
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Psychiatry , 22 April 2024
Sec. Psychopathology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1378600
This article is part of the Research Topic Psychological Intervention for Suicidal Ideation, Behavior, and Attempted Suicide View all 12 articles
 Samantha A. Chalker1,2*†
Samantha A. Chalker1,2*† Roxanne Sicotte3,4†
Roxanne Sicotte3,4† Lindsay A. Bornheimer5,6†Emma M. Parrish7†
Lindsay A. Bornheimer5,6†Emma M. Parrish7† Heather Wastler8†Blaire Ehret9†Jordan DeVylder10†Colin A. Depp1,2†
Heather Wastler8†Blaire Ehret9†Jordan DeVylder10†Colin A. Depp1,2†Although it is well established that individuals living with psychosis are at increased risk for suicidal ideation, attempts, and death by suicide, several gaps in the literature need to be addressed to advance research and improve clinical practice. This Call-to-Action highlights three major gaps in our understanding of the intersection of psychosis and suicide as determined by expert consensus. The three gaps include research methods, suicide risk screening and assessment tools used with persons with psychosis, and psychosocial interventions and therapies. Specific action steps to address these gaps are outlined to inform research and practice, and thus, improve care and prognoses among persons with psychosis at risk for suicide.
Persons with schizophrenia spectrum disorders have an increased risk of suicide, up to 20 times that of the general population (1–3). While the risk of suicide is particularly elevated in the first episode and early stages of psychosis, it remains a major concern throughout the course of illness (4), with the lifetime rate of death by suicide estimated to range between 4 to 13% (5–7). According to a recent meta-analysis, individuals in the general population who self-report psychotic experiences are twice as likely to present with subsequent suicide ideation than the general population, three times as likely to attempt suicide, and four times as likely to die by suicide (8). Relatedly, approximatively 30-50% of individuals with schizophrenia spectrum disorders or affective disorders with psychotic features will have suicide ideation in their lifetime (9–11) and 20-50% will attempt suicide (7, 12, 13) highlighting the impact of suicide risk among those with psychosis.
While there has been substantial progress in research and clinical care for individuals experiencing psychosis with suicide risk, gaps remain. Notably, there are three major gaps identified determined by expert consensus (14) that deserve attention: 1) lack of research design standards, 2) unknown reliability and validity of suicide risk screening and assessment tools in a psychosis population, and 3) insufficient evidence of efficacious suicide-focused psychosocial interventions and therapies for those experiencing psychosis. We outlined several action steps that we believe will help researchers and providers fill these gaps.
Both suicide risk and psychosis encompass a wide range of definitions and broad continuum of severity (Table 1), contributing to unresolved variability in findings across studies. For example, a recent meta-analysis showed that the prevalence of suicide attempts varies according to the specific diagnosis of the schizophrenia spectrum disorder, the setting (outpatient vs. inpatient), and geographical region (23). A better understanding of these consistencies and inconsistencies is an important step in further the translation of this research into effective clinical intervention. Furthermore, in every stage of the research process possible, including research design, delivery, and implementation, researchers should include individuals with lived experience of psychosis and suicide risk (24–26). This may also include the acknowledgement that many researchers have lived experience themselves. The inclusion of people with lived experience will improve the quality and relevance of research to those who are most impacted: those seeking services. Finally, it is important to acknowledge the challenges of recruiting and retain participants with psychosis in research and how these challenges impact data ascertainment, e.g., (27). We therefore present recommendations for implementing research design standards on suicide risk in psychosis, while considering their heterogeneity and the aforementioned factors.
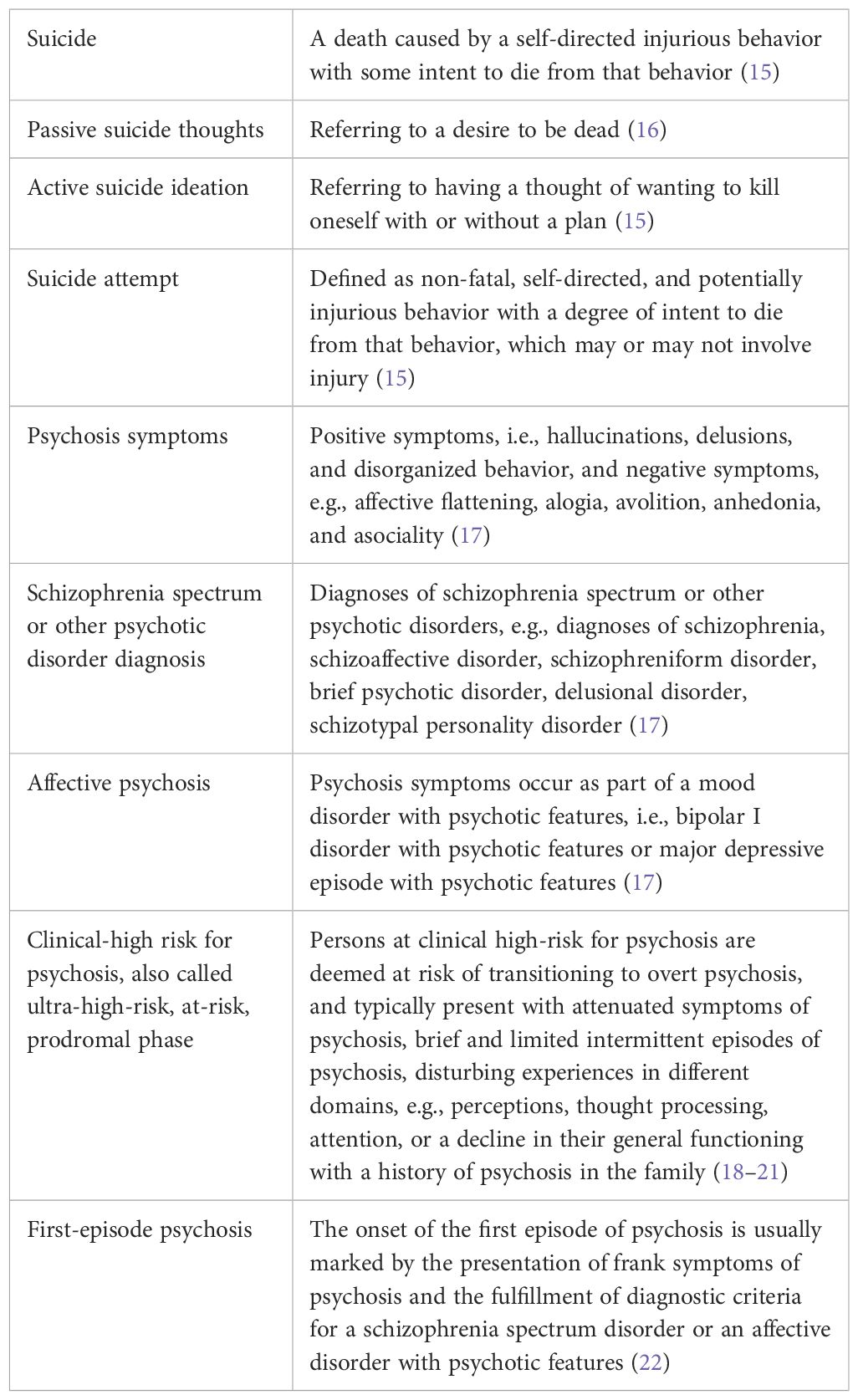
Table 1 Term Definitions.
Researchers should aim to recruit samples of people along a spectrum of psychosis symptom severity. This would include those with self-reported psychotic experiences in the general population who meet ultra or clinical high-risk criteria or who have experienced a first episode of psychosis, to those who have had a chronic schizophrenia spectrum disorder or disorder with psychotic features for many years. The needs and characteristics of young adults with a first episode of psychosis are different from those of people who have been living with the illness for several years, including in terms of stage of development and expectations of treatment (28, 29). It is therefore possible that suicide risk factors, as well as effective suicide prevention treatments, differ across people at different stages of illness.
