
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 26 July 2024
Sec. Intellectual Disabilities
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1379497
This article is part of the Research Topic Break the Stigma: People with Intellectual Disability View all 7 articles
 Rosalie Power1
Rosalie Power1 Michael David2,3
Michael David2,3 Iva Strnadová4,5
Iva Strnadová4,5 Lauren Touyz2
Lauren Touyz2 Caroline Basckin4
Caroline Basckin4 Julie Loblinzk4,6
Julie Loblinzk4,6 Heather Jolly7Elizabeth Kennedy2
Heather Jolly7Elizabeth Kennedy2 Jane Ussher1
Jane Ussher1 Sally Sweeney7
Sally Sweeney7 Ee-Lin Chang7
Ee-Lin Chang7 Allison Carter8
Allison Carter8 Deborah Bateson2*
Deborah Bateson2*Background: The World Health Organisation’s vision of eliminating cervical cancer as a public health problem is achievable, but elimination must be achieved equitably, including for people with intellectual disability. A better understanding of cervical screening within the context of the lives of people with intellectual disability is needed. This study systematically reviewed research on the rates of cervical screening participation among people with intellectual disability, and facilitators and barriers that affect participation.
Method: Six electronic databases were systematically searched: MEDLINE, CINAHL, Scopus, PsycINFO, Embase and Pro-Quest Central Social Sciences Collection. Empirical studies published between 1986 and 2023, in English language peer-reviewed journals were eligible for inclusion. Further articles were identified through forward and backward citation tracking, and hand-searching the index lists of two key journals. Two authors screened the studies, extracted the data and collated study outcomes using a standardised software program. A meta-analysis was performed using the DerSimonian and Laird method to estimate pooled effect sizes in prevalence rates and odds ratios (ORs). The socio-ecological model (SEM) was used as a framework to thematically analyse facilitators and barriers impacting participation in cervical screening.
Results: Sixty-three articles met the inclusion criteria. Of these, 42 reported on rates of cervical screening participation and 24 reported on facilitators or barriers to cervical screening for people with intellectual disability. Overall, the studies reported a screening prevalence of 35% (95% CI: 26% to 45%), indicating that just over a third of people with intellectual disability have had cervical screening. The pooled odds ratio of 0.30 (95% CI: 0.23 to 0.41) indicated that people with intellectual disability are significantly less likely to have a cervical screening test compared with people without intellectual disability. Most studies examined individual and interpersonal factors impacting cervical screening. These included: (i) fear and anxiety among people with intellectual disability, (ii) misassumptions preventing screening participation, (iii) the role of support people, (iv) the need for education, (v) accessible information, and time to prepare for screening, (vi) patient-provider communication including challenges obtaining informed consent, and (vii) healthcare provider lack of confidence.
Conclusion: Future research, policy and practice efforts must address barriers to cervical screening participation among people with intellectual disability and ensure these efforts are co-produced and community-led. This is critical to ensuring equity in global and local efforts to eliminate cervical cancer.
Cervical cancer is a major public health problem and is the fourth leading cause of cancer incidence and death in women worldwide (1). However, cervical cancer can be prevented (2, 3), and it can be cured if detected at an early stage and treated effectively (3). The primary cause of cervical cancer is persistent infection with oncogenic types of the human papilloma virus (HPV) (4), a common viral infection of the genital tract, transmitted through sexual contact. The three pillars of prevention include HPV vaccination, cervical screening with a high-performance test, and treatment of pre-cancerous lesions (5). Countries with organised screening programs are increasingly switching from cytology-based screening with Pap smears to primary HPV screening (6). People with oncogenic HPV detected on their screening test can then either undergo surveillance with repeat testing or be referred for colposcopy and, if necessary, be treated for pre-cancerous lesions. Remarkable progress has been made in reducing cervical cancer-related diagnoses and mortality through these population-based screening programs, resulting in up to a 92% increase in survival rates (7). However, there are disparities in participation in cancer screening programs.
In 2020, the World Health Organisation (WHO) launched a Global Strategy to accelerate the elimination of cervical cancer as a public health problem (5). To be successful, elimination must be achieved equitably, including for cisgender women, trans and non-binary people with intellectual disability. Globally, 78 million people (1% of the population) have intellectual disability (8). This population are reported to have significantly poorer health and healthcare experiences compared with people without disability (9), including being twice as likely to die prematurely from preventable causes (10, 11) including cervical cancer (12) and six times more likely to experience barriers accessing healthcare services (13). Both the Disability (14) and Reproductive Justice Movements (15) have long recognised that structural and systemic issues, including negative social discourse about people with disability, impact access to healthcare and that multiple, intersecting forms of oppression deny people with disability the right to make decisions about their bodies (16). Barriers include lack of accessibility among services (including financial and transport issues) (13), communication issues (17), low levels of education including exclusion from sex education and information (18), and healthcare provider stigmatising (19) and discriminatory (20) attitudes and lack of knowledge (19).
People with intellectual disability are reported to have unique risk factors for cervical cancer, including low participation in HPV vaccination programs (21), and high rates of sexual abuse (22), including child sexual abuse (23), potentially increasing exposure to HPV. Despite the importance of cervical screening for this population, minimal attention has been paid to the barriers and facilitators of cervical screening. Currently, there are no internationally representative data on cervical screening participation among people with intellectual disability, and most countries lack screening data for this population group, except for those with nationally linked data sets such as Sweden (24). Broader disability research (i.e., focused on people with other forms of disability, including physical disability) has found that women with disability have 0.63 lower odds of participating in cervical screening (25), and are more likely to receive a later diagnosis of cervical cancer, less treatment, and to have higher mortality rates, compared with women without any disability (26). As findings are potentially worse for people with intellectual disability (11), there is a need to understand cervical screening participation rates for this group to inform prevention, policy and practice. There is also a need to understand facilitators and barriers that impact screening uptake, to enable long-term systemic change (15) for people with intellectual disability to equitably engage in cervical screening programs. To address these needs, our research questions were:
1. What percentage of people with intellectual disability participate in cervical screening?
2. What is the likelihood of people with intellectual disability participating in cervical screening compared with people without intellectual disability?
3. What are the facilitators and barriers that influence participation in cervical screening by people with intellectual disability?
An Easy Read version of this paper is available in the Supplementary Material.
This systematic review is part of ScreenEQUAL, a 3-year Australian Government National Health and Medical Research Council (NHMRC) funded multifaceted, inclusive study, using a co-production framework (27, 28), to improve cervical screening in people with intellectual disability. Our multidisciplinary team included social scientists, clinician researchers, non-government organisation (NGO) health promotion experts and includes an advisory group of people with intellectual disability and cervical screening healthcare providers.
This review was conducted according to a pre-defined protocol, registered with the International Prospective Register of Systematic Reviews (PROSPERO CRD42023393799). It includes a meta-analysis, which involves using statistical techniques to synthesise the data from several studies into a single quantitative estimate or summary effect size (29). The methods used for the review align with Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (30).
Predefined inclusion criteria were articles that: (a) report rates, facilitators or barriers to cervical screening participation among people with intellectual disability. Articles were considered in scope if they defined their sample as being people with intellectual disability, learning disability, developmental disability/disorder or discussed a specific intellectual disability diagnosis such as Down Syndrome; (b) empirical research papers published in peer-reviewed English language journals; (c) published between 1986 to 2023. The year 1986 was selected to align with the development of the first WHO guidelines for cervical screening (31). Quantitative, qualitative and mixed-methods papers were included. Review articles, opinion pieces and grey literature were excluded. Studies were also excluded if they did not report specific results about cervical screening (i.e., if results about cervical screening could not be distinguished from results about other cancer screening programs) or if they did not report results specifically about participants with intellectual disability (i.e., if results of participants with intellectual disability could not be distinguished from the results of participants with other disabilities).
Six electronic databases, MEDLINE (OVID), Cumulative Index to Nursing and Allied Health (CINAHL) (EBSCO), Scopus (Elsevier), PsycINFO (EBSCO), Embase (OVID), ProQuest Central Social Sciences Collection (ProQuest), were searched between January and February 2023. The search strategy focused on terms and synonyms for intellectual disability (such as learning disability and developmental disorders), specific intellectual disability diagnoses (such as Down Syndrome) and cervical screening (such as Papanicolaou test, cervical smear, early detection of cancer) (Supplementary Table 1). Medical subject heading (MeSH) terms and free text terms were combined. Further articles were identified through forward and backward citation tracking of the included articles, and hand-searching the index lists of two key international peer-review journals that focus on intellectual disability research, Journal of Applied Research in Intellectual Disabilities and Journal of Intellectual Disability Research.
Study selection is shown in Figure 1. A total of 7,762 records were identified from the searches and 2,180 duplicates were removed. Two reviewers (RP, LW) independently screened the title and abstract of articles for eligibility and removed a further 5,445 articles. The full text of the shortlisted articles was then examined against the eligibility criteria by the two reviewers resulting in a further 69 articles being excluded. Disagreements between reviewers were resolved through discussion with the senior author (DB) until a consensus was reached. Inter-rater reliability was calculated using Cohen’s kappa, with the average score being very high, K=0.96. The search strategy was re-run in August 2023 to identify studies published since the original search. A further four studies were identified, resulting in a total of 63 articles included in this review.
