 Kate Maguire
Kate Maguire Hayley Warman1
Hayley Warman1 Frances Blumenfeld
Frances Blumenfeld Peter E. Langdon
Peter E. Langdon
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 27 March 2024
Sec. Autism
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1375170
This article is part of the Research Topic World Autism Awareness Day 2024 View all 7 articles
Background and methods: The aim of this systematic review was to synthesise research examining the relationship between autism and psychopathy to: (a) better understand the relationship between these two constructs, and (b) describe the clinical manifestation of the two when they co-occur. A systematic search of the literature returned 36 studies.
Results: Across all ages, autistic individuals and those with elevated autistic traits but no autistic diagnoses appeared to have increased callous and unemotional traits or psychopathy relative to the general population. Several studies evidenced that although both constructs are associated with empathetic dysfunction, the underlying mechanisms differ. In adults, psychopathy/psychopathic traits were associated with diminished affective empathy and intact cognitive empathy, whilst the opposite was seen autistic adults and those with elevated autistic traits. In children, those with autistic traits or a diagnosis of autism had diminished cognitive empathy, but not affective empathy, while the relationship between callous and unemotional traits/psychopathy and empathy amongst children was less clear. The co-occurrence of autism and psychopathy was seen to lead to additional empathic and cognitive impairment, but findings were mixed making it challenging to clearly describe the clinical manifestation.
Conclusion: There remains a paucity of research investigating the interaction between autism and psychopathy and included studies were characterised by multiple measurement difficulties. Attention should be directed toward developing better methods for identifying psychopathic traits in autistic individuals to advance our understanding of the relationship between autism and psychopathy to allow for the development of appropriate care pathways for this population.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=413672, identifier CRD42023413672.
Autism is a neurodevelopmental disorder characterised by social and communication deficits and restricted or repetitive patterns of behaviour (1), with prevalence currently estimated as one in 100 (2). Aggression is not a core symptom of autism but rates of aggression in autistic children and adolescents range from 25% (3) to 53% (4). This aspect of autism has been growing in interest with research increasingly focusing on the relationship between autism and psychopathy.
Psychopathy is characterised by shallow emotional response, a diminished capacity for empathy or remorse, callousness, and poor behavioural control (5, 6). Prevalence in the general population is estimated at 4.5%, with a higher prevalence among offenders (7). It has long been associated with criminal and violent behaviour and is a key predictor of recidivism (8). Psychopathy can be categorised into primary and secondary psychopathy; primary psychopathy results from largely genetic and biological influences, and secondary psychopathy is related to adverse environmental factors (such as developmental trauma/maltreatment) (9). Primary psychopathy is associated with increased emotionally stability, fearlessness, and being more self-assured than secondary psychopathy, which is often associated with greater psychopathology. As children and young people are still developing, they are not considered capable of presenting with psychopathy; instead, a precursor is observed, referred to as callous and unemotional traits [CUTs; (10)].
Whilst the link between psychopathy and criminality is well evidenced (11), the relationship between autism and criminality is less clear. Collins et al. (12) reported that criminality rates amongst those with autism ranged from 0.2% (13) to 62.8% (14) within their systematic review, indicating an overrepresentation of autism amongst offenders. Despite this, the review suggested that there is little evidence that autistic individuals have an increased risk of committing crimes, highlighting methodological limitations which impacted the reliability of conclusions. It was hypothesised that social communication difficulties may make autistic individuals more likely to be viewed as risky, encounter the criminal justice system, and receive custodial sentences.
Autism and psychopathy are both characterised by empathic dysfunction which plays a role in their behavioural phenotypes, and whilst they may appear to share surface similarities, the underlying difficulties may differ (15). Empathy involves understanding and sharing others’ emotions, thoughts or feelings and can be divided into cognitive (understanding thoughts and feelings) and affective (sharing emotional experiences) empathy (15). It has been proposed that autistic people struggle with cognitive empathy but not affective empathy, whereas the opposite is found within psychopathy (16–18).
Cognitive empathy requires theory of mind (ToM)/perspective taking skills, and together with affective empathy both are required when making moral decisions (19). Autistic people who have difficulties with cognitive empathy may inadvertently cause harm to others due to difficulty interpreting the behaviour of others (20), while individuals with psychopathy are more likely to engage in criminality and have difficulties with affective empathy and emotion recognition, but present with intact ToM skills (15, 21). Those with psychopathy are thought to have difficulties with recognising aversive emotions in others (e.g., fear and sadness) resulting from deficits in amygdala and orbital/ventrolateral frontal cortex function (22) and these difficulties interfere with learning and subsequent avoidance. For example, fearfulness is aversive, and if attenuated, an individual may behave in self-gratifying manner without concern about the consequence as they experience no fear of negative consequences for themselves or others. There is also evidence of difficulties with recognising non-aversive emotions (23) which may be related to difficulties with attention allocation to the eyes of others (24). Diminished affective empathy, paired with the ability to mentalise, enables psychopaths to successfully manipulate others for personal gain (15). This contrasts with autistic individuals who experience aversive emotions if they believe they have caused harm (20). Therefore, although both autism and psychopathy are characterised by empathic dysfunction, behaviour and decision-making are very different and driven by distinct empathetic pathways.
Little is known about the co-existence of autism and psychopathy. Rogers et al. (25), proposed the ‘double hit’ hypothesis, whereby autistic individuals may also show additional impairments in empathy, best explained by the presence of psychopathy as a distinct and additional disorder. However, research in this area is limited. Therefore, the aim of the current study was to systematically review the literature to: (a) understand the relationship between psychopathy and autism, and (b) to describe the clinical manifestation of the two constructs when they co-occur. Studies examining this relationship are critical in furthering our knowledge of this small but clinically significant population group and may help to inform the types of interventions appropriate for those who meet the criteria for both constructs, and especially those who encounter criminal justice as a consequence of their behaviour. The review will encompass traits of each disorder to reflect the spectrum nature of both constructs. Research on children with CUTs (considered a pre-cursor to adult psychopathy) will be included because early identification can help prevent serious risk through successful early intervention.
This systematic review was conducted according to PRISMA guidelines (26) and was registered with PROSPERO (registration number CRD42023413672).
Relevant studies were identified by systematic searching of the following databases: PsychINFO; CINAHL Ultimate; Medline Ultimate. Google Scholar was also searched and backward searching of identified papers was completed. Grey literature was searched through www.opengrey.eu. Initial searches were undertaken in March 2023 and completed in April 2023. Key terms were searched using English and American terminology, spelling, and truncation to ensure that all variant word endings were identified. Search terms were combined using the term ‘AND’, Table 1.
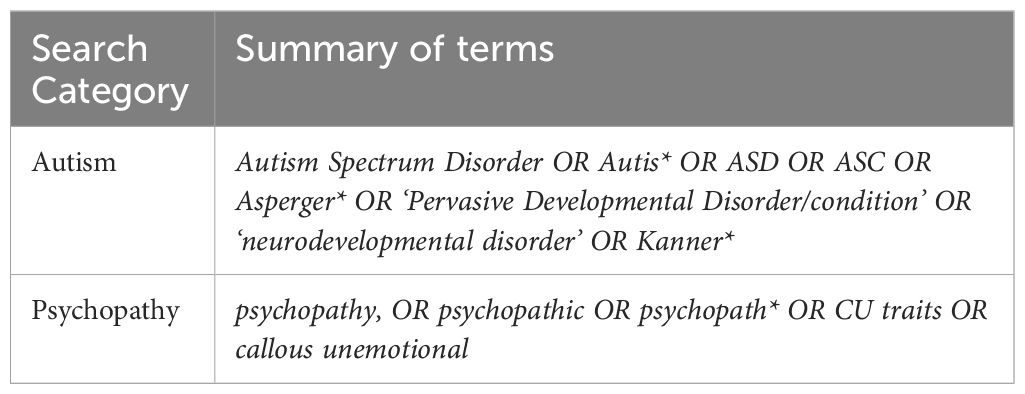
Table 1 Summary of search terms.
To ensure searches produced relevant results only, the above search terms were restricted to title only and a further specified term of ‘NOT psychopathology’ was included within the title or abstract. This was because initial searches without this clarification produced multiple inapplicable results. Searches were restricted to English language and academic journals or dissertations, in line with the eligibility criteria below, Table 2.
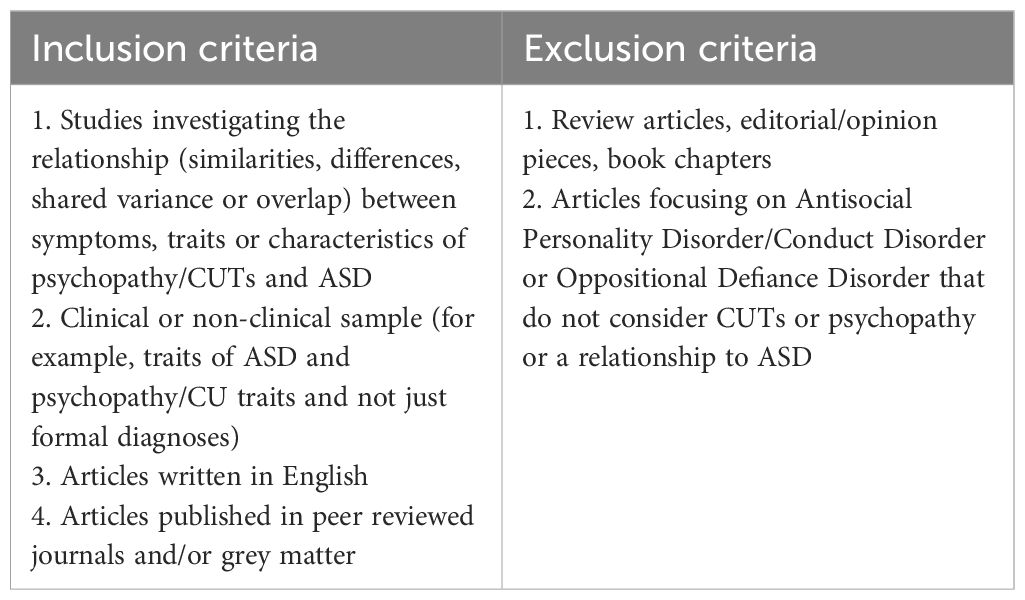
Table 2 Eligibility criteria.
