 Camila Corrêa Matias Pereira
Camila Corrêa Matias Pereira Vahid Najafi Moghaddam Gilani
Vahid Najafi Moghaddam Gilani José Ignacio Nazif-Munoz
José Ignacio Nazif-Munoz
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry, 25 July 2024
Sec. Aging Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1354030
This article is part of the Research TopicSuicide in Geriatric PopulationsView all 11 articles
Objectives: Aiming to disseminate information related to suicide prevention in Brazil, the “Setembro Amarelo” campaign has been conducted since 2015. The objective of this study is to assess the association between this campaign and elderly suicide rates over a 12-year period.
Methods: Data were gathered from the Mortality Information System and the Notifiable Diseases Information System, established by public institutions in Brazil. An interrupted time-series framework was applied to assess the association between the “Setembro Amarelo” campaign and suicide mortality rates in the elderly population (60 et plus) in the southeastern region of Brazil. We consider three monthly outcomes: all suicides, suicides in males and suicide in females. We operationalize the campaign assuming three effects: short-term, declining and sustained. The period of analysis was from 2011-2022.
Results: The suicide-mortality rate over time has remained stable; the average rate in the pre-campaign period was 0.028 and increased slightly to 0.035. Regardless of the campaign’s operationalization and the outcome used, results show no significant associations between the campaign and elderly suicide rates. The campaign was associated with non-significant decreased effects of 15% (P=0.532) in the short term, and 16% (P=0.446) assuming the campaign was sustained.
Conclusions: There is a lack of association between the campaign and suicide rates, among the elderly in Brazil’s southeastern region. As suicide is complex and multifactorial, more research is needed. The campaign, while raising awareness and reducing stigma, may not reduce suicides. To reduce the suicide rate in the elderly requires addressing social, economic and cultural factors, multisectoral interventions, and upholding basic human rights.
The World Health Organization (WHO) underscores the alarming worldwide impact of suicide, with more than 700,000 deaths annually. Suicide prevention prominently features on the WHO’s agenda and is integrated as an indicator in the United Nations’ Sustainable Development Goals (1). Effective suicide prevention strategies require understanding of risk and protective factors across different life stages (2). Elderly individuals face the highest global suicide risk, with elevated lethality (3–6). Unique risk factors for this group include among others social isolation, bereavement, loss of social roles, debilitating illnesses, depression, loneliness, and access to lethal means (items that can be used in a suicide, such as firearms and certain drugs or toxic substances) (3–10). In general elderly individuals exhibit a heightened suicide rate, attributed to more lethal attempts (11, 12).To address prevention, there is an urgent need for comprehensive suicide prevention programs (SPP) involving diverse sectors such as health, education, social welfare, media and case notification, aiming to optimize tailored initiatives across contexts (2, 13, 14).
The rapid aging of the population underscores a pressing issue regarding the deteriorating epidemiological circumstances for older adults, as the provision of care, aid, and backing for this demographic fails to advance adequately in terms of speed, urgency, or scope. Among the specific challenges encountered by this demographic, especially in low and middle-income countries, is the prevalence of suicide (15–18). While the World Health Organization (WHO) marks the onset of old age at 65, as this may be indicative of potential retirement and eligibility for certain benefits, this age threshold may drop to 60 in areas with shorter life expectancies (19, 20). In Brazil, its Federal Law No. 8.842/1994, classifies individuals as elderly if they are 60 years of age or older (21). The suicide death rates of elderly in Brazil from 1996 to 2018 have increased by 162.2% (age group 60-69), 141.4% (70–79), and 189.3% (80 years and above) respectively (11). Overall, all Brazilian regions have experienced an increase of suicide rates in older adulthood from 1996 to 2018, with notable percentages in the North (81.1%), Northeast (126.5%), Southeast (26.6%), Central-West (28.5%) and South (17.8%) (11).
Studies conducted in Brazil have identified that the most frequent social reasons triggering suicide among the elderly include financial problems, unemployment, employment instability (e.g., farming, mining), relationship difficulties, family conflicts, social isolation, and loneliness (22–26). In general, the prevalence of male suicides is higher, associated with the fact that men are more competitive, impulsive, and have easier access to lethal means (27). Additionally, societal expectations within the Brazilian patriarchal culture, which cast men in the role of the primary provider for the family, further contribute to this phenomenon (27). Also, retirement, social exclusion and deprivation of social support, very common in the reality of the elderly, are linked to preliminary depression diagnoses and demoralization, important risk factors for suicide (28–30). In Brazil, there are scientific publications addressing aging and suicide in general; however, few focus on elderly suicide mortality, underscoring the need for further research on these topics within the country (4, 31–33).
In Brazil, in 2015, an initiative led by the Center for Valorization of Life (CVV- Brazilian helpline), the Federal Medical Council, and the Brazilian Psychiatric Association created a campaign called “Setembro Amarelo,” (Yellow September), aimed at suicide prevention and raising awareness. While the campaign runs throughout the year, its concentrated events occur in September. Throughout this month, the campaign endeavors to raise societal awareness and disseminate information related to suicide prevention in the country. This includes organizing events to discuss mental health and suicide prevention, reducing stigma, sharing data on suicide rates, promoting help channels, distributing educational materials, providing specific training, and lighting national landmarks in yellow (34–36). A limited number of studies from Brazil (37–40) have endeavored to evaluate changes following the campaign’s implementation. The impact of this campaign on suicide mortality rates, in this specific age-group, remains unexamined. The present study investigated Brazilian elderly suicide rates over a 12-year period, considering the launch and implementation of the “Setembro Amarelo” campaign.
We applied a quasi-experimental design by using an interrupted time-series (ITS) framework (41) spanning twelve years (2011 to 2022). We specifically assess the association between the “Setembro Amarelo” campaign and suicide mortality rates in the elderly population. We selected three outcomes: i) all suicides, ii) suicides in males and iii) suicide in females.
We utilized publicly available and official information derived from the Brazilian Government. Data were extracted from the Mortality Information System (SIM) and the Notifiable Diseases Information System (SINAN), both established by the Brazilian Ministry of Health and accessible via the DATASUS online platform. This system functions through the systematic compilation of data concerning vital statistics, encompassing mortality and survival rates, as well as epidemiological and morbidity insights. We restricted our analysis to monthly suicide mortality rates for the southeastern region of Brazil, which encompasses São Paulo, Rio de Janeiro, Minas Gerais, and Espírito Santo. This dataset covers the years from 2011 to 2022. The database (case registration) for the SIM and SINAN was more complete in the southeast region, therefore, this region was chosen for the analyzed years. Additionally, we included data on unemployment rates obtained from the International Labour Organization (ILO) for the same period, 2011 to 2022.
Counts of suicide mortality rates in the elderly population (Yij) and counts of suicides for male (YMij) and female (YWij) respectively, were derived from the total number of fatal self-inflicted injuries of individuals of 60 years and over, information gathered from the Brazilian Ministry of Health. We have included the classification according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (42), including ICD codes (X60 to X84), corresponding to Intentional self-harm. The rate was obtained by dividing the total number of individuals aged 60 and more, population numbers were gathered from the Brazilian census data.
