
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Psychiatry , 28 May 2024
Sec. Autism
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1378572
This article is part of the Research Topic Case Reports in Autism: 2023 View all 9 articles
 Barbara Carpita
Barbara Carpita Chiara Bonelli*
Chiara Bonelli* Federico GiovannoniFrancesca ParriMatteo Gambini
Federico GiovannoniFrancesca ParriMatteo Gambini Benedetta Nardi
Benedetta Nardi Giulia Amatori
Giulia Amatori Ivan Mirko CremoneStefano PiniLiliana Dell’Osso
Ivan Mirko CremoneStefano PiniLiliana Dell’OssoDuring the last few decades, a growing field of literature is focusing on hikikomori, a phenomenon described as a form of pathological social withdrawal or social isolation that lasts for more than 6 months leading to significant functional impairment and/or distress. Despite initially considered a culture-bound syndrome, hikikomori syndrome later gained a wider recognition in different countries, ranging from an attempt to take refuge in an idealistic world, when society success’ standards are not reached, to a maladaptive coping strategy complicating several psychiatric illnesses such as anxiety disorders, major depression, internet addiction, internet gaming disorder (IGD) and autism spectrum disorder (ASD). In this framework, difficulties in social interaction, in problem solving strategies and socio-emotional reciprocity, may lead to social withdrawal and hikikomori-like behaviors. In this work, we described two cases of patients where the presence of underlying autism spectrum may have represented a sign of vulnerability towards the development of a possible full-blown case of hikikomori with IGD.
Hikikomori is a Japanese term based on the combination of two words: hiku which means “to pull” and komoru which means “to withdraw” (1). This term became widely used in the second half of the 1990s (2, 3), after the publication of the book “Hikikomori – Adolescence Without End” (4), where it was used to describe “those who withdraw entirely from society and stay in their own homes for more than six months, with onset usually during the latter half of their twenties, and for whom other psychiatric disorders do not better explain the primary causes of this condition”. Initially, hikikomori was believed to be a phenomenon specific to Japanese society but, more recently, instances of this condition have been documented in several other nations, such as South Korea, France, Spain and the United States, and extensive coverage of it has appeared in worldwide media (5–13). The growing interest toward this condition also led to the proposal of two distinct categories of hikikomori: “primary hikikomori” where the social withdrawal is not caused by any comorbid psychiatric disorder, and “secondary hikikomori” where, on the contrary, social withdrawal can be attributed to a psychiatric disorder (14–16). A distinction was also highlighted between “hikikomori in the strict sense” (subjects who do not leave the house or leave it only for going to the convenience store, etc) and “quasi-hikikomori”, who would go out for pursuing their hobbies (17). In this context, the Italian version of the Hikikomori Questionnaire (HQ-25) (18) was recently developed and validated. The questionnaire features 25 items that investigate socialization, isolation and emotional support in suspected hikikomori subjects (19).
Despite the importance of this emerging condition, an agreement about the definition of hikikomori still has to be reached. It is commonly described as a pathological social withdrawal or social isolation that lasts for more than 6 months and causes significant functional impairment and/or distress (20, 21), not caused or influenced by an undergoing psychosis, and where some sort of social contact is not necessary but still allowed over the internet. Despite hikikomori was initially considered a culture-bound syndrome mainly relevant in Japan, it later gained a wider recognition as a syndrome that could be present also in different cultures in specific social conditions, characterized by the youths’ attempt to take refuge in an idealistic world when society success’ standards are not reached (1, 19). Recent literature further reconsidered hikikomori as a maladaptive coping strategy that could complicate several psychiatric illnesses and sometimes even be comparable to an alternative form of suicide attempt (1). In fact, hikikomori is now known to be comorbid with many psychiatric disorders including various anxiety disorders, major depression, personality disorders, internet addiction and internet gaming disorder (IGD) (10, 22–25). In particular, some authors highlighted how hikikomori and IGD may reinforce each other in a vicious circle, with hikikomori condition opening the way to the use of internet as a tool to communicate with the outside world and escaping towards videogames, while IGD would enhance the tendency towards social withdrawal for spending more time playing (26, 27). It has also been highlighted that hikikomori co-occurs in around one-third of those with autism spectrum disorder (ASD), which, in turn, has been associated with IGD (14, 25, 27–31).
Autism spectrum disorder (ASD) is a heterogeneous neurodevelopmental condition with varying degrees of symptom severity and with or without intellectual impairment. Its core symptoms are represented by pervasive impairment in reciprocal and social communication and interactions, restricted interests, repetitive, stereotyped behaviors, a lack of socio-emotional reciprocity, and impaired sensory integration processing (32). While ASD and hikikomori share some similar manifestations in the area of social skills, hikikomori is characterized in terms of social withdrawal, whereas ASD is defined in terms of social difficulties (33). In recent years studies examining how ASD presents in adults have progressively grown in number, with a particular focus on those mild manifestations without intellectual impairment that frequently remain under-diagnosed for many years (34, 35), coming to clinical attention only after the development of psychiatric comorbidities. Moreover, in the framework of a dimensional approach, sub-threshold autistic traits (AT) have been reported to be continuously distributed from the clinical to the general population is now generally acknowledged, probably sharing their genetic underpinnings with full-fledged clinical forms (36–39). It was also hypothesized that AT could be a vulnerability factor for different psychiatric conditions, also increasing the risk of suicidal ideation and behaviors (40–45). Noticeably, AT have been linked to a worse quality of life and a greater risk of suicidality, even at subthreshold levels (37, 45–48). Even though ASD and hikikomori may share some symptomatologic overlap such as deficits in social reciprocity and social withdrawal and, eventually, restricted and intensively pursued interests, to date the relationship between the two is still poorly investigated in the scientific literature (27). In this framework, it should be noted that a comorbidity with IGD has been reported for both conditions (27). Some studies highlighted that subject diagnosed with hikikomori reports higher AT, showing lower social skills and deficits in communication, imagination, attention span, multitask ability and adaptation to change compared to healthy controls (49), while ASD dysfunctional social interaction, causing deficiencies in introspectiveness and problem-solving strategies, may lead to a low self-esteem and social withdrawal (49, 50). In this work, we reported two cases of patients who manifested a severe social withdrawal comparable to western hikikomori-like syndrome, showing also significant autistic traits and IGD symptoms. Implications of the possible mediating role of AT in the development of hikikomori syndrome are discussed. Both subjects were given comprehensive information about the aim of this work and have been informed of the risks and benefits of allowing personal information to be used in this case report. Moreover, they were given the chance to ask questions prior to completing a written informed consent form.