Due to limited research in this area, no limiters or restrictions were placed upon study design or study date.
Article selection was completed by author KM, with 30% of search results also screened by an independent, masked, second rater (HW), with an interrater agreement of 100%. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (26) guidance was used to refine studies and can be seen in Figure 1 which details article selection. First, duplicates were electronically removed using EBSCO. Abstracts were then screened against the eligibility criteria and results were rejected which did not meet criteria. This included book chapters or papers not specifically looking at both autism and psychopathy in some manner. Full text screening of remaining articles was then completed.
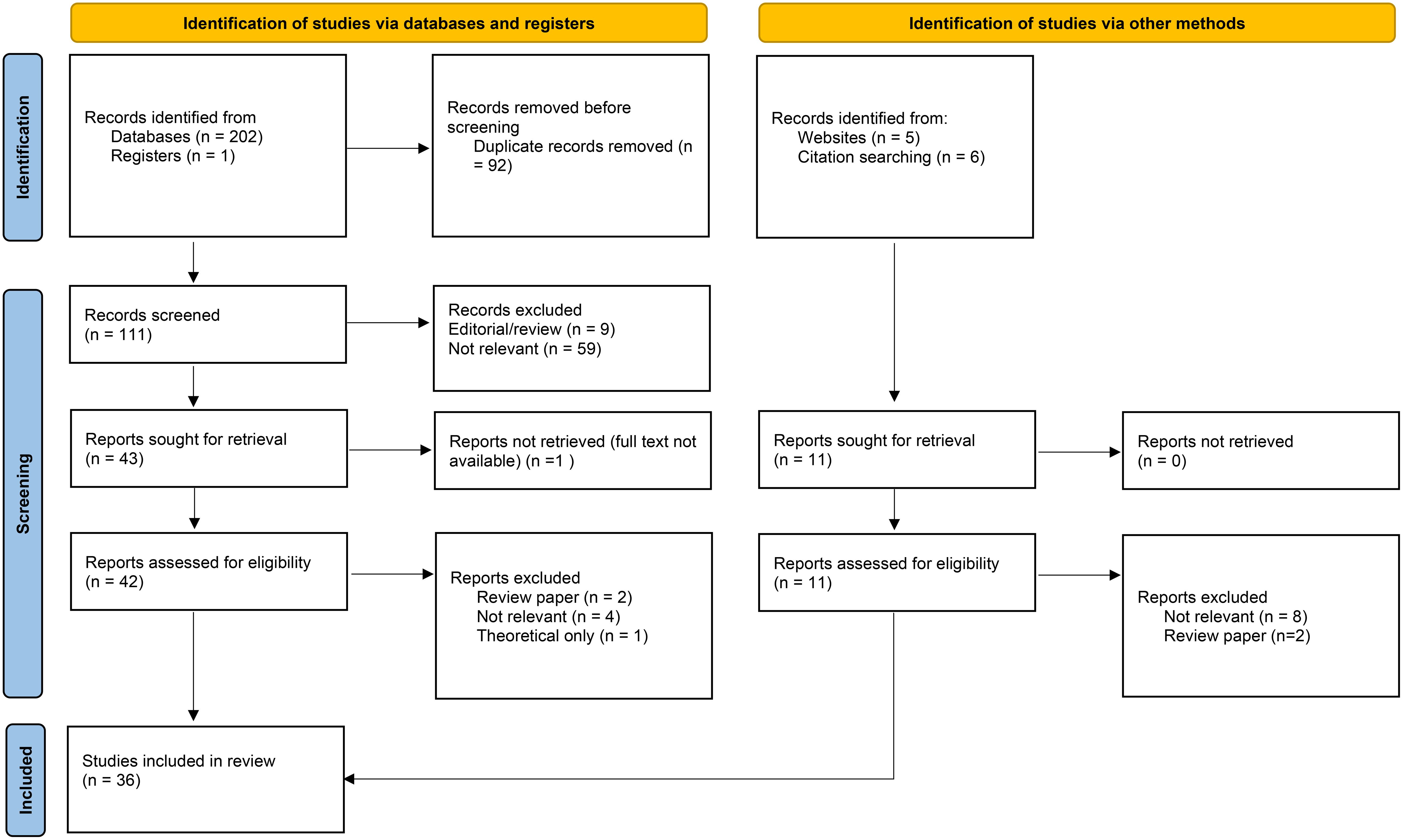
Figure 1 PRISMA diagram showing screening and identification of eligible studies (27).
The following data were extracted from each paper: author and country, study population and participant characteristics, measure of autism/psychopathy/CUTs administered and main findings. These data were considered relevant to either quality appraisal of the studies or relevant for synthesis of findings in relation research question. Thirty percent of papers were checked by HW, with an inter-rater agreement of 88%. All disagreements were resolved through discussion.
Prior to evidence synthesis, a critical appraisal of the literature is required to enable a judgement about bias and subsequent effectiveness. Study quality was assessed using the ‘Checklist for Analytical Cross-Sectional Studies’ (28). This tool is used to assess the methodological quality of each included study and assess sources of bias. One included study (29) was a longitudinal cohort study and therefore the ‘Checklist for Cohort Studies’ was used instead (30). These tools are recognised as a reliable tool for use in systematic reviews to evaluate variation in study designs and methodology (31). Again, 30% of papers were checked by HW, with an inter-rater agreement of 82% and disagreements resolved through discussion.
A narrative synthesis approach was adopted due to the broad spectrum of included research. This was conducted in line with guidance by Popay et al. (32), who describe this technique as a synthesis of studies relying on the use of words to summarise and explain findings.
Of the 214 papers identified during initial searches, 92 duplicates were removed, 71 were not relevant and 13 were reviews or editorial pieces. The full text article was unavailable for one paper, and another was theoretical only, leaving 36 studies that met the eligibility criteria and were included, Figure 1. Table 3 shows 22 studies that recruited children and Table 4 shows 14 studies that included adult participants.
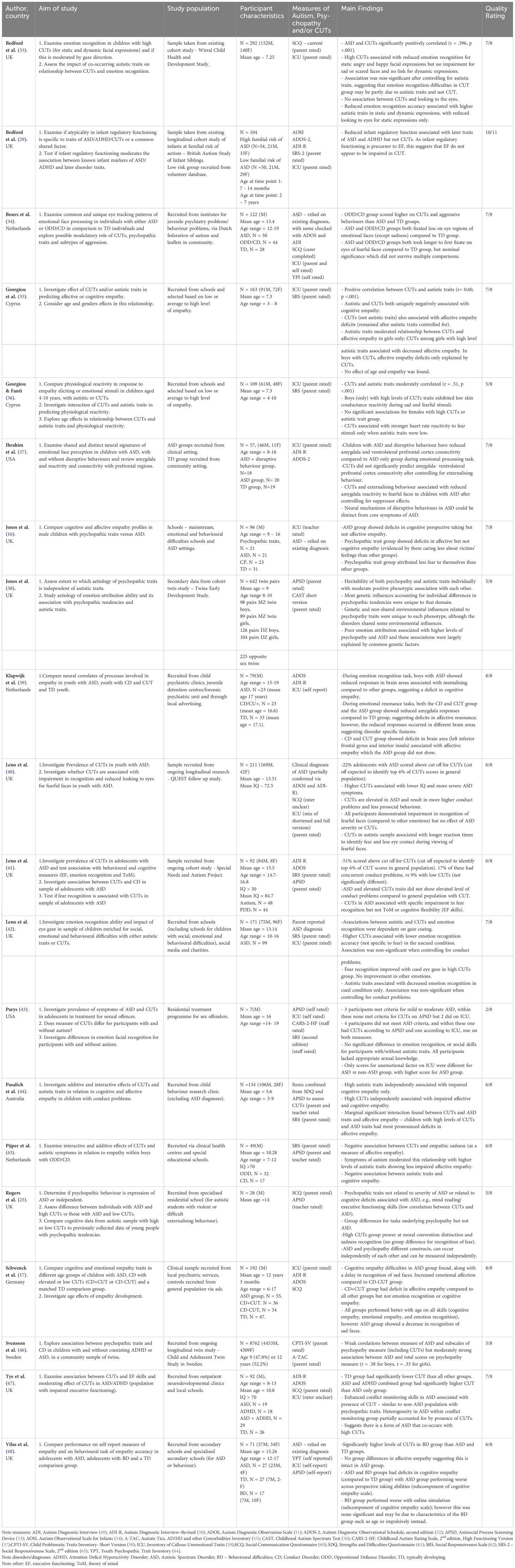
Table 3 Studies investigating the relationship between psychopathy/ callous unemotional traits and autism/autistic traits in children.
