
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry, 15 February 2024
Sec. Schizophrenia
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1327928
This article is part of the Research TopicPsychoneuroendocrinology of Psychosis Disorders, Volume IIView all 6 articles
 Eloi Giné-Servén1,2*
Eloi Giné-Servén1,2* Ester Boix-Quintana3Eva Daví-Loscos3Sandra Cepedello3Lara Moreno-Sancho3Marta Niubó3Rebeca Hernández-Antón3Manuel J. Cuesta1,2
Ester Boix-Quintana3Eva Daví-Loscos3Sandra Cepedello3Lara Moreno-Sancho3Marta Niubó3Rebeca Hernández-Antón3Manuel J. Cuesta1,2 Javier Labad3,4,5
Javier Labad3,4,5Introduction: Previous research has shown that lower lactate dehydrogenase (LDH) concentrations in cerebrospinal fluid (CSF) are associated with longer prodromal symptoms in first-episode psychosis (FEP). We aimed to study whether there is a relationship between the duration of untreated psychosis (DUP) and LDH and other CSF biomarkers in FEP and whether stressful life events moderate this association.
Methods: Ninety-five inpatients with FEP and with less than 6 weeks of antipsychotic treatment were included in the study. All participants were informed about the nature of the study, which was approved by the local ethics committee, and signed an informed consent form. A lumbar puncture was performed at index admission (baseline) to measure CSF parameters (glucose, total protein, LDH). The DUP was assessed with the Quick Psychosis Onset and Prodromal Symptoms Inventory (Q-POPSI). Stressful life events (SLEs) in the previous 6 months were assessed with the List of Threatening Experiences. We dichotomized the SLE variable into having experienced at least one SLE or no experience of SLEs. Statistical analyses were performed with SPSS v. 25.0. Total protein and LDH concentrations were natural log transformed (ln) to reduce skewness. Multiple linear regression analyses were conducted to explore the association between the DUP and CSF parameters (considered the dependent variable). Age, sex, DUP and SLEs were considered independent variables. We tested the DUP by SLE interaction. Significant interactions were included in the final model. The threshold for significance was set at p<0.05.
Results: Fifty-four FEP patients (56.8%) reported an SLE in the previous 6 months. There were no significant differences in the DUP between patients with or without SLEs. There were no significant differences in CSF biomarkers between the SLE groups. In the multiple linear regression analyses, we found a significant DUP by SLE interaction effect on CSF LDH concentrations (standardized beta= -0.320, t= -2.084, p= 0.040). In patients with SLEs, a shorter DUP was associated with higher CSF LDH concentrations and vice versa. No significant associations were found between the DUP or SLEs and other CSF biomarkers (glucose, total proteins).
Conclusions: Our study suggests that psychosocial stress moderates the relationship between the onset of psychosis and CSF biomarkers related to bioenergetic systems.
The onset of psychotic illness typically occurs in late adolescence or early adulthood. Approximately 3% of the population experience a first episode of psychosis (FEP), and its clinical evolution tends toward chronicity (1). In recent decades, a substantial body of evidence has emerged that highlights the importance of early intervention for psychotic disorders, with a specific focus on reducing the duration of untreated psychosis (DUP; the time from the onset of psychotic symptoms until first treatment) (2). These studies have revealed that a longer DUP is linked to more severe positive symptoms (3, 4), negative symptoms (3–5), and impairment of functioning (3, 4). Furthermore, certain studies have indicated higher relapse rates or poorer responses to antipsychotic medications in individuals with a longer DUP (5). The development of psychotic disorders is probably linked to abnormalities in brain development during early life, which then interact with abnormal pathophysiological processes during puberty, ultimately culminating in the onset of psychotic illness (6, 7). Aberrant synaptic pruning (7), sensitization of the dopaminergic system (8), and neurobiological adaptations to chronic N-methyl-D-aspartate receptor dysfunction (9) are possible pathophysiological mechanisms that produce limited neurodegeneration early in the course of psychotic illness (10). The question of whether psychosis itself has a neurotoxic effect is still a topic of debate (11), and there are several hypotheses regarding how untreated psychosis might influence brain function. Dopaminergic hyperactivity, resulting in a gradual decrease in regional brain volumes (12), and oxidative damage due to persistent catecholaminergic activity and prolonged activation of the hypothalamic–pituitary–adrenal axis (13) are potential explanations for the neurotoxic effect of chronic psychosis. Neurotransmitter dysfunction could be a consequence of cell membrane pathology in individuals with schizophrenia (14). Certain areas of the brain, such as the temporal regions, may be particularly susceptible to the impacts of a longer DUP (2).
On the other hand, the interplay between stress and vulnerability has been recognized as a factor in the development of psychotic disorders (15–17). Previous studies suggest that early life stress, particularly childhood trauma (18, 19), is a risk factor for psychotic disorders. Several studies have also reported increased perceived stress in individuals at clinical high risk of psychosis (CHR) or with psychotic disorders, measured using self-report questionnaires (20–22) or electronic sampling methods (23). Regarding hypothalamic-pituitaryadrenal (HPA) axis measures, previous longitudinal studies suggest that diurnal cortisol (24, 25), an increased cortisol awakening response (CAR) (26), and a higher stressor-cortisol concordance (27) are found in CHR individuals who will later develop psychotic symptoms. However, in first episode psychosis (FEP) patients, a blunted CAR has been described (28–30), suggesting that biological markers of stress response might be influenced by the stage of psychotic illness. Consistent with this, previous studies exploring stress responsiveness with the Trier Social Stress Test in CHR and FEP patients (31) found differences in autonomic measures between groups (elevated heart rate and blood pressure were observed in FEP patients), suggesting that the stage of illness contributes to variations in the psychobiological stress response.
