 Martin Blay1,2
Martin Blay1,2 Miguel Duarte3Marie-Alix Dessouli4Amaury Durpoix5
Miguel Duarte3Marie-Alix Dessouli4Amaury Durpoix5 Eva Rüfenacht3
Eva Rüfenacht3 Sébastien Weibel5,6Mario Speranza2,7
Sébastien Weibel5,6Mario Speranza2,7 Nader Perroud3*
Nader Perroud3*- 1ADDIPSY, Addictology and Psychiatry Outpatient Center, Santé Basque Développement Group, Lyon, France
- 2Centre de recherche en Epidemiologie et Sante des Populations Team ‘DevPsy’, INSERM, Universite Paris-Saclay, UVSQ, Villejuif, France
- 3Psychiatric Specialties Unit, University Hospitals of Geneva, Geneva, Switzerland
- 4Department of Emergency Psychiatry, University Hospital Edouard Herriot, Hospices Civils de Lyon, Lyon, France
- 5Department of Psychiatry, University Hospitals of Strasbourg, Strasbourg, France
- 6U1114, INSERM, Strasbourg, France
- 7University Department of Child and Adolescent Psychiatry, Versailles Hospital Center, Le Chesnay-Rocquencourt, France
- 8Department of Psychiatry, University of Geneva, Geneva, Switzerland
Emotion dysregulation (ED) has primarily been described in patients suffering from borderline personality disorder (BPD) and is an integral part of this diagnosis, but it is also a transdiagnostic construct that can be found in several other psychiatric disorders. The strong relationships between ED and BPD may lead clinicians to underestimate ED associated to other clinical contexts. This can lead to difficulties in diagnostic and treatment orientation, especially in the context of comorbidities. In this article, after reviewing the literature on the development and functioning of emotion dysregulation, and on the evidence for emotion dysregulation in eight disorders (borderline personality disorder, pathological narcissism with/without narcissistic personality disorder, obsessive-compulsive personality disorder, antisocial personality disorder, bipolar disorder, autism spectrum disorder, complex post-traumatic stress disorder, and adult attention deficit hyperactivity disorder), we present a transdiagnostic processual model of emotion dysregulation based on core triggers and interpersonal styles to try to address this issue and to provide a simple but technical tool to help clinicians in their diagnostic assessment and treatment orientation. By focusing more on typical patterns and interpersonal dynamics than only on categories, we believe that this model may contribute to the actual need for improvement of our current psychiatric classifications, alongside other well-studied and under-used dimensional models of psychopathology (e.g., HiTOP, AMPD), and may be useful to build more specific treatment frameworks for patients suffering from ED.
1 Introduction
Emotions can be defined as whole-body phenomena, that include changes in subjective experience, behaviors, and physiology, and that emerges in response to a specific object/situation perceived as relevant for oneself (1). On the other hand, emotion regulation can be defined as the way people attempt to influence this phenomenon, using different type of strategies (2). One of the most popular model of emotion regulation development and difficulties is the biosocial model developed by Marsha Linehan in patients suffering from borderline personality disorder (3). According to the latter, emotion dysregulation (ED) arises from the encounter of biological vulnerabilities (that include a lower threshold for emotion triggering, a larger increase in emotion intensity, and a slower decrease afterwards) with an invalidating environment, which can be defined as an environment that persistently ignores, disregards or punishes emotion expression. Invalidation ranges from pervasive minimizing and criticizing of emotional expression to physical and sexual abuse. Progressively in their development, these patients face more and more emotional crises, and start undergoing dysfunctional behaviors to regulate their emotions (including non-suicidal self-injury (NSSI), impulsive or suicidal behaviors or interpersonal conflicts), which may lead to the maintenance and/or aggravation of ED. This pioneer theoretical work has allowed the development of a manualized and validated therapy for BPD patients, Dialectical Behavioral Therapy (DBT), which has been shown to be effective notably in reducing self-harm behaviors or suicide attempts (4, 5). Finally, apart from DBT, other manualized treatments aiming to treat emotion regulation issues have been developed. These treatments, even though also focusing on emotion regulation, are often based on related but different conceptualizations of ED. The most studied remains mentalization-based therapy (MBT), another treatment initially developed for BPD patients, postulating that emotion dysregulation is linked to impairments in the development of mentalizing abilities (i.e., the ability to understand and process the combination of emotions, beliefs, intentions, thoughts and motivations that underlies our own and others’ behaviors) (6).
As mentioned earlier, ED has primarily been described in patients suffering from BPD, a disorder marked by important difficulties in emotion regulation (7). ED is an integral part of the borderline diagnosis, as emphasized by the presence of the construct and of its related symptoms (NSSI, recurrent suicide attempts, impulsive behaviors, interpersonal conflicts…) in the list of the 9 criteria. In this context, clinicians often associate these symptoms with the BPD diagnosis, and patients with ED often fulfill criteria for BPD, even if it is now well-known that ED can also be encountered in many other psychiatric disorders than BPD, and is currently considered as a transdiagnostic construct (8–10). In the field of personality pathology, patients suffering from pathological narcissism (PN) (with/without narcissistic personality disorder, NPD), obsessive-compulsive personality disorder (OCPD) and antisocial personality disorder (ASPD) may also present several of the above mentioned symptoms of ED (11–18). Apart from the field of personality disorders, ED can also be found in patients suffering from bipolar disorder [BD, (19, 20)], autism spectrum disorder [ASD, (21, 22)], complex post-traumatic stress disorder [cPTSD, (23)] and adult attention deficit hyperactivity disorder [ADHD, (24, 25)]. These disorders may therefore be diagnosed as BPD at the behavioral level, even though they don’t share BPD specific psychopathological issues. This could be linked with the high BPD comorbidity rates found in these disorders. Indeed, studies have reported a 37% prevalence rate of BPD in NPD patients, of 16.6% in OCPD patients, and of 21% in ASPD patients (26). Regarding bipolar disorder, empirical studies have found a 20% prevalence rate of BPD in patients with type II bipolar disorder (27). Regarding trauma, 25–30% of adults meeting criteria for either PTSD or BPD also meet criteria for the other disorder, and BPD is comorbid in 8-79% of cPTSD cases (23). Regarding neurodevelopmental disorders, prevalence rate of BPD is 27.2% in patients with adult ADHD (28) and between 0 and 10.6% in patients with ASD (29). Given these issues, when facing patients suffering from ED, the distinction between these disorders, BPD, and true comorbid presentations remains a common clinical challenge.
If categories are useful [because they offer important opportunities in terms of psychoeducation and treatment orientation, and because they provide a global meaning to suffering that patients can often easily understand (30)], the categorical approach has been the subject of large criticisms over the last decades. Indeed, describing mental health issues in taxa and categories (such as the DSM-5 does) is often considered as not supported by empirical data, the latter indicating that these issues should be considered dimensionally (31). These considerations have led researchers to develop new dimensional ways of conceptualizing psychopathology. One of the most developed dimensional conceptualization is the Hierarchical Taxonomy Of Psychopathology (HiTOP) model (32, 33). According to this model, psychopathology should be understood as a hierarchy of spectra. At the top of the model lies the super-spectrum dimensions, including the well-known general factor of psychopathology “p”, extensively studied and described by pioneer researchers like Caspi (34) and considered as underlying every dimension of psychopathology. These general dimensions can then be divided in several spectra (e.g., internalization, thought disorders, disinhibited externalization, antagonist externalization, detachment, somatoform), many being subdivided in several subfactors (e.g., the internalizing spectra can be divided into sexual and eating disorders, fear, distress and mania) (32). In order to cross these new conceptualizations with the most commonly used conceptualization of mental disorders (categories) and to make it more readable for non-specialists, the HiTOP model also indicates in which dimensions each of the well-known categories can be found, one category being not restricted to one dimension (e.g., the BPD category can be found both in the distress subfactor of the internalizing spectra and in the antagonist externalization spectra, which is representative of the large spectrum of expression this disorder may have). To note, the spectra constituting the model are still evolving, with several super-spectra being still described and proposed [e.g., (35, 36)]. Regarding the main subject of this paper (emotion dysregulation), some authors have described a possible “emotion dysfunction” super-spectrum, composed of the internalizing and somatoform spectra (36), emphasizing the transdiagnostic aspect of emotion regulation issues. Moreover, this movement of dimensionalization of mental health disorders also has its correlates in specific fields, for example in the personality disorder field with the development of dimensional models like the Alternative Model of Personality Disorders of the DSM-5 (7) or the ICD-11 model of personality disorders (37), both describing personality pathology as the association of both a general factor of personality functioning (criterium A) and up to 5 specific domains of personality traits (criterium B). However, these new models, although highly inspiring to overcome classic categorical approach, are currently hardly implemented in common clinical practice (32, 38), where categorical approach remains the most used, even though work groups are working on implementing dimensional approaches (32, 39). Finally, these models are also not free of criticisms, either on their overall utility [e.g., for HiTOP (40)] or on their representativeness of the clinical complexity of patients [e.g., for AMPD/ICD-11 (41)].
The fact that the main commonly used approach in clinical practice remains the categorical one may be particularly problematic in the context of ED. Indeed, these disorders have specific core psychopathological and interpersonal issues, and a confusion between them (or on which to prioritize in case of comorbidity) may have an impact on treatment orientation and outcomes. For example, BPD criteria (and thus emotion dysregulation symptoms) is thought to represent a general core feature of personality pathology severity and may be found in severe personality disorders more as an indicator of the level of personality functioning than as an indicator of underlying borderline processes (42). Thus, by focusing on a pure categorical approach, severe OCPD and NPD patients may be also diagnosed with BPD and may thus be seen as classic borderline patients, which may lead clinicians to miss core underlying issues and impact the course of treatment [given that, for example, pathological narcissism is associated with drop out in psychotherapy (43)]. Following the same rationale, when facing ASD patients with ED symptoms, clinicians may focus only on externalized symptoms (like NSSI or anger outbursts) and under-estimate typical autistic traits [e.g., cognitive rigidity, hypersensoriality), even though it seems important to take them into account in the treatment process (for example, some authors have suggested the importance of a quiet and stable environment in DBT programs for ASD patients (44)]. Moreover, when considering PTSD/cPTSD, an overfocus on associated ED-symptoms may also have consequences on treatment, given that – for example - several authors suggested that complex PTSD should be treated first when comorbid with BPD given that these patients are often too vigilant to be challenged (45). Finally, this could also have consequences in patients suffering from ADHD or BD, given the importance of medication in these disorders and the global consensus on its unusefulness in BPD (46).
In this context, we believe that a simple, transdiagnostic processual approach based on core triggers of emotion dysregulation (i.e., what specifically induces it in each disorder) could be useful for clinicians and could provide a complementary perspective to the classic categorical approach. We also believe that the investigation of recurrent and typical interpersonal issues could enhance such approach. Therefore, the aim of this paper is to describe this approach, after reviewing the literature on the development and functioning of emotion dysregulation, and on the presence and characteristics of ED in eight disorders (with a focus on the main relevant triggers and interpersonal styles): borderline personality disorder, pathological narcissism with/without narcissistic personality disorder, obsessive-compulsive personality disorder, antisocial personality disorder, bipolar disorder, autism spectrum disorder, classic and complex post-traumatic stress disorder, and adult attention deficit hyperactivity disorder. To note, this list is non exhaustive, as other disorders are linked to ED (e.g., substance use disorder). Our aim is to provide a simple and easy to implement transdiagnostic model of emotion dysregulation to help clinicians in their daily practice, in terms of diagnostic assessment, but also in terms of psychotherapeutic treatment orientation.
