 Chloe Molnar1
Chloe Molnar1 Iva Strnadová2,3,4Manjekah Dunn1,5
Iva Strnadová2,3,4Manjekah Dunn1,5 Julie Loblinzk2,4Skie Sarfaraz4Yasmin Cathcart-King2Michelle Tso2Joanne Danker2Sarah Hayes2Sierra Angelina Willow2Jennifer Hansen2Tiffany Qing Lim2Jackie Boyle6Bronwyn Terrill7,8,9Jackie Leach Scully3
Julie Loblinzk2,4Skie Sarfaraz4Yasmin Cathcart-King2Michelle Tso2Joanne Danker2Sarah Hayes2Sierra Angelina Willow2Jennifer Hansen2Tiffany Qing Lim2Jackie Boyle6Bronwyn Terrill7,8,9Jackie Leach Scully3 Elizabeth Emma Palmer1,5*
Elizabeth Emma Palmer1,5*- 1Discipline of Paediatrics and Child Health, Faculty of Medicine and Health, University of New South Wales, Sydney, NSW, Australia
- 2School of Education, University of New South Wales, Sydney, NSW, Australia
- 3Disability Innovation Institute, University of New South Wales, Sydney, NSW, Australia
- 4Self-Advocacy Sydney Inc., Sydney, NSW, Australia
- 5Centre for Clinical Genetics, Sydney Children’s Hospitals Network, Sydney, NSW, Australia
- 6The New South Wales Genetics of Learning Disability (GOLD) Service, Waratah, NSW, Australia
- 7Australian Genomics, Melbourne, VIC, Australia
- 8Kinghorn Centre for Clinical Genomics, Garvan Institute of Medical Research, Darlinghurst, NSW, Australia
- 9School of Clinical Medicine, Faculty of Medicine and Health, University of New South Wales, Sydney, NSW, Australia
Introduction
According to the medical model, intellectual disability is a neurodevelopmental condition of childhood onset that presents with limitations in intellectual and adaptive functioning (1). However, as emphasised by Robert Strike, recipient of the Medal of the Order of Australia (OAM) and co-founder of Self Advocacy Sydney, an organisation that empowers people with intellectual disability to speak up for themselves, “Intellectual disability is not an inability to think!” (2, 3). Intellectual disability is also not an inability to feel and remember experiences, as evidenced by GeneEQUAL research (4). GeneEQUAL is an inclusive research program at the University of New South Wales, Sydney, that aims to improve genetic healthcare for people with intellectual disability (5).
Healthcare rights
There is growing emphasis on person-centred care that recognises an individual’s capability and potential to manage their own health and involves shared decision-making between patients and health professionals (6, 7). This can improve physical and psychological health outcomes and increase individuals’ skills and confidence in managing their own health (6). The United Nations (UN) Convention on the Rights of Persons with Disabilities (CRPD) states that people with disability should have “full and equal enjoyment of all human rights” without discrimination, including the right to the highest attainable standard of health, which includes person-centred care (Article 25) and equal access to medical facilities and information (Article 9) (8). Currently, 164 countries, including Australia, have signed the Convention (9), and some countries have additional legislation aiming to reduce stigma and discrimination in the healthcare setting (10–12). Examples include the Equality Act 2010 in the United Kingdom and the Disability Discrimination Act 1992 in Australia, both of which require healthcare professionals to make reasonable adjustments to improve accessibility (10, 12). Reasonable adjustments are changes that do not impose an undue burden but ensure that people are not disadvantaged or harmed (11, 13). They can include adapting communication to meet a person’s needs, providing information in alternative formats including Easy Read, and allowing extra time to share information and provide support (13).