The experience of stress – psychosocial, biological, or both – influences neurobiology via a range of pathways, including immune, stress/endocrine, redox, and metabolic systems (32). Neurobiological substrates of the aberrant stress response to HPA axis dysregulation, disruption of inflammatory processes, increased oxidative stress, gut dysbiosis, and altered brain signaling provide mechanistic links between environmental risk factors and the development of psychotic symptoms (33). The importance of stress in triggering the onset and relapse of psychosis is now widely acknowledged. In the last decade, the major research challenge in this area has been to clarify the biological mechanisms underlying the interplay between stress and the onset of psychosis. A clear emphasis of this research is the examination of the biological systems implicated in the stress response. Stress biomarkers seem to have substantial potential as predictors of psychosis and clinical outcomes and may serve as ideal targets for the development of new therapeutic treatments for psychosis (34). It is also important to balance the timing of the stress response including the immune and inflammatory mechanisms within diathesis-stress models of psychosis, as acute stress and inflammation is usually useful and adaptive, turning off once resolved, whereas chronic stress and inflammation is typically maladaptive and associated with tissue-specific or systemic pathology (28).
Our previous studies have reported associations between cerebrospinal fluid (CSF) biomarkers that involve bioenergetics systems (e.g., lactate dehydrogenase [LDH] and glucose) and the clinical expression of first-episode psychosis, including an association between lower CSF LDH concentrations and prodromal symptoms (35). LDH plays a crucial role in brain function by participating in the conversion of lactate to pyruvate, a process essential for energy metabolism in neurons; this enzyme helps maintain the delicate balance between glycolysis and oxidative phosphorylation, ensuring sufficient energy production to support various neurological functions (35). As lower LDH concentrations in CSF have been associated with prodromal symptoms, and these symptoms might be associated with a longer DUP, we hypothesized that the DUP would be associated with lower LDH concentrations in CSF. Additionally, we aimed to explore whether stressful life events moderate this association.
Patients experiencing FEP admitted to acute inpatient units (adult or child and adolescent units) at the Department of Mental Health at the Hospital of Mataró between June 1st, 2018, and March 31st, 2021, were invited to participate in the study. FEP was defined as new-onset disorganized behavior accompanied by delusions or hallucinations, not caused by drugs, that met the DSM-IV criteria for a psychotic disorder (schizophrenia, bipolar disorder or unipolar major depression with psychotic features, schizophreniform disorder, brief psychotic disorder, delusional disorder, psychotic disorder not otherwise specified). Patients were excluded if they had (1) positive symptoms of psychosis lasting more than 6 months, (2) received treatment with antipsychotics for more than 6 weeks, (3) a past history of positive symptoms of psychosis, (4) a previous diagnosis of intellectual disability (IQ < 70), or (5) active medical or neurological diseases that could explain the current symptoms. Ninety-five FEP patients participated in the current study. This sample partially overlapped with the sample in a previous study (36) that explored different hypotheses.
The study was approved by the local ethics committee (Hospital of Mataró, Barcelona, Spain). All participants were informed about the nature of the study and provided written informed consent to participate in the study.
During the first week of hospital admission, all patients underwent psychiatric and neurological evaluations. Two trained attending psychiatrists carried out diagnostic interviews using the Structured Clinical Interview for DSM-IV-TR (SCID-I) (36) for individuals ≥18 years old, the Schedule for Affective Disorders and Schizophrenia for school-age children, and the Present and Lifetime version (K-SADS-PL) (37) for individuals <18 years old.
The onset of prodromal and psychotic symptoms was assessed retrospectively by means of a semi structured interview with a specific ad hoc inventory (Quick Psychosis Onset and Prodromal Symptoms Inventory [Q-POPSI]). The duration of untreated illness (DUI) and duration of untreated psychosis (DUP) were calculated. A full description of the Q-POPSI has been provided elsewhere (35).
Psychopathology at admission was assessed using three psychometric scales. The Positive and Negative Syndrome Scale (PANSS) (38) was used to assess positive, negative and general psychopathology symptoms. The Young Mania Rating Scale (YMRS) (39, 40) was administered to assess manic symptoms. The Hamilton Depression Rating Scale (HAM-D) (41, 42) was also administered to assess depressive symptoms.
Stressful life events (SLEs) in the previous 6 months were assessed with the List of Threatening Experiences (43); individuals were categorized into groups according to whether they had experienced at least one SLE.
Baseline functioning was assessed at admission in the acute inpatient unit using the Global Assessment of Functioning Scale (GAF) (44) for individuals ≥18 years old and the Children’s Global Assessment Scale (C-GAS) (45) for individuals <18 years old.
A description of the clinical and biological assessments is provided in Table 1.
