 Geneviève Piché1,2,3*
Geneviève Piché1,2,3* Aude Villatte2,4
Aude Villatte2,4 Marie-Ève Clément1Marie-Hélène Morin5
Marie-Ève Clément1Marie-Hélène Morin5 Darryl Maybery6
Darryl Maybery6 Andrea Reupert7Stéphane Richard-Devantoy8
Andrea Reupert7Stéphane Richard-Devantoy8 Marianne Fournier-Marceau1
Marianne Fournier-Marceau1- 1Département de psychoéducation et de psychologie, Université du Québec en Outaouais, Saint-Jérôme, QC, Canada
- 2Centre de Recherche Universitaire Sur les Jeunes et les Familles (CRUJEF), Québec, QC, Canada
- 3Réseau de recherche en santé des populations du Québec (RRSPQ), Montréal, QC, Canada
- 4Unité de Formation et de Recherches (UFR) de Psychologie, Université Toulouse Jean Jaurès, Laboratoire Psychologie de la Socialisation - Développement et Travail (PSDT), Toulouse, France
- 5Département de travail social, Université du Québec à Rimouski, Rimouski, QC, Canada
- 6Department of Rural and Indigenous Health, Monash University, Melbourne, VIC, Australia
- 7School of Educational Psychology and Counseling, Monash University, Melbourne, VIC, Australia
- 8Department of Psychiatry and Douglas Mental Health University Institute, McGill Group for Suicide Studies, McGill University, Montréal, QC, Canada
Context: Engaging family members in the ongoing care of individuals with mental illness is a practice known to bolster the client’s recovery journey and enhance the overall wellbeing of both children and families involved. Despite its potential benefits, there remains a dearth of understanding surrounding the implementation of family-focused practices (FFP) by mental health professionals serving adults, as well as the factors that could either promote or hinder such practices. This knowledge gap is particularly pronounced within North American settings.
Goal: The goal of this study was to identify potential hindering and enabling factors of FFP used in adult mental health services.
Methods: A sample of 512 professionals working with adult mental health clients, from all regions of Quebec, Canada, with a variety of disciplinary backgrounds and working in different work settings, completed the Family Focused Mental Health Practice Questionnaire (FFMHPQ). Multinominal logistic regression analysis was performed to assess the impact of several factors – organizational, professional, and personal – on the degree of family-based practices of mental health workers.
Results and discussion: Findings of this study show that the strongest predictors for the adoption of higher FFP levels among adult mental health professionals in Quebec, are being employed on a full-time basis, perceiving a higher level of skills, knowledge, and confidence toward FFP, and having a supportive workplace environment. Results underscore the need to address both organizational and worker-related aspects to effectively promote better FFP in mental health services.
Background
Fostering the mental health of children of parents with a mental illness, in addition to providing support to the parent with a mental illness, is recommended practice in Canada and elsewhere (1–4). Children with a parent with a mental illness (4, 5) represent a highly vulnerable group (6, 7), and are at greater risk of developing psychosocial and school adjustment difficulties, as well as mental illnesses, than other children (8–10). Additionally, some children will provide significant support to their parent, by helping them with their treatment, assuming domestic responsibilities, and providing them emotional support, often at the expense of their own needs (10, 11). Compared to their same-aged peers, children who have a parent with a mental illness report more conflictual parent-child relationships, as well as situations of verbal or physical abuse (12, 13), trauma and neglect (14, 15). Moreover, parents with a mental illness may worry about fulfilling their parenting role, when the symptoms of their mental illness interfere with their ability to meet their children’s needs (16). For example, parents report feelings of “guilt” and have perceptions of “failure as a person and as a parent” and describe a loss of hope in their parenting role (16). Parental stress has also been shown to predict high levels of depressive symptoms in mothers (17).
As nearly half of adult users of mental health services are parents (18), adult mental health professionals have an important role to play in identifying and supporting children, parents and families, and, when needed, referring them to other services (19, 20). Family focused practices (FFP) involve mental health professionals working with the client and his or her family, including children (4). In mental health services, practices may involve identifying client's children, offering information to families supporting the parent in his parenting role, proposing a support group for children, depending on the families’ needs (4, 19, 21–23). FFP has been found to reduce the risk of intergenerational transmission of mental illnesses and improve the psychosocial adjustment and mental health of children of parents with a mental illness, while promoting the mental health recovery of parents who have a mental illness (4, 24–26). Notably, the risk of developing a mental illness decreases by 40-50% when children of parents with a mental illness receive appropriate support (2, 9). Such practices form part of a promising selective prevention strategy to improve the mental health of children, parents and families at a population level (27).
Thus, there is a need for a family-focused approach in psychiatry and mental health services, that goes beyond solely working with the adult client and entails addressing the needs of the whole family. However, to date, FFP appears to be scarcely provided in adult mental health services (28–30). To illustrate, in Norway, only 56% of clients’ minor children are identified by professionals (31), and of these, only one-third have benefited from some kind of support (32).
A number of organizational, professional, and personal factors have been highlighted as enabling or inhibiting the use of FFP (33–36). First, organizational-related factors, such as perceived workplace support (37–40), has been identified as an important predictor of FFP. Coworkers can offer guidance and emotional support to mental health professionals confronted with difficult or sensible situations, while managers can give access to specific training or supervision. Some studies have explored other organizational factors such as time and workload, or the proportion of caseloads with a parental status. However, the results are still inconclusive, particularly regarding which element plays the most significant role (39, 41–44). Additionally, a high workload perception may be linked to the employment status of the professional (45), as well as the nature or complexity of the cases in their caseload (46).
Previous research has emphasized the significance of worker-related factors in predicting practices that aim to identify dependent children of adults receiving mental health services, or of practices that offer support to families. One key factor is the nature of the profession or job role, which can influence the extent to which workers engage in these practices (28, 47–49). Studies suggest that psychologists tend to engage in such practices to a lesser extent than social workers, who are more likely to identify and support families on a routine and systematic basis. In addition, some studies have looked at the impact of professionals’ attitudes towards FFP and their beliefs about the benefits of such practices for their clients and families (38, 50, 51). Results are mixed, with some studies indicating that attitudes and beliefs strongly influence FFP (51) while others have found no significant associations (50).
Furthermore, prior research underscores the pivotal role of professionals’ perceived skill and knowledge around parental mental illness and family relationships as an important enabler of FFP (38, 39, 42, 43, 52). As such, some professionals express a lack of confidence in their preparedness to assist parents with mental health challenges in navigating their parental challenges or in evaluating family needs, thereby impeding the adoption of FFP (51, 53). Nonetheless, while a perceived need for training was not significantly associated with lower scores of FFP in one study (43), receiving training in family intervention or FFP specifically was identified as a predictor of FFP uptake in various studies (41, 43, 47). Similarly, the number of years of experience has been recognized as a predictor of FFP in some instances (44, 53), although its significance was not consistently supported across all studies (e.g., 43). Consequently, the literature remains inconclusive regarding the impact of training, years of experience, and perceived proficiency on the facilitation of FFP.
Finally, certain personal characteristics of professionals may impact their use of FFP. These include being a female (41, 43), being a parent or having confidence around children (42, 44). Additionally, personal experience of mental illness may also play a role (44). However, the evidence is still scarce as very few studies have investigated these factors.