Stigma and abuse in healthcare
People with intellectual disability continue to experience high levels of stigma, resulting in a denial of equal rights, psychological distress (14, 15), and a disproportionately high risk of physical, sexual, emotional, financial, and disability-related abuse (16, 17). This extends to healthcare settings, and GeneEQUAL co-researchers shared their adverse and often traumatic experiences of neglect and abuse, including not having the opportunity to make their own healthcare decisions, being ignored when they present with a support person, and feeling pressured to provide consent (18). In Australia, the 2023 Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (the Disability Royal Commission) found ongoing systemic neglect and abuse of people with intellectual disability within the health system (19). An additional study surveying over 600 intellectual disability experts and organisations across 88 countries showed that people with intellectual disability in low- and middle-income countries were often denied human rights and freedoms and experienced high levels of sigma (14), including in healthcare (20). People with intellectual disability mostly relied on family for support, and, in some countries, it was usual to segregate people with intellectual disability from society (14).
Stigma and trauma in healthcare are also directly associated with poor health outcomes (21, 22). During hospitalisation, people with intellectual disability commonly experience worse care (23) and have longer inpatient stays compared with the general population (24). The Australian Government’s National Roadmap for Improving the Health of People with Intellectual Disability highlighted that people with intellectual disability face barriers accessing safe and quality care, evidenced by significantly lower rates of preventative healthcare, including regular health checkups and screening for disease, more than double the rate of avoidable mortality, and twice the rate of emergency department and hospital admissions compared to the general population (25). This mirrors findings in other countries, for example, a Confidential Inquiry, commissioned by the Department of Health in England and conducted between 2010 and 2012 in England and Wales, concluded that there was a higher risk of avoidable deaths amongst people with intellectual disability that could be attributed to untreated illness and poor quality healthcare (26). There is also evidence that people with intellectual disability have less access to information and reduced awareness of their healthcare rights than people without intellectual disability (21). Moreover, such negative healthcare experiences can reduce patient expectations and engagement, further contributing to poor health outcomes and setting up a vicious cycle (27).
Factors contributing to stigma and abuse at a system level
At a system level, there is limited availability of accessible health information, such as Easy Read and multimodal health resources (including videos, booklets, and websites), and often poor access to alternative communication resources (including sign language interpreters and assistive communication aides) (21). A study looking at 32 consultations between people with intellectual disability and a primary care physician found that only six consultations included the use of Easy Read documents (28). In addition, non-inclusive clinical environments can form major barriers to equitable healthcare, including appointment times that are too short to allow for effective health communication and shared decision-making (29), unwelcoming hospital environments (19, 27), and inadequate integration of healthcare services and continuity of care (30).
Factors contributing to stigma and abuse at a clinician level
Limited knowledge amongst clinicians about the lived experiences of people with intellectual disability is a major barrier to the delivery of accessible, inclusive, and respectful healthcare (21, 31). A systematic review of 30 studies of various study design revealed that some health professionals considered people with intellectual disability to be unlike other patients and, at times, to be childlike, strange, or intimidating (31). People with intellectual disability also commonly reported experiencing stigma and discrimination from health professionals, including being made to feel inferior, pitied, or over-valorised for their disability (21). In Australia, public hearings held as part of the Disability Royal Commission found that some health professionals made assumptions about the quality of life of people with disability, which could restrict access to high quality healthcare services (19). In addition, because of poor understanding of underlying intellectual disability-related conditions, some health professionals assumed that new symptoms were related to a person’s intellectual disability rather than a new condition (i.e., diagnostic overshadowing), resulting in incorrect or delayed diagnoses and negatively impacting care received (19, 32).
Effective communication is vital for equitable care (27) and health literacy (21) but is often poor in consultations with people with intellectual disability (19, 30). Health professionals are generally unaware of communication challenges faced by people with intellectual disability and how best to modify communication approaches to support inclusion (27). As health professionals often rely on the family and/or support person, health information may not be adequately explained to the individual patient, reducing opportunities for empowerment and shared decision-making (27). This can lead to people with intellectual disability being ignored, contributing to feelings of stress and vulnerability, and this is an overt form of stigmatisation (24, 27). There is also a perception that health professionals may avoid direct communication with people with intellectual disability due to limited understanding of individual needs and the fear that it would entail additional workload, which they are reluctant to take on (24).