The clinical profile of patients may vary depending on the community or clinical setting (e.g., inpatient units, outpatient services, specialized services for psychosis, such as early intervention services), and certain protective factors may also influence suicidal behaviors (e.g., safety measures during hospitalization (23). Studies should recruit participants from a variety of settings to ensure that samples include varying levels of suicide risk and psychosis symptom severity.
This is especially important given racial and ethnic disparities in psychosis risk across the continuum (30–32) and that risk factors may vary across racial and ethnic groups (33–35). For example, in first generation immigrants and Hispanic/Latinx persons with a schizophrenia spectrum disorder, maintaining cultural traditions from their country of origin, religious beliefs, and practices, and having a positive ethnic identity may be protective against suicide ideation (36, 37). This could translate into specific targets for assessment and suicide prevention interventions in these groups. Ethnicity and race should be carefully assessed (e.g., based on self-identification, multiple data sources, migratory status (35)). Increased culturally sensitive and inclusive research will contribute to the development of culturally sensitive suicide prevention interventions.
Knowledge and evidence on prevalence, risk factors, theoretical models (38, 39) and suicide prevention interventions (40, 41) come predominantly from high-income countries. However, there have been reports of different rates and risk factors for suicide thoughts and behaviors in persons with schizophrenia spectrum disorders between low- and middle-income countries and high-income countries (42–45). A cross-national comparative study revealed that self-reported psychotic experiences were less distressing for adults living in low- and middle-income countries than for those in high-income countries (46). However, it is possible that the cross-cultural validity of current measures of psychotic experiences is limited, that psychotic experiences of equal severity are less clinically relevant in some low- and middle-income countries due to certain social and cultural protective factors (e.g., collectivist communities), or that the association between psychotic experiences and distress, and possibly suicide thoughts and behaviors, differs between countries due to cultural differences (47). Measures of psychotic experiences need to be validated across countries to minimize intra-category variability and refined to focus more on distress to better identify individuals with greater needs among different cultures, notably in terms of suicide screening and prevention (47).
LGBTQ+ groups have a higher risk of suicidal ideation and behavior, owing in part to the unique challenges they may face and minority stressors (48–50), and may be a greater risk for experiencing psychosis (51, 52). It is crucial to better understand the unknown role of LGBTQ+ identities on suicide risk in psychosis as well as providing a broader understanding of the intersection of LGBTQ+ identities and psychosis. Including affirming questions include asking one’s gender identity as well as sex (e.g., 53, 54), can be a step forward to address these questions in future research.
Many studies of psychosis and suicide in the literature are cross-sectional (55–57), limiting the conclusions that can be drawn to impact the assessment of suicide risk, suicide prevention interventions, and understanding of mechanisms underlying the association between psychosis and suicide risk (55). While many studies have reported that psychosis is a risk factor for suicide (8, 10), recent evidence suggests a bidirectional relationship between psychosis-like experiences and suicide thoughts and behaviors (58, 59). Further longitudinal studies designed specifically to address these questions of clinical relevance are needed to inform suicide prevention practices. Study designs that combine short-term high intensity measurement and long-term panel type designs (i.e., measurement burst) may be useful to uncover the dynamics of psychosis-like experiences on suicide thoughts and behaviors.
Although the risk of suicide is high in persons with psychosis, the lifetime prevalence of all schizophrenia spectrum disorders and affective disorders with psychotic features is estimated at 3.06% (60), and up to half will experience suicide ideation or attempts in their lifetime (7, 9–13). Thus, to conduct studies with sufficient statistical power, largescale, multisite research studies are needed, with large sample sizes to provide a more robust evidence base. Pooling resources from different sites together may be one approach. Fortunately, large data sets already exist across a range of general and clinical populations and countries; more effort can be dedicated to merging these data sets for cross-site analyses. Future research should establish consistent measurement harmonization, which is needed for these analyses. Initiatives, such as the National Institutes of Health (NIH) Data Management and Sharing policy (61), the NIH Data Archive (62), and the National Institute of Mental Health MAP-PRO (Meaningful Assessment Protocol- Patient-reported outcomes) platform (63, 64), are also needed to improve our understanding of relatively rare phenomenon, such as suicide in people with psychosis.
Suicide screeners are used to identify those at risk for suicide (e.g., recent suicide thoughts or behaviors) while assessment tools develop a more comprehensive understanding of that suicide risk (e.g., severity and frequency of suicide thoughts, risk and protective factors). Both are crucial for early identification and prognosis of care. Moreover, using valid and reliable tools are necessary to develop an accurate understanding of suicide risk (65, 66) and an understanding of the unique phenomenology of suicide risk in those experiencing psychosis.
Overall, it is important to be screening and assessing for suicide risk in all populations and studies in the general population have consistently demonstrated that asking about suicide does not increase the risk of suicide (67, 68). In fact, there may be a benefit to asking about suicide (69). Given the increased suicide risk in a psychosis population it may be that much more crucial.
It is possible that existing current suicide risk screening tools are appropriate for individuals with psychosis, but this has yet to be established. Establishing the validity, reliability and utility of existing validated screeners or measures of suicide risk (e.g., the Ask Suicide-Screening Questions (ASQ) Toolkit (70–72)), the Beck Scale for Suicide Ideation (BSS (73, 74)), the Columbia – Suicide Severity Rating Scale (C-SSRS (75, 76)); in people with psychosis will help foster the harmonization and use of gold-standard measures of suicide thoughts and behaviors in this population. Notably, one study found that both the BSS and the C-SSRS were able to collect suicide attempt history for patients with schizophrenia spectrum disorders (77). Measures of suicide thoughts and behaviors, as well as psychosis experiences, should be harmonized across studies, building off broader efforts to standardize assessments to allow direct comparison across research studies. Additionally, future cross-sectional and longitudinal studies should carefully consider the timing of assessments. Many studies assess risk factors long before the suicide outcome occurs or use lifetime measures, which while useful may miss nuance captured by measures that incorporate questions about current suicide ideation (56). Future studies should examine lifetime and current suicide risk-related symptoms to better capture chronic risk factors (e.g., demographics) versus acute risk factors.
There are several unique aspects of psychosis and schizophrenia spectrum disorders that may influence the assessment of suicide risk. For some people with psychosis symptoms, psychiatric treatment or involuntary hospitalization can be unpleasant and potentially traumatic (78, 79). Therefore, it is possible that people with psychosis may hesitate to disclose suicide ideation to a provider for fear of further hospitalization. Second, there is some evidence that people with psychosis have impairments in metacognition and awareness of their thoughts (80, 81), which may impact their ability to report on suicide risk. This may be particularly relevant for details of such thoughts (e.g., recency, content). Third, people with psychosis experience both public and internalized stigma related to their mental health diagnoses or symptoms (82–84), which may increase risk of suicide (85, 86). It is possible that the stigma that people with psychosis experience compounds with stigma about suicide risk, further impacting their willingness to disclose suicidal thoughts.
Psychosis impacts the phenomenology of suicide. There is some evidence for greater medically lethal means used in psychosis populations (e.g., firearms (87)) and a longer duration of untreated psychosis is associated with an increased risk of suicide behavior (88). For some individuals with a schizophrenia spectrum disorder, suicide behaviors represent a direct response to command auditory hallucinations (e.g., 89). However, in one study, the rate of suicide attempts did not differ between those who experienced command hallucinations and those who did not, suggesting that other factors are important in identifying individuals at risk of suicide behavior among those with schizophrenia spectrum disorders (89).
Given inconsistent findings regarding the relationship between psychosis experiences and suicide thoughts and behaviors, a fine-grained analysis of specific psychosis symptoms (and their severity) with subtypes of suicide thoughts and behaviors (i.e., ideation, plans, attempts, death) could help better understand whether, for example, the association between psychosis and suicide thoughts and behaviors is due to the presence of psychosis symptoms, to specific symptoms (e.g., auditory versus visual hallucinations (90), to the frequency or intensity of these (90), to the associated distress (91), or is mediated by another variable (55). Relatedly, considerations of unique risk factors and protective factors and sources of strengths for this population should be determined and routinely assessed. For example, negative symptoms may be related to reduced suicidal behavior (10, 92) and defeatist attitudes may further be protective from suicide (93).
