
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 01 May 2024
Sec. Aging Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1199119
 Sze Ting Joanna Ngan1
Sze Ting Joanna Ngan1 Calvin Pak Wing Cheng1*
Calvin Pak Wing Cheng1* Wai Chi Chan2
Wai Chi Chan2 Kam Hung Harry Tsui1
Kam Hung Harry Tsui1 Sau Man Corine Chan3
Sau Man Corine Chan3 Kit Wa Sherry Chan1
Kit Wa Sherry Chan1Introduction: Impairment in mentalization is implicated in the development and maintenance of depression. Major depressive disorders showed significant impairment in social cognition and such impairment appears to be positively associated with the severity of depression. Self-referential gaze perception (SRGP), a measurement of mentalization, was predominantly measured in patients with psychosis but rarely examined in late-life depression (LLD).
Methods: To assess the effect of cognition on the interpretation bias of mentalization, 29 LLD patients and 29 healthy controls were asked to judge if various gaze directions were directed to self in SRGP.
Results: Patients with better cognition showed less unambiguous-SRGP bias than those with worse cognitive scores; this difference was not found in healthy controls. Global cognition and executive function contributed to the SRGP rate in patients.
Conclusion: The current study is the first study to explore the relationship between cognition and SRGP in the LLD population. Our study findings suggested that the cognitive function of LLD patients may contribute to the modulation of interpretation bias, which in turn underlie the role of SRGP bias. Greater SRGP bias in patients may reflect social cognition deterioration, impairing the social interaction and functioning of LLD patients. This highlights the need for early intervention and cognitive decline identification to facilitate better prognosis and treatment effectiveness; thus, further studies could navigate the potential of SRGP task as a screening tool for high-risk group of LLD likely to develop dementia.
The high prevalence and poor treatment outcomes of geriatric depression have become a pressing health care issue in Hong Kong. It is estimated that one in six people worldwide will be aged at least 60 years old by 2030 (1). A local study found that around 10% of community dwellers (2) aged 60 years or above suffered from clinically significant depression, referred to as late-life depression (LLD) (3). Compared with depression in adults, LLD is implicated with greater impairment in executive functions and psychomotor retardation (3). Furthermore, LLD is also associated with poor long-term prognosis and a higher relapse rate (4). Most importantly, LLD is related to an increased risk of cognitive impairment and dementia (5). Hence, it is important to examine geriatric depression as a separate and unique entity. Also, it is of importance to identify people at risk of LLD of further cognitive impairment.
Mentalization, as a form of social cognition, infers the ability to identify, perceive, and interpret socially relevant information (6). Mentalization impairment in depression is partly contributed by the inability to interpret emotional stimuli and mental states accurately (7). The negative interpretation bias, which is the tendency to infer ambiguous social information as negative valence, has been identified as the core feature of depression for decades (8). Recent theory suggests that interpretation bias plays an important role in the onset and maintenance of depression (9, 10).
Self-referential gaze perception (SRGP) was predominantly measured in patients with psychosis but rarely in the depression cohort. Tendence of perceiving averted gaze as self-referential was more prominent in bipolar disorder and schizophrenia patients than healthy adult controls (11, 12). For depression patients, biased self-referential processing was commonly measured with the interpretation of cognitive information related to self-schemas. Depressogenic self-schemas measured by self-referential encoding task were more prevalent in patients with depression than controls in children, adolescents, and adults (13–15). While self-referential bias was implicated in depression consistently across different age groups, no studies, to our knowledge, explored self-referential processing among old-age adults with depression. Existing literature indicated healthy older adults had poorer social cognitive function than the younger adults (16). Other suggested that the impairments vary between subsets of social cognition where attribution process in older adults declined but emotional perception remained intact (17–20).