Mr. X.Y. is a 40-years-old, single South-American man who lives alone in Italy. He reported family history of psychiatric disorders (mother with major depression). Since childhood, he manifested panic-agoraphobic traits and social anxiety symptoms. Furthermore, he also showed relevant obsessive-compulsive traits with a tendency to order and precision, moral rigidity. Mr. X.Y. also displayed since childhood a behavioral pattern characterized by narrow and repetitive interests (a deep interest in manga and anime was maintained until present), strong adherence to routine, difficulties in socio-emotional reciprocity, empathy alterations, hyper-reactivity to sensory input, suggestive of an autism spectrum. Indeed, he described himself as an obstinate and stubborn child with few friends and who would have preferred study at home. He was not interested in other children’s games and had difficulties in establishing new friendships. He loved collecting objects and was extremely careful about his books and toys and did not like others to touch them. As a teenager, excelled in Maths and Physics, while showing poor performances in other fields. He spent the most of his spare time in solitary activities such as playing videogames. He was often teased by schoolmates or bullied during adolescence. Excelled in Maths and Physics, while showing poor performances in other fields.
The onset of clinical history was reported to be at the age of 15 when, subsequently to familiar economic troubles, with the need to move in another house, he developed swings in mood and energy and irritability, lack of motivation in studying, apathy, anhedonia and death thoughts. He did not seek medical help and maintained sufficient school and familiar functioning. At the age of 18, he moved to Italy and enrolled in bachelor program in Engineering. Soon after, he developed emotional lability, asthenia, anhedonia, lack of concentration, subsyndromal panic attacks with cardiorespiratory symptoms, anticipatory and performance anxiety, feelings of worthlessness and overwhelm, with inability to achieve regular academic standards and reduced interpersonal relationships. This clinical picture led to a progressive social withdrawal to the point of staying confined at home for about eight months without ever going out. He spent most his days studying in his bedroom, ordering food online with his only leisure activity being using internet especially for playing videogames. He interrupted contact with friends, contacted his family no more than once a week via phone and rarely maintained personal hygiene. He decided to return in South America, where, at the age of 20, he contacted a mental health expert and started a psychopharmacological therapy based on Sertraline up to 100 mg/day, with reported partial clinical benefit. Two years later, due to the presence of insomnia, Clonazepam was added to the therapy. Two years later, he moved again to Italy, but interrupted his studies and started his first job as seasonal employee and, for the persistence of the psychopathological symptoms described above, he seek again medical help, where he received the diagnosis of ‘Bipolar Disorder type II, depressive episode’ and was prescribed a psychopharmacological therapy based on Trazodone 15 mg/day, Fluvoxamine up to 200 mg/day (that was later replaced with Venlafaxine up to 150 mg/day) and Oxcarbamazepine up to 300 mg/day with partial clinical benefit. During the following years, the clinical picture improved, although he reported residual anxious and mood symptoms and a tendency towards social withdarawal. He went back to university and tried to engage in new social relations. In concomitance of the SARS-CoV-2 pandemic, Mr. X.Y. developed a dysphoric-irritable mood with emotional lability, decreased energy level and apathy, anhedonia, lack in concentration, intense rumination about its difficulties in maintaining social relations and suicidal thoughts, panic attacks, insomnia. Progressively he felt again pushed towards extreme social withdrawal, reducing contact with others to sporadic phone calls and going out when absolutely necessary (buy food, go to work in the months of employment) for about 1 year. Moreover, Mr. X.Y. increased progressively the time he spent on internet games. He also reported craving for high calorie food in the evening, with some binge eating episodes which led to an increasing of weight, reaching 121 Kg. After that, a therapy based on Melatonin 2 mg/die, Zopiclone 7.5 mg/day and Clomipramine up to 150 mg/day was recommended, determining a progressive improvement of affective symptoms and sleep, despite maintaining a tendency toward social isolation, going out from home only when necessary for work or for buying food, spending most of its spare time alone focusing on its specific interest about manga and anime, which he preferred not to share with other people.
One year later, the patient experienced again a decrease in mood, low energy levels, a worsening of social isolation and anxiety with hypersomnia and non-restorative sleep, avoidant and procrastinating behaviors, social withdrawal. Duloxetine up to 60 mg/day was introduced by the clinicians, together with perphenazine up to 2 mg/die, gradually reducing Clomipramine to 37.5 mg/day with reported partial improvement of well-being. During one of his most recent evaluations, Mr. X.Y. was assessed with the AdAS Spectrum questionnaire, in order to investigate underlying autistic traits, the Italian Version of the Hikikomori Questionnaire (HQ-25), and with the at assessment of Internet and Computer Game Addiction Scale (AICA CVS-S) for IGD. He reported a total score 89/160 at the AdAS Spectrum (35), over the validated threshold of 70 for possible clinically relevant ASD symptoms (35) (Table 1). On HQ-25, he reported a score of 84/100 (Table 2), above the threshold of 42/100 needed to underline an hikikomori condition (19), while at AICA CVS-S (51, 52) scale he reported a total score of 12.0, above the threshold of 7.0 for possible clinical symptoms of IGD (51) (Table 3). While the diagnosis of bipolar II disorder remained, it was updated underlining the presence of autistic traits and a tendency towards hikikomori-like social withdrawal and pathological gaming, now in remission.