2 How does emotion (dys)regulation work and develop?
In the introduction, we described Marsha Linehan’s model of development and expression of emotion dysregulation. Even though this model has gained large audience over the last decades, notably linked to the efficacy of its associated psychotherapy to treat BPD, many other models, often more complex, have been built (and are currently improved) to better understand how emotion dysregulation works and how it develops in one individual (47). In this paragraph, we want to provide a larger picture of the literature regarding on how emotion regulation works and develops, and to present why we believe our trigger-based approach may be relevant with regards to these conceptualizations.
2.1 Emotion regulation development and processes
Emotions are adaptive. They are necessary for survival, allowing the subject to evaluate the significance of his/her environment for well-being, to organize behaviors to achieve and maintain this well-being, and to communicate about these goals (48). Emotions are generated when facing a situation considered relevant for oneself, leading to attentional focus on the important aspects of this situation, appraisal of these aspects in relation to one’s aims and goals, and finally to physiological and behavioral response (2). Thus, emotions should not be restricted to the physiological and behavioral response; and, as a corollary, emotion regulation (ER) should not be considered only as a rigid ability to regulate this response (49). Instead, ER can be better defined as a dynamic set of extrinsic and intrinsic processes responsible for monitoring, evaluating and changing the intensity and temporality of emotional reactions, that one’s uses to achieve his/her goals, taking into account social expectations (50). Such definition is more helpful and accurate as it encompasses the other domains of emotion generation and considers the context in which the emotion arises and the goals underlying emotion regulation. Several theoretical models have been developed to describe the different ways subjects engage in ER and determine which strategies are the most effective and adaptive (2). One of the most used is the process model of emotion regulation develop by Gross and colleagues (51). According to the latter, the ER cycle starts when there is a discrepancy between desired and actual emotional state. When facing such discrepancy, the subject 1°) identify the opportunity for regulation, and 2°) select and 3°) implement one or several of the 5 main emotion regulation strategies (namely, situation selection and modification, attentional deployment, cognitive change, and response modulation), the whole cycle being monitored for the efficacy of emotion regulation (2). This model, among other, allows clinicians to consider emotion regulation more holistically than models focusing only on emotional arousal.
But, if these dynamic processes are central for the subject’s adaptation to his/her environment, how do they develop in one individual? Even though this question is not fully answered and is still being studied nowadays (47), development and acquisition of emotion regulation during development is mostly considered as a complex and continuous phenomenon (52, 53). At birth and during the first months, toddlers, when activated, are only regulated by their environment (54). Then, progressively, the baby/child translate from being regulated by others (external regulation) to being self-regulated (internal regulation). This is allowed notably through progressive development of intra psychic strategies (i.e., attentional redirection, cognitive reevaluation), flexibility (i.e., ability to adapt the strategies to one context, possible use of multiple strategies), specification (i.e., ability to use specific strategies for each emotion/situation), and integration of social norms and goals (55). However, this development also relies on the type of environment in which the subject grows, and notably on the interaction with caregivers. Indeed, emotion regulation acquisition must also be considered under the light of attachment theory (56). Attachment can be defined as a universal and specific human need of security in relationships, notably between the new-born baby and his/her caregivers (56). Indeed, toddlers have the innate ability to seek closeness to the caregiver through skills allowing the mobilization of the caregiver’s interest and attention (e.g., crying, clinging, etc.). Normally, the caregiver is attracted and can therefore intervene to try to help the baby regulate his or her experience. Such regulation ability acquisition develops notably through contingent, congruent, and marked parental mirroring in early interactions. If these interactions are adequate, they will allow the child to feel safe enough to explore and learn from the environment around him/her, an aspect that is crucial for the development of emotion regulation abilities, notably because it confers the ability to learn how to select relevant information in the environment. On the other hand, when these interactions are inadequate, the child will experience low reliability and availability of the attachment figure, which impedes the possibility to securely explore the environment and to develop productive emotion regulation abilities (57, 58).
Altogether, emotions cannot be defined only as physiological and behavioral manifestations. They arise in specific, attention-grabbing, relevant situations, and their regulation is a complex process including identification of the opportunity to regulate, selection of the most relevant strategies, and implementation of these strategies. These abilities are built continuously during development, where subjects go from external regulation to internal regulation, this process requiring safe and adequate interactions with caregivers. But how can these processes go awry?
2.2 Development of emotion dysregulation
Emotion regulation is thus a core aspect of human experience and interactions, notably to attain and maintain well-being. However, this dimension can become problematic when an individual’s emotion regulation patterns impair developmental goals in short and/or long-term time frame (47). According to specialized literature, impairments are considered either when interfering with achieving short and/or longer term goals for well-being, when violating developmental expectations for appropriate behavior, or when violating sociocultural standards for emotion-related communication and behavior (47). Thus, emotion dysregulation is not necessarily characterized by having negative, overwhelming, or sustained emotions. Instead, the level of impairment depends on the context in which emotions arise and on how the subject deals between the well-being goals and the reality of the environment (47, 59). Indeed, some patterns can be adaptive in the immediate context but can become maladaptive at a larger time frame. For example, in the case a child whose parents punishes (e.g., through physical abuse) their offspring’s sadness expression, some pattern of emotion regulation (e.g., emotion suppression) can be efficient for short term goals (i.e., self-protection). However, these same patterns, learnt and integrated in a specific environment, may also become irrelevant when the child grows up and when the context changes (e.g., when the offspring leaves his/her parents’ house and start to build his/her adult life). Such emotion regulation patterns may therefore lead to impairments in long-term goals for well-being (e.g., inability to develop close relationships due to avoidance of situations requiring vulnerability expression). In this example, it is more the discrepancy between past emotion regulation patterns and actual context (e.g., less abusive and more secure social interactions) that lead to emotion dysregulation, rather than the strategy used or the intensity of emotions. Finally, the same observation can be made in terms of attachment. When early interactions and parental mirroring are inadequate, insecure attachment styles may develop. These attachment patterns (except for disorganized attachment) can be considered as adaptive reactions to real-life experiences, because they allow the subject to survive in an environment that does not fulfill his/her needs (56). However, this perceived absence of reliability and security of environment, when integrated, can become problematic when the context changes and when relational threats become less common.
Altogether, emotion dysregulation cannot be limited to the valence or intensity of the emotion arousal nor to a deficit in the use of emotion regulation strategies. Instead, emotion dysregulation can be better understood as a mismatch between 1°) specific emotion regulation patterns developed to fulfill well-being goals in a specific environment and 2°) the reality of the actual environment, that need different emotion regulation patterns to fulfill short and long-term well-being goals.
2.3 Specificities in terms of triggers of emotion dysregulation
It is important to note that the considerations we presented in this section are general and not restricted to clinical population. However, emotion dysregulation is a transdiagnostic risk factor for psychopathology (60, 61) and it can be found in a large number of psychiatric disorders (8). At this point, readers may ask how these processes (i.e., process model of emotion regulation, context-dependent conceptualization of emotion dysregulation…) can be differentially impaired in a way that leads to different categories of psychopathology. Such important question may require large theoretical and empirical works to be fully answered. Here, we will only focus on the aforementioned conceptualizations, and describe how, in our perspective, the triggers we present below can be understood under this lens.
First, emotion dysregulation may develop and express differentially depending on the actual biological and neurocognitive background associated with the disorder. This may be particularly relevant (but not exclusively) for neurodevelopmental and bipolar disorders. Indeed, depending on underlying neurocognitive functioning, the identification of relevant situations and/or the access to the five main emotion regulation strategies could be impaired. For example in ASD patients, as suggested elsewhere (22, 62), impaired ability to filter environmental stimuli may impact the ability to adequately identify and select relevant situations, and intolerance to change and cognitive rigidity may be associated with a lower ability to use cognitive change strategies. These neurocognitive specificities, and their associated emotion regulation issues, may lead to specific hypersensitivities/triggers in this population. The same rationale may also be applied for ADHD and bipolar disorders, where disorders’ associated executive function deficits also impact emotion regulation processes (63, 64). Altogether, if the classic processes at play in emotion regulation can be impaired by neurocognitive deficits, and if different disorders have different types of neurocognitive alterations, it seems plausible to assume that each disorder may be associated with specific patterns of emotion regulation dysfunction and specific hypersensitivities/triggers, depending on the underlying neurocognitive impairments. This aspect could be the first level of analysis when considering disorders’ specificities in emotion dysregulation.
Second, emotion dysregulation may develop differentially depending on the context in which emotion regulation abilities were developed. This may be particularly relevant (but not exclusively) for personality disorders or cPTSD. Indeed, depending on the type of environment the patient grew up, he/she may be confronted to different types of interpersonal threats, attachment issues, and may develop different types of emotional strategies to attain immediate well-being. All these aspects may foster different types of sensibilities. For example, a patient growing up in a familial context punishing failures, weaknesses, and communicating either directly or indirectly that one cannot be loved if failing, may be at a higher risk for specific sensibilities related to self-esteem. Thus, situations that may not be considered as relevant in terms of self-esteem by most people (e.g., not being congratulated for work) may be identified as so by the subject and may trigger emotion generation. Moreover, in such invalidating context, the patient may be at higher odds of developing emotion regulation strategies like emotional suppression (to not communicate vulnerabilities) and avoidance of difficult situations (to avoid failure). These patterns of emotion regulation could be thus considered adaptive in such environment, to attain immediate well-being (e.g., less punishment and critics, more closeness to caregivers). However, these same patterns (e.g., never showing vulnerabilities, avoiding difficulty) may also become maladaptive in a less adverse environment (e.g., in a social sphere where defaults are not punished or criticized). Altogether, such patient, by experiencing emotion generation more often when facing self-esteem threats, and by maintaining the use of formerly adaptive emotion regulation patterns, may be impaired (e.g., having repeated conflicts in workplace, frequent job quitting) in his/her ability to fulfill long-term well-being goals (e.g., building a career), which could lead to the diagnosis of pathological narcissism. In resume, the environment development and the context in which emotions arise may influence how emotion regulation develops and expresses, which may once again lead to different ways of emotion regulation dysfunction, and to different hypersensitivities/triggers. This aspect could be the second level of analysis when considering disorders’ specificities in emotion dysregulation.
Even though our review may be seen as oversimplifying and partial, we believe that these two dimensions (the influence of underlying neurocognitive impairments and of the type of environment in which emotion regulation abilities developed) could – at least partly- explain the different in terms of triggers of emotion dysregulation between the 8 disorders we will present in the paragraph 3. Moreover, given that these triggers could be seen as the expression of different impairments in the emotion regulation cycle, the trigger-based psychotherapeutic approach we present in paragraph 5 may also be relevant to target these specific impairments indirectly but more specifically, compared to general approaches focusing on the whole cycle that may miss each disorder specificities.
3 Emotion dysregulation, triggers and interpersonal style
In this paragraph, we will review the evidence regarding emotion dysregulation in the aforementioned disorders, with a focus on specific triggers and interpersonal styles. A summary can be found in Table 1.