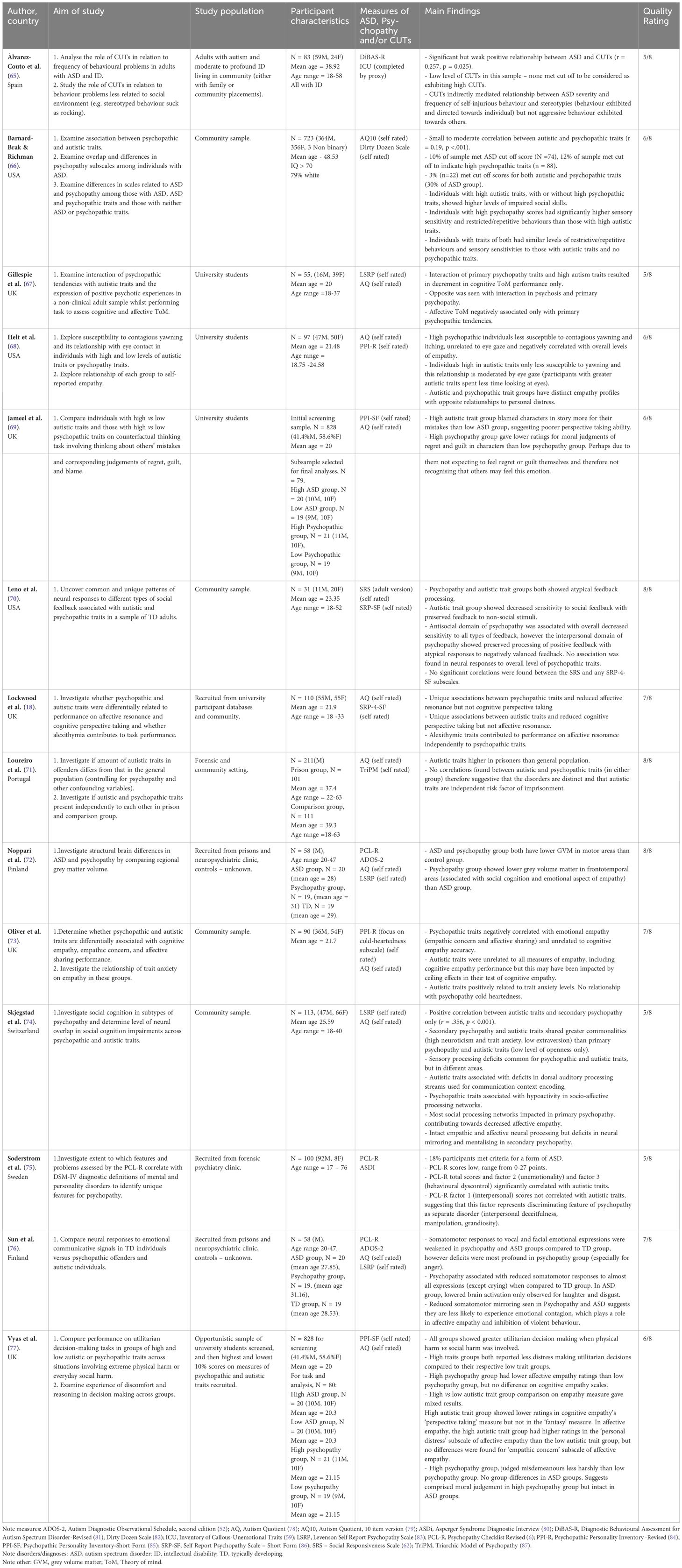
Table 4 Studies Investigating the Relationship Between Psychopathy/Psychopathic Traits and Autism/Autistic Traits in Adults.
Studies were conducted in 11 Western countries: UK (17), USA (5), Netherlands (3), Sweden (2), Finland (2), Cyprus (2), Spain (1), Switzerland (1), Germany (1), Portugal (1) and Australia (1). Twenty studies recruited from community settings, including schools and universities, and a further five were recruited from existing cohort/longitudinal studies. Five studies recruited from clinical settings such as child behaviour clinics and six recruited from forensic settings. One study focused specifically on sex offenders (43). Sample sizes ranged from seven (43), in an unpublished thesis, to several thousand in large scale twin studies (46, 88).
A total of 12115 children were recruited across the included studies, including 6654 males and 5461 females. Of these, 746 had primary diagnoses of autism, autistic traits, or were identified as being at familial risk of autism, although many also had co-morbid diagnoses or additional behavioural difficulties. Three hundred and nineteen were considered to have oppositional defiant disorder, conduct disorder/problems, CUT or psychopathic traits, whilst 11032 were either identified as typically developing or no information was provided. Eighteen participants only had a diagnosis of ADHD. A total of 1888 adults were recruited across our included studies, including 1133 males, 752 females and 3 people who identified as non-binary. Of these, 163 had diagnoses of autism or had autistic traits, 80 had psychopathic traits and the remaining were either considered typically developing or the information was not provided.
Twenty-four studies included males and females, whereas 12 only recruited males. Participant age ranged from seven months (29) to 63 years (71). One study included participants with intellectual disability (65), and three studies included those with mixed ability levels: Leno et al. (41) reported a mean IQ of 84.7, Leno et al. (40) reported a mean IQ of 72.5, and Soderstrom et al. (75) reported that 17% of participants had an IQ below 70.
Quality appraisal ratings are found in Tables 1 and 2. Scores ranged from two to eight, with five fulfilling the full criteria (17, 39, 70–72). An unpublished thesis (43), scored two out of eight. This low score was due to the small sample size (N=7) meaning that the statistical analysis was judged as inappropriate, whilst there was little information on eligibility criteria, confounding variables or appropriateness of the measures used.
Some studies involved administering a gold standard diagnostic tool to participants including the Autism Diagnostic Observation Schedule (ADOS) (89) and the Autism Diagnostic Interview-Revised (ADI-R) (50), while two studies did not confirm existing diagnoses (16, 48), although both had large sample sizes, making this a time-consuming exercise. Commonly used measures of autistic traits were the Autism Quotient (AQ), the Social Communication Questionnaire (SCQ), and the Social Responsiveness Scale (SRS). These were considered reliable and valid measures, and appropriate screening tools. Research has shown that screening tools are not entirely predictive of diagnosis (90), making it important to differentiate between autistic traits and a formal diagnosis of autism across studies.
There was large variation in the measurement of psychopathy/CUTs. Many studies used the Inventory of Callous Unemotional Traits (ICU) (59), which is a 24-item scale designed to measure CUTs in children. Whilst this is a well-researched and validated measure (see Cardinale and Marsh (10) for a review), no study has validated its use in autistic children. Several studies used this measure (34, 37, 40, 47, 65). Other researchers (16, 25, 41) administered the Antisocial Process Screening Device (APSD) (53), measuring the wider construct of psychopathy in young people, but again, this has not been validated for use with autistic children. Rogers et al. (25), acknowledged this and confirmed that the APSD positively correlated with conduct problems as expected, suggesting convergent validity.
The authors of three studies (72, 75, 76) administered the Psychopathy Check List-Revised (PCL-R) (6), which is considered to be a gold standard tool. All other studies relied on self-report measures of psychopathy, which should be viewed critically as psychopathic individuals tend to lack insight into the nature of their psychopathology (91). Additionally, using self-report measures with those known to be manipulative and deceptive increases the risk of response bias (92). Research about the reliability and validity of self-report measures of psychopathy in autistic people is lacking. There is evidence that self-report personality measures used with autistic children are questionable (93), and three of the included studies used a psychopathy self-report measure with children (39, 43, 48). Vilas et al. (48) acknowledged the limitations of this and administered multiple measures to circumvent this problem. The use of a single measure of psychopathy is advised against (91); however, only five studies administered multiple measures (34, 43, 48, 72, 76).
Leno et al. (40) reported that 22% of autistic children scored above their designated cut off to indicate the presence of CUTs. However, some participants completed the full ICU measure and others a shortened version. Ideally, prevalence studies should include a representative sample and exclude any possible biases; the full ICU should have been administered to all participants, and their autism diagnosis confirmed. Two groups of researchers administered the ASPD, reporting different rates of CUTs. Leno et al. (41) reported that 51% of autistic adolescents fell into their category of high CUTs. In contrast, Rogers et al. (25) reported that their sample had a mean CUT score of 4.77, which is considered an ‘average’ CUT score. However, methodological differences between these studies make comparison challenging.
Three studies (33, 35, 36) with large, mixed gender samples reported a positive correlation between CUTs and autistic traits (r = .40, r = 0.60 and r = .51 respectively) amongst typically developing children. Studies reporting higher correlations recruited participants based upon having either low or high empathy levels which may have inflated the correlation.
Three studies made use of samples of those with an existing autism diagnosis (25, 40, 46). Svensson et al. (46) undertook a large twin study (N = 8762), and administered the Child Problematic Trait Inventory – Short Version to index psychopathy. They reported a significant relationship between psychopathy and autism amongst boys, r = .38, and girls, r = .33, bearing in mind that there may be validity issues with their choice of measure (94). Leno et al. (40) reported that higher CUTs were associated with more severe autistic traits, lower levels of prosocial behaviour and increased conduct problems. In contrast, Rogers et al. (25) reported no relationship between CUTs or psychopathy and autism and cognitive abilities in a much smaller study of autistic boys.