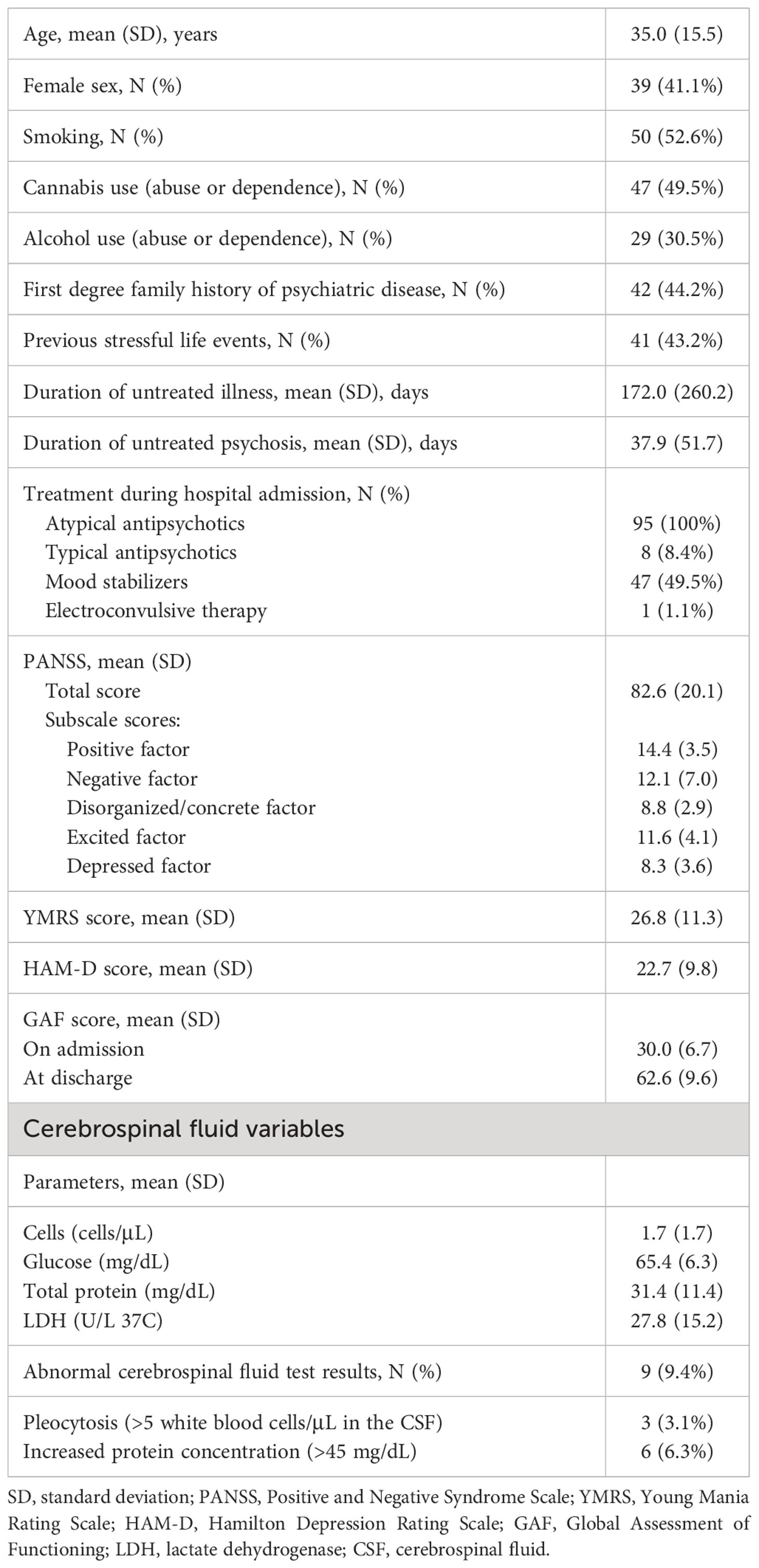
Table 1 Clinical characteristics of the sample.
All patients underwent lumbar puncture by a neurologist, either at the emergency department before admission or at the inpatient unit during the first week of admission. All participants were studied for NMDAR-Abs and GAD65-Abs in their CSF while they participated in another study dealing with autoimmune encephalitis in psychosis (46). None of them had a diagnosis of encephalitis.
CSF samples were examined to determine blood cell counts (ref <5/µL) with on a Sysmex XN 1000 (Sysmex Corporation, Japan) automatic counting versus manual counting chamber. Quantitative determination of glucose, total protein and lactate dehydrogenase levels was performed on a COBAS INTEGRA (Roche Diagnostics, Spain) using the hexokinase method (glucose), the Biuret method (total protein) and the lactate to pyruvate reaction in N-methylglucamine buffer (lactate dehydrogenase), respectively. The sensitivity of the assays was 4.35 mg/dL for glucose, 4 mg/dL for total proteins, and 10 (IU/L) for LDH. The intra-assay and interassay coefficients of variation were 0.8% and 2.5% for glucose, 2.25% and 5% for total proteins, and 1.29% and 1.7% for LDH, respectively.
All data analyses were performed using IBM SPSS for Windows, version 25.0 (IBM Corporation, USA). Continuous CSF parameters (glucose, total protein, LDH levels) were natural log transformed (ln) to reduce skewness and achieve normalization before conducting parametric analyses and regression analyses. We used a dichotomous variable for SLEs, according to whether individuals had experienced at least one SLE.
Spearman and Pearson correlation analyses were used to explore associations between variables. Partial correlation analyses were used to adjust for covariates. To compare continuous data between groups (e.g., FEP patients with or without SLE), Student’s t test was used. The statistical significance threshold was set at p value <0.05 (two-tailed).
Regarding the cell count in the CSF, as only 3 patients had pleocytosis (>5 white blood cells/μL), we decided not to explore associations between this CSF measure and symptoms or diagnoses in the multivariate analyses. Therefore, all hypotheses involving CSF variables considered only the three parameters treated as continuous variables (total protein, LDH and glucose levels).
Multiple linear regression analyses were used to test the hypotheses and explore the association between the DUP and CSF biochemical parameters. In these analyses, we developed three independent equations (one for each CSF parameter [glucose, total protein, LDH levels]; CSF parameters were considered the dependent variable). Age, sex, DUP and SLEs were considered independent variables. We tested the DUP by SLE interaction. Significant interactions were included in the final model. The significance threshold was set at p<0.05.
Demographic, clinical and biochemical data of the sample at the baseline assessment are shown in Table 1. Only a small proportion of FEP patients (<10%) had abnormal CSF findings.
Fifty-four patients (56.8%) reported an SLE in the previous 6 months. There were no significant differences in the DUP between patients with and without SLEs (40.2 ± 60.6 vs. 34.9 ± 37.5, p= 0.625). There were no significant differences in CSF biomarkers between the SLE groups.
No significant correlations were found between CSF biomarkers (glucose, total proteins, LDH).
