 Yuanli Liu
Yuanli Liu Chaomei Chen
Chaomei Chen Ying Zhou3
Ying Zhou3 Na Zhang
Na Zhang Shen Liu
Shen Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 01 March 2024
Sec. Personality Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1361535
Borderline personality disorder (BPD), a complex and severe psychiatric disorder, has become a topic of considerable interest to current researchers due to its high incidence and severity of consequences. There is a lack of a bibliometric analysis to visualize the history and developmental trends of researches in BPD. We retrieved 7919 relevant publications on the Web of Science platform and analyzed them using software CiteSpace (6.2.R4). The results showed that there has been an overall upward trend in research interest in BPD over the past two decades. Current research trends in BPD include neuroimaging, biological mechanisms, and cognitive, behavioral, and pathological studies. Recent trends have been identified as “prevention and early intervention”, “non-pharmacological treatment” and “pathogenesis”. The results are like a reference program that will help determine future research directions and priorities.
Borderline personality disorder (BPD) is a complex and severe psychiatric disorder characterized by mood dysregulation, interpersonal instability, self-image disturbance, and markedly impulsive behavior (e.g., aggression, self-injury, suicide) (1). In addition, people with BPD may have chronic, frequent, random feelings of emptiness, fear, and so on. These symptoms often lead them to use unhealthy coping mechanisms in response to negative emotions, such as alcohol abuse (2). BPD has a long course, which makes treatment difficult and may have a negative impact on patients’ quality of life (3). Due to its clinical challenge, BPD is by far the most studied category of personality disorder (4). This disorder is present in 1−3% of the general population as well as in 10% of outpatients, 15−20% of inpatients, and 30−60% of patients with a diagnosed personality disorder, and has a suicide rate of up to 10% (5, 6). Families of individuals with serious mental illness often experience distress, and those with relatives diagnosed with BPD tend to carry a heavier burden compared to other mental illnesses (7, 8). As early as the 20th century, scholars began describing BPD and summarizing its symptoms. However, there was some debate regarding the precise definition of BPD.
In the past few decades, the research community has made remarkable progress in the study of BPD, equipping us with a wider range of perspectives and tools for understanding this intricate condition. However, numerous challenges still remain to be tackled by researchers. Diagnosing BPD is inherently challenging and often more difficult than anticipated. The symptoms of BPD are complex, diverse, and often overlap with those of other mental health conditions. For example, individuals with BPD may experience extreme mood swings similar to those observed in individuals with bipolar disorder (9); At the same time, they may also be entrenched in long-term depression, making it easy for doctors to initially misdiagnose them with depression (10). Because these symptoms overlap and interfere with each other, doctors often face the risk of misdiagnosing or overlooking the condition during initial diagnosis. Therefore, researchers are working to develop more accurate and comprehensive diagnostic tools and methods.
According to the “Neuro-behavioral Model” proposed by Lieb (1), the process of BPD formation is very complex and is determined by the interaction of several factors. The interaction between different factors can be complex and dynamic. Genetic factors and adverse childhood experiences may contribute to emotional disorders and impulsivity, leading to dysfunctional behaviors and inner conflicts. These, in turn, can reinforce emotional dysregulation and impulsivity, exacerbating the preexisting conditions. Genetic factors are an important factor in the development of BPD (11). Psychosocial factors, including adverse childhood experiences, have also been strongly associated with the development of BPD (12). Emotional instability and impulsive behavior are even more common in patients with BPD (13). The current study is based on the “Neuro-behavioral Model” and conducts a literature review of previous scientific research on BPD through bibliometric analysis to reorganize the influencing factors. Through large-sample data analysis, the association between BPD and other diseases is explored, which contributes to further refining this theory’s explanation of the common neurobiological mechanisms among various mental illnesses.
It is worth noting that with the development of BPD, some scholars have conducted bibliometrics studies on BPD to provide insights into this academic field. To date, the current study has identified two published bibliometric studies on the field: One is Ilaria M. A. Benzi and her colleagues’ 2020 metrological analysis of the literature in the field of BPD pathology for the period 1985−2020 (14). The other is a bibliometric analysis by Taylor Reis and his colleagues of the growth and development of research on personality disorders between 1980 and 2019 (15). Ilaria M. A. Benzi and her colleagues integrated and sorted out the research results of borderline personality pathology, and revealed the research results and development stages in this field through the method of network and cluster analysis. The results of the study clearly demonstrate that the United States and European countries are the main contributors, that institutional citations are more consistent, and that BPD research is well developed in psychiatry and psychology. At the same time, the development of research in borderline personality pathology is demonstrated from the initial development of the construct, through studies of treatment effects, to the results of longitudinal studies. Taylor Reis and his colleagues used a time series autoregressive moving average model to analyze publishing trends for different personality disorders to reveal their historical development patterns, and projected the number of publications for the period 2024 to 2029. The study finds a trend towards diversity in the research and development of personality disorders, with differences in publication rates for different types of personality disorders, and summarizes the reasons that influence these differences. This may ultimately determine which personality disorders will remain in future psychiatric classifications. These studies have provided valuable insights into the evolution of BPD, focusing primarily on its pathology or a broader personality disorder perspective. While basic bibliometric analyses of these studies have been conducted, there is a need for more in-depth investigations of specific trends in the evolution of BPD and a clearer delineation of emerging research foci. Therefore, in order to enhance the current study, this study extends the analysis to 2022 and utilizes a comprehensive structural variation analysis of the literature using scientometric methods. Building on previous bibliometric studies, we expect to provide new insights and additions to research in this area. At the same time, the research trends and hot topics in the field of BPD are further explored. In addition, several cocitation-based analyses are also carried out in order to better understand citation performance.
One of our goals was to understand the current status and progress of researches on BPD, and to summarize the latest developments and research findings in BPD, such as new treatment methods and disease mechanisms. Through the intuitive presentation of knowledge graphs and other images or data, we aimed to provide clinical practice and research guidance for clinicians, researchers, and policymakers.
Our second goal was to help identify future research directions and priorities, and provide more scientific and systematic research guidance for researchers. For example, by identifying hotspots and associations in certain research areas, we can determine the fields and issues that require further investigations, thus providing clearer directions and focus for researches. Additionally, through bibliometric analysis, we can provide researchers with more targeted and practical research strategies and methods, improving research efficiency and the quality of research outcomes.
The selection of appropriate methods and tools in the process of analyzing research information is crucial. Web of Science (WOS) is a popular database for bibliometric analysis that includes numerous respectable and high-impact academic journals. In addition, data information, such as references and citations, is more extensive than other academic databases (16). Data collection took place on the date of May 10, 2023. The search strategy included the following: topic=“Neuro-behavioral Model” or “borderline characteristics” or “borderline etiology” or “borderline personality disorder”, database selected=WOS Core Collection, time span=2003−2022, index=Science Citation Index Expanded (SCI-EXPENDED) and Social Sciences Citation Index (SSCI). The “Neuro-behavioral Model” serves as a theoretical framework that is useful for explaining the development and pathophysiology of BPD; “borderline characteristics” can describe the related symptoms and features of BPD; “borderline etiology” helps to understand the factors that contribute to the development of BPD; “borderline personality disorder” is the most commonly used terms in relevant research. Using these as keywords in title searches can help researchers find researches related to BPD more accurately, facilitating deeper understanding of the characteristics, pathophysiology, etiology, and other aspects of BPD. In the current study, we focused only on two types of literature: articles and review articles, and limited the language to English. After removing all literature unrelated to BPD, a total of 7919 records met the criteria. They were exported in record and reference formats, and saved in plain text file format.
Bibliometrics was first proposed by Alan Pritchard in 1969, as a method that combines data visualization to analyze publications statistically and quantitatively in specific fields and journals (17). Bibliometric analysis is a good way to analyze the trend of knowledge structure and research activities in scientific fields over time, and has been widely used in various fields since it was first used (18). Scientometrics is the application of bibliometrics in scientific fields, and it focuses on the quantitative characteristics and features of science and scientific researches (19). Compared to traditional literature review studies, visualized knowledge graphs can accurately identify key articles from many publications, comprehensively and systematically combing existing research in a field (20).
Currently, two important academic indicators are included in research. The impact factor (IF) is used as an indicator of a publication’s impact to assess the quality and importance of the publication (21). However, some researchers believe that IF has defects such as inaccuracy and misuse (22). Although many researchers have proposed to replace the impact factor with other indicators, IF is still one of the most effective ways to measure the impact of a journal (23). The IF published in the 2021 Journal Citation Reports were used. Another indicator is the H-index, which is an important measure of a scholar’s academic achievements. Some researchers consider it as a correction or supplement to the traditional IF (24).
All data were imported into CiteSpace (6.2.R4) and Scimago Graphica (1.0.30) for analysis. CiteSpace was used to obtain collaboration networks and impact networks. Scimago Graphica was used to construct a network graph of country collaboration. CiteSpace is a Java-based software developed in the context of scientometrics and data visualization (25). It combines scientific knowledge mapping with bibliometric analysis to determine the progress and current research frontiers in a particular field, as well as predict the development trends in that field (26). Scimago Graphica is a no-code tool. It can not only perform visualization analysis on communication data but also explore exploratory data (27). Currently, it is used for visual analysis of national cooperation relationships, displaying the geographic distribution of countries and publication trends.
Annual publications can provide an overview of the evolution of a research area and its progress (28). We retrieved 7919 articles from the WOS database on BPD between 2003 and 2022, including 6834 research articles and 1085 reviews (Figure 1). As of the search date, these articles had received a total of 289,958 citations, equating to an average of 14,498 citations per year. Over the past two decades, the number of research articles published on BPD has shown a fluctuating upward trend. In addition, citations to these publications have increased significantly. A polynomial curve fit of the literature on BPD clearly indicates a strong correlation between the year of publication and the number of publications (R2 = 0.973). The number of research articles on BPD has indeed fluctuated and increased over the past two decades. This observation does, to some extent, indicate an upward trend, probably due to increasing interest in BPD. However, there are other factors to consider as well. For example, the accumulation of data or technological advances, government policies and corporate investment may also affect the direction of BPD research development.
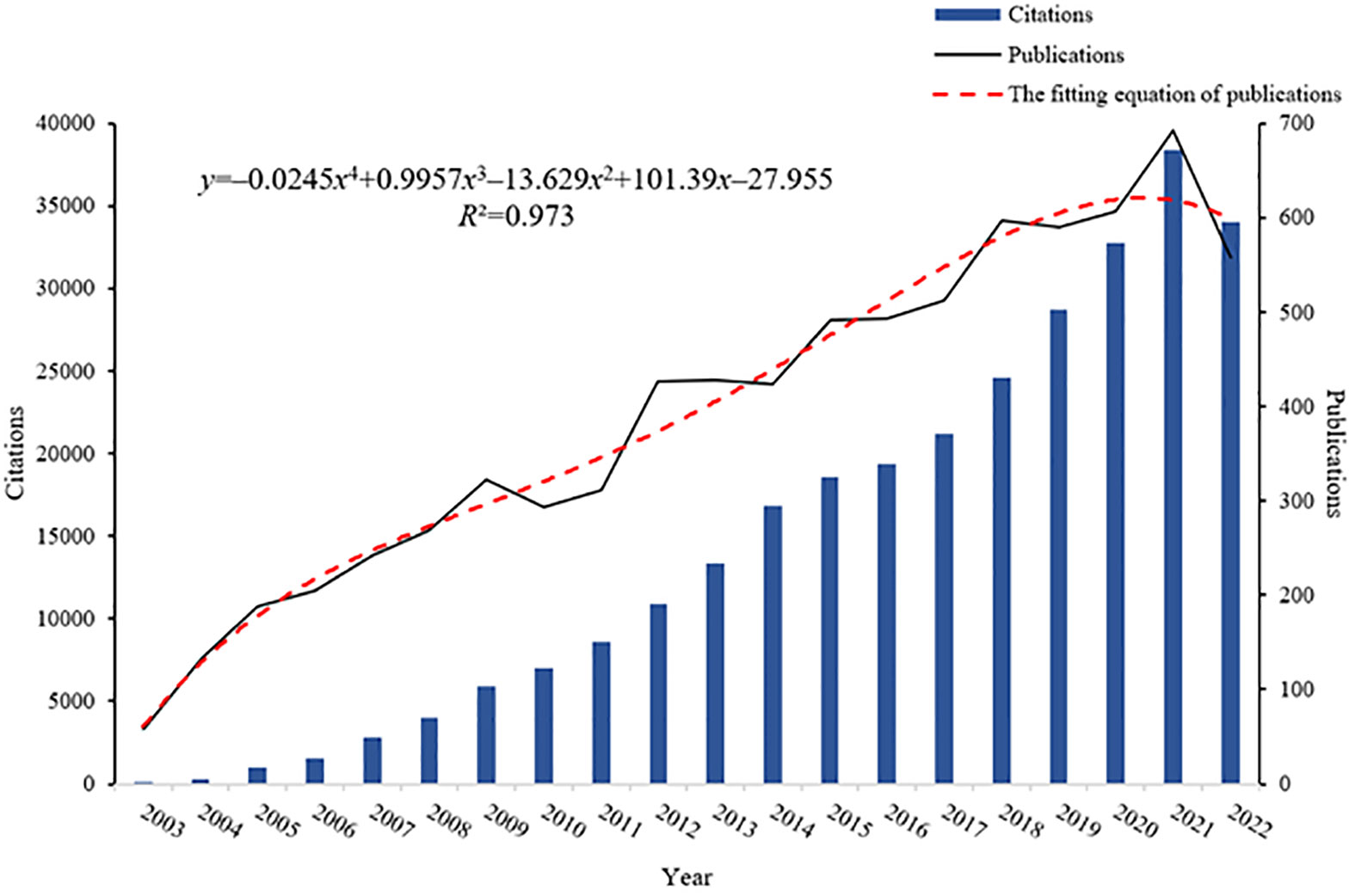
Figure 1 Annual publications, citation counts, and the fitting equation for annual publications in BPD.