In summary, several studies have delved into the determinants influencing the adoption of FFP among mental health professionals. However, the current body of evidence presents a heterogeneous picture concerning the influence of workplace (such as support, caseload loading, and employment status), worker (including training, years of experience, and perceived competence) and personal experiential factors (such as familiarity with children or mental illness). Additionally, this study is the first to investigate predictors of FFP within North American contexts.
Thus, the aim of the current study is to investigate the practices, attitudes, knowledge, and skills related to FFP of a sample of the Quebec adult mental health professional workforce. The study also aims to identify the factors that predict the use of FFP with parents who have a mental illness and to examine their relative importance. This is important information that can be used to benchmark practices, inform training and policy and the deployment of resources. Based on previous research, it is hypothesized that professionals’ attitudes around the relevance of FFP, workplace support, and confidence about using FFP will be associated with higher FPP scores, compared to those with lower FFP scores.
Methods
Design
This study was approved by the Research Ethics Boards of the Université du Québec en Outaouais (#2021-1167), the CIUSSS de la Capitale-Nationale (#MP-13-2021-2135). A cross-sectional design was used to recruit a convenience sample of French-speaking Canadian adult mental health workers across Quebec (Canada). To be eligible, professionals had to meet the following criteria: 1) work at the time of the survey with adult with mental illness (under 65 years old), 2) have direct contact with clients, and 3) be fluent in French. Those working exclusively with children were excluded.
From March to December 2021, all eligible professionals were invited to read a detailed description of the study, sign a consent form and respond to an online questionnaire via a LimeSurvey platform. Following Fan and Yan (54) recommendations, various recruitment strategies were employed to ensure a satisfactory participation rate: 1) emails to professional groups and orders, 2) emails sent through managers of all integrated health and social services centers (CISSS) from each of the 17 administrative regions of Quebec, medical clinics and community organizations offering adult mental health services and 3) promotion on social networks and local newspapers. Presentations conducted by the principal investigator were delivered at targeted workplaces (13 CISSS) to explain the project and to seek assistance with the recruitment of professionals. To encourage participation, compensation prizes were drawn among study participants, with one $25 prize per 50 participants. A total of 512 French-speaking adult mental health workers completed the questionnaire.
Measures
The study collected sociodemographic and occupational information such as gender, age, ethnicity, years of experience in mental health, workplace and location of services, employment status (full-time or part-time), percentage of parents with mental illness on caseload (low: ≥ 20%, moderate: 21-50%, high: >50%), level of education, personal experience of mental illness (yes or no), level of comfort around children.
The French version of the Family-Focused Mental Health Practice Questionnaire (FFMHPQ-FR) was used to collect self-report data on mental health professional’s FFP and related factors. The original questionnaire consisted of 45 items rated on a seven-point Likert scale (1=strongly disagree to 7=strongly agree) and demonstrated good psychometric properties for 13 of the 16 subscales (Cronbach’s alphas = 0.61 to 0.89) (55). The development of the FFMHPQ-FR underwent a rigorous process, as detailed in Piché et al. (56). It was initially translated into French through a back-translation procedure (57) and was subsequently adapted to improve its psychometric proprieties (i.e. seven items added to the subscales with limited consistency) and to consider recent literature (i.e. three item added on attitudes and beliefs toward FFP) (36). Finally, it was validated through both exploratory and confirmatory factor analysis, resulting in 42 items grouped into five subscales (Family-Focused Practices; Workplace support for FFP; Skills, knowledge and confidence; Openness to improve practice; Attitudes and beliefs toward FFP), with good psychometric properties (α = 0.61 to 0.89) (Table 1) (56). Scores are calculated by averaging the items included within each subscale for every participant.
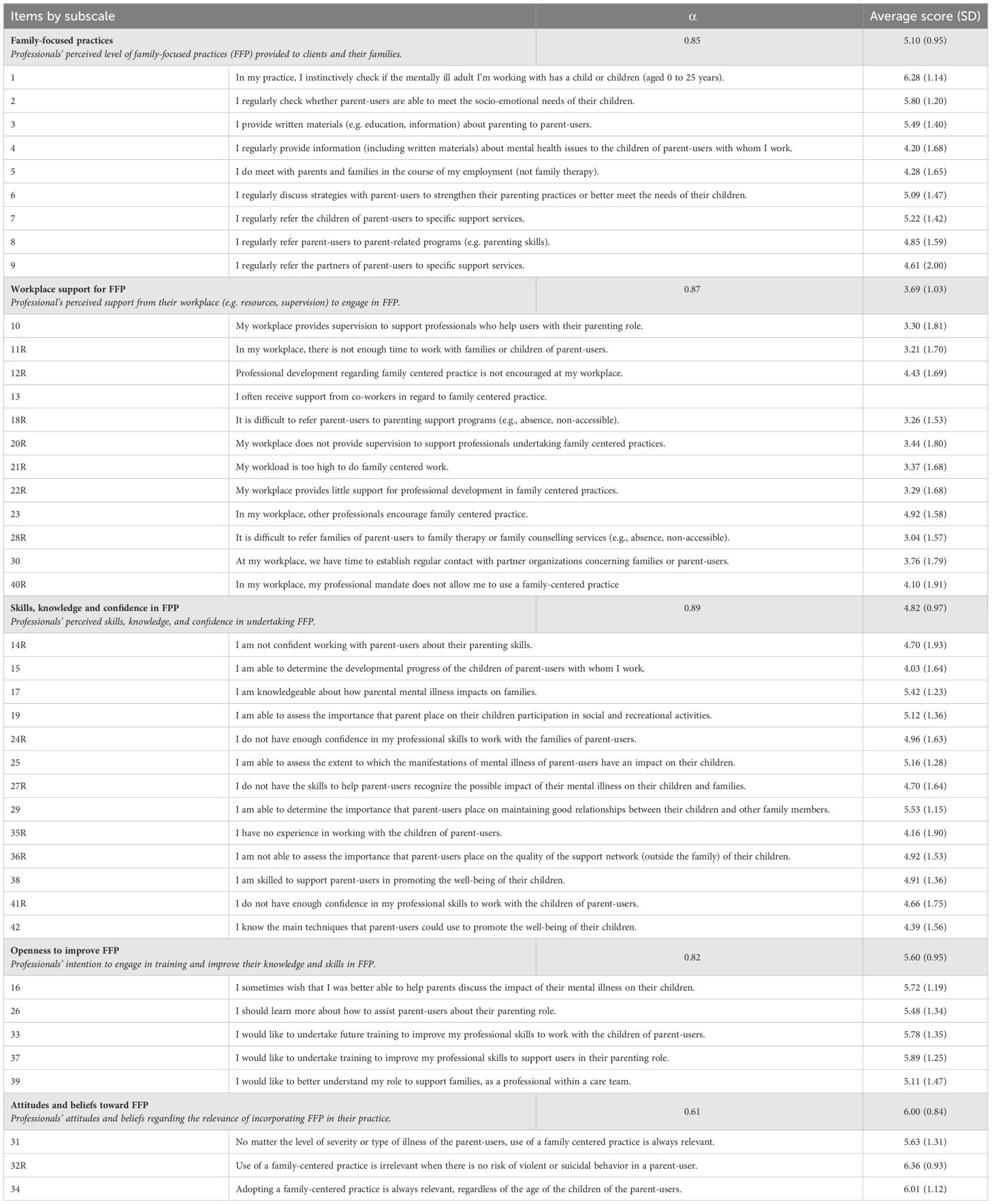
Table 1 FFMHPQ-FR and average subscale’s scores among participants.