As expected, there was evidence that autism/autistic traits and CUTs/psychopathy in children is associated with distinct empathetic profiles. Children with autistic traits demonstrated deficits in cognitive empathy with intact affective empathy (35, 44, 45), and the same relationship was observed in children with diagnoses of autism (16, 17, 39, 48). These results appeared consistent despite the variation in the measurement of empathy and methods across studies. The relationship between CUTs/psychopathy and empathy appeared less clear; some studies reported diminished affective empathy and intact cognitive empathy (16, 17), whilst others reported diminished affective and cognitive empathy (35, 44).
Studies looking at the relationship between CUTs and autistic traits had contradictory results. While Pijper et al. (45) reported a negative association between CUTs and affective empathy in their sample of 10-year-old boys with conduct disorder as expected, the relationship was moderated by autistic traits; those with higher autistic traits and CUTs exhibited less impaired affective empathy. In contrast, Pasalich et al. (44) found that 5-year-old boys and girls with conduct disorder and high levels of both CUTs and autistic traits displayed the most pronounced deficits in affective empathy. These contradictory findings may be explained by: (a) sex differences: there is limited evidence that high CUTs and high autistic traits are associated with decreased affective empathy in girls only (35) and Pijper et al. (45) only included a sample of boys, and (b) difficulties with the measurement of empathy: both Georgiou et al. (35) and Pasalich et al. (44) used the Griffith Empathy Measure (95) and there is evidence that the affective empathy scale lacks construct validity (96). Age may also have impacted on these findings as there is evidence of improved performance with age on both types of empathy in all participants (17), as would be expected, and Pijper et al. (45) included older children relative to Pasalich et al. (44). Nonetheless, it’s worth noting that another study reported no relationship between age and empathy (35).
There was some evidence that psychopathy and autism are distinct constructs and the interaction of these may create a distinct cognitive profile. Bedford et al. (29) reported that reduced infant regulatory function (a precursor to executive functioning) is associated with later autistic traits but not CUTs in their longitudinal study, suggesting the two constructs are associated with differing executive functioning abilities. However, they did not include data for children older than seven years, and thus lacked information about continued development. When exploring the interaction of CUTs and autistic traits, Tye et al. (47) reported that autistic children with high CUTs exhibited enhanced conflict monitoring skills. Whilst this indicates a potentially advantageous role of CUTs on executive functioning in this group of children, the study was a small-scale preliminary study using a specific task to assess conflict monitoring, which may not be generalisable to other executive functioning skills. Two studies found that CUTs/psychopathic traits in autistic children were unrelated to the executive functioning skills associated with autism (25, 41).
Nine studies explored emotion recognition. Ibrahim et al. (37) reported that autistic children with CUTs displayed reduced amygdala activity to fearful faces compared to those with autism only. Conversely, Rogers et al. (25) found that all autistic children demonstrated fear recognition, regardless of the presence or absence of psychopathic traits, although this study focused on the wider construct of psychopathy (not CUTs). Results for sadness differed, with Rogers et al. (25) reporting that autistic boys with high psychopathic traits had poorer sadness recognition than those with low psychopathic traits. These studies used morphed faces (25) or still pictures (37) which may not accurately reflect how emotions are viewed during in-person social interactions. Bedford et al. (33) theorised that dynamic expressions are a more accurate representation of social interactions and compared static pictures with short video clips of people performing facial expressions. They reported that CUTs in typically developing children were associated with reduced emotion recognition for static facial expressions depicting anger and happiness. This association was not observed for dynamic facial expressions and disappeared when controlling for autistic traits. In contrast, autistic traits were associated with poorer overall emotion recognition for both static and dynamic expressions. Leno et al. (40) adapted the emotion recognition stimuli from Bedford et al. (33) and investigated emotion recognition in autistic adolescents, reporting that all participants demonstrated impairment in recognition of fearful faces with no relationship with autism severity or CUTs.
Several studies investigated the role of eye gaze on emotion recognition (33, 34, 40, 42). Bours et al. (34) reported that autistic adolescents and adolescents with CUTs both showed reduced fixations of the eye regions compared to typically developing adolescents. When considering the interaction of autism and CUTs, Leno et al. (40) found that CUTs in autistic adolescents was associated with longer times to identify fear and reduced eye contact during viewing of fearful faces. Leno et al. (42) then investigated the effect of cueing attention to the eyes in children with either CUTs or autistic traits, finding that this improved fear recognition in children with CUTs (no improvement in other emotions) but had the opposite effect on overall emotion recognition in their autistic trait group, suggesting different underlying mechanisms. However, the relationship between autistic traits, emotion recognition and gaze cueing was non-significant after controlling for conduct problems, emphasising the importance of considering co-occurring psychiatric traits.
Finally, Georgiou and Fanti (36) investigated the relationship between emotional recognition and physiological reactivity and reported that boys with CUTs exhibited low skin conductance reactivity during sad and fearful stimuli, whilst no associations were found amongst girls with CUTs or children of either gender with autistic traits. CUTs were associated with stronger heart reactivity to fear stimuli amongst children with low levels of autistic traits. They theorised that low skin conductance reflected fearlessness in children with CUTs, whilst stronger heart rate reflected thrill seeking. Unfortunately, the authors did not measure anxiety which may impact physiological responses.
Barnard-Brak and Richman (66) looked at the prevalence of autistic and psychopathic traits amongst a community sample (N = 723) without a diagnosis of autism, finding that 10% met screening cut off to indicate autistic traits and 12% met screening cut off to indicate psychopathic traits; 30% of the autistic trait group also meet criteria for psychopathic traits. The study relied on brief self-report measures of autistic [AQ-10; (79)] and psychopathic traits =[Dirty Dozen Scale; (82)], which are not diagnostic, and findings should be viewed in the context this limitation.
Several studies commented on the correlation between psychopathy and autism, with wide variation in the source of participants, measures, and methodology and all administering self-reports of psychopathic and autistic traits. In community samples, Barnard-Brak and Richman (66), reported a weak but significant positive corelation, r = .19, whilst other studies reported no significant correlation (70, 71). No correlation was found between autistic and psychopathic traits in a forensic setting (71).
On the other hand, Soderstrom et al. (75) recruited violent offenders and administered the gold standard, PCL-R, and reported a significant but small positive correlation between PCL-R total, factor two (unemotionality), factor three (behavioural dyscontrol), and autistic traits. No correlation between autistic traits and factor one (interpersonal) was found. Only one study differentiated primary and secondary psychopathy, reporting a positive correlation between autistic traits and secondary psychopathy traits only (74). All the aforementioned studies measured autistic traits, and only one study recruited adults with a diagnosis of autism and intellectual disability, observing a small but significant positive relationship between autism and CUTs (65).
Many studies recruited typically developing individuals without a diagnosis of autism and grouped them according to whether they had high or low autistic or psychopathic traits, drawing comparisons. As expected, findings indicated that psychopathic traits were associated with diminished affective empathy and intact cognitive empathy (18, 73, 77) whilst autistic traits are associated with reduced cognitive empathy but not affective empathy (18, 69). Of note, these studies all recruited participants with a mean age of 20-21 years, an age at which the human brain is still developing, and therefore results may not be applicable to older adults. In one study, Oliver et al. (73) failed to find a relationship between autistic traits and all measures of empathy, but the cognitive empathy test used was subject to ceiling effects, reducing the sensitivity of this task.
Studies of emotional contagion (thought to reflect affective empathy) highlighted impairment in typically developing adults with psychopathic traits and individuals with autistic traits, with greatest impairment observed in those with psychopathic traits (68). Helt et al. (68) observed that individuals with high traits of either autism or psychopathy both showed reduced yawn contagion, but the psychopathic trait group also showed reduced contagion of itching. The relationship between autistic traits and yawn contagion was moderated by eye gaze suggesting that some of the reduced contagion was due to less time spent looking at the eyes. These findings contribute to the evidence that psychopathy is associated with diminished affective empathy to a greater extent than autism. Similar results were found in autistic adults with a diagnosis; Noppari et al. (72) recruited violent offenders with high psychopathic traits, autistic adults and a typically developing comparison group. They observed weakened somatomotor responses in both their violent offender group and their autistic group (compared to their comparison group), however the most pronounced deficits were observed in the violent offender group.
Only one study investigated the interaction of psychopathic and autistic traits in relation to empathy. Gillespie et al. (67) measured primary and secondary psychopathy traits and autistic traits amongst university students and observed diminished cognitive ToM performance in students with both high primary psychopathy traits and autistic traits, concluding that people with co-occurring traits of both constructs have additional empathy impairments. No interaction effect was seen for affective ToM, which was uniquely associated with primary psychopathic tendencies. Unfortunately, this was a small-scale study, relying on self-report measures.