We operationalized “Setembro Amarelo” campaign, in three forms: i) Short-term effect: 0 for the years 2011 to 2014, 0 for January to August and for October to December for the years 2015 to 2022, and 1 for September for the years 2015 to 2022. We assumed this campaign was effective only during September since 2015; ii) Declining effect: 0 for the years 2011 to 2014, 0 for January to August and for December for the years 2015 to 2022, and since 2015 1, for Sep, 0.5 for October, and 0.25 for November. We assume this campaign was effective from September to November however its effect may have declined at the third month of implementation; iii) Sustained effect: 0 for the years 2011 to 2014, 0 for January to August and for December for the years 2015 to 2022, and since 2015 1 for the months of September, October, and November.
In our study, we addressed the potential impact of seasonal variations by incorporating Fourier terms, using pairs of sine and cosine functions to model these patterns. Additionally, unemployment rates were included as a control variable. Specifically, these rates pertain to adults aged 60 years and older.
An extension of generalized linear models was employed, incorporating both the Poisson and Negative Binomial models. These models are well suited for the analysis of count data, such as number of suicides. The Poisson model is a reliable choice for modeling count data when events occur at a consistent rate over time. On the other hand, the Negative Binomial model offers flexibility and accounts for data over-dispersion, which is common when dealing with rare events like suicides. The use of the Poisson and Negative Binomial models within the ITS analysis ensures a thorough exploration of temporal patterns and trends, providing more nuanced insights into the connection between the campaign and suicide rates.
Table 1 provides an overview of summary statistics regarding suicide mortality rates across all gender categories. Figures 1–3 present monthly time-series plots for the suicide mortality rates: all individuals, males, and females aged above 60 years old, respectively. Tables 2, 3 provide the results Poisson and the Negative Binomial models.

Table 1 Monthly suicide rates per 100 000 population before, during and after three operationalizations of the “Setembro Amarelo” Campaign.
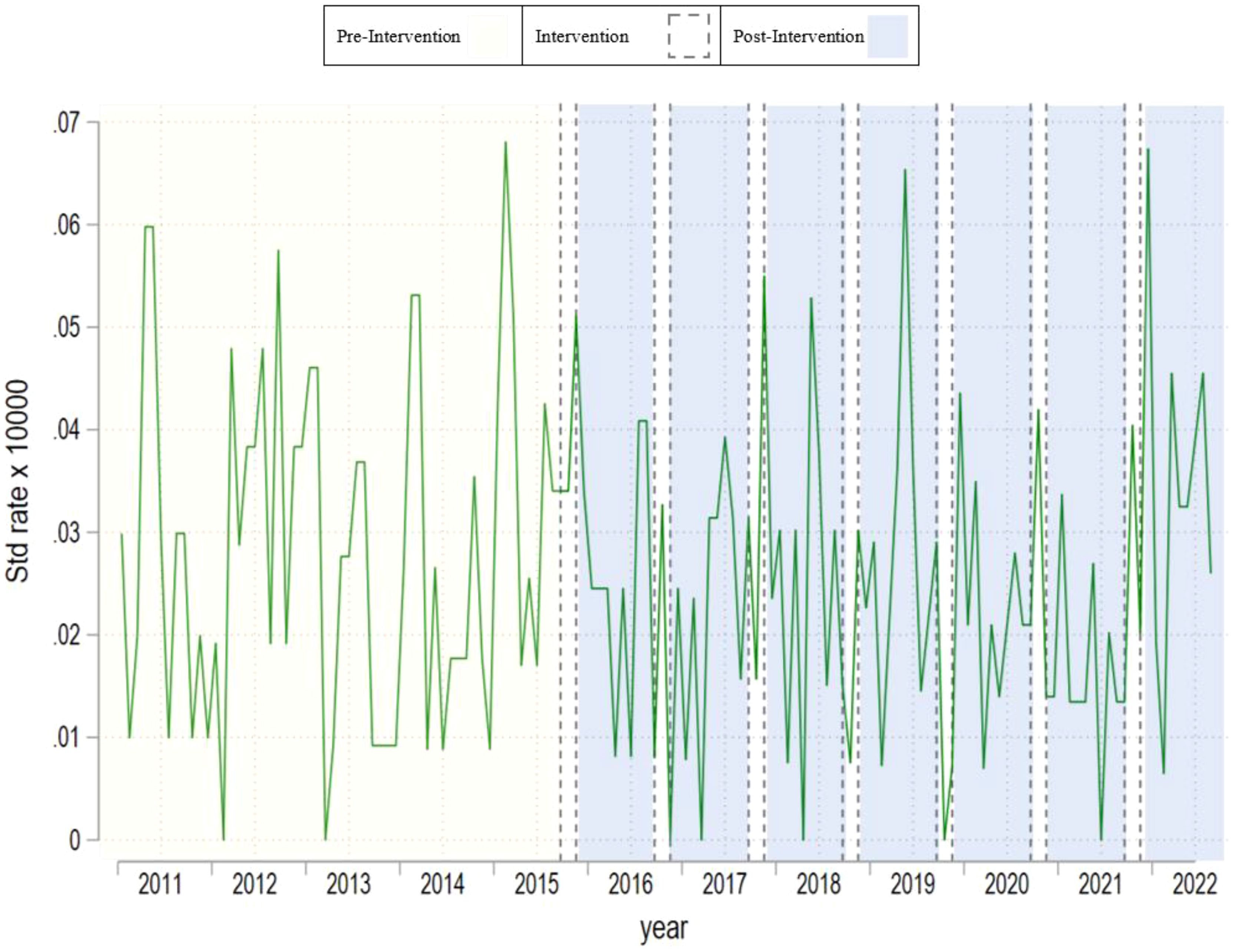
Figure 1 Monthly time–series plot for suicide rate of all individuals aged above 60 years old.
