 Jose Monzon1,2
Jose Monzon1,2 Joaquin Barnoya2,3*
Joaquin Barnoya2,3* Sophia Mus2Gustavo Davila2Desirée Vidaña-Pérez4James F. Thrasher4,5
Sophia Mus2Gustavo Davila2Desirée Vidaña-Pérez4James F. Thrasher4,5- 1Health Sciences School, Rafael Landívar University, Guatemala City, Guatemala
- 2Research Department, Cardiovascular Surgery Unit of Guatemala (UNICAR), Guatemala City, Guatemala
- 3Research Department, Integra Cancer Institute, Guatemala City, Guatemala
- 4Department of Health Promotion, Education, and Behavior, Arnold School of Public Health, University of South Carolina, Columbia, SC, United States
- 5Center for Population Health Research, National Institute of Public Health (Mexico), Cuernavaca, Mexico
Objectives: Due to the COVID-19 pandemic, on March 16th, schools had to be closed in Guatemala and went to online teaching. We sought to analyze the change in substance use among high school students in Guatemala associated with the lockdown.
Methods: Data from two surveys (2019, n=2096, and 2020, n=1606) of a student cohort in private high schools in Guatemala City was used. Logistic models for past 30-day cigarette, e-cigarette, marijuana, and alcohol (including binge drinking) were used, regressing these on survey wave, while adjusting for sex, scholastic performance, high school year of student, parental education, substance use, and household member tobacco use.
Results: Prevalence declined for smoking (10% to 3%, p<0.001), e-cigarette (31% to 14%, p<0.001), marijuana (4.3% to 1.9%, p<0.001), and alcohol use (47% to 38.5%, p<0.001), and binge drinking (24% to 13%, p<0.001). Adjusted models showed wave 2 associated with lower odds of using cigarettes (AOR=0.44, 95%CI=0.32-0.62), e-cigarettes (AOR=0.41, 95% CI=0.35-0.49, p<0.001), and binge drinking (AOR=0.73, 95%CI=0.59-0.89; p=0.002)
Conclusion: Among Guatemalan adolescents, COVID-19 restrictions were associated with a significant decrease in smoking, e-cigarette use, and binge drinking.
Introduction
Adolescence is a critical development stage of life that is accompanied by physical, cognitive, emotional, social, and behavioral changes (1). It is the peak time for substance use initiation, including smoking, alcohol, and other illicit drugs (2). Substance use might disrupt cognitive and emotional development and can also lead to substance use disorders, dependence, and poorer physical and mental health (1, 3) and has been reported as a leading risk factor for premature death globally (4). Substance use prevalence varies across the globe, for example, people from low-and middle-income countries (LMICs) as defined by the World Bank (5), were reported to have higher smoking prevalence than those in high-income countries (HIC) (6) due, in part, because of the rapid pace of globalization which facilitated the expansion of tobacco markets across borders (7, 8).
Electronic Nicotine Delivery Systems (ENDS) were first introduced in the market in 2007 (9, 10) and first documented in Guatemala in 2014 (11, 12) and now include Heated Tobacco Products (HTPs). Since then, consumption has increased, particularly in HIC. In the U.S., for example, e-cigarette use has been the most commonly used tobacco product among youths since 2014, and in 2020, 13.1% of middle and high school students were current users with 80% of them using flavored e-cigarettes (13). This increase is consistent with other countries as well (14–19) and in LMICs and upper-middle-income countries, like Guatemala (20). Even though Guatemala signed and ratified the Framework Convention on Tobacco Control (FCTC) (21), it lacks strong tobacco control strategies and ENDS remain unregulated. In 2014, 15.7% of adolescents were smoking compared to 5.6% using e-cigarettes (22). However, in 2019, we found a 27.7% e-cigarette and 8.7% cigarette use prevalence among adolescents (23). Therefore, it appears that consumption patterns shifted towards e-cigarettes in Guatemala City over time.
In March 2020, the World Health Organization (WHO) declared a pandemic the COVID-19 outbreak caused by the novel SARS-CoV-2 virus (24). To curb the pandemic countries (including Guatemala) implemented lockdowns (25), curfews (26), and school and workplace closures, among other non-pharmacological measures (27, 28). These measures also led to adolescent substance use (29, 30), including tobacco (31, 32), psychological distress (33–35), and economic impact (36, 37). Data on changes in adolescent substance use is for the most part from high-income countries (3, 13, 29, 38–41) and suggests a change and particularly a decline in smoking prevalence use during the pandemic (3, 38, 41–43). Possible explanations for this decrease include fewer interactions with peers, social gatherings, and access to retailers and advertising exposure. In addition, increased parental supervision and fear of COVID-19 are likely to play a role in decreasing smoking prevalence (38, 39, 42, 44).
