 Julia Treml
Julia Treml Katja Linde1
Katja Linde1 Elmar Brähler
Elmar Brähler Anette Kersting
Anette Kersting- 1Department of Psychosomatic Medicine and Psychotherapy, Medical Faculty, University of Leipzig, Leipzig, Germany
- 2Department of Psychosomatic Medicine and Psychotherapy, University Medical Center, Johannes Gutenberg-University Mainz, Mainz, Germany
- 3Department of Medical Psychology and Medical Sociology, University of Leipzig, Leipzig, Germany
Background: Prolonged grief disorder (PGD) was recently included as a disorder in the ICD-11 and DSM-5-TR. Although both classification systems use the same name, the criteria content, and diagnostic approach vary. This study aimed to estimate the respective prevalence of PGDICD-11 and PGDDSM-5-TR and examine the diagnostic agreement while varying the diagnostic algorithm of PGDICD-11 (bereavement vs. symptom period; varying number of accessory symptoms).
Methods: A representative sample of the German general population (N = 2,509) was investigated, of which n=1,071 reported the loss of a close person. PGD symptoms were assessed with the Traumatic Grief Inventory - Self Report Plus (TGI-SR+).
Results: The point prevalence of PGD among the bereaved varied between 4.7%-6.8%, depending on the criteria and diagnostic algorithm. The prevalence of PGDDSM-5-TR was significantly lower than the prevalence of PGDICD-11. The diagnostic agreement between both criteria sets was substantial and increased after the number of accessory symptoms for PGDICD-11 was increased from one to three. The most common symptoms were intrusive thoughts/images related to the deceased person, longing for the deceased person, and difficulty accepting the loss.
Conclusion: The results demonstrate that the prevalence of PGD significantly varies depending on the application of the diagnostic algorithm and criteria. PGD affects a substantial proportion of the general population and should be addressed by healthcare providers. However, applying the minimum ICD-11 criteria could lead overestimating the prevalence. Therefore, further harmonizing the ICD-11 and DSM-5-TR criteria and diagnostic algorithm for PGD seems appropriate.
Introduction
Losing a loved one is often accompanied by intense feelings of grief and longing for the deceased. Most bereaved people are able to adapt to the loss over time without professional support (1). However, when grief reactions persist and impede daily functioning, a disorder called Prolonged Grief Disorder (PGD) should be considered.
The conceptualization, diagnostic criteria, and assessment of PGD have been the topics of debate among researchers for many years (2). Some have called for the inclusion of PGD in the International Statistical Classification of Diseases and Related Health Problems (ICD) and the Diagnostic and Statistical Manual of Mental Disorders (DSM) while proposing different diagnostic criteria-sets [e.g., (3–5)]. The DSM-5 workgroup on Trauma/Stress-Related and Dissociative Disorders first decided to include PGD as Persistent Complex Bereavement Disorder (PCBD) in Section III, “Conditions for Further Study” within the DSM-5 to encourage research into the condition (2, 6, 7). Later, the ICD-11 workgroup on Stress-Associated Disorders found the evidence for PGD sufficient and included PGD in the ICD-11 as a new diagnostic entity (8). Based on this inclusion and the collected evidence, the DSM Steering Committee reviewed a proposal to modify the criteria for PCBD. The American Psychiatric Association (APA) then approved the inclusion of PGD in Section II of the DSM-5-TR, thus replacing the criteria for PCBD (9, 10).
Although both classification systems included PGD as a disorder and used the same name, the criteria content and diagnostic approach vary. While the DSM-5-TR provides an explicit diagnostic algorithm, the ICD-11 only uses a typological approach without strict requirements for the number of symptoms that must be present to meet the diagnostic threshold (11). Table 1 provides an overview of the diagnostic criteria. A PGDDSM-5-TR diagnosis requires one of two separation distress symptoms (persistent and pervasive longing for the deceased and/or persistent and pervasive preoccupation with the deceased), and at least three out of eight accessory symptoms to a functionally impairing degree, with a minimum of 12 months since the loss (12). A PGDICD-11 diagnosis, however, only requires at least one of two separation distress symptoms, combined with any of ten accessory symptoms to a functionally impairing degree for an atypically long period of time (at least six months) after the loss (8).
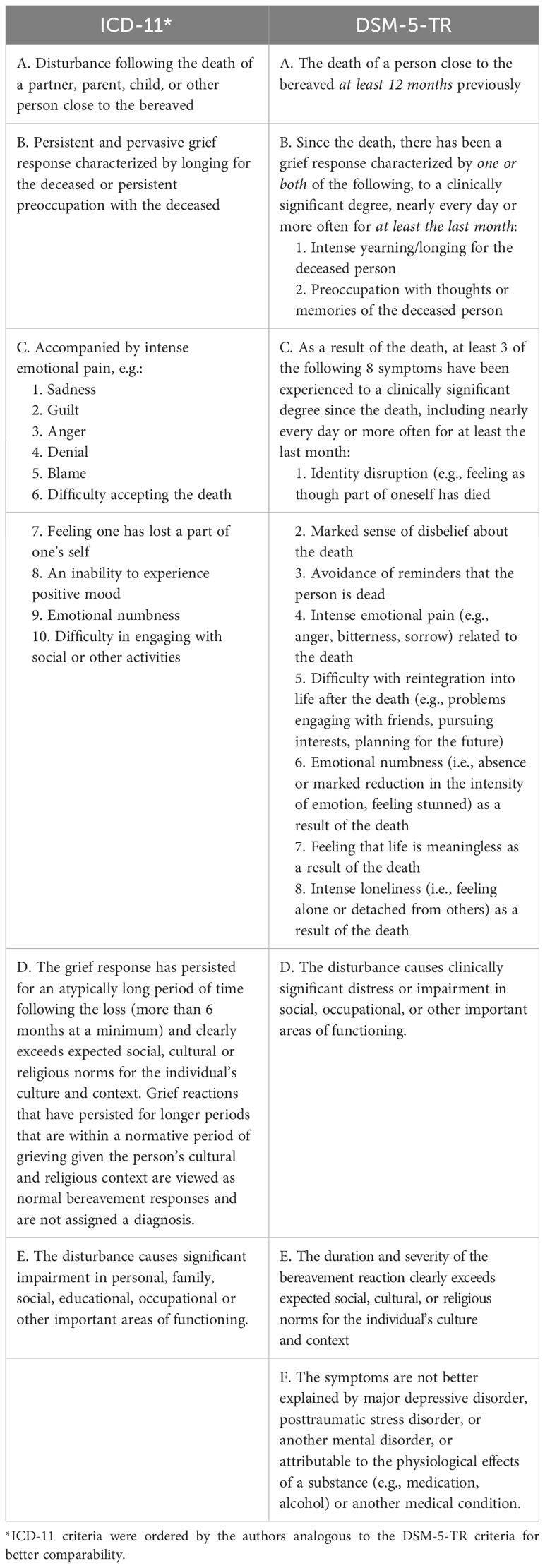
Table 1 Diagnostic criteria for PGD.