In the multiple linear regression analyses, we found a significant DUP by SLE interaction effect on CSF LDH concentrations (standardized beta= -0.320, t= -2.084, p= 0.040; Table 2). This interaction is described in Figure 1: in patients with SLEs, a shorter DUP was associated with higher CSF LDH concentrations and vice versa. No significant associations were found between the DUP or SLEs and other CSF biomarkers (glucose, total proteins).
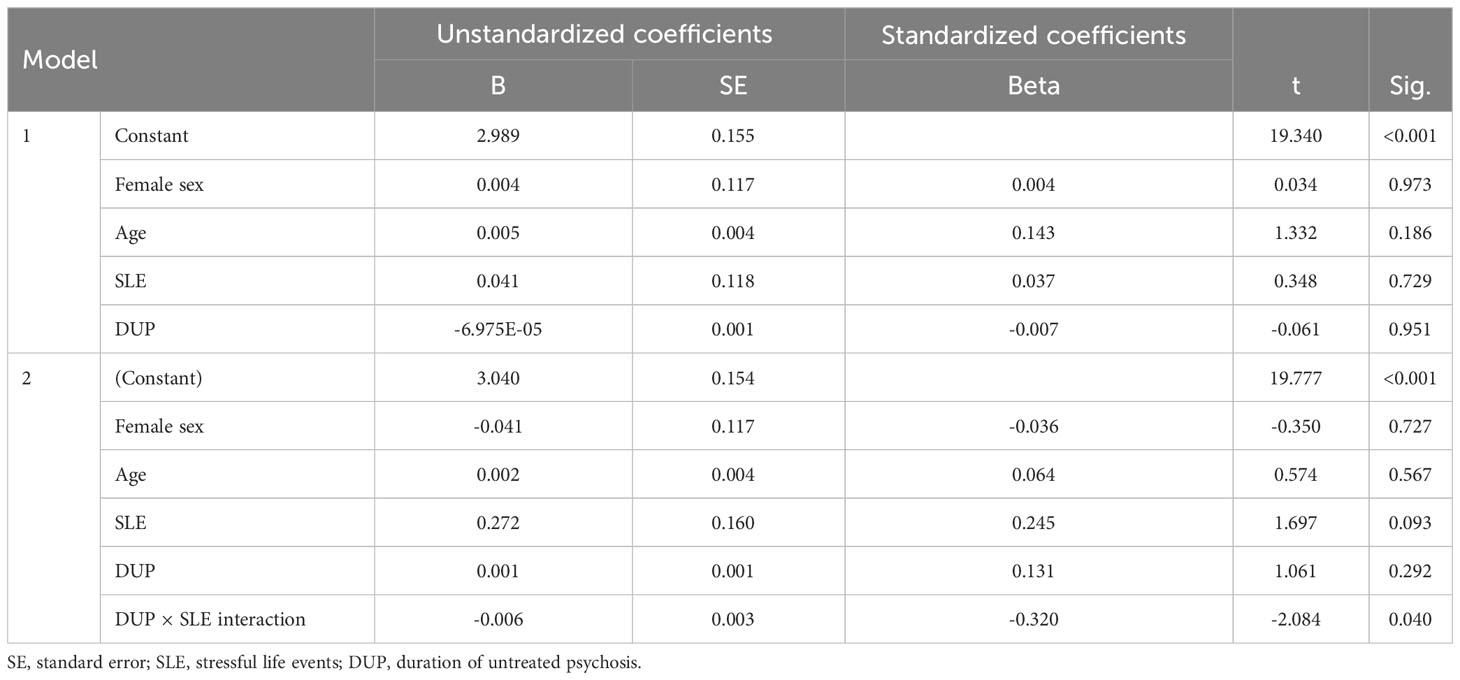
Table 2 Results of the multiple linear regression analysis for cerebrospinal fluid levels of lactate dehydrogenase.
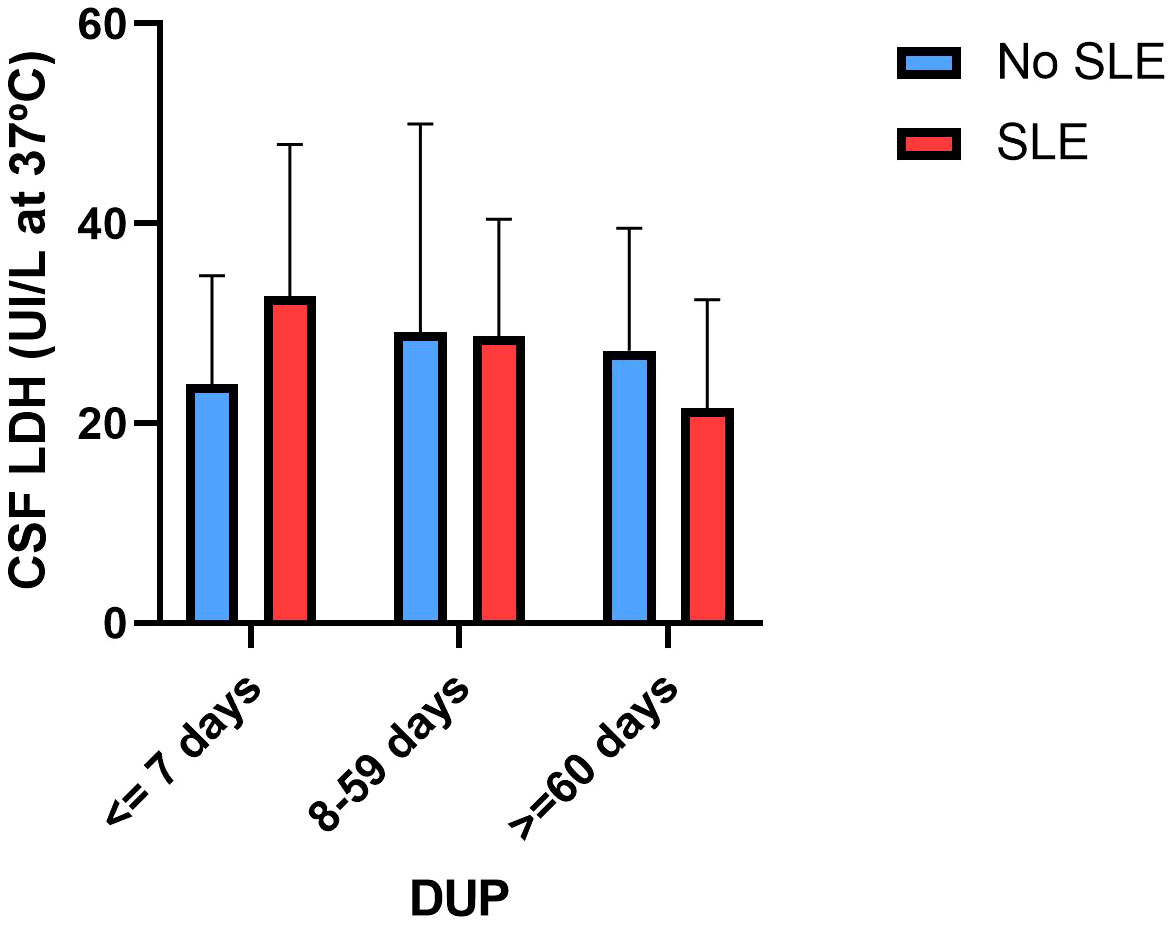
Figure 1 Lactate dehydrogenase concentrations in cerebrospinal fluid according to stressful life events and the duration of untreated psychosis.
In our study that included 95 FEP patients, we found a significant interaction DUP by SLE interaction effect on CSF LDH concentrations. No significant associations were found between the DUP or SLEs and other CSF biomarkers (glucose, total proteins). However, it is important to note that most patients had CSF biomarkers within the normal range, and <10% of participants had abnormal CSF indices.
Our findings indicate that psychosocial stress moderates the relationship between DUP and CSF LDH concentrations. In patients with a shorter DUP, the presence of an SLE around the onset of psychosis is associated with higher CSF LDH concentrations, whereas in those patients with a longer DUP and SLEs, lower CSF LDH concentrations are found. LDH is a ubiquitous enzyme that catalyzes the interconversion of pyruvate and lactate, representing the intersection of key pathways of energy metabolism. A major concept in brain metabolism is the astrocyte-to-neuron lactate-shuttle hypothesis, which posits that astrocytes synthesize lactate through the action of LDH, which is then transported into adjacent neurons as a metabolic substrate under physiologic or pathologic conditions. Once inside the neuron, lactate is converted again by LDH to pyruvate, which then enters the mitochondrion to feed into the tricarboxylic acid (TCA) cycle. Through oxidative phosphorylation within the mitochondrial respiratory chain (MRC), adenosine triphosphate (ATP) is produced and released into the cytosolic compartment. According to a model based on refractory epilepsy, neuronal excitability can be dampened by interference with the astrocyte- to-neuron lactate shuttle: higher LDH levels are conducive to increased pyruvate levels, and higher ATP levels can lead to potassium channel inhibition, rendering the neuron more excitable (47). In a previous study from our group (35), we found that lower CSF LDH concentrations were associated with a more severe phenotype in terms of more severe prodromal symptoms and social withdrawal. Few studies have explored the role of stress in LDH activity. The SLE × DUP interaction effect on CSF LDH concentrations is intriguing. The DUP may