Judgment of self-referential gaze intention with gaze perception task is a relatively simple assessment of mentalization, which is an important component in social cognition. However, limited studies to date explored mentalization of LLD and to our knowledge, no studies examined eye gaze interpretation among LLD patients. Therefore, the current study aimed to examine the SRGP of patients with LLD compared with healthy controls (HCs). We hypothesized that patients would have greater SRGP bias than HCs. The secondary aim of the study was to explore the relationships between symptomology, global cognition, and gaze perception. We hypothesized that both depressive symptoms and global cognition would be related to SRGP bias. The findings of this study will help to provide further understanding in the interpretation bias in LLD, hence, develop a screening tool for detecting high risk LLD.
Fifty-eight Chinese older adults aged 60 years or above were recruited, with 29 in patient group and 29 age- and gender-matched health controls. Patients with primary diagnosis of major depressive disorder (MDD) screened by psychiatrists from outpatient psychiatric clinics of the public hospital in Hong Kong with structured Clinical Interview for the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), and no change in dosage of antidepressant for at least 2 weeks was included. Patients with a DSM-5 diagnosis other than MDD [e.g., major neurocognitive disorder of any types, including Alzheimer’s disease (AD)], a score of Hong Kong Chinese version of the Montreal Cognitive Assessment (HK-MoCA) (21) below second percentile relative to the subject’s age and education level, with comorbid alcohol or substance dependence or any concomitant unstable major medical or neurological conditions will be excluded. HCs with the same exclusion criteria, in addition to no personal or family history of mental illnesses, were recruited from the community. Face-to-face interviews were conducted to screen for normal or corrected-to-normal vision and obtain written informed consent. This current study was approved by the institutional review board of the University of Hong Kong and Hong Kong West Cluster of Hospital of Authority (IRB: UW 22-712).
Demographics including age, gender, and level of education was collected. Depressive symptoms were assessed with the Hamilton depression rating scale (HAM-D-17 (22). Information regarding symptomology including medical comorbidity and independent functioning ability were assessed by the Cumulative Illness Rating Scale (CIRS) and the Hong Kong Chinese version of the Lawton Instrumental Activities of Daily Living (IADL), respectively. While global cognition was measured by Mini-Mental State Examination (MMSE), working memory and attention were examined by the forward and backward digit span, and executive function was assessed by the Stroop color and word test, Trail Making Test (TMT) and verbal fluency test (VFT).
A gaze perception task developed in the previous study (12) was used. In short, the task consists of six blocks, and each block contains 30 trials of randomly selected facial stimuli of one model with pre-determined distribution of gaze directions and was programmed using E-prime Professional 2.0. There were six Chinese models (three men and three women) facing straight to camera with 13 different gaze directions (0°, 5°, 10°, 15°, 20°, 25°, and 30° to the left and to the right, respectively). Participants were instructed to press the right key “yes” or the left key “no” to the question in evaluation for self-referential gaze: “Do you feel as if the person in the picture is looking at you?” Each trial began with 200 ms presentation of the face, followed by a fixation cross remained on the screen for 1800 ms and ended with a blank page for 500 ms (23). Accuracy and response time were collected automatically by the program within the 2500 ms time frame in each trial. Missing responses in the 2500 ms were coded as nil response. All participants would begin with a short practice run of the task using new stimuli before the start of the experiment. The experiment lasted for approximately 20–25 min.
Ambiguous-SRGP rate and unambiguous-SRGP rate were calculated for the gaze perception task as suggested in the previous study (12). Ambiguous-SRGP rate was indicated by the average rate of reporting the gaze as self-directing (SRGP) with trials of averted gaze direction of 10° and 15°, whereas the unambiguous-SRGP rate was the average rate of reporting the gaze as self-directing (SRGP) with trials of averted gaze direction of 20°, 25°, and 30°. Demographic, clinical, and cognitive measures were compared between patient and control groups using paired samples t-tests for the parametric variables and Mann–Whitney U tests for the non-parametric variables. Group differences in ambiguous-SRGP, unambiguous-SRGP, depressive symptomology, and cognitive function were analyzed using generalized linear model, controlled for age, gender, and education years. Considering the non-parametric nature of the variables, Spearman’s correlation was performed to examine relationship between gaze perception, cognitive functioning, and symptomatology. P-values were adjusted (p = .001) for multiple testing using with Benjamini–Hochberg false discovery rate correction (FDR = 0.1). Linear regression was used to explore the contribution of cognitive functions on SRGP. All tests would be two-tailed with the significance level set at p < 0.05. Analyses were performed with SPSS for Windows, version 27.0.