To fully assess for suicide risk in psychosis, understanding specific suicide risk factors and the phenomenology of suicide in this population, and whether these constructs differ from the general population, is crucial. Literature to date suggest the presence of various demographic characteristics (e.g., age, gender, history of suicide attempt), psychiatric symptom experiences (e.g., depression, hopelessness, psychosis symptoms), clinical insight, and substance use disorders contribute to suicide risk in the psychosis population (1, 8, 56, 57, 94–100). There is variability across studies in terms of whether risk factors (1) statistically explain the association between psychotic symptoms and suicide behavior or (2) whether psychotic symptoms themselves are an independent risk factor for suicide risk, adjusting for these factors (55, 101).
Psychosocial interventions and treatments to address suicide outcomes among psychosis populations are limited. (Note. We do not address pharmacologic treatments in this review but acknowledge that many gaps exist in that treatment domain as well.) A recent systematic review and meta-analysis examined 11 studies of psychosocial interventions among participants with psychosis with measurement of suicide outcomes and found a significant treatment effect that pooled across suicide ideation, attempt, and death (7). Interventions of the 11 studies included various approaches (i.e., supportive treatment, cognitive-behavioral, cognitive, case management) compared to treatment as usual or a waitlist, with cognitive-behavioral therapy (CBT) being the most prevalent approach (7). While the meta-analytic study by Bornheimer and colleagues (2020) had potential methodological limitations associated with selection bias due to the requirement of suicide-related outcomes being measured in the studies examined, the study provides preliminary support for psychosocial interventions in psychosis that captured suicide ideation, attempt, and death. Importantly, it also highlights the lack of empirical studies investigating their effect and the lack of consensus on best practices due to the wide variety of intervention characteristics in the included studies (7). Further gaps remain as there is little understanding of interventions directly targeting suicide thoughts and behaviors in psychosis. Moreover, and relatedly, the potential moderators of treatment uptake and retention are unknown, which may include more severe psychosis (e.g., 27).
Aside from studies who focus on suicide and psychosis within their research, many trials investigating suicide-related outcomes often exclude psychosis populations, and vice-versa (e.g., 102–107). For example, a recent systematic review of psychotherapy trials with suicide-related primary outcomes found that 75% excluded individuals with psychosis (102). Given this exclusion rate, this review highlights that there is a dearth of information on if suicide prevention interventions are effective for those with psychosis. In the review, few studies provided a rationale for excluding people with psychosis (102). Therefore, existing suicide-focused interventions (e.g., Brief Cognitive-Behavioral Therapy for suicide prevention (BCBT (108, 109)), Cognitive Therapy for Suicide Prevention (CT-SP (110)), Collaborative Assessment and Management of Suicidality (CAMS (111)), crisis lifelines (112), lethal means counseling ((113), safety planning type interventions (114)) should be evaluated in psychosis, and if needed, modifications and adaptations should be made to make these interventions more acceptable or effective. Furthermore, trials should provide a rationale for why psychosis is excluded so that interventions could be developed to reduce barriers (e.g., support for decisional capacity to consent to research).
It is possible that existing suicide prevention interventions do not require modification for use with people with psychosis, but in the absence of specialized research, licensed practitioners may consider how suicide prevention interventions may need to be adapted due to unique facets of working with this population. For instance, people who have a schizophrenia spectrum disorder may experience cognitive impairments (115–119), so compensatory strategies may help with intervention retention and skill use. Additionally, positive psychosis symptoms such as hallucinations may be indicators of greater risk for suicide thoughts or behaviors (10, 120, 121), and their assessment should be incorporated into interventions if applicable. Furthermore, people with psychosis may have limited social supports (122–125). Lacking social connection may be associated with increased suicidal desire (e.g., thwarted belongingness and perceived burdensomeness (126)) and a higher risk for future suicide attempt or death if social contacts are not listed on their suicide safety plan (127). People with psychosis may be less likely to use crisis lines (128) and interventions exist to practice and gain exposure to crisis line calls and safety planning may need to be augmented (e.g., 129). See examples of interventions that have explicitly been adapted for psychosis in Table 2.
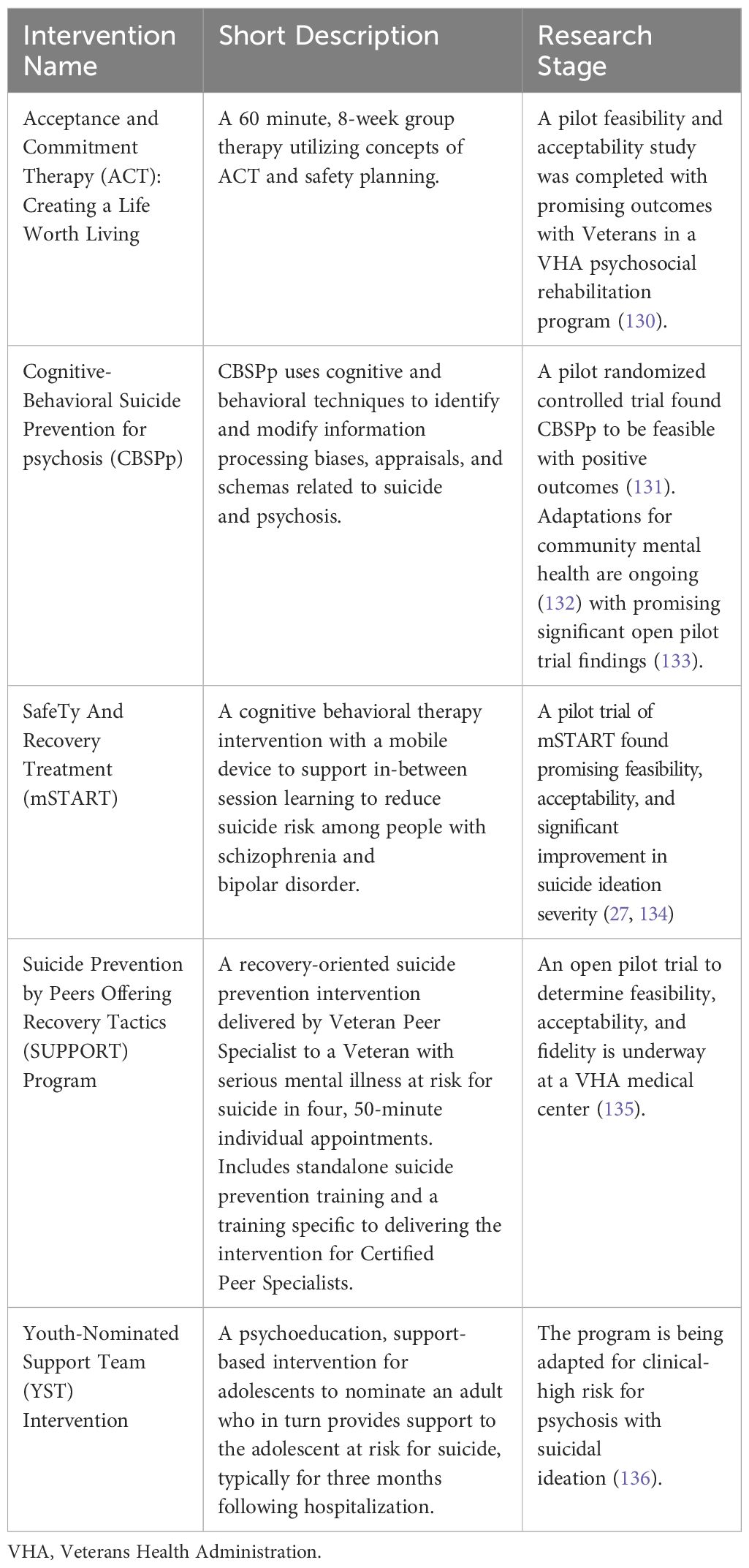
Table 2 Examples of suicide-focused interventions that have explicitly been adapted for psychosis.