Some researchers have argued that the ICD-11’s typological approach, with simple diagnostic descriptions and no strict requirement for the number of symptoms needed to meet a diagnostic threshold, has the advantage of increasing cross-cultural applicability and being helpful in clinical practice as it results in greater sensitivity in case identification (13). Others, however, criticize this approach for being too liberal since the application of the minimal criteria leads to much higher prevalence rates than the prior used criteria sets for PGD (such as PCBD) or the PGDDSM-5-TR criteria (11). For instance, Boelen and colleagues compared the PGDICD-11 criteria to the former PCBDDSM-5 criteria and found prevalence rates of 18% vs. 6.4%, respectively. Furthermore, Rosner and colleagues found prevalence rates of 4.2% for PGDICD-11 compared to 3.3% for PGDDSM-5-TR in a representative bereaved sample in Germany (14). A recent study extended these findings and demonstrated limited content overlap between both criteria sets and their predecessors (15). However, these studies are all based on outdated assessment tools not designed to measure PGD according to the DSM-5-TR and ICD-11 criteria. Therefore, researchers recommend the use of validated instruments that capture both criteria sets to assess the prevalence and determine which PGDICD-11 algorithm leads to the greatest concordance with PGDDSM-5-TR (15).
As demonstrated, the information on prevalence rates strongly depends on the chosen diagnostic algorithm. However, accurate estimates of prevalence rates are necessary to understand the health burden and then allocate economic and professional resources accordingly. When estimating the prevalence of PGD, not only the number of symptoms present might be decisive, but also the application of the time or duration criterion. The DSM-5-TR specifies that the loss of a loved one must have occurred at least 12 months ago before a diagnosis can be made. In ICD-11, however, the grief reaction must persist for an atypically long period of time following the loss, with a minimum of 6 months. This wording indicates an alternative application of the duration criterion, that is, that the grief response in itself and not just the bereavement period should last for at least six months. However, in some studies, only the time since loss was assessed, while in others, it is unclear whether the duration of symptoms or simply the time since the loss was assessed (e.g., 16–18).
To avoid medicalizing normal grief and overestimating the prevalence of PGD (19), determining the optimal diagnostic threshold for PGDICD11 is essential (20). The aims of the current study were therefore: 1) to estimate the probable point prevalence of PGD according to the DSM-5-TR and ICD-11 criteria using a validated instrument designed to capture both criteria sets and examine the diagnostic agreement, 2) to assess the frequency of occurrence of each symptom of prolonged grief, 3) to investigate the difference between time since loss and symptom duration for a PGDICD-11 diagnosis and 4) to determine which PGDICD-11 algorithm results in the greatest concordance with PGDDSM-5-TR when varying the number of required accessory symptoms for a PGDICD-11 diagnosis in a representative sample of the population in Germany.
Materials and methods
Participants and procedures
Data from a representative sample of the population in Germany was collected between October and December 2021 with the assistance of a demographic consulting company (USUMA, Berlin, Germany). The sample size was determined by the ADM sampling consortium (ADM Arbeitskreis Deutscher Markt- und Sozialforschungsinstitute e.V.) that provides a sampling frame that allows to create representative samples of private households and the people living in them. The random sampling procedure involved three stages: 1) random selection of 258 regional sample point areas representing different regions of the country, 2) random selection of target households within those sample point areas using the random-route procedure, 3) random selection of one target member within target households based on a Kish-selection-grid. Inclusion criteria for target persons were age equal or above 16 years, sufficient fluency in the German language, and written informed consent. The multi-stage sampling design ensured that households were selected with equal probability. Design weighting equalized the selection probabilities within households. Distortions due to non-response were corrected by weighting adjustments. At household level, the distribution was adjusted to the population and at the individual level, further weighting was carried out to correct for biases based on the characteristics age, gender and geographic region. Regarding these characteristics the sample was representative compared to the German microcensus. The microcensus is a representative survey based on 1% of the German population (approximately 810,000 Germans), which is used for political decision-making in Germany (21).
A total of 5,901 target persons were approached by one of 198 trained interviewers. If the target person was not at home, a maximum of three further attempts were made to contact the selected person. Reasons for non-response were: a) household could not be reached (n = 791, 13.4%), b) household declined participation (n = 1,374, 23.3%), c) target person could not be reached (n = 288, 4.9%), d) target person was absent (n = 61, 1.0%), e) target person was ill or unable to follow the interview (n = 75, 1.3%), f) target person declined participation (n = 786, 13.3%). Seventeen interviews (0.3%) were not applicable for analyses. Interviews were scheduled with the remaining 2,509 participants (42.5%). The participants received oral and written information about the study and provided written informed consent. Additional parental informed consent was acquired for target persons under the age of 18. Face-to-face interviews were conducted to assess sociodemographic information. Thereafter, participants completed self-report questionnaires, and interviewers provided assistance in case of questions. The study and the procedures were approved by the local ethical review board (Leipzig University, Medical Faculty; AZ: 298/21-ek, 12.7.2021) and conducted in following the declaration of Helsinki.
Measures
Sociodemographic data included age, gender, education, monthly household income and employment status. Bereaved participants were further asked to provide information on the characteristics of the deceased and the loss (e.g., relationship to the deceased, time since loss, cause of death). The cause of death was categorized as violent if participants indicated losing their loved one by suicide, homicide or accident. In the case of multiple losses, the participants were asked to refer to the person whose death had affected them the most.
Grief symptoms were assessed using the German version of the Traumatic Grief Inventory – Self Report Plus (TGI-SR+), which contains 22 items about grief reactions (22). All items can be found in Table 2. The TGI-SR+ assesses the criteria sets for PGD as defined in the DSM-5-TR and the ICD-11 (as well as the former criteria, for example PCBD). Items are rated on a 5-point Likert Scale from 1 = never to 5 = always. The TGI-SR+ has been demonstrated to be reliable and valid (22). Cronbach’s alpha in the present study indicated excellent internal consistency for the TGI-SR+ (α = .97).