The need for improved clinician education
Minimal clinician knowledge reflects limited teaching about intellectual disability to health students and professionals (24, 32, 33). Australian medical curricula include little education about the healthcare needs of, and minimal exposure to, people with intellectual disability (33). There are also no mandatory training requirements for health professionals to improve their knowledge and skills when working with people with intellectual disability (32), and many health professionals are unaware of relevant legislation (24). Furthermore, a 2017 study of medical schools in the United States estimates that less than a quarter of all medical schools include a disability awareness program (34).
Well-designed educational programs have the potential to improve clinician capabilities, knowledge and skills in delivering accessible, person-centred, and respectful healthcare for people with intellectual disability (29). Effective clinical educational programs could, therefore, be a powerful way to reduce the stigma that people with intellectual disability currently face in the healthcare system (Figure 1) (29). The World Health Organisation Disability-Inclusive Health Services Toolkit recommends that education programs about disability and disability-inclusive healthcare are included in medical school curricula, are a requirement for accreditation, and are offered as training to health professionals (21). In addition, the UN policy guidelines included in a Sustainable Development Goals–CRPD resource package recommend that health professionals receive training to develop skills, improve attitudes, and learn about the rights of people with intellectual disability and how to provide reasonable adjustments (35). Increased knowledge can reduce stigma and allow health professionals to respond to the needs of people with intellectual disability (24), for example, by adapting the hospital environment (23), avoiding diagnostic overshadowing, and communicating effectively (21). Finally, in view of the recognised frequency of trauma and abuse experienced by people with intellectual disability (36), it is also critical that clinician education also incorporates how to deliver trauma-informed care (37).
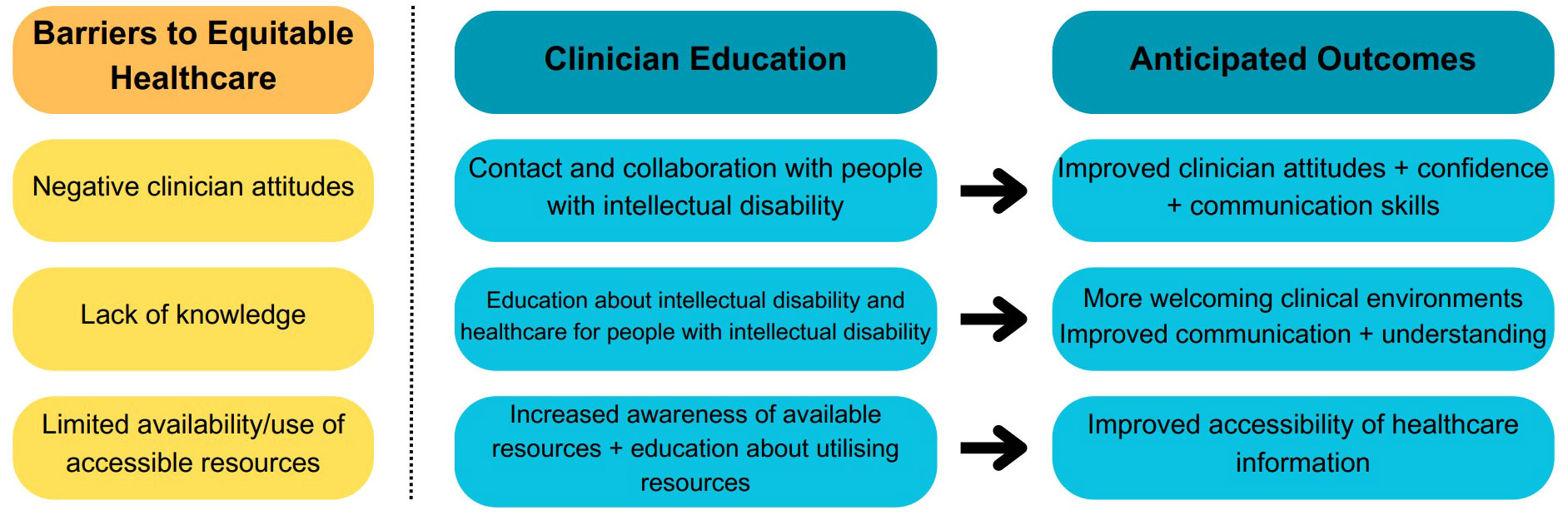
Figure 1 Summary of the impact of education on addressing barriers to equitable healthcare for people with intellectual disability. The arrow represents how aspects of clinician education programs might reduce healthcare barriers (created using https://www.canva.com/).
