 45:385–8. doi: 10.1016/j.ajem.2020.09.009
16. Pines JM, Zocchi MS, Black BS, Carlson JN, Celedon P, Moghtaderi A, et al. Characterizing pediatric emergency department visits during the COVID-19 pandemic. Am J Emergency Med. (2021) 41:201–4. doi: 10.1016/j.ajem.2020.11.037
17. Dragovic M, Pascu V, Hall T, Ingram J, Waters F. Emergency department mental health presentations before and during the COVID-19 outbreak in Western Australia. Australas Psychiatry Bull R Aust New Z Coll Psychiatrists. (2020) 28:627–31. doi: 10.1177/1039856220960673
18. Gonçalves-Pinho M, Mota P, Ribeiro J, Macedo S, Freitas A. The impact of COVID-19 pandemic on psychiatric emergency department visits - A descriptive study. Psychiatr Q. (2021) 92:621–31. doi: 10.1007/s11126-020-09837-z
19. McAndrew J, O’Leary J, Cotter D, Cannon M, MacHale S, Murphy KC, et al. Impact of initial COVID-19 restrictions on psychiatry presentations to the emergency department of a large academic teaching hospital. Irish J psychol Med. (2021) 38:108–15. doi: 10.1017/ipm.2020.115
20. Pedruzo B, Catalan A, Aymerich C, Bordenave M, Estevez O, Gómez DA, et al. Psychological impact of COVID-19 lockdown on a population with serious mental illness. A prospective cohort study. Rev psiquiatria y salud Ment. (2023) 16:59–67. doi: 10.1016/j.rpsm.2022.04.004
21. Devoe D, Han A, Anderson A, Katzman DK, Patten SB, Soumbasis A, et al. The impact of the COVID-19 pandemic on eating disorders: A systematic review. Int J eating Disord. (2023) 56:5–25. doi: 10.1002/eat.23704
22. Di Stefano R, Di Pietro A, Talevi D, Rossi A, Socci V, Pacitti F, et al. Personality disorders (PD) and interpersonal violence (IV) during COVID-19 pandemic: a systematic review. Ann Gen Psychiatry. (2022) 21:11. doi: 10.1186/s12991-022-00388-0
23. Moreira-de-Oliveira ME, de Menezes GB, Loureiro CP, Laurito LD, Albertella L, Fontenelle LF. The impact of COVID-19 on patients with OCD: A one-year follow-up study. J Psychiatr Res. (2022) 147:307–12. doi: 10.1016/j.jpsychires.2022.01.065
24. Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PloS Med. (2015) 12:e1001885. doi: 10.1371/journal.pmed.1001885
26. World Health Organization. International classification of diseases, eleventh revision (ICD-11)(2021). Available online at: https://icd.who.int/browse11.
28. R Foundation for Statistical Computing R. A language and environment for statistical computing. (2021). p. 1.4.1106.
29. Sun H, Liu H, Ma C, Chen Z, Wei Y, Tang X, et al. Psychiatric emergency department visits during the coronavirus disease-2019 pandemic. Front Psychiatry. (2023) 14:1236584. doi: 10.3389/fpsyt.2023.1236584
30. Kim HK, Carvalho AF, Gratzer D, Wong AHC, Gutzin S, Husain MI, et al. The impact of COVID-19 on psychiatric emergency and inpatient services in the first month of the pandemic in a large urban mental health hospital in Ontario, Canada. Front Psychiatry. (2021) 12:563906. doi: 10.3389/fpsyt.2021.563906
31. Pikkel Igal Y, Meretyk I, Darawshe A, Hayek S, Givon L, Levy A, et al. Trends in psychiatric emergency department visits in northern Israel during the COVID-19 outbreak. Front Psychiatry. (2021) 12:603318. doi: 10.3389/fpsyt.2021.603318
32. Holland KM, Jones C, Vivolo-Kantor AM, Idaikkadar N, Zwald M, Hoots B, et al. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry. (2021) 78:372–9. doi: 10.1001/jamapsychiatry.2020.4402
33. Wang D, Mao Z. A comparative study of public health and social measures of COVID-19 advocated in different countries. Health Pol. (2021) 125:957–71. doi: 10.1016/j.healthpol.2021.05.016
34. Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci Prog. (2021) 104:3685042110198–368504211019854. doi: 10.1177/00368504211019854
35. Flodin P, Sörberg Wallin A, Tarantino B, Cerchiello P, Mladá K, Kuklová M, et al. Differential impact of the COVID-19 pandemic on primary care utilization related to common mental disorders in four European countries: A retrospective observational study. Front Psychiatry. (2023) 13:1045325. doi: 10.3389/fpsyt.2022.1045325
36. Office for Health Improvements & Disparities. UK Government. COVID-19 mental health and wellbeing surveillance: report. (2022).