In Guatemala, since the first COVID-19 case was detected in March of 2020, curfews, lockdowns, and building occupancy restrictions based on epidemiological indicators (45, 46) were implemented (47, 48). Schools were shut down on March 22nd, 2020, and turned to a fully virtual mode throughout that year until 2021. Regarding tobacco control, Guatemala has only a weakly enforced smoke-free environment law and consequently a frail tobacco control program (49). In addition, e-cigarettes are readily available and heavily advertised at the point of sale (50). Therefore, we sought to assess whether the COVID-19 school shutdown influenced adolescent cigarette, e-cigarette, marijuana, and alcohol (including binge drinking) use in a sample of high school students in Guatemala City.
Methods
We analysed data from an ongoing, open cohort of students attending private schools in Guatemala City (51). Paper surveys were conducted in person from May to September 2019 (wave 1) and online from June to November 2020 (wave 2). Of the 2666 students, 1036 students were surveyed at both waves, and 1630 were surveyed once, due to maturation (out of and into high school) or absence during survey administration (n=3702 observations including those surveyed 2 times plus those surveyed only once). Passive parental consent was obtained by asking parents to respond to a consent letter only if they wished their kid to be removed from the study. After that, students provided active assent as described elsewhere (23, 52). Study protocols and data collection instruments were approved by the Institutional Review Board of Central America and Panama Nutrition Institute (INCAP).
The questionnaire focused on smoking and e-cigarette use and their risk factors, including alcohol and marijuana use. It was adapted from the Population Assessment of Tobacco and Health (PATH) study (53) and previously implemented in Mexico (54) and Guatemala (23). Current use was defined as using any product (cigarettes, e-cigarettes, marijuana, and alcohol) in the past 30 days. Participants were asked about their marijuana used as “during the past 12 months, have you smoked marijuana?” For the analysis, it was coded as a dichotomic variable (yes/no). We assessed binge drinking by asking “Have you ever had about 4 or more drinks on one occasion over the prior 30 days?”. They also reported on smoking and vaping among household members and their five closest friends dichotomized variables as follows: (1) At least one household member smokes; (2) at least one household member uses e-cigarettes; (3) at least one friend smokes; (4) at least one friend uses e-cigarettes. Sociodemographic variables included gender, grade (7th to 11th), scholastic performance (from 1-100), and parental highest educational attainment (None, middle school and high school, some college and bachelor’s degree or more).
For the descriptive analysis, we compared sample characteristics across survey waves using omnibus chi-square statistics. We used logistic Generalized Estimating Equations (GEE) to estimate the influence of the COVID-19 lockdown over the use of cigarettes, e-cigarettes, marijuana, alcohol, and binge drinking. Models were adjusted for repeated measures and clustered within individuals using an exchangeable correlation structure. Models were adjusted for school performance, friends, and household member smoking and/or vaping, and sociodemographic characteristics. In total, we fitted 5 logistic GEE, one for each outcome assessed, all models were also adjusted for the use of the other substances that were not modeled as the outcome. All analyses were conducted in Stata version 17 (StataCorp LLC, College Station, Texas).
Results
The response rate was 87% for wave 1 and 70% for wave 2. When comparing both waves (Table 1), there was a decrease in the reported prevalence of smoking (10% to 3%, p<0.001), e-cigarette (31% to 14%, p<0.001), marijuana (4.3% to 1.9%, p<0.001), alcohol use (47% to 38.5%, p<0.001), and binge drinking (24% to 13%, p<0.001). There was also a decrease in the friends and household members reported smoking (59% to 47% and 46% to 37%, respectively) and vaping (67% to 59%, and 24% to 18%, respectively) (Table 1).