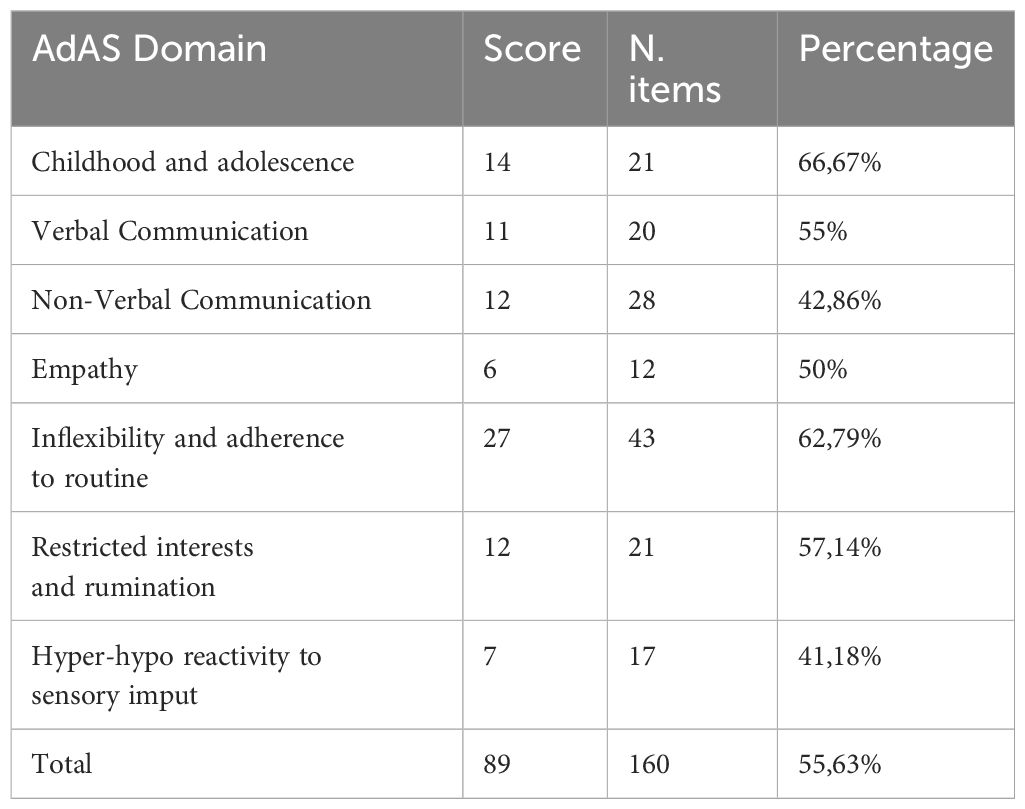
Table 1 Case A AdAS score.
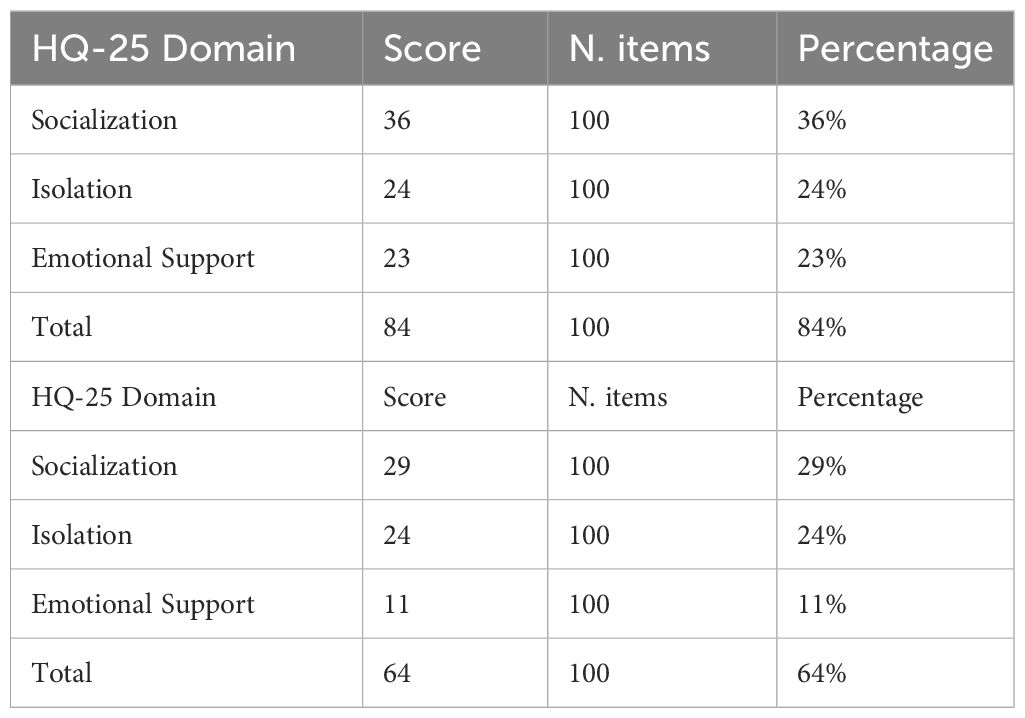
Table 2 Case A, Case B HQ-25 score.
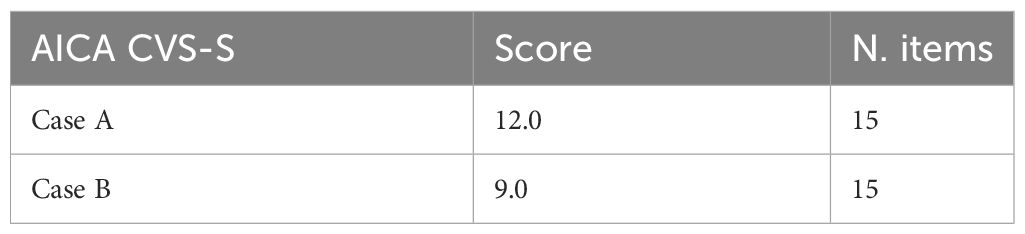
Table 3 Case A and B AICA CVS-S scores.