There was no significant difference in age, gender, and education years between group (Table 1). Also, no significant difference was found in cognitive functions, but among symptomology, significant group difference was found in the HAM-D scores.
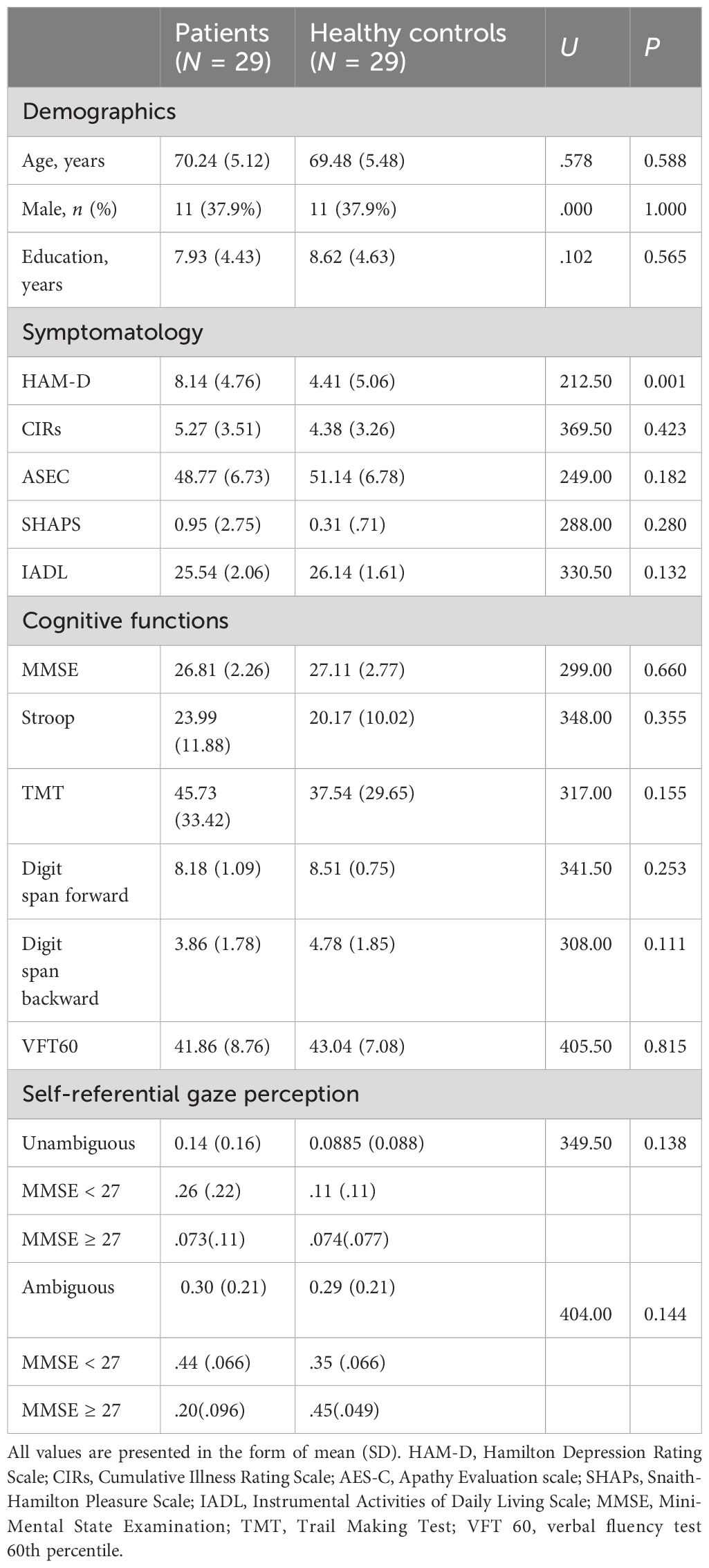
Table 1 Group difference in demographics, cognitive function, and symptomology.