Suicide is a critical public health issue among individuals with psychosis. Although progress has been made in research and clinical care for individuals at risk for suicide and experiencing psychosis, important gaps remain. This paper presented three major areas for attention and action, including: 1) implement research design standards that consider the heterogeneity of both psychosis and suicide thoughts and behaviors, 2) determine the impact and utility of suicide risk screening and assessment tools in psychosis populations, and 3) determine effective psychosocial interventions and therapies that directly target suicide risk among persons with psychosis. In addition to the above recommendations, there are two additional points we would like to highlight. First, funding agencies should seek to increase funding opportunities at the intersection of suicide and psychosis to support critically needed research in these areas to impact practice and policy. Second, trainings should be developed, tested, and implement to prepare providers with competency and effectiveness in treating suicide risk and psychosis. Overall, the action steps provided in the areas above aim to provide a framework for addressing these critical gaps in research.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
SC: Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. RS: Conceptualization, Writing – original draft, Writing – review & editing. LB: Writing – review & editing, Writing – original draft, Conceptualization. EP: Conceptualization, Writing – original draft, Writing – review & editing. HW: Writing – original draft, Writing – review & editing. BE: Writing – review & editing, Writing – original draft. JD: Writing – original draft, Writing – review & editing. CD: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported in part by CDA Award Number IK2RX004239-01 from the United States (U.S.) Department of Veterans Affairs; Rehabilitation Research and Development Service, awarded to SC. RS was supported by a Canadian Institutes of Health Research (CIHR) Vanier Canada Graduate Scholarship. Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number F31MH131368, awarded to EP. This project was supported by YIG-0-184-20 awarded to HW from the American Foundation for Suicide Prevention.
SC and BE disclose past financial support from CAMS-care a consulting/training company, and SC discloses past financial support from the Zero Suicide Institute. MG discloses consulting with Boerhinger-Ingelheim and WCG Clinical.
Author BE was employed by company Lyra Health.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The contents do not represent the views of the U.S. Department of Veterans Affairs, the United States Government, the American Foundation for Suicide Prevention, Lyra Health, or the University of California, San Diego. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
1. Zaheer J, Olfson M, Mallia E, Lam JSH, de Oliveira C, Rudoler D, et al. Predictors of suicide at time of diagnosis in schizophrenia spectrum disorder: A 20-year total population study in Ontario, Canada. Schizophr Res. (2020) 222:382–8. doi: 10.1016/j.schres.2020.04.025
2. Nordentoft M, Wahlbeck K, Hällgren J, Westman J, Ösby U, Alinaghizadeh H, et al. Excess mortality, causes of death and life expectancy in 270,770 patients with recent onset of mental disorders in Denmark, Finland and Sweden. PloS One. (2013) 8:e55176. doi: 10.1371/journal.pone.0055176
3. Too LS, Spittal MJ, Bugeja L, Reifels L, Butterworth P, Pirkis J. The association between mental disorders and suicide: A systematic review and meta-analysis of record linkage studies. J Affect Disord. (2019) 259:302–13. doi: 10.1016/j.jad.2019.08.054
4. Dutta R, Murray RM, Hotopf M, Allardyce J, Jones PB, Boydell J. Reassessing the long-term risk of suicide after a first episode of psychosis. Arch Gen Psychiatry. (2010) 67:1230–7. doi: 10.1001/archgenpsychiatry.2010.157
5. Hor K, Taylor M. Suicide and schizophrenia: A systematic review of rates and risk factors. J Psychopharmacol. (2010) 24:81–90. doi: 10.1177/1359786810385490
6. Palmer BA, Pankratz VS, Bostwick JM. The lifetime risk of suicide in schizophrenia: A reexamination. Arch Gen Psychiatry . (2005) 62:247–53. doi: 10.1001/archpsyc.62.3.247
7. Bornheimer LA, Zhang A, Li J, Hiller M, Tarrier N. Effectiveness of suicide-focused psychosocial interventions in psychosis: A systematic review and meta-analysis. Psychiatr Services. (2020) 71:829–38. doi: 10.1176/appi.ps.201900487
8. Yates K, Lång U, Cederlöf M, Boland F, Taylor P, Cannon M, et al. Association of psychotic experiences with subsequent risk of suicidal ideation, suicide attempts, and suicide deaths: A systematic review and meta-analysis of longitudinal population studies. JAMA Psychiatry Am Med Assoc. (2019) 76:180–9. doi: 10.1001/jamapsychiatry.2018.3514
9. Chapman CL, Mullin K, Ryan CJ, Kuffel A, Nielssen O, Large MM. Meta-analysis of the association between suicidal ideation and later suicide among patients with either a schizophrenia spectrum psychosis or a mood disorder. Acta Psychiatr Scand. (2015) 131:162–73. doi: 10.1111/acps.12359
10. Huang X, Fox KR, Ribeiro JD, Franklin JC. Psychosis as a risk factor for suicidal thoughts and behaviors: A meta-analysis of longitudinal studies. Psychol Med. (2018) 48:765–76. doi: 10.1017/S0033291717002136
11. Duko B, Ayano G. Suicidal ideation and attempts among people with severe mental disorder, Addis Ababa, Ethiopia, comparative cross-sectional study. Ann Gen Psychiatry. (2018) 17:1–5. doi: 10.1186/s12991-018-0193-3
12. Pompili M, Amador XF, Girardi P, Harkavy-Friedman J, Harrow M, Kaplan K, et al. Suicide risk in schizophrenia: Learning from the past to change the future. Ann Gen Psychiatry. (2007) 6:10. doi: 10.1186/1744-859X-6-10
13. Suokas JT, Perälä J, Suominen K, Saarni S, Lönnqvist J, Suvisaari JM. Epidemiology of suicide attempts among persons with psychotic disorder in the general population. Schizophr Res. (2010) 124:22–8. doi: 10.1016/j.schres.2010.09.009
14. Jorm AF. Using the Delphi expert consensus method in mental health research. Aust New Z J Psychiatry. (2015) 49:887–97. doi: 10.1177/0004867415600891
15. Crosby A, Ortega L, Melanson C, National Center for Injury Prevention and Control (U.S.), Division of Violence Prevention. Self-directed violence surveillance; uniform definitions and recommended data elements (2011). Available online at: https://stacks.cdc.gov/view/cdc/11997.