Data analysis
Across the 42 items of the FFMHPQ-FR, the rate of valid data amounted to 90.8%. Participants were required to answer each question in the questionnaire, while also having the option to select the responses “refusal to answer” or “does not apply.” These response choices were coded as missing data and treated using mean imputation per item (58).
All statistical analyses were performed using SPSS Version 27.0 software. As a preliminary analysis, the following assumptions were tested: sample size, multicollinearity, outliers and normality. Outliers were treated by winsorizing 2nd and 98th percentile. Descriptives (means, standard deviations) were calculated for all variables. Analyses of variance (ANOVA) and chi-square tests were conducted aiming to verify the relationship between mental health worker’s FFP and variables of interest in this study. Post-hoc analyses allowed to specify the nature of the differences between the groups.
A multinomial logistic regression analysis was performed to assess prediction of mental health worker’s FFP on the basis of ten factors: Workplace support for FFP subscale, employment status, percentage of parents with mental illness on caseload, years of experience in mental health, level of education, Skills, knowledge and confidence subscale, Openness to improve practice subscale, Attitudes and beliefs toward FFP subscale, level of comfort around children, and personal experience of mental illness. To perform this, scores from the FFP subscale were recoded into three categories: low (1.00-4.77), moderate (4.78-5.55) and high (5.56-7.00) score of FFP, based on percentile-based cut-points (respectively on the 33rd and 67th percentiles). Using a three-categorical variable will provide interpretable coefficients to quantify the relationship between predictors and the outcome variable. Thus, the high score category allows to discriminate professionals that provide more FFP to clients and their families. The results are presented as inverted odds ratio (IOR), easier to interpret with negative beta. The significance level in all analyses was .05.
Results
Participants
The majority of participants were female (87.1%) and the average age was 40.34 years (range 19-75 years). Most were Caucasians (95.9%), born in Quebec (92.0%). The majority (85.7%) were university graduates, from various disciplines including social work (27.9%), nursing (20.9%), psychology (13.9%), psychoeducation (13.1%) and special education (8.0%). The average number of years’ of experience in mental health was 11.77 (range 1-40 years). Among the participants, 27% reported that more than half of their caseload included clients with mental illness who have at least one minor child. In the past five years, 43.3% had received family-focused training, while 34.8% had attended child-focused training.
Table 1 presents the average scores of participants on the FFMHPQ-FR’s subscales and items. The average score on the FFP subscale (M=5.13; SD=1.06) indicates a moderate level of FFP among mental health professionals in this sample. The highest item scores were reported on Identification of children, Evaluating parenting competencies and Information to parents, while the lowest were attributed to Information to children, Family meetings and Referrals to support services. Among the subscales, the participants scored the lowest on Workplace support for FFP (M=3.70; SD=1.13), with most items scoring under 4. The highest subscale scores were reported on the Attitudes and beliefs toward FFP (M=5.58; SD=1.04) and the Openness to improve FFP (M=6.00; SD=0.85).
Table 2 presents descriptive statistics of all variables, according to the three percentile-based categories of FFP score (low, 34.8%; moderate, 32.4%; high, 32.8%). Differences between groups for the following eight independent variables have been identified through post-hoc analyses: Workplace support for FFP, employment status, proportion of parental clientele, Skills, knowledge and confidence in FFP, Openness to improve FFP, Attitudes and beliefs toward FFP, highest academic degree, and years of experience in mental health.
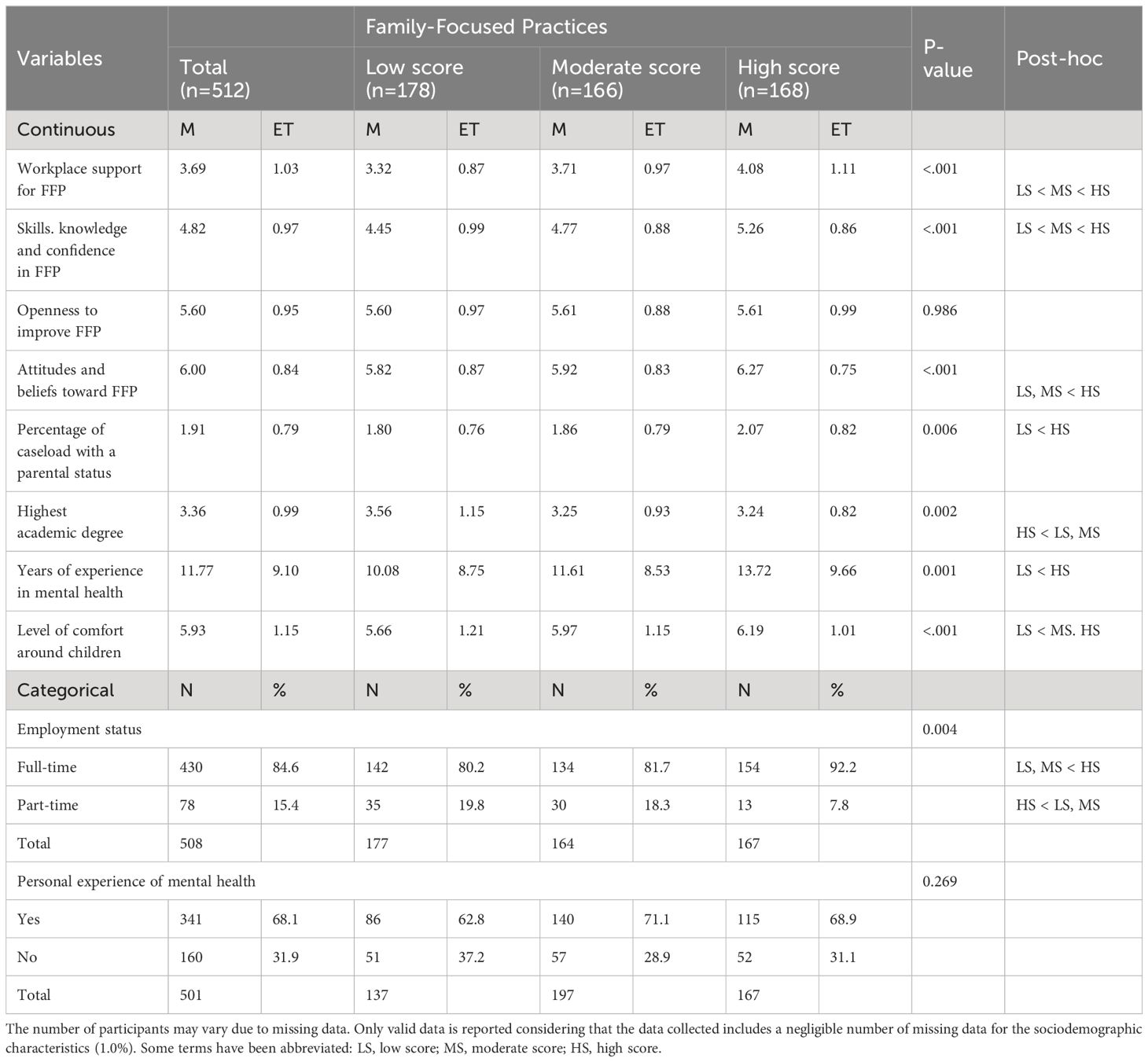
Table 2 Comparisons of variables of interest on Family-Focused practice score.