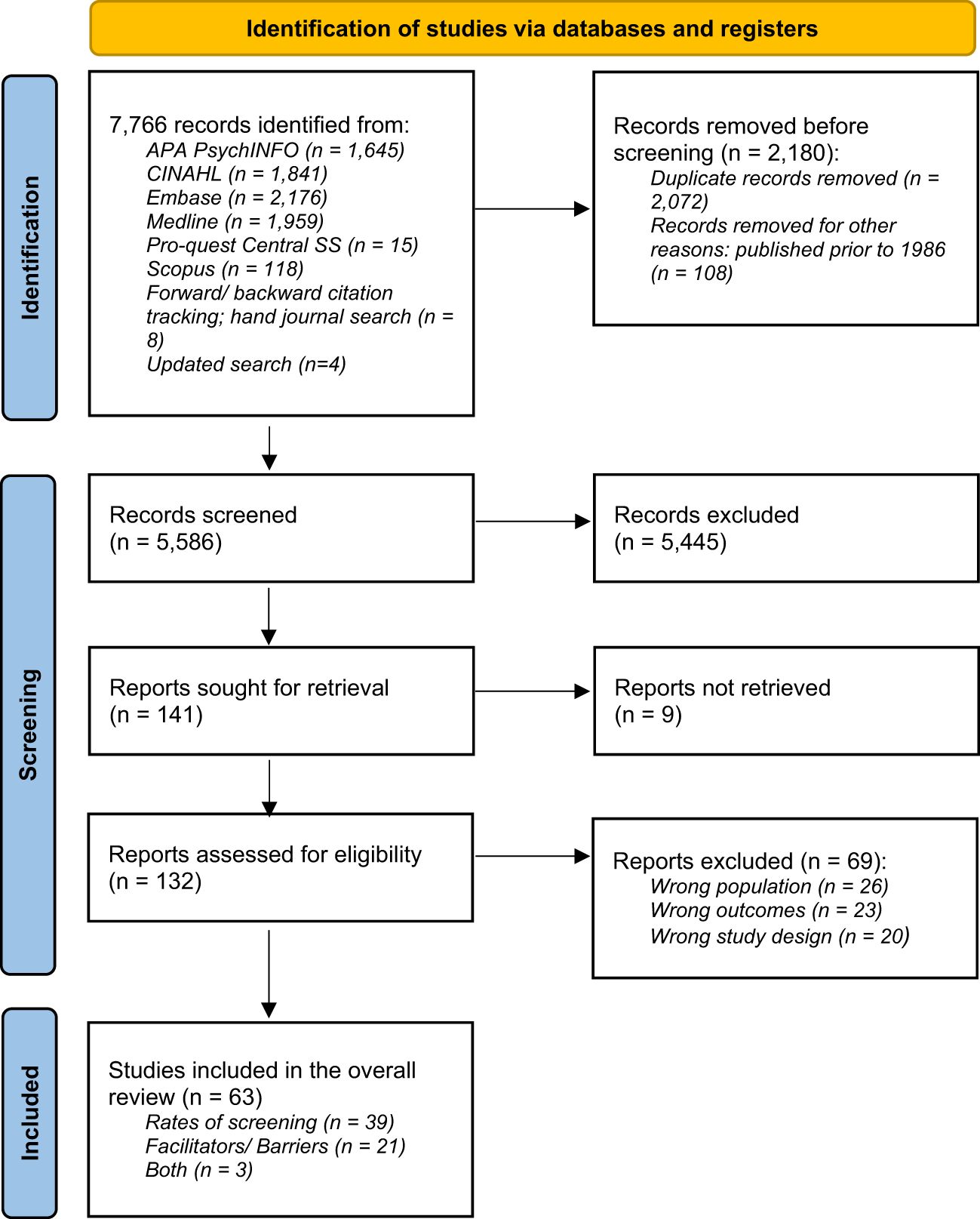
Figure 1 PRISMA chart.
The Standard Quality Assessment Criteria for Evaluating Primary Research Papers From Various Fields (32) was used to assess the quality of each study. Two authors (RP, IS) independently reviewed each study and assigned scores of yes (2), partial (1), no (0) and N/A (1) for each quality assessment criteria (14 items for quantitative and 10 for qualitative studies). Disagreements between reviewers were resolved through discussion until a consensus was reached. A total score was then derived for each study, expressed a decimal between zero (lowest possible quality) and one (highest possible quality) indicating the strength of evidence and any concern of bias. For mixed methods studies, quantitative and qualitative scores were calculated, with the higher value used to define the study’s overall quality. A quality threshold of 0.55 was set to exclude the lowest quality bracket to ensure that questionable evidence and findings were not included (32). Interrater agreement for the quality assessment achieved a rating of “almost perfect” (33)(p.3) using Cohen’s Linearly Weighted Kappa (κ) for each criterion in each study. This was calculated using Vassar Stats online calculator (34), which yielded a result of κ=0.9781 (observed kappa).
This meta-analysis was performed by calculating pooled screening prevalence and odds ratios (ORs) for studies with comparators. For each, random effects modelling was applied to calculate effect sizes and 95% confidence intervals (95% CI) calculated using the DerSimonian and Laird method (35) and presented visually by forest plots. Prevalence rates were transformed using the Freeman-Tukey double arcsine method with the corresponding back-transformation equation (36, 37). For ORs, and when reported, the adjusted OR for screening participation from an individual study was included. In comparative studies where this was not the case, unadjusted ORs with corresponding standard errors were calculated. Statistical heterogeneity was quantified by the I-squared statistic and tested using Cochran’s Q statistic (38, 39). To visually and analytically investigate the source of heterogeneity, subgroup analysis and meta-regression were undertaken, respectively. In addition, for a time-cumulative meta-analyses, studies were arranged in chronological order, with multiple meta-analyses being performed by grouping studies by year. Publication bias, failure to publish the results of a study based on the direction or strength of the study findings, was assessed using Egger’s regression test (40). All statistical tests were two-sided, and a p-value of less than 0.05 was considered statistically significant. All analyses were performed using Stata Version 18.0 (Stata Corporation, College Station, TX, USA).
Thematic analysis was conducted on the included data about facilitators or barriers to cervical screening for people with intellectual disability. The Socio-ecological Model (41) (SEM) was used as a guiding framework for this analysis. The model provides a multi-level lens for understanding facilitators and barriers to cervical screening as it recognises that health behaviours are shaped not only by an individual’s characteristics but also by social and environmental influences (41). Initially, data were extracted from the included studies by one author (EK), into a standardised software analysis program (Covidence) (42). A second author checked this for completeness and accuracy and disagreements were resolved through discussion (RP). A pre-defined data extraction template was used to organise information using the five levels of the SEM: (1) individual, such as attitudes and beliefs and sociodemographic characteristics; (2) interpersonal, such as healthcare provider communication and access to support; (3) organisational, such as service provider training, collaboration and accessibility; (4) community, such as promotion of, and education about, cervical screening; and, (5) policy, such as inclusion and exclusion in organised cervical cancer screening programs. Each level included the heading ‘other’, to allow recording of unanticipated facilitators or barriers. In reporting results, community and policy-level facilitators and barriers were presented together.
The extracted data were read and re-read to identify patterns, similarities, and differences across the studies. Data under each heading were summarised to facilitate the identification and development of themes, with the broader research team consulted on the interpretation and reporting of data. Different perspectives on the same data by the multi-disciplinary researchers helped the team reflect on and develop themes. This iterative process produced a textual description highlighting the common facilitators and barriers to cervical screening among individuals with intellectual disability. Analysing facilitators and barriers in the interconnected levels of the SEM enabled identification of knowledge and gaps in the existing research to develop recommendations for effective interventions and future research to optimise cervical screening in people with intellectual disability.
This review encompasses research conducted in various countries, where diverse terminology is used to refer to people with cognitive disabilities - including intellectual disability, learning disabilities, learning difficulties, and developmental disabilities. For instance, in Ireland, Australia, and New Zealand, the term “intellectual disability” is used, while in the United Kingdom, the terms “learning difficulties” or “learning disabilities” are used. Our team of authors consists of academic researchers from Australia, who have extensive experience in conducting inclusive research. After thorough discussions within our team and considering the cross-cultural nature of this article, we have decided to use the term ‘people with intellectual disability’ (43).
A total of 63 articles met the inclusion criteria, reporting on rates of cervical screening participation (n=39), facilitators or barriers to cervical screening (n=21) or both (n=3). Studies were published between 1994 to 2023 (no studies published between 1986 to 1994 were identified) and were all conducted in high-income countries (44), see Table 1. Over a quarter of studies (n=16, 25.4%) focused on cervical cancer screening only. The remainder examined cervical screening alongside other cancer screening programs (i.e., breast or bowel) or as part of broader healthcare research including health behaviour change interventions. Studies sought data from people with intellectual disability (n=15, 23.8%), family members (n=8, 12.7%), paid support workers (n=7, 11.7%) and health providers (n=8, 12.7%), or accessed data from medical records or data linkage (n=38, 60.3%). Standard Quality Assessment scores ranged from 0.75 to 1 (Supplementary Table 2).
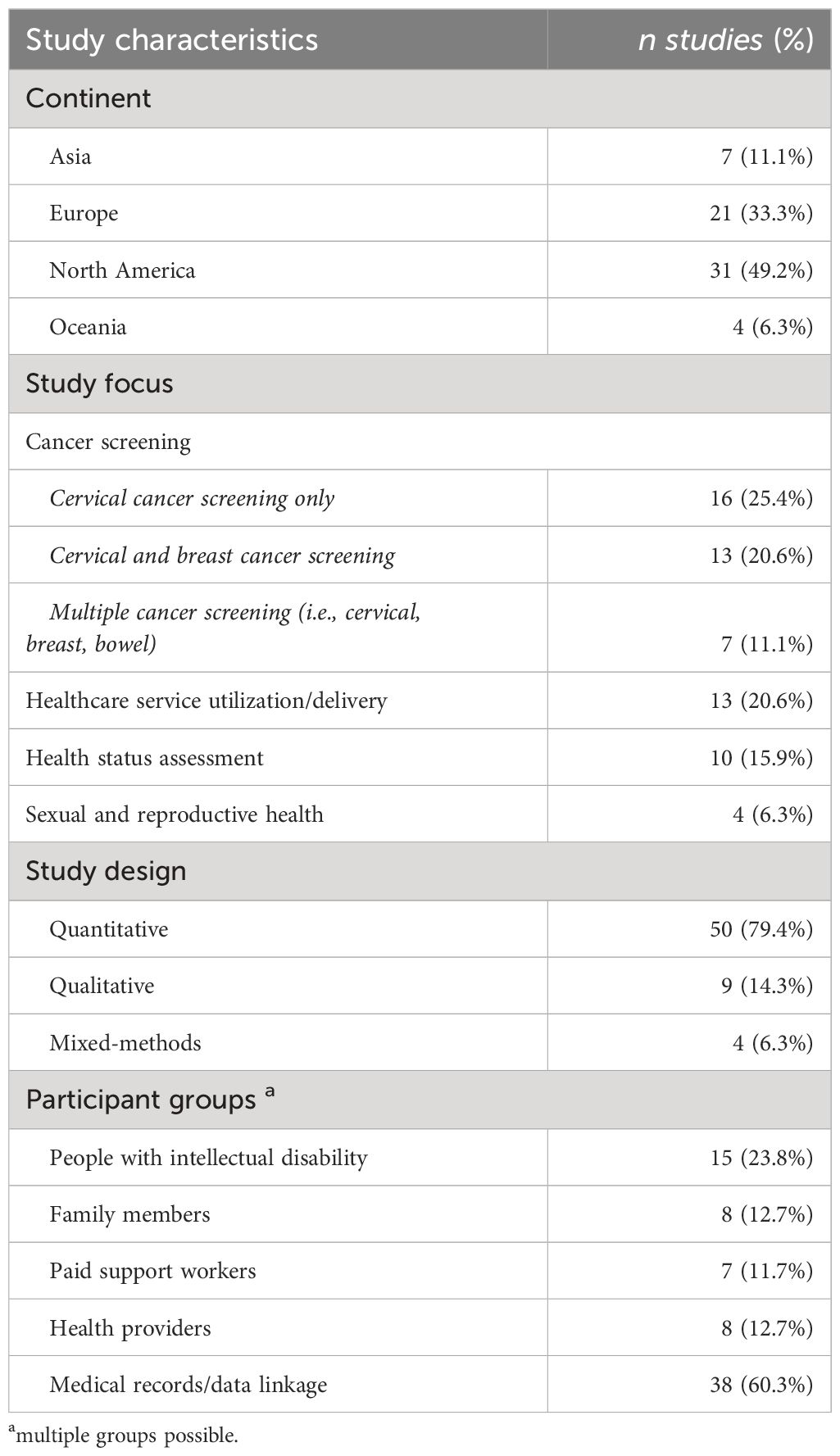
Table 1 Study characteristics (all included studies n=63).