Mr. W.Z. is a 20-year-old man who lives in a small town with his parents and sister. He reported no family history for psychiatric disorders. He described himself as shy and introverted, with social-phobic symptoms, including avoidance of public/school baths. He displayed narrow interests focused on computer and videogames, difficulties in interpersonal relationship, inflexibility, impaired social emotional reciprocity, hyper-reactivity to sensory inputs, ascribable to an autism spectrum.
During adolescence, at the age of 16, after a motorcycle accident, the patient began to experience swings in mood and energy, apathy and anhedonia, tendency to social withdrawal, panic attacks. The clinical picture worsened during the SARS-CoV-2 pandemic with a progressive avoidance of interpersonal relationships. He did not seek medical help and symptoms partially improved when returning to normal school life, although maintaining a pattern of difficulties in social relationships, with few and superficial friendships. During summer of 2022, in concomitance with his graduation exams, he experienced increased energy levels, irritability, decreased need for sleep. Few months later, following graduation and moving in another city for enrollment in a bachelor program in Informatics, he experienced difficulties in copying with the social and academic environment, with panic attacks and agoraphobic symptoms, ruminative thinking, mood decline, feelings of guilt, circadian rhythm dysregulation, insomnia. He progressively developed a complete social withdrawal with total interruption of relationships at the age of 20. While returning in his parents’ home during summer 2023, he spent most of his time closed in his room, going out only if pushed by his family for eating, avoiding even to use the bathroom, holding back urine or urinating in a bottle. The patient began to spend more and more hours on internet and online video games: he reported that the use of video games was his main distraction and link with other people. In august 2023, with the help of his family, he came to clinical observation. He reported a depressed mood with reduced energy and slight dysphoric notes, deep rumination on interpersonal experiences, feelings of self-worthlessness and guilt and anxiety elevation. He also reported pain and difficulties during urination, for which he was referred to an andrologist who made a diagnosis of prostatitis probably caused by excessive urine holding. He was treated with Valproic Acid 500 mg/die, Paroxetine 20 mg/die. The patient was also assessed with AdAS spectrum, HQ-25, AICA CVS-S questionnaires. He reported a total score of 96/160 on AdAS spectrum (35) (Table 4). On HQ-25 (19) he reported 64/100 (Table 2), while at AICA CVS-S (51) he reported a total score of 9.0 (Table 3). He received ae diagnosis of bipolar II disorder, panic disorder in a patient with autistic traits, and tendency towards hikikomori-like social withdrawal and IGD, now in remission. During the following months, W.Z. underwent a progressive improvement in symptoms, with a reduction in social withdrawal and resumption of university, while persisting the preference for solitary and household activities. He reported to not hold back urine anymore.
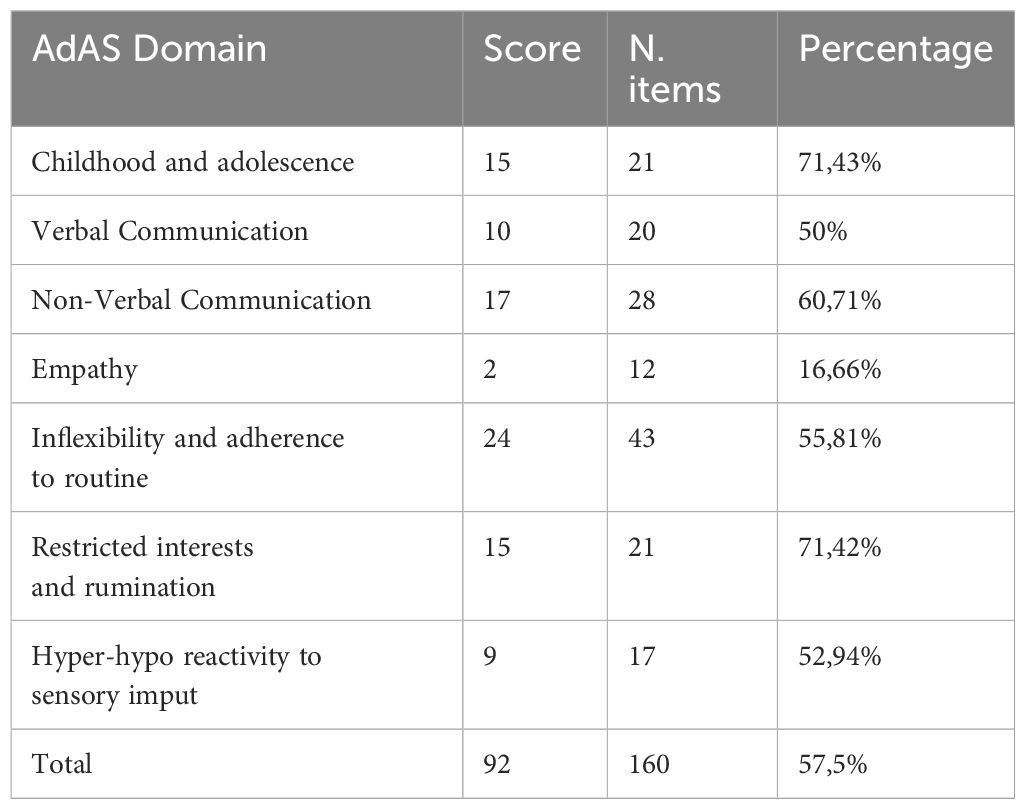
Table 4 Case B AdAS score.
We described two cases of a 40-year-old and of 20-year-old men with relevant autistic traits who, while displaying a number of autistic symptoms since early infancy, finally sought medical assistance after experiencing a severe hikikomori-like social withdrawal. As expected, given the comorbidity pattern of both autistic traits and hikikomori, the patients also manifested mood symptoms and traits of the IGD spectrum. During their infancy and later in life, Mr X.Y. and W.Z. manifested many autistic features that have represented the substance for the development of an affective disorder, a severe social withdrawal and a possible behavioral addiction.