Predictors of FFP
The model including all ten predictors, when compared to a constant-only model, was statistically significant, χ2 (5, N=482) = 145.22, p<.001. This indicates that the predictors, as a set, significantly discriminate between low, moderate, and high score participants. The model explained 29.3% of the variance in FFP score, according to Nagelkerke R².
This model classified 53.3% of cases correctly, which is greater than the proportional by chance criterion of 41.7% (Table 3). However, specific classification rates (low score, 66.1%; moderate score, 28.4%; high score, 64.2%) underline the model’s tendency to under classify the moderate FFP scores compared to low and high score categories.
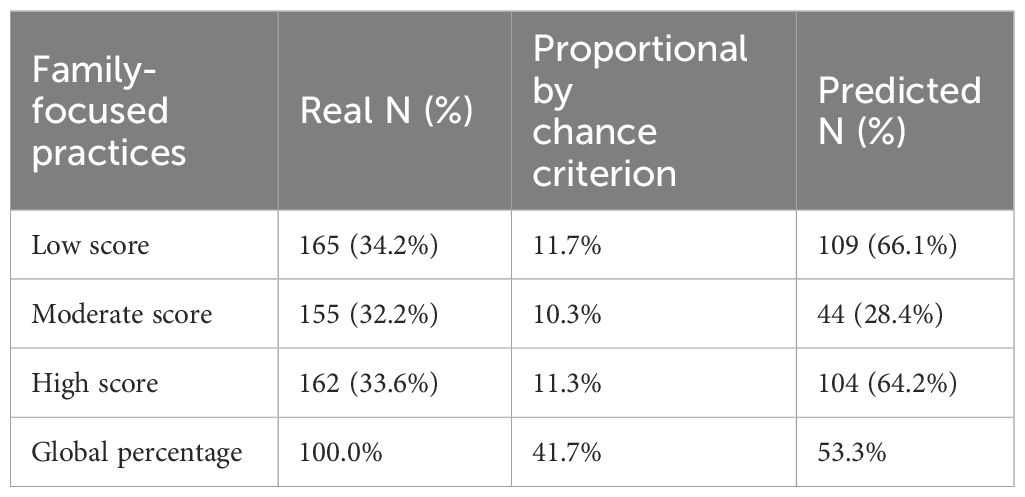
Table 3 Multinomial logistic regression results – Classification table.
Comparing low score FFP with high score FFP categories, it was found that the strongest predictors of reporting a high FFP score as a professional are employment status (full versus part time) (IOR=2.34), and skills, knowledge, and confidence toward FFP (high versus low score) (IOR=2.26) (Table 4). This indicates that professionals employed full-time are 2.34 times more likely to report a high FFP score rather than a low FPP one, controlling for all other factors in the model. Likewise, for every point increase on the Skills, knowledge and confidence subscale, professionals are 2.26 times more likely to present a high FFP score. The perceived level of workplace support for FFP (high versus low) (IOR = 1.90), openness to improve FFP (high versus low) (IOR = 1.52), and attitudes and beliefs towards FFP (high versus low) (IOR =1.61) were also found as important predictors of FFP. Weaker predictions were found between high FFP and the proportion of caseloads with a parental status (high versus low) (IOR = 1.49) and the professional’s years of experience working in mental health (high versus low) (IOR = 1.04). The professional’s education (highest diploma), being comfortable with children, and personal experience with mental illness were not found to predict a high score of FFP compared with a low FFP score.
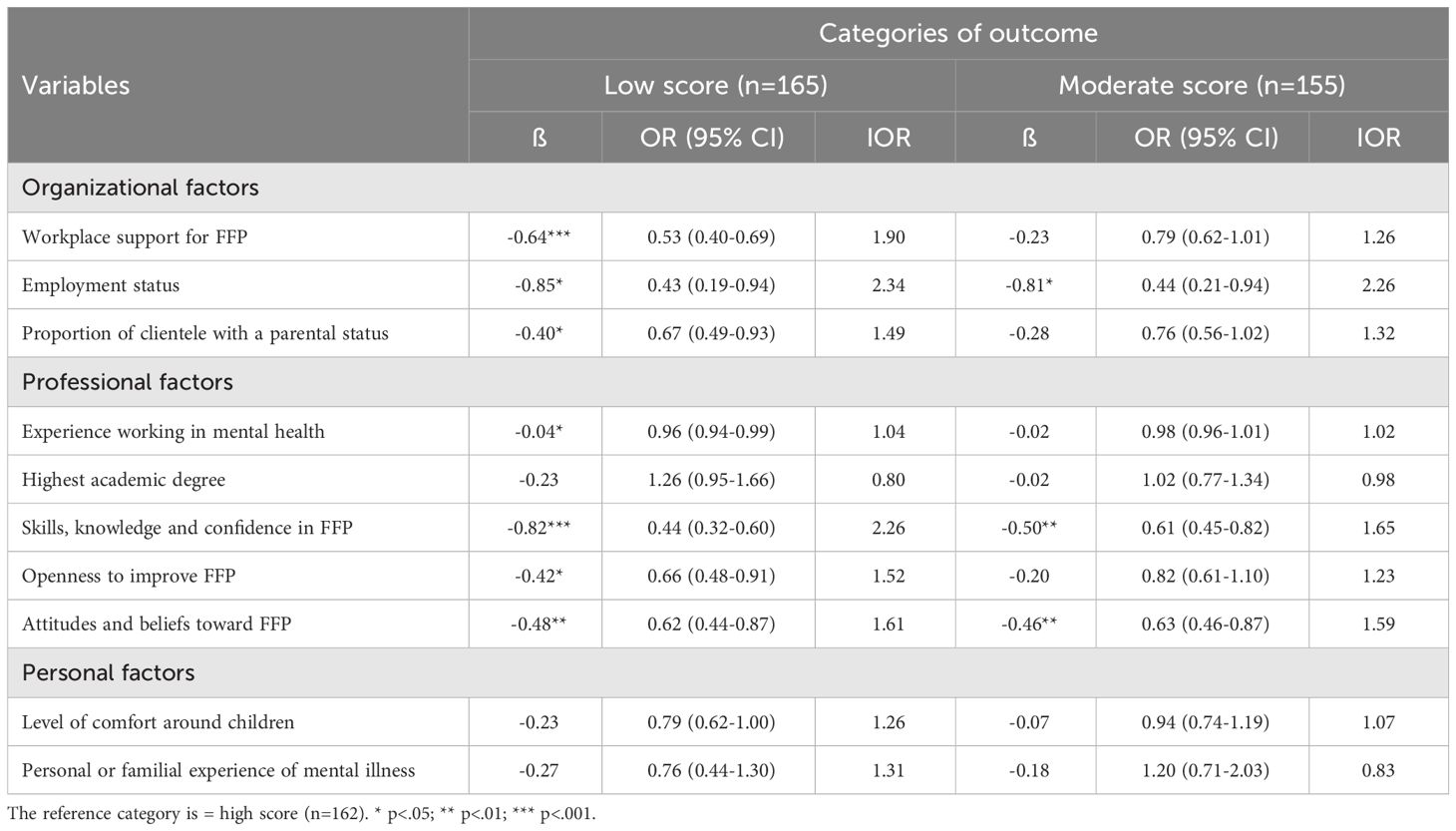
Table 4 Multinomial logistic regression results – High FFP score compared to low and moderate FFP scores.