No significant group difference was identified for ambiguous-SRGP (U = 404.00, p = 0.144) or unambiguous-SRGP rate (U = 349.50, p = 0.138). A two-way analysis of variance (ANOVA) was conducted to explore the interaction effect of subject group and cognitive function (Table 2). Global cognition was compared using median split of MMSE, that is 27 as cutoff. There was statistical significant interaction effect, [F(1, 47) = 4.719, p =.035], main effects of subject group, F(1,47) = 4.631, p = .037, and MMSE severity, F(1, 47) = 10.010, p =.003, on unambiguous SRGP rate. Pairwise comparison revealed higher MMSE scores in patients had a significantly lower unambiguous SRGP (M = .074, SD = .11) rate than those with lower MMSE scores (M = .26, SD = .22). No significant interaction effect was found in the ambiguous SRGP task performance (p = .252).
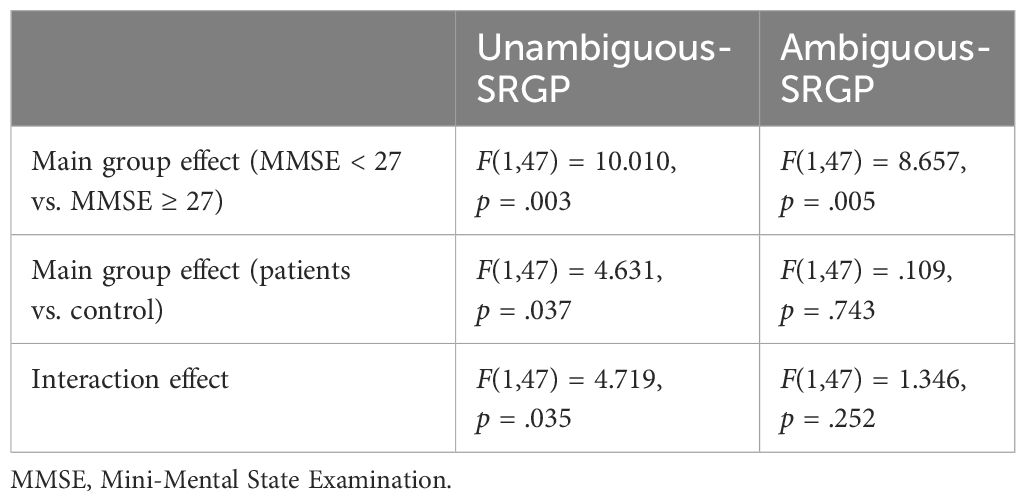
Table 2 ANOVA on differentiating group difference in cognitive function on SRGP.
Relationships between clinical and cognitive function, and SRGP were explored, when age, gender, and year of education were controlled for (Table 3). The results of linear regressions indicated that only in patient group alone, MMSE (β = −.060, p = .002), CIRS (β = .026, p = .018), and digit span forward (β = −.070, p = .020) contributed to ambiguous SRGP rate. While CIRs contributed to the unambiguous SRGP in both patients (β = .020, p = .021) and in HCs (β = .009, p = .039), only MMSE (β = −.045, p = .002) and VFT (β = −.008, p = .046) contributed to the unambiguous SRGP in patient group. And, digit span forward (β = −.031, p = .046) contributed to the unambiguous SRGP only on control group.