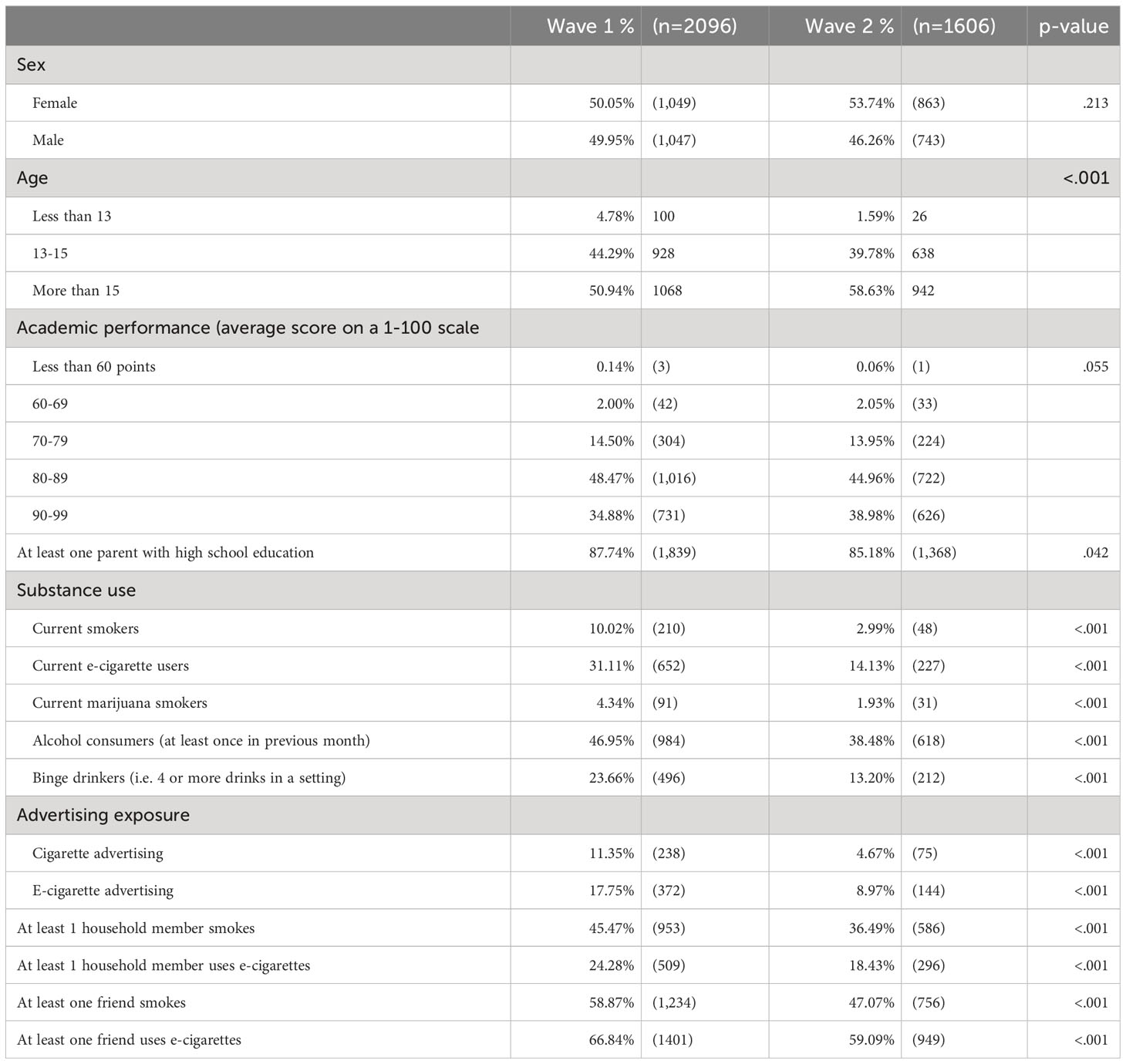
Table 1 Demographic characteristics and substance use in Wave 1 and Wave 2 of adolescents’ cohort in Guatemala City.
Table 2 shows the results of the adjusted logistic regression models showing the odds ratios of past 30-day substance use among adolescents. Wave 2 was associated with lower odds of reported smoking (AOR=0.44, 0.32-0.62; p=<.001), e-cigarette use (AOR=0.41, 95% CI=0.35-0.49; p=<.001), and binge drinking (AOR=0.73, 95% CI=0.60-0.89; p=.002). However, time-related differences in the use of marijuana (AOR 0.72, CI=0.47-1.1) and alcohol (AOR=0.91, CI=0.79-1.05) were no longer statistically significant after adjustment.
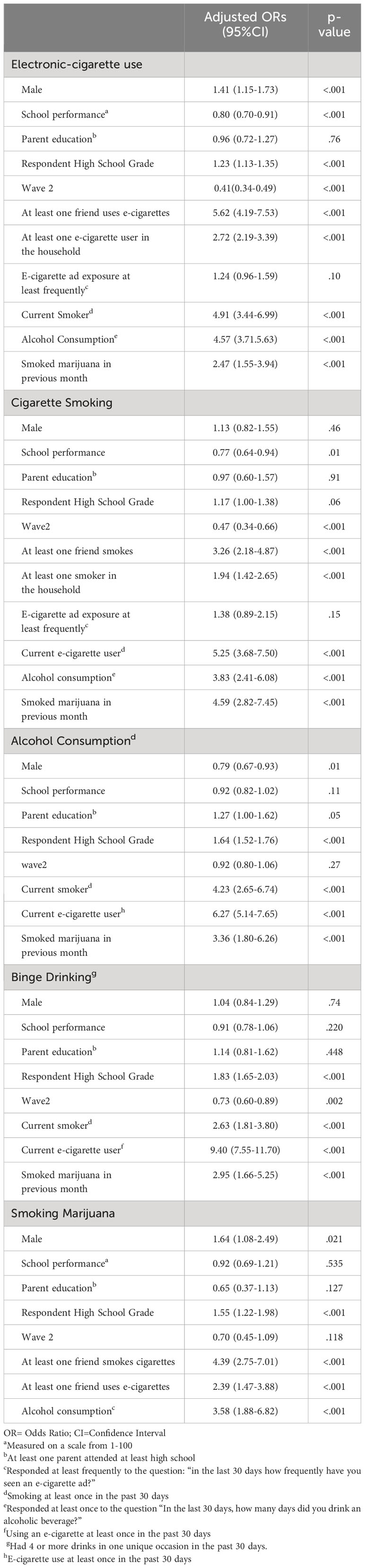
Table 2 Adjusted Odd Ratios of past 30-day substance among adolescents.