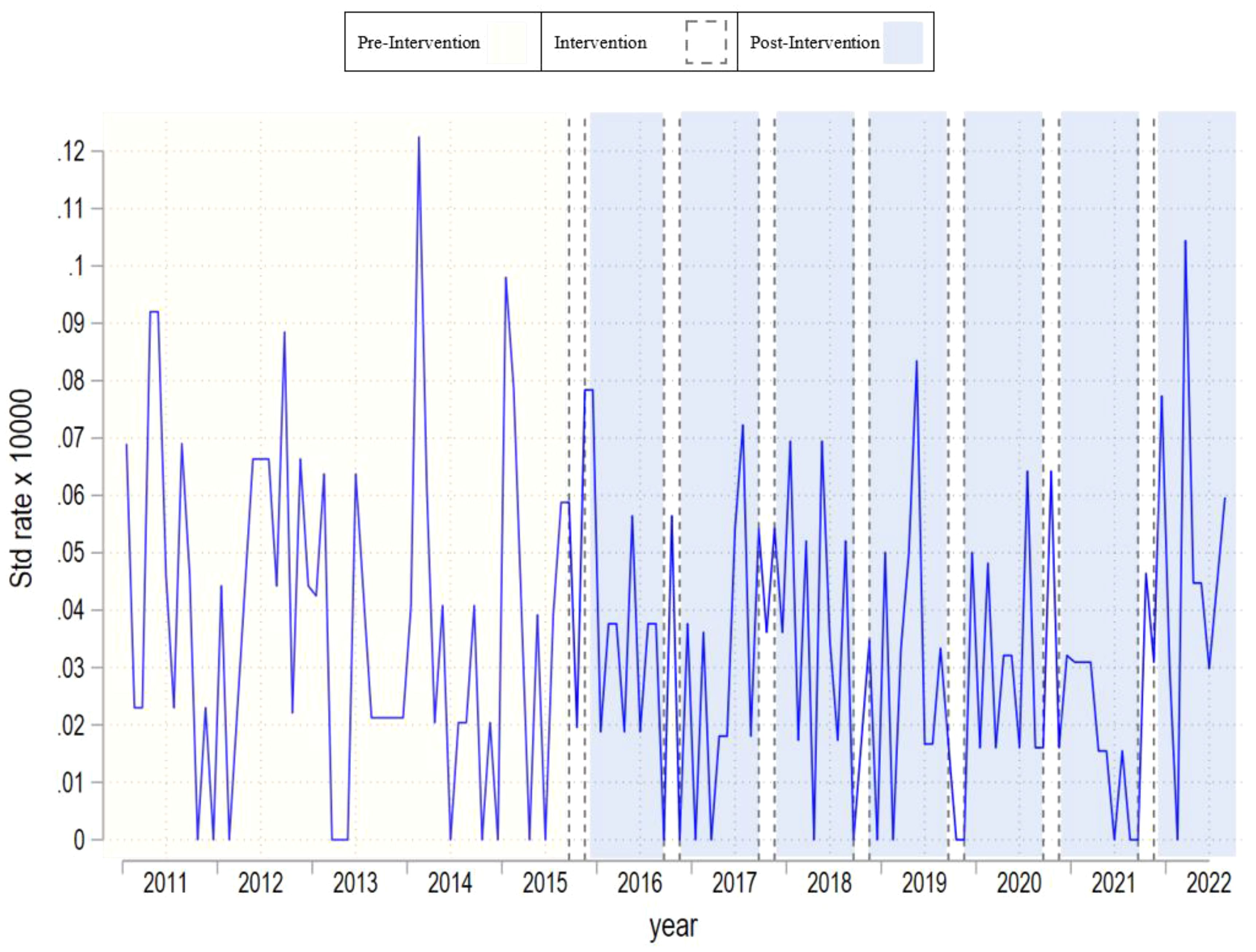
Figure 2 Monthly time–series plot for suicide rate of males aged above 60 years old.
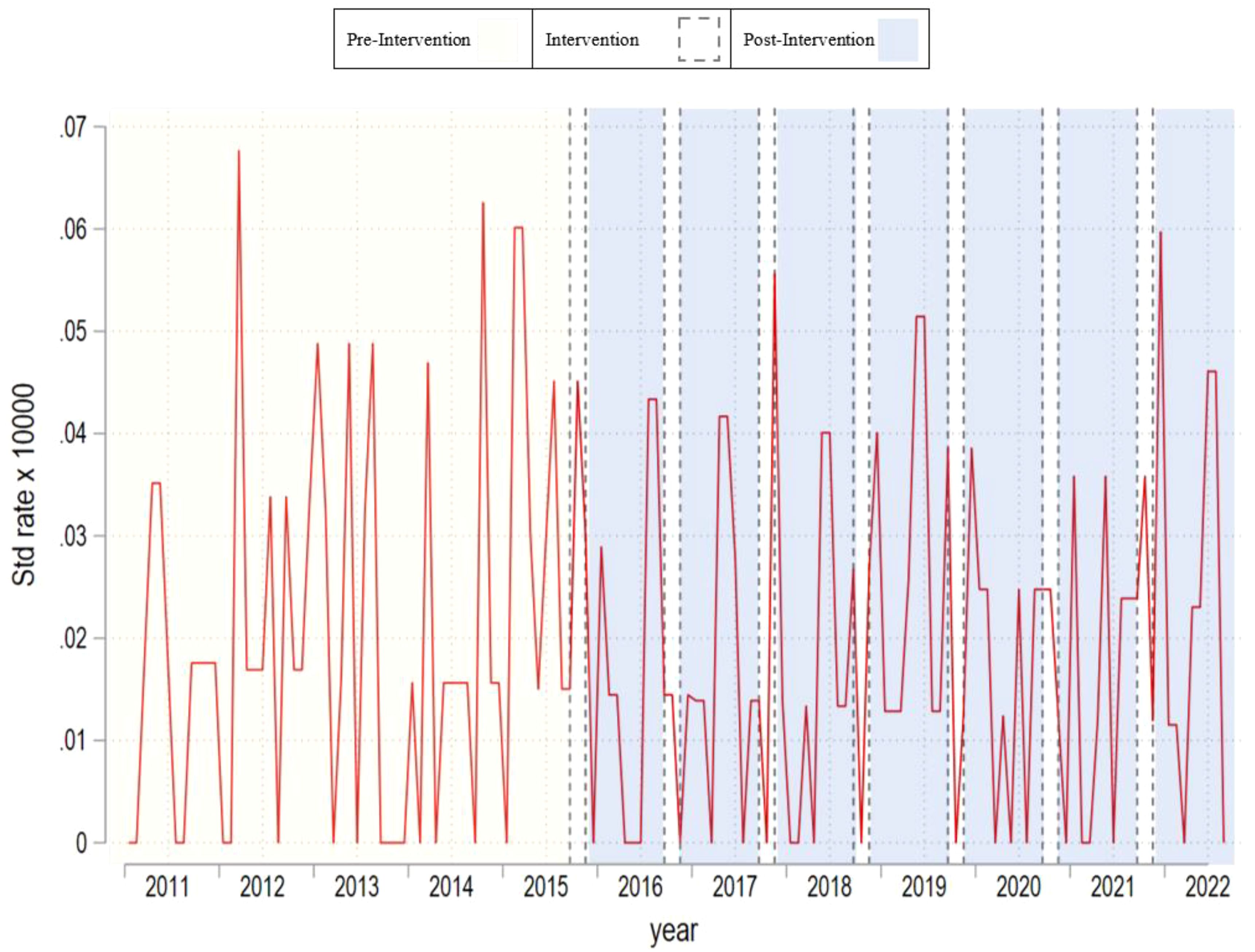
Figure 3 Monthly time–series plot for suicide rate of females aged above 60 years old.