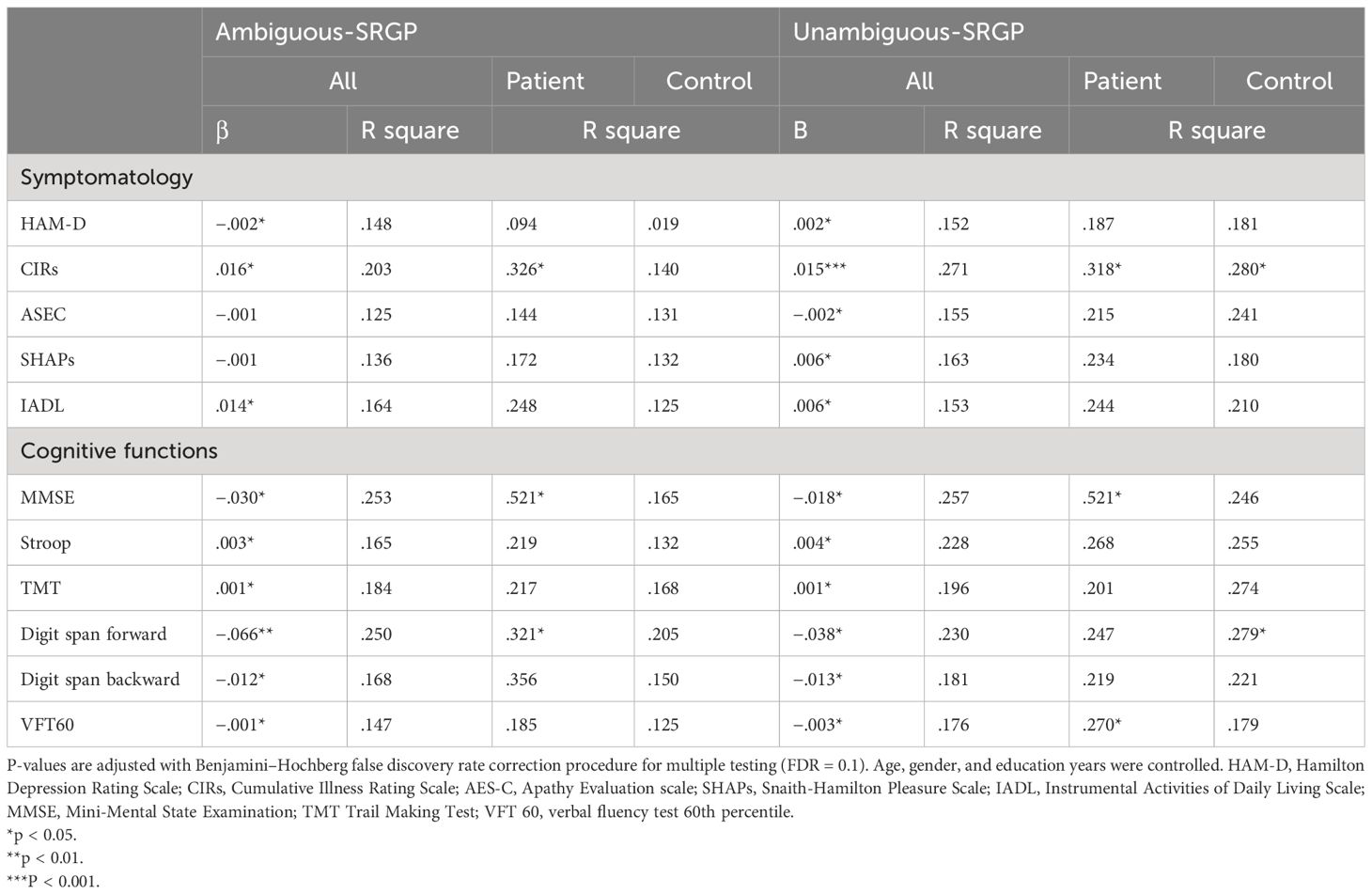
Table 3 Relationships between SRGP responses, clinical and cognitive information.