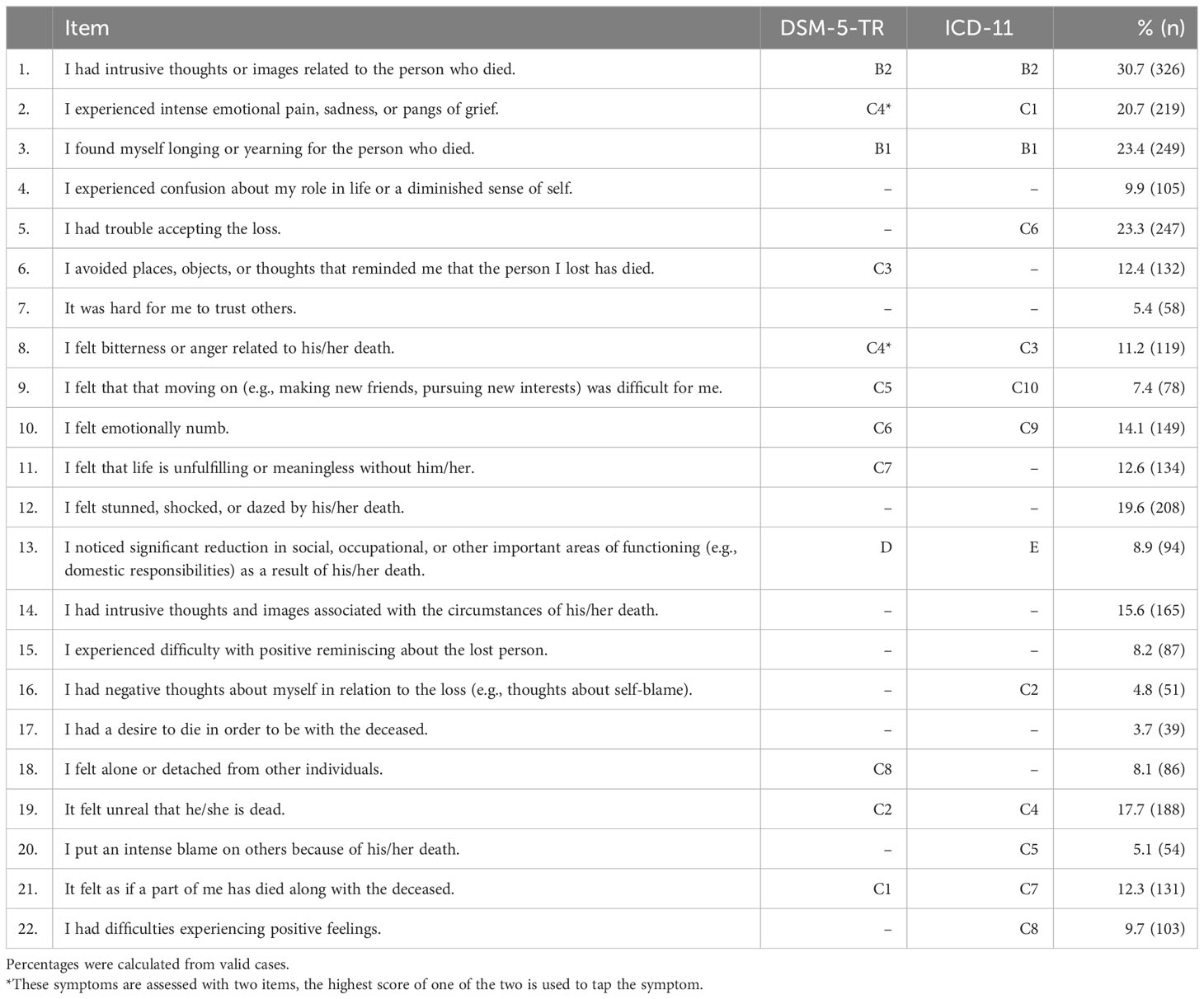
Table 2 Frequency of occurrence of single symptoms of PGD.
To meet DSM-5-TR criteria for PGD, at least one of the two Criterion B symptoms, at least three of the eight Criterion C symptoms, and the Criterion D symptom (i.e., functional impairment) must be endorsed for those who experienced the death of a loved one at least 12 months prior (Criterion A) (9, 10). All Criterion C symptoms are tapped by one item, except for one symptom (C4: “Intense emotional pain (e.g., anger, bitterness, sorrow) related to the death”), which is captured by two items. The highest score on one of these two items was used to represent the C4 criterion. The time criterion of 12 months was assessed with the following question: “How much time has passed since the loss? (In Months)”. All participants who indicated at least 12 months were counted.
To meet ICD-11 criteria for PGD, at least one of the two Criterion B symptoms, at least one Criterion C symptom, the Criterion D symptom (i.e., functional impairment) and the Criterion E (the grief response has persisted for at least six months) should be endorsed for those who experienced the death of a loved one (Criterion A).
The duration criterion E was assessed with the following question: “Have you had the feelings described above for at least six months?”.
Statistical analyses
All statistical analyses were conducted using the Statistical Package for Social Sciences, version 27 (IBM® SPSS®). The significance level was set to α = .05.
To estimate the prevalence of PGD, the number of participants fulfilling the criteria described above was counted. A symptom was considered present if scores were ≥ 4 (at least ‘often’) (22). Each symptom was dichotomously coded as ‘not present’ (0) or ‘present’ (1). For exploratory reasons, percentages of endorsement of each item were calculated.
To examine the difference between PGDDSM-5-TR and PGDICD-11, Fisher’s exact test was used. Pairwise agreement between both diagnostic algorithms was evaluated using kappa statistics with a 95% confidence interval. To investigate the difference between time since loss and symptom duration for a PGDICD-11 diagnosis, the duration criterion E was applied in two different ways (time since loss = 6 months vs. symptom duration = 6 months). Fisher’s exact test was again used to test statistical significance. Furthermore, the diagnostic rates of PGDICD-11 were calculated with an increasing number of required accessory symptoms from 2+ to 7+ symptoms, and pairwise agreement with PGDDSM-5-TR was evaluated again using kappa statistics.
Results
Of the 2,509 participants between the ages of 16 and 95 years, 50.9% were female. The mean age was 49.48 years (SD=17.81). Table 3 provides an overview of the participant characteristics. Of all participants, 1,071 (54.2%) reported having experienced the loss of a close person (e.g., a partner, relative or good friend). Nine participants had to be excluded due to missing data leading to a final data set of n=1,062. Bereaved individuals were primarily middle-aged, and 55.6% were female. The majority reported having lost a parent (40.9%), or other relatives besides children, parent, or partner (28.8%), and natural nonviolent deaths were reported most frequently (89.0%) as the cause of death (see Table 4).
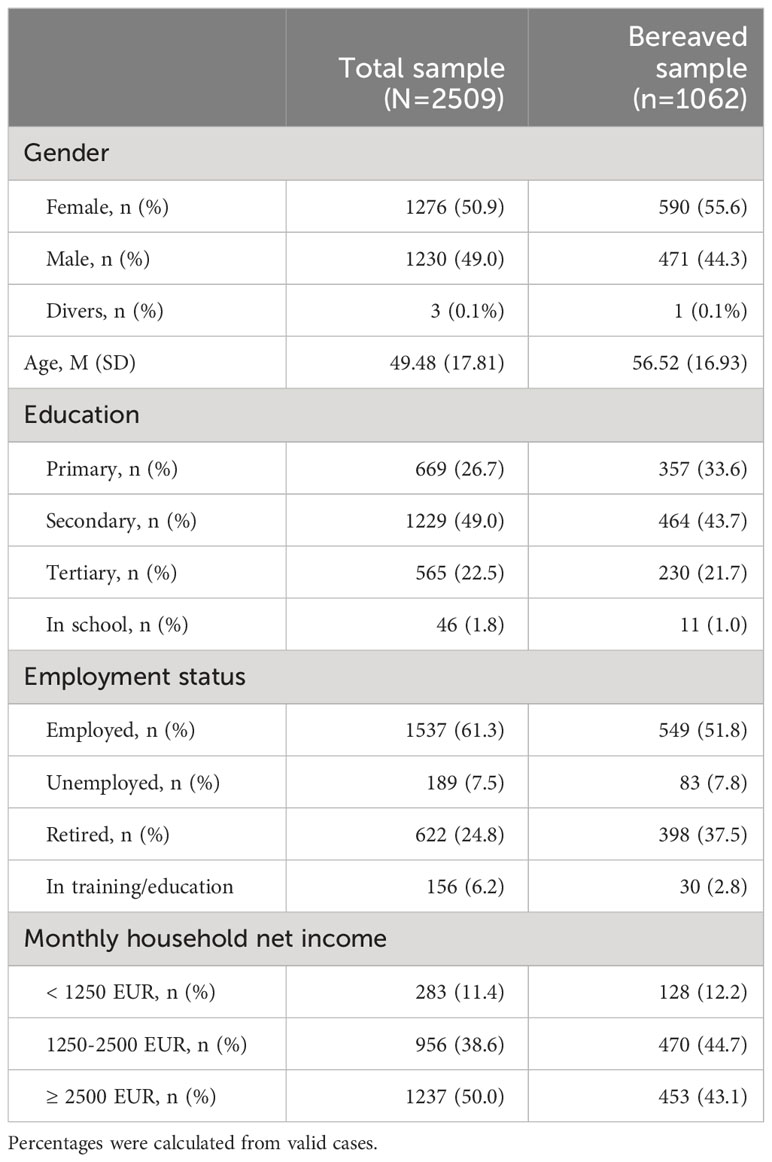
Table 3 Demographic characteristics of the sample.