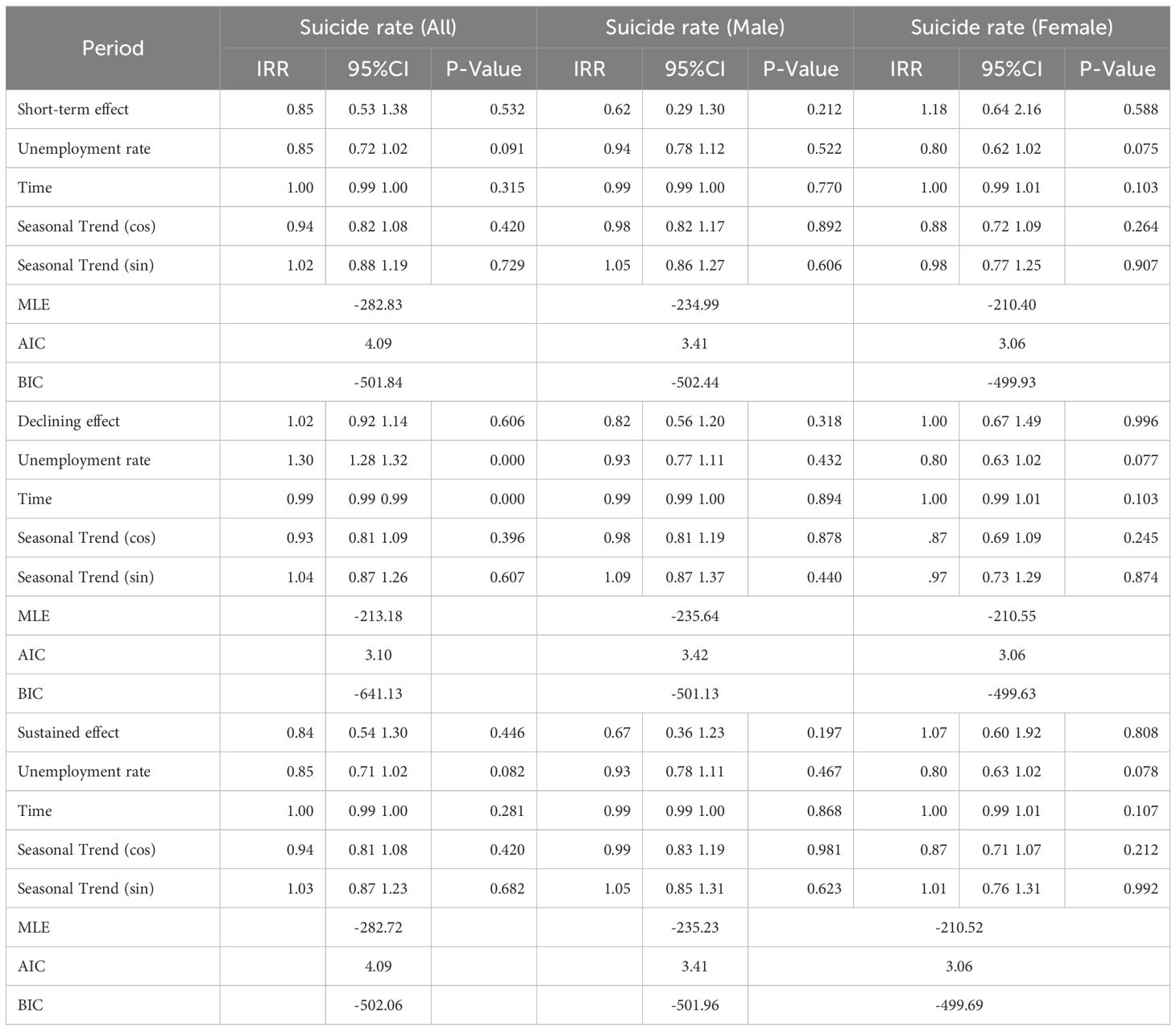
Table 2 Poisson model results for suicide rate of all types of gender groups.
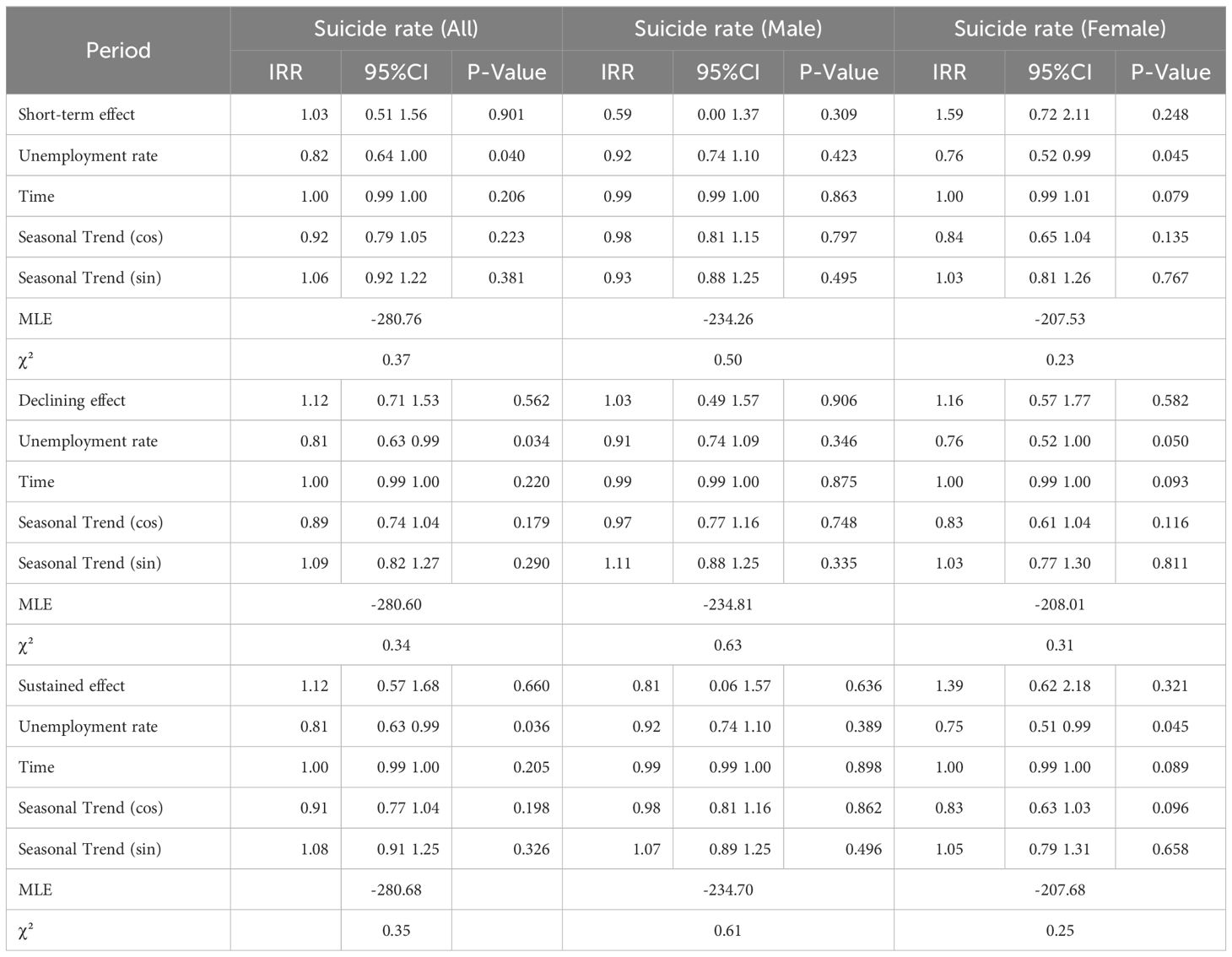
Table 3 Negative binomial model results for suicide rate of all types of gender groups.