reflect different psychotic phenotypes (FEP patients with a shorter DUP exhibiting an acute onset of psychosis and those with a longer DUP exhibiting a more insidious onset of psychosis) that involve different pathophysiological mechanisms regarding brain energy metabolism and LDH concentrations. Alternatively, the presence of psychotic symptoms and psychosocial stress might affect some CSF biomarkers (e.g., LDH) in a different way if this combination (stress and psychosis) occurs over a shorter period of time (more acute exposure) or over a longer period of time (more chronic exposure). Exposure to different stressors might activate various biological processes that have adaptive allostatic functions (48). The sustained activation of these processes, known as the “allostatic load” (AL), can potentially be harmful, potentially resulting in the onset of chronic health issues (49). Therefore, the active process of responding to a challenge to the body by triggering chemical mediators of adaptation (HPA, autonomic, metabolic, immune activity) can be adaptive in the short term (allostasis) and maladaptive in the long term (allostatic load) (48). Although speculative, we wonder whether the relationship between SLE, DUP and LDH might be explained in part by this model (adaptative responses in the short term; maladaptative responses in the long term). In those FEP patients with a shorter DUP, which would mean a more acute onset of psychosis, higher CSF LDH concentrations were found in people reporting SLEs in the previous months of the psychotic outbreak. However, in FEP patients with a longer DUP, suggesting a more insidious onset, the opposite finding was found (lower CSF LDH concentrations were found in patients with SLEs). Our speculative explanation would be that in people with psychosocial stress, higher CSF LDH concentrations represent an adaptative response but that when psychotic symptoms and SLEs last over time (equivalent to chronic stress and greater allostatic load), the reduction of CSF LDH concentrations would be a maladaptative response to stress. It is important to note that this discussion is highly speculative due to a lack of research regarding LDH and psychosocial stress based on the allostatic load model, in contrast to other HPA axis or immune biomarkers
Previous studies have established associations of serum biomarkers related to inflammatory (50–52), oxidative stress (53), immune (54), neuroendocrine (55), and metabolic systems (56) with the DUP. To our knowledge, the current study is the first to report that a CSF biomarker related to brain bioenergetics is correlated with the DUP. As the DUP is a predictor of poor clinical outcome in FEP patients (3, 4) and is associated with social withdrawal (57), future longitudinal studies might explore whether brain bioenergetics biomarkers mediate the relationship between the DUP and social functioning in the years following psychotic onset.