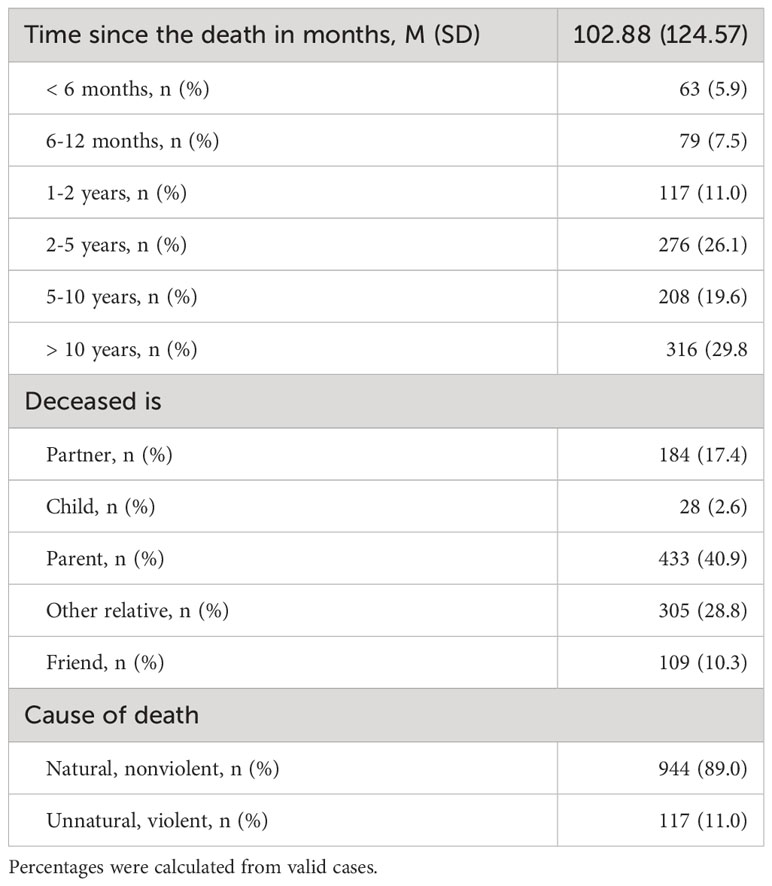
Table 4 Characteristics of the bereaved sample (n=1062).
The conditional prevalence of PGD using the DSM-5-TR diagnostic algorithm was 4.7% (n = 50), within the population-based sample (including non-bereaved), 2.0%. Using the diagnostic algorithm of the ICD-11 led to a conditional prevalence of PGD of 5.4% (n=57), within the population-based sample (including non-bereaved) 2.3%.
The PGDDSM-5-TR diagnostic rate was significantly lower than the rate of PGDICD-11 (Fisher’s exact test, p <.001). The pairwise agreement between PGDDSM-5-TR and PGDICD-11 was substantial with κ = 0.75, 95% CI [0.66–0.85]. There were nine unique PGDDSM-5-TR cases (i.e., meeting PGDDSM-5-TR but not PGDICD-11 criteria) and 16 unique PGDICD-11 cases (i.e., meeting PGDICD-11 but not PGDDSM-5-TR criteria). The remaining 41 participants (3.9%) met both PGD criteria (see Figure 1).
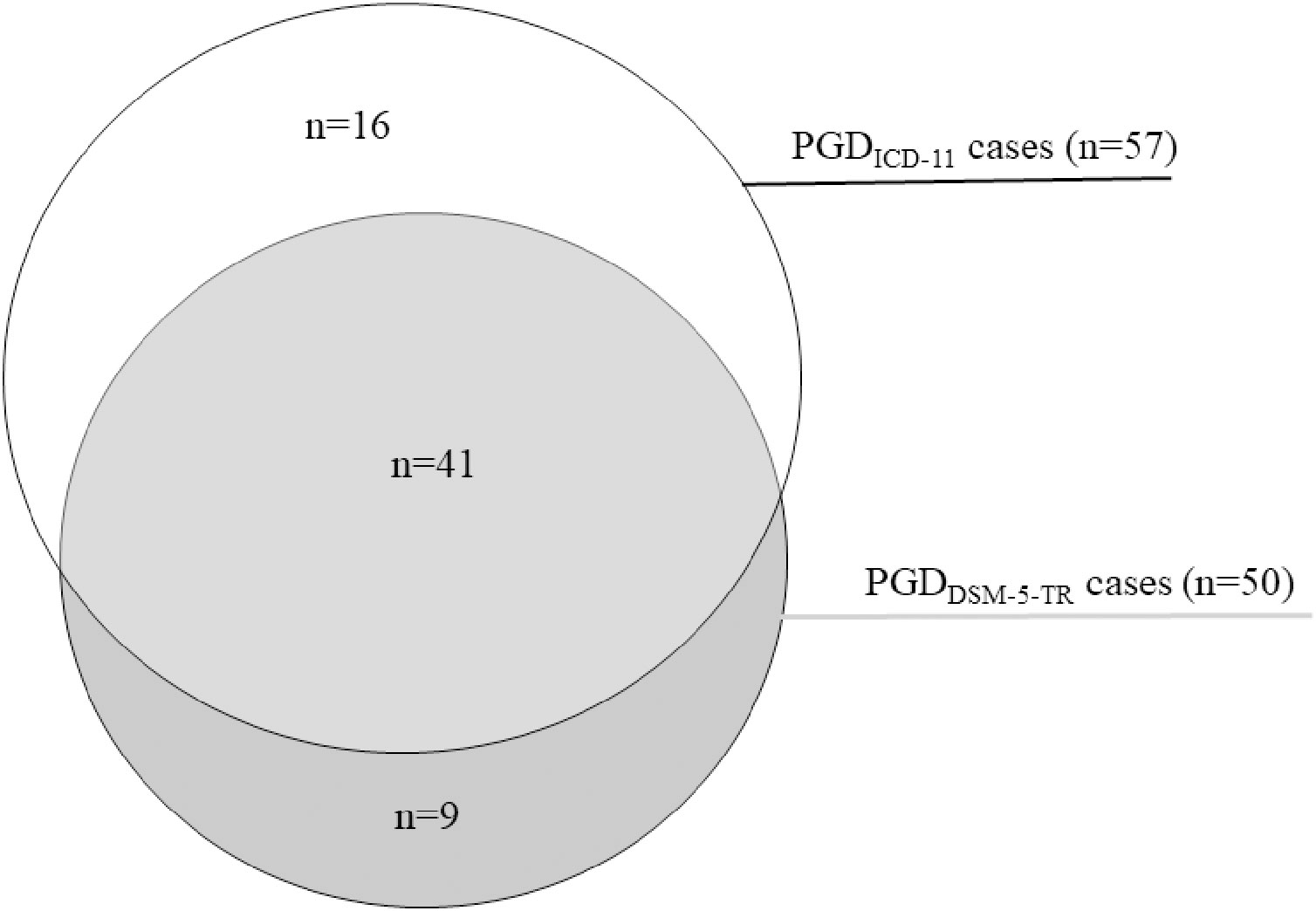
Figure 1 PGDDSM-5-TR cases vs. PGDICD-11 cases.