Discussion
To our knowledge, this is the first study assessing adolescent substance use before and during the COVID-19 restrictions in an upper-middle-income country in Latin America. We found that the reported smoking, vaping, marijuana and alcohol use, and binge drinking significantly decreased during COVID-19 restrictions. These declines remained significant in the adjusted models for all substances except alcohol and marijuana use. Although reports in other countries show mixed results (3, 41, 55–58), the US the National Survey on Drug Use and Health (NSDUH) did show a consistent decrease in adolescent substance use right before and after the COVID-19 restrictions (59). Similarly, in Ontario, Canada, data among 14-18-year-old adolescents before and after the emergency stay-at-home order in Ontario, yield a significant decrease (approximately 5%) in substance use after the shutdown (except for alcohol) (3). Even though these findings agree with what we found, these countries have significantly different tobacco control environments compared to Guatemala.
We also found that the reported friends’ and household members' substance use was significantly associated with teenagers' substance use, and they all significantly decreased in wave 2 (Table 1). This may be associated with a change in substance use during COVID-19 restrictions and is consistent with studies that suggest social networking as a significant means for initiation and continuation of substance use (60, 61) and particularly e-cigarettes. It also supports the idea that ENDS are generally obtained through peer networks and not from family members or direct purchasing as suggested elsewhere (62, 63).
The report of cigarette and e-cigarette use significantly declined in our sample, this makes sense during the lockdowns given that adolescent substance use is a highly social behaviour (57) and is consistent with another publication from Guatemala (64) a Canadian study in teens who provided information 3 weeks before and 3 weeks after the start of the COVID-19 lockdown (3).
Regarding alcohol use, binge drinking, and marijuana use, we also found a consistent decrease although in the adjusted models binge drinking decrease was not statistically significant. Other studies show mixed results, for instance, the Canadian study reported that fewer teens reported drinking, or using marijuana, however, alcohol use remained unchanged (3). Interestingly, among teens who did use substances, the mean number of days they used alcohol (0.76-0.96) and marijuana (0.94-1.1 days) were significantly higher after COVID-19 compared with before (3). Finally, another study among 12th graders reported that adolescent marijuana and alcohol use had no significant changes during the pandemic despite decreases in the substances' perceived availability (55).
These mixed results underscore the importance of fully characterizing the effects of the pandemic on adolescent substance use patterns in the context of well-known risk factors for substance use such as drug availability, association with peers who use drugs, a lack of parental supervision, boredom, and coping with negative affect (44, 57) and be better prepared to address them.
Possible reasons that could explain our findings include that societal restrictions during the pandemic may have contributed to a decrease in the time youth spent with their peers, which ultimately has an impact on adolescent substance use though studies on this effect were done before the pandemic (65, 66). Another study suggested decreased commercial availability and access to vape devices which may be associated with decreased rates of vaping (39). Other studies however, attribute the increased amount of time spent within the household as a risk factor for familiar substance use exposure (67). These findings warrant future research on how significant policy changes affecting social behaviour (i.e. lockdowns) can affect substance use while also pointing to the fact that different substances may respond to its various determinants in a particular way and thus public policies will not function as a “one size fits all” for each substance.
Limitations
This study should be interpreted considering some limitations. First, data from both waves is self-reported. However, this method has proved to be reliable to assess substance use in adolescents (68) and therefore internal validity should not be a source of bias. Also, we have reports that in 2019 and 2020, the Centers for Disease Control in the United States reported various outbreaks of Lung Injury Associated with the Use of E-cigarettes (EVALI), and thus we need to considerate that this could have also affected the e-cigarette use in adolescents in our sample, however, no reports of EVALI cases in Guatemala have been documented.
Furthermore, we changed survey implementation across waves, from in-person to online self-administration due to COVID-19 restrictions. It is yet unclear whether any resulting bias would have under- or over-estimated the changes we found. Finally, cigarettes and e-cigarettes utilize high-income status and exclusivity as part of its advertising and people with low-income status are less likely to afford these products and given that our sample was drawn from private schools in Guatemala City, our results might not be generalizable to public schools, lower-income status populations and rural Guatemala. Regardless, our findings provide evidence of the potential impact that the COVID-19 pandemic had in the substance use from our sample.