As with children, there was evidence that psychopathy and autism have different cognitive profiles and the authors of two studies compared high and low autistic or psychopathic trait groups on cognitive processes. The first group reported that adults with high autistic traits tend to blame vignette characters for their mistakes more so than those with low autistic traits, while those with high psychopathic traits attributed lower regret and guilt to vignette characters (69). The second group investigated moral judgment, reporting that the high psychopathic trait group judged misdemeanours less harshly than the low psychopathy group, with no differences in those with high or low autistic traits, leading them to conclude that moral judgement was only affected by psychopathy (77). Although offering insight into the cognitive profiles of autism and psychopathy, neither study investigated the interaction of the two constructs, and both relied on self-report measures from university students, limiting generalisability.
Two additional studies employed brain imagining techniques in individuals with autistic or psychopathic traits. Leno et al. (70) investigated neural feedback processing of social and non-social information, reporting atypical neural feedback processing in both trait groups. Autistic traits were associated with decreased sensitivity to social feedback, whilst those with traits of the antisocial domain of psychopathy showed decreased sensitivity to all feedback and those with traits of the interpersonal domain of psychopathy showed attenuated processing of negative feedback only. Skjegstad et al. (74) reported deficits in both trait groups for socio-affective processing, but again these showed different areas of association; autistic traits were associated with deficits in dorsal auditory processing streams (used for communication context encoding), whilst psychopathic traits were associated with hypoactivity in socio-affective processing networks. This study was exploratory and lacked an a priori power calculation, but both studies suggested distinct neural mechanisms across these constructs. Again, these studies did not investigate the interaction of these traits, failing to shed light on the ‘double hit’ hypothesis.
Regarding the interaction of psychopathy and autistic traits, (65) investigated the mediating role of CUTs in different types of challenging behaviours in a sample of autistic adults with intellectual disability. They reported that CUTs mediated the relationship between challenging behaviours directed towards the self, but not aggressive behaviours directed towards others, therefore proposing that CUTs may have a protective role for self-directed challenging behaviours. However, results must be viewed tentatively as this was a small-scale study that looked only at frequency and not severity of behaviour amongst those with both intellectual disability and autism.
This review sought to investigate the relationship between psychopathy and autism and what happens when they co-occur. Thirty-six studies were identified as meeting eligibility criteria, largely published within the last 10 years. The variation in methodologies, study focus, measures and samples recruited, made comparisons difficult, allowing only provisional conclusions to be drawn. Further, few studies investigated the co-occurrence of autism and psychopathy and directly investigated the ‘double hit’ hypothesis making it difficult to draw clear conclusions.
Across all ages, an increased prevalence of CUTs/psychopathy in autistic individuals or in those with high autistic traits appeared to exist relative to the general population and regardless of methodology used. Prevalence rates ranged from 22%-56%, whilst prevalence of psychopathy in the general population is estimated at 4.5% (7). It remains unclear whether autistic children are at risk of developing CUTs and later psychopathy, or whether autism and CUTs/psychopathy are similar constructs and overlap. Multiple limitations were associated with the measures used, drawing urgency to the need to develop measurement tools sensitive enough to untangle this relationship.
Generally, authors reported a positive correlation between autistic and psychopathic traits amongst children (33, 35, 36). However, the authors of one study reported no significant correlation between autistic symptoms and CUTs in diagnosed autistic boys (25). In adults, the positive relationship between autistic and psychopathic traits was generally attenuated relative to children (66, 75) or not found (70, 71). This was also observed in adults with autism and intellectual disability (65). The relationship between psychopathy and autism amongst adults and children may differ due to issues with the sensitivity of measurement tools and development; autistic and psychopathic traits will likely change with maturation.
Several papers evidenced that although the constructs are both associated with empathy dysfunction, the underlying mechanisms differ. In adults, psychopathy/psychopathic traits were generally found to be associated with diminished affective empathy and intact cognitive empathy, whilst the inverse relationship was seen in autism/autistic traits which is consistent with both theory and other research (21, 97). A recent meta-analysis confirmed that psychopathy is associated with diminished affective empathy (98). Research about autism and affective empathy is inconsistent but points towards fewer deficits in this area compared to cognitive empathy (99), with some studies reporting intact affective empathy in autistic individuals (100).
In children, autism/autistic traits were also associated with difficulties with cognitive empathy but not affective empathy while the results for those with CUTs/psychopathy were inconsistent. Some studies reported deficits in both types of empathy and others reported difficulties with affective empathy only. This inconsistency may be due to developmental maturation throughout childhood (101) or gender, as children of both genders with psychopathic traits had difficulties with cognitive empathy but there was some evidence that males overcame these difficulties during their pubertal years (102). However, the authors of one study reported no relationship between age and empathy (35), which is unexpected, whilst another reported improved performance with increasing chronological age (17); however, they included a broader age range (six to 17 years) of boys only with intact cognitive empathy, whereas Georgiou et al. (35) included younger boys and girls (three to eight years).
In the current review, the findings from studies about emotion recognition were mixed. In adults and children, CUTs/psychopathy was associated with reduced emotion experience and emotion recognition ability, in particular, recognition of fear and sadness was diminished. These deficits largely remained in the presence of autism, for example, autistic boys with psychopathic traits showed poorer sadness recognition (25), and reduced amygdala activity to fearful faces was observed in autistic children with CUTs (37). However, results were inconsistent across studies with one study reporting a non-significant association between CUTs and emotion recognition after controlling for autism (33).
Previous research has indicated that fear recognition deficits in psychopathy are associated with poor attention to the eyes, resulting in blunted affect and impaired processing of affective cues in others (103). This association has been found across many samples, including children with CUTs (24, 103), community samples (104) and psychopathic offenders (105, 106), with similar findings in the current review identified by Bours et al. (34). Regarding the co-occurrence of CUTs and autism, it appears that deficits in eye gaze remain, with autistic children with CUTs taking longer to identify fear and showing reduced eye contact when viewing fearful faces, relative to autistic children with fewer CUTs (40).
Cueing to the eyes has been shown to improve fear recognition in children with CUTs (103). This was replicated in a single study identified in the current review, but the converse relationship was found in an autistic trait group who evidenced reduced fear recognition following cueing (42). It is possible that autistic individuals view eyes as threatening or over-arousing stimuli, thus avoiding this area and missing social processing cues which then interferes with emotion processing (107). This may explain why cueing to the eyes reduced fear recognition ability in autistic individuals but not in individuals with CUTs.
With regards to the ‘double hit’, Rogers et al. (25) reported that although psychopathy and autism can co-occur, they are not part of the same construct, finding that autistic boys with CUTs have additional impairments in moral convention distinction and sadness recognition. In the current review, two studies reported increased empathy deficits in individuals with traits of both; Pasalich et al. (44) found that boys with elevated CUTs and autistic traits showed greater impairment in affective empathy and in adults, and Gillespie et al. (67) found that the interaction of autistic and psychopathic traits was associated with reduced cognitive ToM but not affective ToM. They defined cognitive ToM as the ability to infer thoughts, intentions and beliefs of another and affective ToM as the ability to understand another’s emotions. These studies offer support to the ‘double hit’ hypothesis, suggesting increased deficits when the constructs co-exist. However, contrasting results were reported by other studies which indicated that the co-occurrence of these constructs offers enhanced skills, including less impaired affective empathy (45) and greater conflict monitoring skills (47). Unfortunately, based upon the studies included with the current systematic review, it was difficult to coherently describe the clinical manifestation of co-occurring autism and psychopathy due to some mixed findings. However, our findings offer support to the suggestion that autism and psychopathy are distinct constructs which further alter the empathic ability and cognitive ability of an individual when they co-exist.
In the current review, the search strategy restricted the search terms to the title only and included the specifier ‘NOT psychopathology’. Although this was done in efforts to screen out inapplicable results, it could have potentially led to the exclusion of some studies. The inclusion of the grey literature was a strength, but only one unpublished thesis was found. It is also important to recognise the wide focus of the review as both a strength and a limitation. Whilst this allowed for inclusion of a broad range of research, the wide focus also made it challenging to draw more specific conclusions, which may have been possible by restricting the eligibility criteria. Psychopathy and autism are highly heterogeneous, and the studies recruited a broad range of participants which is perhaps reflected in the variation of results.
In terms of limitations of the included research, only two studies (67, 74) differentiated between primary and secondary psychopathy and none considered the impact of adverse childhood experiences. In psychopathy research, children with CUTs showed strongest deficits in emotion recognition when there was no history of maltreatment, suggesting that this may be a feature of the primary variant only (108). As adverse childhood experiences are common in autistic children (109), this is an important variable to consider when seeking to determine the relationship between psychopathy and autism.
The increased prevalence of CUTs/psychopathy in autistic individuals underscores the importance of assessing psychopathy as part of the evaluation of autistic offenders or those at risk of offending to better understand their presentation. Understanding this at an early stage could lead to more targeted treatment options. The studies included within this review were characterised by multiple difficulties with measurement, including lack of validated measures for identifying psychopathic traits within autistic individuals, highlighting this as an area requiring attention. There was a lack of intervention studies, however there was some evidence to suggest that interventions to improve eye contact may be a helpful strategy to improve emotion recognition in psychopathic individuals but may have a detrimental impact for autistic individuals (42). The impact of such interventions for individuals with both psychopathy and autism is unclear but clinicians should be aware of the different underlying mechanisms and consider this with implementation of any emotion recognition strategies used.