Of the 42 studies included in the meta-analysis, 41 reported the prevalence of cervical screening among people with intellectual disability, with a total of 15,629,260 participants. Overall, the studies reported a screening prevalence of 35% (95% CI: 26% to 45%), indicating that just over one-third of eligible people with intellectual disability participated in cervical screening (see Figure 2). To assess heterogeneity (variability) among studies, a visual subgroup analysis by Year of Publication and Continent was performed (Supplementary Figures 1, 2). For the Year of Publication, the only pairing displaying a noticeable difference was the comparison between studies published from 1996 to 2002 (Screening Prevalence: 18%; 95% CI: 11% - 26%) and studies published from 2017 to 2023 (34%; 28% - 40%). When estimates were pooled across four continents, noticeable differences were also seen between studies published in North America (53%; 44% - 62%) and the three other continents (Asia, Europe and Oceania). A multivariable meta-regression (Supplementary Table 3) identified significantly higher rates of screening in North America than the other continents (p<0.01), thereby confirming Continent to be a source of study heterogeneity. However, the Year of Publication was not seen to be a source of study heterogeneity, as its effect was not statistically significant (p=0.31), Additionally, there was no evidence of publication bias, with Egger’s test being non-significant (p=0.70).
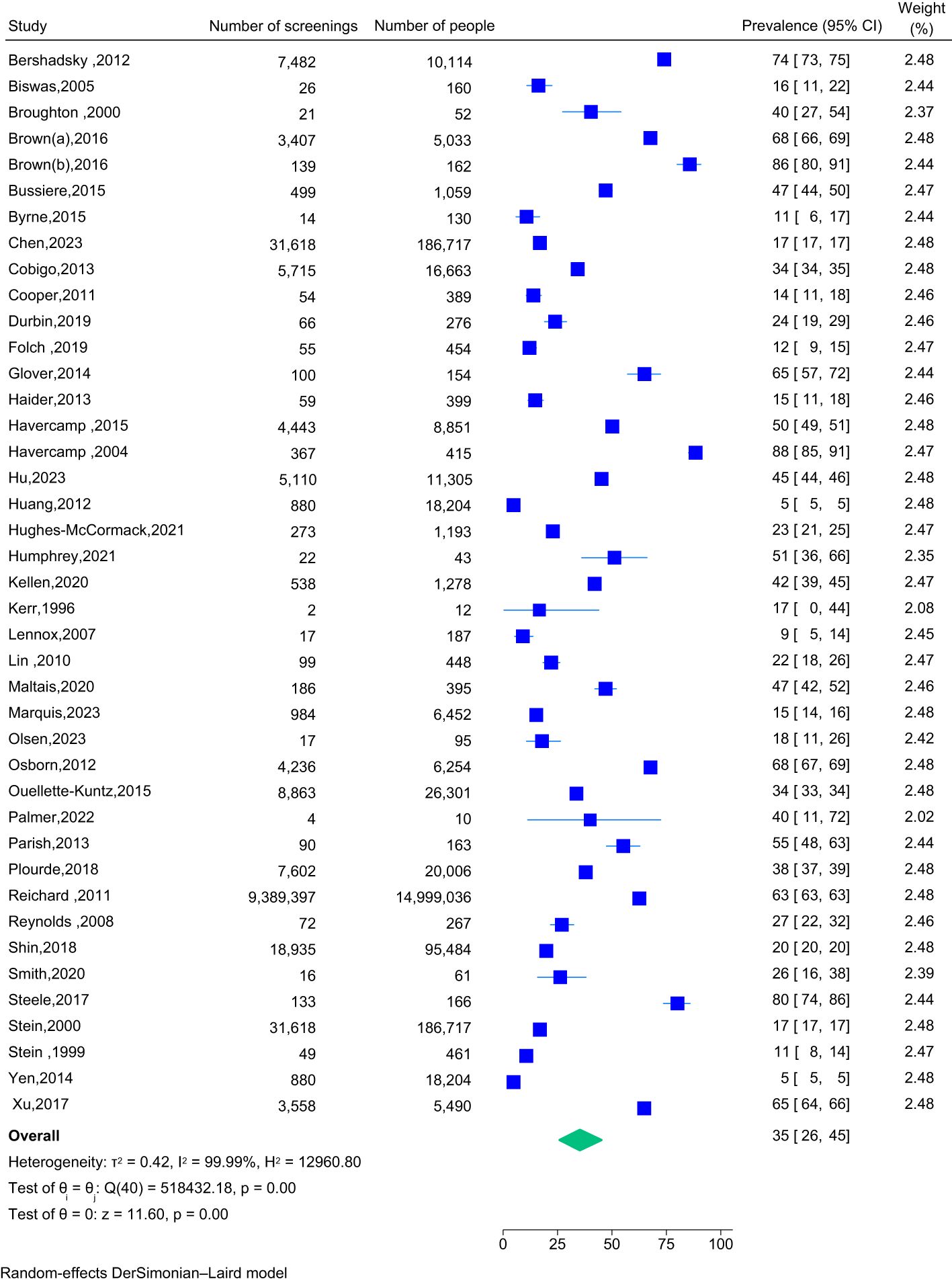
Figure 2 Forest plot for cervical screening prevalence for people with intellectual disability (n=41 studies).
Eighteen studies used a randomised controlled trial design with an appropriate control group to compare cervical screening participation of people with intellectual disability with participation by those without intellectual disability. The overall pooled OR of 0.30 (95% CI: 0.23 to 0.41) indicates that people with intellectual disability are significantly less likely to participate in cervical screening, compared with people without intellectual disability (Figure 3). Furthermore, whilst a time-cumulative forest plot (Figure 4) shows an upward trend in ORs from 0.18 (0.10 - 0.31) in 2004 to 0.29 (0.22 - 0.39) in 2013, over the past 10 years, the pooled OR has plateaued, increasing minimally to 0.30 (0.23 - 0.41). An analytical assessment of heterogeneity across Type of Analysis, Continent and Year of Publication by a multivariable meta-regression (Supplementary Table 4) confirmed the effects of Type of Analysis (p=0.45) and Year of Publication (p=0.97) as being non-significant. Whilst Oceania studies reported much lower screening rates for people with intellectual disability compared to studies from North America (β=-1.49; 95%CI: -3.37 - 0.40), the overall effect for Continent was also not found to be statistically significant (p=0.42). There was no evidence of publication bias, with Egger’s test being non-significant (p=0.68).
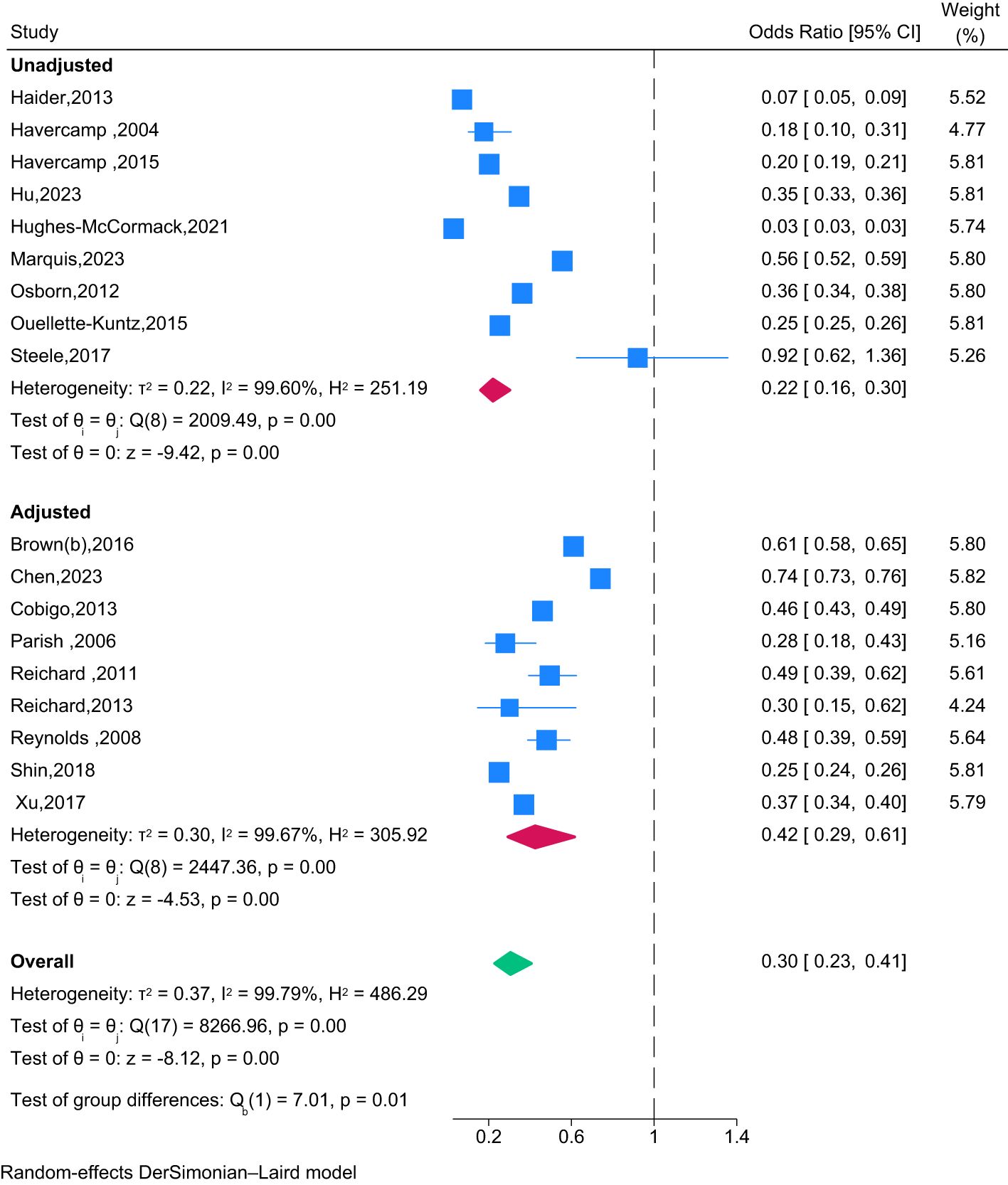
Figure 3 Forest plot of the association between screening participation and intellectual disability compared to those without intellectual disability by type of analysis (unadjusted, adjusted) (n=18 studies).