In Table 1, we observe that suicide mortality rates over time are relatively stable. Whereas the mean in the pre campaign period is 0.028 at the end of studied period the rate is slightly higher with 0.035. This trend is also observed in men and women respectively. Nevertheless, we observe differences across men and women rates. In the per period campaign men’s rates were 0.038 and women’s 0.020, and at the end of the analyzed period these rates were 0.048 and 0.024 respectively. Based on the results of Tables 2, 3, we fail to observe significant associations between the campaign and suicide mortality rates regardless of the campaign’s operationalization and the outcome used. The decision to collapse the data for the declining and sustained effects was made due to their similar statistical outcomes in preliminary analyses, simplifying the presentation and focusing on the most significant findings. Results were robust after we included unemployment rates as well.
Our analysis of the association between unemployment rates and suicide rates showed variability by the model and demographic group. In the Poisson model, unemployment rates were not significantly associated with changes in suicide rates. However, the Negative Binomial model indicated a significant impact for all individuals and females, but not for males, suggesting differing economic effects across demographic groups. Statistical tests for stationarity confirmed the reliability of these findings. The Augmented Dickey-Fuller (ADF) tests showed that the series are stationary, and the Kwiatkowski-Phillips-Schmidt-Shin (KPSS) tests indicated a presence of a stochastic trend at zero lags. These tests are detailed in the newly added Table 4, enhancing our understanding of the data’s characteristics and the robustness of our analysis.

Table 4 Results of Augmented Dickey-Fuller (ADF) and Kwiatkowski-Phillips-Schmidt-Shin (KPSS) Tests.
In this quasi-experimental study, we observe no significant differences between three different operationalizations of the “Setembro Amarelo” campaign and suicide mortality rates in the elderly population in four Brazilian States: São Paulo, Rio de Janeiro, Minas Gerais, and Espírito Santo. This lack of association is observed regardless of the operationalization of the campaign and statistical method applied. Our analyses also indicate that the campaign was not necessarily effective when targeting men nor women specifically. While the World Health Organization recommends conducting awareness and prevention campaigns utilizing mass media to promote mental health, raise awareness, reduce mental health stigma, and disseminate information about support resources, these efforts should be accompanied with specific prevention interventions (6, 43). Indeed, sparsely evaluated outcomes of suicide prevention campaigns have demonstrated contradictory and inconsistent results (43, 44), with positive effects on awareness and help-seeking (43–45), or the need for caution when developing strategies because of prejudice, misinformation and questioning how to reach vulnerable populations not considered in more consistent prevention efforts (44, 46).
Our study partially aligns with at least three studies developed in Brazil. First, a time-series study analyzed the temporal pattern of suicide mortality in the state of Ceará between 2009 and 2019. The study observed that the population aged 60 to 79 experienced a stabilization in suicide rates, raising questions about the campaign’s potential impact in this age group within this state (38). A second study conducted to identify changes following the implementation of “Setembro Amarelo”, in the Brazilian population, revealed that suicide-related incidence rates showed an upward trend after the program’s implementation. The suicide rate increased by 66.6% (37). Third, an interrupted time series study analyzed the evolution of elderly suicide rates in Brazil between 2011 and 2019 (30), observing a 14.3% increase in suicide rates after the campaign was implemented. These results raised considerable questions as to whether this increment was due to an adverse effect of the campaign’s implementation or a result of more effective case reporting (37).
The following elements are necessary to interpret our results. First, while there are guidelines issued by the Brazilian Psychiatric Association (47), based on international guidelines, on how to safely communicate or address suicidal behavior, many recommendations may not be followed. More specifically, the campaign may lack multi-sectoral actions, establishing an assistance network, implementing longitudinal strategies for monitoring at-risk groups (i.e. men, or elderly), as well as offering training and professional development opportunities (39). Relatedly, in September, the Brazilian campaign may lead many to discuss the topic of suicide, however, taking preventive actions and ensuring secure communication about suicide requires a more nuanced approach to avoid the risk of contagion (38, 48).
Second, suicide is generally underreported more than other causes of death, a trend that intensifies when concerning the elderly (2, 49–51). Death certificate data may be underreported due to various factors, including differing professional perspectives and training regarding their completion. Suspected suicide cases may be recorded as accidental poisonings or other external causes of mortality. Numerous taboos (for religious, cultural, or other reasons) and bureaucratic challenges, such as idealized post-mortem perceptions, life insurance implications, and the need for accurate cause of death, contribute to this context. Overcoming underreporting is crucial to enable reliable epidemiological analyses and, consequently, to inform effective care strategies (4, 52, 53). Two Brazilian studies analyzing suicide notifications after the campaign found no changes regarding self-harm case notifications; it may have even triggered the opposite effect as increases in cases in October compared to August were observed (37, 40).
Third, public campaigns aimed at preventing suicide among the elderly effectively should include widespread societal efforts on mental health and suicide awareness, information about help seeking, investing in access policies to mental health professionals and therapists, proactive engagement with psychiatric patients following discharge or a suicidal crisis, integration with primary health care services, fiscal support from professionals, social cohesion via social media, targeted online discussion forums for the elderly, telephone helplines, community integration interventions to combat loneliness, and public health messages emphasizing the importance of social involvement for all older individuals (4, 54–57). Particular attention to reducing stigma in the elderly should be considered in these campaigns. Indeed, the elderly often do not recognize or seek help for mental illness due to stigma, seeing it as a weakness and fearing the loss of independence. Tackling stigma needs focused efforts through professional training, public education, media collaboration, and inclusion in health and social care programs to encourage help-seeking and community integration (58, 59). Much of these elements have not been considered in the “Setembro Amarelo” campaigns and therefore next versions of this campaign should discern some of these strategies to target elderly more properly (47, 48).
Fourth, in addition to the need for interventions tailored to different life stages, it is also crucial to develop gender-specific interventions. Studies indicate that women are more likely to seek healthcare services, exhibit better coping with stigma, prejudice, and taboos compared to men, resulting in increased access to mental health services for this population (60, 61). Furthermore, social roles, such as being mothers and grandmothers, are often viewed differently for men. Men, traditionally seen as providers, tend to lose this role as they age. The loss of this social role represents a significant risk factor for suicide in the elderly, that is why socioeconomic issues, including economic crises, unemployment, and reductions in personal income, are significant risk factors, especially among men (33, 60, 61). Studies conducted in Brazil corroborate the international literature, as it is believed that men exhibit more competitive and impulsive behaviors than women, along with higher substance abuse rates, including alcohol and drug consumption (4, 62).