16. Wastler HM, Khazem LR, Ammendola E, Baker JC, Bauder CR, Tabares J, et al. An empirical investigation of the distinction between passive and active ideation: Understanding the latent structure of suicidal thought content. Suicide Life Threat Behav. (2023) 53:219–26. doi: 10.1111/sltb.12935
17. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
18. Fusar-Poli P, Borgwardt S, Bechdolf A, Addington J, Riecher-Rössler A, Schultze-Lutter F, et al. The psychosis high-risk state. JAMA Psychiatry. (2013) 70:107. doi: 10.1001/jamapsychiatry.2013.269
19. Olsen KA, Rosenbaum B. Prospective investigations of the prodromal state of schizophrenia: Assessment instruments. Acta Psychiatr Scand. (2006) 113:273–82. doi: 10.1111/j.1600-0447.2005.00698.x
20. Taylor PJ, Hutton P, Wood L. Are people at risk of psychosis also at risk of suicide and self-harm? A systematic review and meta-analysis. Psychol Med. (2015) 45:911–26. doi: 10.1017/S0033291714002074
21. McGorry PD, Yung AR, Phillips LJ. The “Close-in” or ultra high-risk model: A safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr Bull. (2003) 29:771–90. doi: 10.1093/oxfordjournals.schbul.a007046
22. Tandon R, Nasrallah HA, Keshavan MS. Schizophrenia, “just the facts” 4. Clin features conceptualization. Schizophr Res. (2009) 110:1–23. doi: 10.1016/j.schres.2009.03.005
23. Álvarez A, Guàrdia A, González-Rodríguez A, Betriu M, Palao D, Monreal JA, et al. A systematic review and meta-analysis of suicidality in psychotic disorders: Stratified analyses by psychotic subtypes, clinical setting and geographical region. Neurosci Biobehav Rev. (2022) 143:104964. doi: 10.1016/j.neubiorev.2022.104964
24. Fleurence R, Selby JV, Odom-Walker K, Hunt G, Meltzer D, Slutsky JR, et al. How the Patient-Centered Outcomes Research Institute is engaging patients and others in shaping its research agenda. Health Aff. (2013) 32:393–400. doi: 10.1377/hlthaff.2012.1176
25. Watling D, Preece M, Hawgood J, Bloomfield S, Kõlves K. Developing an intervention for suicide prevention: A rapid review of lived experience involvement. Arch Suicide Res. (2022) 26:465–80. doi: 10.1080/13811118.2020.1833799
26. Schlichthorst M, Ozols I, Reifels L, Morgan A. Lived experience peer support programs for suicide prevention: A systematic scoping review. Int J Ment Health Systems. BioMed Cent Ltd. (2020) 14:65. doi: 10.1186/s13033-020-00396-1
27. Depp C, Parrish E, Chalke S, Ehret B, Kamarsu S, Perivoliotis D, et al. Pilot feasibility trial of a brief mobile augmented suicide prevention intervention for serious mental illness. Psychiatr Rehabil J. (2022) 46(1):74–82. doi: 10.1037/prj0000547
28. Bertulies-Esposito B, Sicotte R, Iyer SN, Delfosse C, Girard N, Nolin M, et al. Early detection and intervention for psychosis: Why and how? Sante Ment Que. (2021) 46:45–83. doi: 10.7202/1088178ar
29. Malla AM, Norman RM. Treating psychosis: Is there more to early intervention than intervening early? The Canadian. J Psychiatry. (2001) 46:645–8. doi: 10.1177/070674370104600710
30. DeVylder JE, Anglin D, Munson MR, Nishida A, Oh H, Marsh J, et al. Ethnoracial variation in risk for psychotic experiences. Schizophr Bull. (2023) 49:385–96. doi: 10.1093/schbul/sbac171
31. Bresnahan M, Begg MD, Brown A, Schaefer C, Sohler N, Insel B, et al. Race and risk of schizophrenia in a US birth cohort: Another example of health disparity? Int J Epidemiol. (2007) 36:751–8. doi: 10.1093/ije/dym041
32. Anglin DM, Ereshefsky S, Klaunig MJ, Bridgwater MA, Niendam TA, Ellman LM, et al. From womb to neighborhood: A racial analysis of social determinants of psychosis in the United States. Am J Psychiatry. (2021) 178:599–610. doi: 10.1176/appi.ajp.2020.20071091
33. Forte A, Trobia F, Gualtieri F, Lamis DA, Cardamone G, Giallonardo V, et al. Suicide risk among immigrants and ethnic minorities: A literature overview. Int J Environ Res Public Health. (2018) 15:1438. doi: 10.3390/ijerph15071438
34. Lee CS, Sirin SR, Choi E, Sin EJ. Meta-Analysis of acculturation and suicide-related outcomes: A test of the immigrant paradox. J Racial Ethn Health Disparities. (2023) 11(2):913–27. doi: 10.1007/s40615-023-01572-y
35. Troya MI, Spittal MJ, Pendrous R, Crowley G, Gorton HC, Russell K, et al. Suicide rates amongst individuals from ethnic minority backgrounds: A systematic review and meta-analysis. EClinicalMedicine. (2022) 47:101399. doi: 10.1016/j.eclinm.2022.101399
36. Weisman de Mamani A, Lopez D. Enculturation and acculturation’s relationship to suicidal ideation in Hispanic/Latinx individuals with psychotic spectrum disorders. Psychiatry Res. (2022) 307:114298. doi: 10.1016/j.psychres.2021.114298
37. Termorshuizen F, Wierdsma AI, Visser E, Drukker M, Sytema S, Laan W, et al. Psychosis and suicide risk by ethnic origin and history of migration in the Netherlands. Schizophr Res. (2012) 138:268–73. doi: 10.1016/j.schres.2012.03.035
38. Robinson J, Krysinska K. Youth suicide prevention in low-income and middle-income countries. Lancet Child Adolesc Health. (2019) 3:200–1. doi: 10.1016/S2352-4642(19)30002-1
39. Aggarwal S, Patton G, Reavley N, Sreenivasan SA, Berk M. Youth self-harm in low- and middle-income countries: Systematic review of the risk and protective factors. Int J Soc Psychiatry. (2018) 63:359–75. doi: 10.1177/0020764017700175
40. Robinson J, Bailey E, Witt K, Stefanac N, Milner A, Currier D, et al. What works in youth suicide prevention? A systematic review and meta-analysis. EClinicalMedicine. (2018) 4–5:52–91. doi: 10.1016/j.eclinm.2018.10.004
41. Fleischmann A, Arensman E, Berman A, Carli V, De Leo D, Hadlaczky G, et al. Overview evidence on interventions for population suicide with an eye to identifying best-supported strategies for LMICs. Global Ment Health. (2016) 3:e5. doi: 10.1017/gmh.2015.27
42. Lu L, Dong M, Zhang L, Zhu XM, Ungvari GS, Ng CH, et al. Prevalence of suicide attempts in individuals with schizophrenia: A meta-analysis of observational studies. Epidemiol Psychiatr Sci. (2020) 29:e39. doi: 10.1017/S2045796019000313
43. Bai W, Liu ZH, Jiang YY, Zhang QE, Rao WW, Cheung T, et al. Worldwide prevalence of suicidal ideation and suicide plan among people with schizophrenia: A meta-analysis and systematic review of epidemiological surveys. Transl Psychiatry. (2021) 11:1–10. doi: 10.1038/s41398-021-01671-6
44. Altamura AC, Mundo E, Bassetti R, Green A, Lindenmayer JP, Alphs L, et al. Transcultural differences in suicide attempters: Analysis on a high-risk population of patients with schizophrenia or schizoaffective disorder. Schizophr Res. (2007) 89:140–6. doi: 10.1016/j.schres.2006.08.023
45. Bhatia T, Thomas P, Semwal P, Thelma BK, Nimgaonkar VL, Deshpande SN. Differing correlates for suicide attempts among patients with schizophrenia or schizoaffective disorder in India and USA. Schizophr Res. (2006) 86:208–14. doi: 10.1016/j.schres.2006.04.015
46. Wüsten C, Schlier B, Jaya ES, Alizadeh BZ, Bartels-Velthuis AA, van Beveren NJ, et al. Psychotic experiences and related distress: A cross-national comparison and network analysis based on 7141 participants from 13 countries. Schizophr Bull. (2018) 44:1185–94. doi: 10.1093/schbul/sby087
47. DeVylder JE, Koyanagi A. Evaluating the clinical relevance of psychotic experiences in low- and middle-income countries. Schizophr Bull. (2018) 44:1167–9. doi: 10.1093/schbul/sby120
48. Hatchel T, Polanin JR, Espelage DL. Suicidal thoughts and behaviors among LGBTQ youth: Meta-analyses and a systematic review. Arch Suicide Res. (2021) 25:1–37. doi: 10.1080/13811118.2019.1663329
49. Marshal MP, Dietz LJ, Friedman MS, Stall R, Smith HA, McGinley J, et al. Suicidality and depression disparities between sexual minority and heterosexual youth: A meta-analytic review. J Adolesc Health. (2011) 49:115–23. doi: 10.1016/j.jadohealth.2011.02.005
50. de Lange J, Baams L, van Bergen DD, Bos HMW, Bosker RJ. Minority stress and suicidal ideation and suicide attempts among LGBT adolescents and young adults: A meta-analysis. LGBT Health. (2022) 9:222–37. doi: 10.1089/lgbt.2021.0106
51. Barr SM, Roberts D, Thakkar KN. Psychosis in transgender and gender non-conforming individuals: A review of the literature and a call for more research. Psychiatry Res. (2021) 306:114272. doi: 10.1016/j.psychres.2021.114272
52. Savill M, Nguyen T, Shim RS, Loewy RL. Online psychosis screening: Characterizing an underexamined population to improve access and equity. Psychiatr Services. (2022) 73:1005–12. doi: 10.1176/appi.ps.202100257