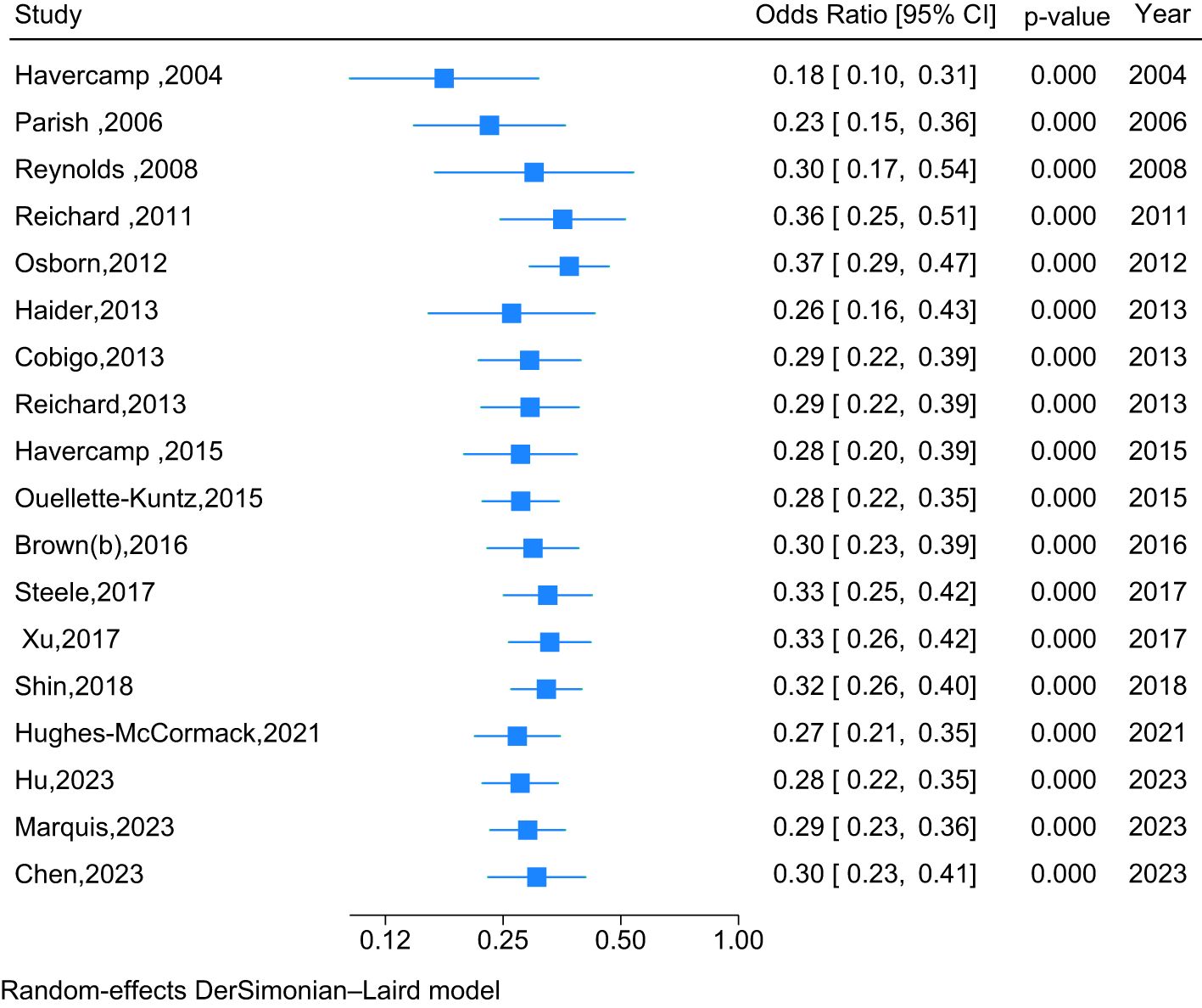
Figure 4 Cumulative forest plot of the association between screening participation and intellectual disability compared to those without intellectual disability, by year of publication (2004 – 2023).
Twenty-four studies examined facilitators or barriers to cervical screening among people with intellectual disability. Included studies used either a qualitative (n=8), quantitative (n=11) or mixed methods approach (n=5). Figure 5 presents facilitators and barriers to cervical screening, grouped by individual, interpersonal, organisational, community and policy-level factors from the Socio-ecological Model (SEM) and Table 2 provides a summary of each of the studies. In the analysis below, we describe how the identified factors were understood to impact cervical screening participation for people with intellectual disability.
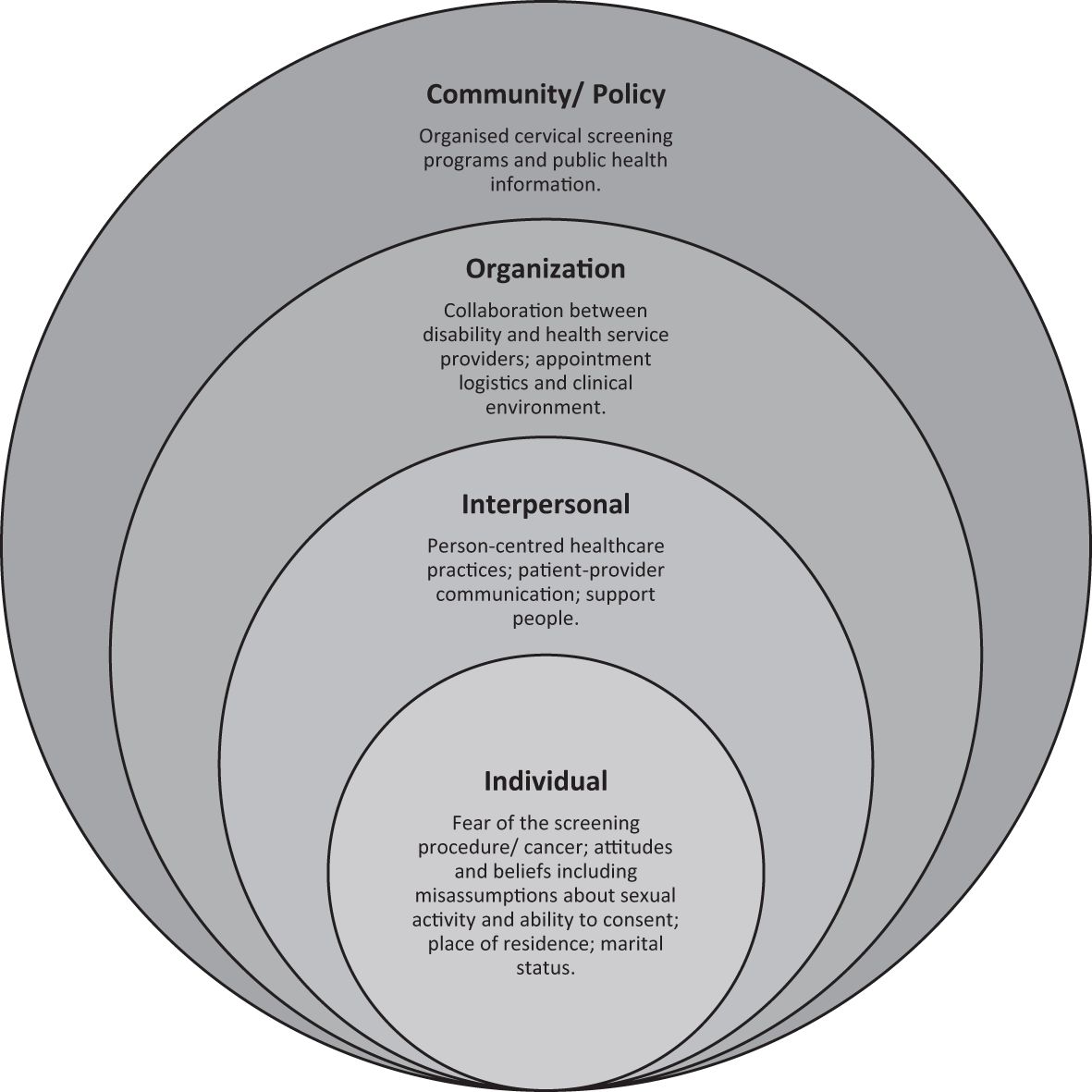
Figure 5 Socio-ecological factors impacting cervical screening participation for people with intellectual disability.
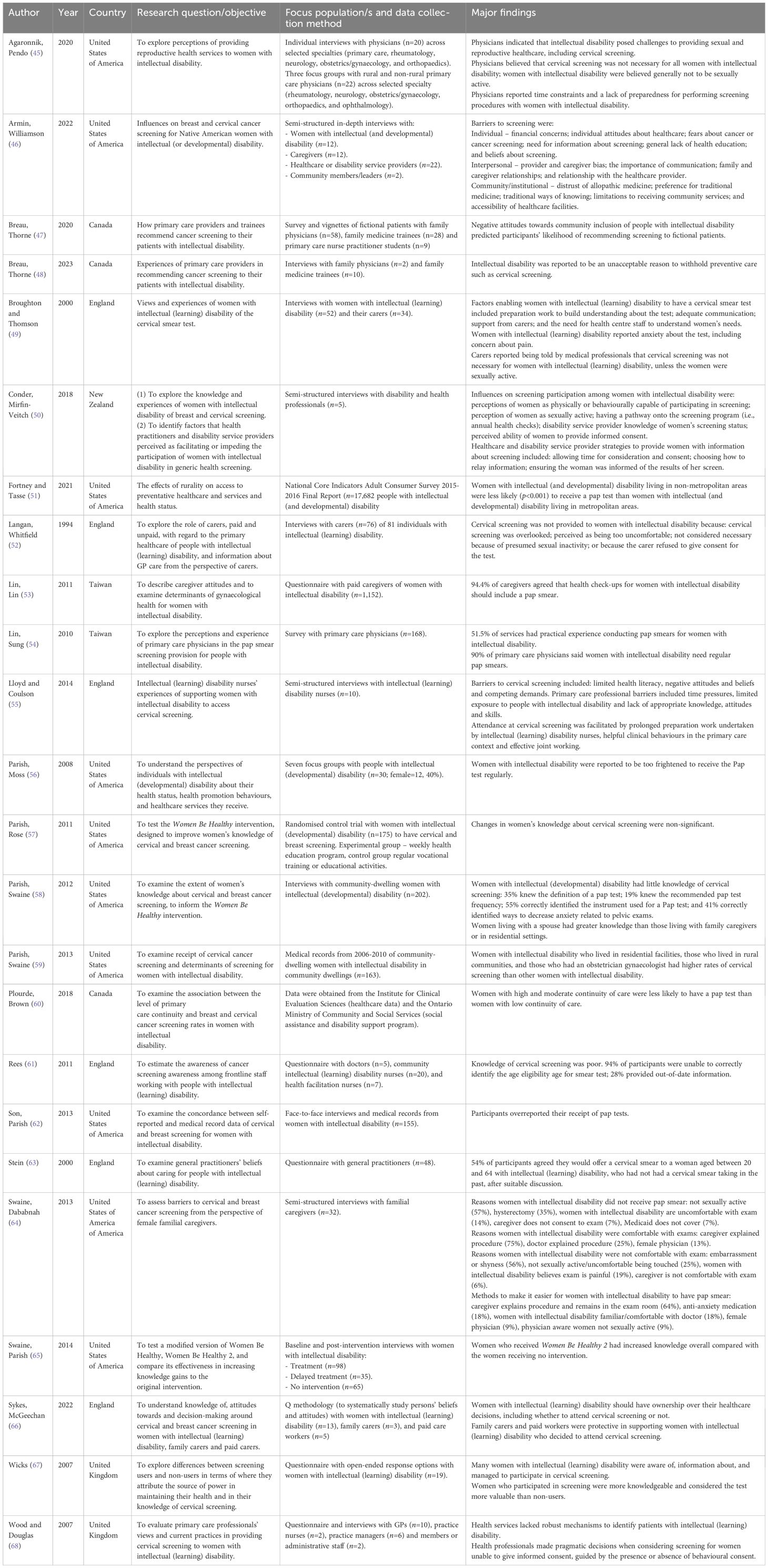
Table 2 Studies reporting barriers or facilitators to cervical screening (n=24).