Conclusion
Our results suggest that during the COVID-19 restrictions, substance use among Guatemalan adolescents declined, as well as smoking and e-cigarette use among peers and household members. However, declines in marijuana use and alcohol consumption appear independent of these influences and merit further investigation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comite de Etica Instituto de Nutricion de Centroamerica y Panama. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
JM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. JB: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. SM: Conceptualization, Investigation, Writing – review & editing. GD: Conceptualization, Writing – review & editing. DV: Data curation, Formal analysis, Writing – review & editing. JT: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. National Institutes of Health grant number 3R01TW010652-04S1.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gray KM, Squeglia LM. Research Review: What have we learned about adolescent substance use? J Child Psychol Psychiatry (2018) 59(6):618–27. doi: 10.1111/jcpp.12783
2. Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. Lancet Psychiatry (2016) 3(3):251–64. doi: 10.1016/S2215-0366(15)00508-8
3. Dumas TM, Ellis W, Litt DM. What does adolescent substance use look like during the COVID-19 pandemic? Examining changes in frequency, social contexts, and pandemic-related predictors. J Adolesc Heal Off Publ Soc Adolesc Med (2020) 67(3):354–61. doi: 10.1016/j.jadohealth.2020.06.018
4. Ozeylem F, de la Torre-Luque A, Essau CA. Factors related to substance use among adolescents from six low-and middle-income countries. Addict Behav Rep (2021) 14:100370. doi: 10.1016/j.abrep.2021.100370
5. Prydz EB. Classifying countries by income. Washington D.C. USA: The World Bank (2019). Available at: https://datatopics.worldbank.org/world-development-indicators/stories/the-classification-of-countries-by-income.html.
6. World Bank. Tobacco Tax Reform at the Crossroads of Health and Development: A multisectoral Perspective. Washington, D.C: World Bank Group Publications (2017). Available at: http://hdl.handle.net/10986/28494.
7. World Health Organization. WHO global report on trends in prevalence of tobacco use 2000-2025 (2021). Available at: https://www.who.int/publications/i/item/9789240039322.
8. Glynn T, Seffrin JR, Brawley O, Grey N, Ross H. The globalization of tobacco use: 21 challenges for the 21st century. CA A Cancer J Clin (2010) 60:50–61. doi: 10.3322/caac.20052
9. Regan AK, Promoff G, Dube SR, Arrazola R. Electronic nicotine delivery systems: adult use and awareness of the “e-cigarette” in the USA. Tob Control (2013) 22(1):19–23. doi: 10.1136/tobaccocontrol-2011-050044
10. Sleight V. A brief history of the electronic cigarette. J Lung Pulm Respir Res (2016) 3(5):135–6. doi: 10.15406/jlprr.2016.03.00097
11. Arriaza A. Características, patrón y razón de uso de los cigarrlos electrónicos en Guatemala, amenaza para el control del tabaco. Guatemala City, Guatemala: Universidad Rafael Landivar (2016). Available at: http://recursosbiblio.url.edu.gt/tesiseortiz/2016/09/11/Arriaza-Astrid.pdf.
12. Chacon V, Arriaza A, Cavazos-Rehg P, Barnoya J. Availability, price, and packaging of electronic cigarettes and E-liquids in Guatemala City retailers. Nicotine Tob Res (2018) 20(2):253–7. doi: 10.1093/ntr/ntx071
13. Gentzke A, Wang T, Jamal A. Tobacco product use among middle and high school students - United States. Morb Mortal Wkly Rep (2020) 69:1881–8. doi: 10.15585/mmwr.mm6950a1
14. Pepper JK, Brewer NT. Electronic nicotine delivery system (electronic cigarette) awareness, use, reactions and beliefs: a systematic review. Tob Control (2014) 23(5):375–84. doi: 10.1136/tobaccocontrol-2013-051122
15. Miech R, Johnston L, O’Malley PM, Bachman JG, Patrick ME. Adolescent vaping and nicotine use in 2017–2018 — U.S. National estimates. N Engl J Med (2019) 380(2):192–3. doi: 10.1056/NEJMc1814130
16. Arrazola RA, Singh T, Corey CG, Husten CG, Neff LJ, Apelberg BJ, et al. Tobacco use among middle and high school students - United States, 2011-2014. MMWR Morb Mortal Wkly Rep (2015) 64(14):381–5.