The most frequently indicated symptoms of the TGI-SR+ were having intrusive thoughts or images related to the person who died (30.7%), followed by longing or yearning for the person who died (23.4%), having trouble accepting the loss (23.3%) and feeling stunned, shocked, or dazed by his/her death (19.6%; see Table 2). Functional impairment due to the death was reported by 8.9% (n=94).
When simply examining time since the loss (i.e., six months) instead of symptom duration, the prevalence of PGD using the ICD-11 criteria B, C, and D, here referred to as PGDICD-11-6M increased to 6.8% (n=72), which is significantly higher than the rate of 5.4% for PGDICD-11 (Fisher’s exact test, p <.001) and higher than the rate of 4.7% for PGDDSM-5-TR (Fisher’s exact test, p <.001). Within the population-based sample (including non-bereaved), the prevalence increased to 2.9%. The pairwise agreement between PGDDSM-5-TR and PGDICD-11-6M with time since loss six months was substantial with κ = 0.81, 95% CI [0.73-0.89]. There were no unique PGDDSM-5-TR cases and 22 unique PGDICD-11-6M cases. The remaining 50 participants (4.7%) met both PGD criteria (see Figure 2).
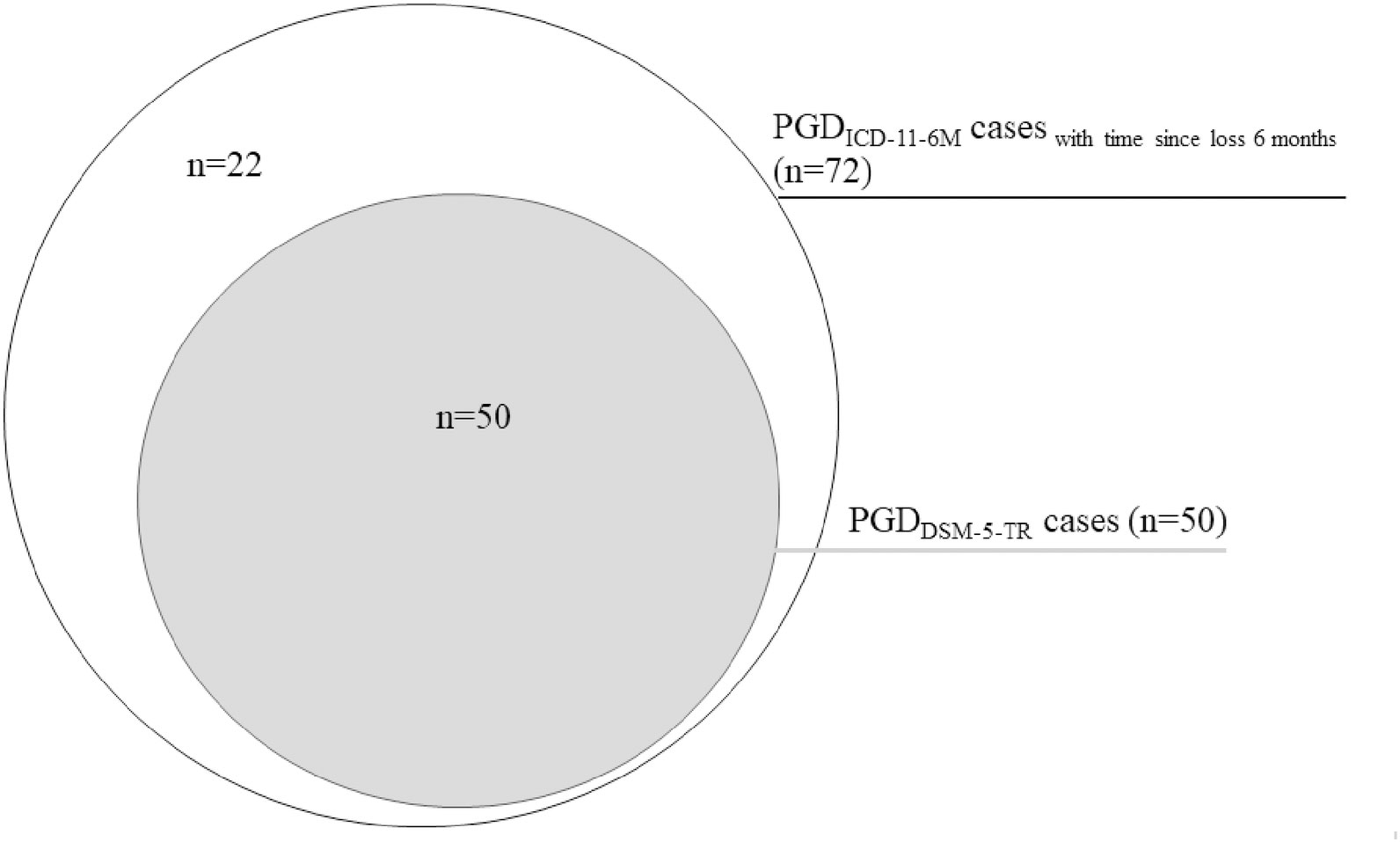
Figure 2 PGDDSM-5-TR cases vs. PGDICD-11-6M cases.
The number of required diagnostic criteria for PGDICD-11 was subsequently increased in additional analyses. The conditional prevalence decreased from 5.4% with one accessory symptom to 0.9% with seven accessory symptoms (see Table 5). The highest pairwise agreement with PGDDSM-5-TR was achieved when the number of accompanying symptoms was increased to 3 with κ = 0.79, 95% CI [0.70-0.88]. Increasing the number of accompanying symptoms to 3 for a PGDICD-11 diagnosis led to a prevalence of 4.7% (n=50). There were 10 unique PGDDSM-5-TR cases and 10 unique PGDICD-11 cases in this case. The remaining 40 participants (3.8%) met both PGD criteria (see Figure 3).