During the clinical assessment, the AdAS Spectrum questionnaire was used, showing the presence of a high level of autistic traits, over the threshold for the presence of a full-blown ASD without intellectual impairment. In this framework, even though some studies highlighted a correlation between hikikomori and neurodevelopmental disorders (22, 25), the literature specifically focused on the relationship between hikikomori and ASD is still scant (49). A particularly consistent contribution to the field came from a recent study from Brosnan et al. (2023), carried on a sample of 646 subjects, that highlighted how autistic traits can strongly influence the risk of developing a form of hikikomori, also via mediating a poor psychological well-being (33). It also seems that poor social and problem-solving skills, typical of autistic subjects, can easily increase the risk of being involved in potentially traumatic events (53), such as bullying or peer rejection (49). This can lead to a reduced self-esteem and extra-punitive coping behaviors such as hikikomori-like social withdrawal (49). Furthermore, repetitive failures in the school and working environment, most easily found in autism spectrum subjects and lived as traumatic experiences, are strongly involved in the hikikomori condition (50). These evidences are all in line with Japanese studies that highlighted a link between hikikomori risk and higher levels of autistic features (29, 54).
Moreover, Mr. X.Y. and Mr. W.Z. both strongly manifested mood symptoms, associated with panic attacks and other anxious symptoms. This is in line with the evidence of a high rate of comorbidity between both ASD and hikikomori with many psychiatric disorders including anxiety and mood disorders (10, 22–26, 34, 42, 44, 55). In this context, low motivation, typical of depressive mental state, or the anxiety pattern in social situations typical of social phobia may favor the hikikomori state (56). Indeed, recent literature recognizes in what is defined as Modern Type Depression, some distinctives hikikomori traits, such as depressed mood, extrapunitive and strong avoidance tendencies, which may lead easily to social withdrawal (6, 57).
Another interesting aspect is represented by the fact that during their periods of social withdrawal, X.Y. and W.Z. reported a history of consistent internet gaming. During their clinical evaluation, they were assessed with the Italian version of AICA CVS-S scale reporting a total score higher than 7.0 points, which is clearly significative for the presence of IGD (57). Now added to the third section of the DSM-5 TR, IGD is described as a “persistent and recurrent use of the internet to engage in games leading to clinically significant impairment or distress and last up to 12 months” (32). For what concerns hikikomori state, the recent literature has introduced the Compensatory Internet Use (CIU) concept, defined as the refuge into the virtual world of Internet, which becomes a way to escape social deficits and a protective isolation against the outside world (26, 58, 59). Indeed, the use of internet games seems to be directly proportional to the prolongation of social withdrawal (60). In a similar way, the difficulties in establishing relationships and in social interaction, typical of the autistic dimension, could induce an increase in time spent on the internet through a pathologic social isolation (28, 30, 43). Moreover, ASD subjects are known to show marked reward dependency mechanisms and, therefore, are more easily exposed to behavioral addictions such as IGD (35, 36). On the other hand, the use of virtual communication can be seen as an attempt of adaptative behavior that can allow ASD subjects to present a completely different personality from themselves, appearing successful and socially acceptable (28, 61–63).
Finally, it should be noticed that these are not the first cases of hikikomori-like social withdrawal in Italy (64). While hikikomori has been initially conceptualize as a culture-bond syndrome linked to the structure of Japanese society, it has been stressed how social changes in Western countries may open the way to the spreading of hikikomori outside Japan (65). In particular, difficulties in finding employment and marginalization due to economy stagnation led to an increase of the “Not in Employment Education or Training’ (NEET) phenomenon, especially in high-income countries, where there is a greater percentage of higher-educated people in spite of a decline of occupational possibilities. NEET and hikikomori share the tendency towards social isolation, unemployment, lack of sense of belonging. Interestingly, in both have been described a tendency to deviate from mainstream values and culturally common behaviors, which is also frequent among subjects in the autism spectrum (66). In this framework, NEET and hikikomori have been considered to be part of a same sectrum, with hikikomori at the extreme severe end (66).
In our case, in line with the literature available, the presence of an underlying autism spectrum may have represented a sign of vulnerability towards the development of a possible full-blown case of hikikomori with IGD tendency.
In both patients, the pharmacological treatment revealed its importance for the improvement of anxiety and mood symptoms, as well as for reducing social withdrawal and computer gaming time, leading to a global improvement of the well-being. In the first case, it required the inclusion of an antipsychotic drug. While patients did not follow a psychotherapy treatment, psycho-education about their conditions was provided during the clinical sessions with the psychiatrist, increasing the awareness about their symptoms and the compliance towards pharmacotherapy.
This work should be considered in light of some limitations. First of all, the high number of questionnaire items. Despite HQ and AICA CVS-S are relatively short questionnaires, AdAS questionnaire requiries long compilation times increasing the risk of inaccurate and hasty answers. Conversely, large number of items allow us to explore a broad spectrum of symptoms. Moreover, all the questionnaires remain self-assessment that may lead patients to bias of symptoms’ overestimation/underestimation. Finally, the report of two patients limits general considerations about treatment indications. Moreover, patients were not assessed with quantitative psychometric instruments for anxiety and mood disorders, which were instead assessed towards a clinical evaluation according to DSM-5 criteria.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study of human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
BC: Conceptualization, Supervision, Writing – review & editing. CB: Writing – original draft. FG: Writing – original draft. FP: Writing – original draft. MG: Writing – original draft. BN: Supervision, Writing – original draft. GA: Writing – review & editing. IC: Writing – review & editing. SP: Conceptualization, Writing – review & editing. LD: Conceptualization, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors thank the participants for their continued support and participation in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Martinotti G, Vannini C, Di Natale C, Sociali A, Stigliano G, Santacroce R, et al. Hikikomori: psychopathology and differential diagnosis of a condition with epidemic diffusion. Int J Psychiatry Clin Pract. (2021) 25:187–94. doi: 10.1080/13651501.2020.1820524
2. Kato TA, Kanba S, Teo AR. A 39-year-old ‘Adultolescent’: understanding social withdrawal in Japan. Am J Psychiatry. (2016) 173:112–4. doi: 10.1176/appi.ajp.2015.15081034
3. Kato TA, Kanba S, Teo AR. Hikikomori: experience in Japan and international relevance. World Psychiatry. (2018) 17:105–6. doi: 10.1002/wps.20497
4. Saito T. Shakaiteki Hikikomori-Owaranai Shishunki [Hikikomori: Adolescence without end, University of Minnesota Press]. Tokyo: PHP Shinsho (1998).