Last, suicide, in Brazil as a social phenomenon, must account for religious practices (63). In this country, most individuals claim a religious affiliation and consider religion a significant aspect of their existence (64, 65). The relationship between religion and suicidal behavior is complex and it needs more research in different cultures and religious backgrounds, as it can offer both protective factors, (e.g. coping mechanism and support system) and risk elements (e.g. assigning all life responsibility to God, blaming spiritual beliefs for failures when feeling forsaken, and interpreting stressors as either divine retribution or the influence of “evil forces.”) (66–70). For the elderly, spirituality and religiosity have been linked to improved quality of life and mental health promotion promising valuable contributions to geriatric psychiatry effective interventions and campaigns (71, 72). The extent to which “Setembro Amarelo” should consider religious aspects in its messages is something that should be studied further.
Our study should consider the following limitations to better temper the implication of its results. First, a large range of suicide risk factors and regional inequalities play significant roles in Brazil (33). Indeed, this country is characterized by multiple cultures and deep social inequalities, emphasizing that our findings cannot be generalized to the entire nation. It may be the case that in other regions, the campaign was effective not only in the elderly population but in others too. Our results suggest thus the identification of region-specific public policies to properly assess the extent to which this campaign may have not been effective (33). Secondly, to analyze suicide mortality rates and the “Setembro Amarelo” campaign, it is essential to consider case notification challenges, a prevalent issue in several countries, including Brazil, where underreporting in official records maybe prevalent (4, 38). Suicide statistics result from a complex process involving various stages, including reports from family members, witnesses, physicians, law enforcement, coroners, and statisticians. Due to these procedural intricacies, data may be distorted throughout, particularly in regions where social, economic, cultural, and religious factors contribute to the stigma surrounding suicidal behavior (38, 52). Third, while we used different operationalizations to understand the potential impact of the campaign, our application considered the overall post period after the campaign was implemented. So, we did not study if there were specific years in which the campaign could have been more effective. Last, while suicide is a multifactorial phenomenon, our study only covered specific results in terms of sex, and some models also included the variable unemployment—which was robust to our main results. As this is the first study in the elderly population, and no significant associations were found in this region, one potential explanation could be a more consistent network of social support and better access to health services for the elderly. However, this should be tested with other variables, such as family composition, state programs, and health services designed to support this population. Nevertheless, other factors such as socioeconomic status or marital status, which have been consistently associated with suicide outcomes were not considered and therefore other analyses are necessary to better understand the potential impact of this campaign in other subgroups of the elderly population in Brazil.
To our knowledge, this is the first study to assess the impact of the “Setembro Amarelo” campaign on suicide rates among the elderly population in Brazil’s Southeast region. Regardless of the campaign’s operationalization and the outcome used, no significant variation was observed. It is important to emphasize that suicide is a complex and multifactorial phenomenon. Therefore, the campaign alone, which aims to raise awareness and reduce stigma related to mental health promotion and suicide prevention, requires other actions to effectively tackle suicides at the population level.
We emphasize the importance of developing more scientific research and public policies for suicide prevention in Brazil, based on scientific knowledge, culturally adapted, focused on different stages of the life cycle, as well as sex and gender-specific interventions. Public policies, regardless of their format, need to be evaluated and planned to achieve continuous interventions, not limited to specific campaign months, as suicide is a public health issue that occurs daily in Brazil and around the world.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/fruf.def Official morbimortality data in Brazil are made available by DATASUS - Information Technology Department of the Brazilian Public Health Care System (SUS).
CC: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation, Visualization. VN: Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. JN: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Fonds de recherche du Québec -Santé (JN-M, Grant 330642), Charles Le Moyne scholarship of CC.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. SUPRE Prevention of suicidal behaviours: a task for all (2020). Available online at: https://www.who.int/mental_health/prevention/suicide/information/en/.
2. World Health Organization. Suicide in the world: global health estimates. World Heal Organ. (2019) 32:1–32.
3. Dombrovski AY, Szanto K, Duberstein P, Conner KR, Houck PR, Conwell Y. Sex differences in correlates of suicide attempt lethality in late life. Am J Geriatr Psychiatry. (2008) 16:905–13. doi: 10.1097/JGP.0b013e3181860034
4. Santos MCLd, Giusti BB, Yamamoto CA, Ciosak SI, Szylit R. Suicide in the elderly: an epidemiologic study. Rev da Esc Enferm da USP. (2021) 55:1–9. doi: 10.1590/s1980-220x2019026603694
5. Snowdon J, Phillips J, Zhong B, Yamauchi T, Chiu HFK, Conwell Y. Changes in age patterns of suicide in Australia, the United States, Japan and Hong Kong. J Affect Disord. (2017) 211:12–9. doi: 10.1016/j.jad.2017.01.007
7. Beautrais AL. A case control study of suicide and attempted suicide in older adults. Suicide Life-Threatening Behav. (2002) 32:1–9. doi: 10.1521/suli.32.1.1.22184
8. Erlangsen A. Loss of partner and suicide risks among oldest old: a population-based register study. Age Ageing. (2004) 33:378–83. doi: 10.1093/ageing/afh128
9. Rubenowitz E, Waern M, Wilhelmson K, Allebeck P. Life events and psychosocial factors in elderly suicides – a case–control study. Psychol Med. (2001) 31:1193–202. doi: 10.1017/S0033291701004457
10. Johnson RM, Frank EM, Ciocca M, Barber CW. Training mental healthcare providers to reduce at-risk patients’ Access to lethal means of suicide: evaluation of the CALM project. Arch Suicide Res. (2011) 15:259–64. doi: 10.1080/13811118.2011.589727
11. Silva da, Marcolan JF. Tentativa de suicídio e suicídio no Brasil: análise epidemiológica. Med (Ribeirão Preto). (2021) 54(4):e-181793. doi: 10.11606/issn.2176-7262.rmrp.2021.181793
12. Stanley IH, Hom MA, Rogers ML, Hagan CR, Joiner TE. Understanding suicide among older adults: a review of psychological and sociological theories of suicide. Aging Ment Health. (2016) 20:113–22. doi: 10.1080/13607863.2015.1012045
13. Fakhari A, Azizi H, Farahbakhsh M, Esmaeili E. Effective programs on suicide prevention: Combination of review of systematic reviews with expert opinions. Int J Prev Med. (2022) 13:39. doi: 10.4103/ijpvm.IJPVM_454_20
14. Sakashita T, Oyama H. Developing a hypothetical model for suicide progression in older adults with universal, selective, and indicated prevention strategies. Front Psychiatry. (2019) 10:161/full. doi: 10.3389/fpsyt.2019.00161/full
15. Farahbakhsh M, Fakhari A, Davtalab Esmaeili E, Azizi H, Mizapour M, Asl Rahimi V, et al. The role and comparison of stressful life events in suicide and suicide attempt: A descriptive-analytical study. Iran J Psychiatry Behav Sci. (2020) 14(2):e96051. doi: 10.5812/ijpbs.96051
16. Fleischmann A, De Leo D. The world health organization’s report on suicide. Crisis. (2014) 35:289–91. doi: 10.1027/0227-5910/a000293
17. Naghavi M. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the Global Burden of Disease Study 2016. BMJ. (2019) 364:l94. doi: 10.1136/bmj.l94
18. De Leo D, Giannotti AV. Suicide in late life: A viewpoint. Prev Med (Baltim). (2021) 152:106735. doi: 10.1016/j.ypmed.2021.106735
20. World Health Organization. Global Health Observatory (GHO) – Life Expectancy at Birth. Geneva: WHO Press (2020).
21. Ministério da Saúde. Estatuto do Idoso. Brasil (2013). Available at: https://www.gov.br/mdh/pt-br/centrais-de-conteudo/pessoa-idosa/estatuto-do-idoso-2013/view.