To the best knowledge of the authors, this is the first study to explore the relationship between cognition and SRGP in the LLD population. This study explored the difference in SRGP between LLD patients and HCs. There was a trend for group difference in SRGP bias but has not reached significant level. However, when cognitive abilities were taken into account, patients with better MMSE scores showed less unambiguous-SRGP bias than those with lower MMSE scores, this difference was not found in HCs. Consistent with our hypothesis, global cognition and executive function were associated with SRGP rate. Medical comorbidity was also positively correlated to SRGP rate. Cognitive measurements on global cognition and working memory, as well as medical comorbidity significantly explained the ambiguous-SRGP rate only in patients. Meanwhile, unambiguous-SRGP bias was contributed by the global cognition and verbal functioning in patients, whereas in control group, working memory performance differentiated perception bias.
The null group difference in both ambiguous-SRGP and unambiguous-SRGP may be explained by the limited sample size of this study. In addition, most of the LLD subjects in the current study fall only into mild depression category. As mentioned, MDDs showed significant impairment in social cognition and such impairment appears to be positively associated with the severity of depression (7). Therefore, we suggest a significant group difference may be present when a larger sample size with more severe depression subjects is included for comparison.
Despite no significant difference in SRGP between LLD and HC group, we found that LLD with more cognitive impairment showed a significant SRGP bias compared with those with less cognitive impairment, particularly in the unambiguous stimuli. A possible explanation is that the more difficult condition (i.e., ambiguous SRGP) requires more cognitive resources; thus, patient or HC performed levelly inferior than unambiguous SRGP. In other words, the inherent cognitive bias tendency in depressive disorder only prevailed in the easier condition (i.e., unambiguous SRGP) that requires less cognitive resources, highlighting the influence of possible cognitive bias in LLD but not HC.
LLD subjects with more impaired cognitive function was related to greater SRGP bias in both ambiguous and unambiguous gaze direction, similar to schizophrenia patients (12). In patients with LLD, greater working memory was related to less ambiguous-SRGP bias. Such pattern was not found in HCs. On the other hand, in unambiguous gaze perception condition, global cognition and executive functioning explained unambiguous-SRGP rate in patients. In HC, working memory ability served as the only cognitive indicator to explain unambiguous-SRGP rate. In other words, consistent with our hypothesis, the presence of SRGP bias in LLD patients vary according to the degree of cognitive impairment. Based on this finding, we postulated that the cognitive function in LLD patients plays an unique role in explaining the SRGP bias. The relatively intact cognitive function may help LLD patients to filter the SRGP bias. Regarding only those LLD subjects with significant cognitive impairment displayed SRGP bias, this may be explained by losing the “error detection” function, which believed to be associated with executive function impairment (24). Specifically, our findings revealed better working memory and executive functions in patient had less SRGP bias which was in supportive of our postulation. This adds new evidence into understanding social cognition in depression in older adults.
Existing research revealed that symptomatic psychosis patients displayed higher ambiguous SRGP and were negatively associated with cognitive functions in the psychosis population (12, 25). The findings are consistent with our results. Since cognitive impairment is very common in LLD, we expected that impairment would extend to eye gaze interpretation. In other words, the high SRGP bias in gaze perception task may indicate the presence of a significant cognitive impairment in addition to self-referential bias in LLD, by further replicating and expanding upon the current study, the SRGP task could serve as a potential screening tool to identify the high-risk group likely to develop dementia.
The limitation of this study is the sample size was small. Group difference in SRGP bias was not detected which might be contributed by the limited severity of depression subjects for comparison. In addition, depressive symptoms closely related to gaze perception including thought delusion or reference ideation were not assessed in this study. Therefore, future studies can further explore the SRGP bias in depression patients in various directions. First, future studies can include subjects with from mild to severe depression to further understand the role of SRGP in depression of different severity. Second, the inclusion of assessing thought delusion and thought insertion symptoms in depression patients can help to elucidate if SRGP bias is sensitive towards the particular symptoms that is present in both psychosis patients and depression patients, or it is a unique trait factor of LLD. Our study focused on the role of executive function and SRGP in which other cognitive domains such as memory or visual spatial functioning can be additional measures in future studies to help elucidate the predictive value and differentiation of different types of dementia, including AD, vascular dementia or frontotemporal dementia.