Our study has several limitations that need to be acknowledged. First, the project was initially designed to study autoimmunity in the CSF and serum, and our study is a secondary analysis, as we had available information on routine CSF biomarkers that we did not explore in our previous study (46). However, the original project was not designed to control for factors that could affect the bioenergetics system (such as dietary habits or fasting lumbar puncture data). Second, the FEP patients were receiving antipsychotic treatment and were not drug-naïve. However, we aimed to reduce any long-term treatment effects by excluding patients who had received antipsychotic treatment for a period longer than 6 weeks.
In summary, our study suggests that psychosocial stress moderates the relationship between the onset of psychosis and CSF biomarkers related to bioenergetic systems.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Hospital of Mataró, Barcelona, Spain; Institute Ethics Committee number: 1/18. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
EG-S: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. EB-Q: Investigation, Methodology, Project administration, Writing – review & editing. ED-L: Investigation, Methodology, Writing – review & editing. SC: Investigation, Methodology, Writing – review & editing. LM-S: Data curation, Investigation, Writing – review & editing. MN: Data curation, Software, Writing – review & editing. RH-A: Investigation, Methodology, Writing – review & editing. MC: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. JL: Funding acquisition, Investigation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by the Instituto de Salud Carlos III (Grant PI22/01400).
The authors thank the Adult and the Child and Adolescent Psychiatry Services of Hospital de Mataró for their care of patients and collaboration with the study. We are indebted to the patients and their families who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Perälä J, Suvisaari J, Saarni SI, Kuoppasalmi K, Isometsä E, Pirkola S, et al. Lifetime prevalence of psychotic and bipolar i disorders in a general population. Arch Gen Psychiatry (2007) 64:19. doi: 10.1001/archpsyc.64.1.19
2. Zoghbi AW, Lieberman JA, Girgis RR. The neurobiology of duration of untreated psychosis: A comprehensive review. Mol Psychiatry (2023) 28:168–90. doi: 10.1038/s41380-022-01718-0
3. Penttilä M, Jääskeläinen E, Hirvonen N, Isohanni M, Miettunen J. Duration of untreated psychosis as predictor of long-term outcome in schizophrenia: Systematic review and meta-analysis. Br J Psychiatry (2014) 205:88–94. doi: 10.1192/bjp.bp.113.127753
4. Perkins DO, Gu H, Boteva K, Lieberman JA. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: A critical review and meta-analysis. Am J Psychiatry (2005) 162:1785–804. doi: 10.1176/appi.ajp.162.10.1785
5. Boonstra N, Klaassen R, Sytema S, Marshall M, De Haan L, Wunderink L, et al. Duration of untreated psychosis and negative symptoms — A systematic review and meta-analysis of individual patient data. Schizophr Res (2012) 142:12–9. doi: 10.1016/j.schres.2012.08.017
6. Weinberger DR. Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychiatry (1987) 44:660. doi: 10.1001/archpsyc.1987.01800190080012
7. Keshavan MS, Anderson S, Pettergrew JW. Is Schizophrenia due to excessive synaptic pruning in the prefrontal cortex? The Feinberg hypothesis revisited. J Psychiatr Res (1994) 28:239–65. doi: 10.1016/0022-3956(94)90009-4
8. Sheitman B, Lieberman J. The natural history and pathophysiology of treatment resistant schizophrenia. J Psychiatr Res (1998) 32:143–50. doi: 10.1016/S0022-3956(97)00052-6
9. Javitt DC, Zukin SR, Heresco-Levy U, Umbricht D. Has an angel shown the way? Etiological and therapeutic implications of the PCP/NMDA model of schizophrenia. Schizophr Bull (2012) 38:958–66. doi: 10.1093/schbul/sbs069
10. Lieberman JA. Is schizophrenia a neurodegenerative disorder? a clinical and neurobiological perspective. Biol Psychiatry (1999) 46:729–39. doi: 10.1016/S0006-3223(99)00147-X
11. Rund BR. Does active psychosis cause neurobiological pathology? A critical review of the neurotoxicity hypothesis. Psychol Med (2014) 44:1577–90. doi: 10.1017/S0033291713002341
12. Crespo-Facorro B, Roiz-Santiáñez R, Pelayo-Terán JM, González-Blanch C, Pérez-Iglesias R, Gutiérrez A, et al. Caudate nucleus volume and its clinical and cognitive correlations in first episode schizophrenia. Schizophr Res (2007) 91:87–96. doi: 10.1016/j.schres.2006.12.015
13. Keshavan MS, Haas GL, Kahn CE, Aguilar E, EL D, NR S, et al. Superior temporal gyrus and the course of early schizophrenia: Progressive, static, or reversible? J Psychiatr Res (1998) 32:161–7. doi: 10.1016/S0022-3956(97)00038-1
14. Mukherjee S, Mahadik SP. A new paradigm for schizophrenia? Schizophr Res (1994) 13:191–4. doi: 10.1016/0920-9964(94)90042-6