When comparing moderate FFP score with high FFP score categories, the strongest predictor was found to be the employment status of professionals (full-time versus part-time) (IOR=2.26). Thus, professionals who work full-time are 2.26 times more likely to have a high FFP score than a moderate one, controlling for all other factors in the model. The perceived skills, knowledge, and confidence in FFP (IOR=1.65) and attitudes and beliefs towards FFP (IOR=1.59) were also found to be important predictors of FFP. This indicates that for every point increase on the Perceived skills, knowledge and confidence and the Attitudes and beliefs toward FFP subscale, professionals are respectively 1.65 times and 1.59 times more likely to have a high FFP score rather than a moderate one. None of the other factors were found to be associated with a high score of FFP compared with a moderate FFP score.
Discussion
The present study investigated the FFP of a sample of Quebec adult mental health professionals, FPP predictors and the relative importance of these predictors. Our study addressed a notable gap in the literature by investigating the use of FFP among mental health professionals in North American settings, as well as the factors influencing their engagement in such practices. By doing so, the study contributes to bolstering the evidence base in this critical area of research.
FFP among Quebec adult mental health professionals
The study’s findings shed light on the state of FFP among mental health professionals in Quebec, revealing a generally moderate level of engagement with families. This involves actions such as checking if clients have minor children, providing written materials on mental health and parenting, and discussing parenting strategies. Moreover, professionals reported a moderate level of perceived skills, knowledge and confidence around FFP. Results also suggest that most workers understand the relevance of offering support to children and families whose parent has a mental illness, and that they are generally open to improve their practice to better support families. Interestingly, the results seem to contrast with international studies that show lower self-reported FFP levels among adult mental health workers than FFP scores in our study. For example, in Skogøy et al. (43), the average scores for the FFP subscales are respectively 3.85 (Family support) and 4.08 (Referrals). This could suggest a unique context in Quebec where professionals appear more inclined towards FFP practices.
It is however worth noting that even though the participants in this study reported using moderate FFP levels, there were variations in responses across specific FFP activities. While a majority of the sample (84%) report that they routinely inquired about clients having minor children, discussing parenting strategies and providing mental health information directly to clients’ children were not frequently reported. These findings emphasize the need for improvement in mental health care practices concerning support for children of parents with mental illness. Professionals should not only identify such children but also play a proactive role, including offering age-appropriate information on mental illness, offering help around parenting issues and referring children and parents to appropriate support services. The results underscore the importance of expanding professionals’ awareness of their role in supporting families affected by mental illness, urging them to go beyond identification and incorporate further comprehensive strategies.
Simultaneously, results indicate that workplace support scored the lowest among all the other worker or workplace factors reported by participants. This finding generally converges with the literature, underlining that few organizations have clear guidelines supporting a family-focused approach and that most professionals feel that there are still major obstacles in their workplace for them to adopt FFP with their caseload, such as lack of necessary space and resources to invite their clients’ children for family meetings, as well as limited time to do so (36, 59). Our findings thus show that Quebec professionals feel unsupported by their work environment when it comes to offering support to families of parents receiving mental health services. Most professionals report not having sufficient time to work with families, indicated that their workload is too high, and that there are no specific parenting or family programs to refer clients’ families to when needed.
Predictors of FFP
The study revealed significant predictors of FFP, encompassing both organizational and professional factors. Surprisingly, neither of the two personal factors examined—comfort with children or personal experience with mental illness—emerged as significant predictors of professionals’ FFP scores. This finding contrasts with previous research findings (44), thus enriching the existing literature. Additionally, while some predictors were consistent across high versus low FFP scores and high versus moderate FFP scores, a closer examination reveals a greater number of significant associations between low and high FFP levels.
Worker-related predictors
Results underscore the significance of professionals’ attitudes toward FFP, and their perceived competence, knowledge, and confidence in predicting higher levels of self-reported engagement in FFP. These findings align with prior research, emphasizing that professionals who exhibit confidence in using FFP and acknowledge its importance are more likely to integrate it into their daily practice (39, 43, 52). Recognizing the unique parenting challenges faced by parents that have a mental illness, understanding the needs of their children, and feeling confident in engaging with and offering them support, are identified as crucial elements for the successful adoption of FFP with parents and their families. Notably, participants reported moderate to high scores on these factors, indicating a positive trend toward FFP.
Two additional professional characteristics emerged as significant predictors of FFP adoption: years of experience in adult mental health and professionals’ openness to improving their practice. This aligns with previous findings, showing that professionals with more than five years of experience were more likely to report higher levels of family and parenting support than their less-experienced counterparts (41). Hence, these worker-related characteristics play a pivotal role in ensuring the adoption of FFP in their interactions with clients. On this basis, it is recommended to offer targeted FFP training to professionals, to empower them to feel confident and prepared to use FFP with parents and families (41). Specifically, such training should include informing professionals about the impact of mental illness on parenting and equipping them with practical skills for engaging, communicating, and offering support to families (60). Best practices for interacting with children and families in the context of adult mental health should be systematically integrated into treatment protocols.
The importance of the workplace
Results show that three workplace-related factors significantly predict a high FFP score: perceived workplace support for FFP, the professional’s employment status and the percentage of their clients with children. These findings converge with earlier research (43, 52), underlining the crucial role of workplace factors, including time constraints, workload, and access to supervision, as important predictors of FFP engagement among adult mental health professionals. These findings support the importance of raising awareness among responsible for clinical programs in mental health services and community organizations, about professionals’ roles and responsibilities in FFP and the need to provide adequate resources, particularly time.
Moreover, our finding regarding employment status, revealing that full-time work basis predicts a higher level of FFP, has not been yet addressed in the literature. It is possible to hypothesize that professionals employed on a full-time basis may have more time to work with families and may benefit from enhanced training or supervision, compared to those working part-time. This is an important finding, especially considering that more and more professionals work part-time in industrialized countries (61, 62). While this could account for their higher level of FFP, future research should investigate the differences between professionals working full-time and part-time, specifically around workload, training, and supervision. Furthermore, recognizing that working with families is complex and may require more time, organizations might adjust caseload expectations when screening and assessing the needs of clients with children, as well as ensure that all professionals, regardless of their employment status, receive comprehensive support in FFP.
To further support professionals in adopting FFP, the implementation of clear clinical guidelines and procedures is recommended. Additionally, providing access to specific FFP supervision or facilitating multi-disciplinary team discussions, might enhance understanding and acceptance of FFP as an integral part of all professions within the team (43). These measures may not only contribute to a shared sense of responsibility within the team but also help professionals feel actively involved and supported in embracing FFP practices (36). Overall, fostering a supportive work environment with the necessary resources and infrastructure is crucial to encouraging widespread adoption of FFP among mental health professionals.