Co-cited references, which are cited by multiple papers concurrently, are considered a crucial knowledge base in any given field (28). In the current study, CiteSpace clustering was utilized to identify common themes within BPD-related literature. Figure 2 presented a co-citation network of highly cited references between 2003 and 2022, comprising 1163 references. A time slice of 1 was used, with the g-index was set at k=25, which resulted in the identification of 14 clusters representing distinct research themes in BPD. The significant cluster structure is denoted by a modularity value (Q value) of 0.7974, and the high confidence level in the clusters by an average profile value (S value) of 0.9176.
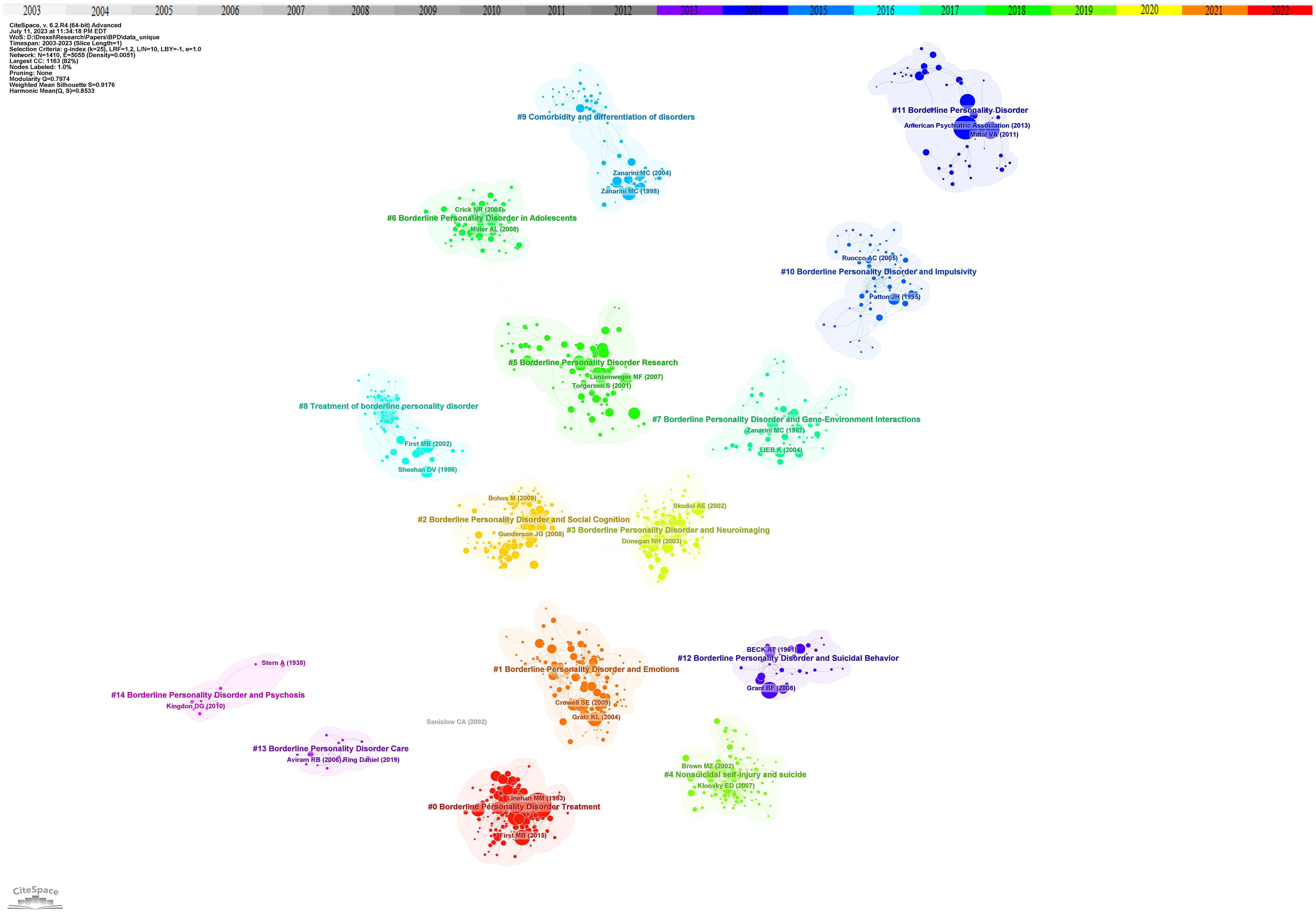
Figure 2 Reference co-citation network with cluster visualization in BPD. Trend 1 clinical researches, sub-trend clinical characteristics includes clusters #1, #2, #4, #10, #12; biological mechanisms include clusters #3, #7; nursing treatments includes clusters #0, #8, #13. Trend 2 associations and complications includes clusters #5, #6, #9, #11, #14.
Cluster analysis is performed through CiteSpace. Related clusters are classified into the same trend based on the knowledge of related fields and whether the clusters show similar trends. At the same time, based on the analysis of time series, to identify the movement of one cluster to another. Based on the cluster map of co-cited references on BPD, several different research trends were identified. The first major research trend is clinical research on BPD, which in turn consists of three sub-trends: clinical characterization of BPD, biological mechanisms, and nursing treatment. Of the data obtained, the earliest research on the clinical characterization of BPD began in 1992 with cluster #12, “borderline personality disorder and suicidal behavior” (S=0.979; 1992). Paul H. Soloff and his colleagues conducted a comparative study of suicide attempts between major depressives and patients with BPD. The aim of this study was to develop more effective intervention strategies for suicide prevention (29). This cluster was further developed in cluster #4, “nonsuicidal self-injury and suicide” (S=0.96; 2004). Thomas A. Widiger and Timothy J. Trull proposed a more flexible dimension-based categorization model to overcome the previous drawbacks of personality disorder categorization (30). Next in cluster #10 “borderline personality disorder and impulsivity” (S=0.93; 2000), Jim H. Patton and his colleagues revised the Barratt Impulsivity Scale to measure impulsivity to facilitate practical clinical research (31). Related research continues to evolve into cluster #1 “borderline personality disorder and emotions” (S=0.87; 2007) and cluster #2 “borderline personality disorder and social cognition” (S=0.911; 2009), researchers have focused on understanding the causal relationship between BPD traits and factors such as social environment, emotion regulation, and interpersonal evaluative bias, as well as their potential impact (32, 33). In the sub-trend of biological mechanisms, two main clusters are involved: cluster #7 “borderline personality disorder and gene-environment interactions” (S=0.871; 2002) and cluster #3 “borderline personality disorder and neuroimaging” (S=0.938; 2007). In the related cluster, researchers have found a relationship between BPD and genetic and environmental factors (34). Researchers have also utilized various external techniques to explore the degree of correlation between the risk of developing BPD and its biological mechanisms, aiming to reveal the complex mechanisms that influence the emergence and development of BPD (35). In nursing treatment, cluster #8 “treatment of borderline personality disorder “ (S=0.968; 2001), Silvio Bellino and his colleagues systematically analyzed the current publications on BPD pharmacotherapy research and summarized relevant clinical trials and findings (36). However, due to the complexity of BPD, there is still a lack of information on the exact efficacy of pharmacotherapy in BPD, and therefore pharmacotherapy remains an area of ongoing development and research. This trend continues to be developed in cluster #0 “borderline personality disorder treatment” (S=0.887; 2006), which emphasizes the development of novel pharmacotherapies for BPD. Cluster #13 “borderline personality disorder care” (S=0.997; 2013) mainly focuses on the comprehensive care of people with borderline personality disorder and the education of patients and families. The goal is to improve patients’ quality of life, reduce self-injury and suicidal behavior, and promote full recovery.
The second major research trend is association and comorbidity. This trend first began in cluster #9 “comorbidity and differentiation of disorders” (S=0.946; 1999). Mary C Zanarini and his colleagues explored the comorbidity of BPD with other psychiatric disorders on Axis I (37). Cluster #14 “borderline personality disorder and psychosis” (S=0.966; 2003) also explored symptoms associated with BPD (38). This trend continues, with researchers studying BPD research in cluster #11 “borderline personality disorder” (S=0.935; 2004) and cluster #5 “borderline personality disorder research” (S=0.881; 2007) (39, 40). In addition, cluster #6 “borderline personality disorder in adolescents” (S=0.894; 2011) points out that the focus of BPD research is increasingly shifting towards adolescents (41).
Figure 3 showed the time span and research process of the developmental evolution of these different research themes. The temporal view reveals the newest and most active clusters, namely #0 “dialectical behavior therapy”, #1 “daily life”, and #2 “social cognition”, which have been consistently researched for almost a decade. Cluster #0 “dialectical behavior therapy” has the largest number and the longest duration, lasting almost 10 years. Similarly, this article by Rebekah Bradley and Drew Westen on understanding the psychodynamic mechanisms of BPD from the perspective of developmental psychopathology has the largest node (34).