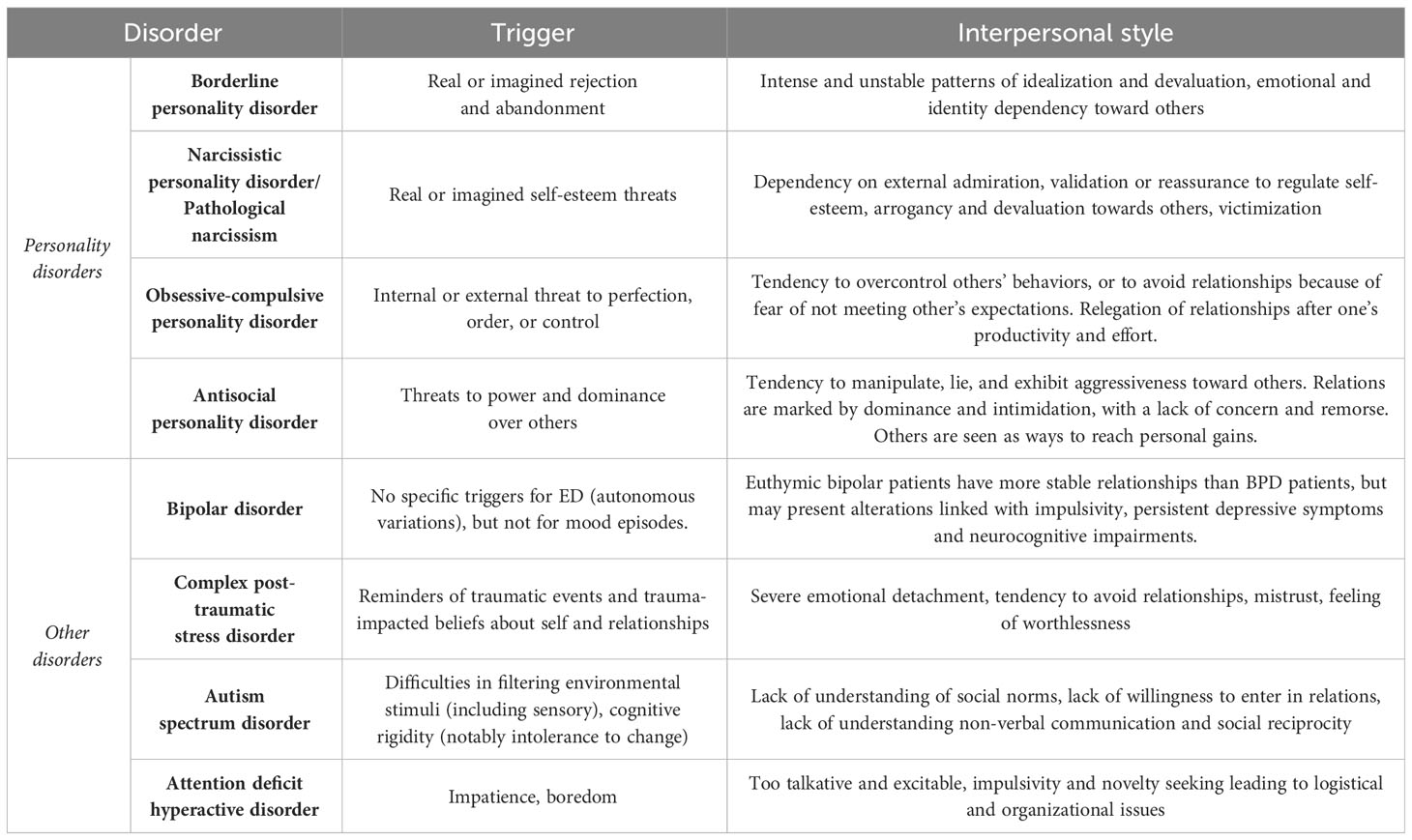
Table 1 Summary of specific triggers and interpersonal styles.
3.1 Personality disorders
3.1.1 Borderline personality disorder
Borderline personality disorder (BPD) is a common and potentially severe personality disorder that affects around 1.6% of the general population (65). It is characterized by difficulties in emotion regulation, with an unstable sense of identity and intense and conflictual interpersonal relationships, associated with impulsive behaviors, self-harm, and repeated suicide attempts (7). Even though different conceptualizations of the disorder have been described over the last decades (3, 6, 45, 66, 67), several authors have emphasized that the core trigger of BPD symptoms is fear of rejection and abandonment (45, 68). When considering interpersonal style, the specificity of BPD patients lies in hyperintense and unstable relationships, with fluctuations between idealization and devaluation of others and concomitant fluctuations in emotions and sense of identity, dimensions that are mainly associated with the perceived quality of the interpersonal relationships. In this context, patients suffering from BPD can often threaten or beg others to not abandon them, with sometimes the use of self-harm or suicidal threats to avoid abandonment (45, 65).
3.1.2 Narcissistic personality disorder/pathological narcissism
Narcissism is a normal and important psychological function that describes one’s capacity to regulate self-esteem without relying on social environment validation or self-enhancement. Development of normal narcissism is a continuous phenomenon that may be altered, thus resulting in the development of pathological narcissism, that may be defined as significant deficits in self-esteem regulation and use of maladaptive strategies to cope with self-esteem threats (69). Two non-exclusive forms of pathological narcissism (depending on the patient’s reaction when facing self-esteem threats) have been described. Grandiose narcissism is characterized by a tendency to use self-enhancement, entitlement, fantasies of power and fame and exploitative or aggressive behaviors, whereas vulnerable narcissism is more characterized by internalized feelings of shame, depression, with a tendency to self-criticism, social withdrawal, and a heightened risk of suicidal attempts (69, 70). From a categorical perspective, the related disorder of the DSM is narcissistic personality disorder (NPD), with a prevalence in general population up to 1% (71). Many criticisms has emerged regarding the clinical validity of the NPD diagnosis, given its overemphasis on narcissistic grandiosity and the lack of consideration of narcissistic vulnerability, which may explain its low prevalence rate compared to the prevalence of pathological narcissism as a construct in clinical practice (69, 72). Narcissistic patients also struggle with emotion dysregulation (13, 17, 73), especially with emotion like anger/rage, shame and envy (74), and show several ED-related behaviors [e.g., NSSI (12)]. According to current research, the main trigger of emotion dysregulation in narcissistic patients is real or perceived self-esteem threats (75). Moreover, regarding interpersonal style, as emphasized by the alternative model of the DSM-5 (7), the specificity of narcissistic patients lies in the place given to relationships, that often exist mainly to regulate self-esteem, with excessive reference to others for self-definition, goal setting based on gaining approval from others, over-sensitivity to others’ reactions (but only if they are perceived as relevant to oneself), and with a tendency towards arrogancy, devaluation of others and victimization when feeling threatened.
3.1.3 Obsessive-compulsive personality disorder
OCPD is the most frequent personality disorder that affects around 4.3% of the general population (76). It is associated with a significant number of psychiatric comorbidities, including anxiety and mood disorders, even though OCPD patients have a better clinical functioning than patients with BPD (77, 78). According to several experts, OCPD is a disorder characterized by difficulties in tolerating loss of control, imperfection or disorderliness (79), and OCPD patients can be separated in two subtypes: anxious type (reacting to control threats with self-criticism, anxiety, worrying, procrastination and social avoidance) and controlling type (reacting to control threats with detachment, irritability, criticisms and judgment, or anger) (80). Moreover, patients with OCPD also struggle with high perfectionism, with a sense of self-worth overdependent on striving and achievement that leads to counterproductive behaviors and self-criticism when these patients fail to meet the inflexible standards they place on themselves (81). Thus, when facing internal or external threats to control or meeting their high standards, these patients (mostly – but not exclusively – the controlling type) may experience emotion dysregulation and related symptoms, like interpersonal issues or self-harm (11, 18, 82). Regarding interpersonal style, OCPD specificity lies in the view of relationships as secondary to work and productivity, with rigidity and stubbornness combined with high moral standards for others when these patients enter in relation (controlling type), or with a tendency to be submissive, self-critical and over-attentive to not meeting expectations of others (anxious type) (7, 79).
3.1.4 Antisocial personality disorder
ASPD is one of the most common personality disorder in the general population, with a prevalence rate around 3% (76), and is described in the DSM-5 as a « pervasive pattern of disregard for and violation of the rights of others », with clinical features such as failure to conform to social norms with aggressiveness, deceitfulness and lack of remorse (7). It is associated with increased morbidity (both psychiatric and somatic) and mortality (with – for example – 4 to 5% of ASPD patient completing suicide) (83). It is also associated with extended harm and large societal costs, notably due to aspects like interpersonal aggressiveness & criminality (84). ASPD patients are also well-known to be prone to emotion dysregulation and related aspects like NSSI or impulsive behaviors (15, 16). Regarding triggers, ASPD seems to be specifically triggered by threats to power and dominance over others (e.g., by hierarchy, societal norms or barriers to obtain personal gains), which can be linked to fear of exploitation and victimization by others and to fundamental beliefs such as « I should hurt him before he hurts me » (85). Regarding interpersonal styles, as emphasized by the AMPD, the specificity of ASPD patients lies in a tendency to manipulate, lie to and sometimes aggress others, in order to maintain dominance and intimidation, with a clear lack of concern and remorse about negative effects on others, that are often seen as ways to fulfill personal needs (7).
3.2 Other disorders
3.2.1 Bipolar disorder
Bipolar disorder (BD) is a common and severe psychiatric disorder that can be defined as the presence of manic episodes (type I), or the concomitant presence of hypomanic and depressive episodes (type II) (7). It has an overall lifetime prevalence of 0.6% for bipolar type I and 0.4% for bipolar type II (86), and it is associated with significant impairment in professional, social, and familial functioning (87). BD patients also often struggle with emotion dysregulation (19), and engage in ED-related behaviors like NSSI (88), impulsive and suicidal behaviors (89). Notably, emotion dysregulation can be found in euthymic bipolar patients (90). Specific triggers are often found in mood episodes (91, 92), with some authors suggesting different types of triggers for depressive and manic episodes. However, regarding emotion dysregulation and affective instability, several authors have proposed that ED in BD patients may not have specific triggers compared to patients with BPD, with emotional swing being quite autonomous and non-driven by specific types of interpersonal or intrapsychic events (27). Moreover, regarding interpersonal style, euthymic bipolar patients are thought to be able to maintain relatively stable relationships compared to BPD patients (93), with a lower tendency to avoid relationships due to fear of rejection (27, 94). However, interpersonal functioning can also be altered in euthymic bipolar patients, notably linked to impulsivity, persistent depressive symptoms, and persistent neurocognitive impairment (95, 96).
3.2.2 Complex post-traumatic stress disorder
Post-traumatic stress-disorder (PTSD) is a common mental disorder affecting around 5.6% of the general population (97) and is defined in the 11th version of the ICD (37) as the occurrence of three symptoms clusters after the onset of a traumatic event: re-experiencing, avoidance of reminders, and a perception of heightened current threat (98). However, observation of chronically traumatized patients that experienced repeated physical or sexual abuses have underlined that these patients often present more complex presentations than classic PTSD patients due to an effect of prolonged traumatisms on self-organization (99). To address this issue, a new diagnosis of complex post-traumatic stress disorder (cPTSD) has been introduced in the ICD-11 and can be defined as the association of classic PTSD symptoms with severe and persistent disturbances of self-organization (DSO, namely, problems in affect regulation, beliefs about oneself as worthless, accompanied by feelings of shame, guilt or failure related to the traumatic event, and persistent difficulties in sustaining relationships and in feeling close to others (100). cPTSD affects around 1 to 8% of the general population and up to half of the patients in clinical population (100). Given that chronically traumatized patients are also at risk of developing borderline personality disorder, that cPTSD and BPD share clinical symptoms (notably the DSO symptoms), and given the important comorbid rates between the two disorders (101), there has been a large debate on the differences between the two disorders, with some authors proposing cPTSD as an alternative diagnosis for BPD patients (102) while other emphasizing the concurrent validity of the two diagnoses (103).
Recently, Ford & Courtois reviewed the existing literature on the link between PTSD, cPTSD and BPD and summarized important information regarding differences in comorbidity, neurobiology, and in several clinical dimensions including emotion dysregulation (23). Notably, they described emotion dysregulation in BPD as a difficulty in regulating intense distress related to real or perceived abandonment (the main trigger that we presented earlier), whereas emotion dysregulation would be better described as a difficulty in regulating trauma-related distress, primarily due to trauma-impacted beliefs about self and relationships in cPTSD. Moreover, regarding interpersonal style, authors describe cPTSD patients’ interpersonal style as a severe emotional detachment and tendency to avoidance in relationships, often marked by mistrust and feeling of worthlessness, while BPD interpersonal style is more characterized by intense fluctuations and tendency to interpersonal dependency (an aspect that we also described earlier) (23, 100).