37. Daly M, Sutin AR, Robinson E. Longitudinal changes in mental health and the COVID-19 pandemic: evidence from the UK Household Longitudinal Study. Psychol Med. (2022) 52:2549–58. doi: 10.1017/S0033291720004432
38. Lillehei A. The second pandemic: Mental health. EXPLORE. (2022) 18:257–8. doi: 10.1016/j.explore.2022.03.007
39. Choi KR, Heilemann MV, Fauer A, Mead MA. Second pandemic: mental health spillover from the novel coronavirus (COVID-19). J Am Nurses Assoc. (2020) 26:340–3. doi: 10.1177/1078390320919803
40. Moreno C, Wykes T, Galderisi S, Nordentoft M, Crossley N, Jones N, et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:813–24. doi: 10.1016/S2215-0366(20)30307-2
42. World Health Organization. Regional Office for Europe. Long-stay mental health care institutions and the COVID-19 crisis: identifying and addressing the challenges for better response and preparedness. (2020).
43. Tsamakis K, Dimitrakakis G, Stefanadi E, Tsiptsios D.i., Dimitrakaki IA, Mueller C, et al. The challenges of planetary mental health in the COVID-19 era. Exp Ther Med. (2020) 20:1843–4. doi: 10.3892/etm.2020.8927
44. Lawson JL, Doran JM, O’Shea M, Abel EA. The good, the bad, the uncertain: diverse provider experiences with telemental health during COVID-19. Psychiatr Q. (2022) 93:753–74. doi: 10.1007/s11126-022-09990-7
45. Rodriguez-Jimenez R, García-Fernández L, Baón-Pérez B, Ansede-Cascudo JC, Arroba CM, Sendra-Gutierrez JM, et al. Hospital admissions due to suicide attempts during the COVID-19 pandemic, a 3-year longitudinal study. Psychiatry Res. (2023) 327:115346. doi: 10.1016/j.psychres.2023.115346
46. Instituto Nacional de Estadística INE. (2022). Available online at: https://www.ine.es/prensa/edcm_2020.pdf.
47. Merayo-Cano JM, Porras-Segovia AA, Baca-García E. COVID-19 impact vs. suicide impact in Spain. Spanish J Psychiatry Mental Health. (2023) 16:129–30. doi: 10.1016/j.rpsm.2022.05.006
48. Vieta E, Pérez V, Arango C. Psychiatry in the aftermath of COVID-19 Spanish J Psychiatry Mental Health. (2020) 13:105–10. doi: 10.1016/j.rpsm.2020.04.004
49. Yan Y, Hou J, Li Q, Yu NX. Suicide before and during the COVID-19 Pandemic: A Systematic Review with Meta-Analysis. Int J Environ Res Public Health. (2023) 20:3346. doi: 10.3390/ijerph20043346
50. Pathirathna ML, Nandasena HMRK, Atapattu AMMP, Weerasekara I. Impact of the COVID-19 pandemic on suicidal attempts and death rates: a systematic review. BMC Psychiatry. (2022) 22:1–506. doi: 10.1186/s12888-022-04158-w
51. Martínez-Alés G, López-Cuadrado T, Morrison C, Keyes K, Susser E. The impact of the COVID-19 pandemic on suicide mortality in Spain: Differences by sex and age. J Affect Disord. (2023) 329:315–23. doi: 10.1016/j.jad.2023.02.115
52. Anonymous. The Economic Impact of the SARS-COV-2 (COVID-19) Pandemic in Spain. Health at a glance: Europe 2018. (2018). doi: 10.1787/health_glance_eur-2018-en
53. Khalil-Khan A, Khan MA. The impact of COVID-19 on primary care: A scoping review. Cureus. (2023) 15:. doi: 10.7759/cureus.33241
54. Burrai J, Roma P, Barchielli B, Biondi S, Cordellieri P, Fraschetti A, et al. Psychological and emotional impact of patients living in psychiatric treatment communities during covid-19 lockdown in Italy. J Clin Med. (2020) 9:3787. doi: 10.3390/jcm9113787