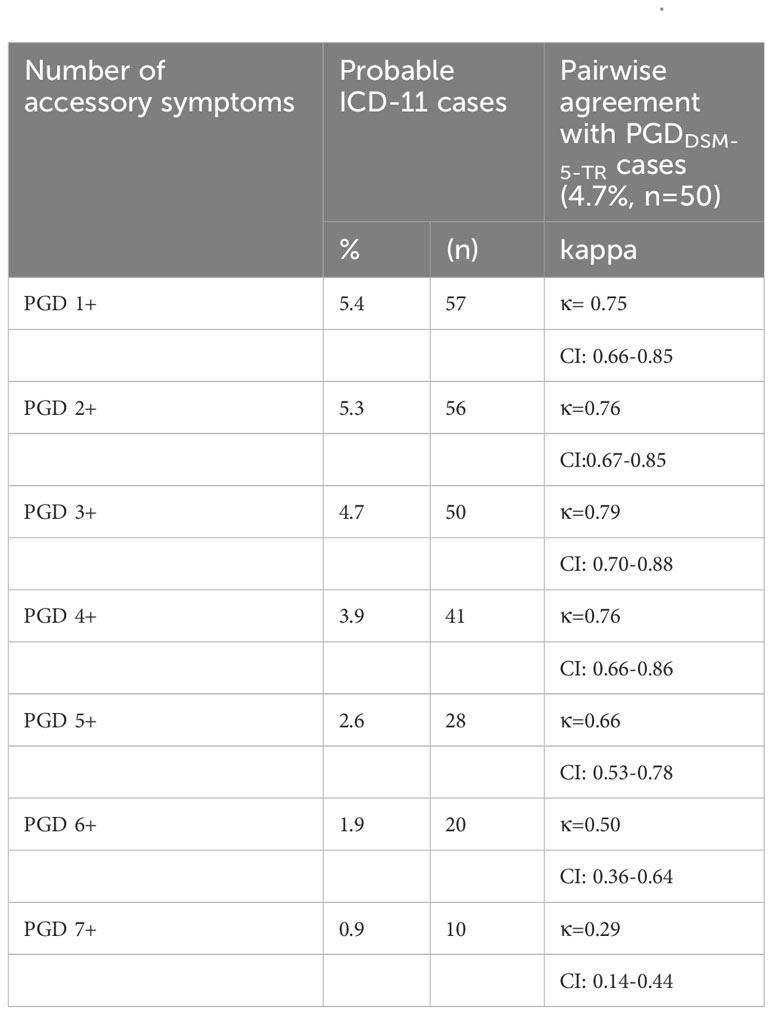
Table 5 The prevalence rate of PGDICD-11 with increasing numbers of accessory symptoms and pairwise agreement with PGDDSM-5-TR.
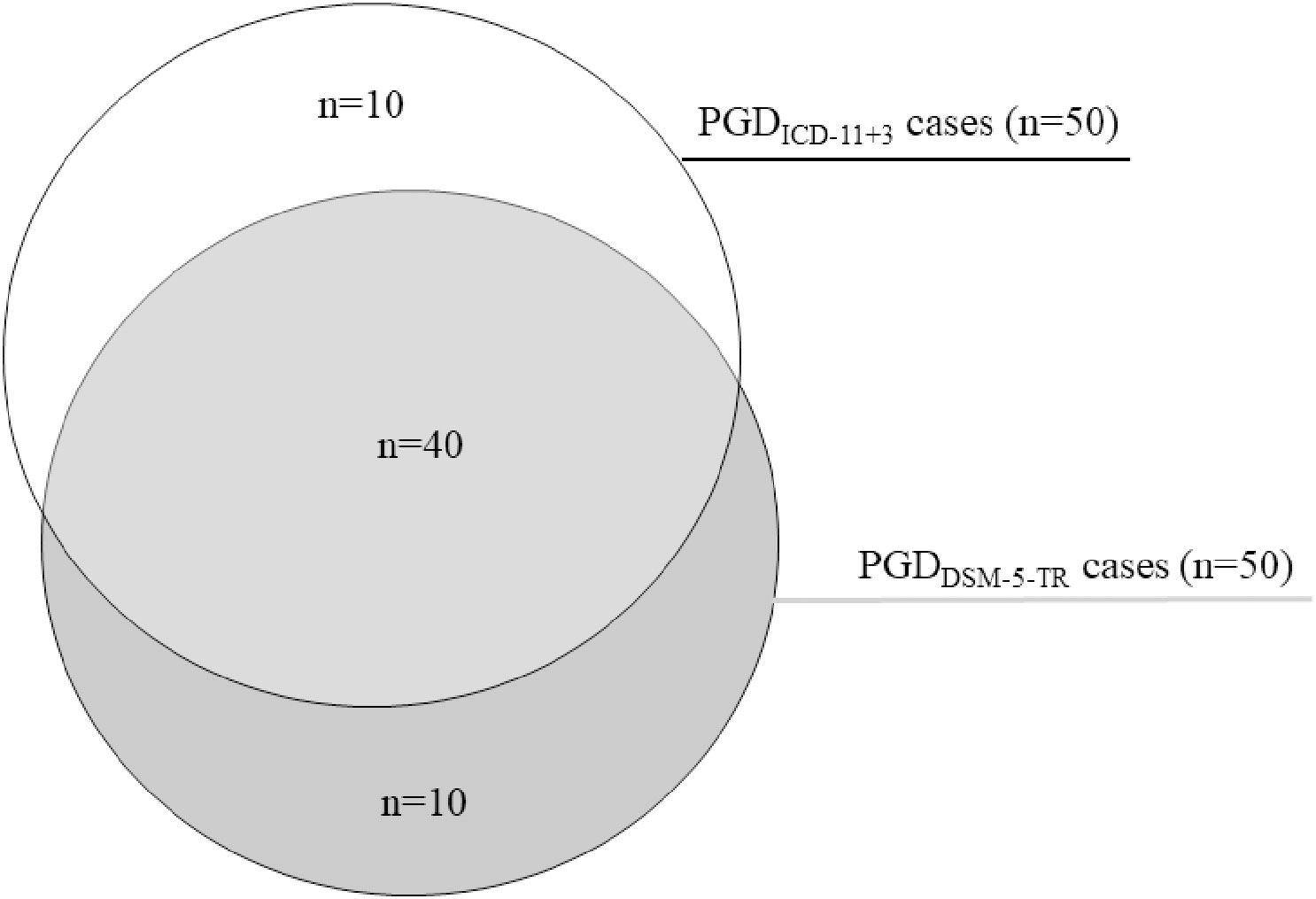
Figure 3 PGDDSM-5-TR cases vs. PGDICD-11+3 cases with 3 additional symptoms.
Discussion
One aim of this study was to estimate the probable point prevalence of PGD using a validated instrument designed to capture the DSM-5-TR and ICD-11 criteria sets and evaluate their diagnostic agreement in a population-based sample. Previous prevalence estimates were predominantly based on old criteria sets or outdated assessment tools. Previous studies also showed little content overlap between diagnostic criteria and found varying prevalence rates. Determining the optimal diagnostic threshold seems essential to avoid medicalizing normal grief and overestimating the prevalence of PGD.