3.2.3 Autism spectrum stress disorder
Autism spectrum disorder (ASD) is a common and heritable neurodevelopmental disorder affecting around 1% of the general population that consists in impairments in social communication and interaction, hypersensoriality, stereotypic behaviors, sometimes associated with intellectual disability (104). Even though it is not a core symptom, emotion dysregulation has been found to be an important symptom in ASD patients (22, 105). Moreover, patients with ASD are also at risk for ED-related behaviors like self-harm or anger outbursts (21, 44). Regarding this issue, several authors has hypothesized that ASD patients may experiment ED in relation to core deficits of the disorder, such as difficulties in filtering environmental stimuli (including sensory) and cognitive rigidity (notably intolerance to change) (22, 105). Moreover, ASD patients’ interpersonal style is typically characterized by lack of understanding of social norms, lack of willingness to enter in relations with others that do not share their restricted interests, and with trouble understanding non-verbal communication and social reciprocity.
3.2.4 Adult attention deficit hyperactive disorder
Attention-deficit hyperactivity disorder (ADHD) is a valid and recognized neurodevelopmental disorder affecting around 2.8% of the adult population (106) and is characterized by hyperactive-impulsive and/or inattentive symptoms with onset in childhood, before 12 years old (7). ED is considered as a central symptom of adult ADHD (25, 107), and several authors have emphasized its central role in externalizing behaviors and functional impairment in social and professional spheres (8, 25, 107). When looking at ED triggers in adult ADHD, we believe – as suggested by some authors (25) - that impatience and boredom are the most relevant one, especially in patients with hyperactivity, even though this aspect has not specifically been studied to our knowledge. Moreover, regarding interpersonal style, preliminary studies have found that ADHD patient often has difficulties caused by executive functioning difficulties, with troubles to keep contact with peers due to their impulsivity and novelty seeking, and with a global tendency to be perceived as too talkative and excitable (108).
4 Integration of current approach in diagnostic assessment
This model provides a simple clinical tool to help clinicians who are not familiar with the current literature on emotion dysregulation to better orientate their treatment by focusing more on the main difficulties rather than only on categories. In this paragraph, we will provide preliminary clinical diagnostic assessment guidelines for clinicians facing a patient with emotion dysregulation as the main complaint. A summary of these guidelines can be found in Figure 1.
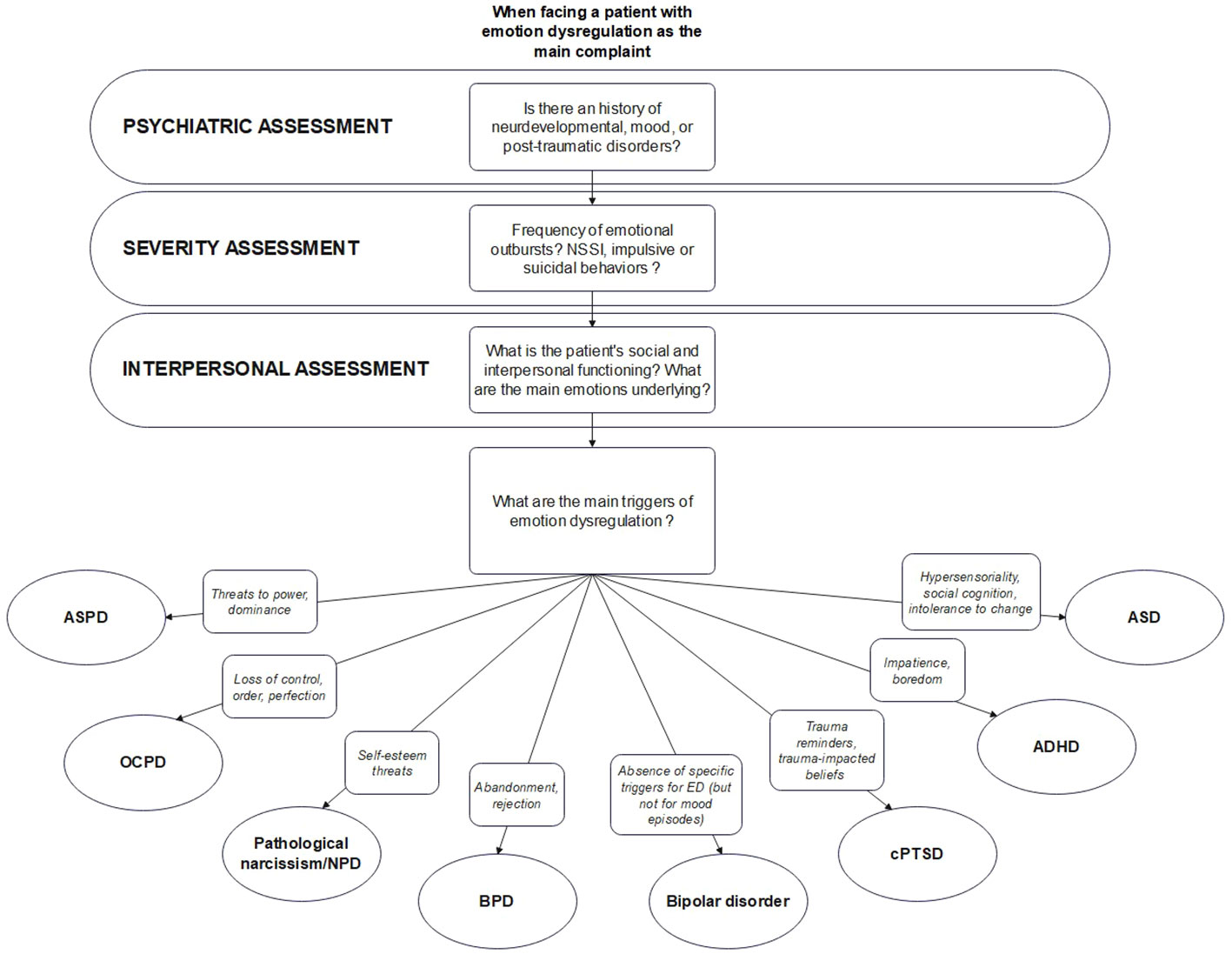
Figure 1 Sumary of our processual approach. ADHD, attention deficit hyperactivity disorder; ASD, autism spectrum disorder; BPD, borderline personality disorder; cPTSD, complex post-traumatic stress disorder; NPD, narcissistic personality disorder; OCPD, obsessive-compulsive personality disorder.
When facing a patient whose chief complaint is emotion dysregulation, clinicians should start by systematically assess past/actual mood episodes (with an emphasis on the length of the episodes to avoid confusing mood and emotional swings), traumatic events (with or without post-traumatic stress syndrome), presence of autistic traits (including stereotypic behaviors and restricted interests), hyperactive or inattentive symptoms (appearing in childhood) or other neurodevelopmental issues (including learning disabilities) in their classic psychiatric examination. Then, clinicians should go further by assessing ED severity, notably through the investigation of the frequency of emotional outbursts and the presence/frequency of ED-related behaviors. Notably, clinicians should search for non-suicidal self-injuries [like cutting, biting, hitting, burning, scratching, but also less studied behaviors like high number of body modifications, especially tattoos and piercing, as they are linked to emotion dysregulation and are thought to be socially acceptable forms of NSSI by some authors (109)], impulsive behaviors in response to emotional outbursts (sexual endangerment, eating disorder, substance use, reckless driving and other types of orderly behaviors) and suicidal ideations/attempts. If present, each of these elements should be carefully explored in term of potential legal or physical consequences, notably somatic, especially for impulsive behaviors. This exhaustive behavioral assessment could be of great interest to estimate the potential severity and dangerousness of the syndrome. Then, when a clear behavioral picture is available, clinicians should continue by assessing social and interpersonal functioning, including patient’s perception and understanding of others, satisfaction and interest in social interactions, number of significant relationships, avoidance of social situations (with motives), and occurrence of conflicts (with motives). We believe that clinicians should put a large emphasis on the patients’ emotions typically associated with interpersonal interactions, like shame, anger, fear or guilt, and should try to understand how these emotions may be linked with ED-related behaviors. Finally, after this overall assessment, clinicians could start to focus on the underlying emotional triggers.
After a presentation of the main triggers listed in Table 1, and using all the information that has emerged throughout the interview (notably on psychiatric history and interpersonal style), clinicians could start a collaborative discussion with the patient and try to estimate the most important aspects that are triggering emotional crises. Once the main triggers are identified and linked with psychiatric history and interpersonal styles, clinicians should discuss with the patient how to hierarchize them, in order to target the most debilitating (i.e., that is the most commonly found in emotional crises) and to start to set treatment framework.
5 Trigger-based treatment orientation: general vs. specific interventions
Once specific triggers in terms of emotion dysregulation have been identified, we believe that clinicians should incorporate both general (i.e., applicable to every patient, regardless of the underlying triggers) and specific (i.e., linked to the underlying triggers) therapeutic interventions. In the next paragraph, we suggest several propositions regarding these interventions, again based on a narrative review of the literature. To make it more readable for readers, we decided to divide them in three main categories: psychoeducation, narrative work (i.e., building a person-centered understanding on how and why each difficulty has arisen), and goals setting. These interventions are summarized in Table 2.
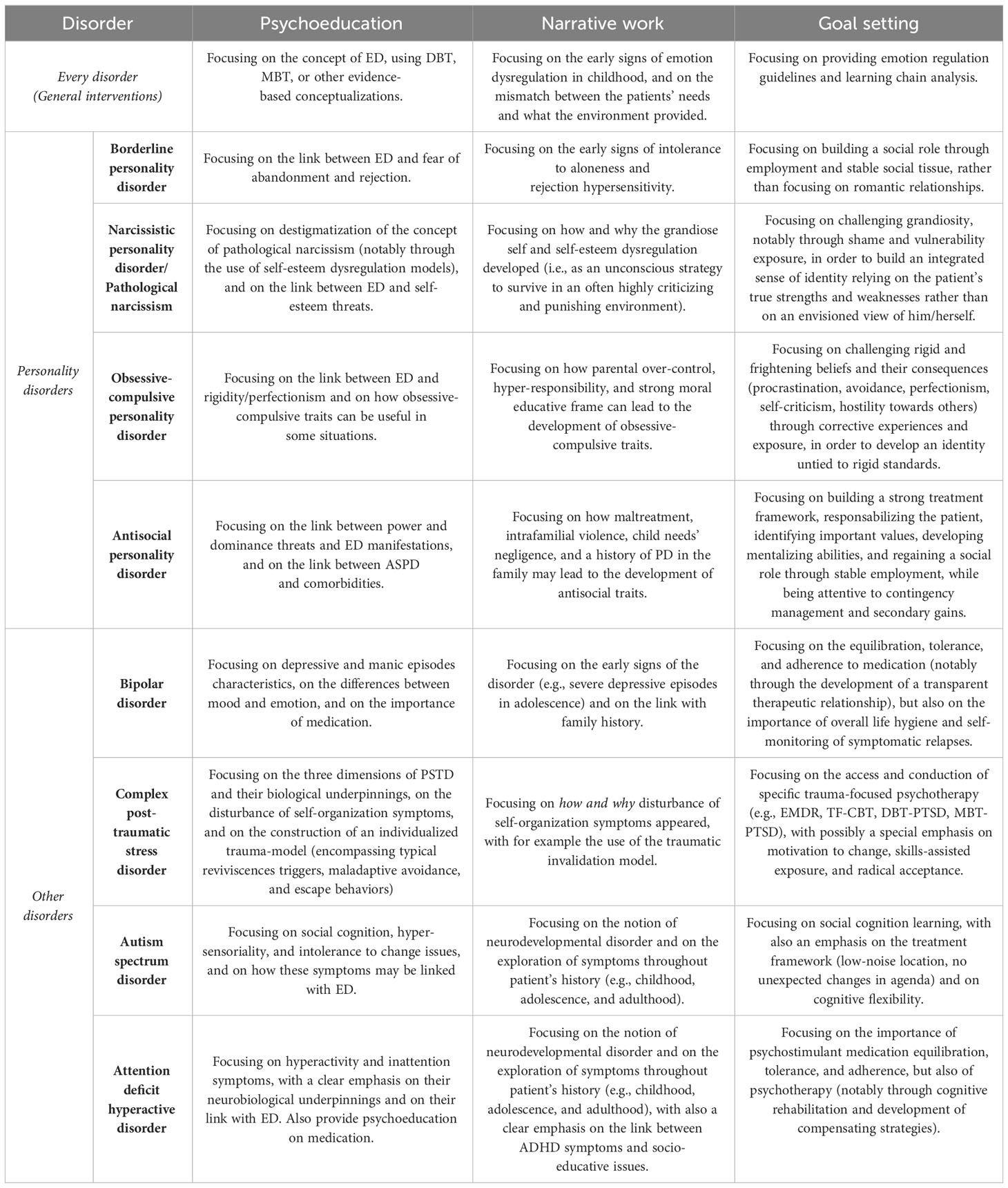
Table 2 Summary of general and specific therapeutic interventions in terms of psychoeducation, narrative work, and goal setting.