15. Corcoran C, Walker E, Huot R, Mittal V, Tessner K, Kestler L, et al. The stress cascade and schizophrenia: Etiology and onset. Schizophr Bull (2003) 29:671–92. doi: 10.1093/oxfordjournals.schbul.a007038
16. Gispen-de Wied CC. Stress in schizophrenia: an integrative view. Eur J Pharmacol (2000) 405:375–84. doi: 10.1016/S0014-2999(00)00567-7
17. Zubin J, Spring B. Vulnerability: A new view of schizophrenia. J Abnorm Psychol (1977) 86:103–26. doi: 10.1037/0021-843X.86.2.103
18. Radua J, Ramella-Cravaro V, Ioannidis JPA, Reichenberg A, Phiphopthatsanee N, Amir T, et al. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry (2018 ) 17:49–66. doi: 10.1002/wps.20490
19. Arseneault L, Cannon M, Fisher HL, Polanczyk G, Moffitt TE, Caspi A. Childhood trauma and children’s emerging psychotic symptoms: A genetically sensitive longitudinal cohort study. Am J Psychiatry (2011) 168:65–72. doi: 10.1176/appi.ajp.2010.10040567
20. Studerus E, Ittig S, Beck K, Del Cacho N, Vila-Badia R, Butjosa A, et al. Relation between self-perceived stress, psychopathological symptoms and the stress hormone prolactin in emerging psychosis. J Psychiatr Res (2021) 136:428–34. doi: 10.1016/j.jpsychires.2020.06.014
21. Ortega L, Montalvo I, Monseny R, Burjales-Martı́ MD, Martorell L, Sanchez-Gistau V, et al. Perceived stress, social functioning and quality of life in first-episode psychosis: A 1-year follow-up study. Early Interv Psychiatry (2021) 15:1542–50. doi: 10.1111/eip.13092
22. Ortega L, Montalvo I, Monseny R, Vilella E, Labad J. Perceived stress mediates the relationship between social adaptation and quality of life in individuals at ultra high risk of psychosis. Early Interv Psychiatry (2019) 13:1447–54. doi: 10.1111/eip.12791
23. Lataster T, Valmaggia L, Lardinois M, van Os J, Myin- Germeys I. Increased stress reactivity: a mechanism specifically associated with the positive symptoms of psychotic disorder. Psychol Med (2013) 43:1389–400. doi: 10.1017/S0033291712002279
24. Cullen AE, Fisher HL, Gullet N, Fraser ER, Roberts RE, Zahid U, et al. Cortisol levels in childhood associated with emergence of attenuated psychotic symptoms in early adulthood. Biol Psychiatry (2022) 91:226–35. doi: 10.1016/j.biopsych.2021.08.009
25. Walker EF, Trotman HD, Pearce BD, Addington J, Cadenhead KS, Cornblatt BA, et al. Cortisol levels and risk for psychosis: initial findings from the North American prodrome longitudinal study. Biol Psychiatry (2013) 74:14–17. doi: 10.1016/j.biopsych.2013.02.016
26. Labad J, Stojanovic-érez A, Montalvo I, Solé M, Cabezas Á, Ortega L, et al. Stress biomarkers as predictors of transition to psychosis in at-risk mental states: roles for cortisol, prolactin and albumin. J Psychiatr Res (2015) 60:163–9. doi: 10.1016/j.jpsychires.2014.10.011
27. Cullen AE, Addington J, Bearden CE, Stone WS, Seidman LJ, Cadenhead KS, et al. Stressor-cortisol concordance among individuals at clinical high-risk for psychosis: Novel findings from the NAPLS cohort. Psychoneuroendocrinology (2020) 115:104649. doi: 10.1016/j.psyneuen.2020.104649
28. Cullen AE, Labad J, Oliver D, Al-Diwani A, Minichino A, Fusar-Poli P. The translational future of stress neurobiology and psychosis vulnerability: A review of the evidence. Curr Neuropharmacol (2024) 22:350–77. doi: 10.2174/1570159X21666230322145049
29. Labad J. The role of cortisol and prolactin in the pathogenesis and clinical expression of psychotic disorders. Psychoneuroendocrinology (2019) 102:24–36. doi: 10.1016/j.psyneuen.2018.11.028
30. Pruessner M, Boekestyn L, Béchard-Evans L, Abadi S, Vracotas N, Joober R, et al. Sex differences in the cortisol response to awakening in recent onset psychosis. Psychoneuroendocrinology (2008) 33:1151–4. doi: 10.1016/j.psyneuen.2008.04.006
31. Shah JL, Paquin V, McIlwaine SV, Malla AK, Joober R, Pruessner M. Examining the psychobiological response to acute social stress across clinical stages and symptom trajectories in the early psychosis continuum. Dev Psychopathol (2023) 28:1–13. doi: 10.1017/S0954579423000056
32. Karanikas E. The immune-stress/endocrine-redox-metabolic nature of psychosis’ etiopathology; focus on the intersystemic pathways interactions. Neurosci Lett (2023) 794:137011. doi: 10.1016/j.neulet.2022.137011
33. Xenaki L-A, Dimitrakopoulos S, Selakovic M, Stefanis N. Stress, environment and early psychosis. Curr Neuropharmacol (2024) 22:437–60. doi: 10.2174/1570159X21666230817153631
34. Mondelli V. From stress to psychosis: whom, how, when and why? Epidemiol Psychiatr Sci (2014) 23:215–8. doi: 10.1017/S204579601400033X
35. Giné-Servén E, Martinez-Ramirez M, Boix-Quintana E, Davi-Loscos E, Guanyabens N, Casado V, et al. Routine cerebrospinal fluid parameters as biomarkers in first-episode psychosis: A prospective observational study. Prog Neuropsychopharmacol Biol Psychiatry (2022) 112:110424. doi: 10.1016/j.pnpbp.2021.110424
36. First M, Spitzer R GM. Structured clinical interview for DSM-IV axis I disorders. Washington DC Am Psychiatr Press (1994).
37. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J Am Acad Child Adolesc Psychiatry (1997) 36:980–8. doi: 10.1097/00004583-199707000-00021
38. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
39. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: Reliability, validity and sensitivity. Br J Psychiatry (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
40. Lukasiewicz M, Gerard S, Besnard A, Falissard B, Perrin E, Sapin H, et al. Young Mania Rating Scale: How to interpret the numbers? Determination of a severity threshold and of the minimal clinically significant difference in the EMBLEM cohort. Int J Methods Psychiatr Res (2013) 22:46–58. doi: 10.1002/mpr.1379
41. Hamilton MA. Rating scale for depression. J Neurol Neurosurg Psychiatry (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
42. Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K. Severity classification on the Hamilton depression rating scale. J Affect Disord (2013) 150:384–8. doi: 10.1016/j.jad.2013.04.028
43. Brugha TS, Cragg D. The list of threatening experiences: The reliability and validity of a brief life events questionnaire. Acta Psychiatr Scand (1990) 82:77–81. doi: 10.1111/j.1600-0447.1990.tb01360.x
44. Hall RCW. Global assessment of functioning. Psychosomatics (1995) 36:267–75. doi: 10.1016/S0033-3182(95)71666-8
45. Shaffer D. A children’s global assessment scale (CGAS). Arch Gen Psychiatry (1983) 40:1228. doi: 10.1001/archpsyc.1983.01790100074010
46. Guasp M, Giné-Servén E, Maudes E, Rosa-Justicia M, Martínez-Hernández E, Boix-Quintana E, et al. Clinical, neuroimmunologic, and CSF investigations in first episode psychosis. Neurology (2021) 97:e61–75. doi: 10.1212/WNL.0000000000012191
47. Rho JM. Inhibition of lactate dehydrogenase to treat epilepsy. N Engl J Med (2015) 373:187–9. doi: 10.1056/NEJMcibr1503558
48. McEWEN BS. Stress, adaptation, and disease: Allostasis and allostatic load. Ann N Y Acad Sci (1998) 840:33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
49. Misiak B, Kowalski K, Piotrowski P, Grąźlewski T, Samochowiec J. Neurodevelopmental aspects of adverse childhood experiences in psychosis: Relevance of the allostatic load concept. Psychoneuroendocrinology (2022) 143:105850. doi: 10.1016/j.psyneuen.2022.105850
50. Dunjic-Kostic B, Jasovic-Gasic M, Ivkovic M, Radonjic NV, Pantovic M, Damjanovic A, et al. Serum levels of interleukin-6 and tumor necrosis factor-alpha in exacerbation and remission phase of schizophrenia. Psychiatr Danub (2013) 25:55–61.
51. Śmierciak N, Krzyściak W, Szwajca M, Szczęsny-Malysiak E, Kij A, Chłopicki S, et al. Improvement in clinical symptoms in patients with the first episode of psychosis is associated with a decrease in systemic nitric oxide availability. A pilot study. Psychiatr Pol (2021) 55:541–54. doi: 10.12740/PP/131531
52. Rizos EN, Michalopoulou PG, Siafakas N, Stefanis N, Douzenis A, Rontos I, et al. Association of serum Brain-Derived neurotrophic factor and duration of untreated psychosis in First-Episode patients with Schizophrenia. Neuropsychobiology (2010) 62:87–90. doi: 10.1159/000315438
53. Becklén M, Orhan F, Piehl F, Cervenka S, Sellgren CM, Flyckt L, et al. Plasma bilirubin levels are reduced in first-episode psychosis patients and associates to working memory and duration of untreated psychosis. Sci Rep (2021) 11:7527. doi: 10.1038/s41598-021-87096-z
54. Pollak TA, Vincent A, Iyegbe C, Coutinho E, Jacobson L, Rujescu D, et al. Relationship between serum NMDA receptor antibodies and response to antipsychotic treatment in First-Episode psychosis. Biol Psychiatry (2021) 90:9–15. doi: 10.1016/j.biopsych.2020.11.014
55. Gine-Serven E, Martinez-Ramirez M, Boix-Quintana E, Davi-Loscos E, Guanyabens N, Casado V, et al. Association between free thyroxine levels and clinical phenotype in first-episode psychosis: a prospective observational study. PeerJ (2023) 11:e15347. doi: 10.7717/peerj.15347
56. Śmierciak N, Krzyściak W, Szwajca M, Bryll A, Popiela T, Karcz P, et al. Relationship of metabolic parameters with the course of the first episode of psychosis – preliminary research. Psychiatr Pol (2021) 55:525–40. doi: 10.12740/PP/119021
57. Izquierdo A, Cabello M, de la Torre-Luque A, Ayesa-Arriola R, Setien-Suero E, Mayoral-van-Son J, et al. A network analysis approach to functioning problems in first psychotic episodes and their relationship with duration of untreated illness: Findings from the PAFIP cohort. J Psychiatr Res (2021) 136:483–91. doi: 10.1016/j.jpsychires.2020.10.019
Keywords: psychosis, duration of untreated psychosis, stress, cerebrospinal fluid, lactate dehydrogenase, glucose
Citation: Giné-Servén E, Boix-Quintana E, Daví-Loscos E, Cepedello S, Moreno-Sancho L, Niubó M, Hernández-Antón R, Cuesta MJ and Labad J (2024) Psychosocial stress moderates the relationship between cerebrospinal fluid lactate dehydrogenase and the duration of untreated psychosis in first-episode psychosis. Front. Psychiatry 15:1327928. doi: 10.3389/fpsyt.2024.1327928
Received: 25 October 2023; Accepted: 29 January 2024;
Published: 15 February 2024.
Edited by:
Mary V. Seeman, University of Toronto, CanadaReviewed by:
Evangelos Karanikas, 424 General Military Hospital, GreeceCopyright © 2024 Giné-Servén, Boix-Quintana, Daví-Loscos, Cepedello, Moreno-Sancho, Niubó, Hernández-Antón, Cuesta and Labad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eloi Giné-Servén, ZWxvaS5naW5lLnNlcnZlbkBuYXZhcnJhLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.