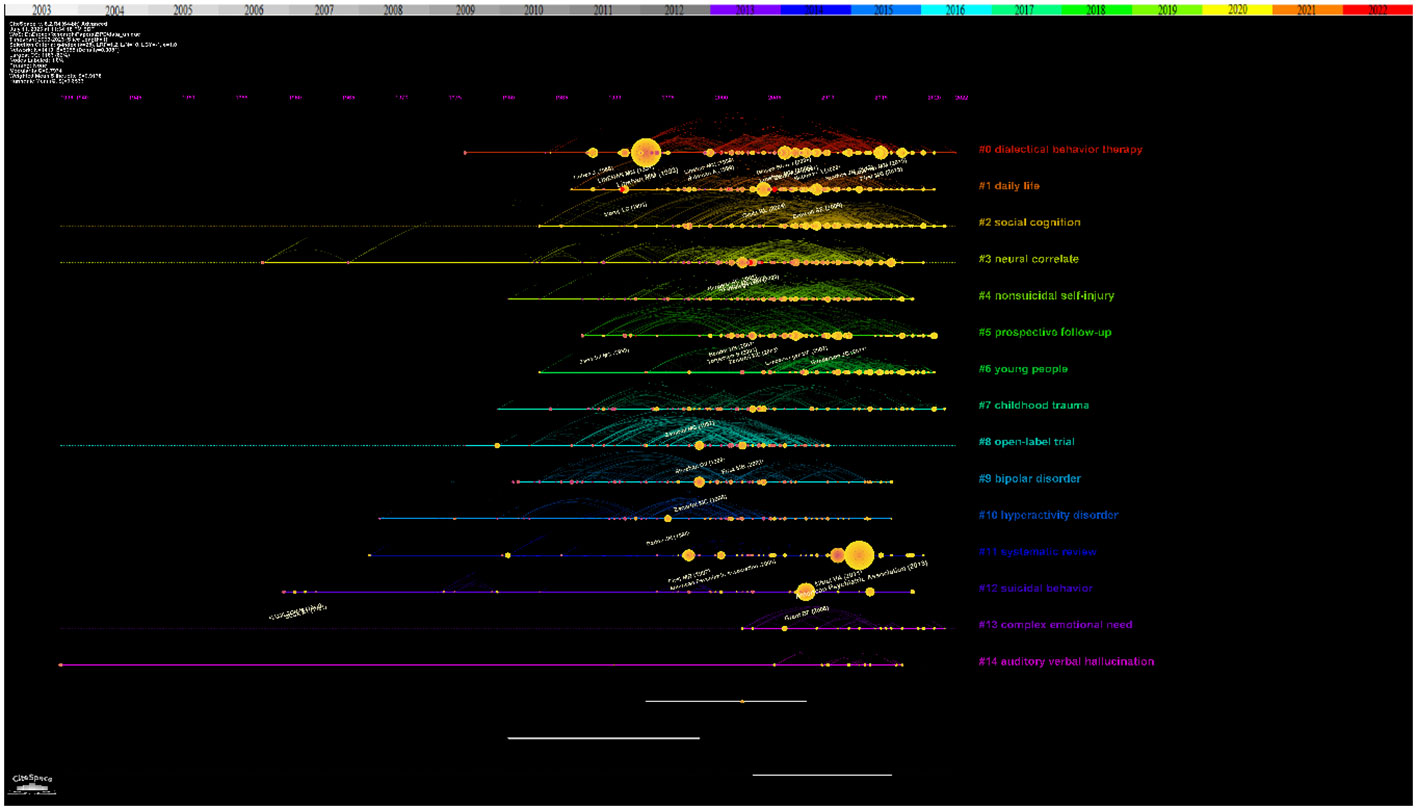
Figure 3 Reference co-citation network with timeline visualization in BPD.
The top 10 highly cited papers on BPD research were presented in Table 1. The most cited paper, by Marsha M. Linehan and colleagues, focus on the treatment of suicidal behavior in BPD (42). The transition between suicidal and non-suicidal self-injurious behavior in individuals with BPD has attracted researchers’s attention, mainly in cluster #4 “nonsuicidal self-injury and suicide” (52). The second is the experimental study by Josephine Giesen-Bloo and his colleagues on the psychotherapy of BPD (43). In cluster #0 “borderline personality disorder treatment” and Cluster #8 “treatment of borderline personality disorder”, researchers strive to find non-pharmacological approaches with comparable or enhanced therapeutic effects. This was followed by Sheila E. Crowell and her colleagues’ study of the biological developmental patterns of BPD (44). Research on the biological mechanisms and other contributing factors of BPD, including #7 “borderline personality disorder and gene-environment interactions” have been closely associated with the development of BPD (53).
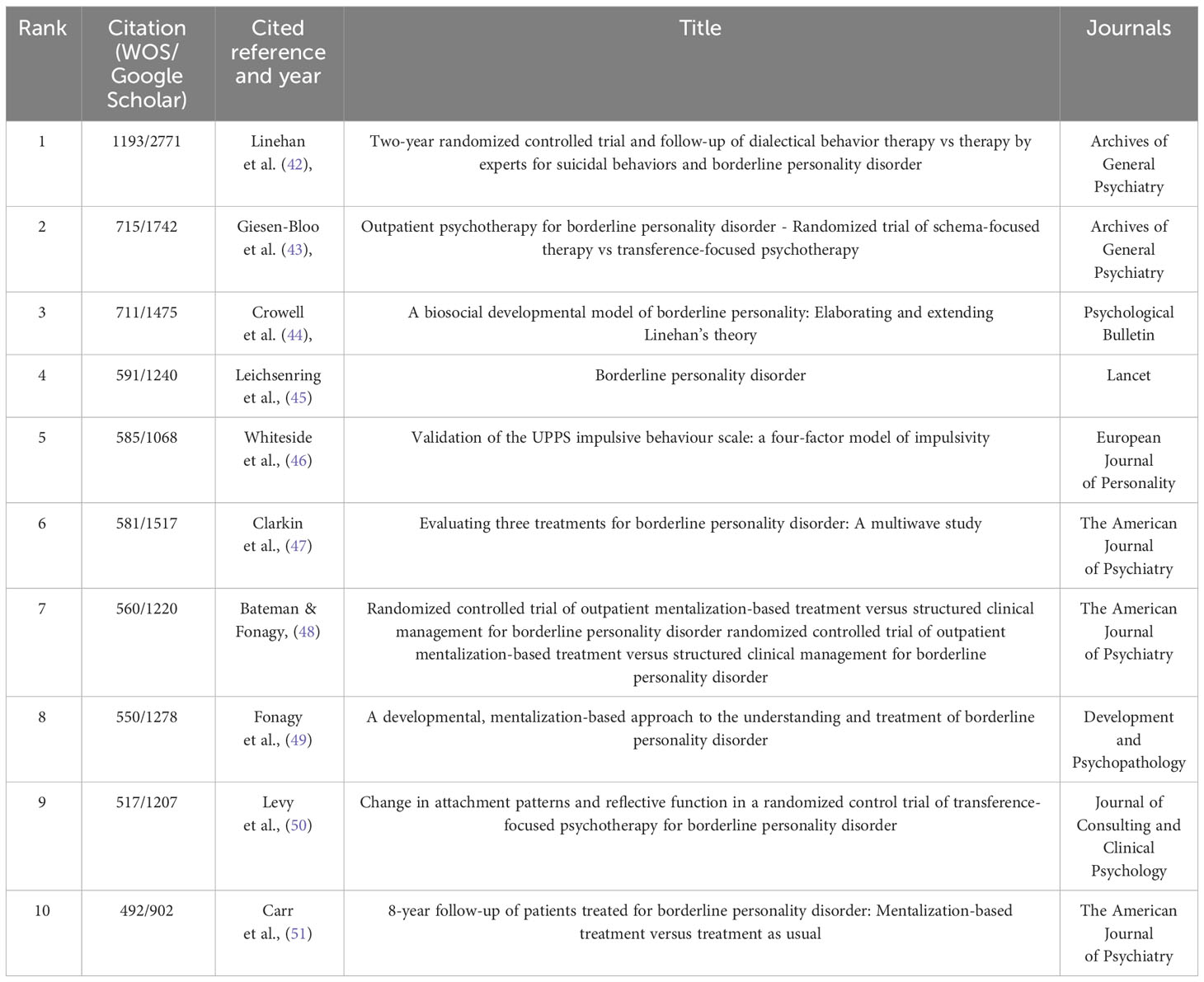
Table 1 Top 10 cited references that published BPD researches.
The “citation explosion” reflects the changing research focus of a field over time and indicates that certain literature has been frequently cited over time. Figure 4 showed the top 9 references with the highest citation intensity. The three papers with the greatest intensity of outbursts during the period 2003−2022 are: The first is the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (54). In the second article, Vijay A. Mittal and Elaine F. Walker discuss key issues surrounding dyspraxia, tics, and psychosis that are likely to appear in an upcoming edition of the Diagnostic and Statistical Manual of Mental Disorders (39). In addition, Ioana A. Cristea and colleagues conducted a systematic review and meta-analysis to evaluate the effectiveness of psychotherapy for borderline personality disorder (55).
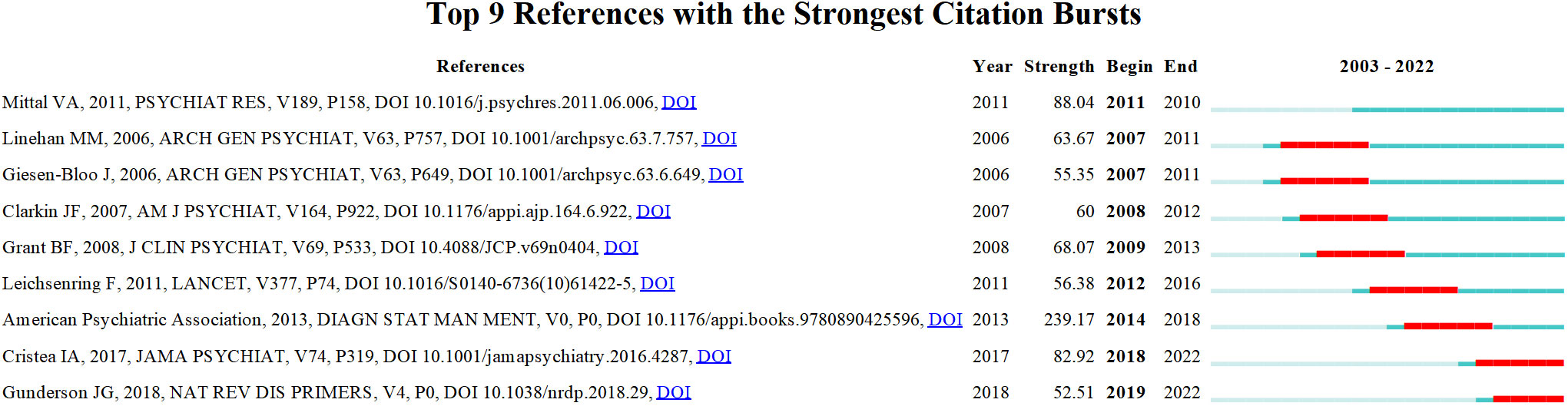
Figure 4 References with the strongest occurrence burst on BPD researches. Article titles correspond from top to bottom: Mittal VA et al. Diagnostic and Statistical Manuel of Mental Disorders; Linehan MM et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder; Giesen-Bloo J et al. Outpatient psychotherapy for borderline personality disorder: Randomized trial of schema-focused therapy vs transference-focused psychotherapy; Clarkin Jf et al. Evaluating three treatments for borderline personality disorder: A multiwave study; Grant BF et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: Results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions; Leichsenring F et al. Borderline personality disorder; American Psychiatric Association, DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.); Cristea IA et al. Efficacy of psychotherapies for borderline personality disorder: A systematic review and meta-analysis; Gunderson JG et al. Borderline personality disorder.
Structural variation analysis can be understood as a method of measuring and studying structural changes in the field, mainly reflecting the betweenness centrality and sigma of the references. The high centrality of the reference plays an important role in the connection between the preceding and following references and may help to identify critical points of transformation, or intellectual turning points. Sigma values, on the other hand, are used to measure the novelty of a study, combining a combination of citation burst and structural centrality (56). Table 2 listed the top 10 structural change references that can be considered as landmark studies connecting different clusters. The top three articles with high centrality are the studies conducted by Milton Z. Brown and his colleagues on the reasons for suicide attempts and non-suicidal self-injury in BPD women (57); the research by Nelson H. Donegan and his colleagues on the impact of amygdala on emotional dysregulation in BPD patients (59); and the fMRI study by Sabine C. Herpertz and her colleagues on abnormal amygdala function in BPD patients (61). In addition, publications with high sigma values are listed. They are Larry J. Siever and Kenneth L. Davis on psychobiological perspectives on personality disorders (58); Ludger Tebartz van Elst and his colleagues on abnormalities in frontolimbic brain functioning (60); and Marsha M. Linehan on therapeutic approaches in BPD research (62). These works are recognized as having transformative potential and may generate some new ideas.