In terms of general interventions, we believe that every patient suffering from emotion dysregulation should benefit from three main elements. First, psychoeducation on the concept of ED should be provided, with a focus on the concepts of emotional vulnerability and emotional invalidation (3), on mentalizing impairments (6), or on any other evidence-based conceptualizations of ED. Second, clinicians should highlight how and when such difficulties developed in their patients’ childhood and adolescence, with several examples, in order to build a coherent narrative of the apparition and perpetuation of ED. Third, general emotion regulation guidelines should be provided, the most commonly used being the DBT skills (developed by Linehan) and mentalizing training (developed by Bateman and Fonagy). Usually, such skills are taught in group format as parts of global psychotherapeutic programs (3, 110). However, these skills can also be useful outside their classic framework, an assumption underlined by their efficacy as a stand-alone treatment [e.g., for DBT (111)]. Thus, clinicians working with patients suffering from ED may implement several of these skills in their practice, either in session (if trained and possible) or through other means (e.g., online platforms, self-help books…). For example, some authors have suggested how YouTube videos made by professionals may be useful in this indication (112). Finally, another important general aspect of treatment for patients with ED is to provide basic guidelines on how to conduct what behavioral therapists call “chain analysis” (i.e., analyzing what leads to problematic behaviors). Indeed, the latter is central to gain awareness about the main processes at play in difficult situations and may be crucial to both the diagnostic and treatment processes. Once patients have identified the main elements leading to their ED manifestations, they may be able - with the help of their therapists - to try to change the typical pathological patterns.
Once these general elements have been provided, clinicians may start to work on more specific aspects, depending on what trigger(s) was(were) found in the diagnostic process. These specific interventions should be based on the core psychopathological processes and specific issues of each disorder. Thus, specific psychoeducation should focus on linking ED manifestations and specific triggers, specific narrative work should focus on how and why such triggers appeared throughout the patient history, and specific goal setting should focus on solving the underlying issues characteristic of the trigger.
Regarding personality pathology, for borderline patients, a specific emphasis should be made on intolerance of aloneness and fear of abandonment, and goal setting should be focused on building a life outside fusional relationships (i.e., employment, stable social tissue…) (45). For narcissistic patients, given the large amount of stigma associated with the construct (113), we believe that psychoeducation should focus on destigmatizing the concept (notably through the use of self-esteem dysregulation models) and should underline the core relevance of self-esteem threats, with goal setting focusing on challenging the envisioned view of oneself through shame and vulnerability exposure (75, 114). For obsessive-compulsive patients, psychoeducation should focus on explaining rigidity and perfectionism constructs, as well as the role of control and perfection threats in ED manifestations (79, 81). A discussion on the sometimes positive and adaptive aspects of these traits is also encouraged. On the other hand, narrative work should explain how parental over-control, hyper-responsibility, and strong moral educative frame can lead to the development of obsessive-compulsive traits, and goal setting should focus on living corrective experiences (through expositions to fearful and rigid beliefs) in order to build an integrated sense of self-worth (i.e., not relying only on effort and work) (79, 81). Finally, for antisocial patients, a specific emphasis should be made on building a strong treatment framework, with careful attention on contingency management and secondary gains, with psychoeducation on how antisocial traits typically develop (mistreatment, intrafamilial violence, child needs’ negligence…) and on the link between ASPD and comorbidities (mood, substance use disorders…) (115). Finally, specific interventions for ASPD patients should focus on identifying important values, developing mentalizing abilities (notably through group interventions), and regaining a social role through stable employment (116, 117).
Regarding other disorders, ADHD and bipolar patients care should include a specific attention on treatment equilibration, tolerance, and adherence (notably through the development of a transparent therapeutic relationship). For bipolar patients, it should also include psychoeducation on both types of episodes, with a narrative work on the early signs of the disorder (e.g., severe depressive episodes in adolescence) and on the link with a family history of bipolar disorder. Moreover, discussions should be conducted on the difference between mood episodes and emotions and on the importance of overall life hygiene and self-monitoring of symptomatic relapses (118, 119). For ADHD patients, psychoeducation should include a sensibilization to the concept of neurodevelopment, clear explanations on the symptoms of the disorder and their neurobiological underpinnings, and a discussion on the importance of cognitive rehabilitation and development of compensating strategies (120, 121). These patients should also benefit from a narrative work exploring ADHD symptoms throughout patient’s history (e.g., childhood, adolescence, and adulthood), to underline the link between their symptoms and socio-educative issues. For ASD patients, specific care should also include sensibilization on the concept of neurodevelopment, psychoeducation on ASD manifestations, with once again a narrative exploration of symptoms development throughout the patient’s history (44, 104). These patients should also benefit from social cognition and cognitive flexibility training, with a special emphasis on respecting hypersensoriality and intolerance to change. Finally, cPTSD patients should benefit from psychoeducation focusing on the PSTD triad and on the disturbance of self-organization symptoms, narrative work focusing on how and why DSO symptoms appeared [with for example the use of the traumatic invalidation model (122)], and goal setting focusing on the access and conduction of specific trauma-focused psychotherapy (e.g., EMDR, TF-CBT, DBT-PTSD, MBT-PTSD), with possibly a special emphasis on motivation to change, skills-assisted exposure, and radical acceptance (100, 122).
All these elements can be hard to implement concomitantly. Thus, clinicians should be aware of the risk of confusing patients through information overload (123). This underlines the importance of establishing a clear treatment hierarchy in terms of triggers, and a clear treatment framework in terms of interventions. Our main idea is not to offer every specific intervention to every patient suffering from one trigger, but more to adapt the treatment content individually for each patient.
6 Discussion
Given its transnosographic aspect, emotion dysregulation can be found in a large number of psychiatric disorders, and is considered by several authors to be central in the development, expression and maintenance of these disorders (8). However, in our current classifications, it is only emphasized in BPD criteria, and clinicians may be confused when facing a patient with emotion regulation issues, even more if this is associated with self-harm, impulsive behavior and suicide attempts, all often considered to be classic borderline symptoms. In this context, the probability of BPD co-diagnosis is high in those patients and may increase the likelihood of over-focusing on BPD relevant aspects (e.g., fear of abandonment and rejection) and thus neglecting other important aspects. We believe that a processual approach focusing on triggers (i.e., what’s underlying ED) and enhanced by an exploration of the typical interpersonal styles of the patient may be useful to improve diagnostic assessment and treatment orientation of patients suffering from ED.
Indeed, these high levels of comorbidity enlightens the flaws of our categorical approach, mostly because these multiples comorbidities do not orient towards the most relevant disorder for the patient. However, as mentioned earlier, categories are still useful, because they offer important opportunities, especially in terms of psychoeducation. We believe that focusing on the main psychopathological processes may help overcome this issue, by incorporating the positive aspects of categories (i.e., patient’s global understanding of his/her suffering) and setting aside its negative sides (e.g., rigidity and heterogeneity). Such approach could offer an interesting option for clinicians facing ED, especially in patients with multiple comorbidities, to help them determine, through a collaborative discussion with the patient, what aspect is the more invalidating and should be addressed first, and what aspect should be taken care of afterwards. This could allow to set goals that are closer to the patient’s experience and that does not only rely on BPD categorical diagnosis or behavioral aspects of emotion dysregulation, even though these are important aspects. This could also enhance the quality of therapeutic relationship. According to Fonagy & Allison (124), correspondence between the patient’s experience and what the patient thinks the therapist thinks he/she is experiencing is crucial in the establishment of a productive therapeutic relationship. By moving the focus from classic symptoms to recurrent interpersonal patterns, this approach could help the patient to become aware of the internal coherence of his/her behaviors, which may help to decrease self-stigmatization and contribute to generate epistemic trust towards the therapist. Finally, we believe that incorporating the patient at all steps of the diagnostic and goal setting process may continue to increase the patient’s trust and, thus, his/her active participation in the treatment, which would allow a better compliance in both its psychotherapeutic and pharmacological components.
One aspect that could be opposed to our approach is the fact that evidence based dimensional models incorporating emotion regulation issues already exists. We presented some of them in the introduction, and some might say that our model stands more as a duplicate than as a real contribution to the field, especially when considering the HiTOP model and its “emotion dysfunction” super-spectra. However, these models are mostly theoretical, and are only scarcely used in clinical practice. Clinicians are, for a vast majority, still using the categorical approach, with its flaws and limitations. Moreover, there is to date no specific treatment interventions based on these models, which is not the case for categorical approach. Thus, we are now in a complex situation where categorical approach is flawed but remains the most used and studied. In this context, we believe that our model offers an interesting in-between, offering the possibility to incorporate dimensional aspects, while remaining pragmatically based on classic categories.
With this model, our primary aim is to provide a simple transdiagnostic model for generalist clinicians who are not familiar with the current literature on dimensional approaches or ED, and that may need some help in their daily practice. Given the large increase in the scientific production in the last decades (125), clinicians often struggle to maintain up-to-date knowledge and to apply guidelines (126). As described earlier, we believe that this could lead them to overfocus on categorical diagnoses which may in turn lead to underestimation of relevant psychopathological processes that are not accounted in these categories. Providing simple and condensed knowledge is useful to overcome this issue (127, 128). In this paper, we tried to condense clinically useful information on ED in several disorders, while adopting a more didactic approach than classic systematic reviews, meta-analyses, or umbrella reviews. Simple models are easier to implement in daily practice, even though some might say that they are oversimplifying or incorrect. Our aim was not to conduct a systematic review of the current literature regarding ED (see (8) for an updated review), but more to participate in the current movement that highlights the importance of adopting a more dimensional approach to psychiatric disorders.