The first main finding was a conditional prevalence of PGDDSM-5-TR of 4.7%, which was significantly lower than the rate of PGDICD-11 of 5.4%. These estimates are slightly higher than the ones found in other population-based studies by Rosner et al. (PGDDSM-5-TR 3.3%, PGDICD-11 4.2%) (14) and Treml et al. (PGDDSM-5-TR 3.4%) (23). These differences might emerge from the fact that both prior studies used outdated instruments designed for previous diagnostic sets, thus not assessing all criteria, while the TGI-SR+ used in the current study was specifically designed to capture all current diagnostic criteria sets. The pairwise agreement between criteria sets in the present study was substantial (κ = 0.75), with 3.9% of the bereaved meeting both PGD criteria. However, there were still nine unique PGDDSM-5-TR cases and 16 unique PGDICD-11 cases, demonstrating that there is a need for further convergence of the diagnostic criteria and their algorithm.
Another aim was to assess the frequency of occurrence of each symptom of prolonged grief. The advantage of the TGI-SR+ is that it captures not only the current diagnostic criteria but also former criteria for PGD such as PCBD or the criteria set proposed by Prigerson in 2009 (PGD2009), on which much research was based (4). The most frequently indicated symptoms were having intrusive thoughts or images related to the person who died (criterion B2, 30.7%) and longing or yearning for the person who died (criterion B1, 23.4%), which are considered the core criteria for PGD (15). The core criteria were followed by having trouble accepting the loss (23.3%). The last-mentioned symptom, however, is only a criterion within the ICD-11 and not listed within the DSM-5-TR, even though it was listed within all previous diagnostic criteria sets (for an overview see 15). Since this criterion is frequently reported, it could contribute to the higher prevalence rate of PGDICD-11 compared to PGDDSM-5-TR. The next most common symptom, reported by nearly 20%, was feeling stunned, shocked, or dazed by his/her death. This symptom originates from the previous PGD2009 diagnostic criteria by Prigerson (4). In their study, 19.2% indicated feeling stunned, shocked, or dazed about the death, which led the authors to propose this symptom as a diagnostic criterion for PGD. Every study using for instance the PG-13 or the Inventory of Complicated Grief (ICG) subsequently assessed this item as one of the diagnostic criteria. However, the symptom was later not included in the ICD-11 or DSM-5-TR. Some studies used the item “feeling stunned, shocked, or dazed by his/her death” to assess emotional numbness (e.g., 14). In the current study, only 14% reported emotional numbness, indicating that these symptoms might be similar but do not assess the same feelings.
The third aim was to investigate the difference between the time since loss and symptom duration for a PGDICD-11 diagnosis. The prevalence rate of PGDICD-11 was significantly higher when only the bereavement period rather than the symptom duration was examined (6.8% vs 5.4%). In this case, the diagnostic agreement between PGDICD-11-6M and PGDDSM-5-TR increased (κ = 0.81), since all individuals meeting the DSM-5-TR criteria were also enclosed when assessing the PGDICD-11-6M criteria, and there were no unique PGDDSM-5-TR cases (see Figure 2). However, this algorithm led to 22 unique PGDICD-11-6M cases and a high prevalence rate of 6.8%. This prevalence rate is likely an overestimation of the true prevalence since all people bereaved for six months who meet the minimum criteria according to ICD-11 are included, even those whose symptoms have persisted for a shorter period of time. This finding indicates that the bereavement period alone might not be a reliable indicator for PGD but rather the symptom duration. Only considering bereaved with symptoms for at least six months leads to a much smaller and presumably more precise estimate that corresponds more closely to the DMS-5-TR. Nevertheless, the intersection between PGDICD-11 and PGDDSM-5-TR still needs improvement. For the clinical practice, we recommend assessing the symptom duration as a vital part in diagnosing PGD instead of simply assessing the bereavement period.
The last aim was to determine which PGDICD-11 algorithm results in the greatest concordance with PGDDSM-5-TR when varying the number of required accessory symptoms for a PGDICD-11 diagnosis. The results show that the highest agreement with PGDDSM-5-TR was achieved when the number of accompanying symptoms for a PGDICD-11 diagnosis was increased to 3, which resulted in a lower prevalence of 4.7%. This result aligns with other studies that demonstrated that the minimal criteria of PGDICD-11 might be too liberal, as they lead to relatively high prevalence rates (20, 24), and a more conservative scoring rule might be beneficial. For instance, Rosner and colleagues found the highest agreement between both criteria sets with four accessory symptoms (14), while others recommend even five or more accessory symptoms for a PGDICD-11 diagnosis (22, 24). Increasing the accompanying symptoms for a PGDICD-11 diagnosis leads to a better agreement with PGDDSM-5-TR, and in our case, even to the same prevalence rate. Nonetheless, there were still 10 unique PGDDSM-5-TR cases and 10 unique PGDICD-11 cases, indicating that there is still variability within the groups of people meeting grief disorder criteria. A less heterogeneous diagnosis would be more beneficial for clinical practice and research.
Taken together, our results have implications for clinical practice. PGD is a serious disorder in the general population that is associated with significant impairments. Healthcare providers should be aware of the diagnosis and screen for it if indicated. However, this should be done using up-to-date measurement tools that capture the current diagnostic criteria, such as the TGI-SR+. When diagnosing PGD, the symptom duration, in particular, should be taken into account. Furthermore, the minimum criteria according to ICD-11 seem to be too liberal, as they lead to relatively high prevalence rates, and a more conservative scoring rule seems appropriate in order to avoid misdiagnosis.
Our findings have to be interpreted in light of some limitations. First, our results are based on self-reported data rather than clinician-administered structured interviews. The exclusive use of self-report measures could have led to bias due to misinterpretation of questions. Furthermore, a cross-sectional design was applied, eliminating any causal conclusions and conclusions about the stability of prolonged grief symptoms. Since grief naturally fluctuates in response to external stressors (e.g., anniversaries, birthdays, holidays), a longitudinal approach using multiple assessments beyond six and twelve months might be more appropriate to avoid diagnosing temporary distress. In our study, the data was collected between October and December, i.e. in some cases shortly before Christmas, which could be such an external stressor. However, the question of whether the symptoms have persisted for at least six months may provide some indication of symptom stability. Additionally, our results regarding the prevalence might be specific to the German general population. Hence, attempts should be made to replicate the findings in different cultures, in order to confirm the generalizability of our findings to other populations. Lastly, general mental health problems and psychiatric comorbidities were not examined. Therefore, the extent to which possible comorbid psychopathology influenced the results is unknown, challenging the interpretation of the results.
A major strength of the current study is the population-based setting, with a sample constructed to be representative in terms of age, gender, and education. The representativeness of the sample is especially relevant since most studies on PGD include predominately female participants leading to an underrepresentation of men.
The results demonstrate that the prevalence of PGD varies significantly depending on the application of the diagnostic algorithm and criteria. The prevalence ranged from 4.7% for PGDDSM-5-TR to 5.4% for PGDICD-11 to even 6.8% for PGDICD-11-6M when only considering the bereavement period. Yet, at the same time, the diagnostic agreement between all sets was substantial. Increasing the accessory symptoms for a PGDICD-11 diagnosis to 3 lowered the prevalence to 4.7%, which is equivalent to the DSM-5-TR prevalence. However, the overlap between the two systems could to be improved by harmonizing the criteria. PGD remains a substantial disorder among the bereaved and should not be neglected by healthcare providers.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study and the procedures were approved by the local ethical review board (Leipzig University, Medical Faculty; AZ: 298/21-ek, 12.7.2021). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants themselves or by legal guardians/next of kin in case of minors.