Numerous studies (46, 49, 52, 55, 56, 64, 67) reported fear and anxiety among people with intellectual disability, regarding cervical screening, with many “too frightened” (56)(p.419) to receive the test. In studies with people who had previously experienced cervical screening, participants used words such as “painful” (49)(p.908) (67)(p.14), “awkward” (49)(p.908) and “scary” (67)(p.14) to describe the test. In one study, a participant with intellectual disability explained, ‘‘I hate Pap smears. They pinch when they are inside of you. I kick and scream when I have to get them.’’ (56)(p.419).
Studies with family members found that women with intellectual disability were often uncomfortable with the screening procedure, due to “general embarrassment or shyness with the private nature of the exam” (64)(p.68) and “because of the women’s lack of sexual experience.” (64)(p.66) Family members also suggested that women with intellectual disability may require anti-anxiety medications or sedatives to tolerate the exam including the use of a speculum (64). Other study participants, including disability and healthcare providers, acknowledged that histories of sexual abuse among people with intellectual disability could be a barrier to screening participation (46).
Research participants frequently reported that people with intellectual disability experienced negative experiences with healthcare providers, such as not being listened to and respected, which impacted their engagement with cervical screening, as explained by an intellectual disability nurse:
[ … ] she [the practice nurse] attempted to do the smear test, the lady couldn’t cope with it and was absolutely screaming and what have you and I just said ‘stop’. I don’t know why but the practice nurse didn’t stop at that point she just tried to carry on. So I intervened and said ‘stop’ so she did and then she was really sort of aggressive to me and mum saying ‘why have you come for this appointment, why have you put this woman through this?’ and tried to blame us. (55)(p. 138).
One study (46) reported that women with intellectual disability might avoid cervical screening due to fear that they could be diagnosed with cancer and that treatment would reduce their ability to live independently.
Most studies (45, 46, 48–50, 52, 55, 60, 61, 63, 64) reported that family members and disability and healthcare providers held misassumptions about the need for people with intellectual disability to have a cervical screening test. Incorrect beliefs included that people with intellectual disability were sexually inactive, precluding cervical screening. For example, in one study, only 54% of doctors said they would offer cervical screening to “a woman aged between 20 and 64 with intellectual disability” who “had not had a cervical smear test taken in the past [ … ], after suitable discussion” (63)(p.13), with most citing sexual inactivity as a principal determinant of their decision. A family member in another study explained, “I do feel that because a person has some sort of intellectual difficulty their sexual life is dismissed. They should have the same screening as any person has.” (52)(p.361) Only one study (46) reported awareness among service providers regarding the high rates of sexual assault experienced by people with intellectual disability. It emphasised the importance of avoiding assumptions about HPV exposure when determining cervical screening eligibility:
Women with disability are some of the highest risk for unwanted sexual assault. And so you can’t assume, you know, that somebody hasn’t been exposed to HPV even if it wouldn’t seem as if they would have had an opportunity to be exposed. (46)(p.8).
Health care providers reportedly made presumptions about the healthcare priorities of patients with intellectual disability such as that the patient’s primary diagnosis presented more pressing need than cervical screening. In one study, a rural woman with intellectual disability stated, “she’s [healthcare provider] more concerned with my disability than anything.” (46) In the same study a disability service provider commented:
For people with disabilities in general, they tend not to get asked about healthcare screening and [are] more likely to be asked about stress and stuff like that. So, women particularly with disability are often assumed not to be sexually active, they never get a sexual history taken. It’s called diagnostic overshadowing … where that primary diagnosis is all the physician can see. (46)(p.5).
Another study found that whilst many healthcare providers said they would “never take a unilateral decision not to invite women with intellectual disability for cervical screening,” (68) (p.88) some providers indicated that “women with severe intellectual disability would only ‘sometimes’ be invited”(p.88). Health care provider misassumptions regarding the importance of cervical screening for patients with intellectual disability and their inconsistencies offering cervical screening for this group, left people with intellectual disability feeling “dismissed, insignificant and overlooked.” (46)(p.6).
Several sociodemographic characteristics were reported to be associated with low participation in cervical screening for people with intellectual disability. Two studies (59, 69) reported that people with intellectual disability living with parents or relatives were significantly less likely to participate in cervical screening than those living in residential facilities as well as those living with parents or relatives being quoted to have “alarmingly limited accurate knowledge”. (59)(p.84) Studies reported mixed findings regarding access to cervical screening by location. One study (51) found that people with intellectual disability living in rural locations were significantly less likely to receive cervical screening compared with people with intellectual disability living in metropolitan locations. Conversely, another study (59) found that people with intellectual disability living in rural areas had a significantly higher likelihood of receiving a Pap test than those living in urban settings. People with intellectual disability who were married or who had tubal ligation surgery were reportedly more likely to have had a cervical screening test compared with people with intellectual disability who were not married or who had not had tubal ligation surgery (54). Other factors reported to be associated with cervical screening included sexual activity; number of sexual partners; pregnancy; and a past history of smoking (49).
Several studies (46, 48, 49, 64, 66) reported that having a support person present (i.e., family members or support worker) was beneficial for people with intellectual disability when undertaking a cervical screening test. People with intellectual disability recommended taking a support person to cervical screening appointments because “having someone with you gives you more confidence.” (49)(p.909) In one study, family members described providing comfort, such as “holding the woman’s hand” (64)(p.69) and “repeating the phrase ‘breathe’ just to keep her calm.” (64)(p.68) Overall, support people highlighted that having good rapport with the person with intellectual disability was crucial for empowering this group to participate in screening and to have a positive experience with the test. A disability service provider explained the factors they considered when selecting staff members to accompany a person with intellectual disability to a cervical screening appointment:
It’s about who has the right rapport, the right demeanour that suits the person … who they feel comfortable with [ … ] There’s no point putting someone on that’s been employed for two weeks to go and take someone … To become familiar with the person … may take up to a 12-month period … especially if you are from a culture where … women’s health screening is not talked about. (50)(p.92).
While most studies reported positive perceptions of support people, one study noted that the “viewpoints [of caregivers] must be considered during the clinical encounter”, suggesting that “the presence of an additional caregiver may make coordination of care more burdensome and thus more difficult to offer cancer screening.” (48) (p.256) Overall, these findings provide important insight into the role of support people in the provision of cervical screening with people with intellectual disability.
Numerous studies (45, 46, 48, 55) provided information about strategies and approaches utilised by healthcare providers to successfully “[ … ] prepare women [with intellectual disability] psychologically for screening to enhance understanding, increase predictability and minimise anxiety.” (55) (p.143) Health care providers in these studies said they took time to explain the cervical screening procedure in depth, before the test was performed, including using “visual communication with pictures and diagrams.” (46) (p.7) One healthcare provider said, “I will draw it out, I explain what I’m doing before we do it” (46) (p.7) and another said, “we just have a uterus, not a picture, but a 3D little thing, where you can actually see and hold it towards my belly and say, ‘that’s where it is…’.” (45) (p.368) Health care providers in these studies said that they “don’t go straight to the Pap smear first thing” (46) (p.8), as an intellectual disability nurse explained,
[ … ] we go down just to look at the room, let them sit on the couch you know look at the speculum all those kind of things, you know the little brush that actually takes the specimen you know takes the cells away, just so they’ve got an understanding of what it involves. You know getting in position without doing anything invasive at the time and just maybe build on that so you take two or three trips maybe beforehand just to kind of desensitise and build that bit of insight really and obviously the person who’s going to actually do the procedure get them involved as well if possible [ … ] I would look at doing that really because that’s automatically going to make the person hopefully feel comfortable (55). (p.135).
Health care providers discussed adjusting their clinical practices to “meet them [patients with intellectual disability] where they’re at and not push them out of their comfort zone” (46) (p.8). For example, a healthcare provider said:
I’ve had a couple patients where they don’t want me to elevate the table up or they get really dizzy or anxious with that, so I have to leave the table basically pretty low to the ground, and then we still try to put their feet in the foot rests, but I kind of have to crouch on the ground sometimes, because I can’t raise the table up” (46) (p.8).
These person-centred strategies were reported to build trust between patients with intellectual disability and healthcare providers and build the knowledge of patients so that “[ … ] eventually you can get to the point where sometimes you can do a Pap smear.” (46) (p.8) However, a number of studies (45, 48, 50, 55) reported that clinical time constraints meant healthcare providers lacked the time to adequately explain the need and nature of cervical screening and perform the test. In these instances, healthcare providers were reported to ask patients to return for a second appointment to conduct the screening procedure. However, this was acknowledged to increase the risk of losing patients to follow-up.
The importance for people with intellectual disability to feel comfortable with their doctor to have cervical screening, was discussed in a number of studies (46, 49, 60). A woman with intellectual disability said that she could proceed with having a cervical screening test because, “I’m able to talk with my doctor. I’m able to explain to my doctors what’s wrong with me.” (46) (p.8) In another study, a person with intellectual disability said they found it helpful when “the nurse tried to relax me, talked with me and joked with me to take my mind off it.” (49) (p.909) Although a positive relationship with the healthcare provider was important, in one study (60) people with intellectual disability were found less likely to receive cervical screening when they had a long-term relationship with their doctor, attributed to entrenched misassumptions by the doctor about sexual activity/inactivity and vulnerability to sexual assault (60). One study (46) reported that people with intellectual disability were more comfortable having a cervical screening test with female healthcare providers.
Studies (46, 49, 50, 55, 68) also reported healthcare provider concerns about navigating informed consent, described as a “long and repetitive process that has to be individually tailored to each woman.” (50) (p.91) Health care providers were reported to lack the communicative competence required to navigate consent and perform cervical screening with patients with intellectual disability, as an intellectual disability nurse commented:
[ … ] They [GPs] wouldn’t show any accessible information, they wouldn’t check for retention [of information], they wouldn’t even necessarily get the decision-making process right (55) (p.139).
Similarly, Conder, Mirfin-Veitch (50) reported that healthcare providers often directed questions to support people (i.e., family members or disability service providers) rather than the individual with intellectual disability, which could fail to elicit a full sexual history, including experiences of sexual abuse. Family members and disability and healthcare providers were also reported to believe that patients with intellectual disability could not understand information about cervical screening, as a service provider explained:
“…sometimes I feel like in certain situations, some facilities just think that because they’re not capable of understanding these things, they don’t take the time to explain it to them, so they automatically write them off as they don’t need it or they waive their right…” (46) (p.7).
In another study a healthcare provider commented, “I’ll talk to my patients, even the ones that aren’t able to interact at all, and I’ve had family members tell me ‘no they don’t understand you,’ but I’ll talk to them anyway.” (45) (p.367).