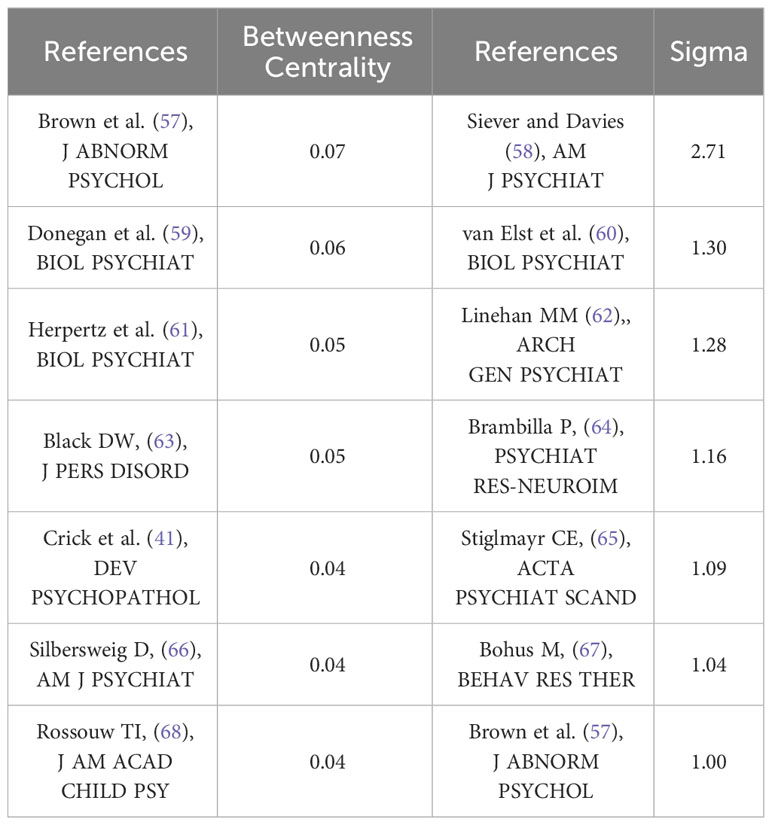
Table 2 Top 7 betweenness centrality and stigma references.
Figure 5 showed a map of the co-authorship network over the last two decades. In total, 10 different clusters are shown, each of which gathers co-authors around the same research topic. For example, the main co-authors of cluster #0 “remission” are Christian Schmahl, Martin Bohus, Sabine C. Herpertz, Timothy J. Trull and Stefan Roepke. More recently, the three authors with the greatest bursts of research have been Mary C. Zanarini, Erik Simonsen, and Carla Sharp. As shown in Table 3, the three most published authors are Martin Bohus (145 publications; 1.83%; H-index=61), Mary C. Zanarini (144 publications; 1.82%; H-index=80) and Christian Schmahl (142 publications; 1.79%; H-index=54).
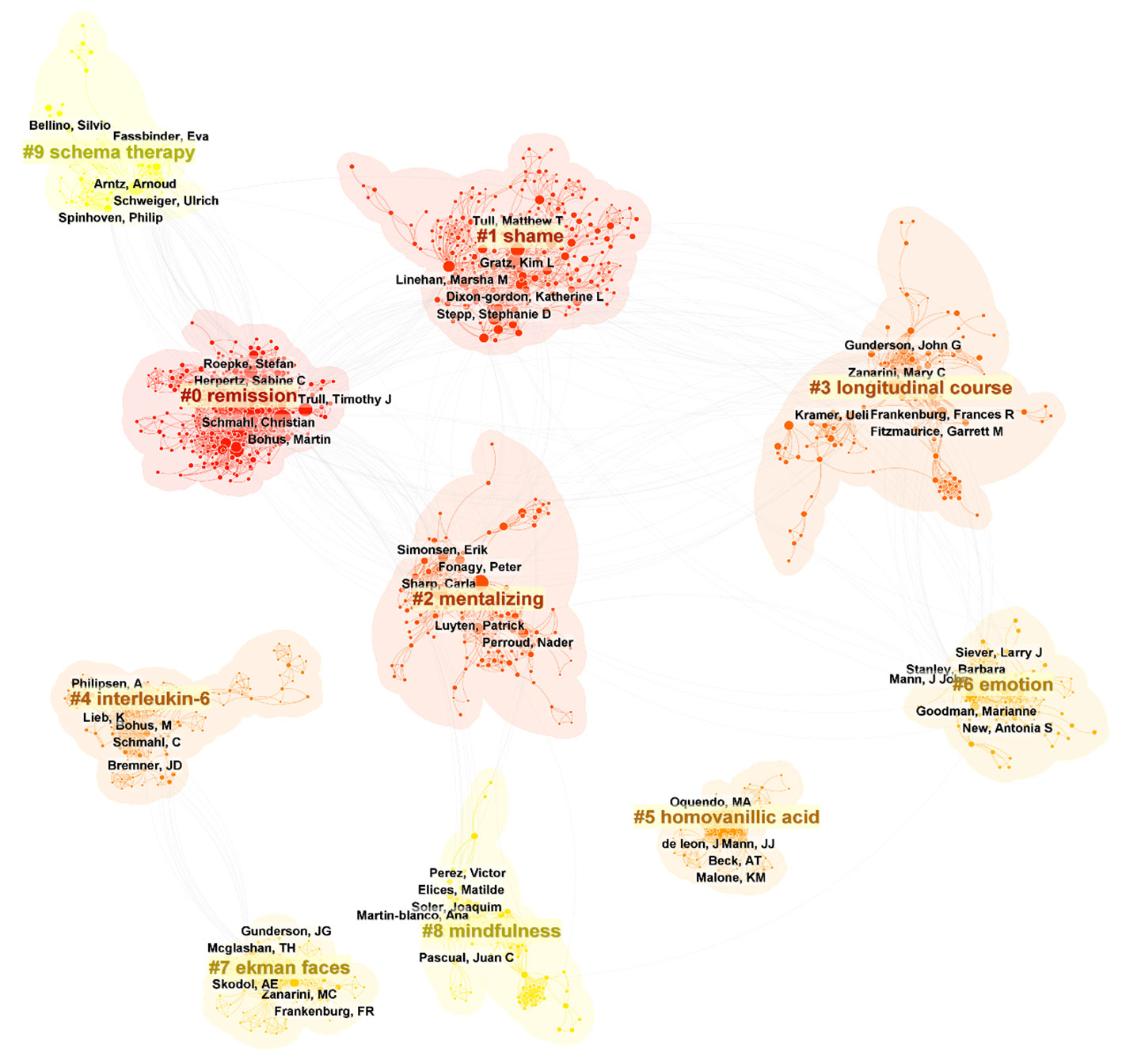
Figure 5 Top 10 clusters of coauthors in BPD (2003–2023). Selection Criteria: Top 10 per slice. Clusters labeled by keywords. The five authors with the highest number of publications in each cluster were labeled.
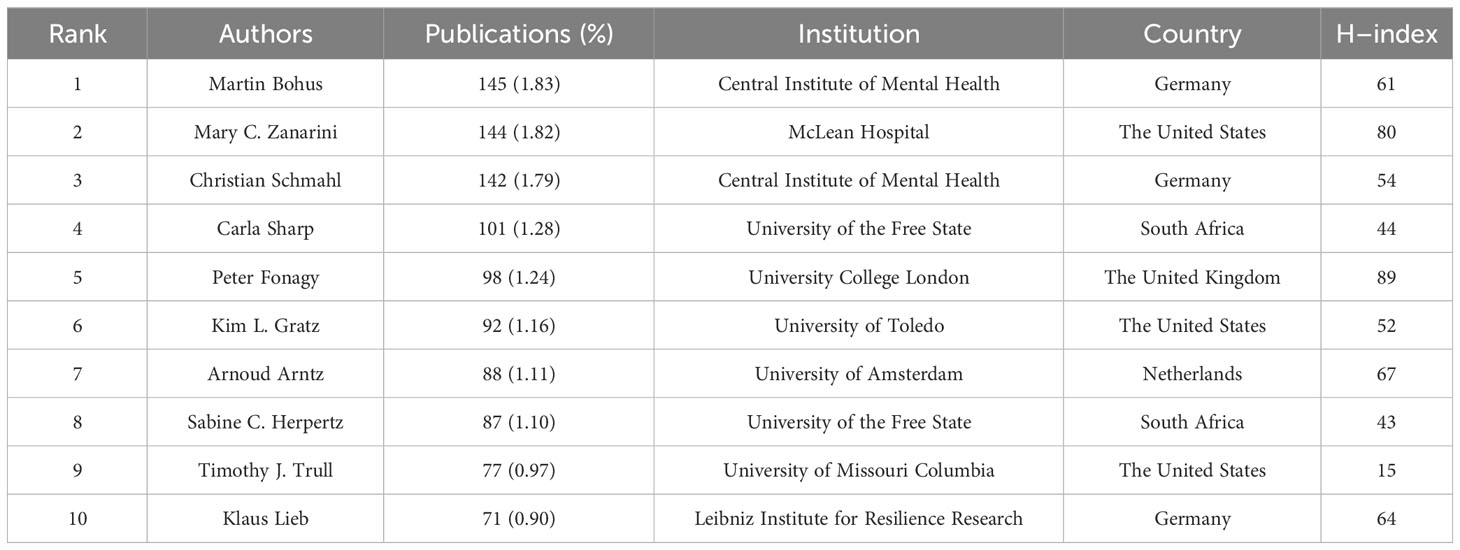
Table 3 Top 10 authors that published BPD researches.
The top 10 countries in terms of number of publications in the BPD are added in Table 4. With 3,440 published papers, or nearly 43% of all BPD research papers, the United States is the leading contributor to BPD research. This is followed by Germany (1196 publications; 15.10%) and the United Kingdom (1020 publications; 9.32%). Centrality refers to the degree of importance or centrality of a node in a network and is a measure of the importance of a node in a network (69). In Table 4 the United States is also has the highest centrality (0.43). Figure 6 shows the geographic collaboration network of countries in this field, with 83 countries contributing to BPD research, primarily from the United States and Europe.
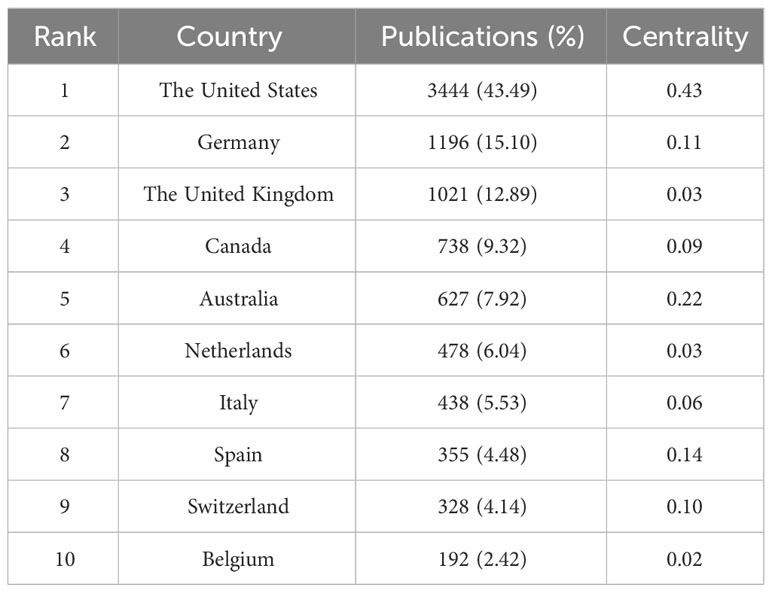
Table 4 Top 10 countries that published BPD researches.