Author contributions
JT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. KL: Data curation, Formal analysis, Methodology, Writing – review & editing. EB: Investigation, Methodology, Validation, Writing – review & editing. AK: Conceptualization, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We acknowledge the support by the Open Access Publishing Fund of Leipzig University and German Research Foundation within the program Open Access Publication Funding.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jordan AH, Litz BT. Prolonged grief disorder: diagnostic, assessment, and treatment considerations. Prof Psychol-Res Pract (2014) 45:180–7. doi: 10.1037/a0036836
2. Prigerson HG, Kakarala S, Gang J, Maciejewski PK. History and status of prolonged grief disorder as a psychiatric diagnosis. Annu Rev Clin Psychol (2021) 17:109–26. doi: 10.1146/annurev-clinpsy-081219-093600
3. Horowitz MJ, Siegel B, Holen A, Bonanno GA, Milbrath C, Stinson CH. Diagnostic criteria for complicated grief disorder. Am J Psychiatry (1997) 154:904–10. doi: 10.1176/ajp.154.7.904
4. Prigerson HG, Horowitz MJ, Jacobs SC, Parkes CM, Aslan M, Goodkin K, et al. Prolonged grief disorder: psychometric validation of criteria proposed for DSM-V and ICD-11. PloS Med (2009) 6:e1000121. doi: 10.1371/journal.pmed.1000121
5. Shear K, Simon N, Wall M, Zisook S, Neimeyer R, Duan N, et al. Complicated grief and related bereavement issues for DSM-5. Depress Anxiety (2011) 28:103–17. doi: 10.1002/da.20780
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Wash DC Am Psychiatr Publ (2013). doi: 10.1176/appi.books.9780890425596
7. Maciejewski PK, Maercker A, Boelen PA, Prigerson HG. “Prolonged grief disorder” and “persistent complex bereavement disorder”, but not “complicated grief”, are one and the same diagnostic entity: an analysis of data from the Yale Bereavement Study. World Psychiatry (2016) 15:266–75. doi: 10.1002/wps.20348
8. WHO. ICD-11. Prolonged Grief Disorder (2018). Available at: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1183832314 (Accessed April 14, 2021).
9. American Psychiatric Association. View and Comment on Recently Proposed Changes to DSM–5 (2020). Available at: https://www.psychiatry.org/psychiatrists/practice/dsm/proposed-changes/proposed-changes (Accessed April 13, 2021).
10. Prigerson HG, Boelen PA, Xu J, Smith KV, Maciejewski PK. Validation of the new DSM-5-TR criteria for prolonged grief disorder and the PG-13-Revised (PG-13-R) scale. World Psychiatry (2021) 20:96–106. doi: 10.1002/wps.20823
11. Eisma MC, Rosner R, Comtesse H. ICD-11 prolonged grief disorder criteria: turning challenges into opportunities with multiverse analyses. Front Psychiatry (2020) 11:752. doi: 10.3389/fpsyt.2020.00752
12. American Psychiatric Association. APA Releases Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) (2022). Available at: https://psychiatry.org:443/news-room/news-releases/apa-releases-diagnostic-and-statistical-manual-of (Accessed April 11, 2022).
13. Killikelly C, Maercker A. Prolonged grief disorder for ICD-11: the primacy of clinical utility and international applicability. Eur J Psychotraumatol (2017) 8:1476441. doi: 10.1080/20008198.2018.1476441
14. Rosner R, Comtesse H, Vogel A, Doering BK. Prevalence of prolonged grief disorder. J Affect Disord (2021) 287:301–7. doi: 10.1016/j.jad.2021.03.058
15. Eisma MC, Janshen A, Lenferink LIM. Content overlap analyses of ICD-11 and DSM-5 prolonged grief disorder and prior criteria-sets. Eur J Psychotraumatol (2022) 13:2011691. doi: 10.1080/20008198.2021.2011691
16. Boelen PA, Lenferink LIM, Nickerson A, Smid GE. Evaluation of the factor structure, prevalence, and validity of disturbed grief in DSM-5 and ICD-11. J Affect Disord (2018) 240:79–87. doi: 10.1016/j.jad.2018.07.041
17. Bryant RA, Bawaneh A, Giardinelli L, Awwad M, Al-Hayek H, Akhtar A. A prevalence assessment of prolonged grief disorder in Syrian refugees. World Psychiatry (2021) 20:302–3. doi: 10.1002/wps.20876
18. Zhou N, Wen J, Stelzer E-M, Killikelly C, Yu W, Xu X, et al. Prevalence and associated factors of prolonged grief disorder in Chinese parents bereaved by losing their only child. Psychiatry Res (2020) 284:112766. doi: 10.1016/j.psychres.2020.112766
19. Lichtenthal WG, Maciejewski PK, Craig Demirjian C, Roberts KE, First MB, Kissane DW, et al. Evidence of the clinical utility of a prolonged grief disorder diagnosis. World Psychiatry (2018) 17:364–5. doi: 10.1002/wps.20544
20. Boelen PA, Lenferink LIM, Smid GE. Further evaluation of the factor structure, prevalence, and concurrent validity of DSM-5 criteria for persistent complex bereavement disorder and ICD-11 criteria for prolonged grief disorder. Psychiatry Res (2019) 273:206–10. doi: 10.1016/j.psychres.2019.01.006
21. Desatatis. Was ist der Mikrozensus? Stat Bundesamt (2023). Available at: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Haushalte-Familien/Methoden/mikrozensus.html (Accessed June 30, 2023).
22. Lenferink LIM, Eisma MC, Smid GE, de Keijser J, Boelen PA. Valid measurement of DSM-5 persistent complex bereavement disorder and DSM-5-TR and ICD-11 prolonged grief disorder: The Traumatic Grief Inventory-Self Report Plus (TGI-SR+). Compr Psychiatry (2022) 112:152281. doi: 10.1016/j.comppsych.2021.152281
23. Treml J, Brähler E, Kersting A. Prevalence, factor structure and correlates of DSM-5-TR criteria for prolonged grief disorder. Front Psychiatry (2022) 13:880380. doi: 10.3389/fpsyt.2022.880380
Keywords: prolonged grief disorder, ICD-11, DSM-5, bereavement, prevalence
Citation: Treml J, Linde K, Brähler E and Kersting A (2024) Prolonged grief disorder in ICD-11 and DSM-5-TR: differences in prevalence and diagnostic criteria. Front. Psychiatry 15:1266132. doi: 10.3389/fpsyt.2024.1266132
Received: 24 July 2023; Accepted: 19 January 2024;
Published: 08 February 2024.
Edited by:
Mushtaq Ahmad Margoob, Government Medical College (GMC), IndiaReviewed by:
Ajit Avasthi, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaAbdul Majid Gania, Sher-I-Kashmir Institute of Medical Sciences, India
Copyright © 2024 Treml, Linde, Brähler and Kersting. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Treml, anVsaWEudHJlbWxAbWVkaXppbi51bmktbGVpcHppZy5kZQ==