In several studies (46, 49, 50, 55, 59, 68), healthcare providers were reported to have a “lack of experience or skill or confidence” (55) (p.138) conducting cervical screening with people with intellectual disability. One study reported that only 57.5% of healthcare providers were confident in providing cervical screening for people with intellectual disability (54). An intellectual disability nurse explained:
[ … ] I don’t think we always realise how difficult it is for people who haven’t worked with people with an intellectual disability. We go in all guns blazing about reasonable adjustments but people who have no experience of people with an intellectual disability, it’s understandable sometimes why their decision-making process isn’t okay or maybe their approach isn’t. [ … ] I do think that we do have to think that someone’s experience of intellectual disability is very limited and you’re doing a very invasive procedure with someone who’s very distressed. You may not handle it that well (55). (p.138).
Some studies reported perceived healthcare provider difficulties in performing the test with “women who might find it difficult to keep still throughout the procedure.” (50) (p.89) For example, healthcare providers said they would not perform cervical screening for people with intellectual disability “where the level of disability is too high” as “it is such a very delicate procedure and a very delicate part of the human anatomy, and we felt that we couldn’t control the situation enough to do it properly.” (45) (p.368) Some doctors said they would refer patients with intellectual disability to a gynaecologist rather than performing these themselves (45). These findings were similar to another study (59) that found women who were regularly seeing a specialist obstetrician/gynaecologist were significantly more likely to receive cervical screening than those who were seeing a GP.
Facilitating positive experiences of cervical screening extended beyond the test itself and included the whole clinical experience, such as time spent in the clinic waiting room and “setting appointment times that worked for the woman, which might mean scheduling a longer appointment, or one at a particular time of day.” (50) (p.92) Studies reported that collaboration between disability and health services was essential to facilitate appointment logistics that worked for the person with intellectual disability. This included sharing “information from support services about the woman’s special needs [ … ] such as the need for a quiet waiting room [ … ] and [ … ] if the practice staff know there is going to be a delay, they actually ring if we need to know.” (50) (p.92) These person-centred approaches were reported to help alleviate anxiety and contributed to positive experiences of cervical screening. However, another study (50) reported that disability service providers often didn’t know the screening status of their clients, particularly if clients lived independently, making it difficult to facilitate participation in cervical screening.
Studies reported lack of clinical practices to ensure the cervical screening needs of patients with intellectual disability were met. This included that health services “rarely proactively consider the health needs of people with intellectual disability as a specific patient group with additional needs.” (68) (p.88).
Only one practice had nominated a member of staff to take lead responsibility for patients with disabilities (including intellectual disability), very few practices said they routinely kept up-to-date records of the named Community Intellectual Disability Team (CLDT) nurse for their patients under the Team’s care, awareness of the general health checks provided by the CLDTs was low, and practices rarely provided general health checks for patients with intellectual disability themselves (68)(p.88).
In one study, a service provider recommended clinics adopt design features to improve women’s experiences of cervical screening, such as “making one room that’s colorful” and “making your rooms more friendly looking, bright.” (46) (p.10) These findings provide insight into optimising the roles of disability and health services in supporting access to cervical screening for people with intellectual disability.
People with intellectual disability were reported to lack knowledge about cervical screening (46, 67), often believing they were not eligible for the test. A woman with intellectual disability stated, “I thought I wouldn’t be able to have a smear test. Women with intellectual disability feel like they can’t have a test, not like other women.” (67) (p.14) In one study (58) only 35% of participants with intellectual disability knew the definition of a Pap test and only 19% knew the recommended Pap test frequency. Studies attributed this lack of knowledge to the exclusion of people with intellectual disability from cervical screening information, as a service provider commented:
There’s a whole network of informal ways that people learn … and this goes across the board with a lot of health messaging, less accessible to people with disability, or they don’t see it as pertaining to them because it’s never targeted (46)(p.6).
Standard cervical screening invitations and reminder letters often failed to meet the literacy needs of people with intellectual disability (55, 68). For example, in one study, only a minority of clinics surveyed “would always check whether a woman had an intellectual disability or other communication difficulty before issuing her invitation for cervical screening” (68) (p.89). The study reported that “even when issuing invitations to women known to have intellectual disability, most practices said they would send their usual standard letter and/or information leaflet.” (68) (p.89) This was reported to be “simpler for the practice, and avoided potentially insulting people by sending simplified letters or information leaflets to selected recipients.” (68) (p.89) This approach meant that patients required a family member to read the letter or that letters were discarded without being read (55, 68).
This systematic review and meta-analysis provide compelling evidence of the extremely low prevalence of cervical screening among people with intellectual disability, and the significantly lower likelihood of this population receiving screening than people without intellectual disability. The review also highlighted the numerous and often unique barriers that hinder participation among this population.
The screening prevalence reported in our review, with just over one-third of people with intellectual disability having had a cervical screening test, was comparatively lower than has been reported in broader disability research (i.e., including people with other forms of disability) (25), although similar to results from a recent Swedish national database study of women with intellectual disability (24). Most studies have grouped people with intellectual disability together with people with psychosocial, sensory, physical, and other disabilities, which highlights the need for intellectual disability-focused research to adequately understand cervical screening participation among this population (70). Our review also highlighted that, with the exception of the Swedish study (24), studies linking national cancer screening registries and population demographics which can shine a spotlight on cervical screening participation at a population level for people with intellectual disability, were lacking. However, the WHO Global Strategy to Eliminate Cervical Cancer (5) has raised awareness of cervical screening data gaps and may lead to improvements, including in Australia where a government data linkage initiative, PLIDA (Person Level Integrated Data Asset) (71), will support the identification of people with disability within the National Cancer Screening Register.
Our review identified numerous factors that impacted participation in cervical screening by people with intellectual disability. Applying the socio-ecological model (SEM) to our analysis revealed multilevel factors influencing screening and enabled us to identify evidence gaps in the current literature (41). While most studies focused on individual and interpersonal level factors, there was less research examining organisational, community, and policy level influences. The majority of studies also looked at uptake and barriers to Pap test-based screening rather than HPV screening which was only introduced in 2017 in Australia (one of the earliest countries to switch from Pap tests to HPV testing) and, as expected, none included the relatively recent option of a self-collected sample for HPV testing without a speculum examination.
At the individual level, people with intellectual disability were reported to experience fear and anxiety about cervical screening, including fear of the test results, similar to previous research with women with other disabilities (72) and women without disability (73). However, for people with intellectual disability, fear and anxiety may be exacerbated by additional issues. These include a lack of accessible information and education to prepare for screening, and previous negative screening experiences due to poor healthcare provider communicative practices or having experienced a painful procedure where the healthcare provider failed to stop when requested to do so. Perceptions by healthcare providers, family members and support people that people with intellectual disability would not tolerate the cervical screening procedure can also preclude this population (19). The recent implementation in Australia of universal self-collection of an HPV test (whereby people can choose to take the sample themselves, or by a clinician if preferred, from the vagina without the need for a speculum examination) (74) offers promise to overcome some of these barriers posed by fears and anxiety. Raising awareness of this option, including amongst families, support people and disability organisations is essential (74).
Similarly, it was often assumed that people with intellectual disability would lack capacity to consent to cervical screening and healthcare providers frequently described the processes as difficult. Decisions to deny screening were made for people on the basis that they would not be able to consent, reflecting the findings of other intellectual disability health research (75). The shift in focus away from determining whether a person has the capacity to consent to medical procedures, to ensure that they are supported to make an informed decision through the use of accessible information and appropriate supports will hopefully lead to improvements in access to screening (75, 76). Training new generations of healthcare providers would also go some way in addressing the fear and anxiety experienced by women with intellectual disability through improved patient-provider communication and enhanced trust (77, 78).
Negative cultural discourse about people with intellectual disability contributed to misassumptions about cervical screening eligibility. This may include assumptions by healthcare providers and support people that people with intellectual disability are not engaging in consensual sexual relationships and a lack of recognition that this group is at significantly greater risk of sexual assault than the general community (22). Healthcare providers therefore may fail to ask relevant questions during a consultation, and may also focus on the person’s disability rather than broader healthcare needs (79). Training has been demonstrated to be an effective method to improve knowledge, broaden perspectives, and increase the confidence of healthcare providers in providing healthcare to people with intellectual disability (80). However, broader organisational and policy-level changes are also required to facilitate long-term change (15). For instance, strategies such as tailored communication about cervical screening, increased clinical appointment times and the availability of accessible information about cervical screening for people with intellectual disability (77) are essential to facilitate improved care.
Our review highlighted that support people could positively influence cervical screening participation for people with intellectual disability. Previous research has reported that support people do not always allow people with intellectual disability to speak for themselves in medical consultations, potentially preventing people with intellectual disability from exerting control over their healthcare needs (77). Healthcare providers’ over reliance on support people’s accounts when determining healthcare needs (81) is problematic, particularly when considering the pervasive misassumptions reported throughout the included literature that people with intellectual disability are sexually inactive. Denial of the sexuality of people with intellectual disability has far-reaching negative consequences including exclusion from sexual healthcare and education (22, 82). These findings underscore the need for cervical screening information and education that is inclusive of support people, and that emphasises the appropriate roles, to maximise positive screening outcomes.
People with intellectual disability may also not believe they are eligible for screening (46) due to a lack of visibility in health promotion information. In addition to the lack of accessible information about screening, systems that generate invitations to have a cervical screening test at a service or programmatic level also neglect to meet the needs people with intellectual disability.
Our review found that healthcare providers lacked information about the screening status of their clients, posing a significant challenge in ensuring participation in cervical screening. However, in Australia, a recent national digital cancer screening registry allows healthcare providers to access patients’ screening history (83), offering a promising solution to overcome this barrier. Enhanced coordination of preventative healthcare activities aims to improve equitable healthcare access and tailored support for people with intellectual disability. These findings emphasise the urgency for intellectual disability-focused initiatives to enhance participation in cervical screening programs.
There were a number of limitations in the published literature. Only a quarter of the studies included in this review focused specifically on cervical screening. Most studies included cervical screening within a broader focus on healthcare, which may fail to identify barriers that are particular to cervical screening. We found that less than a quarter of studies in this review sought data directly from people with intellectual disability. Most collected information through medical records, while qualitative studies often engaged with service providers such as disability support workers and healthcare providers. There is, therefore, a need to hear directly from people with intellectual disability to understand lived experiences of cervical screening (78). Furthermore, cervical cancer can impact anyone with a cervix (84), however studies focused primarily on white cisgender women. There is a need for future research to include all people with intellectual disability who have a cervix, including non-binary and gender diverse people who were assigned female at birth and trans men with a cervix (84) as well as Indigenous and Black people and people of colour.
There are several limitations to the present study. Only articles published in the English language were included in this review, representing high-income countries, and we did not explore grey literature. Although we used a comprehensive search strategy, terminology about intellectual disability differs internationally (85) and may pose limitations on the generalisability and comparability of our findings. We also did not assess the timeframe of cervical screening participation by subgroup or meta-regression, which could be a source of heterogeneity between the included studies.