53. LGBTQ. Subcommittee of the UCSD. San Diego: Department of Psychiatry. LGBTQ+ Fact Sheet For Researchers (2022).
54. Hughes JL, Camden AA, Yangchen T, Smith GPA, Domenech Rodríguez MM, Rouse SV, et al. Guidance for researchers when using inclusive demographic questions for surveys: Improved and updated questions. Psi Chi J psychol Res. (2022) 27:232–55. doi: 10.24839/2325-7342.JN
55. Hielscher E, DeVylder JE, Saha S, Connell M, Scott JG. Why are psychotic experiences associated with self-injurious thoughts and behaviors? A systematic review and critical appraisal of potential confounding and mediating factors. Psychol Med. (2018) 48:1410–26. doi: 10.1017/S0033291717002677
56. Cassidy RM, Yang F, Kapczinski F, Passos IC. Risk factors for suicidality in patients with schizophrenia: A systematic review, meta-analysis, and meta-regression of 96 studies. Schizophr Bull. (2018) 44:787–97. doi: 10.1093/schbul/sbx131
57. Sicotte R, Iyer SN, Kiepura B, Abdel-Baki A. A systematic review of longitudinal studies of suicidal thoughts and behaviors in first-episode psychosis: Course and associated factors. Soc Psychiatry Psychiatr Epidemiol. (2021) 1:1–38. doi: 10.1007/s00127-021-02153-2
58. Murphy J, Shevlin M, Arseneault L, Bentall R, Caspi A, Danese A, et al. Externalizing the threat from within: A new direction for researching associations between suicide and psychotic experiences. Dev Psychopathol. (2022) 34:1034–44. doi: 10.1017/S0954579420001728
59. Stanyon D, DeVylder J, Yamasaki S, Yamaguchi S, Ando S, Usami S, et al. Auditory hallucinations and self-injurious behavior in general population adolescents: Modeling within-person effects in the Tokyo teen cohort. Schizophr Bull. (2023) 49:329–38. doi: 10.1093/schbul/sbac155
60. Perälä J, Suvisaari J, Saarni SI, Kuoppasalmi K, Isometsä E, Pirkola S, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry. (2007) 64:19. doi: 10.1001/archpsyc.64.1.19
61. National Institutes of Health. Scientific Data Sharing: Data Management and Sharing Policy (2023). Available online at: https://sharing.nih.gov/data-management-and-sharing-policy.
62. National Institutes of Health. The National Institute of Mental Health Data Archive (NDA) (2023). Available online at: https://nda.nih.gov/.
63. McGill University. MAP-PRO (2023). Available online at: https://www.mcgill.ca/mappro/.
64. Ferrari M, Pawliuk N, Pope M, MacDonald K, Boruff J, Shah J, et al. A scoping review of measures used in early intervention services for psychosis. Psychiatr Services. (2023) 74:523–33. doi: 10.1176/appi.ps.202100506
65. Ammerman BA, Burke TA, Jacobucci R, McClure K. How we ask matters: The impact of question wording in single-item measurement of suicidal thoughts and behaviors. Prev Med (Baltim). (2021) 152:106472. doi: 10.1016/j.ypmed.2021.106472
66. Baca-Garcia E, Perez-Rodriguez MM, Oquendo MA, Keyes KM, Hasin DS, Grant BF, et al. Estimating risk for suicide attempt: Are we asking the right questions? Passive suicidal ideation as a marker for suicidal behavior. J Affect Disord. (2011) 134:327–32. doi: 10.1016/j.jad.2011.06.026
67. Polihronis C, Cloutier P, Kaur J, Skinner R, Cappelli M. What’s the harm in asking? A systematic review and meta-analysis on the risks of asking about suicide-related behaviors and self-harm with quality appraisal. Arch Suicide Res. (2022) 26:325–47. doi: 10.1080/13811118.2020.1793857
68. Gould MS, Marrocco FA, Kleinman M, Thomas JG, Mostkoff K, Cote J, et al. Evaluating iatrogenic risk of youth suicide screening programs. JAMA. (2005) 293:1635. doi: 10.1001/jama.293.13.1635
69. Blades CA, Stritzke WGK, Page AC, Brown JD. The benefits and risks of asking research participants about suicide: A meta-analysis of the impact of exposure to suicide-related content. Clin Psychol Rev. (2018) 64:1–12. doi: 10.1016/j.cpr.2018.07.001
70. Horowitz LM, Bridge JA, Teach SJ, Ballard E, Klima J, Rosenstein DL, et al. Ask suicide-screening questions (ASQ): A brief instrument for the pediatric emergency department. Arch Pediatr Adolesc Med. (2012) 166:1170–6. doi: 10.1001/archpediatrics.2012.1276
71. Horowitz LM, Snyder DJ, Boudreaux ED, He JP, Harrington CJ, Cai J, et al. Validation of the ask suicide-screening questions for adult medical inpatients: A brief tool for all ages. Psychosomatics. (2020) 61:713–22. doi: 10.1016/j.psym.2020.04.008
72. Horowitz LM, Mournet AM, Sheftall A, He JP, Lowry NJ, Aguinaldo LD, et al. Assessing the validity of the Ask Suicide-Screening Questions (ASQ) in black youth. J Acad Consult Liaison Psychiatry. (2022) 64(4):332–5. doi: 10.1016/j.jaclp.2022.10.001
73. Beck AT, Brown GK, Steer RA. Psychometric characteristics of the scale for suicide ideation with psychiatric outpatients. Behav Res Ther. (1997) 35:1039–46. doi: 10.1016/S0005-7967(97)00073-9
74. Riblet NB, Matsunaga S, Shiner B, Schnurr PP, Watts BV. Are suicide risk scales sensitive to change? A scoping review. J Psychiatr Res. (2023) 161:170–8. doi: 10.1016/j.jpsychires.2023.03.007
75. Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, et al. The Columbia–suicide severity rating scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. (2011) 168:1266–77. doi: 10.1176/appi.ajp.2011.10111704
76. Posner K, Brent D, Lucas C, Gould M, Stanley B, Brown G, et al. Columbia-suicide severity rating scale (C-SSRS). New York, NY: Columbia University Medical Center (2008). p. 10.