6. Kato TA, Shinfuku N, Sartorius N, Kanba S. Are Japan's hikikomori and depression in young people spreading abroad? Lancet. (2011) 378:1070. doi: 10.1016/S0140-6736(11)61475-X
7. Kato TA, Tateno M, Shinfuku N, Fujisawa D, Teo AR, Sartorius N, et al. Does the ‘hikikomori’; syndrome of social withdrawal exist outside Japan? A preliminary international investigation. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1061–75. doi: 10.1007/s00127-011-0411-7
8. Liu LL, Li TM, Teo AR, Kato TA, Wong PW. Harnessing social media to explore youth social withdrawal in three major cities in China: cross-sectional web survey. JMIR Ment Health. (2018) 5:e34. doi: 10.2196/mental.8509
9. Malagón-Amor ÁChecktae, Martín-López LM, Córcoles D, González A, Bellsolà M, Teo AR, et al. A 12-month study of the hikikomori syndrome of social withdrawal: Clinical characterization and different subtypes proposal. Psychiatry Res. (2018) 270:1039–46. doi: 10.1016/j.psychres.2018.03.060
10. Teo AR, Fetters MD, Stufflebam K, Tateno M, Balhara Y, Choi TY, et al. Identification of the hikikomori syndrome of social withdrawal: Psychosocial features and treatment preferences in four countries. Int J Soc Psychiatry. (2015) 61:64–72. doi: 10.1177/0020764014535758
11. Wong PW, Li TM, Chan M, Law YW, Chau M, Cheng C, et al. The prevalence and correlates of severe social withdrawal (hikikomori) in Hong Kong: A cross-sectional telephone-based survey study. Int J Soc Psychiatry. (2015) 61:330–42. doi: 10.1177/0020764014543711
12. Wong PWC, Liu LL, Li TMH, Kato TA, Teo AR. Does hikikomori (severe social withdrawal) exist among young people in urban areas of China? Asian J Psychiatr. (2017) 30:175–6. doi: 10.1016/j.ajp.2017.10.026
13. Wu AFW, Ooi J, Wong PWC, Catmur C, Lau JYF. Evidence of pathological social withdrawal in non-Asian countries: a global health problem? Lancet Psychiatry. (2019) 6:195–6. doi: 10.1016/S2215-0366(18)30428-0
14. Suwa M, Suzuki K. The phenomenon of “hikikomori” (social withdrawal) and the socio-cultural situation in Japan today. J Psychopathol. (2013) 19:191–8.
15. Li TM, Wong PW. Editorial Perspective: Pathological social withdrawal during adolescence: A culture-specific or a global phenomenon? J Child Psychol Psychiatry. (2015) 56:1039–41. doi: 10.1111/jcpp.12440
16. Cabinet-Office Wakamono-no seikatsu-ni kansuru chosa. Hikikomori: The Cabinet Office’s 2016 Survey of Acute Social Withdrawal. Cabinet office survey - Mental Health and Social Withdrawal in Contemporary Japan: Beyond the Hikikomori Spectrum (Accessed December 2023).
17. Tajan N. Mental health and social withdrawal in contemporary Japan: beyond the Hikikomori spectrum. New York, NY: Routledge/Taylor & Francis Group (2021). doi: 10.4324/9781351260800
18. Amendola S, Presaghi F, Teo AR, Cerutti R. Psychometric properties of the italian version of the 25-item hikikomori questionnaire for adolescents. Int J Environ Res Public Health. (2022) 19:10408. doi: 10.3390/ijerph191610408
19. Teo AR, Chen JI, Kubo H, Katsuki R, Sato-Kasai M, Shimokawa N, et al. Development and validation of the 25-item hikikomori questionnaire (HQ-25). Psychiatry Clin Neurosci. (2019) 72:780–8. doi: 10.1111/pcn.12691
20. Kato TA, Kanba S, Teo AR. Hikikomori: Multidimensional understanding, assessment, and future international perspectives. Psychiatry Clin Neurosci. (2019) 73:427–40. doi: 10.1111/pcn.12895
21. Kato TA, Kanba S, Teo AR. Defining pathological social withdrawal: proposed diagnostic criteria for hikikomori. World Psychiatry. (2020) 19:116–7. doi: 10.1002/wps.20705
22. Kondo N. Shishunki no hikikomori to hattatsu shougai [Adolescent withdrawal and developmental disorders]. Japanese J Psychosomatic Med. (2010), 285–91. doi: 10.1111%2Fpcn.13154"10.1111/pcn.13154
23. Lee YS, Lee JY, Choi TY, Choi JT. Home visitation program for detecting, evaluating and treating socially withdrawn youth in Korea. Psychiatry Clin Neurosci. (2013) 67:193–202. doi: 10.1111/pcn.12043
24. Saito K. (2010). No Hyouka-Shien Ni Kansuru Gaido-Rain [Guideline of Hikikomori for their evaluations and supports]. Tokyo: Ministry of Health, Labour and Welfare Available at: http://www.ncgmkohnodai.go.jp/pdf/jidouseishin/22ncgm_hikikomori.pdf.