Addressing disparity in cervical screening participation is essential to achieving the elimination of cervical cancer as a public health problem equitably and to improving the overall health and wellbeing of people with intellectual disability (5). Our findings highlight the need for multilevel strategies (41) to challenge negative cultural discourse about people with intellectual disability, which leads to stigmatisation and discrimination, and facilitates the continuation of systemic barriers. Inclusive, accessible, and supportive environments that encourage regular cervical screening with this population are needed. Furthermore, healthcare facilities should be designed and staffed to be inclusive of individuals with intellectual disability, ensuring that the physical, social, sensory and communication needs of people with intellectual disability are addressed (86). Collaboration between healthcare providers, disability service organisations, and policymakers is essential to implement targeted interventions and policies to improve cervical screening (86). Additionally, cervical screening information and public health campaigns should be tailored to reach people with intellectual disability, emphasising the importance of cervical screening. These resources and campaigns should utilise accessible formats, such as easy-to-read materials, visual aids, and multimedia resources, to ensure the information is accessible and engaging for this population (86). These efforts must be co-designed and community-led to ensure that the voices of people with intellectual disability with a diverse range of experiences are foregrounded in all initiatives aimed at enhancing cervical screening participation.
People with intellectual disability face significant disparities in cervical screening. Future research, policy, and practice initiatives are needed to address the barriers impacting cervical screening participation, facilitating long-term systemic change and social transformation. These efforts must be co-designed and community-led to effectively address the unique challenges faced by this population. By prioritising inclusive approaches, we can work towards achieving equity in both global and local endeavours aimed at eliminating cervical cancer.
RP: Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. MD: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. IS: Conceptualization, Formal analysis, Funding acquisition, Methodology, Supervision, Writing – review & editing. LT: Data curation, Methodology, Writing – review & editing, Writing – original draft. CB: Data curation, Methodology, Writing – review & editing. JL: Funding acquisition, Methodology, Writing – review & editing. HJ: Methodology, Writing – review & editing. EK: Methodology, Writing – review & editing. JU: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. SS: Funding acquisition, Methodology, Writing – review & editing. EC: Funding acquisition, Methodology, Writing – review & editing. AC: Funding acquisition, Methodology, Writing – review & editing. DB: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is supported by a National Health and Medical Research Council of Australia (NHMRC) Targeted Cancer Research Grant (APP2015215).
The chief investigators on this project were DB, JU, IS, MD, E-LC, AC, JL and SS. We acknowledge Yasmine Bahwich for assistance in data collection. We thank the ScreenEQUAL Advisory Group who provide the voices and lived experience of people with intellectual disability to produce meaningful and relevant work in the field of intellectual disability.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1379497/full#supplementary-material
Supplementary tables and figures | EASY READ VERSION - CERVICAL SCREENING FOR PEOPLE WITH INTELLECTUAL DISABILITY
1. Arbyn M, Weiderpass E, Bruni L, de Sanjose S, Saraiya M, Ferlay J, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. (2020) 8:e191–203. doi: 10.1016/S2214-109X(19)30482-6
2. Lei J, Ploner A, Elfstrom KM, Wang J, Roth A, Fang F, et al. HPV vaccination and the risk of invasive cervical cancer. N Engl J Med. (2020) 383:1340–8. doi: 10.1056/NEJMoa1917338
3. Canfell K. Towards the global elimination of cervical cancer. Papillomavirus Res. (2019) 8:100170. doi: 10.1016/j.pvr.2019.100170
4. de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. (2020) 8:e180–e90. doi: 10.1016/S2214-109X(19)30488-7
5. World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organization (2020). Available at: https://www.who.int/publications/i/item/9789240014107.
6. Sundstrom K, Herweijer E, Wang J. Cervical screening in high-income countries: the need for quality assurance, adjunct biomarkers and rational adaptation to HPV vaccination. Prev Med. (2021) 144:106382. doi: 10.1016/j.ypmed.2020.106382
7. Jansen EEL, Zielonke N, Gini A, Anttila A, Segnan N, Voko Z, et al. Effect of organised cervical cancer screening on cervical cancer mortality in Europe: a systematic review. Eur J Cancer. (2020) 127:207–23. doi: 10.1016/j.ejca.2019.12.013
8. McKenzie K, Milton M, Smith G, Ouellette-Kuntz H. Systematic review of the prevalence and incidence of intellectual disabilities: current trends and issues. Curr Dev Disord Rep. (2016) 3:104–15. doi: 10.1007/s40474-016-0085-7
9. Havercamp SM, Scott HM. National health surveillance of adults with disabilities, adults with intellectual and developmental disabilities, and adults with no disabilities. Disabil Health J. (2015) 8:165–72. doi: 10.1016/j.dhjo.2014.11.002
10. Trollor J, Srasuebkul P, Xu H, Howlett S. Cause of death and potentially avoidable deaths in Australian adults with intellectual disability using retrospective linked data. BMJ Open. (2017) 7:e013489. doi: 10.1136/bmjopen-2016-013489
11. Commonwealth of Australia. National Roadmap for Improving the Health of People with Intellectual Disability. Australia: Department of Health and Aged Care, Australian Government (2021).
12. Cuypers M, Schalk BWM, Boonman AJN, Naaldenberg J, Leusink GL. Cancer-related mortality among people with intellectual disabilities: A nationwide population-based cohort study. Cancer. (2022) 128:1267–74. doi: 10.1002/cncr.34030
13. World Health Organization. Global report on health equity for persons with disabilities. Geneva: World Health Organization (2022). Available at: https://www.who.int/publications/i/item/9789240063600.
14. Fletcher J, Yee H, Ong B, Roden RC. Centering disability visibility in reproductive health care: Dismantling barriers to achieve reproductive equity. Womens Health (Lond). (2023) 19:17455057231197166. doi: 10.1177/17455057231197166
15. Morison T. Reproductive justice: A radical framework for researching sexual and reproductive issues in psychology. Soc Pers Psychol Compass. (2021) 15. doi: 10.1111/spc3.12605
16. Adams L. Forgotten by donors: a call to action by persons with disabilities to resource disability justice within sexual and reproductive health rights funding. Sexual Reprod Health Matters. (2023) 31:1–7. doi: 10.1080/26410397.2023.2261688
17. Emerson E, Baines S, Allerton L, Welch VA. Health inequalities and people with learning disabilities in the UK (2011). Available online at: https://strathprints.strath.ac.uk/34862/1/vid_7479_IHaL2010_3HealthInequality2010.pdf.
18. Strnadová I, Loblinzk J, Danker J. Importance of sex education for a successful transition to life after school: Experiences of high school girls with intellectual disability. Br J Learn Disabilities. (2021) 49:303–15. doi: 10.1111/bld.12403
19. Pelleboer-Gunnink HA, Van Oorsouw W, Van Weeghel J, Embregts P. Mainstream health professionals’ stigmatising attitudes towards people with intellectual disabilities: a systematic review. J Intellect Disabil Res. (2017) 61:411–34. doi: 10.1111/jir.12353
20. Ali A, Scior K, Ratti V, Strydom A, King M, Hassiotis A. Discrimination and other barriers to accessing health care: perspectives of patients with mild and moderate intellectual disability and their carers. PloS One. (2013) 8:e70855. doi: 10.1371/journal.pone.0070855
21. Carter A, Strnadová I, Watfern C, Pebdani R, Bateson D, Loblinzk J, et al. The sexual and reproductive health and rights of young people with intellectual disability: A scoping review. Sexuality Res Soc Policy. (2021) 19:372–90. doi: 10.1007/s13178-021-00549-y
22. Tomsa R, Gutu S, Cojocaru D, Gutierrez-Bermejo B, Flores N, Jenaro C. Prevalence of sexual abuse in adults with intellectual disability: systematic review and meta-analysis. Int J Environ Res Public Health. (2021) 18. doi: 10.3390/ijerph18041980
23. Royal Commission into Violence A. Neglect and exploitation of people with disability. In: Final Report 2023. (2023) Available at: https://disability.royalcommission.gov.au/publications/final-report.
24. Hu K, Wang J, Sparen P, Herweijer E, Sjolander A, Adami HO, et al. Invasive cervical cancer, precancerous lesions, and cervical screening participation among women with mental illness in Sweden: a population-based observational study. Lancet Public Health. (2023) 8:e266–e75. doi: 10.1016/S2468-2667(23)00026-9
25. Andiwijaya FR, Davey C, Bessame K, Ndong A, Kuper H. Disability and participation in breast and cervical cancer screening: A systematic review and meta-analysis. Int J Environ Res Public Health. (2022) 19:15. doi: 10.3390/ijerph19159465
26. Choi JY, Yeob KE, Hong SH, Kim SY, Jeong EH, Shin DW, et al. Disparities in the Diagnosis, Treatment, and Survival Rate of Cervical Cancer among Women with and without Disabilities. Cancer Control. (2021) 28:10732748211055268. doi: 10.1177/10732748211055268
27. Strnadová I, Dowse L, Watfren C. Doing research inclusively: guidelines for co-producing research with people with disability. Sydney: Disability Innovation Institute, UNSW (2020).
28. Strnadová I, Dowse L, Garcia-Lee B, Hayes S. Ethical issues in co-production research with people with disability: Guidance for researchers and ethics committees. Sydney: Disability Innovation Institute, UNSW (2023).
29. Petticrew M, Roberts H. Systematic reviews in the social sciences: A practical guide. United Kingdom: John Wiley & Sons (2008).
30. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
31. Hammer A, Soegaard V, Maimburg RD, Blaakaer J. Cervical cancer screening history prior to a diagnosis of cervical cancer in Danish women aged 60 years and older-A national cohort study. Cancer Med. (2019) 8:418–27. doi: 10.1002/cam4.1926
32. Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton: Alberta Heritage Foundation for Medical Research (AHFMR (2004).
33. Bockhorn LN, Vera AM, Dong D, Delgado DA, Varner KE, Harris JD. Interrater and intrarater reliability of the beighton score: A systematic review. Orthop J Sports Med. (2021) 9:2325967120968099. doi: 10.1177/2325967120968099
34. Lowry R. Kappa as a Measure of Concordance in Categorical Sorting (2023). Available online at: http://vassarstats.net/kappa.html.
35. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
36. Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Statistics. (1950) 21:607–11. doi: 10.1214/aoms/1177729756
37. Miller JJ. The inverse of the Freeman-Tukey double arc-sine transformation. Am Statistician. (1978) 32. doi: 10.1080/00031305.1978.10479283
38. Cochran WG. The combination of estimates from different experiments. Biometrics. (1954) 10:101–29. doi: 10.2307/3001666
39. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
40. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
41. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. (1988) 15:351–77. doi: 10.1177/109019818801500401
42. Veritas Health Innovation. Covidence systematic review software. Melbourne, Australia. Available at: www.covidence.org.