Although research in this area appear to have grown substantially since Rogers et al. (25) introduced the concept of the ‘double hit’ hypothesis, clear gaps remain. Firstly, there remains a lack of research focusing on the interaction of both autism and psychopathy which is critical in furthering our understanding of the clinical manifestation of the two constructs when they co-occur. Age and gender remain relatively unexplored variables, with fewer studies focusing on females which may be important given indicated sex differences in psychopathy (110). The presentation of primary and secondary psychopathy variants in autistic individuals is unexplored and may be important as autistic individuals experience increased adverse childhood events. Furthermore, future research would benefit from longitudinal studies exploring the developmental trajectory of autistic adults with co-morbid psychopathy or autistic children with CUT. Finally, to aid research in this area, it is essential to establish the validity of measures of psychopathy within autistic individuals, as well as the validity of measures of autism with those scoring high on measures of psychopathy. It was notable that there was a lack of studies about autistic traits amongst those with high psychopathy. These directions will all support better understanding of the relationship between psychopathy and autism and support the development of appropriate care pathways within clinical and forensic systems.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
KM: Methodology, Formal analysis, Conceptualization, Writing – review & editing, Writing – original draft. HW: Formal analysis, Writing – review & editing. FB: Supervision, Writing – review & editing. PL: Writing – review & editing, Writing – original draft, Supervision, Methodology, Formal analysis, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organisation. ICD-11: International classification of diseases (2022). Available at: https://icd.who.int/.
2. Zeidan J, Fombonne E, Scorah J, Ibrahim A, Durkin MS, Saxena S, et al. Global prevalence of autism: A systematic review update. Autism Res. (2022) 15:778–90. doi: 10.1002/aur.2696
3. Hill AP, Zuckerman KE, Hagen AD, Kriz DJ, Duvall SW, Van Santen J, et al. Aggressive behavior problems in children with autism spectrum disorders: Prevalence and correlates in a large clinical sample. Res Autism Spectr Disord. (2014) 8:1121–33. doi: 10.1016/J.RASD.2014.05.006
4. Mazurek MO, Kanne SM, Wodka EL. Physical aggression in children and adolescents with autism spectrum disorders. Res Autism Spectr Disord. (2013) 7:455–65. doi: 10.1016/j.rasd.2012.11.004
5. Cleckley H. The mask of sanity; an attempt to reinterpret the so-called psychopathic personality. Mosby. (1941).
7. Sanz-García A, Gesteira C, Sanz J, Mp G-V. Prevalence of psychopathy in the general adult population: A systematic review and meta-analysis. Front Psychol. (2021) 12:661044. doi: 10.3389/fpsyg.2021.661044
8. Hare RD. Psychopathy as a risk factor for violence. Psychiatr Q. (1999) 70:181–97. doi: 10.1023/a:1022094925150
9. Yildirim BO, Derksen JJL. Clarifying the heterogeneity in psychopathic samples: Towards a new continuum of primary and secondary psychopathy. Aggression Violent Behav. (2015) 24:9–41. doi: 10.1016/j.avb.2015.05.001
10. Cardinale EM, Marsh AA. The reliability and validity of the Inventory of Callous Unemotional Traits: A meta-analytic review. Assessment. (2020) 27:57–71. doi: 10.1177/1073191117747392
11. Tharshini NK, Ibrahim F, Kamaluddin MR, Rathakrishnan B, Che Mohd Nasir N. The link between individual personality traits and criminality: A systematic review. Int J Environ Res Public Health. (2021) 18:8663. doi: 10.3390/ijerph18168663
12. Collins J, Horton K, Gale-St Ives E, Murphy G, Barnoux M. A systematic review of autistic people and the criminal justice system: An update of King and Murphy, (2014). J Autism Dev Disord. (2022). doi: 10.1007/s10803-022-05590-3
13. Newman C, Cashin A, Waters C. A hermeneutic phenomenological examination of the lived experience of incarceration for those with autism. Issues Ment Health Nurs. (2015) 36:632–40. doi: 10.3109/01612840.2015.1014587
14. Bleil Walters J, Hughes TL, Sutton LR, Marshall SN, Crothers LM, Lehman C, et al. Maltreatment and depression in adolescent sexual offenders with an autism spectrum disorder. J Child Sexual Abuse. (2013) 22:72–89. doi: 10.1080/10538712.2013.735357
15. Blair RJR. Fine cuts of empathy and the amygdala: Dissociable deficits in psychopathy and autism. Q J Exp Psychol. (2008) 61:157–70. doi: 10.1080/17470210701508855
16. Jones AP, Happé FGE, Gilbert F, Burnett S, Viding E. Feeling, caring, knowing: different types of empathy deficit in boys with psychopathic tendencies and autism spectrum disorder. J Child Psychol Psychiatry. (2010) 51:1188–97. doi: 10.1111/J.1469-7610.2010.02280.X
17. Schwenck C, Mergenthaler J, Keller K, Zech J, Salehi S, Taurines R, et al. Empathy in children with autism and conduct disorder: group-specific profiles and developmental aspects. J Child Psychol Psychiatry. (2012) 53:651–9. doi: 10.1111/j.1469-7610.2011.02499.x
18. Lockwood PL, Bird G, Bridge M, Viding E, Decety J, Frith C. Dissecting empathy: high levels of psychopathic and autistic traits are characterized by difficulties in different social information processing domains. Front Hum Neurosci. (2013) 7:760. doi: 10.3389/fnhum.2013.00760
19. Garrigan B, Adlam ALR, Langdon PE. Moral decision-making and moral development: Toward an integrative framework. Dev Rev. (2018) 49:80–100. doi: 10.1016/j.dr.2018.06.001
20. Baron-Cohen S, Wheelwright S. The Empathy Quotient: An investigation of adults with asperger syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord. (2004) 34. doi: 10.1023/b:jadd.0000022607.19833.00
21. Blair J, Sellars C, Strickland I, Clark F, Williams A, Smith M, et al. Theory of mind in the psychopath. J Forensic Psychiatry. (1996) 7:15–25. doi: 10.1080/09585189608409914
22. Blair RJR, Peschardt KS, Budhani S, Mitchell DGV, Pine DS. The development of psychopathy. J Child Psychol Psychiatry Allied Disciplines. (2006) 47:262–76. doi: 10.1111/J.1469-7610.2006.01596.X
23. Dawel A, O’kearney R, Mckone E, Palermo R. Not just fear and sadness: Meta-analytic evidence of pervasive emotion recognition deficits for facial and vocal expressions in psychopathy. Neurosci Biobehav Rev. (2012) 36:2288–304. doi: 10.1016/j.neubiorev.2012.08.006
24. Dadds MR, Jambrak J, Pasalich D, Hawes DJ, Brennan J. Impaired attention to the eyes of attachment figures and the developmental origins of psychopathy. J Child Psychol Psychiatry Allied Disciplines. (2011) 52:238–45. doi: 10.1111/J.1469-7610.2010.02323.X
25. Rogers J, Viding E, Blair RJ, Frith U, Happé F. Autism spectrum disorder and psychopathy: Shared cognitive underpinnings or double hit? psychol Med. (2006) 36:1789–98. doi: 10.1017/S0033291706008853
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PloS Med. (2009) 6. doi: 10.1371/journal.pmed.1000097
27. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
28. Joanna Briggs Institute. Checklist for analytical cross sectional studies. (2020). Available at: https://jbi.global/critical-appraisal-tools.
29. Bedford R, Gliga T, Hendry A, Jones EJH, Pasco G, Charman T, et al. Infant regulatory function acts as a protective factor for later traits of autism spectrum disorder and attention deficit/hyperactivity disorder but not callous unemotional traits. J Neurodev Disord. (2019) 11. doi: 10.1186/s11689-019-9274-0
30. Joanna Briggs Institute. Checklist for cohort studies (2020). Available at: https://jbi.global/critical-appraisal-tools.