55. Catalan A, Aymerich C, Bilbao A, Pedruzo B, Pérez JL, Aranguren N, et al. Psychosis and substance abuse increase the COVID-19 mortality risk. Psychol Med. (2023) 53:4236–44. doi: 10.1017/S0033291722000976
56. Moise N, Wainberg M, Shah RN. Primary care and mental health: Where do we go from here? World J Psychiatry. (2021) 11:271–6. doi: 10.5498/wjp.v11.i7.271
57. Aalami S, Kattan L. Fair dynamic resource allocation in transit-based evacuation planning. Transp Res Part C Emerg. (2018) 94:307–22. doi: 10.1016/j.trc.2017.10.018
58. Aymerich C, Pedruzo B, Pérez J, Laborda M, Herrero J, Blanco J, et al. Covid-19 pandemic effects on health workers’ mental health: systematic review and meta-analysis. Eur Psychiatry. (2022) 65(1):e10. doi: 10.1192/j.eurpsy.2022.1
59. Greenberg N, Brooks SK, Wessely S, Tracy DK. How might the NHS protect the mental health of health-care workers after the COVID-19 crisis? Lancet Psychiatry. (2020) 7:733–4. doi: 10.1016/S2215-0366(20)30224-8
60. Poudel AN, Zhu S, Cooper N, Roderick P, Alwan N, Tarrant C, et al. Impact of Covid-19 on health-related quality of life of patients: a structured review. PLoS One. (2021) 16:. doi: 10.1371/journal.pone.0259164
61. Kang E, Lee H, Sohn JH, Yun J, Lee JY, Hong Y. Impact of the COVID-19 pandemic on the health status and behaviors of adults in Korea: national cross-sectional web-based self-report survey. JMIR Public Health Surveill. (2021) 7:. doi: 10.2196/31635
62. Tai DBG, Shah A, Doubeni CA, Sia IG, Wieland ML. The disproportionate impact of COVID-19 on racial and ethnic minorities in the United States. Clin Infect Dis. (2021) 72:703–6. doi: 10.1093/cid/ciaa815
63. Long E, Patterson S, Maxwell K, Blake C, Bosó Pérez R, Lewis R, et al. COVID-19 pandemic and its impact on social relationships and health. J Epidemiol Community Health. (2022) 76:128–32. doi: 10.1136/jech-2021-216690
64. Thrasher T, Aggarwal A, Popoola O. COVID-19 pandemic and its impact on social relationships and health. Cultural competence in emergency psychiatry. (2023) 97–C6P79. doi: 10.1093/med/9780197624005.003.0006
65. Fortea A, Fortea L, Gómez-Ramiro M, Fico G, Giménez-Palomo A, Sagué-Vilavella M, et al. Upward trends in eating disorders, self-harm, and suicide attempt emergency admissions in female adolescents after COVID-19 lockdown. Spanish J Psychiatry Mental Health. (2023). doi: 10.1016/j.sjpmh.2023.09.003
66. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. (2021) 8:141–9. doi: 10.1016/S2215-0366(20)30482-X
67. Bu F, Steptoe A, Fancourt D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health. (2020) 186:31–4. doi: 10.1016/j.puhe.2020.06.036
Keywords: emergency, pandemic, coronavirus, psychiatric, ED
Citation: Aymerich C, Pedruzo B, Salazar de Pablo G, Olazabal N, Catalan A and González-Torres MÁ (2024) Number and nature of psychiatric emergency department visits in a tertiary hospital before, during, and after coronavirus pandemic. Front. Psychiatry 15:1380401. doi: 10.3389/fpsyt.2024.1380401
Received: 01 February 2024; Accepted: 01 April 2024;
Published: 18 April 2024.
Edited by:
Johannes M. Hennings, kbo Kliniken des Bezirks Oberbayern, GermanyReviewed by:
Marcelo O’Higgins, National University of Asunción, ParaguayCopyright © 2024 Aymerich, Pedruzo, Salazar de Pablo, Olazabal, Catalan and González-Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudia Aymerich, Y2xhdWRpYS5heW1lcmljaG5pY29sYXNAb3Nha2lkZXR6YS5ldXM=
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.