Findings underscore the importance of ongoing monitoring and benchmarking of FFP within every workplace. To cultivate a work environment conducive to FFP, it is crucial for managers responsible for clinical programs to not only be aware of professionals’ roles and responsibilities but also to continually monitor the integration of FFP practices. Regular assessments and benchmarking can provide valuable insights into the effectiveness of existing support systems, allowing for necessary adjustments and improvements (63).
Limits and recommendations for future research
Although the sample size is adequate and the profile of participating professionals is comparable to that of other studies conducted in Quebec (e.g., 64), it is nevertheless a convenience sample and may not be representative of the population of professionals working with adults receiving mental health services in Quebec. It is possible that those who participated were more concerned about children who have a parent with a mental illness, which could have led to a bias in the representativeness of the results, resulting in a tendency to overestimate their use of FFP, as evoked by Gregg et al. (36). Future studies should be conducted with a larger and more diverse sample that is representative of all professionals working with adults receiving mental health services, to enhance the generalizability of findings. It is also important to remember that the data are self-reported, questionnaire-based, and may not reflect the actual practice of professionals. More studies including direct observations or audits of professionals’ interactions with families and children (32), or qualitative interviews, should be conducted to ensure the accuracy of results, as well as longitudinal studies to track professionals’ practices over time. Finally, this study is cross-sectional, indicating that the relationships identified in our analysis may not be causative. Based on our results, it is not possible to determine whether the consideration of these predictors in the care and services provided to adults with a mental illness and their families might impact their recovery and well-being.
Conclusion
Given the crucial role of interpersonal relationships and social networks in individual recovery, it is imperative for all mental health professionals to adopt a family-focused approach. This approach involves systematically considering the involvement of children in their interventions. Despite a wealth of evidence supporting family involvement in mental health (65), achieving systematic implementation remains challenging. Findings of this study show that the strongest predictors for the adoption of higher FFP levels among adult mental health professionals in Quebec, are being employed on a full-time basis, perceiving a higher level of skills, knowledge, and confidence toward FFP, and having a supportive workplace environment. Results underscore the need to address both organizational and worker-related aspects to effectively promote better FFP in mental health services. This study significantly contributes to the existing literature by facilitating global learning and knowledge transfer on predictors of FFP, improving understanding of global standards in mental health. Understanding the predictors for adopting family-focused practices can facilitate the development of more effective strategies and interventions that can be implemented globally.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by the Research Ethics Boards of the Université du Québec en Outaouais (#2021-1167), the CIUSSS de la Capitale-Nationale (#MP-13-2021-2135). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
GP: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AV: Conceptualization, Funding acquisition, Investigation, Methodology, Validation, Visualization, Writing – review & editing. M-EC: Conceptualization, Investigation, Methodology, Validation, Writing – review & editing. M-HM: Conceptualization, Investigation, Methodology, Validation, Writing – review & editing. DM: Validation, Writing – review & editing. AR: Writing – review & editing. SR-D: Methodology, Writing – review & editing. MF-M: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors thank the Social Sciences and Humanities Research Council of Canada (SSHRC) for their financial support to the project (#435-2020-1092). We are also grateful for the financial support that we received from the Centre de recherche universitaire sur les jeunes et les familles (CRUJeF).
Acknowledgments
The authors wish to thank all the organizations that helped us with the recruitment of participants, and all professionals who agreed to take part in this study. We are also grateful for the statistical guidance provided by Denis Lacerte, advisor at CRUJeF for the research development.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gouvernement du Québec. Instaurer une société bienveillante pour nos enfants et nos jeunes: Résumé du rapport de la Commission spéciale sur les droits des enfants de la protection de la jeunesse. Québec, QC, Canada: Government of Quebec (2021). Available at: https://www.csdepj.gouv.qc.ca/fileadmin/Fichiers_clients/Rapport_final_3_mai_2021/2021_CSDEPJ_Rapport_version_finale_numerique.pdf.
2. Lannes A, Bui E, Arnaud C, Raynaud J-P, Revet A. Preventive interventions in offspring of parents with mental illness: A systematic review and meta-analysis of randomized controlled trials. Psychol Med. (2021) 51(14):2321–36. doi: 10.1017/S0033291721003366
3. Ministère de la Santé et des Services Sociaux. Plan d’action interministériel en santé mentale 2022-2026 - S’unir pour un mieux-être collectif. Gouvernement du Québec., Quebec, Canada (2022). Available at: https://publications.msss.gouv.qc.ca/msss/fichiers/2021/21-914-14W.pdf.
4. Reupert A, Bee P, Hosman C, van Doesum K, Drost LM, Falkov A, et al. Editorial Perspective: Prato research collaborative for change in parent and child mental health–principles and recommendations for working with children and parents living with parental mental illness. JJ Child Psychol Psychiatry. (2022) 63(3):350–3. doi: 10.1111/jcpp.13521
5. Christesen AMS, Knudsen CK, Fonager K, Johansen MN, Heuckendorff S. Prevalence of parental mental health conditions among children aged 0–16 years in Denmark: A nationwide register-based cross-sectional study. Scandinavian J Public Health. (2021) 50:1124–32. doi: 10.1177/14034948211045462
6. Nordentoft M, Jeppesen P, Thorup AAE. Prevention in the mental health field should be implemented synergically at different levels. World Psychiatry. (2021) 20:230. doi: 10.1002/wps.20856
7. Waldmann T, Stiawa M, Dinc Ü, Saglam G, Busmann M, Daubmann A, et al. Costs of health and social services use in children of parents with mental illness. Child Adolesc Psychiatry Ment Health. (2021) 15:1–11. doi: 10.1186/s13034-021-00360-y
8. Weissman MM, Wickramaratne P, Gameroff MJ, Warner V, Pilowsky D, Kohad RG, et al. Offspring of depressed parents: 30 years later. Am J Psychiatry. (2016) 173:1024–32. doi: 10.1176/appi.ajp.2016.15101327
9. Thanhäuser M, Lemmer G, de Girolamo G, Christiansen H. Do preventive interventions for children of mentally ill parents work? Results of a systematic review and meta-analysis. Curr Opin Psychiatry. (2017) 30:283–99. doi: 10.1097/YCO.0000000000000342
10. Villatte A, Piché G, Benjamin S. Perceived support and sense of social belonging in young adults who have a parent with a mental illness. Front Psychiatry. (2022) 12:793344. doi: 10.3389/fpsyt.2021.793344
11. Villatte A, Piché G, Habib R. Comment soutenir la résilience des jeunes en transition vers l’âge adulte qui ont un parent atteint d’un trouble mental? Ce qu’en pensent les jeunes concernés. Int J Child Adolesc Resilience/Revue internationale la résilience Des enfants Des adolescents. (2021) 8:62–79. doi: 10.7202/1077723ar
12. Cudjoe E, Tam CHL, Effah D, Amegashie EF, Tweneboah AO. Living with parental mental illness is like a roller coaster: Reflections on children’s lifeworld in the family setting. J Clin Nurs. (2023) 32:3516–27. doi: 10.1111/jocn.16417
13. Radley J, Barlow J, Johns LC. A family perspective on parental psychosis: An interpretative phenomenological analysis study. Psychol Psychother: Theory Res Pract. (2023) 96:347–63. doi: 10.1111/papt.12443
14. Östman M. Interviews with children of persons with a severe mental illness—Investigating their everyday situation. Nordic J Psychiatry. (2008) 62(5):354–9. doi: 10.1080/08039480801960065
15. Hughes K, Lowey H, Quigg Z, Bellis MA. Relationships between adverse childhood experiences and adult mental well-being: results from an English national household survey. BMC Public Health. (2016) 16:1–11. doi: 10.1186/s12889-016-2906-3
16. Harries CI, Smith DM, Gregg L, Wittkowski A. Parenting and serious mental illness (SMI): A systematic review and metasynthesis. Clin Child Family Psychol Rev. (2023) 26(2):303–42. doi: 10.1007/s10567-023-00427-6
17. Clément M, Piché G, Villatte A. Symptômes dépressifs vécus par les parents dans la population générale: État des travaux québécois et canadiens. [Depressive symptoms experienced by parents in the general population: Status of work in Quebec and Canada.]. Can J Behav Science/Revue Can Des Sci du comportement. (2022) 54:107–20. doi: 10.1037/cbs0000298
18. Maybery D, Reupert A. The number of parents who are patients attending adult psychiatric services. Curr Opin Psychiatry. (2018) 31:358–62. doi: 10.1097/YCO.0000000000000427
19. Foster K, Goodyear M, Grant A, Weimand B, Nicholson J. Family-focused practice with EASE: A practice framework for strengthening recovery when mental health consumers are parents. Int J Ment Health Nurs. (2019) 28:351–60. doi: 10.1111/inm.12535
20. Piché G, Villatte A, Habib R. Les meilleures pratiques préventives ciblant les enfants, adolescents et jeunes adultes vivant avec un parent ayant un trouble mental. In: Trouble mental chez le parent: enjeux familiaux et implications cliniques. Presses de l’Université Laval, Quebec, Canada (2021). p. 315–41.