25. Tateno M, Park TW, Kato TA, Umene-Nakano W, Saito T. Hikikomori as a possible clinical term in psychiatry: a questionnaire survey. BMC Psychiatry. (2012) 12:169. doi: 10.1186/1471-244X-12-169
26. Kato TA, Shinfuku N, Tateno M. Internet society, internet addiction, and pathological social withdrawal: the chicken and egg dilemma for internet addiction and hikikomori. Curr Opin Psychiatry. (2020) 33:264–70. doi: 10.1097/YCO.0000000000000601
27. Dell’Osso L, Bonelli C, Nardi B, Amatori G, Cremone IM, Carpita B. Autism spectrum disorder in a patient with bipolar disorder and its relationship with catatonia spectrum: A case study. Brain Sci. (2023) 13:704. doi: 10.3390/brainsci13050704
28. Tateno M, Horie K, Shirasaka T, Nanba K, Shiraishi E, Tateno Y, et al. Clinical usefulness of a short version of the internet addiction test to screen for probable internet addiction in adolescents with autism spectrum disorder. Int J Environ Res Public Health. (2023) 20:4670. doi: 10.3390/ijerph20054670
29. Hamasaki Y, Pionnié-Dax N, Dorard G, Tajan N, Hikida T. Identifying social withdrawal (hikikomori) factors in adolescents: understanding the hikikomori spectrum. Child Psychiatry Hum Dev. (2021) 52:808–17. doi: 10.1007/s10578-020-01064-8
30. Millington E, Simmons DR. Cleland woods H. Brief report: investigating the motivations and autistic traits of video gamers. J Autism Dev Disord. (2022) 52:1403–7. doi: 10.1007/s10803-021-04994-x
31. Teo AR, Gaw AC. Hikikomori, a Japanese culture-bound syndrome of social withdrawal? A proposal for DSM-V. J Nervous Ment Dis. (2010) 198:444. doi: 10.1097/NMD.0b013e3181e086b1
32. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fifth edition, text revision. Washington: American Psychiatric Association (2022). doi: 10.1176/appi.books.9780890425787
33. Brosnan M, Gavin J. The impact of higher levels of autistic traits on risk of hikikomori (pathological social withdrawal) in young adults. PloS One. (2023) 18:e0281833. doi: 10.1371/journal.pone.0281833
34. Dell’Osso L, Dalle Luche R, Maj M. Adult autism spectrum as a transnosographic dimension. CNS Spectr. (2016) 21:131–3. doi: 10.1017/S1092852915000450
35. Dell'Osso L, Gesi C, Massimetti E, Cremone IM, Barbuti M, Maccariello G, et al. Adult Autism Subthreshold Spectrum (AdAS Spectrum): Validation of a questionnaire investigating subthreshold autism spectrum. Compr Psychiatry. (2017) 73:61–83. doi: 10.1016/j.comppsych.2016.11.001
36. Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord. (2001) 31:5–17. doi: 10.1023/A:1005653411471
37. Skylark WJ, Baron-Cohen S. Initial evidence that non-clinical autistic traits are associated with lower income. Mol Autism. (2017) 8:61. doi: 10.1186/s13229-017-0179-z
38. Suzuki T, Miyaki K, Eguchi H, Tsutsumi A. Distribution of autistic traits and their association with sociodemographic characteristics in Japanese workers. Autism. (2018) 22:907–14. doi: 10.1177/1362361317716605
39. Carpita B, Muti D, Muscarella A, Dell'Oste V, Diadema E, Massimetti G, et al. Sex differences in the relationship between PTSD spectrum symptoms and autistic traits in a sample of university students. Clin Pract Epidemiol Ment Health. (2019) 15:110–9. doi: 10.2174/1745017901915010110
40. Sucksmith E, Roth I, Hoekstra RA. Autistic traits below the clinical threshold: re-examining the broader autism phenotype in the 21st century. Neuropsychol Rev. (2011) 21:360–89. doi: 10.1007/s11065-011-9183-9
41. Sucksmith E, Allison C, Baron-Cohen S, Chakrabarti B, Hoekstra RA. Empathy and emotion recognition in people with autism, first-degree relatives, and controls. Neuropsychologia. (2013) 51:98–105. doi: 10.1016/j.neuropsychologia.2012.11.013
42. Takara K, Kondo T. Comorbid atypical autistic traits as a potential risk factor for suicide attempts among adult depressed patients: a case–control study. Ann Gen Psychiatry. (2014) 13:1–8. doi: 10.1186/s12991-014-0033-z
43. Dell’Osso L, Lorenzi P, Carpita B. The neurodevelopmental continuum toward the neurodevelopmental gradient hypothesis. J Psycopathol. (2019) 25:179–82.
44. Carpita B, Muti D, Cremone IM, Fagiolini A, Dell'Osso L. Eating disorders and autism spectrum: links and risks. CNS Spectr. (2022) 27:272–80. doi: 10.1017/S1092852920002011
45. Kato K, Mikami K, Akama F, Yamada K, Maehara M, Kimoto K, et al. Clinical features of suicide attempts in adults with autism spectrum disorders. Gen Hosp Psychiatry. (2013) 35:50–3. doi: 10.1016/j.genhosppsych.2012.09.006
46. Pelton MK, Cassidy SA. Are autistic traits associated with suicidality? A test of the interpersonal-psychological theory of suicide in a non-clinical young adult sample. Autism Res. (2017) 10:1891–904. doi: 10.1002/aur.1828
47. Carpita B, Marazziti D, Palego L, Giannaccini G, Betti L, Dell'Osso L. Microbiota, immune system and autism spectrum disorders: an integrative model towards novel treatment options. Curr Med Chem. (2020) 27:5119–36. doi: 10.2174/0929867326666190328151539
48. Dell'Osso L, Cremone IM, Amatori G, Cappelli A, Cuomo A, Barlati S, et al. Investigating the relationship between autistic traits, ruminative thinking, and suicidality in a clinical sample of subjects with bipolar disorder and borderline personality disorder. Brain Sci. (2021) 11:621. doi: 10.3390/brainsci11050621
49. Katsuki R, Tateno M, Kubo H, Kurahara K, Hayakawa K, Kuwano N, et al. Autism spectrum conditions in hikikomori: A pilot case-control study. Psychiatry Clin Neurosci. (2021) 74:652–8. doi: 10.1111/pcn.13154
50. Shimono Y, Hasegawa A, Tsuchihara K, Tanaka K, Matsuda Y. Longitudinal association between autistic traits and affinity for hikikomori in Japanese university students. Curr Psychol. (2021) 41:8841–9. doi: 10.1007/s12144-020-01287-x
51. Wölfling K, Müller KW, Beutel M. Reliabilität und Validität der Skala zum Computerspielverhalten (CSV-S) [Reliability and validity of the Scale for the Assessment of Pathological Computer-Gaming (CSV-S)]. Psychother Psychosom Med Psychol. (2011) 61:216–24. doi: 10.1055/s-0030-1263145
52. Peracchia S, Presaghi F, Curcio G. Italian adaption of the Assessment of Internet and Computer Game Addiction Scale Rassegna di Psicologia, Vol. 3. (2018). pp. 5–16. doi: 10.4458/1415-01.