22. Minayo MC de S, Cavalcante FG. Suicídio entre pessoas idosas: revisão da literatura. Rev Saude Publica. (2010) 44:750–7. doi: 10.1590/S0034-89102010000400020
23. Minayo MC de S, Cavalcante FG. Tentativas de suicídio entre pessoas idosas: revisão de literatura (2002/2013). Cien Saude Colet. (2015) 20:1751–62. doi: 10.1590/1413-81232015206.10962014
24. Souza ERde, Minayo MC de S, Cavalcante FG. O impacto do suicídio sobre a morbimortalidade da população de Itabira. Cien Saude Colet. (2006) 11:1333–42. doi: 10.1590/S1413-81232006000500022
25. Pires DX, Caldas ED, Recena MCP. Uso de agrotóxicos e suicídios no Estado do Mato Grosso do Sul, Brasil. Cad Saude Publica. (2005) 21:598–604. doi: 10.1590/S0102-311X2005000200027
26. Bucci MED, Silva LF, de Barbosa GT, Araújo CDFN, de Souza AC, dos Santos JBSV. The risk of dying of suicide in Brazil: a study carried out accordingto sex, age and indigenous ethnicy. Hygeia Rev Bras Geogr Médica e da Saúde. (2020) 16:333–47. doi: 10.14393/Hygeia16056140
27. Meneghel SN, Gomes Victora C, Xavier Faria NM, Alves de Carvalho L, Falk JW. Características epidemiológicas do suicídio no Rio Grande do Sul. Rev Saude Publica. (2004) 38:804–10. doi: 10.1590/S0034-89102004000600008
28. Cavalcante FG, Minayo MC de S, Mangas RM do N. Diferentes faces da depressão no suicídio em idosos. Cien Saude Colet. (2013) 18:2985–94. doi: 10.1590/S1413-81232013001000023
29. Marinho Alves AA, Rodrigues NFR. Determinantes sociais e económicos da Saúde Mental. Rev Port Saúde Pública. (2010) 28:127–31. doi: 10.1016/S0870-9025(10)70003-1
30. Ramm M, Jedamzik J, Lenz P, Jürgens L, Heuft G, Conrad R. Older adults coping with critical life events - results of the revised demoralization scale in a representative sample of older adulthood. Front Psychiatry. (2024) 15:1389021/full. doi: 10.3389/fpsyt.2024.1389021/full
31. De Oliveira LB, Rodrigues O IV de, Boágua JS da S, Gomes EP. Suicídio na terceira idade: fatores de risco e de proteção/Suicide in old age: risk and protective factors. Braz J Heal Rev. (2021) 4:8337–49. doi: 10.34119/bjhrv4n2-358
32. Fernandes-Eloi J, Costa Lourenço JR. Suicídio na Velhice – Um Estudo de Revisão Integrativa da Literatura. CES Psicol. (2019) 12:80–95. doi: 10.21615/cesp
33. Aleixo AG, Fasciani JS, Braga DDR, De Sousa FC, Vilela HR. Suicídio em idosos e a importância do fomento à saúde mental: uma revisão integrativa. Braz J Heal Rev. (2023) 6:24439–47. doi: 10.34119/bjhrv6n5-493
34. Associação Brasileira de Psiquiatria. Setembro Amarelo® começou: junte-se a nós na maior campanha antiestigma do mundo!. Associação Brasileira, suicídio em todo o país, Brasília, Brasil. (2022). Available at: https://www.abp.org.br/post/setembro-amarelo-comecou-junte-se-a-nos-na-maior-campanha-antiestigma-do-mundo.
35. Bezerra JDJ, Silva FVda. AS CORES DA VIDA: ESTRATÉGIAS BIOPOLÍTICAS NAS CAMPANHAS SETEMBRO AMARELO, OUTUBRO ROSA E NOVEMBRO AZUL. Miguilim - Rev Eletrônica do Netlli. (201) 8:728–41. doi: 10.47295/mgren.v8i2.1902
36. Centro De Valorização Da Vida (CVV). História do Setembro Amarelo (2016). Available online at: https://www.cvv.org.br/blog/setembro-amarelo-mes-de-prevencao-do-suicidio/.
37. de OMEC, Gomes KA de L, Nóbrega WFS, Gusmão ECR, Dos Santos RD, Franklin RG. Série temporal do suicídio no Brasil: o que mudou após o Setembro Amarelo? Rev Eletrônica Acervo Saúde. (2020) 48:e3191. doi: 10.25248/reas.e3191.2020
38. Lima DPA, Brandão CB. 5 anos de Campanha Setembro Amarelo: Estamos conseguindo prevenir suicídios? Res Soc Dev. (2021) 10:e16210716312. doi: 10.33448/rsd-v10i7.16312
39. Cruz WGN, Jesuino TA, Moreno HF, Santos LG, de Almeida AG. Analysis of the impact of the Brazilian suicide prevention campaign “Yellow September”: an ecological study. Trends Psychiatry Psychother. (2023) 3. doi: 10.47626/2237-6089-2022-0564
40. Lopes Silva Y, Avraham Ribas L, Rodrigues Neves T, Bardela de Oliveira J, De Matos Costa de Menezes M, Antonio Mendonça M. Setembro Amarelo: A campanha influencia no número de casos de auto-agressões no Rio de Janeiro? Rev Saúde. (2023) 14:34–8. doi: 10.21727/rs.v14i3.3465
41. Lopez Bernal J, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. (2016) 46(1):348–55. doi: 10.1093/ije/dyw098
42. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (2019). Available online at: https://icd.who.int/browse10/2019/en#/X60-X84.
43. Hofstra E, van Nieuwenhuizen C, Bakker M, Özgül D, Elfeddali I, de Jong SJ, et al. Effectiveness of suicide prevention interventions: A systematic review and meta-analysis. Gen Hosp Psychiatry. (2020) 63:127–40. doi: 10.1016/j.genhosppsych.2019.04.011
44. Platt S, Arensman E, Rezaeian M. National suicide prevention strategies – progress and challenges. Crisis. (2019) 40:75–82. doi: 10.1027/0227-5910/a000587
45. Bohanna I, Wang X. Media guidelines for the responsible reporting of suicide. Crisis. (2012) 33:190–8. doi: 10.1027/0227-5910/a000137
46. Niederkrotenthaler T, Reidenberg DJ, Till B, Gould MS. Increasing help-seeking and referrals for individuals at risk for suicide by decreasing stigma. Am J Prev Med. (2014) 47:S235–43. doi: 10.1016/j.amepre.2014.06.010
47. Associação Brasileira de Psiquiatria. Suicídio: informando para prevenir. (Brasília: Conselho Federal de Medicina (CFM)) (2014).