21. Mottaghipour Y, Bickerton A. The pyramid of family care: a framework for family involvement with adult mental health services. Aust E-Journal Advancement Ment Health. (2005) 4:210–7. doi: 10.5172/jamh.4.3.210
22. MacCourt P. National guidelines for a comprehensive service system to support family caregivers of adults with mental health problems and illnesses (2013). Available online at: https://policycommons.net/artifacts/1189569/national-guidelines-for-a-comprehensive-service-system-to-support-family-caregivers-of-adults-with-mental-health-problems-and-illnesses/1742693/.
23. Piché G, Villatte A, Bourque S. Trouble mental chez le parent: Enjeux familiaux et implications cliniques. Presses de l’Université Laval, Quebec, Canada (2021).
24. Falkov A, Goodyear M, Hosman CM, Biebel K, Skogøy BE, Kowalenko N, et al. A systems approach to enhance global efforts to implement family-focused mental health interventions. Child Youth Serv. (2016) 37:175–93. doi: 10.1080/0145935X.2016.1104104
25. Foster K, Maybery D, Reupert A, Gladstone B, Grant A, Ruud T, et al. Family-focused practice in mental health care: An integrative review. Child Youth Serv. (2016) 37:129–55. doi: 10.1080/0145935X.2016.1104048
26. Organisation mondiale de la Santé. Personnels de santé. S’engager pour la santé: plan d’action quinquennal pour l’emploi en santé et la croissance économique inclusive, (2017-2021) (A74/12). Rapport du Directeur général, Geneva, Switzerland (2021). Available at: https://apps.who.int/iris/bitstream/handle/10665/357977/A74_12-fr.pdf?sequence=1.
27. Wahlbeck K. Public mental health: the time is ripe for translation of evidence into practice. World Psychiatry. (2015) 14:36–42. doi: 10.1002/wps.20178
28. Maybery D, Goodyear M, O’Hanlon B, Cuff R, Reupert A. Profession differences in family focused practice in the adult mental health system. Family Process. (2014) 53:608–17. doi: 10.1111/famp.12082
29. Nicholson J, Reupert A, Grant A, Lees R, Maybery D, Mordoch E, et al. The policy context and change for families living with parental mental illness. In: Parental psychiatric disorder: Distressed parents and their families, Vol. 3. Cambridge University Press, Cambridge, UK (2015). p. 354–64.
30. Eckardt JP. Barriers to WHO Mental Health Action Plan updates to expand family and caregiver involvement in mental healthcare. Gen Psychiatry. (2022) 35(2):e100784. doi: 10.1136/gpsych-2022-100784
31. Lauritzen C, Reedtz C, Rognmo K, Nilsen MA, Walstad A. Identification of and support for children of mentally ill parents: a 5 year follow-up study of adult mental health services. Front Psychiatry. (2018) 9:507. doi: 10.3389/fpsyt.2018.00507
32. Reedtz C, Jensaas E, Storjord T, Kristensen KB, Lauritzen C. Identification of children of mentally Ill patients and provision of support according to the Norwegian health legislation: a 11-year review. Front Psychiatry. (2022) 12:815526. doi: 10.3389/fpsyt.2021.815526
33. Maybery D, Reupert A. Parental mental illness: A review of barriers and issues for working with families and children. J Psychiatr Ment Health Nurs. (2009) 16:784–91. doi: 10.1111/j.1365-2850.2009.01456.x
34. Eassom E, Giacco D, Dirik A, Priebe S. Implementing family involvement in the treatment of patients with psychosis: a systematic review of facilitating and hindering factors. BMJ Open. (2014) 4:e006108. doi: 10.1136/bmjopen-2014-006108
35. Landeweer E, Molewijk B, Hem MH, Pedersen R. Worlds apart? A scoping review addressing different stakeholder perspectives on barriers to family involvement in the care for persons with severe mental illness. BMC Health Serv Res. (2017) 17:1–10. doi: 10.1186/s12913-017-2213-4
36. Gregg L, Adderley H, Calam R, Wittkowski A. The implementation of family-focused practice in adult mental health services: A systematic review exploring the influence of practitioner and workplace factors. Int J Ment Health Nurs. (2021) 30:885–906. doi: 10.1111/inm.12837
37. Lauritzen C, Reedtz C. Support for children of service users in Norway. Ment Health Pract. (2013) 16(10):12–18. doi: 10.7748/mhp2013.07.16.10.12.e875
38. Grant A, Reupert A. The impact of organizational factors and government policy on psychiatric nurses’ family-focused practice with parents who have mental illness, their dependent children, and families in Ireland. J Family Nurs. (2016) 22:199–223. doi: 10.1177/1074840716643770
39. Maybery D, Goodyear M, Reupert A, Grant A. Worker, workplace or families: What influences family focused practices in adult mental health? J Psychiatr Ment Health Nurs. (2016) 23:163–71. doi: 10.1111/jpm.12294
40. Skogøy BE, Sørgaard K, Maybery D, Ruud T, Stavnes K, Kufås E, et al. Hospitals implementing changes in law to protect children of ill parents: a cross-sectional study. BMC Health Serv Res. (2018) 18:1–11. doi: 10.1186/s12913-018-3393-2
41. Goodyear M, Maybery D, Reupert A, Allchin R, Fraser C, Fernbacher S, et al. Thinking families: A study of the characteristics of the workforce that delivers family-focused practice. Int J Ment Health Nurs. (2017) 26:238–48. doi: 10.1111/inm.12293
42. Grant A, Reupert A, Maybery D, Goodyear M. Predictors and enablers of mental health nurses’ family-focused practice. Int J Ment Health Nurs. (2019) 28:140–51. doi: 10.1111/inm.12503
43. Skogøy BE, Ogden T, Weimand B, Ruud T, Sørgaard K, Maybery D. Predictors of family focused practice: Organisation, profession, or the role as child responsible personnel? BMC Health Serv Res. (2019) 19:1–13. doi: 10.1186/s12913-019-4553-8
44. Leonard R, Linden M, Grant A. Predictors of family focused practice among health visitors: A mixed methods study. J Adv Nurs. (2020) 76:1255–65. doi: 10.1111/jan.14310