17. Kang H, Cho S. Heated tobacco product use among Korean adolescents. Tob Control (2019) 29(4):466–8. doi: 10.1136/tobaccocontrol-2019-054949
18. Bialous SA, Glantz SA. Heated tobacco products: another tobacco industry global strategy to slow progress in tobacco control. Tob Control (2018) 27(Suppl 1):s111 LP–s117. doi: 10.1136/tobaccocontrol-2018-054340
19. Breland A, Soule E, Lopez A, Ramôa C, El-Hellani A, Eissenberg T. Electronic cigarettes: what are they and what do they do? Ann N Y Acad Sci (2017) 1394(1):5–30. doi: 10.1111/nyas.12977
20. World Health Organization. Tobacco fact Sheet (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/tobacco.
21. World Health Organization. WHO Framework Convention on Tobacco Control. Parties´ report (2005). Available at: https://www.who.int/fctc/reporting/party_reports/gtm/en/.
22. World Health Organization. Global Youth Tobacco Survey Guatemala Fact sheet. Geneva, Switzerland: World Health Organization (2015).
23. Gottshclich A, Mus S, Monzon JC, Thrasher JF, Barnoya J. A cross-sectional study on the awareness, susceptibility, and use of heated tobacco products among adolescents in Guatemala City, Guatemala. BMJ Open (2020) 10(12):e039792.
24. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed (2020) 91(1):157–60. doi: 10.23750/abm.v91i1.9397
25. Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci Prog (2021) 104(2):3685042110198. doi: 10.1177/00368504211019854
26. Dimeglio C, Miedougé M, Loubes J-M, Mansuy J-M, Izopet J. Side effect of a 6 p.m curfew for preventing the spread of SARS-CoV-2: A modeling study from Toulouse, France. J Infect (2021) 82(5):186–230. doi: 10.1016/j.jinf.2021.01.021
27. Brauner JM, Mindermann S, Sharma M, Johnston D, Salvatier J, Gavenčiak T, et al. Inferring the effectiveness of government interventions against COVID-19. Science (80-) (2021) 371(6531):eabd9338. doi: 10.1126/science.abd9338
28. Liu Y, Morgenstern C, Kelly J, Lowe R, Munday J, Villabona-Arenas CJ, et al. The impact of non-pharmaceutical interventions on SARS-CoV-2 transmission across 130 countries and territories. BMC Med (2021) 19(1):40. doi: 10.1186/s12916-020-01872-8
29. Dodge KA, Skinner AT, Godwin J, Bai Y, Lansford JE, Copeland WE, et al. Impact of the COVID-19 pandemic on substance use among adults without children, parents, and adolescents. Addict Behav Rep (2021) 14:100388. doi: 10.1016/j.abrep.2021.100388
30. Sen LT, Siste K, Hanafi E, Murtani BJ, Christian H, Limawan AP, et al. Insights into adolescents’ Substance use in a low–middle-income country during the COVID-19 pandemic. Front Psychiatry (2021) 12:739698. doi: 10.3389/fpsyt.2021.739698
31. Gendall P, Hoek J, Stanley J, Jenkins M, Every-Palmer S. Changes in tobacco use during the 2020 COVID-19 lockdown in New Zealand. Nicotine Tob Res Off J Soc Res Nicotine Tob (2021) 23(5):866–71. doi: 10.1093/ntr/ntaa257
32. Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic — United states, june 24–30, 2020. MMWR Morb Mortal Wkly Rep (2020) 69(32):1049–57. doi: 10.15585/mmwr.mm6932a1
33. Zhang C, Ye M, Fu Y, Yang M, Luo F, Yuan J, et al. The psychological impact of the COVID-19 pandemic on teenagers in China. J Adolesc Heal Off Publ Soc Adolesc Med (2020) 67(6):747–55. doi: 10.1016/j.jadohealth.2020.08.026
34. Jones EAK, Mitra AK, Bhuiyan AR. Impact of COVID-19 on mental health in adolescents: A systematic review. Int J Environ Res Public Health (2021) 18(5):2470. doi: 10.3390/ijerph18052470
35. Every-Palmer S, Jenkins M, Gendall P, Hoek J, Beaglehole B, Bell C, et al. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PloS One (2020) 15(11):e0241658. doi: 10.1371/journal.pone.0241658
36. Chen S, Igan D, Pierri N, Presbitero A. Tracking the economic Impact of COVID-19 and Mitigation Policies in Europe and the United States (2020). Available at: https://www.imf.org/en/Publications/WP/Issues/2020/07/10/Tracking-the-Economic-Impact-of-COVID-19-and-Mitigation-Policies-in-Europe-and-the-United-49553.