48. Domaradzki J. The werther effect, the papageno effect or no effect? A literature review. Int J Environ Res Public Health. (2021) 18:2396. doi: 10.3390/ijerph18052396
49. Tøllefsen IM, Hem E, Ekeberg Ø. The reliability of suicide statistics: a systematic review. BMC Psychiatry. (2012) 12:9. doi: 10.1186/1471-244X-12-9
50. O’Rourke MC, Jamil RT, Siddiqui W. Suicide Screening and Prevention. Treasure Island (FL: StatPearls Publishing (2019).
51. Jorge MHP de M, Laurenti R, Lima-Costa MF, Gotlieb SLD, Filho ADPC. A mortalidade de idosos no Brasil: a questão das causas mal definidas. Epidemiol e Serviços Saúde. (2008) 17(4):271–81. doi: 10.5123/S1679-49742008000400004
52. Vidal CEL, Gontijo ECDM, Lima LA. Tentativas de suicídio: fatores prognósticos e estimativa do excesso de mortalidade. Cad Saúde Pública Rio Janeiro. (2013) 29:175–87. doi: 10.1590/S0102-311X2013000100020
53. Crestani C, Masotti V, Corradi N, Schirripa ML, Cecchi R. Suicide in the elderly: a 37-years retrospective study. Acta Biomed. (2019) 90:68–76. doi: 10.23750/abm.v90i1.6312
54. Madej M, Pogorzelska M, Wróblewski K, Gaj M, Wichary A, Gnus J, et al. Suicide in the elderly-risk assessment and prevention. Challenges. (2020) 9:199–212.
55. Ding OJ, Kennedy GJ. Understanding vulnerability to late-life suicide. Curr Psychiatry Rep. (2021) 23:58. doi: 10.1007/s11920-021-01268-2
56. de Mendonça Lima CA, De Leo D, Ivbijaro G, Svab I. Loneliness and abuse as risk factors for suicide in older adults: new developments and the contribution of the WPA Section on Old Age Psychiatry. World Psychiatry. (2021) 20:455–6. doi: 10.1002/wps.20899
57. Gonçalves LRC, Gonçalves E, Oliveira Júnior LBde. Determinantes espaciais e socioeconômicos do suicídio no Brasil: uma abordagem regional. Nov Econ. (2011) 21:281–316. doi: 10.1590/S0103-63512011000200005
58. Evans-Lacko S, Henderson C, Thornicroft G. Public knowledge, attitudes and behaviour regarding people with mental illness in England 2009-2012. Br J Psychiatry. (2013) 202:s51–7. doi: 10.1192/bjp.bp.112.112979
59. Sousa RMA de C, Mendes GS, Carneiro GF da C, Oliveira GALde, Almeida MRGde. O processo de envelhecimento e sua relação com o suicídio na pessoa idosa: uma revisão bibliográfica. In: Serviço social: Aplicação da ciência e seus antagonismos. Ponta Grossa – PR, Brasil: Atena Editora (2021). p. 99–110. Available at: https://www.atenaeditora.com.br/post-ebook/4252.
60. Marquetti FR, Marquetti FC. Suicídio e feminilidades. Cad Pagu. (2017) 49. doi: 10.1590/18094449201700490021
61. Schrijvers DL, Bollen J, Sabbe BGC. The gender paradox in suicidal behavior and its impact on the suicidal process. J Affect Disord. (2012) 138:19–26. doi: 10.1016/j.jad.2011.03.050
62. Ciulla L, Lopes Nogueira E, da Silva Filho IG, Tres GL, Engroff P, Ciulla V, et al. Suicide risk in the elderly: Data from Brazilian public health care program. J Affect Disord. (2014) 152–154:513–6. doi: 10.1016/j.jad.2013.05.090
64. Mosqueiro BP, Caldieraro MA, Messinger M, da Costa FBP, Peteet JR, P Fleck M. Religiosity, spirituality, suicide risk and remission of depressive symptoms: a 6-month prospective study of tertiary care Brazilian patients. J Affect Disord. (2021) 279:434–42. doi: 10.1016/j.jad.2020.10.028
65. Moreira-Almeida A, Pinsky I, Zaleski M, Laranjeira R. Envolvimento religioso e fatores sociodemográficos: resultados de um levantamento nacional no Brasil. Arch Clin Psychiatry (São Paulo). (2010) 37:12–5. doi: 10.1590/S0101-60832010000100003
66. Edward R, Dana G. Religion and suicide: new findings. J Relig Health. (2018) 57:2478–99. doi: 10.1007/s10943-018-0629-8
67. Pargament KI, Lomax JW. Understanding and addressing religion among people with mental illness. World Psychiatry. (2013) 12:26–32. doi: 10.1002/wps.20005
68. Gureje O, Nortje G, Makanjuola V, Oladeji BD, Seedat S, Jenkins R. The role of global traditional and complementary systems of medicine in the treatment of mental health disorders. Lancet Psychiatry. (2015) 2:168–77. doi: 10.1016/S2215-0366(15)00013-9
69. Braam AW, Schrier AC, Tuinebreijer WC, Beekman ATF, Dekker JJM, de Wit MAS. Religious coping and depression in multicultural Amsterdam: A comparison between native Dutch citizens and Turkish, Moroccan and Surinamese/Antillean migrants. J Affect Disord. (2010) 125:269–78. doi: 10.1016/j.jad.2010.02.116
70. O’Brien B, Shrestha S, Stanley MA, Pargament KI, Cummings J, Kunik ME, et al. Positive and negative religious coping as predictors of distress among minority older adults. Int J Geriatr Psychiatry. (2019) 34:54–9. doi: 10.1002/gps.4983
71. Lucchetti A, Barcelos-Ferreira R, Blazer DG, Moreira-Almeida A. Spirituality in geriatric psychiatry. Curr Opin Psychiatry. (2018) 31:373–7. doi: 10.1097/YCO.0000000000000424
Keywords: suicide, suicide prevention, public health, aged, health campaign, public policy, mortality
Citation: Corrêa Matias Pereira C, Najafi Moghaddam Gilani V and Nazif-Munoz JI (2024) A brief research report of suicide rates in the Brazilian elderly over a 12-year period: the lack of association of the "Setembro Amarelo" campaign for suicide prevention. Front. Psychiatry 15:1354030. doi: 10.3389/fpsyt.2024.1354030
Received: 11 December 2023; Accepted: 11 July 2024;
Published: 25 July 2024.
Edited by:
Vincenzo De Luca, University of Toronto, CanadaReviewed by:
Xenia Gonda, Semmelweis University, HungaryCopyright © 2024 Corrêa Matias Pereira, Najafi Moghaddam Gilani and Nazif-Munoz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camila Corrêa Matias Pereira, Y2FtaWxhLmNvcnJlYS5tYXRpYXMucGVyZWlyYUB1c2hlcmJyb29rZS5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.