77. Cha M, Al-Chalabi N, Qian J, Chaudhary Z, Graff A, Gerretsen P, et al. Concordance between the Columbia-Suicide Severity Rating Scale and Beck Scale for Suicide Ideation in assessing suicide behavior in young adults with schizophrenia spectrum disorders. Psychiatry Res. (2023) 319:114965. doi: 10.1016/j.psychres.2022.114965
78. Paksarian D, Mojtabai R, Kotov R, Cullen B, Nugent KL, Bromet EJ. Perceived trauma during hospitalization and treatment participation among individuals with psychotic disorders. Psychiatr Services. (2014) 65:266–9. doi: 10.1176/appi.ps.201200556
79. Lu W, Mueser KT, Rosenberg SD, Yanos PT, Mahmoud N. Posttraumatic reactions to psychosis: A qualitative analysis. Front Psychiatry. (2017) 8. doi: 10.3389/fpsyt.2017.00129
80. MacBeth A, Gumley A, Schwannauer M, Carcione A, Fisher R, McLeod HJ, et al. Metacognition, symptoms and premorbid functioning in a First Episode Psychosis sample. Compr Psychiatry. (2014) 55:268–73. doi: 10.1016/j.comppsych.2013.08.027
81. Drake RJ. Insight into illness: Impact on diagnosis and outcome of nonaffective psychosis. Curr Psychiatry Rep. (2008) 10:210–6. doi: 10.1007/s11920-008-0035-0
82. Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: A systematic review and meta-analysis. Soc Sci Med. (2010) 71:2150–61. doi: 10.1016/j.socscimed.2010.09.030
83. Thompson AH, Stuart H, Bland RC, Arboleda-Florez J, Warner R, Dickson RA. Attitudes about schizophrenia from the pilot site of the WPA worldwide campaign against the stigma of schizophrenia. Soc Psychiatry Psychiatr Epidemiol. (2002) 37:475–82. doi: 10.1007/s00127-002-0583-2
84. Angermeyer MC, Matschinger H, Schomerus G. Attitudes towards psychiatric treatment and people with mental illness: changes over two decades. Br J Psychiatry. (2013) 203:146–51. doi: 10.1192/bjp.bp.112.122978
85. Wastler HM, Lucksted A, Phalen P, Drapalski A. Internalized stigma, sense of belonging, and suicidal ideation among veterans with serious mental illness. Psychiatr Rehabil J. (2020) 43:91–6. doi: 10.1037/prj0000386
86. Xu Z, Müller M, Heekeren K, Theodoridou A, Metzler S, Dvorsky D, et al. Pathways between stigma and suicidal ideation among people at risk of psychosis. Schizophr Res. (2016) 172:184–8. doi: 10.1016/j.schres.2016.01.048
87. Hunt IM, Kapur N, Windfuhr K, Robinson J, Bickley H, Flynn S, et al. Suicide in schizophrenia: Findings from a national clinical survey. J Psychiatr Pract. (2006) 12:139–47. doi: 10.1097/00131746-200605000-00002
88. Melle I, Johannessen JO, Friis S, Haahr U, Joa I, Larsen TK, et al. Course and predictors of suicidality over the first two years of treatment in first-episode schizophrenia spectrum psychosis. Arch Suicide Res. (2010) 14:158–70. doi: 10.1080/13811111003704787
89. Harkavy-Friedman JM, Kimhy D, Nelson EA, Venarde DF, Malaspina D, Mann JJ. Suicide attempts in schizophrenia: The role of command auditory hallucinations for suicide. J Clin Psychiatry. (2003) 64:871–4. doi: 10.4088/JCP.v64n0803
90. Jay SY, DeVylder JE, Schiffman J, Pitts SC, Marsh J, Zhou S, et al. Exploring the relation between psychosis-like experiences and suicidal ideation, plans, and attempts among college students in the United States. Early Interv Psychiatry. (2023) 17:272–80. doi: 10.1111/eip.13325
91. Hielscher E, DeVylder JE, Connell M, Hasking P, Martin G, Scott JG. Investigating the role of hallucinatory experiences in the transition from suicidal thoughts to attempts. Acta Psychiatr Scand. (2020) 141:241–53. doi: 10.1111/acps.13128
92. Barbeito S, Vega P, Sánchez-Gutiérrez T, Becerra JA, González-Pinto A, Calvo A. A systematic review of suicide and suicide attempts in adolescents with psychotic disorders. Schizophr Res. (2021) 235:80–90. doi: 10.1016/j.schres.2021.07.029
93. Ehret BC, Titone MK, Carey CJ, Martinez A, Chalker SA, Granholm EL, et al. Are all reasons for living made equally? Reasons for living and dysfunctional attitudes in psychotic disorders and bipolar I. Psychol Psychotherapy: Theory Res Pract. (2023) 2023:748–61. doi: 10.1111/papt.12466
94. Baldessarini RJ, Innamorati M, Erbuto D, Serafini G, Fiorillo A, Amore M, et al. Differential associations of affective temperaments and diagnosis of major affective disorders with suicidal behavior. J Affect Disord. (2017) 210:19–21. doi: 10.1016/j.jad.2016.12.003
95. Chong BTW, Wahab S, Muthukrishnan A, Tan KL, Ch’ng ML, Yoong MT. Prevalence and factors associated with suicidal ideation in institutionalized patients with schizophrenia. Psychol Res Behav Manag. (2020) 13:949–62. doi: 10.2147/PRBM.S266976
96. DeVylder JE, Lukens EP, Link BG, Lieberman JA. Suicidal ideation and suicide attempts among adults with psychotic experiences. JAMA Psychiatry. (2015) 72:219. doi: 10.1001/jamapsychiatry.2014.2663
97. Pompili M, Lester D, Grispini A, Innamorati M, Calandro F, Iliceto P, et al. Completed suicide in schizophrenia: Evidence from a case-control study. Psychiatry Res. (2009) 167:251–7. doi: 10.1016/j.psychres.2008.03.018
98. Pompili M, Baldessarini RJ, Innamorati M, Vázquez GH, Rihmer Z, Gonda X, et al. Temperaments in psychotic and major affective disorders. J Affect Disord. (2018) 225:195–200. doi: 10.1016/j.jad.2017.08.026
99. Bornheimer LA, Jaccard J. Symptoms of depression, positive symptoms of psychosis, and suicidal ideation among adults diagnosed with schizophrenia within the clinical antipsychotic trials of intervention effectiveness. Arch Suicide Res. (2017) 21:633–45. doi: 10.1080/13811118.2016.1224990
100. Bornheimer LA, Wojtalik JA, Li J, Cobia D, Smith MJ. Suicidal ideation in first-episode psychosis: Considerations for depression, positive symptoms, clinical insight, and cognition. Schizophr Res. (2021) 228:298–304. doi: 10.1016/j.schres.2020.12.025
101. DeVylder JE, Jahn DR, Doherty T, Wilson CS, Wilcox HC, Schiffman J, et al. Social and psychological contributions to the co-occurrence of sub-threshold psychotic experiences and suicidal behavior. Soc Psychiatry Psychiatr Epidemiol. (2015) 50:1819–30. doi: 10.1007/s00127-015-1139-6
102. Villa J, Ehret BC, Depp CA. Systematic review of the inclusion of people with psychosis in suicide-specific clinical trials. Crisis: J Crisis Intervention Suicide Prev. (2020) 41:233–6. doi: 10.1027/0227-5910/a000628
103. Stroup TS, McEvoy JP, Swartz MS, Byerly MJ, Glick ID, Canive JM, et al. The National Institute of Mental Health Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Project: Schizophrenia trial design and protocol development. Schizophr Bull. (2003) 29:15–31. doi: 10.1093/oxfordjournals.schbul.a006986
104. Kane JM, Schooler NR, Marcy P, Correll CU, Brunette MF, Mueser KT, et al. The RAISE Early treatment program for first-episode psychosis: Background, rationale, and study design. J Clin Psychiatry. (2015) 76:240–6. doi: 10.4088/JCP.14m09289
105. Kane JM, Robinson DG, Schooler NR, Mueser KT, Penn DL, Rosenheck RA, et al. Comprehensive versus usual community care for first-episode psychosis: 2-year outcomes from the NIMH RAISE early treatment program. Am J Psychiatry. (2016) 173:362–72. doi: 10.1176/appi.ajp.2015.15050632
106. Swartz MS, Stroup TS, McEvoy JP, Davis SM, Rosenheck RA, Keefe RSE, et al. What CATIE found: Results from the schizophrenia trial. Psychiatr Services. (2008) 59:500–6. doi: 10.1176/appi.ps.59.5.500
107. Mueser KT, Cook JA. Rising to the challenge of first episode psychosis: The NIMH Recovery After Initial Schizophrenia Episode (RAISE) initiative. Psychiatr Rehabil J. (2014) 37:267–9. doi: 10.1037/prj0000108
108. Bryan CJ, Rudd MD. Brief cognitive-behavioral therapy for suicide prevention. New York, New York: Guilford Press (2018).