Finally, we also believe that a trigger-based approach could be useful not only in terms of diagnostic orientation, but also in terms of improving classic psychotherapeutic treatments. Several specific treatments have been developed to treat ED, the two most popular approaches being dialectical behavioral therapy [DBT (3)] and mentalization-based therapy [MBT (6)], initially developed for BPD patients. Adaptations of DBT and MBT have already been proposed for cPTSD (122, 129), ASD (44, 130), adult ADHD (131, 132), or ASPD (116, 133). Indeed, it seems legitimate to assume that, even if these patients present the same behavioral difficulties, given that the underlying core triggers are different, a part of the content of classic DBT and MBT programs should be modified to be more tailored to these different underlying difficulties. On a neurocognitive perspective, such adaptation could be understood as a way to target more specifically each disorder emotion regulation patterns, given that these triggers could be seen as the expression of different impairments in the emotion regulation cycle. Another example of the relevance of such adaptation can be found in another BPD treatment, Good Psychiatric Management, that has been adapted for NPD and OCPD patients. These adaptations emphasized the usefulness of a self-esteem centered approach for narcissistic patients (to take into account the NPD-specific therapeutic challenges) and a more control centered approach in obsessive-compulsive patients (with an emphasis on challenging the perfectionist and rigid standards of the patient) (75, 79). In this paper, we tried to summarize the main therapeutic contents that we believe are the most relevant for each disorder. One could assume that these propositions could be implemented in already existing specialized treatments for each diagnostic category. Even though this summary should not be taken as holistic and complete, we believe that it provides simple and preliminary guidelines that could (and should) be modified and improved in the future.
However, our model has several limits. First, it does not capture the complexity of each of the presented disorders, and it cannot be considered as definitive or holistic view of such disorders, or of emotion dysregulation. Second, it does not include every disorder associated with ED. We made a subjective selection based on our clinical experience in BPD-treatment centers, and further research is needed to support our clinical claims. Third, we chose to focus on only two aspects (triggers and interpersonal style), which may also be considered as subjective and incomplete. However, we believe that, in the emotion dysregulation construct and its related aspects, these two elements are the most likely to reflect underlying psychopathology, given that the other elements (like impulsivity, self-harm, suicide attempts) are almost purely behavioral. Fourth, there is currently a lack of comparative studies investigating the differences in terms of emotion regulation development, triggers and emotion regulation strategies between the 8 disorders. Thus, further research should be conducted on this aspect to confirm/infirm our theoretical claims. Fifth, this model mostly focuses on adult patients. Even though we tried to provide developmental perspectives on the origins of triggers that may also be relevant in adolescents, future theoretical and empirical works should be conducted on this specific population to potentially adapt some parts of our model to this population specificities. However, despite these important limitations, we consider that this model constitutes a useful tool for general (and maybe specialists) clinicians and may positively contributes to the development of a more dimensional and transdiagnostic approach of emotion dysregulation.
7 Conclusion
In this article, we presented a transdiagnostic processual model of emotion dysregulation based on core triggers and interpersonal styles. Our aim was to provide a simple but technical tool to help clinicians in the diagnosis assessment and treatment orientation of their emotionally dysregulated patients. By focusing more on typical patterns and interpersonal dynamics than only on categories, we believe that this model may contribute to the actual need for improvement of our current psychiatric classifications, alongside other well-studied and under-used dimensional models of psychopathology (e.g., HiTOP, AMPD…), and may be useful to build more specific treatment frameworks for patients suffering from ED.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
MB: Conceptualization, Writing – original draft, Writing – review & editing. MD: Conceptualization, Writing – review & editing. M-AD: Writing – review & editing. AD: Writing – review & editing. ER: Writing – review & editing. SW: Writing – review & editing. MS: Conceptualization, Supervision, Writing – review & editing. NP: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ADHD, Attention Deficit Hyperactivity Disorder; AMPD, Alternative Model of Personality Disorders of the DSM-5; ASD, Autism Spectrum Disorder; ASPD, Antisocial Personality Disorder; BD, Bipolar Disorder; BPD, Borderline Personality Disorder; DBT, Dialectical Behavioral Therapy; DSM-5, Diagnostic and Statistical Manual of Mental Disorder – 5th edition; DSO, Disturbances of Self-Organization; ED, Emotion Dysregulation; ER, Emotion Regulation; ICD, International Classification of Diseases; MBT, Mentalization-Based Therapy; NPD, Narcissistic Personality Disorder; NSSI, Non-Suicidal Self-Injury; OCPD, Obsessive-Compulsive Personality Disorder; PN, Pathological Narcissism; cPTSD, complex Post traumatic stress disorder.
References
1. Gross JJ, Thompson RA. Emotion regulation: conceptual foundations. In: Handbook of emotion regulation. New York, NY, US: The Guilford Press. (2007). p. 3–24.
3. Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY, US: Guilford Press (1993). p. 558.
4. Cristea IA, Gentili C, Cotet CD, Palomba D, Barbui C, Cuijpers P. Efficacy of psychotherapies for borderline personality disorder: A systematic review and meta-analysis. JAMA Psychiatry (2017) 74(4):319. doi: 10.1001/jamapsychiatry.2016.4287
5. Prada P, Perroud N, Rüfenacht E, Nicastro R. Strategies to deal with suicide and non-suicidal self-injury in borderline personality disorder, the case of DBT. Front Psychol (2018) 9:2595. doi: 10.3389/fpsyg.2018.02595
6. Bateman A, Fonagy P. Mentalization based treatment for borderline personality disorder. World Psychiatry (2010) 9(1):11–5. doi: 10.1002/j.2051-5545.2010.tb00255.x
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
8. Carmassi C, Conti L, Gravina D, Nardi B, Dell’Osso L. Emotional dysregulation as trans-nosographic psychopathological dimension in adulthood: A systematic review. Front Psychiatry (2022) 13:900277. doi: 10.3389/fpsyt.2022.900277
9. Sloan E, Hall K, Moulding R, Bryce S, Mildred H, Staiger PK. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin Psychol Review. (2017) 57:141–63. doi: 10.1016/j.cpr.2017.09.002
10. Koenigsberg HW. Affective instability: toward an integration of neuroscience and psychological perspectives. J Pers Disord (2010) 24(1):60–82. doi: 10.1521/pedi.2010.24.1.60
11. Bowen R, Rahman H, Dong LY, Khalaj S, Baetz M, Peters E, et al. Suicidality in people with obsessive-compulsive symptoms or personality traits. Front Psychiatry (2019) 9:747. doi: 10.3389/fpsyt.2018.00747
12. Dawood S, Schroder HS, Donnellan MB, Pincus AL. Pathological narcissism and nonsuicidal self-injury. J Pers Disord (2018) 32(1):87–108. doi: 10.1521/pedi_2017_31_291
13. Di Pierro R, Di Sarno M, Madeddu F. Investigating the relationship between narcissism and emotion regulation difficulties: The role of grandiose and vulnerable traits. Clin Neuropsychiatry: J Treat Evaluation (2017) 14:209–15.
14. Gabbard GO. Narcissism and suicide risk. Ann Gen Psychiatry (2022) 21(1):3. doi: 10.1186/s12991-022-00380-8
15. Garofalo C, Velotti P, Callea A, Popolo R, Salvatore G, Cavallo F, et al. Emotion dysregulation, impulsivity and personality disorder traits: A community sample study. Psychiatry Res (2018) 266:186–92. doi: 10.1016/j.psychres.2018.05.067
16. Meszaros G, Horvath LO, Balazs J. Self-injury and externalizing pathology: a systematic literature review. BMC Psychiatry (2017) 17:160. doi: 10.1186/s12888-017-1326-y
17. Ronningstam E. Intersect between self-esteem and emotion regulation in narcissistic personality disorder - implications for alliance building and treatment. Borderline Pers Disord Emotion Dysregulation. (2017) 4(1):3. doi: 10.1186/s40479-017-0054-8
18. Steenkamp MM, Suvak MK, Dickstein BD, Shea MT, Litz BT. Emotional functioning in obsessive-compulsive personality disorder: comparison to borderline personality disorder and healthy controls. J Pers Disord (2015) 29(6):794–808. doi: 10.1521/pedi_2014_28_174
19. De Prisco M, Oliva V, Fico G, Fornaro M, de Bartolomeis A, Serretti A, et al. Defining clinical characteristics of emotion dysregulation in bipolar disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev (2022) 142:104914. doi: 10.1016/j.neubiorev.2022.104914
20. Green MJ, Cahill CM, Malhi GS. The cognitive and neurophysiological basis of emotion dysregulation in bipolar disorder. J Affect Disord (2007) 103(1):29–42. doi: 10.1016/j.jad.2007.01.024
21. Maddox BB, Trubanova A, White SW. Untended wounds: Non-suicidal self-injury in adults with autism spectrum disorder. Autism (2017) 21(4):412–22. doi: 10.1177/1362361316644731
22. Mazefsky CA. Emotion regulation and emotional distress in autism spectrum disorder: foundations and considerations for future research. J Autism Dev Disord (2015) 45(11):3405–8. doi: 10.1007/s10803-015-2602-7
23. Ford JD, Courtois CA. Complex PTSD and borderline personality disorder. bord Pers Disord emot dysregul. (2021) 8(1):16. doi: 10.1186/s40479-021-00155-9
24. Balázs J, Győri D, Horváth LO, Mészáros G, Szentiványi D. Attention-deficit hyperactivity disorder and nonsuicidal self-injury in a clinical sample of adolescents: the role of comorbidities and gender. BMC Psychiatry (2018) 18(1):34. doi: 10.1186/s12888-018-1620-3
25. Retz W, Stieglitz RD, Corbisiero S, Retz-Junginger P, Rösler M. Emotional dysregulation in adult ADHD: what is the empirical evidence? Expert Rev Neurother (2012) 12(10):1241–51. doi: 10.1586/ern.12.109
26. Grant BF, Chou SP, Goldstein RB, Huang B, Stinson FS, Saha TD, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the wave 2 national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry (2008) 69(4):533–45. doi: 10.4088/JCP.v69n0404
27. Bayes A, Parker G, Paris J. Differential diagnosis of bipolar II disorder and borderline personality disorder. Curr Psychiatry Rep (2019) 21(12):125. doi: 10.1007/s11920-019-1120-2
28. Jacob CP, Romanos J, Dempfle A, Heine M, Windemuth-Kieselbach C, Kruse A, et al. Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits and related disorders in a tertiary referral center. Eur Arch Psychiatry Clin Neurosci (2007) 257(6):309–17. doi: 10.1007/s00406-007-0722-6
29. Rinaldi C, Attanasio M, Valenti M, Mazza M, Keller R. Autism spectrum disorder and personality disorders: Comorbidity and differential diagnosis. World J Psychiatry (2021) 11(12):1366–86. doi: 10.5498/wjp.v11.i12.1366
30. Craddock N, Mynors-Wallis L. Psychiatric diagnosis: impersonal, imperfect and important. Br J Psychiatry (2014) 204(2):93–5. doi: 10.1192/bjp.bp.113.133090
31. Haslam N, Holland E, Kuppens P. Categories versus dimensions in personality and psychopathology: a quantitative review of taxometric research. Psychol Med (2012) 42(5):903–20. doi: 10.1017/S0033291711001966
32. Krueger RF, Kotov R, Watson D, Forbes MK, Eaton NR, Ruggero CJ, et al. Les progrès dans la réalisation de la classification quantitative de la psychopathologie. Ann Med Psychol (Paris). (2021) 179(1):95–106. doi: 10.1016/j.amp.2020.11.015
33. Eaton NR, Bringmann LF, Elmer T, Fried EI, Forbes MK, Greene AL, et al. A review of approaches and models in psychopathology conceptualization research. Nat Rev Psychol (2023) 2(10):622–36. doi: 10.1038/s44159-023-00218-4
34. Caspi A, Moffitt TE. All for one and one for all: mental disorders in one dimension. Am J Psychiatry (2018) 175(9):831–44. doi: 10.1176/appi.ajp.2018.17121383
35. Kotov R, Jonas KG, Carpenter WT, Dretsch MN, Eaton NR, Forbes MK, et al. Validity and utility of hierarchical taxonomy of psychopathology (HiTOP): I. Psychosis superspectrum. World Psychiatry (2020) 19(2):151–72. doi: 10.1002/wps.20730
36. Watson D, Levin-Aspenson HF, Waszczuk MA, Conway CC, Dalgleish T, Dretsch MN, et al. Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry (2022) 21(1):26–54. doi: 10.1002/wps.20943