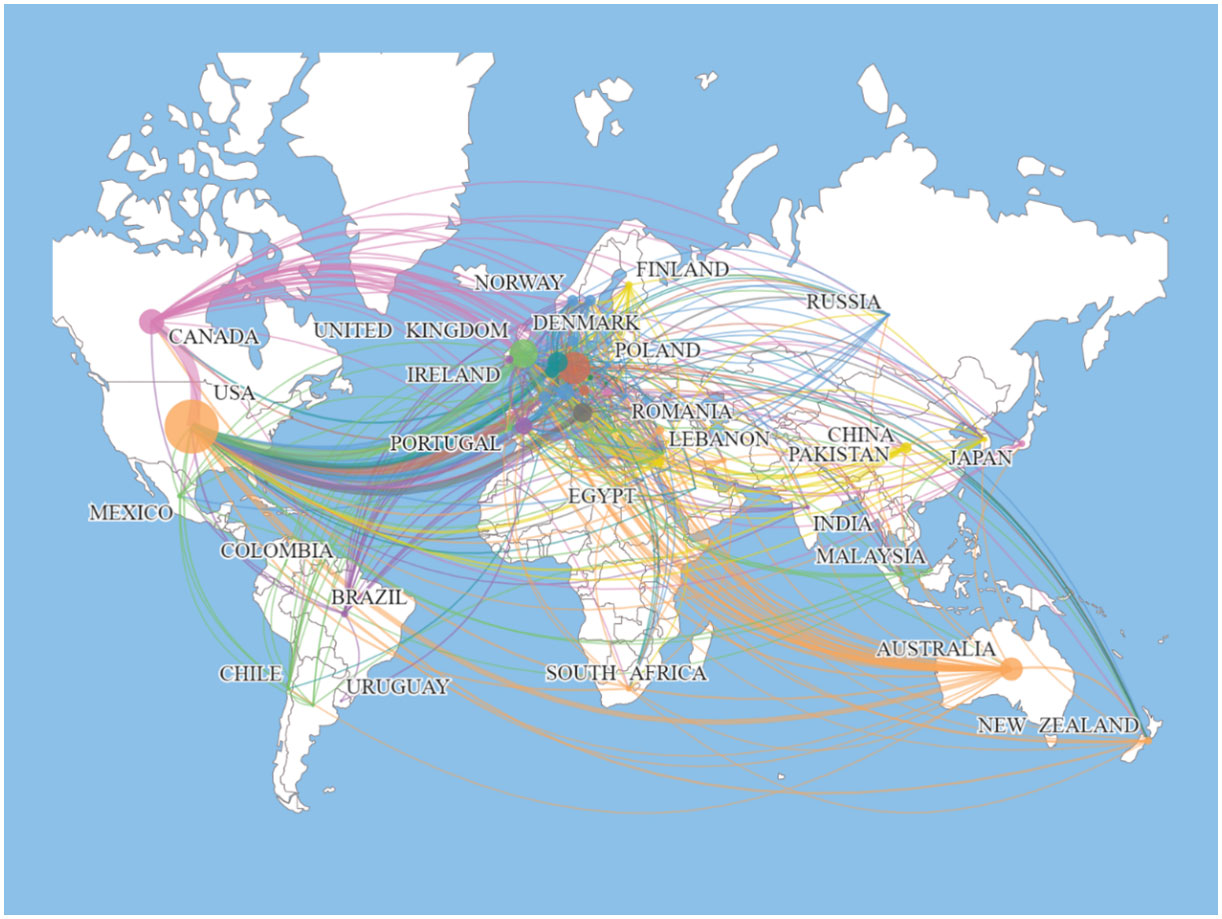
Figure 6 Map of the distribution of countries/regions engaged in BPD researches.
Table 5 listed the top 10 institutions ranked by the number of publications. The current study shows that Research Libraries Uk is the institution with the highest number of publications, with 766 publications (9.67%). The subsequent institutions are Harvard University and Ruprecht Karls University Heidelberg with 425 (5.37%) and 389 (4.91%) publications respectively. As can be seen from Table 4, six of the top 10 institutions in terms of number of publications are from the United States. In part, this reflects the fact that the United States institutions are at the forefront of the BPD field and play a key role in it.
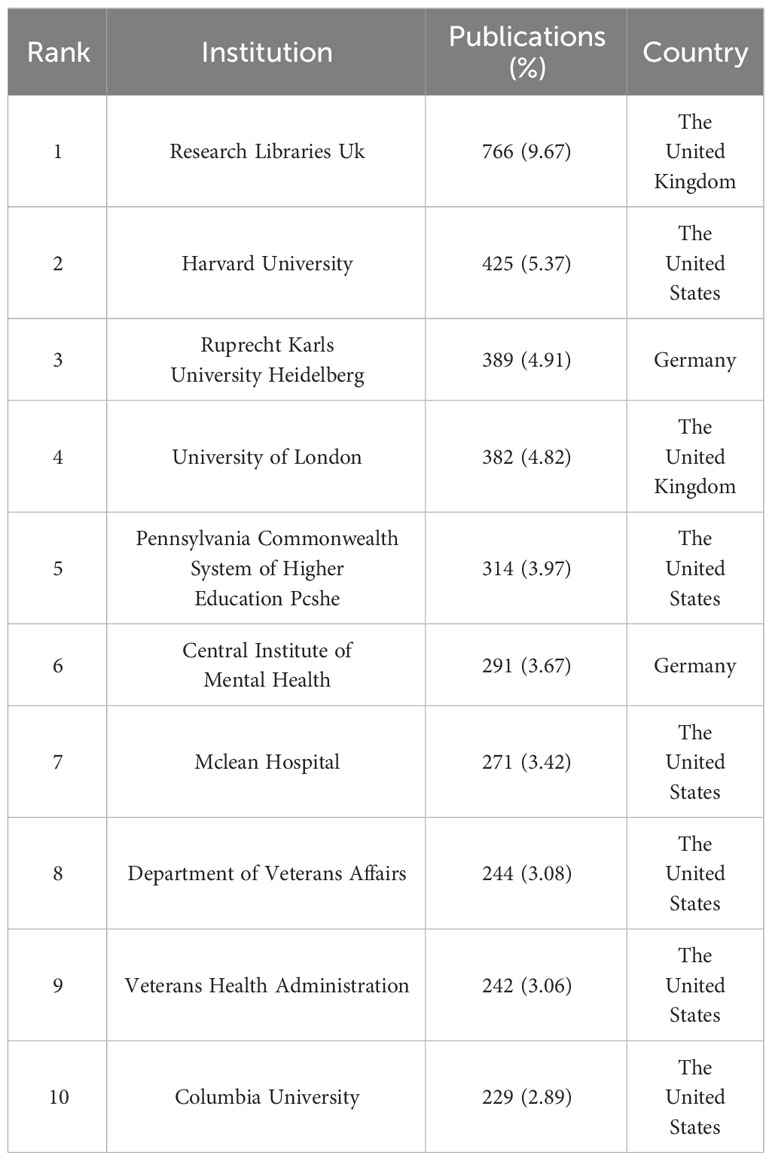
Table 5 Top 10 institutions that published BPD researches.
If the more papers are published in a particular journal and at the same time it has a high number of citations, then it can be considered that the journal is influential (70). The top 10 journals in the field of BPD in terms of number of publications are listed in Table 6. Journal of Personality Disorders from the Netherlands published the most literature on BPD with 438 (5.53%; IF=3.367) publications. This was followed by two journals from the United States: Psychiatry Research and Personality Disorders Theory Research and Treatment, with 269 (3.40%, IF=11.225) and 232 (2.93%; IF=4.627) publications, respectively. Among the top 10 journals in terms of number of publications published, Psychiatry Research has the highest impact factor.
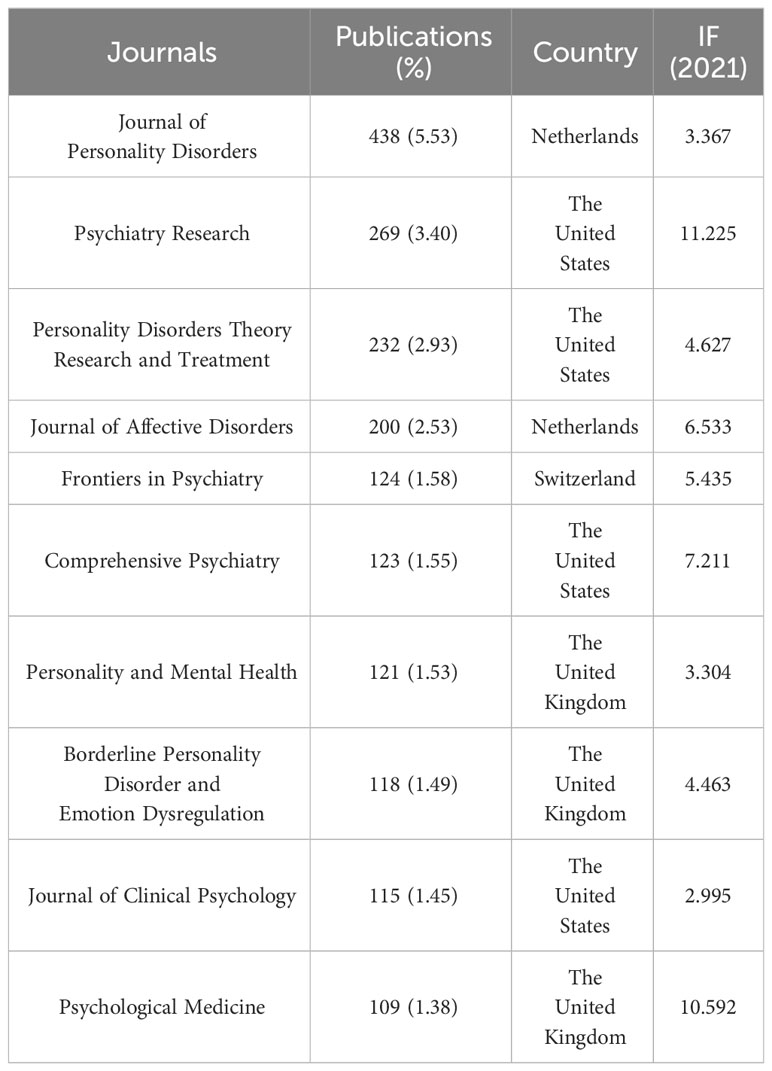
Table 6 Top 10 journals that published BPD researches.
Keyword co-occurrence analysis can help researchers to understand the research hotspots in a certain field and the connection between different research topics. As shown in Figure 7, all keywords can be categorized into 9 clusters: cluster #0 “diagnostic interview”, cluster #1 “diagnostic behavior therapy”, cluster #3 “social cognition”, cluster #4 “emotional regulation”, cluster #5 “substance use disorders “, cluster #6 “posttraumatic stress disorder”, cluster #7 “suicide” and cluster #8 “double blind”. These keywords have all been important themes in BPD research during the last 20 years.
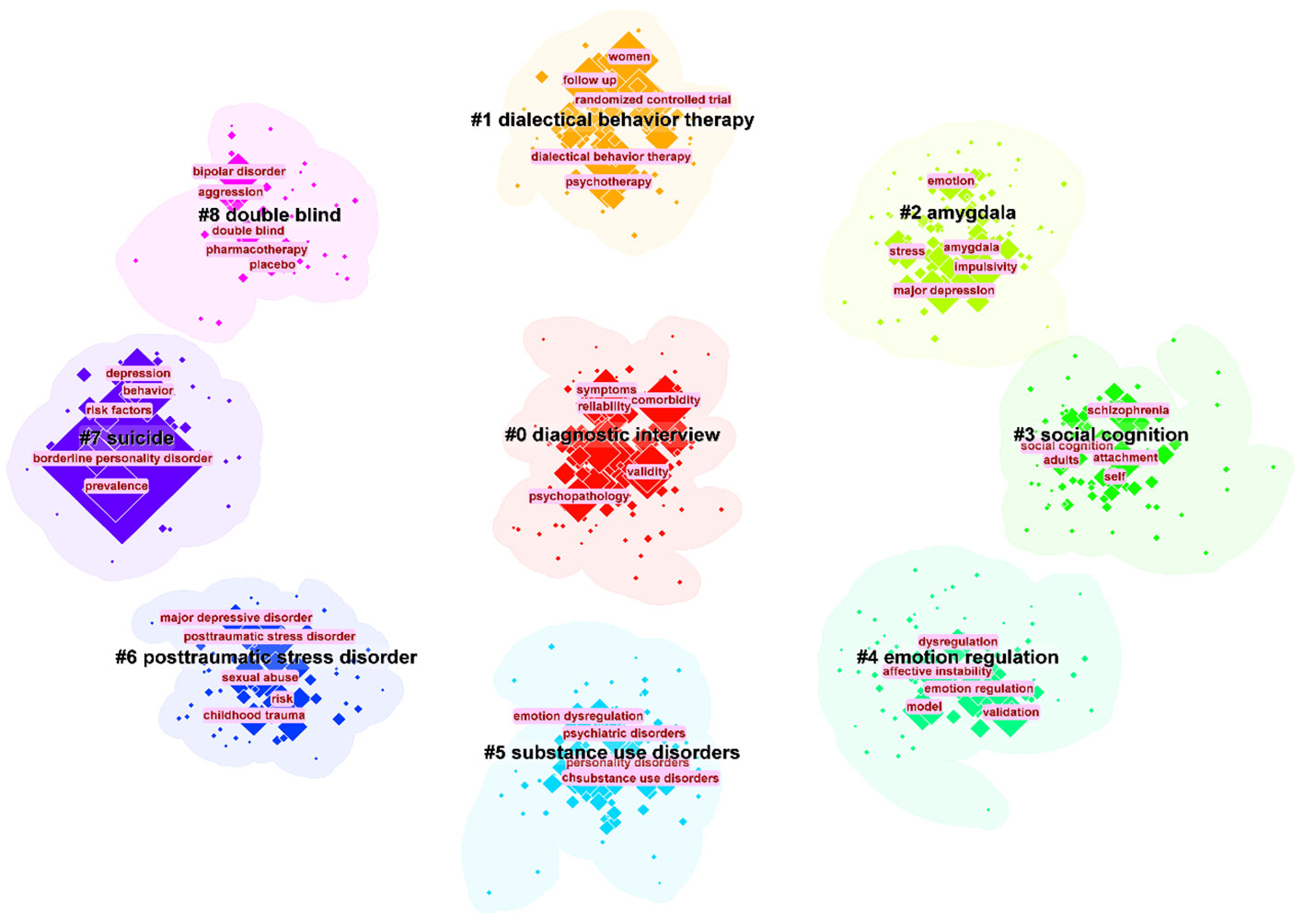
Figure 7 The largest 9 clusters of co-occurring keywords. The top 5 most frequent keywords in each cluster are highlighted.