53. Dell'Osso L, Chiarantini I, Bonelli C, Cappellato G, Carpita BA. comprehensive perspective of autistic traits and catatonic symptoms in a patient with Fronto-Temporal Dementia and Bipolar Disorder: a case report. BMC Psychiatry. (2023) 23:216. doi: 10.1186/s12888-023-04709-9
54. Yong RK, Fujita K, Chau PY, Sasaki H. Characteristics of and gender difference factors of hikikomori among the working-age population: a cross-sectional population study in rural Japan. Japanese J Public Health. (2020) 67:237–46. doi: 10.11236/jph.67.4_237
55. Mattila ML, Hurtig T, Haapsamo H, Jussila K, Kuusikko-Gauffin S, Kielinen M, et al. Comorbid psychiatric disorders associated with Asperger syndrome/high-functioning autism: a community- and clinic-based study. J Autism Dev Disord. (2010) 40:1080–93. doi: 10.1007/s10803-010-0958-2
56. Yamada M, Kato TA, Katsuki RI, Yokoi H, Igarashi M, Komine Y, et al. Pathological social withdrawal in autism spectrum disorder: A case control study of hikikomori in Japan. Front Psychiatry. (2023) 14:1114224. doi: 10.3389/fpsyt.2023.1114224
57. Teo AR, Nelson S, Strange W, Kubo H, Katsuki R, Kurahara K, et al. Social withdrawal in major depressive disorder: a case-control study of hikikomori in Japan. J Affect Disord. (2020) 274:1142–6. doi: 10.1016/j.jad.2020.06.011
58. Stavropoulos V, Anderson EE, Beard C, Latifi MQ, Kuss D, Griffiths MA. preliminary cross-cultural study of Hikikomori and Internet Gaming Disorder: The moderating effects of game-playing time and living with parents. Addict Behav Rep. (2021) 9:001–1. doi: 10.1016/j.abrep.2018.10.001
59. Carpita B, Muti D, Nardi B, Benedetti F, Cappelli A, Cremone IM, et al. Biochemical correlates of video game use: from physiology to pathology. A narrative review. Life (Basel). (2021) 11:775. doi: 10.3390/life11080775
60. Stip E, Thibault A, Beauchamp-Chatel A, Kisely S. Internet addiction, hikikomori syndrome, and the prodromal phase of psychosis. Front Psychiatry. (2016) 7:6. doi: 10.3389/fpsyt.2016.00006
61. Dell'Osso L, Amatori G, Muti D, Giovannoni F, Parri F, Violi M, et al. Autism spectrum, Hikikomori syndrome and Internet Gaming Disorder: Is there a link? Brain Sci. (2023) 13(7):1116. doi: 10.3390/brainsci13071116
62. Dell'Osso L, Carmassi C, Cremone IM, Muti D, Salerni A, Barberi FM, et al. Defining the optimal threshold scores for adult autism subthreshold spectrum (AdAS spectrum) in clinical and general population. Clin Pract Epidemiol Ment Health. (2020) 16:204–11. doi: 10.2174/1745017902016010204
63. Cremone IM, Carpita B, Nardi B, Casagrande D, Stagnari R, Amatori G, et al. Measuring social camouflaging in individuals with high functioning autism: A literature review. Brain Sci. (2023) 13:469. doi: 10.3390/brainsci13030469
64. Orsolini L, Longo G, Bellagamba S, Kato TA, Volpe U. Hikikomori-like social withdrawal: An Italian case report. Psychiatry Clin Neurosci. (2023) 77:510. doi: 10.1111/pcn.13570
65. Orsolini L, Bellagamba S, Volpe U, Kato TA. Hikikomori and modern-type depression in Italy: A new phenotypical trans-cultural characterization? Int J Soc Psychiatry. (2022) 68:1010–7. doi: 10.1177/00207640221099408
Keywords: autistic spectrum disorder, internet gaming disorder, autistic traits, social withdrawal, hikikomori
Citation: Carpita B, Bonelli C, Giovannoni F, Parri F, Gambini M, Nardi B, Amatori G, Cremone IM, Pini S and Dell’Osso L (2024) Case report: hikikomori syndrome in Italy and its link with autistic traits and internet gaming disorder. Front. Psychiatry 15:1378572. doi: 10.3389/fpsyt.2024.1378572
Received: 29 January 2024; Accepted: 22 April 2024;
Published: 28 May 2024.
Edited by:
Fengyu Zhang, Global Clinical and Translational Research Institute, United StatesReviewed by:
Teruhisa Uwatoko, Kyoto University, JapanCopyright © 2024 Carpita, Bonelli, Giovannoni, Parri, Gambini, Nardi, Amatori, Cremone, Pini and Dell’Osso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Bonelli, Y2hpYXJhYm9uZWxsaS45NUBob3RtYWlsLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.