The present study examined the difference in SRGP bias between LLD patients and HCs. Results revealed that cognitive functioning modulated the interpretation bias in LLD patients, that SRGP is likely to be a trait phenomenon. The greater SRGP bias in patients may reflect social cognition deterioration, impairing the social interaction and functioning of LLD patients. Early intervening and identifying cognitive decline facilitate better prognosis and treatment effectiveness; hence, further studies on gaze perception task could explore the potential of the SRGP task as a screening tool for high-risk group of LLD likely to develop dementia. Future studies could explore the difference in SRGP bias in LLD patients with a bigger sample and greater severity to elucidate the differential effect of cognition to SRGP bias in LLD population.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
This current study was approved by the Institutional Review Board of the University of Hong Kong and Hong Kong West Cluster of Hospital of Authority (IRB: UW 22-712). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JN drafted and prepared the manuscript. JN, CC, and SC contributed to the interpretation of data. JN and HT contributed to the acquisition and analysis of data. CC, WCC, and SC contributed to the conception and design of the study. All authors contributed to the article and approved the submitted version.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Alexopoulos GS. Mechanisms and treatment of late-life depression. Trans Psychiatry. (2019) 9:1–16. doi: 10.1038/s41398-019-0514-6
3. Alexopoulos GS, Kelly RE Jr. Research advances in geriatric depression. Focus. (2013) 11:107–17. doi: 10.1176/appi.focus.11.1.107
4. Taylor WD. Depression in the elderly. New Engl J Med. (2014) 371:1228–36. doi: 10.1056/NEJMcp1402180
5. Linnemann C, Lang UE. Pathways connecting late-life depression and dementia. Front Pharmacol. (2020) 11:279. doi: 10.3389/fphar.2020.00279
6. Kliemann D, Adolphs R. The social neuroscience of mentalizing: challenges and recommendations. Curr Opin Psychol. (2018) 24:1–6. doi: 10.1016/j.copsyc.2018.02.015
7. Weightman MJ, Air TM, Baune BT. A review of the role of social cognition in major depressive disorder. Front Psychiatry. (2014) 5:179. doi: 10.3389/fpsyt.2014.00179
8. Elliott R, Zahn R, Deakin J, Anderson IM. Affective cognition and its disruption in mood disorders. Neuropsychopharmacology. (2011) 36:153–82. doi: 10.1038/npp.2010.77
9. Everaert J, Podina IR, Koster EH. A comprehensive meta-analysis of interpretation biases in depression. Clin Psychol Rev. (2017) 58:33–48. doi: 10.1016/j.cpr.2017.09.005
10. Everaert J. Interpretation of ambiguity in depression. Curr Opin Psychol. (2021) 41:9–14. doi: 10.1016/j.copsyc.2021.01.003
11. Yao B, Mueller SA, Grove TB, McLaughlin M, Thakkar K, Ellingrod V, et al. Eye gaze perception in bipolar disorder: Self-referential bias but intact perceptual sensitivity. Bipolar Disord. (2018) 20:60–9. doi: 10.1111/bdi.12564
12. Chan SKW, Liu T, Wong AOY, Wong GHY, Hsiao J, Hui CLM, et al. Self-referential gaze perception of patients with schizophrenia and its relationship with symptomatology and cognitive functions. Schizophr Res. (2021) 228:288–94. doi: 10.1016/j.schres.2020.12.034
13. Liu P, Hayden EP, Dougherty LR, Leung H-C, Goldstein B, Klein DN. The development of depressogenic self-schemas: Associations with children’s regional grey matter volume in ventrolateral prefrontal cortex. Dev Psychopathol. (2020) 35(3):1000–10. doi: 10.31234/osf.io/zmpy8