Co-production and co-education
The GeneEQUAL team wholeheartedly support the recommendation that educational programs should be co-produced and co-delivered with people with intellectual disability, as they are the experts in their own experiences (29, 38). Co-production involves collaboration between clinical educators and healthcare recipients, in this case, people with intellectual disability, to design and deliver educational programs (39) and to ensure that their opinions and preferences are incorporated (40). Involving people with intellectual disability in the design and delivery of content for medical students and health professionals has been demonstrated to bring transformative change to the individuals involved, as well as to health professionals and health systems (41). A global systematic review looking at patient engagement across all health services only found a small number of studies that involved patients in the co-production of educational programs (42). However, it was evident that co-production led to improved healthcare quality and outcomes and ultimately also improved health governance, policies, and organisational planning. Co-production has also been associated with improved attitudes towards and awareness of the needs of people with intellectual disability (31), improved communication skills (33), and the sharing of power between patients and health professionals (42). Finally, learning about people’s lived experiences is enhanced when it is presented by the people themselves (co-education) within a sociocultural framework, as opposed to a purely medicalised perspective (41). This is crucial to facilitate learning about the importance of reasonable adjustments and adapting health assessments and management practices (33). However, it is vital to ensure that co-production is well-planned to ensure that it is not tokenistic (42) and everyone involved feels supported, especially when sharing challenging personal experiences (38).
Our team has recently adopted this co-production approach in our design, delivery, and evaluation of the GeneEQUAL Toolkit, a collection of resources that aim to improve healthcare for people with intellectual disability. We followed the six key steps of co-production recommended by the guidelines Co-production in Action (43), and, therefore, people with intellectual disability were included in each step of the process from the initial project idea to reflecting on the co-production process (44). People with intellectual disability reflected on how their involvement in co-production not only resulted in better resources but also was a valuable experience for them and improved their knowledge of healthcare rights (44).
Conclusion
Despite existing legislation, there are still significant barriers and stigmatisation within the healthcare sector that limit the opportunities for people with intellectual disability to receive the highest standards of healthcare (19, 25). Co-production methodology has been used successfully, although, minimally, in the healthcare sector (42). As the GeneEQUAL team, we call for a greater emphasis on the co-production of new educational resources for health students and professionals to reduce stigmatisation and improve health outcomes for people with intellectual disability, in line with their human rights. This has the potential to facilitate a critically needed change in the model of healthcare, from one reinforcing power imbalance and trauma to an authentic partnership that is inclusive, person-centred, and respectful: indeed, a new model of co-healthcare.
Author contributions
CM: Conceptualization, Formal analysis, Project administration, Writing – original draft. IS: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. MD: Validation, Writing – review & editing. JL: Validation, Writing – review & editing. SS: Validation, Writing – review & editing. YC-K: Validation, Writing – review & editing. MT: Validation, Writing – review & editing. JD: Validation, Writing – review & editing. SH: Validation, Writing – review & editing. SW: Validation, Writing – review & editing. JH: Validation, Writing – review & editing. TL: Validation, Writing – review & editing. BT: Supervision, Validation, Writing – review & editing. JB: Validation, Writing – review & editing. JS: Supervision, Validation, Writing – review & editing. EP: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The GeneEQUAL team acknowledge the input of people with intellectual disability who have participated in focus groups and interviews to inform the vision and mission of our inclusive research group.
Conflict of interest
EP has received funding from the NHMRC and NSW Health. She is a clinical geneticist at Sydney Children’s Hospitals Network-Randwick and a member of the medical and scientific advisory committee for Rare Voices Australia, the national peak body for Australians living with a rare condition. IS has received funding from the NHMRC and the NSW Department of Health. She is also a Board member of Self Advocacy Sydney, an organisation run by and for people with intellectual disability. JS is Director of the Disability Innovation Institute, which has received funding from the NHMRC and the NSW Department of Health. JL, OAM has received funding from the NHMRC and the NSW Department of Health. She is also a Board member of Self Advocacy Sydney, an organisation run by and for people with intellectual disability. SS has received funding from the NHMRC and the NSW Department of Health. She is also an employee at Self-Advocacy Sydney, an organisation run by and for people with intellectual disability. JB and BT have received funding from the NHMRC.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1346423/full#supplementary-material
References
1. Neurodevelopmental Disorders. Diagnostic and Statistical Manual of Mental Disorders. Washington DC: DSM Library: American Psychiatric Association Publishing (2022).