31. Buccheri RK, Sharifi C. Critical appraisal tools and reporting guidelines for evidence-based practice. Worldviews Evidence-Based Nurs. (2017) 14:463–72. doi: 10.1111/wvn.12258
32. Popay J, Robert H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. In: A product from the ESRC methods programme (2006). doi: 10.1001/archderm.1985.01660090059014
33. Bedford R, Leno V, Wright N, Bluett-Duncan M, Smith TJ, Anzures G, et al. Emotion recognition performance in children with callous unemotional traits is modulated by co-occurring autistic traits. J Clin Child Adolesc Psychol. (2021) 50:811–27. doi: 10.1080/15374416.2020.1833338
34. Bours C, Bakker-Huvenaars M, Tramper J, Bielczyk N, Scheepers F, Nijhof K, et al. Emotional face recognition in male adolescents with autism spectrum disorder or disruptive behavior disorder: an eye-tracking study. Eur Child Adolesc Psychiatry. (2018) 27:1143–57. doi: 10.1007/s00787-018-1174-4
35. Georgiou G, Demetriou CA, Fanti KA. Distinct empathy profiles in callous unemotional and autistic traits: Investigating unique and interactive associations with affective and cognitive empathy. J Abnormal Child Psychol. (2019) 47:1863–73. doi: 10.1007/s10802-019-00562-1
36. Georgiou G, Fanti KA. Physiological reactivity in children with high callous-unemotional and autistic traits: investigating unique and interactive effects. Eur Child Adolesc Psychiatry. (2021) 30:1709–22. doi: 10.1007/s00787-020-01643-z
37. Ibrahim K, Eilbott JA, Ventola P, He G, Pelphrey KA, McCarthy G, et al. Reduced amygdala–prefrontal functional connectivity in children with autism spectrum disorder and co-occurring disruptive behavior. Biol Psychiatry: Cogn Neurosci Neuroimaging. (2019) 4:1031–41. doi: 10.1016/J.BPSC.2019.01.009
38. Jones AP, Larsson H, Ronald A, Rijsdijk F, Busfield P, Mcmillan A, et al. Phenotypic and aetiological associations between psychopathic tendencies, autistic traits, and emotion attribution. Criminal Justice Behav. (2009) 36(11):1198–212. doi: 10.1177/0093854809342949
39. Klapwijk ET, Aghajani M, Colins OF, Marijnissen GM, Popma A, Van Lang NDJ, et al. Different brain responses during empathy in autism spectrum disorders versus conduct disorder and callous-unemotional traits. J Child Psychol Psychiatry Allied Disciplines. (2016) 57:737–47. doi: 10.1111/jcpp.12498
40. Leno V, Bedford R, Chandler S, White P, Yorke I, Charman T, et al. Callous-unemotional traits in youth with autism spectrum disorder (ASD): replication of prevalence estimates and associations with gaze patterns when viewing fearful faces. Dev Psychopathol. (2021) 33:1220–8. doi: 10.1017/S0954579420000449
41. Leno V, Charman T, Pickles A, Jones C, Baird G, Happe F, et al. Callous-unemotional traits in adolescents with autism spectrum disorder. Br J Psychiatry. (2015) 207:392–9. doi: 10.1192/bjp.bp.114.159863
42. Leno V, Pickard H, Cybulska L, Smith T, Munafo M, Penton-Voak I, et al. Associations between emotion recognition and autistic and callous-unemotional traits: differential effects of cueing to the eyes. J Child Psychol Psychiatry Allied Disciplines. (2022). doi: 10.1111/jcpp.13736
43. Parys KS. The importance of differentiating between traits of autism spectrum disorders and callous and unemotional traits (2016). Available at: https://dsc.duq.edu/cgi/viewcontent.cgi?article=1102&context=etd.
44. Pasalich DS, Dadds MR, Hawes DJ. Cognitive and affective empathy in children with conduct problems: Additive and interactive effects of callous-unemotional traits and autism spectrum disorders symptoms. Psychiatry Res. (2014) 219:625–30. doi: 10.1016/j.psychres.2014.06.025
45. Pijper J, De Wied M, Van Rijn S, Van Goozen S, Swaab H, Meeus W. Callous unemotional traits, autism spectrum disorder symptoms and empathy in boys with oppositional defiant disorder or conduct disorder. Psychiatry Res. (2016) 245:340–5. doi: 10.1016/j.psychres.2016.08.053
46. Svensson O, Sörman K, Durbeej N, Lichtenstein P, Anckarsäter H, Kerekes N, et al. Associations between conduct disorder, neurodevelopmental problems and psychopathic personality traits in a Swedish twin youth population. J Psychopathol Behav Assess. (2018) 40:586–92. doi: 10.1007/s10862-018-9689-z
47. Tye C, Bedford R, Asherson P, Ashwood KL, Azadi B, Bolton P, et al. Callous-unemotional traits moderate executive function in children with ASD and ADHD: A pilot event-related potential study. Dev Cogn Neurosci. (2017) 26:84–90. doi: 10.1016/J.DCN.2017.06.002
48. Vilas SP, Reniers RLEP, Ludlow AK. An investigation of behavioural and self-reported cognitive empathy deficits in adolescents with autism spectrum disorders and adolescents with behavioural difficulties. Front Psychiatry. (2021) 12:717877. doi: 10.3389/fpsyt.2021.717877
49. Le Couteur A, Rutter M, Lord C, Rios P, Robertson S, Holdgrafer M, et al. Autism diagnostic interview: A standardized investigator-based instrument. J Autism Dev Disord. (1989) 19:363–87. doi: 10.1007/BF02212936
50. Rutter M, Le Couteur A, Lord C. ADI-R: autism diagnostic interview-revised (ADI-R). Los Angeles, CA: Western Psychological Services (2003).
51. Gotham K, Risi S, Pickles A, Lord C. The autism diagnostic observation schedule (ADOS). J Autism Dev Disord. (2007) 37:613–27. doi: 10.1007/s10803-006-0280-1
52. Lord C, Rutter M, DiLavore P, Risi S, Gotham K, Bishop S. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2). Western Psychological Services. (2021).
54. Bryson SE, Zwaigenbaum L, McDermott C, Rombough V, Brian J. The autism observation scale for infants: Scale development and reliability data. J Autism Dev Disord. (2008) 38:731–8. doi: 10.1007/s10803-007-0440-y
55. Larson T. A-TAC - the autism–tics, ADHD and other comorbidities inventory: studies in reliability and validity. Lund: Lund University (2013).
56. Williams J, Scott F, Stott C, Allison C, Bolton P, Baron-Cohen S, et al. ). The CAST (Childhood asperger syndrome test): test accuracy. Autism. (2005) 9:45–68. doi: 10.1177/1362361305049029
57. Schopler E, Van Bourgondien M, Wellman G, Love S. Childhood autism rating scale – 2 (CARS-2). Los Angeles, CA: Western Psychological Services (2010).
58. Colins OF, Andershed H, Frogner L, Lopez-Romero L, Veen V, Andershed A-K. A new measure to assess psychopathic personality in children: The Child Problematic Traits Inventory. J Psychopathol Behav Assess. (2014) 36:4–21. doi: 10.1007/s10862-013-9385-y
59. Frick P. The inventory of callous-unemotional traits. New Orleans, LA: University of New Orleans (2004).
60. Rutter M, Bailey A, Lord C. The social communication questionnaire. Los Angeles, CA: Western Psychological Services (2003).
61. Goodman R. The strengths and difficulties questionnaire: A research note. J Child Psychol Psychiat. (1997) 38:581–6. doi: 10.1037/t00540-000
62. Constantino JN, Davis SA, Todd RD, Schindler MK, Gross MM, Brophy SL, et al. Validation of a brief quantitative measure of autistic traits: Comparison of the Social Responsiveness Scale with the Autism Diagnostic Interview-Revised. J Autism Dev Disord. (2003) 33.
63. Constantino J, Gruber C. Social responsiveness scale, second edition (SRS-2). Torrance, CA: Western Psychological Services (2012).
64. Andershed H, Kerr M, Stattin H, Levander S. Psychopathic traits in non-referred youths: A new assessment tool. In: Blaauw E, Sheridan L, editors. Psychopaths: Current international perspectives. Torrance, CA: Elsevier (2012).
65. Álvarez-Couto M, García-Villamisar D, Del Pozo A, Ia Alvarez-Couto M, Garc Ia-Villamisar D. Callous unemotional traits mediate the presence of challenging behaviors in adults with autism spectrum disorder and intellectual disability. (2023). doi: 10.1080/20473869.2023.2171756
66. Barnard-Brak L, Richman DM. Autistic and psychopathic traits among a community-based sample of adults. Deviant Behav. (2021) 42:950–7. doi: 10.1080/01639625.2019.1706357
67. Gillespie SM, Mitchell IJ, Abu-Akel AM. Autistic traits and positive psychotic experiences modulate the association of psychopathic tendencies with theory of mind in opposite directions. Sci Rep. (2017) 7. doi: 10.1038/s41598-017-06995-2
68. Helt M, Sorensen T, Scheub R, Nakhle M, Luddy A. Patterns of contagious yawning and itching differ amongst adults with autistic traits vs. psychopathic traits. Front Psychol. (2021) 12:645310. doi: 10.3389/fpsyg.2021.645310
69. Jameel L, Vyas K, Bellesi G, Crawford S, Channon S. Thinking about other’s mistakes: contrasting patterns of performance in groups high or low in autistic or psychopathic traits. Cogn Neuropsychiatry. (2019) 24:369–85. doi: 10.1080/13546805.2019.1667317
70. Leno V, Naples A, Cox A, Rutherford H, McPartland JC. Common and distinct modulation of electrophysiological indices of feedback processing by autistic and psychopathic traits. Soc Neurosci. (2016) 11:455–66. doi: 10.1080/17470919.2015.1108223
71. Loureiro D, MaChado A, Silva T, Veigas T, Ramalheira C, Cerejeira J. Higher autistic traits among criminals, but no link to psychopathy: Findings from a high-security prison in Portugal. J Autism Dev Disord. (2018) 48:3010–20. doi: 10.1007/s10803-018-3576-z
72. Noppari T, Sun L, Lukkarinen L, Putkinen V, Tani P, Lindberg N, et al. Brain structural alterations in autism and criminal psychopathy. NeuroImage: Clin. (2022) 32:103116. doi: 10.1016/j.nicl.2022.103116
73. Oliver LD, Neufeld RWJ, Dziobek I, Mitchell DGV. Distinguishing the relationship between different aspects of empathic responding as a function of psychopathic, autistic, and anxious traits. Pers Individ Dif. (2016) 99:81–8. doi: 10.1016/j.paid.2016.04.058
74. Skjegstad CL, Trevor C, Swanborough H, Roswandowitz C, Mokros A, Habermeyer E, et al. Psychopathic and autistic traits differentially influence the neural mechanisms of social cognition from communication signals. Trans Psychiatry. (2022) 12:494. doi: 10.1038/s41398-022-02260-x
75. Soderstrom H, Nilsson T, Sjodin AK, Carlstedt A, Forsman A. The childhood-onset neuropsychiatric background to adulthood psychopathic traits and personality disorders. Compr Psychiatry. (2005) 46:111–6. doi: 10.1016/j.comppsych.2004.07.030
76. Sun L, Lukkarinen L, Noppari T, Nazari-Farsani S, Putkinen V, Seppälä K, et al. Aberrant motor contagion of emotions in psychopathy and high-functioning autism. Cereb Cortex. (2023). doi: 10.1093/cercor/bhac072
77. Vyas K, Jameel L, Bellesi G, Crawford S, Channon S. Derailing the trolley: Everyday utilitarian judgments in groups high versus low in psychopathic traits or autistic traits. Psychiatry Res. (2017) 250:84–91. doi: 10.1016/j.psychres.2017.01.054
78. Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The Autism-Spectrum Quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord. (2001) 31. doi: 10.1023/a:1005653411471
79. Allison C, Auyeung B, Baron-Cohen S. Toward brief “Red Flags” for autism screening: The Short Autism Spectrum Quotient and the Short Quantitative Checklist for Autism in toddlers in 1,000 cases and 3,000 controls. J Am Acad Child Adolesc Psychiatry. (2012) 51:202–212.e7. doi: 10.1016/J.JAAC.2011.11.003
80. Viktorinova M, McPartland J. Asperger syndrome diagnostic interview. In: Volkmar F, editor. Encyclopedia of autism spectrum disorders. New York: Springer (2013). p. 252–6.