45. Rose J, Hewitt B. Does part-time employment status really reduce time pressure? J Sociology. (2019) 55:366–88. doi: 10.1177/1440783318800822
46. Leake R, Rienks S, Obermann A. A deeper look at burnout in the child welfare workforce. Hum Service Organizations: Manag Leadership Governance. (2017) 41:492–502. doi: 10.1080/23303131.2017.1340385
47. Tungpunkom P, Maybery D, Reupert A, Kowalenko N, Foster K. Mental health professionals’ family-focused practice with families with dependent children: a survey study. BMC Health Serv Res. (2017) 17:818. doi: 10.1186/s12913-017-2761-7
48. Skogøy BE, Maybery D, Ruud T, Sørgaard K, Peck GC, Kufås E, et al. Differences in implementation of family focused practice in hospitals: a cross-sectional study. Int J Ment Health Syst. (2018) 12:1–11. doi: 10.1186/s13033-018-0256-5
49. Piché G, Villatte A, Clément M-È, Morin M-H, Fournier-Marceau M, Maybery D, et al. Pratiques centrées sur la famille chez les professionnels en santé mentale adulte : Un portrait de la situation au Québec. Rev Santé Mentale au Québec. (2023) 48(2):121–50. doi: 10.7202/1109836ar
50. Lauritzen C, Reedtz C, Van Doesum K, Martinussen M. Factors that may facilitate or hinder a family-focus in the treatment of parents with a mental illness. J Child Family Stud. (2015) 24:864–71. doi: 10.1007/s10826-013-9895-y
51. Tchernegovski P, Hine R, Reupert A, Maybery D. Adult mental health clinicians’ perspectives of parents with a mental illness and their children: single and dual focus approaches. BMC Health Serv Res. (2018) 18:1–10. doi: 10.1186/s12913-018-3428-8
52. Yao H, Guan L, Zhou T, Zhang C, Pan Y, Han J, et al. Factors that influence family-focused practice in Chinese mental health workers: A cross-sectional survey. J Psychiatr Ment Health Nurs. (2023) 30(6):1216–30. doi: 10.1111/jpm.12950
53. Houlihan D, Sharek D, Higgins A. Psychiatric nurses’ attitudes towards children visiting their parents in psychiatric inpatient units. Irish J Psychol Med. (2013) 30:261–9. doi: 10.1017/ipm.2013.50
54. Fan W, Yan Z. Factors affecting response rates of the web survey: A systematic review. Comput Human Behav. (2010) 26(2):132–9. doi: 10.1016/j.chb.2009.10.015
55. Maybery D, Goodyear M, Reupert A. The family-focused mental health practice questionnaire. Arch Psychiatr Nurs. (2012) 26:135–44. doi: 10.1016/j.apnu.2011.09.001
56. Piché G, Villatte A, Fournier-Marceau M, Clément M-È, Morin M-H, Maybery D, et al. Psychometric proprieties of the french version of the family-focused mental health practice questionnaire (FFMHPQ). Eur Rev Appl Psychol. (2024) 74:1–12. doi: 10.1016/j.erap.2023.100969
57. Beaton D, Bombardier C, Guillemin F, Ferraz MB. Recommendations for the cross-cultural adaptation of health status measures Vol. 12. New York: American Academy of Orthopedic Surgeons (2002) p. 1–9. doi: 10.1037/0033-2909.107.2.238
58. Maybery D, Goodyear M, Reupert A. Manual for the family-focused mental health practice questionnaire (2017) Second edition. Unpublished manuscript. doi: 10.1037/t63879-000
59. Shah-Anwar S, Gumley A, Hunter S. Mental health professionals’ perspectives of family-focused practice across child and adult mental health settings: A qualitative synthesis. Child Youth Serv. (2019) 40:383–404. doi: 10.1080/0145935X.2019.1591947
60. Reupert A, Foster K, Maybery D, Eddy K, Fudge E. Keeping families and children in mind’: an evaluation of a web‐based workforce resource. Child Fam Soc Work. (2019) 16(2):192–200. doi: 10.1111/j.1365-2206.2010.00731.x
61. Hipp L, Bernhardt J, Allmendinger J. Institutions and the prevalence of nonstandard employment. Socio-Economic Rev. (2015) 13:351–77. doi: 10.1093/ser/mwv002
62. Kretsos L, Livanos I. The extent and determinants of precarious employment in Europe. Int J Manpower. (2016) 37:25–43. doi: 10.1108/IJM-12-2014-0243
63. Allchin B, Goodyear M, O’Hanlon B, Weimand BM. Leadership perspectives on key elements influencing implementing a family‐focused intervention in mental health services. J Psychiatr Ment Health Nurs. (2020) 21(5):25–43. doi: 10.1111/jpm.12615
64. Clément M-É, Dufour S, Gagne M-H, Gilbert S. Prediction of health, education, and psychosocial professionals’ attitudes in favor of parental use of corporal punishment. Child Abuse Negl. (2020) 109:104766. doi: 10.1016/j.chiabu.2020.104766
65. Morin M-H, Bergeron A-S, Levasseur MA, Iyer SN, Roy M-A. Les approches familiales en intervention précoce: repères pour guider les interventions et soutenir les familles dans les programmes d’intervention pour premiers épisodes psychotiques (PPEP). Santé mentale au Québec. (2022) 46:139–59. doi: 10.7202/1088181ar
Keywords: family-focused practice, parenting, parental mental illness, mental health professionals, children of parents with a mental illness, mental health services
Citation: Piché G, Villatte A, Clément M-È, Morin M-H, Maybery D, Reupert A, Richard-Devantoy S and Fournier-Marceau M (2024) Predictors of family-focused practices among mental health workers in Quebec. Front. Psychiatry 15:1380001. doi: 10.3389/fpsyt.2024.1380001
Received: 31 January 2024; Accepted: 15 April 2024;
Published: 13 May 2024.
Edited by:
Lawrence T. Lam, Macau University of Science and Technology, Macao SAR, ChinaReviewed by:
Mark Cheuk-man Tsang, Tung Wah College, Hong Kong SAR, ChinaDavid C. N. Wong, University Grants Committee Secretariat, Hong Kong SAR, China
Copyright © 2024 Piché, Villatte, Clément, Morin, Maybery, Reupert, Richard-Devantoy and Fournier-Marceau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Geneviève Piché, Z2VuZXZpZXZlLnBpY2hlQHVxby5jYQ==