2. Council for Intellectual Disability. About Us. (2022). Available at: https://cid.org.au/about-us/.
3. Self Advocacy Sydney. Robert Strike, AM. Available at: https://www.sasinc.com.au/about-us/executive-board/robert-strike/.
4. Strnadová I, Loblinzk J, Scully JL, Danker J, Tso M, Jackaman K-M, et al. “I am not a number!” Opinions and preferences of people with intellectual disability about genetic healthcare. Eur J Hum Genet (2023) 31:1057–65. doi: 10.1038/s41431-023-01282-3
5. GeneEQUAL. GeneEQUAL (2023). Available at: https://geneequal.com/.
6. Coulter A, Oldham J. Person-centred care: what is it and how do we get there? Future Healthcare J (2016) 3(2):114–6. doi: 10.7861/futurehosp.3-2-114
7. Fridberg H, Wallin L, Tistad M. Operationalisation of person-centred care in a real-world setting: a case study with six embedded units. BMC Health Serv Res (2022) 22(1):1160. doi: 10.1186/s12913-022-08516-y
8. United Nations. United Nations Convention on the Rights of Persons with Disability (2006). Available at: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/convention-on-the-rights-of-persons-with-disabilities-2.html.
9. United Nations. 15. Convention on the Rights of Persons with Disabilities (2023). Available at: https://treaties.un.org/pages/ViewDetails.aspx?chapter=4&clang=_en&mtdsg_no=IV-15&src=IND.
10. The UN Convention on the Rights of Persons with Disabilities. UK implementation: House of Commons Library (2022). Available at: https://researchbriefings.files.parliament.uk/documents/CBP-7367/CBP-7367.pdf.
11. Attorney-General’s Department. Rights of people with disability (2020). Available at: https://www.ag.gov.au/rights-and-protections/human-rights-and-anti-discrimination/human-rights-scrutiny/public-sector-guidance-sheets/rights-people-disability#what-are-rights-of-people-with-disability.
12. Australian Government. Disability Discrimination Act 1992 . Available at: https://www.legislation.gov.au/Details/C2016C00763#:~:text=This%20Act%20may%20be%20cited%20as%20the%20Disability%20Discrimination%20Act%201992.&text=(1)%20Sections%201%20and%202,to%20be%20fixed%20by%20Proclamation.
13. NSW Ministry of Health. Responding to Needs of People with Disability during Hospitalisation (2017). Available at: https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2017_001.pdf.
14. Scior K, Hamid A, Hastings R, Werner S, Belton C, Laniyan A, et al. Intellectual disability stigma and initiatives to challenge it and promote inclusion around the globe. J Policy Pract Intellectual Disabilities (2020) 17(2):165–75. doi: 10.1111/jppi.12330
15. Scior K. Toward Understanding Intellectual Disability Stigma: Introduction. In: Scior K, Werner S, editors. Intellectual Disability and Stigma: Stepping Out from the Margins. London: Palgrave Macmillan UK (2016). p. 3–13.
16. Hughes RB, Robinson-Whelen S, Raymaker D, Lund EM, Oschwald M, Katz M, et al. The relation of abuse to physical and psychological health in adults with developmental disabilities. Disability Health J (2019) 12(2):227–34. doi: 10.1016/j.dhjo.2018.09.007
17. Ditchman N, Kosyluk K, Lee E-J, Jones N. How Stigma Affects the Lives of People with Intellectual Disabilities: An Overview. In: Scior K, Werner S, editors. Intellectual Disability and Stigma: Stepping Out from the Margins. London: Palgrave Macmillan UK (2016). p. 31–47.