81. Sappok T, Gaul I, Bergmann T, Dziobek I, Bölte S, Diefenbacher A, et al. The Diagnostic Behavioral Assessment for autism spectrum disorder—Revised: A screening instrument for adults with intellectual disability suspected of autism spectrum disorders. Res Autism Spectr Disord. (2014) 8:362–75.
82. Jonason PK, Webster GD. The dirty dozen: A concise measure of the dark triad. psychol Assess. (2010) 22:420–32. doi: 10.1037/a0019265
83. Levenson MR, Kiehl KA, Fitzpatrick CM. Assessing psychopathic attributes in a non institutionalized population. J Pers Soc Psychol. (1995) 68:151–8. doi: 10.1037//0022-3514.68.1.151
84. Lilienfeld S, Widows M. Psychopathic personality inventory revised. psychol Assess Resour. (2005).
85. Lilienfeld S, Hess T. Psychopathic personality traits and somatization: Sex differences and the mediating role of negative emotionality. J Psychopathol Behav Assess. (2001) 23:11–24. doi: 10.1023/A:1011035306061
86. Paulhuss D, Neumann C, Hare R. Manual for the hare self-report psychopathy scale. Toronto: Multi-Health Systems (20014).
87. Patrick CJ, Fowles DC, Krueger RF. Triarchic conceptualization of psychopathy: Developmental origins of disinhibition, boldness, and meanness. Dev Psychopathol. (2009) 21:913–38. doi: 10.1017/S0954579409000492
88. O’Nions E, Tick B, Rijsdijk F, Happé F, Plomin R, Ronald A, et al. Examining the genetic and environmental associations between autistic social and communication deficits and psychopathic callous-unemotional traits. PloS One. (2015) 10. doi: 10.1371/journal.pone.0134331
89. Lord C, Rutter M, DiLavore P, Risi S. Autism diagnostic observation schedule (ADOS). Los Angeles, CA: Western Psychological Services (1999).
90. Conner CM, Cramer RD, McGonigle JJ. Examining the diagnostic validity of autism measures among adults in an outpatient clinic sample. Autism Adulthood. (2019) 1:60–8. doi: 10.1089/AUT.2018.0023
91. Hare RD, Neumann CS. Psychopathy as a clinical and empirical construct. Annu Rev Clin Psychol. (2008) 4:217–46. doi: 10.1146/annurev.clinpsy.3.022806.091452
92. Edens JF, Hart SD, Johnson DW, Johnson JK, Olver ME. Use of the personality assessment inventory to assess psychopathy in offender populations. psychol Assess. (2000) 12:132–9. doi: 10.1037/1040-3590.12.2.132
93. Bakhtiari R, Hutchison SM, Iarocci G. How do children and youth with autism spectrum disorder self-report on behavior? A study of the validity indexes on the Behavior Assessment System for Children, Second Edition, self-report of personality. Autism. (2021) 25:1100–13. doi: 10.1177/1362361320984601/FORMAT/EPUB
94. Colins OF, Roetman PJ, Lopez-Romero L, Andershed H. Assessing psychopathic traits among children: The first validation study of the child problematic traits inventory in a clinical sample. Assessment. (2020) 27:1242–57. doi: 10.1177/1073191119832654/FORMAT/EPUB
95. Dadds MR, Hunter K, Hawes DJ, Frost ADJ, Vassallo S, Bunn P, et al. A measure of cognitive and affective empathy in children using parent ratings. Child Psychiatry Hum Dev. (2008) 39:111–22. doi: 10.1007/s10578-007-0075-4
96. Murphy BA. The Griffith Empathy Measure does not validly distinguish between cognitive and affective empathy in children. Aust Psychol. (2019) 54:159–64. doi: 10.1111/ap.12336
97. Kimhi Y. Theory of mind abilities and deficits in autism spectrum disorders. Topics Lang Disord. (2014) 34:329–43. doi: 10.1097/TLD.0000000000000033
98. Campos C, Pasion R, Azeredo A, Ramião E, Mazer P, Macedo I, et al. Refining the link between psychopathy, antisocial behavior, and empathy: A meta-analytical approach across different conceptual frameworks. Clin Psychol Rev. (2022) 94. doi: 10.1016/j.cpr.2022.102145
99. Fatima M, Babu N. Cognitive and affective empathy in autism spectrum sisorders: A meta-analysis. Rev J Autism Dev Disord. (2023). doi: 10.1007/s40489-023-00364-8
100. Santiesteban I, Gibbard C, Drucks H, Clayton N, Banissy MJ, Bird G. Individuals with autism share others’ Emotions: evidence from the continuous affective rating and empathic responses (CARER) task. J Autism Dev Disord. (2021) 51:391–404. doi: 10.1007/s10803-020-04535-y
101. Dorris L, Young D, Barlow J, Byrne K, Hoyle R. Cognitive empathy across the lifespan. Dev Med Child Neurol. (2022) 64:1524–31. doi: 10.1111/dmcn.15263
102. Dadds MR, Hawes DJ, Frost ADJ, Vassallo S, Bunn P, Hunter K, et al. Learning to “talk the talk”: The relationship of psychopathic traits to deficits in empathy across childhood. J Child Psychol Psychiatry Allied Disciplines. (2009) 50:599–606. doi: 10.1111/J.1469-7610.2008.02058.X
103. Dadds MR, Perry Y, Hawes DJ, Merz S, Riddell AC, Haines DJ, et al. Attention to the eyes and fear-recognition deficits in child psychopathy. Br J Psychiatry. (2006) 189:280–1. doi: 10.1192/bjp.bp.105.018150
104. Gillespie SM, Rotshtein P, Wells LJ, Beech AR, Mitchell IJ. Psychopathic traits are associated with reduced attention to the eyes of emotional faces among adult male non-offenders. Front Hum Neurosci. (2015) 9:552. doi: 10.3389/fnhum.2015.00552
105. Dargis M, Wolf R, Koenigs M. Psychopathic traits are associated with reduced fixations to the eye region of fearful faces. J Abnormal Psychol. (2018) 127:43–50. doi: 10.1037/abn0000322.supp
106. Gehrer NA, Scheeff J, Jusyte A, Schönenberg M. Impaired attention toward the eyes in psychopathic offenders: Evidence from an eye tracking study. Behav Res Ther. (2019) 118:121–9. doi: 10.1016/j.brat.2019.04.009
107. Kliemann D, Dziobek I, Hatri A, Steimke R, Heekeren HR. Atypical reflexive gaze patterns on emotional faces in autism spectrum disorders. J Neurosci. (2010) 30:12281–7. doi: 10.1523/JNEUROSCI.0688-10.2010
108. Dadds MR, Kimonis ER, Schollar-Root O, Moul C, Hawes DJ. Are impairments in emotion recognition a core feature of callous-unemotional traits? Testing the primary versus secondary variants model in children. Dev Psychopathol. (2018) 30:67–77. doi: 10.1017/S0954579417000475
109. Hoover DW, Kaufman J. Adverse childhood experiences in children with autism spectrum disorder. Curr Opin Psychiatry. (2018) 31:128–32. doi: 10.1097/YCO.0000000000000390
Keywords: autism, psychopathy, callous unemotional traits, review - systematic, narrative synthesis
Citation: Maguire K, Warman H, Blumenfeld F and Langdon PE (2024) The relationship between psychopathy and autism: a systematic review and narrative synthesis. 15:1375170. doi: 10.3389/fpsyt.2024.1375170
Received: 23 January 2024; Accepted: 13 March 2024;
Published: 27 March 2024.
Edited by:
Kleanthes K. Grohmann, University of Cyprus, CyprusReviewed by:
Alexander Westphal, Yale University, United StatesCopyright © 2024 Maguire, Warman, Blumenfeld and Langdon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter E. Langdon, cGV0ZXIubGFuZ2RvbkB3YXJ3aWNrLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.