Keyword burst is used to identify keywords with a significant increase in the frequency of occurrence in a topic or domain, helping to identify emerging concepts, research hotspots or keyword evolutions in a specific domain (71). Figure 8 presented the top 32 keywords with the strongest citation bursts in BPD from 2003−2023. Significantly, the keywords “positron emission tomography” (29.63), “major depression” (27.93), and “partial hospitalization” (27.1) had the highest intensity of outbreaks.
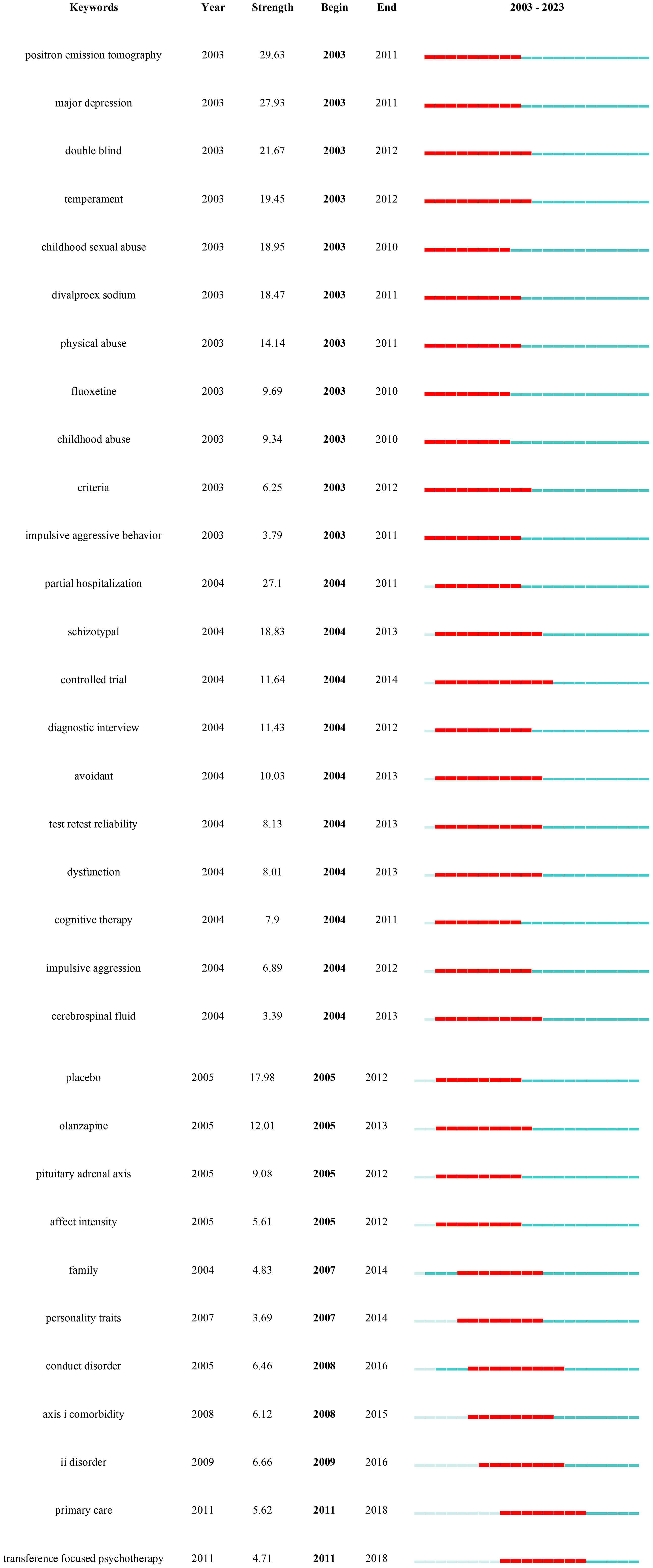
Figure 8 Keywords with the strongest occurrence burst on BPD researches.
In this study, we chose specific search terms, particularly “Neuro-behavioral Model”, to efficiently collect and analyze BPD research literature related to this emerging framework. This choice of keyword helped narrow the research scope and ensure its relevance to our objectives. However, it may have excluded some studies using different terminology, thus limiting comprehensiveness. In addition, the ‘Neuro-behavioral Model’, as an interdisciplinary field, encompasses a wide range of connotations and extensions, which also poses challenges to our research. This undoubtedly adds to the complexity of the study, yet it enhances our understanding of the field’s diversity.
This current study utilized CiteSpace and Scimago Graphic software to conduct a comprehensive bibliometric analysis of the research literature on BPD. The study presented the current status of research, research hotspots, and research frontiers in BPD over the past 20 years (2003–2022) through knowledge mapping. The scientific predictions of future trends in BPD provided by this study can guide researchers interested in this field. This study also uses bibliometrics analysis method to show the knowledge structure and research results in the field of BPD, as well as the scientific prediction of the future trend of BPD research.
Previous studies have indicated an increasing trend in the number of papers focused on BPD, with the field gradually expanding into various areas. The first major research trend involves clinical studies on BPD. This includes focusing on emotional recognition difficulties in BPD patients, as well as studying features related to suicide attempts and non-suicidal self-injury. Clinical recognition and confirmation of BPD remains low, mainly related to the lack of clarity of its biological mechanisms (72). The nursing environment for BPD patients plays an important role in the development of the condition, which has become a focus of research. Researchers are also exploring the expansion of treatment options from conventional medication to non-pharmacological approaches, particularly cognitive-behavioral therapy. Another major research trend involves the associations and complications of BPD, including a greater focus on the adolescent population to reduce the occurrence of BPD starting from adolescence. Additionally, many researchers are interested in the comorbidity of BPD with various clinical mental disorders.
Based on the results of the above studies and the results of the research trends in the table of details of the co-citation network clusters in 2022 (Table 7), several predictions are made for the future trends in the field of BPD. In Table 7, there were some trends related to previous studies, including #1”dialectical behavior therapy”, #7 “dialectical behavior therapy” (73), #5 “mentalization” (74), and #9 “non-suicidal self-injury” (75). The persistence of these research trends is evidence that they have been a complex issue in this field and a focus of researchers. The recently emerged turning point paper provides a comprehensive assessment about BPD, offering practical information and treatment recommendations (76). New research is needed to improve standards and suggest more targeted and cost-effective treatments.
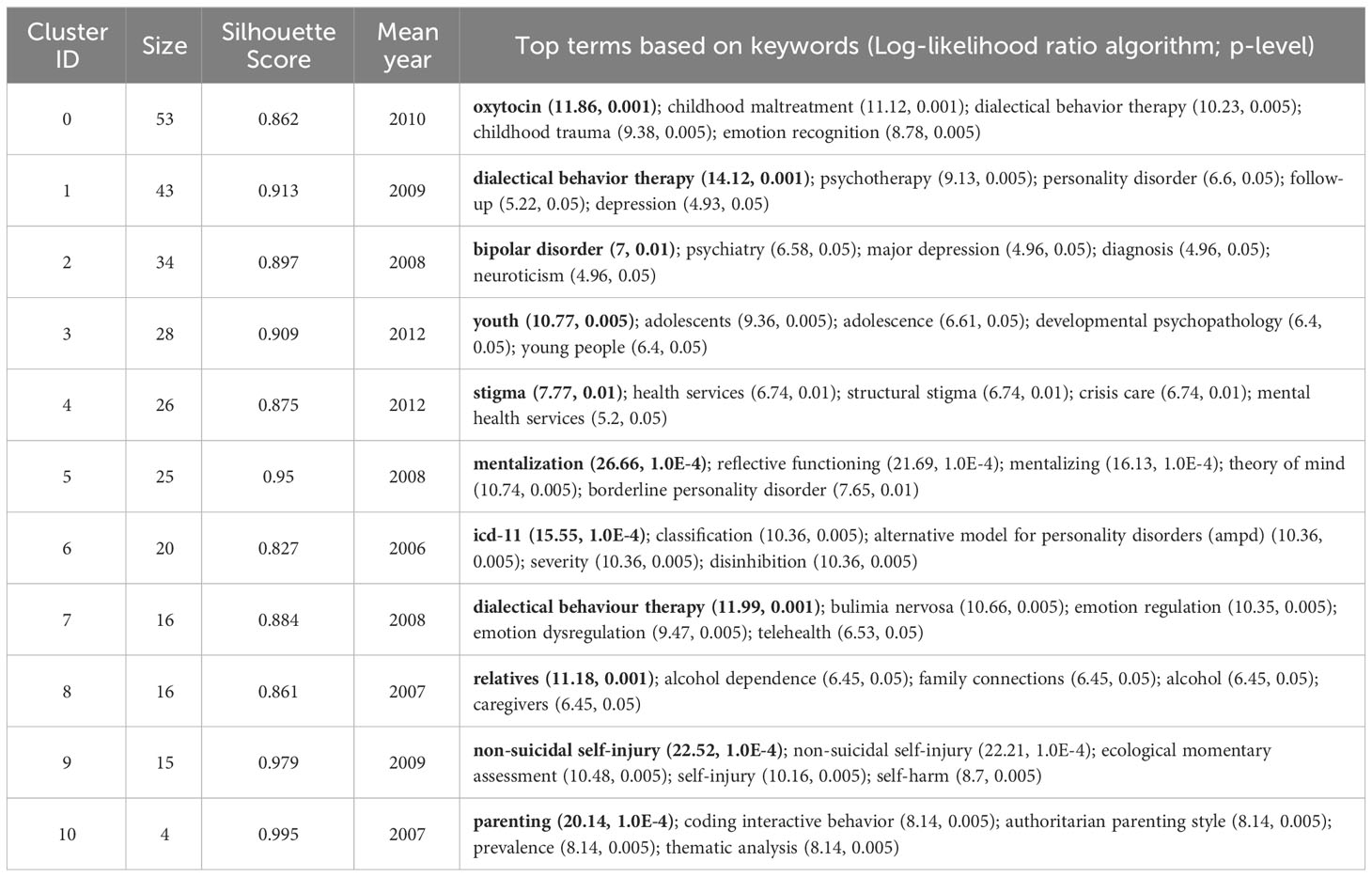
Table 7 The references co-citation network cluster detail (2022).
BPD symptoms in adolescents have been shown to respond to interventions with good results, so prevention and intervention for BPD is warranted (77). This trend can be observed in #3 “youth” (78). Mark F. Lenzenweger and Dante Cicchetti summarized the developmental psychopathology approach to BPD, one of the aims of which is to provide information for the prevention of BPD (79). Prevention and early intervention of BPD has been shown to provide many benefits, including reduced occurrence of secondary disorders, improved psychosocial functioning, and reduced risk of interpersonal conflict (80). However, there are differences between individuals, and different prevention goals are recommended for adolescents at risk for BPD. Therefore, prevention and early intervention for BPD has good prospects for the future.