37. Oruc BE, Baxter A, Keskinocak P, Asplund J, Serban N. Homebound by COVID19: the benefits and consequences of non-pharmaceutical intervention strategies. BMC Public Health (2021) 21(1):655. doi: 10.1186/s12889-021-10725-9
38. Chaffee BW, Cheng J, Couch ET, Hoeft KS, Halpern-Felsher B. Adolescents’ Substance use and physical activity before and during the COVID-19 pandemic. JAMA Pediatr (2021) 175(7):715–22. doi: 10.1001/jamapediatrics.2021.0541
39. Gaiha SM, Lempert LK, Halpern-Felsher B. Underage youth and young adult e-cigarette use and access before and during the coronavirus disease 2019 pandemic. JAMA Netw Open (2020) 3(12):e2027572–e2027572. doi: 10.1001/jamanetworkopen.2020.27572
40. Morello P, Pérez A, Peña L, Lozano P, Thrasher J, Sargent JD, et al. Prevalence and predictors of e-cigarette trial among adolescents in Argentina. Tob Prev Cessat (2016) 2:2–13. doi: 10.18332/tpc/66950
41. Pelham WE 3rd, Tapert SF, Gonzalez MR, McCabe CJ, Lisdahl KM, Alzueta E, et al. Early adolescent substance use before and during the COVID-19 pandemic: A longitudinal survey in the ABCD study cohort. J Adolesc Heal Off Publ Soc Adolesc Med (2021) 69(3):390–7. doi: 10.1016/j.jadohealth.2021.06.015
42. Stokes AC. Declines in electronic cigarette use among US youth in the era of COVID-19—A critical opportunity to stop youth vaping in its tracks. JAMA Netw Open (2020) 3(12):e2028221–e2028221. doi: 10.1001/jamanetworkopen.2020.28221
43. Kreslake JM, Simard BJ, O’Connor KM, Patel M, Vallone DM, Hair EC. E-cigarette use among youths and young adults during the COVID-19 pandemic: United States, 2020. Am J Public Health (2021) 111(6):1132–40. doi: 10.2105/AJPH.2021.306210
44. Richter L. The effects of the COVID-19 pandemic on the risk of youth substance use. J Adolesc Heal (2020) 67(4):467–8. doi: 10.1016/j.jadohealth.2020.07.014
45. Ministerio de Salud Publica y Asistencia Social. Alertas sanitarias Covid-19: MSPAS actualiza disposiciones para establecimientos (2020). Available at: https://www.mspas.gob.gt/noticias/noticias-ultimas/5-noticias-mspas/1079-alertas-sanitarias-covid-19-mspas-actualiza-disposiciones-para-establecimientos.html.
46. Gobierno de Guatemala. Tablero de Alertas Sanitarias de COVID-19 Guatemala (2020). Available at: https://covid19.gob.gt/semaforo.html.
47. Ministerio de Salud Publica y Asistencia Social. Acuerdo Ministerial Numero 146-2020. Estrategia Nacional de Control de la Epidemia De SARS-COV-2 Y Bases Para la Desescalada De Las Medidas De Reapertura. Guatemala City: Ministerio de Salud Publica y Asistencia Social Guatemala (2020). Available at: https://www.mspas.gob.gt/component/jdownloads/category/652-idioma-espanol.html?Itemid=-1.
48. Ministerio de Salud Publica y Asistencia Social. Acuerdo Ministerial Numero 300-2020. Norma Sanitaria Para la Prevencion y Control de Infecciones Por SARS-COV-2 Y Otras Epidemias Para Los Centros del Sistema Educativo Nacional. Guatemala City: Ministerio de Salud Publica y Asistencia Social Guatemala (2020). Available at: https://www.mspas.gob.gt/component/jdownloads/category/862-acuerdo-ministerial-no-300-2020.html?Itemid=-1.
49. Barnoya J, Monzon JC, Briz P, Navas-Acien A. Compliance to the smoke-free law in Guatemala 5-years after implementation. BMC Public Health (2016) 16(1):1–5. doi: 10.1186/s12889-016-2960-x
50. Barnoya J, Monzon D, Pinetta J, Grilo G, Cohen JE. New tobacco products, old advertising strategies: point-of-sale advertising in Guatemala. Tob Control (2021) 30(5):591–93. doi: 10.1136/tobaccocontrol-2020-055681
51. National Institutes of Health. Electronic cigarettes in Latin America: Evaluation o impacts and policy options. Maryland, USA: Grantome (2018). Available at: https://grantome.com/grant/NIH/R01-TW010652-01.