37. World Health Organization. ICD-11 (2018). Available at: https://icd.who.int/en.
38. Wright AGC, Ringwald WR, Hopwood CJ, Pincus AL. It’s time to replace the personality disorders with the interpersonal disorders. Am Psychol (2022) 77(9):1085–99. doi: 10.1037/amp0001087
39. Hutsebaut J, Willemsen E, Bachrach N, Van R. Improving access to and effectiveness of mental health care for personality disorders: the guideline-informed treatment for personality disorders (GIT-PD) initiative in the Netherlands. Borderline Pers Disord Emot Dysregul. (2020) 7:16. doi: 10.1186/s40479-020-00133-7
40. Haeffel G, Jeronimus BF, Fisher AJ, Kaiser BN, Weaver LJ, Vargas I, et al. The hierarchical taxonomy of psychopathology (HiTOP) is not an improvement over the DSM. Clin psychol Science. (2022) 10(2):285–90. doi: 10.1177/21677026211068873
41. Blay M, Benmakhlouf I, Duarte M, Perroud N, Greiner C, Charbon P, et al. Case reports: Using Good Psychiatric Management (GPM) conceptualizations in the dimensional assessment and treatment of personality disorders. Front Psychiatry (2023) 14. doi: 10.3389/fpsyt.2023.1186524
42. Sharp C, Wright AGC, Fowler JC, Frueh BC, Allen JG, Oldham J, et al. The structure of personality pathology: Both general (‘g’) and specific (‘s’) factors? J Abnormal Psychol (2015) 124(2):387–98. doi: 10.1037/abn0000033
43. Campbell MA, Waller G, Pistrang N. The impact of narcissism on drop-out from cognitive-behavioral therapy for the eating disorders: A pilot study. J Nervous Ment Disease. (2009) 197(4):278–81. doi: 10.1097/NMD.0b013e31819dc150
44. Bemmouna D, Coutelle R, Weibel S, Weiner L. Feasibility, acceptability and preliminary efficacy of dialectical behavior therapy for autistic adults without intellectual disability: A mixed methods study. J Autism Dev Disord (2022) 52(10):4337–54. doi: 10.1007/s10803-021-05317-w
45. Gunderson JG. Handbook of Good Psychiatric Management for Borderline Personality Disorder. Washington, DC: American Psychiatric Pub (2014). p. 168.
46. Gartlehner G, Crotty K, Kennedy S, Edlund MJ, Ali R, Siddiqui M, et al. Pharmacological treatments for borderline personality disorder: A systematic review and meta-analysis. CNS Drugs (2021) 35(10):1053–67. doi: 10.1007/s40263-021-00855-4
47. Cole PM, Ashana Ramsook K, Ram N. Emotion dysregulation as a dynamic process. Dev Psychopathol. (2019) 31(3):1191–201. doi: 10.1017/S0954579419000695
48. Barrett KC, Campos JJ. Perspectives on emotional development II: A functionalist approach to emotions. In: Handbook of infant development, 2nd ed. Oxford, England: John Wiley & Sons (1987). p. 555–78.
49. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assessment. (2004) 26(1):41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
50. Thompson RA. Emotion regulation: A theme in search of definition. Monogr Soc Res Child Dev (1994) 59(2-3):25–52.
51. Gross JJ. The extended process model of emotion regulation: elaborations, applications, and future directions. psychol Inquiry. (2015) 26(1):130–7. doi: 10.1080/1047840X.2015.989751
52. Fox NA. The Development of Emotion Regulation: Biological and Behavioral Considerations. Chicago, Ill: University of Chicago Press (1994). p. 308.
53. Gross JJ, editor. Handbook of emotion regulation. Second edition. New York London: The Guilford Press (2015). p. 669.
54. Calkins SD. The emergence of self-regulation: Biological and behavioral control mechanisms supporting toddler competencies. In: Socioemotional development in the toddler years: Transitions and transformations. New York, NY, US: The Guilford Press. (2007) p. 261–84.
55. Thompson RA, Goodman M. Development of emotion regulation: More than meets the eye. In: Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment. New York, NY, US: The Guilford Press (2010). p. 38–58.
56. Debbané M, Prada P, Bouteloup M, Speranza M, Perroud N. Mentaliser, la clé des interactions humaines: concepts et applications. Louvain-la-Neuve (Belgique): De Boeck supérieur (2022).
57. Brenning KM, Braet C. Mentaliser, la clé des interactions humaines: concepts et applications. Louvain-la-Neuve (Belgique): De Boeck supérieur (2013) 20(1):107–23. doi: 10.1111/j.1475-6811.2012.01399.x
58. Shaver PR, Mikulincer M. Adult attachment and emotion regulation. In: Handbook of emotion regulation, 2nd ed. New York, NY, US: The Guilford Press (2014). p. 237–50.
59. Cole PM, Michel MK, Teti LO. The development of emotion regulation and dysregulation: A clinical perspective. Monogr Soc Res Child Dev (1994) 59(2–3):73–102. doi: 10.1111/j.1540-5834.1994.tb01278.x
60. Aldao A, Gee DG, Reyes ADL, Seager I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Dev Psychopathol (2016) 28(4pt1):927–46. doi: 10.1017/S0954579416000638
61. Cole PM, Hall SE, Hajal NJ. Emotion dysregulation as a risk factor for psychopathology. Child Adolesc psychopathology. (2008) 2:341–73.
62. Cai RY, Richdale AL, Uljarević M, Dissanayake C, Samson AC. Emotion regulation in autism spectrum disorder: Where we are and where we need to go. Autism Res (2018) 11(7):962–78. doi: 10.1002/aur.1968
63. Lima IMM, Peckham AD, Johnson SL. Cognitive deficits in bipolar disorders: Implications for emotion. Clin Psychol Review. (2018) 59:126–36. doi: 10.1016/j.cpr.2017.11.006
64. Groves NB, Wells EL, Soto EF, Marsh CL, Jaisle EM, Harvey TK, et al. Executive functioning and emotion regulation in children with and without ADHD. Res Child Adolesc Psychopathol. (2022) 50(6):721–35. doi: 10.1007/s10802-021-00883-0
65. Gunderson JG, Herpertz SC, Skodol AE, Torgersen S, Zanarini MC. Borderline personality disorder. Nat Rev Dis Primers. (2018) 4(1):18029. doi: 10.1038/nrdp.2018.29
66. Kellogg SH, Young JE. Schema therapy for borderline personality disorder. J Clin Psychol (2006) 62(4):445–58. doi: 10.1002/jclp.20240
67. Kernberg OF. Borderline conditions and pathological narcissism. Northvale, NJ: Aronson. (1992). p. 361.
68. Gunderson JG. Disturbed relationships as a phenotype for borderline personality disorder. AJP (2007) 164(11):1637–40. doi: 10.1176/appi.ajp.2007.07071125
69. Pincus AL, Lukowitsky MR. Pathological narcissism and narcissistic personality disorder. Annu Rev Clin Psychol (2010) 6(1):421–46. doi: 10.1146/annurev.clinpsy.121208.131215
70. Pincus AL, Ansell EB, Pimentel CA, Cain NM, Wright AGC, Levy KN. Initial construction and validation of the Pathological Narcissism Inventory. psychol Assessment. (2009) 21(3):365–79. doi: 10.1037/a0016530
71. Trull TJ, Jahng S, Tomko RL, Wood PK, Sher KJ. Revised NESARC personality disorder diagnoses: gender, prevalence, and comorbidity with substance dependence disorders. J Pers Disord (2010) 24(4):412–26. doi: 10.1521/pedi.2010.24.4.412
72. Cain NM, Pincus AL, Ansell EB. Narcissism at the crossroads: Phenotypic description of pathological narcissism across clinical theory, social/personality psychology, and psychiatric diagnosis. Clin Psychol Review. (2008) 28(4):638–56. doi: 10.1016/j.cpr.2007.09.006
73. Zhang H, Wang Z, You X, Lü W, Luo Y. Associations between narcissism and emotion regulation difficulties: Respiratory sinus arrhythmia reactivity as a moderator. Biol Psychol (2015) 110:1–11. doi: 10.1016/j.biopsycho.2015.06.014
74. Weinberg I, Ronningstam E. Narcissistic personality disorder: progress in understanding and treatment. FOC (2022) 20(4):368–77. doi: 10.1176/appi.focus.20220052
75. Weinberg I, Finch E, Choi-Kain L. Implementation of Good Psychiatric Management for Narcissistic Personality Disorder: Good Enough or Not Good Enough? In: Applications of good psychiatric management for borderline personality disorder: A practical guide. Washington, D.C.: American Psychiatric Association Publishing (2019). p. 253–80.
76. Volkert J, Gablonski TC, Rabung S. Prevalence of personality disorders in the general adult population in Western countries: systematic review and meta-analysis. Br J Psychiatry (2018) 213(6):709–15. doi: 10.1192/bjp.2018.202
77. Diedrich A, Voderholzer U. Obsessive–compulsive personality disorder: a current review. Curr Psychiatry Rep (2015) 17(2):2. doi: 10.1007/s11920-014-0547-8
78. Skodol AE, Gunderson JG, McGlashan TH, Dyck IR, Stout RL, Bender DS, et al. Functional impairment in patients with schizotypal, borderline, avoidant, or obsessive-compulsive personality disorder. AJP (2002) 159(2):276–83. doi: 10.1176/appi.ajp.159.2.276
79. Finch EF, Choi-Kain LW, Iliakis EA, Eisen JL, Pinto A. Good psychiatric management for obsessive–compulsive personality disorder. Curr Behav Neurosci Rep (2021) 8(4):160–71. doi: 10.1007/s40473-021-00239-4
80. Grant JE, Pinto A, Chamberlain S. Obsessive-compulsive personality disorder. Washington, D.C: American Psychiatric Association Publishing (2020). p. 259. Available at: http://www.mentalhealth.com/dis/p20-pe10.html.
81. Pinto A. Treatment of obsessive-compulsive personality disorder. In: Storch EA, Lewin AB, editors. Clinical Handbook of Obsessive-Compulsive and Related Disorders. Cham: Springer International Publishing (2016). p. 415–29. doi: 10.1007/978-3-319-17139-5_28
82. Cain NM, Ansell EB, Simpson HB, Pinto A. Interpersonal functioning in obsessive–compulsive personality disorder. J Pers Assessment. (2015) 97(1):90–9. doi: 10.1080/00223891.2014.934376
83. Wetterborg D. Men with borderline personality disorder and antisocial behavior: clinical characteristics, developmental perspectives and interventions. Stockholm: Karolinska Institutet (2018).
84. McManus S, Purdon S, Smith J, Crawford M, Tyrer P, Coid J. Antisocial and borderline personality disorders. In: Adult psychiatric morbidity in England (2007). Results of a household survey. Leeds, UK: The NHS Information Centre for health and social care (2009).
85. Sargın AE, Özdel K, Türkçapar MH. Cognitive-behavioral theory and treatment of antisocial personality disorder. In: Durbano F, editor. Psychopathy - New Updates on an Old Phenomenon. London, United Kingdom: InTech (2017).