The etiology of BPD is closely related to many factors, and its pathogenesis is often ignored by clinicians. The exploration of risk factors has been an important research direction in the study. Some studies have found that BPD is largely the product of traumatic childhood experiences, which may lead to negative psychological effects on children growing up (81). It has also been found that the severity of borderline symptoms in parents is positively associated with poor parenting practices (82). Future researches need to know more about the biological-behavioral processes of parents in order to provide targeted parenting support and create a good childhood environment.
Because pharmacotherapy is only indicated for comorbid conditions that require medication, psychotherapy has become one of the main approaches to treating BPD. The increasingly advanced performance and availability of contemporary mobile devices can help to take advantage of them more effectively in the context of optimizing the treatment of psychiatric disorders. The explosion of COVID-19 is forcing people to adapt to online rather than face-to-face offline treatment (83). The development of this new technology will effectively advance the treatment of patients with BPD. Although telemedicine has gained some level of acceptance by the general public, there are some challenges that have been reported, so further research on the broader utility of telemedicine is needed in the future.
As mentioned earlier, there have been previous bibliometric studies conducted by scholars in the field of BPD. This paper focuses more on BPD in personality disorders than the extensive study of personality disorders as a category by Taylor Reis et al. (15). The results of both studies show an increasing trend in the number of publications in the field of BPD, suggesting positive developments in the field. Taylor Reis et al. focused primarily on quantifying publications on personality disorders and did not delve into other specific aspects of BPD. Ilaria M.A. Benzi et al. focused on a bibliometric analysis of the pathology of BPD (14). They give three trends for the future development of BPD pathology: first, the growing importance of self-injurious behavior research; second, the association of attention deficit hyperactivity disorder with BPD and the influence of genetics and heritability on BPD; and third, the new focus on the overlap between fragile narcissism and BPD. The study in this paper also concludes that there are three future development directions for BPD: first, the prevention and early intervention of BPD; second, the non-pharmacological treatment of BPD; and third, research into the pathogenesis of BPD. Owing to variations in research backgrounds and data sources, the outcomes presented in the two studies diverge significantly. Nevertheless, both contributions hold merit in advancing the understanding of BPD. In addition to this, this paper also identifies trends in BPD over the past 20 years: the first trend is the clinical research of BPD, which is specifically subdivided into three sub-trends; the second trend is association and comorbidity. The identification of these trends is important for understanding the disorder, improving diagnosis and treatment, etc. Structural variant analysis also features prominently in the study. The impact of literature in terms of innovativeness is detected through in-depth mining and analysis of large amounts of literature data. This analysis is based on research in the area of scientific creativity, especially the role and impact of novel reorganizations in creative thinking. Structural variation analysis is precisely designed to find and reveal embodiments of such innovative thinking in scientific literature, enabling researchers to more intuitively grasp the dynamics and cutting-edge advances in the field of science.
However, it must be admitted that our study has some limitations. The first is the limited nature of data resources. The data source for our study came from only one database, WOS. Second, the limitation of article type. Search criteria are limited to papers and reviews in SCI and SSCI databases. Third, the effect of language type. In the current study, only English-language literature could be included in the analysis, which may lead us to miss some important studies published in other languages. Fourth, limitations of research software. Although this study used well-established and specialized software, the results obtained by choosing different calculation methods may vary. Finally, the diversity of results interpretation. The results analyzed by the software are objective, but there is also some subjectivity in the interpretation and analysis of the research results. While we endeavor to be comprehensive and accurate in our research, the choice of search terms inevitably introduces certain limitations. Using “Neuro-behavioral Model” as the search term enhances the study’s relevance, but it may also cause us to miss significant studies in related areas. This limits the generalizability and replicability of our results. Furthermore, the inherent complexity and diversity of neurobehavioral models might introduce subjectivity and bias in our interpretation and application of the literature. Although we endeavored to reduce bias via multi-channel validation and cross-referencing, we cannot entirely eliminate its potential impact on our findings.
Overall, a comprehensive scientometrics analysis of BPD provides a comprehensive picture of the development of this field over the past 20 years. This in-depth examination not only reveals research trends, but also allows us to understand which areas are currently hot and points the way for future research efforts. In addition, this method provides us with a framework to evaluate the value of our own research results, which helps us to more precisely adjust the direction and strategy of research. More importantly, this in-depth analysis reveals the depth and breadth of BPD research, which undoubtedly provides valuable references for researchers to have a deeper understanding of BPD, and also provides a reference for us to set future research goals. In short, this scientometrics approach gives us a window into the full scope of BPD research and provides valuable guidance for future research.
YL: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. CC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. YZ: Validation, Visualization, Writing – review & editing. NZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. SL is supported by the Outstanding Youth Program of Philosophy and Social Sciences in Anhui Province (2022AH030089) and the Starting Fund for Scientific Research of High-Level Talents at Anhui Agricultural University (rc432206).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lieb K, Zanarini MC, Schmahl C, Linehan MM, Bohus M. Borderline personality disorder. Lancet (2004) 364:453–61. doi: 10.1016/S0140-6736(04)16770-6
2. Chugani CD, Byrd AL, Pedersen SL, Chung T, Hipwell AE, Stepp SD. Affective and sensation-seeking pathways linking borderline personality disorder symptoms and alcohol-related problems in young women. J Pers Disord. (2020) 34:420–31. doi: 10.1521/pedi_2018_32_389
3. Bagge CL, Stepp SD, Trull TJ. Borderline personality disorder features and utilization of treatment over two years. J Pers Disord. (2005) 19:420–39. doi: 10.1521/pedi.2005.19.4.420
4. Paris J. Suicidality in borderline personality disorder. Medicina. (2019) 55:223. doi: 10.3390/medicina55060223
5. Lenzenweger MF, Lane MC, Loranger AW, Kessler RC. DSM-IV personality disorders in the National Comorbidity Survey Replication. Biol Psychiatry. (2007) 62:553–64. doi: 10.1016/j.biopsych.2006.09.019
6. Skodol AE, Gunderson JG, Pfohl B, Widiger TA, Livesley WJ, Siever LJ. The borderline diagnosis I: Psychopathology, comorbidity, and personality structure. Biol Psychiatry. (2002) 51:936–50. doi: 10.1016/s0006-3223(02)01324-0
7. Bailey RC, Grenyer BF. Burden and support needs of carers of persons with borderline personality disorder: A systematic review. Harvard Rev Psychiatry. (2013) 21:248–58. doi: 10.1097/HRP.0b013e3182a75c2c
8. Weimand BM, Hedelin B, Sällström C, Hall-Lord M-L. Burden and health in relatives of persons with severe mental illness: A Norwegian cross-sectional study. Issues Ment Health Nursing. (2010) 31:804–15. doi: 10.3109/01612840.2010.520819
9. Saccaro LF, Schilliger Z, Dayer A, Perroud N, Piguet C. Inflammation, anxiety, and stress in bipolar disorder and borderline personality disorder: A narrative review. Neurosci Biobehav Rev. (2021) 127:184−192. doi: 10.1016/j.neubiorev.2021.04.017
10. Dixon-Gordon KL, Laws H. Emotional variability and inertia in daily life: Links to borderline personality and depressive symptoms. J Pers Disord. (2021) 35:162−171. doi: 10.1521/pedi_2021_35_504
11. Torgersen S. Genetics of patients with borderline personality disorder. Psychiatr Clinics North A. (2000) 23:1–9. doi: 10.1016/S0193-953X(05)70139-8
12. Quenneville AF, Kalogeropoulou E, Küng AL, Hasler R, Nicastro R, Prada P, et al. Childhood maltreatment, anxiety disorders and outcome in borderline personality disorder. Psychiatry Res. (2020) 284:112688. doi: 10.1016/j.psychres.2019.112688
13. Antoine SM, Fredborg BK, Streiner D, Guimond T, Dixon-Gordon KL, Chapman AL, et al. Subgroups of borderline personality disorder: A latent class analysis. Psychiatry Res. (2023) 323:115131. doi: 10.1016/j.psychres.2023.115131
14. Benzi IMA, Di Pierro R, De Carli P, Cristea IA, Cipresso P. All the faces of research on borderline personality pathology: Drawing future trajectories through a network and cluster analysis of the literature. J Evidence-Based Psychotherapies. (2020) 20:3–30. doi: 10.24193/jebp.2020.2.9
15. Reis T, Gekker M, Land MGP, Mendlowicz MV, Berger W, Luz MP, et al. The growth and development of research on personality disorders: A bibliometric study. Pers Ment Health. (2022) 16:290–9. doi: 10.1002/pmh.1540
16. Singh VK, Singh P, Karmakar M, Leta J, Mayr P. The journal coverage of Web of Science, Scopus and Dimensions: A comparative analysis. Scientometrics. (2021) 126:5113–42. doi: 10.1007/s11192-021-03948-5
18. Price DJ. Networks of scientific papers. Science. (1965) 149:510–5. doi: 10.1126/science.149.3683.510
19. Sabe M, Chen C, Perez N, Solmi M, Mucci A, Galderisi S, et al. Thirty years of research on negative symptoms of schizophrenia: A scientometric analysis of hotspots, bursts, and research trends. Neurosci Biobehav Rev. (2023) 144:104979. doi: 10.1016/j.neubiorev.2022.104979
20. Shen Z, Ji W, Yu S, Cheng G, Yuan Q, Han Z, et al. Mapping the knowledge of traffic collision reconstruction: A scientometric analysis in CiteSpace, VOSviewer, and SciMAT. Sci Justice. (2023) 63:19–37. doi: 10.1016/j.scijus.2022.10.005
21. Wu H, Wang Y, Tong L, Yan H, Sun Z. Global research trends of ferroptosis: A rapidly evolving field with enormous potential. Front Cell Dev Biol. (2021) 9:646311. doi: 10.3389/fcell.2021.646311
22. Brody S. Impact factor: Imperfect but not yet replaceable. Scientometrics. (2013) 96:255–7. doi: 10.1007/s11192-012-0863-x
23. Kaldas M, Michael S, Hanna J, Yousef GM. Journal impact factor: A bumpy ride in an open space. J Invest Med. (2020) 68:83–7. doi: 10.1136/jim-2019-001009
24. Schubert A, Glänzel W. A systematic analysis of Hirsch-type indices for journals. J Informetrics. (2007) 1:179–84. doi: 10.1016/j.joi.2006.12.002
25. Chen C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. (2006) 57:359–77. doi: 10.1002/asi.20317
26. Cheng K, Guo Q, Shen Z. Bibliometric analysis of global research on cancer photodynamic therapy: Focus on nano-related research. Front Pharmacol. (2022) 13:927219. doi: 10.3389/fphar.2022.927219
27. Hassan-Montero Y, De-Moya-Anegón F, Guerrero-Bote VP. SCImago Graphica: A new tool for exploring and visually communicating data. Profesional la Información. (2022) 31:e310502. doi: 10.3145/EPI