18. Dunn M, Strnadova I, Scully J, Hansen J, Loblinzk J, Sarafaraz S, et al. Exploring the Barriers and Enablers for the equitable and accessible informed healthcare consent process for people with intellectual disability: A systematic literature review. BMJ Qual Saf (2023). doi: 10.1101/2023.03.06.23286791
19. Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability; Interim Report 2020 . Available at: https://disability.royalcommission.gov.au/system/files/2020-10/Interim%20Report.pdf.
20. Hashemi G, Wickenden M, Bright T, Kuper H. Barriers to accessing primary healthcare services for people with disabilities in low and middle-income countries, a Meta-synthesis of qualitative studies. Disability Rehabil (2022) 44(8):1207–20. doi: 10.1080/09638288.2020.1817984
21. World Health Organisation. Regional Office for the Western Pacific. Disability-inclusive health services toolkit: a resource for health facilities in the Western Pacific Region Vol. 2020. Manila: WHO Regional Office for the Western Pacific (2020).
22. Pelleboer-Gunnink HA, van Oorsouw WMWJ, van Weeghel J, Embregts PJCM. Stigma research in the field of intellectual disabilities: a scoping review on the perspective of care providers. Int J Dev Disabilities (2021) 67(3):168–87. doi: 10.1080/20473869.2019.1616990
23. Mimmo L, Harrison R, Hinchcliff R. Patient safety vulnerabilities for children with intellectual disability in hospital: a systematic review and narrative synthesis. BMJ Paediatrics Open (2018) 2(1):e000201. doi: 10.1136/bmjpo-2017-000201
24. McCormick F, Marsh L, Taggart L, Brown M. Experiences of adults with intellectual disabilities accessing acute hospital services: A systematic review of the international evidence. Health Soc Care Community (2021) 29(5):1222–32. doi: 10.1111/hsc.13253
25. Department of Health. National Roadmap for Improving the Health of People with Intellectual Disability. Canberra: Australian Government (2021). Available at: https://www.health.gov.au/sites/default/files/documents/2021/08/national-roadmap-for-improving-the-health-of-people-with-intellectual-disability.pdf.
26. Heslop P, Blair PS, Fleming P, Hoghton M, Marriott A, Russ L. The Confidential Inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study. Lancet (2014) 383(9920):889–95. doi: 10.1016/S0140-6736(13)62026-7
27. Doherty AJ, Atherton H, Boland P, Hastings R, Hives L, Hood K, et al. Barriers and facilitators to primary health care for people with intellectual disabilities and/or autism: an integrative review. BJGP Open (2020) 4(3):1–10. doi: 10.3399/bjgpopen20X101030
28. Chinn D. An empirical examination of the use of Easy Read health information in health consultations involving patients with intellectual disabilities. J Appl Res Intellectual Disabilities (2020) 33(2):232–47. doi: 10.1111/jar.12657
29. Tracy J, McDonald R. Health and disability: partnerships in health care. J Appl Res Intellectual Disabilities (2015) 28(1):22–32. doi: 10.1111/jar.12135
30. Shea B, Bailie J, Dykgraaf SH, Fortune N, Lennox N, Bailie R. Access to general practice for people with intellectual disability in Australia: a systematic scoping review. BMC Primary Care (2022) 23(1):306. doi: 10.1186/s12875-022-01917-2
31. Pelleboer-Gunnink HA, Van Oorsouw WMWJ, Van Weeghel J, Embregts PJCM. Mainstream health professionals’ stigmatising attitudes towards people with intellectual disabilities: a systematic review. J Intellectual Disability Res (2017) 61(5):411–34. doi: 10.1111/jir.12353
32. Ong N, McCleod E, Nicholls LE, Fairbairn N, Tomsic G, Lord B, et al. Attitudes of healthcare staff in the treatment of children and adolescents with intellectual disability: A brief report. J Intellectual Dev Disability (2017) 42(3):295–300. doi: 10.3109/13668250.2016.1236368
33. Trollor JN, Eagleson C, Ruffell B, Tracy J, Torr JJ, Durvasula S, et al. Has teaching about intellectual disability healthcare in Australian medical schools improved? A 20-year comparison of curricula audits. BMC Med Education (2020) 20(1):321. doi: 10.1186/s12909-020-02235-w
34. Seidel E, Crowe S. The state of disability awareness in american medical schools. Am J Phys Med Rehabil (2017) 96(9):673–6. doi: 10.1097
35. Office of the United Nations High Commissioner for Human Rights. Policy Guidelines for Inclusive Sustainable Development Goals: Good Health and Well-being (2020). Available at: https://www.ohchr.org/sites/default/files/Documents/Issues/Disability/SDG-CRPD-Resource/policy-guideline-good-health.pdf.