52. Monzón J, Islam F, Mus S, Thrasher JF, Barnoya J. Effects of tobacco product type and characteristics on appeal and perceived harm: Results from a discrete choice experiment among Guatemalan adolescents. Prev Med (Baltim) (2021) 148:106590. doi: 10.1016/j.ypmed.2021.106590
53. Hyland A, Ambrose BK, Conway KP, Borek N, Lambert E, Carusi C, et al. Design and methods of the population assessment of tobacco and health (PATH) study. Tob Control (2017) 26(4):371–8. doi: 10.1136/tobaccocontrol-2016-052934
54. Thrasher J, Abad-Vivero EN, Barrientos-Gutíerrez I, Pérez-Hernández R, Reynales-Shigematsu LM, Mejía R, et al. Prevalence and correlates of E-cigarette perceptions and trial among early adolescents in Mexico. J Adolesc Heal (2016) 58(3):358–65. doi: 10.1016/j.jadohealth.2015.11.008
55. Miech R, Patrick ME, Keyes K, O’Malley PM, Johnston L. Adolescent drug use before and during U.S. national COVID-19 social distancing policies. Drug Alcohol Depend (2021) 226:108822. doi: 10.1016/j.drugalcdep.2021.108822
56. Rogés J, Bosque-Prous M, Colom J, Folch C, Barón-Garcia T, González-Casals H, et al. Consumption of Alcohol, Cannabis, and Tobacco in a Cohort of Adolescents before and during COVID-19 Confinement. Int J Environ Res Public Health (2021) 18(15):1–14. doi: 10.3390/ijerph18157849
57. Lundahl LH, Cannoy C. COVID-19 and substance use in adolescents. Pediatr Clin North Am (2021) 68(5):977–90. doi: 10.1016/j.pcl.2021.05.005
58. Hawke LD, Barbic SP, Voineskos A, Szatmari P, Cleverley K, Hayes E, et al. Impacts of COVID-19 on Youth Mental Health, Substance Use, and Well-being: A Rapid Survey of Clinical and Community Samples: Répercussions de la COVID-19 sur la santé mentale, l’utilisation de substances et le bien-être des adolescents: un sondage rapide. Can J Psychiatry (2020) 65(10):701–9. doi: 10.1177/0706743720940562
59. Center for Behavioral Health Statistics and Quality. Results from the 2020 National Survey on Drug Use and Health: Detailed tables. Rockville, MD: Substance Abuse and Mental Health Service Administration SAMHSA (2021). Available at: https://www.samhsa.gov/data/.
60. Katrina MJEC, Bridget J, Goosby W. Teen alcohol use and social networks: the contributions of friend influence and friendship selection. J Alcohol Drug Depend (2015) 3(5):224. doi: 10.4172/2329-6488.1000224
61. Balsa AI, Homer JF, French MT, Norton EC. Alcohol use and popularity: social payoffs from conforming to peers’ Behavior. J Res Adolesc (2011) 21(3):559–68. doi: 10.1111/j.1532-7795.2010.00704.x
62. Pepper JK, Coats EM, Nonnemaker JM, Loomis BR. How do adolescents get their E-cigarettes and other electronic vaping devices? Am J Heal Promot (2019) 33(3):420–9. doi: 10.1177/0890117118790366
63. Meyers MJ, Delucchi K, Halpern-Felsher B. Access to tobacco among california high school students: the role of family members, peers, and retail venues. J Adolesc Heal (2017) 61(3):385–8. doi: 10.1016/j.jadohealth.2017.04.012
64. Vidaña-Pérez D, Mus S, Monzón J, Dávila G, Fahsen N, Barnoya J, et al. Factors associated with the changes in smoking and electronic cigarette use in adolescents during the Covid-19 pandemic: a longitudinal analysis. J Adolesc Heal (2024) 10:S1054-139X(23)00980-1. doi: 10.1016/j.jadohealth.2023.11.399
65. Barnes GM, Hoffman JH, Welte JW, Farrell MP, Dintcheff BA. Adolescents’ time use: Effects on substance use, delinquency and sexual activity. J Youth Adolesc (2007) 36(5):697–710. doi: 10.1007/s10964-006-9075-0
66. Cooper ML, Kuntsche E, Levitt A, Barber LL, Wolf S. Motivational models of substance use Vol. 1. Sher KJ, editor. New York, USA: Oxford University Press (2015). Available at: http://oxfordhandbooks.com/view/10.1093/oxfordhb/9780199381678.001.0001/oxfordhb-9780199381678-e-017.
67. Sarvey D, Welsh JW. Adolescent substance use: Challenges and opportunities related to COVID-19. J Subst Abuse Treat (2021) 122:108212. doi: 10.1016/j.jsat.2020.108212
Keywords: COVID-19, lockdown, smoking, adolescents, substance use
Citation: Monzon J, Barnoya J, Mus S, Davila G, Vidaña-Pérez D and Thrasher JF (2024) Changes in substance use among adolescents before and during the COVID-19 pandemic in Guatemala. Front. Psychiatry 15:1331962. doi: 10.3389/fpsyt.2024.1331962
Received: 02 November 2023; Accepted: 25 January 2024;
Published: 29 February 2024.
Edited by:
Saeed Ahmed, Saint Francis Hospital and Medical Center, United StatesReviewed by:
Lakshit Jain, University of Connecticut Health Center, United StatesSouparno Mitra, New York University, United States
Copyright © 2024 Monzon, Barnoya, Mus, Davila, Vidaña-Pérez and Thrasher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joaquin Barnoya, amJhcm5veWFAcG9zdC5oYXJ2YXJkLmVkdQ==