28. Wang Y, Li D, Jia Z, Hui J, Xin Q, Zhou Q, et al. A bibliometric analysis of research on the links between gut microbiota and atherosclerosis. Front Cardiovasc Med. (2022) 9:941607. doi: 10.3389/fcvm.2022.941607
29. Soloff PH, Lynch KG, Kelly TM, Malone KM, Mann JJ. Characteristics of suicide attempts of patients with major depressive episode and borderline personality disorder: a comparative study. Am J Psychiatry. (2000) 157:601–8. doi: 10.1176/appi.ajp.157.4.601
30. Widiger TA, Trull TJ. Plate tectonics in the classification of personality disorder: shifting to a dimensional model. Am Psychol. (2007) 62:71–83. doi: 10.1037/0003-066X.62.2.71
31. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. (1995) 51:768–74. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1
32. Bartow S, Stopsack M, Grabe HJ, Meinke C, Spitzer C, Kronmüller K, et al. Interpersonal evaluation bias in borderline personality disorder. Behav Res Ther. (20092009) 47:359–65. doi: 10.1016/j.brat.2009.02.003
33. Cheavens JS, Rosenthal MZ, Daughters SB, Nowak J, Kosson D, Lynch TR, et al. An analogue investigation of the relationships among perceived parental criticism, negative affect, and borderline personality disorder features: The role of thought suppression. Behav Res Ther. (2005) 43:257–68. doi: 10.1016/j.brat.2004.01.006
34. Bradley R, Westen D. The psychodynamics of borderline personality disorder: a view from developmental psychopathology. Dev Psychopathol. (2005) 17:927–57. doi: 10.1017/s0954579405050443
35. Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. NeuroImage. (2002) 15:273–89. doi: 10.1006/nimg.2001.0978
36. Bellino S, Rinaldi C, Bozzatello P, Bogetto F. Pharmacotherapy of borderline personality disorder: a systematic review for publication purpose. Curr Medicinal Chem. (2011) 18:3322–9. doi: 10.2174/092986711796504682
37. Zanarini MC, Frankenburg FR, Dubo ED, Sickel AE, Trikha A, Levin A. Axis I comorbidity of borderline personality disorder. Am J Psychiatry. (1998) 155:1733–9. doi: 10.1176/ajp.155.12.1733
38. Yee L, Korner AJ, McSwiggan S, Meares RA, Stevenson J. Persistent hallucinosis in borderline personality disorder. Compr Psychiatry. (2005) 46:147–54. doi: 10.1016/j.comppsych.2004.07.032
39. Mittal VA, Walker EF. Diagnostic and statistical manual of mental disorders. Psychiatry Res. (2011) 189:158–9. doi: 10.1016/j.psychres.2011.06.006
40. Torgersen S, Kringlen E, Cramer V. The prevalence of personality disorders in a community sample. Arch Gen Psychiatry. (2001) 58:590–6. doi: 10.1001/archpsyc.58.6.590
41. Crick NR, Murray-Close D, Woods K. Borderline personality features in childhood: A short-term longitudinal study. Dev Psychopathol. (2005) 17:1051–70. doi: 10.1017/S0954579405050492
42. Linehan MM, Comtois KA, Murray AM, Brown MZ, Gallop RJ, Heard HL, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. (2006) 63:757–66. doi: 10.1001/archpsyc.63.7.757
43. Giesen-Bloo J, van Dyck R, Spinhoven P, van Tilburg W, Dirksen C, van Asselt T, et al. Outpatient psychotherapy for borderline personality disorder: Randomized trial of schema-focused therapy vs transference-focused psychotherapy. Arch Gen Psychiatry. (2006) 63:649–58. doi: 10.1001/archpsyc.63.6.649
44. Crowell SE, Beauchaine TP, Linehan MM. A biosocial developmental model of borderline personality: Elaborating and extending Linehan's theory. psychol Bulletin. (2009) 135:495–510. doi: 10.1037/a0015616
45. Leichsenring F, Leibing E, Kruse J, New AS, Leweke F. Borderline personality disorder. Lancet (2011) 377(9759):74–84. doi: 10.1016/S0140-6736(10)61422-5
46. Whiteside SP, Lynam DR, Miller JD, Reynolds SK. Validation of the UPPS impulsive behaviour scale: A four-factor model of impulsivity. Eur J Pers (2005) 19(7):559–74. doi: 10.1002/per.556
47. Clarkin JF, Levy KN, Lenzenweger MF, Kernberg OF. Evaluating three treatments for borderline personality disorder: A multiwave study. Am J Psychiatry (2007) 164(6):922–8. doi: 10.1176/ajp.2007.164.6.922
48. Bateman A, Fonagy P. Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder. Am J Psychiatry (2009) 166(12):1355–64. doi: 10.1176/appi.ajp.2009.09040539
49. Fonagy P, Luyten P. A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Dev Psychopathol (2009) 21(4):1355–81. doi: 10.1017/S0954579409990198
50. Levy KN, Meehan KB, Kelly KM, Reynoso JS, Weber M, Clarkin JF, et al. Change in attachment patterns and reflective function in a randomized control trial of transference-focused psychotherapy for borderline personality disorder. J Consulting Clin Psychol (2006) 74(6):1027–40. doi: 10.1037/0022-006X.74.6.1027
51. Carr DS, Francis A. Childhood familial environment, maltreatment and borderline personality disorder symptoms in a non-clinical sample: A cognitive behavioural perspective. Clin Psychol (2009) 13(1):28–37. doi: 10.1080/13284200802680476
52. Selby EA, Kranzler A, Fehling KB, Panza E. Nonsuicidal self-injury disorder: The path to diagnostic validity and final obstacles. Clin Psychol Review. (2015) 38:79–91. doi: 10.1016/j.cpr.2015.03.003
53. Skoglund C, Tiger A, Rück C, Petrovic P, Asherson P, Hellner C, et al. Familial risk and heritability of diagnosed borderline personality disorder: A register study of the Swedish population. Mol Psychiatry. (2021) 26:999–1008. doi: 10.1038/s41380-019-0442-0
54. American Psychiatric Association, DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5™. 5th ed. Washington: American Psychiatric Publishing, Inc., (2013). doi: 10.1176/appi.books.9780890425596
55. Cristea IA, Gentili C, Cotet CD, Palomba D, Barbui C, Cuijpers P. Efficacy of psychotherapies for borderline personality disorder: A systematic review and meta-analysis. JAMA Psychiatry. (2017) 74:319–28. doi: 10.1001/jamapsychiatry.2016.4287
56. Chen C. Predictive effects of structural variation on citation counts. J Am Soc Inf Sci Technol. (2012) 63:431–49. doi: 10.1002/asi.21694
57. Brown MZ, Comtois KA, Linehan MM. Reasons for suicide attempts and non-suicidal self-injury in women with borderline personality disorder. J Abnormal Psychol. (2002) 111:198–202. doi: 10.1037//0021-843x.111.1.198
58. Siever LJ, Davis KL. A psychobiological perspective on the personality disorders. Am J Psychiatry. (1991) 148:1647–58. doi: 10.1176/ajp.148.12.1647
59. Donegan NH, Sanislow CA, Blumberg HP. Amygdala hyperreactivity in borderline personality disorder: Implications for emotional dysregulation. Biol Psychiatry. (2003) 54:1284–93. doi: 10.1016/S0006-3223(03)00636-X
60. Tebartz van Elst L, Hesslinger B, Thiel T, Geiger E, Haegele K, Lemieux L, et al. Frontolimbic brain abnormalities in patients with borderline personality disorder: A volumetric magnetic resonance imaging study. Biol Psychiatry. (2003) 54:163–71. doi: 10.1016/s0006-3223(02)01743-2
61. Herpertz SC, Dietrich TM, Wenning B, Krings T, Erberich SG, Willmes K, et al. Evidence of abnormal amygdala functioning in borderline personality disorder: A functional MRI study. Biol Psychiatry. (2001) 50:292–8. doi: 10.1016/S0006-3223(01)01075-7
62. Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford Press (1993).
63. Black DW, Blum N, Pfohl B, Hale N. Suicidal behavior in borderline personality disorder: Prevalence, risk factors, prediction, and prevention. J Pers Disord (2004) 18(3):226–39. doi: 10.1521/pedi.18.3.226.35445
64. Brambilla P, Soloff PH, Sala M, Nicoletti MA, Keshavan MS, Soares JC. Anatomical MRI study of borderline personality disorder patients. Psychiatry Res (2004) 131(2):125–33. doi: 10.1016/j.pscychresns.2004.04.003
65. Stiglmayr CE, Grathwol T, Linehan MM, Ihorst G, Fahrenberg J, Bohus M. Aversive tension in patients with borderline personality disorder: A computer-based controlled field study. Acta Psychiatrica Scandinavica (2005) 111(5):372–9. doi: 10.1111/j.1600-0447.2004.00466.x
66. Silbersweig D, Clarkin JF, Goldstein M, Kernberg OF, Tuescher O, Levy KN, et al. Failure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder. Am J Psychiatry (2007) 164(12):18321841. doi: 10.1176/appi.ajp.2007.06010126
67. Bohus M, Haaf B, Stiglmayr C, Pohl U, Böhme R, Linehan M. Evaluation of inpatient dialectical-behavioral therapy for borderline personality disorder–a prospective study. Behav Res Ther (2000) 38(9):875887. doi: 10.1016/s0005-7967(99)00103-5
68. Rossouw TI, Fonagy P. Mentalization-based treatment for self-harm in adolescents: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry (2012) 51(12):13041313. doi: 10.1016/j.jaac.2012.09.018
69. Zhang S, Wang S, Liu R. A bibliometric analysis of research trends of artificial intelligence in the treatment of autistic spectrum disorders. Front Psychiatry. (2022) 13:967074. doi: 10.3389/fpsyt.2022.967074
70. Dzikowski P. A bibliometric analysis of born global firms. J Business Res. (2018) 85:281–94. doi: 10.1016/j.jbusres.2017.12.054
71. Chen C, Ibekwe-SanJuan F, Hou J. The structure and dynamics of cocitation clusters: A multiple-perspective cocitation analysis. J Am Soc Inf Sci Technol. (2010) 61:1386–409. doi: 10.1002/asi.21309
72. Gunderson JG, Herpertz SC, Skodol AE, Torgersen S, Zanarini MC. Borderline personality disorder. Nat Rev Dis Primers. (2018) 4:18029. doi: 10.1038/nrdp.2018.29
73. Tan MYL, McConnell B, Barlas J. Application of Dialectical Behaviour Therapy in treating common psychiatric disorders: Study protocol for a scoping review. BMJ Open. (2002) 12:e058565. doi: 10.1136/bmjopen–2021–058565
74. Quevedo Y, Booij L, Herrera L, Hernández C, Jiménez JP. Potential epigenetic mechanisms in psychotherapy: A pilot study on DNA methylation and mentalization change in borderline personality disorder. Front Hum Neurosci. (2022) 16:955005. doi: 10.3389/fnhum.2022.955005
75. Uhlmann C, Tschöke S, Steinert T, Schmid P. Can you see and hear how bad I feel right now? Self–injury and suicidal communication in borderline personality disorder-A secondary analysis. Psychiatrische Praxis. (2022) 49:329–33. doi: 10.1055/a–1820–0438
76. Bohus M, Stoffers-Winterling J, Sharp C, Krause-Utz A, Schmahl C, Lieb K. Borderline personality disorder. Lancet (2022) 398:1528–40. doi: 10.1016/S0140–6736(21)00476–1
77. Schuppert HM, Giesen-Bloo J, van Gemert TG, Wiersema HM, Minderaa RB, Emmelkamp PMG, et al. Effectiveness of an emotion regulation group training for adolescents—A randomized controlled pilot study. Clin Psychol Psychother. (2009) 16:467–78. doi: 10.1002/cpp.637
78. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, text revision. 4th ed. Washington: American Psychiatric Association (2000).
79. Lenzenweger MF, Cicchetti D. Toward a developmental psychopathology approach to borderline personality disorder. Dev Psychopathol. (2005) 17:893–8. doi: 10.1017/S095457940505042X
80. Chanen AM, Jovev M, McCutcheon LK, Jackson HJ, McGorry PD. Borderline personality disorder in young people and the prospects for prevention and early intervention. Curr Psychiatry Rev. (2008) 4:48–57. doi: 10.2174/157340008783743820
81. Pohl S, Steuwe C, Mainz V, Driessen M, Beblo T. Borderline personality disorder and childhood trauma: Exploring the buffering role of self-compassion and self-esteem. J Clin Psychol. (2021) 77:837–45. doi: 10.1002/jclp.23070
82. Bartsch DR, Roberts R, Proeve M. Relationships between parental borderline symptom severity, empathy, parenting styles and child psychopathology. Clin Psychol. (2022) 26:211–21. doi: 10.1080/13284207.2022.2031947
Keywords: neuro-behavioral model, borderline personality disorder, BPD, bibliometric, Scimago Graphica
Citation: Liu Y, Chen C, Zhou Y, Zhang N and Liu S (2024) Twenty years of research on borderline personality disorder: a scientometric analysis of hotspots, bursts, and research trends. Front. Psychiatry 15:1361535. doi: 10.3389/fpsyt.2024.1361535
Received: 12 January 2024; Accepted: 19 February 2024;
Published: 01 March 2024.
Edited by:
Lionel Cailhol, University Institute in Mental Health of Montreal, CanadaReviewed by:
Dominick Gamache, Université du Québec à Trois-Rivières, CanadaCopyright © 2024 Liu, Chen, Zhou, Zhang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shen Liu, bGl1c2hlbkBhaGF1LmVkdS5jbg==; Chaomei Chen, Y2MzNDVAZHJleGVsLmVkdQ==; Na Zhang, emhhbmduYUBhaGpneHkuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.