36. McNally P, Taggart L, Shevlin M. Trauma experiences of people with an intellectual disability and their implications: A scoping review. J Appl Res Intellectual Disabilities (2021) 34(4):927–49. doi: 10.1111/jar.12872
37. Prevention & Response to Violence Abuse and Neglect (PARVAN). Integrated Trauma-Informed Care Framework: My story, my health, my future St Leonards, NSW2023 . Available at: https://www.health.nsw.gov.au/patients/trauma/Publications/itic-framework.pdf.
38. National Development Team for Inclusion. The Oliver McGowan Mandatory Training Evaluation: Learning about involvement of experts by experience in design and delivery of training (2022). Available at: https://www.hee.nhs.uk/sites/default/files/documents/Final%20Expert%20by%20experience%20final%20report%20-%20December%202022.pdf.
39. Agrawal S, Kalocsai C, Capponi P, Kidd S, Ringsted C, Wiljer D, et al. “It was great to break down the walls between patient and provider”: liminality in a co-produced advisory course for psychiatry residents. Adv Health Sci Education (2021) 26(2):385–403. doi: 10.1007/s10459-020-09991-w
40. Strnadová I, Nevin SM, Scully JL, Palmer EE. The opinions and experiences of people with intellectual disability regarding genetic testing and genetic medicine: A systematic review. Genet Med (2022) 24(3):535–48. doi: 10.1016/j.gim.2021.11.013
41. Vi L, Jiwa MI, Lunsky Y, Thakur A. A systematic review of intellectual and developmental disability curriculum in international pre-graduate health professional education. BMC Med Education (2023) 23(1):329. doi: 10.1186/s12909-023-04259-4
42. Bombard Y, Baker GR, Orlando E, Fancott C, Bhatia P, Casalino S, et al. Engaging patients to improve quality of care: a systematic review. Implementation Sci (2018) 13(1):98. doi: 10.1186/s13012-018-0784-z
43. Strnadová I, Dowse L, Garcia-Lee B. Doing Research Inclusively: Co-Production in Action. UNSW, Sydney: Disability Innovation Institute (2022).
44. GeneEQUAL. Our co-production videos (2023). Available at: https://geneequal.com/genetic-resources/our-co-production-videos/.
Keywords: intellectual disability, co-production, inclusion, healthcare for consistency, education
Citation: Molnar C, Strnadová I, Dunn M, Loblinzk J, Sarfaraz S, Cathcart-King Y, Tso M, Danker J, Hayes S, Willow SA, Hansen J, Lim TQ, Boyle J, Terrill B, Scully JL and Palmer EE (2024) The need for co-educators to drive a new model of inclusive, person-centred and respectful co-healthcare with people with intellectual disability. Front. Psychiatry 15:1346423. doi: 10.3389/fpsyt.2024.1346423
Received: 29 November 2023; Accepted: 29 January 2024;
Published: 13 February 2024.
Edited by:
Mustafa Salih, King Saud University, Saudi ArabiaReviewed by:
Joan Birnberg Beasley, University of New Hampshire, United StatesCopyright © 2024 Molnar, Strnadová, Dunn, Loblinzk, Sarfaraz, Cathcart-King, Tso, Danker, Hayes, Willow, Hansen, Lim, Boyle, Terrill, Scully and Palmer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elizabeth Emma Palmer, ZWxpemFiZXRoLnBhbG1lckB1bnN3LmVkdS5hdQ==