14. Auerbach RP, Stanton CH, Proudfit GH, Pizzagalli DA. Self-referential processing in depressed adolescents: A high-density event-related potential study. J Abnormal Psychol. (2015) 124:233. doi: 10.1037/abn0000023
15. Connolly SL, Abramson LY, Alloy LB. Information processing biases concurrently and prospectively predict depressive symptoms in adolescents: Evidence from a self-referent encoding task. Cogn Emotion. (2016) 30:550–60. doi: 10.1080/02699931.2015.1010488
16. Moran JM, Jolly E, Mitchell JP. Social-cognitive deficits in normal aging. J Neurosci. (2012) 32:5553–61. doi: 10.1523/JNEUROSCI.5511-11.2012
17. Slessor G, Phillips LH, Ruffman T, Bailey PE, Insch P. Exploring own-age biases in deception detection. Cogn Emotion. (2014) 28:493–506. doi: 10.1080/02699931.2013.839438
18. Sambataro F, Safrin M, Lemaitre HS, Steele SU, Das SB, Callicott JH, et al. Normal aging modulates prefrontoparietal networks underlying multiple memory processes. Eur J Neurosci. (2012) 36:3559–67. doi: 10.1111/j.1460-9568.2012.08254.x
19. Rakoczy H, Harder-Kasten A, Sturm L. The decline of theory of mind in old age is (partly) mediated by developmental changes in domain-general abilities. Br J Psychol. (2012) 103:58–72. doi: 10.1111/j.2044-8295.2011.02040.x
20. Bernstein DM, Thornton WL, Sommerville JA. Theory of mind through the ages: Older and middle-aged adults exhibit more errors than do younger adults on a continuous false belief task. Exp Aging Res. (2011) 37:481–502. doi: 10.1080/0361073X.2011.619466
21. Yeung P, Wong L, Chan C, Leung J, Yung C. A validation study of the Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) in Chinese older adults in Hong Kong. Hong Kong Med J. (2014) 20:504–10. doi: 10.12809/hkmj144219
22. Zheng Y, Zhao J, Phillips M, Liu J, Cai M, Sun S, et al. Validity and reliability of the Chinese Hamilton depression rating scale. Br J Psychiatry. (1988) 152:660–4. doi: 10.1192/bjp.152.5.660
23. Koivisto M, Grassini S. Neural processing around 200 ms after stimulus-onset correlates with subjective visual awareness. Neuropsychologia. (2016) 84:235–43. doi: 10.1016/j.neuropsychologia.2016.02.024
24. Rabinovici GD, Stephens ML, Possin KL. Executive dysfunction. CONTINUUM: Lifelong Learn Neurol. (2015) 21:646. doi: 10.1212/01.CON.0000466658.05156.54
25. Chan SKW, Hsiao J, Wong AOY, Liao Y, Suen Y, Yan EWC, et al. Explicit and implicit mentalization of patients with first-episode schizophrenia: a study of self-referential gaze perception with eye movement analysis using hidden Markov models. Eur Arch Psychiatry Clin Neurosci. (2022) 272(7):1335–45. doi: 10.1007/s00406-022-01383-y
Keywords: late-life depression, gaze perception, social cognition, mentalisation, early detection
Citation: Ngan STJ, Cheng CPW, Chan WC, Tsui KHH, Chan SMC and Chan KWS (2024) The modulation effect of cognition on mentalization in late-life depression: a study of gaze perception—a potential screening tool for high-risk group of late-life depression. Front. Psychiatry 15:1199119. doi: 10.3389/fpsyt.2024.1199119
Received: 05 April 2023; Accepted: 12 April 2024;
Published: 01 May 2024.
Edited by:
Francesco Panza, University of Bari Aldo Moro, ItalyReviewed by:
Pui Yin Chung, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2024 Ngan, Cheng, Chan, Tsui, Chan and Chan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Calvin Pak Wing Cheng, Y2hlbmdwc3lAaGt1Lmhr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.