43. Walmsley J, Strnadova I, Johnson K. The added value of inclusive research. J Appl Res Intellect Disabil. (2018) 31:751–9. doi: 10.1111/jar.12431
44. The World Bank. World Bank Country and Lending Groups (2023). Available online at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
45. Agaronnik N, Pendo E, Lagu T, DeJong C, Perez-Caraballo A, Iezzoni LI. Ensuring the reproductive rights of women with intellectual disability. J Intellect Dev Disabil. (2020) 45:365–76. doi: 10.3109/13668250.2020.1762383
46. Armin JS, Williamson HJ, Begay A, Etcitty J, Attakai A, Russell K, et al. Adapting a cancer screening education program for native American women with disabilities. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph19159280
47. Breau G, Thorne S, Baumbusch J, Hislop TG, Kazanjian A. Primary care providers’ Attitudes towards recommending cancer screening to patients with intellectual disability: A cross-sectional survey. Inclusion. (2020) 8:185–93. doi: 10.1352/2326-6988-8.3.185
48. Breau G, Thorne S, Baumbusch J, Hislop TG, Kazanjian A. Family physicians’ and trainees’ experiences regarding cancer screening with patients with intellectual disability: An interpretive description study. J Intellect Disabil. (2023) 27:250–65. doi: 10.1177/17446295211044041
49. Broughton S, Thomson K. Women with learning disabilities: risk behaviours and experiences of the cervical smear test. J Adv Nurs. (2000) 32:905–12. doi: 10.1046/j.1365-2648.2000.t01-1-01555.x
50. Conder J, Mirfin-Veitch B, Payne D, Channon A, Richardson G. Increasing the participation of women with intellectual disabilities in women’s health screening: a role for disability support services. Res Pract Intellectual Dev Disabilities. (2018) 6:86–96. doi: 10.1080/23297018.2018.1466354
51. Fortney S, Tasse MJ. Urbanicity, health, and access to services for people with intellectual disability and developmental disabilities. Am J Intellect Dev Disabil. (2021) 126:492–504. doi: 10.1352/1944-7558-126.6.492
52. Langan J, Whitfield M, Russell O. Paid and unpaid carers: their role in and satisfaction with primary health care for people with learning disabilities. Health Soc Care Community. (1994) 2:357–65. doi: 10.1111/hsc.1994.2.issue-6
53. Lin LP, Lin JD, Chu CM, Chen LM. Caregiver attitudes to gynaecological health of women with intellectual disability. J Intellect Dev Disabil. (2011) 36:149–55. doi: 10.3109/13668250.2011.599316
54. Lin JD, Sung CL, Lin LP, Liu TW, Lin PY, Chen LM, et al. Perception and experience of primary care physicians on Pap smear screening for women with intellectual disabilities: a preliminary finding. Res Dev Disabil. (2010) 31:440–5. doi: 10.1016/j.ridd.2009.10.012
55. Lloyd JL, Coulson NS. The role of learning disability nurses in promoting cervical screening uptake in women with intellectual disabilities: A qualitative study. J Intellect Disabil. (2014) 18:129–45. doi: 10.1177/1744629514528829
56. Parish SL, Moss K, Richman EL. Perspectives on health care of adults with developmental disabilities. Intellect Dev Disabil. (2008) 46:411–26. doi: 10.1352/2008.46:411-426
57. Parish SL, Rose RA, Luken K, Swaine JG, O’Hare L. Cancer screening knowledge changes. Res Soc Work Practice. (2011) 22:43–53. doi: 10.1177/1049731511415550
58. Parish SL, Swaine JG, Luken K, Rose RA, Dababnah S. Cervical and breast cancer-screening knowledge of women with developmental disabilities. Intellect Dev Disabil. (2012) 50:79–91. doi: 10.1352/1934-9556-50.2.79
59. Parish SL, Swaine JG, Son E, Luken K. Determinants of cervical cancer screening among women with intellectual disabilities: evidence from medical records. Public Health Rep. (2013) 128:519–26. doi: 10.1177/003335491312800611
60. Plourde N, Brown HK, Vigod S, Cobigo V. The association between continuity of primary care and preventive cancer screening in women with intellectual disability. Am J Intellect Dev Disabil. (2018) 123:499–513. doi: 10.1352/1944-7558-123.6.499
61. Rees G. Increasing access to cancer screening programmes. Learn Disability Practice. (2011) 14:14–9. doi: 10.7748/ldp2011.09.14.7.14.c8697
62. Son E, Parish SL, Swaine JG, Luken K. Accuracy of self-reported cervical and breast cancer screening by women with intellectual disability. Am J Intellect Dev Disabil. (2013) 118:327–36. doi: 10.1352/1944-7558-188.4.327
63. Stein K. Caring for people with learning disability: a survey of general practitioners’ attitudes in Southampton and South-west Hampshire. Br J Learn Disabilities. (2000) 28:9–15. doi: 10.1046/j.1468-3156.2000.00006.x
64. Swaine JG, Dababnah S, Parish SL, Luken K. Family caregivers’ perspectives on barriers and facilitators of cervical and breast cancer screening for women with intellectual disability. Intellect Dev Disabil. (2013) 51:62–73. doi: 10.1352/1934-9556-51.01.062
65. Swaine JG, Parish SL, Luken K, Son E, Dickens P. Test of an intervention to improve knowledge of women with intellectual disabilities about cervical and breast cancer screening. J Intellect Disabil Res. (2014) 58:651–63. doi: 10.1111/jir.12062
66. Sykes K, McGeechan GJ, Crawford H, Giles EL. Factor influencing women with learning disabilities deciding to, and accessing, cervical and breast cancer screening: Findings from a Q methodology study of women with learning disabilities, family and paid carers. Eur J Cancer Care (Engl). (2022) 31:e13702. doi: 10.1111/ecc.13702
67. Wicks S. Assessing the health screening choices of women with learning disabilities. Learn Disability Pract. (2007) 10:14. doi: 10.7748/ldp2007.11.10.9.10.c6256
68. Wood R, Douglas M. Cervical screening for women with learning disability: current practice and attitudes within primary care in Edinburgh. Br J Learn Disabilities. (2007) 35:84–92. doi: 10.1111/j.1468-3156.2007.00440.x
69. Bershadsky J, Taub S, Engler J, Moseley CR, Lakin KC, Stancliffe RJ, et al. Place of residence and preventive health care for intellectual and developmental disabilities services recipients in 20 states. Public Health Rep. (2012) 127:475–85. doi: 10.1177/003335491212700503
70. Brooker K, van Dooren K, Tseng CH, McPherson L, Lennox N, Ware R. Out of sight, out of mind? The inclusion and identification of people with intellectual disability in public health research. Perspect Public Health. (2015) 135:204–11. doi: 10.1177/1757913914552583
71. Australian Bureau of Statistics. Person Level Integrated Data Asset (PLIDA) (2023). Available online at: https://www.abs.gov.au/about/data-services/data-integration/integrated-data/person-level-integrated-data-asset-plida.
72. Kilic A, Tastan S, Guvenc G, Akyuz A. Breast and cervical cancer screening for women with physical disabilities: A qualitative study of experiences and barriers. J Adv Nurs. (2019) 75:1976–86. doi: 10.1111/jan.14048
73. O’Laughlin DJ, Strelow B, Fellows N, Kelsey E, Peters S, Stevens J, et al. Addressing anxiety and fear during the female pelvic examination. J Prim Care Community Health. (2021) 12:2150132721992195. doi: 10.1177/2150132721992195
74. Creagh NS, Zammit C, Brotherton JM, Saville M, McDermott T, Nightingale C, et al. The experience of under-screened and never-screened participants using clinician-supported self-collection cervical screening within the Australian National Cervical Screening Program. Womens Health (Lond). (2022) 18:17455065221075905. doi: 10.1177/17455065221075905
75. Dunn M, Strnadova I, Scully JL, Hansen J, Loblinzk J, Sarfaraz S, et al. Equitable and accessible informed healthcare consent process for people with intellectual disability: a systematic literature review. BMJ Qual Saf. (2023). doi: 10.1101/2023.03.06.23286791
76. Sullivan WF, Heng J. Supporting adults with intellectual and developmental disabilities to participate in health care decision making. Can Fam Physician. (2018) 64:S32–S6.
77. Doherty AJ, Atherton H, Boland P, Hastings R, Hives L, Hood K, et al. Barriers and facilitators to primary health care for people with intellectual disabilities and/or autism: an integrative review. BJGP Open. (2020) 4. doi: 10.3399/bjgpopen20X101030
78. Iezzoni LI, Long-Bellil LM. Training physicians about caring for persons with disabilities: “Nothing about us without us! Disabil Health J. (2012) 5:136–9. doi: 10.1016/j.dhjo.2012.03.003
79. Mason J, Scior K. ‘Diagnostic overshadowing’ amongst clinicians working with people with intellectual disabilities in the UK. J Appl Res Intellectual Disabilities. (2004) 17:85–90. doi: 10.1111/j.1360-2322.2004.00184.x
80. Hay G, Wilson NJ, Ong N, Benson P, Gallego G. Educating the educated: The impact of educational interventions on knowledge, attitudes and confidence of healthcare professionals in caring for patients with intellectual disability: A systematic review. J Intellectual Dev Disability. (2023) 49(2):1–12. doi: 10.1136/bmjopen-2021-049806
81. Hanlon P, MacDonald S, Wood K, Allan L, Cooper SA. Long-term condition management in adults with intellectual disability in primary care: a systematic review. BJGP Open. (2018) 2:bjgpopen18X101445. doi: 10.3399/bjgpopen18X101445
82. Alexander N, Taylor Gomez M. Pleasure, sex, prohibition, intellectual disability, and dangerous ideas. Reprod Health Matters. (2017) 25:114–20. doi: 10.1080/09688080.2017.1331690
83. Gertig D, Lee J. Supporting health care providers in cancer screening: the role of the National Cancer Screening Register. Med J Aust. (2023) 219:94–8. doi: 10.5694/mja2.52029
84. Connolly D, Hughes X, Berner A. Barriers and facilitators to cervical cancer screening among transgender men and non-binary people with a cervix: A systematic narrative review. Prev Med. (2020) 135:106071. doi: 10.1016/j.ypmed.2020.106071
85. Cluley V. From “Learning disability to intellectual disability”—Perceptions of the increasing use of the term “intellectual disability” in learning disability policy, research and practice. Br J Learn Disabilities. (2017) 46:24–32. doi: 10.1111/bld.12209
86. Australian Government. National Strategy for the Elimination of Cervical Cancer in Australia (2023). Available online at: https://www.health.gov.au/resources/publications/national-strategy-for-the-elimination-of-cervical-cancer-in-Australia?language=en.
Keywords: cervical screening, intellectual disability, facilitators, barriers, cancer screening, early detection of cancer
Citation: Power R, David M, Strnadová I, Touyz L, Basckin C, Loblinzk J, Jolly H, Kennedy E, Ussher J, Sweeney S, Chang E-L, Carter A and Bateson D (2024) Cervical screening participation and access facilitators and barriers for people with intellectual disability: a systematic review and meta-analysis. Front. Psychiatry 15:1379497. doi: 10.3389/fpsyt.2024.1379497
Received: 31 January 2024; Accepted: 27 June 2024;
Published: 26 July 2024.
Edited by:
Andrew Scott LaJoie, University of Louisville, United StatesReviewed by:
Katie Robb, University of Glasgow, United KingdomCopyright © 2024 Power, David, Strnadová, Touyz, Basckin, Loblinzk, Jolly, Kennedy, Ussher, Sweeney, Chang, Carter and Bateson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Deborah Bateson, ZGVib3JhaC5iYXRlc29uQHN5ZG5leS5lZHUuYXU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.