109. Rudd MD, Bryan CJ, Wertenberger EG, Peterson AL, Young-McCaughan S, Mintz J, et al. Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: Results of a randomized clinical trial with 2-year follow-up. Am J Psychiatry. (2015) 172:441–9. doi: 10.1176/appi.ajp.2014.14070843
110. Brown GK, Have TT, Henriques GR, Xie SX, Hollander JE, Beck AT. Cognitive therapy for the prevention of suicide attempts: A randomized controlled trial. JAMA. (2005) 294:563–70. doi: 10.1001/jama.294.5.563
111. Swift JK, Trusty WT, Penix EA. The effectiveness of the collaborative assessment and management of suicidality (CAMS) compared to alternative treatment conditions: A meta-analysis. Suicide Life Threat Behav. (2021) 51(5):882–96. doi: 10.1111/sltb.12765
112. Miller AB, Oppenheimer CW, Glenn CR, Yaros AC. Preliminary research priorities for factors influencing individual outcomes for users of the US National Suicide Prevention Lifeline. JAMA Psychiatry. (2022) 79:1225. doi: 10.1001/jamapsychiatry.2022.3270
113. Sale E, Hendricks M, Weil V, Miller C, Perkins S, McCudden S. Counseling on Access to Lethal Means (CALM): An evaluation of a suicide prevention means restriction training program for mental health providers. Community Ment Health J. (2018) 54:293–301. doi: 10.1007/s10597-017-0190-z
114. Nuij C, van Ballegooijen W, de Beurs D, Juniar D, Erlangsen A, Portzky G, et al. Safety planning-type interventions for suicide prevention: Meta-analysis. Br J Psychiatry. (2021) 219(2):1–8. doi: 10.1192/bjp.2021.50
115. Stergiopoulos V, Cusi A, Bekele T, Skosireva A, Latimer E, Schütz C, et al. Neurocognitive impairment in a large sample of homeless adults with mental illness. Acta Psychiatr Scand. (2015) 131:256–68. doi: 10.1111/acps.12391
116. Velligan DI, Mahurin RK, Diamond PL, Hazleton BC, Eckert SL, Miller AL. The functional significance of symptomatology and cognitive function in schizophrenia. Schizophr Res. (1997) 25:21–31. doi: 10.1016/S0920-9964(97)00010-8
117. Twamley EW, Doshi RR, Nayak GV, Palmer BW, Golshan S, Heaton RK, et al. Generalized cognitive impairments, ability to perform everyday tasks, and level of independence in community living situations of older patients with psychosis. Am J Psychiatry. (2002) 159:2013–20. doi: 10.1176/appi.ajp.159.12.2013
118. Green MF, Kern RS, Heaton RK. Longitudinal studies of cognition and functional outcome in schizophrenia: Implications for MATRICS. Schizophr Res. (2004) 72(1):41–51. doi: 10.1016/j.schres.2004.09.009
119. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. (1996) 153:321–30. doi: 10.1176/ajp.153.3.321
120. DeVylder JE, Hilimire MR. Suicide risk, stress sensitivity, and self-esteem among young adults reporting auditory hallucinations. Health Soc Work. (2015) 40:175–81. doi: 10.1093/hsw/hlv037
121. Comparelli A, Corigliano V, Lamis DA, De Carolis A, Stampatore L, De Pisa E, et al. Positive symptoms and social cognition impairment affect severity of suicidal ideation in schizophrenia. Schizophr Res. (2018) 193:470–1. doi: 10.1016/j.schres.2017.07.027
122. Kilbourne AM, McCarthy JF, Post EP, Welsh D, Blow FC. Social support among veterans with serious mental illness. Soc Psychiatry. Psychiatr Epidemiol. (2007) 42:639–46. doi: 10.1007/s00127-007-0212-1
123. Chronister J, Chou CC, Kwan KLK, Lawton M, Silver K. The meaning of social support for persons with serious mental illness. Rehabil Psychol. (2015) 60:232–45. doi: 10.1037/rep0000038
124. Hendryx M, Green CA, Perrin NA. Social support, activities, and recovery from serious mental illness: STARS study findings. J Behav Health Serv Res. (2009) 36:320–9. doi: 10.1007/s11414-008-9151-1
125. Corrigan PW, Phelan SM, Corrigan P. Social support and recovery in people with serious mental illnesses. Community Ment Health J. (2004) 40:513–23. doi: 10.1007/s10597-004-6125-5
126. Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE. The interpersonal theory of suicide. Psychol Rev. (2010) 117:575–600. doi: 10.1037/a0018697
127. Chalker SA, Parrish EM, Martinez Ceren CS, Depp CA, Goodman M, Doran N. Predictive importance of social contacts on U.S. Veteran suicide safety plans. Psychiatr Serv. (2022) 74(3):244–9. doi: 10.1176/appi.ps.202100699
128. Chalker SA, Parrish EM, Martinez Ceren CS, Depp CA, Ilgen MA, Goodman M, et al. Crisis service utilization following completion of a suicide safety plan for Veterans with and without affective and nonaffective psychosis. J Psychiatr Res. (2022) 154:219–23. doi: 10.1016/j.jpsychires.2022.07.034
129. Thompson EC, Nail M, Yen S. Suicide risk and psychotic experiences: Considerations for safety planning with adolescents. R I Med J. (2013) 105:26–30.
130. Chalker SA, Ehret BC, Oelschlegel J, Ludwig KA. Creating a Life Worth Living: A pilot study of a suicide prevention-focused Acceptance and Commitment Therapy (ACT)-derived group. In: International Academy of Suicide Research / American Foundation for Suicide Prevention’s International Summit on Suicide Research. Barcelona, Spain (2021).
131. Tarrier N, Kelly J, Maqsood S, Snelson N, Maxwell J, Law H, et al. The cognitive behavioral prevention of suicide in psychosis: A clinical trial. Schizophr Res. (2014) 156:204–10. doi: 10.1016/j.schres.2014.04.029
132. Bornheimer LA, Li Verdugo J, Holzworth J, Im V, Smith FN, Sliwa H, et al. Modifying a cognitive behavioral suicide prevention treatment for adults with schizophrenia spectrum disorders in community mental health. Psychiatry Res. (2022) 311:114505. doi: 10.1016/j.psychres.2022.114505
133. Bornheimer LA, Verdugo JL, Krasnick J, Jeffers N, Storey F, King CA, et al. A cognitive-behavioral suicide prevention treatment for adults with schizophrenia spectrum disorders in community mental health: Preliminary findings of an open pilot study. Soc Work Ment Health. (2023) 21(5):1–23. doi: 10.1080/15332985.2023.2186736
134. Depp C, Ehret B, Villa J, Perivoliotis D, Granholm E. A brief mobile-augmented suicide prevention intervention for people with psychotic disorders in transition from acute to ongoing care: Protocol for a pilot trial. JMIR Res Protoc. (2021) 10:e14378. doi: 10.2196/14378
135. Chalker SA, ClinicalTrials.org. A novel peer-delivered recovery-focused suicide prevention intervention for veterans with serious mental illness (2022). Available online at: https://classic.clinicaltrials.gov/ct2/show/NCT05537376.
136. Schiffman JE, ClinicalTrials.gov. Youth Nominated Support Team (YST) (2022). Available online at: https://classic.clinicaltrials.gov/ct2/show/NCT05558332.
Keywords: suicide, psychosis, suicide behavior, psychotic symptoms, schizophrenia
Citation: Chalker SA, Sicotte R, Bornheimer LA, Parrish EM, Wastler H, Ehret B, DeVylder J and Depp CA (2024) A call to action: informing research and practice in suicide prevention among individuals with psychosis. Front. Psychiatry 15:1378600. doi: 10.3389/fpsyt.2024.1378600
Received: 29 January 2024; Accepted: 22 March 2024;
Published: 22 April 2024.
Edited by:
Tushar Singh, Banaras Hindu University, IndiaReviewed by:
Valentin Matei, Carol Davila University of Medicine and Pharmacy, RomaniaCopyright © 2024 Chalker, Sicotte, Bornheimer, Parrish, Wastler, Ehret, DeVylder and Depp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samantha A. Chalker, c2NoYWxrZXJAaGVhbHRoLnVjc2QuZWR1
†ORCID: Samantha A. Chalker, orcid.org/0000-0002-9523-4197
Roxanne Sicotte, orcid.org/0000-0002-3392-423X
Lindsay A. Bornheimer, orcid.org/0000-0002-4684-5696
Emma M. Parrish, orcid.org/0000-0003-1937-8145
Heather Wastler, orcid.org/0000-0003-1519-6926
Blaire Ehret, orcid.org/0000-0002-4783-9503
Jordan DeVylder, orcid.org/0000-0001-5873-4582
Colin A. Depp, orcid.org/0000-0002-1841-6229
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.