86. Merikangas KR, Jin R, He JP, Kessler RC, Lee S, Sampson NA, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry (2011) 68(3):241–51. doi: 10.1001/archgenpsychiatry.2011.12
87. Sanchez-Moreno J, Martinez-Aran A, Tabarés-Seisdedos R, Torrent C, Vieta E, Ayuso-Mateos JL. Functioning and disability in bipolar disorder: an extensive review. Psychother Psychosom. (2009) 78(5):285–97. doi: 10.1159/000228249
88. Wang L, Liu J, Yang Y, Zou H. Prevalence and risk factors for non-suicidal self-injury among patients with depression or bipolar disorder in China. BMC Psychiatry (2021) 21(1):389. doi: 10.1186/s12888-021-03392-y
89. Kulacaoglu F, Izci F. The effect of emotional dysregulation and impulsivity on suicidality in patients with bipolar disorder. Psychiatr Danub. (2022) 34(4):706–14. doi: 10.24869/psyd.2022.706
90. Henry C, Van den Bulke D, Bellivier F, Roy I, Swendsen J, M’Baïlara K, et al. Affective lability and affect intensity as core dimensions of bipolar disorders during euthymic period. Psychiatry Res (2008) 159(1):1–6. doi: 10.1016/j.psychres.2005.11.016
91. Proudfoot J, Whitton A, Parker G, Doran J, Manicavasagar V, Delmas K. Triggers of mania and depression in young adults with bipolar disorder. J Affect Disord (2012) 143(1):196–202. doi: 10.1016/j.jad.2012.05.052
92. Rodrigues Cordeiro C, Côrte-Real BR, Saraiva R, Frey BN, Kapczinski F, de Azevedo Cardoso T. Triggers for acute mood episodes in bipolar disorder: A systematic review. J Psychiatr Res (2023) 161:237–60. doi: 10.1016/j.jpsychires.2023.03.008
93. Kernberg OF, Yeomans FE. Borderline personality disorder, bipolar disorder, depression, attention deficit/hyperactivity disorder, and narcissistic personality disorder: Practical differential diagnosis. Bull Menninger Clinic. (2013) 77(1):1–22. doi: 10.1521/bumc.2013.77.1.1
94. Bayes AJ, McClure G, Fletcher K, Román Ruiz Del Moral YE, Hadzi-Pavlovic D, Stevenson JL, et al. Differentiating the bipolar disorders from borderline personality disorder. Acta Psychiatr Scand (2016) 133(3):187–95. doi: 10.1111/acps.12509
95. Jiménez E, Arias B, Castellví P, Goikolea JM, Rosa AR, Fañanás L, et al. Impulsivity and functional impairment in bipolar disorder. J Affect Disord (2012) 136(3):491–7. doi: 10.1016/j.jad.2011.10.044
96. Gitlin MJ, Miklowitz DJ. The difficult lives of individuals with bipolar disorder: A review of functional outcomes and their implications for treatment. J Affect Disord (2017) 209:147–54. doi: 10.1016/j.jad.2016.11.021
97. Frans Ö, Rimmö PA, Åberg L, Fredrikson M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatrica Scandinavica. (2005) 111(4):291–0. doi: 10.1111/j.1600-0447.2004.00463.x
98. Bryant RA. Post-traumatic stress disorder: a state-of-the-art review of evidence and challenges. World Psychiatry (2019) 18(3):259–69. doi: 10.1002/wps.20656
99. Cloitre M. ICD-11 complex post-traumatic stress disorder: simplifying diagnosis in trauma populations. Br J Psychiatry (2020) 216(3):129–31. doi: 10.1192/bjp.2020.43
100. Maercker A, Cloitre M, Bachem R, Schlumpf YR, Khoury B, Hitchcock C, et al. Complex post-traumatic stress disorder. Lancet (2022) 400(10345):60–72. doi: 10.1016/S0140-6736(22)00821-2
101. Cloitre M, Garvert DW, Weiss B, Carlson EB, Bryant RA, Distinguishing PTSD, et al. and Borderline Personality Disorder: A latent class analysis. Eur J Psychotraumatology (2014) 5(1):25097. doi: 10.3402/ejpt.v5.25097
102. Herman JL. Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. J Traumatic Stress. (1992) 5(3):377–91. doi: 10.1002/jts.2490050305
103. Ford JD. Commentary on the special section on complex PTSD: still going strong after all these years. J Trauma Stress. (2019) 32(6):877–80. doi: 10.1002/jts.22474
104. Lord C, Brugha TS, Charman T, Cusack J, Dumas G, Frazier T, et al. Autism spectrum disorder. Nat Rev Dis Primers. (2020) 6(1):1–23. doi: 10.1038/s41572-019-0138-4
105. Reyes NM, Pickard K, Reaven J. Emotion regulation: A treatment target for autism spectrum disorder. Bull Menninger Clinic. (2019) 83(3):205–34. doi: 10.1521/bumc.2019.83.3.205
106. Fayyad J, Sampson NA, Hwang I, Adamowski T, Aguilar-Gaxiola S, Al-Hamzawi A, et al. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. ADHD Atten Def Hyp Disord (2017) 9(1):47–65. doi: 10.1007/s12402-016-0208-3
107. Soler-Gutiérrez AM, Pérez-González JC, Mayas J. Evidence of emotion dysregulation as a core symptom of adult ADHD: A systematic review. PloS One (2023) 18(1):e0280131. doi: 10.1371/journal.pone.0280131
108. Ginapp CM, Greenberg NR, Macdonald-Gagnon G, Angarita GA, Bold KW, Potenza MN. The experiences of adults with ADHD in interpersonal relationships and online communities: A qualitative study. SSM - Qual Res Health (2023) 3:100223. doi: 10.1016/j.ssmqr.2023.100223
109. Blay M, Hasler R, Nicastro R, Pham E, Weibel S, Debbané M, et al. Body modifications in borderline personality disorder patients: prevalence rates, link with non-suicidal self-injury, and related psychopathology. Borderline Pers Disord Emot Dysregul. (2023) 10:7. doi: 10.1186/s40479-023-00213-4
110. Bateman A, Fonagy P, Campbell C, Luyten P, Debbané M. Cambridge guide to mentalization-based treatment (MBT). Cambridge, United Kingdom; New York, NY: Cambridge University Press (2023).
111. Valentine SE, Bankoff SM, Poulin RM, Reidler EB, Pantalone DW. The use of dialectical behavior therapy skills training as stand-alone treatment: A systematic review of the treatment outcome literature. J Clin Psychol (2015) 71(1):1–20. doi: 10.1002/jclp.22114
112. Durpoix A, Weiner L, Bemmouna D, Lachaux E, Krasny-Pacini A, Weibel S. Psychoéducation et régulation émotionnelle en temps de confinement: faisabilité et intérêt de vidéos YouTube de thérapie comportementale dialectique. Annales Médico-psychologiques Rev psychiatrique. (2023) 181(6):475–81. doi: 10.1016/j.amp.2021.10.016
113. Buss DM, Chiodo LM. Narcissistic acts in everyday life. J Personality. (1991) 59(2):179–215. doi: 10.1111/j.1467-6494.1991.tb00773.x
114. Weinberg I, Ronningstam E. Dos and don’ts in treatments of patients with narcissistic personality disorder. J Pers Disord (2020) 34(Supplement):122–42. doi: 10.1521/pedi.2020.34.supp.122
115. Glenn AL, Johnson AK, Raine A. Antisocial personality disorder: A current review. Curr Psychiatry Rep (2013) 15(12):427. doi: 10.1007/s11920-013-0427-7
116. Bateman AW. Mentalizing and group psychotherapy: A novel treatment for antisocial personality disorder. Am J Psychother. (2022) 75(1):32–7. doi: 10.1176/appi.psychotherapy.20210023
117. Thylstrup B, Schrøder S, Hesse M. Psycho-education for substance use and antisocial personality disorder: a randomized trial. BMC Psychiatry (2015) 15:283. doi: 10.1186/s12888-015-0661-0
118. Yasui-Furukori N, Nakamura K. Bipolar disorder recurrence prevention using self-monitoring daily mood charts: case reports from a 5 year period. Neuropsychiatr Dis Treat (2017) 13:733–6. doi: 10.2147/NDT.S132355
119. Vieta E, Berk M, Schulze TG, Carvalho AF, Suppes T, Calabrese JR, et al. Bipolar disorders. Nat Rev Dis Primers. (2018) 4(1):1–16. doi: 10.1038/nrdp.2018.8
120. Kysow K, Park J, Johnston C. The use of compensatory strategies in adults with ADHD symptoms. Atten Defic Hyperact Disord (2017) 9(2):73–88. doi: 10.1007/s12402-016-0205-6
121. Tajik-Parvinchi D, Wright L, Schachar R. Cognitive rehabilitation for attention deficit/hyperactivity disorder (ADHD): promises and problems. J Can Acad Child Adolesc Psychiatry (2014) 23(3):207–17.
122. Bohus M, Kleindienst N, Hahn C, Müller-Engelmann M, Ludäscher P, Steil R, et al. Dialectical behavior therapy for posttraumatic stress disorder (DBT-PTSD) compared with cognitive processing therapy (CPT) in complex presentations of PTSD in women survivors of childhood abuse: A randomized clinical trial. JAMA Psychiatry (2020) 77(12):1235–45. doi: 10.1001/jamapsychiatry.2020.2148
123. Bawden D, Holtham C, Courtney N. Perspectives on information overload. In: Aslib proceedings. MCB UP Ltd (1999). p. 249–55.
124. Fonagy P, Allison E. The role of mentalizing and epistemic trust in the therapeutic relationship. Psychotherapy (2014) 51(3):372–80. doi: 10.1037/a0036505
125. Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PloS Med (2010) 7(9):e1000326. doi: 10.1371/journal.pmed.1000326
126. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA (1999) 282(15):1458–65. doi: 10.1001/jama.282.15.1458
127. Boussageon R, Blanchard C, Charuel E, Menini T, Pereira B, Naudet F, et al. Project rebuild the evidence base (REB): A method to interpret randomised clinical trials and their meta-analysis to present solid benefit-risk assessments to patients. Therapies (2023) 78(4):353–65. doi: 10.1016/j.therap.2022.10.008
128. Choi GJ, Kang H. The umbrella review: a useful strategy in the rain of evidence. Korean J Pain. (2022) 35(2):127–8. doi: 10.3344/kjp.2022.35.2.127
129. Mitchell S, Steele K. Mentalising in complex trauma and dissociative disorders. Eur J Trauma Dissociation. (2021) 5(3):100168. doi: 10.1016/j.ejtd.2020.100168
130. Krämer K, Vetter A, Schultz-Venrath U, Vogeley K, Reul S. Mentalization-based treatment in groups for adults with autism spectrum disorder. Front Psychol (2021) 12:708557. doi: 10.3389/fpsyg.2021.708557
131. Cole P, Weibel S, Nicastro R, Hasler R, Dayer A, Aubry JM, et al. CBT/DBT skills training for adults with attention deficit hyperactivity disorder (ADHD). Psychiatr Danub. (2016) 28(Suppl-1):103–7.
132. Perroud N, Badoud D, Weibel S, Nicastro R, Hasler R, Küng AL, et al. Mentalization in adults with attention deficit hyperactivity disorder: Comparison with controls and patients with borderline personality disorder. Psychiatry Res (2017) 256:334–41. doi: 10.1016/j.psychres.2017.06.087
Keywords: emotion dysregulation, trigger-based approach, processual, transdiagnostic, borderline personality disorder
Citation: Blay M, Duarte M, Dessouli M-A, Durpoix A, Rüfenacht E, Weibel S, Speranza M and Perroud N (2024) Proposition of a transdiagnostic processual approach of emotion dysregulation based on core triggers and interpersonal styles. Front. Psychiatry 15:1260138. doi: 10.3389/fpsyt.2024.1260138
Received: 17 July 2023; Accepted: 19 January 2024;
Published: 07 February 2024.
Edited by:
Jean Marc Guile, University of Picardie Jules Verne, FranceReviewed by:
Ilaria Maria Antonietta Benzi, University of Pavia, ItalySuzane Renaud, CISSS des Laurentides, Canada
Copyright © 2024 Blay, Duarte, Dessouli, Durpoix, Rüfenacht, Weibel, Speranza and Perroud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nader Perroud, bmFkZXIucGVycm91ZEB1bmlnZS5jaA==