 Barbara Carpita1*
Barbara Carpita1* Benedetta Nardi1
Benedetta Nardi1 Chiara Bonelli1Enrico Massimetti2
Chiara Bonelli1Enrico Massimetti2 Giulia Amatori1
Giulia Amatori1 Ivan Mirko Cremone1Stefano Pini1Liliana Dell’Osso1
Ivan Mirko Cremone1Stefano Pini1Liliana Dell’Osso1- 1Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy
- 2North-Western Tuscany Region NHS Local Health Unit, Department of Psychiatry, Pisa, Italy
Introduction: Due to their similar behavioral presentation, it can sometimes be challenging to distinguish between a social anxiety disorder (SAD) and the social avoidance that is frequently described in autism spectrum disorder (ASD). Moreover, a growing body of evidences is reporting that a significant proportion of subjects with ASD also meet the requirements for SAD and, vice versa, subjects with SAD tend to exhibit a higher prevalence of autistic traits.
Aim: In this framework, the current study aims to evaluate prevalence and correlates of autistic traits in a sample of adult subjects diagnosed with SAD and healthy controls (HC), also evaluating which autism spectrum dimensions may statistically predict higher SAD symptoms.
Methods: 56 subjects with a clinical diagnosis of SAD and 56 gender and age matched HC were recruited from the Psychiatric Clinic of the University of Pisa. Subjects were assessed with the SCID-5, the Social Anxiety Spectrum – Short Version (SHY- SV) and the Adult Autism Subthreshold Spectrum (AdAS Spectrum).
Results: SAD group scored significantly higher in all AdAS Spectrum and SHY-SV domains and total score compared to the HC group with no significant gender difference. SHY-SV total and domain scores, were strongly and positively and strongly correlated with all AdAS Spectrum domains and total score. AdAS Spectrum total score and Childhood/Adolescence, Non-Verbal Communication, Empathy and Restricted interests and Rumination domain scores score were significant predictors of higher SHY-SV score.
Conclusion: Our results confirm the link between SAD and autistic traits also in adult population, describing not only high levels of autistic traits in SAD adults, but also significant correlations between many core features of the two disorders and a predictive role of autistic traits on higher SAD symptoms.
1 Introduction
Social anxiety disorder (SAD), with a reported lifetime prevalence up to 13% (1, 2) is one of the most prevalent mental illnesses and a topic of significant interest for researchers, although being frequently neglected in clinical settings. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition – Text Revision (DSM-5-TR), SAD is a syndrome characterized by elevated fear and anxiety that manifest before or during social settings, worries about being poorly perceived, and a propensity to avoid interactions (3). The feelings of fear and anxiety experienced by the patients typically cover a wide range of scenarios: some patients only experience mild symptoms occurring exclusively in specific contexts, while others experience more severe symptoms that interfere with almost all social interactions (e.g., having a conversation or meeting new people, being watched while eating or drinking, performing in front of others) (3, 4). Typically, SAD has an early onset and a chronic course, frequently lasting lifelong (5–7). In most cases, symptoms begin throughout adolescence and last for several years before assistance is sought (8), rising significantly the chances of dropping out of school, failing exams (9), and failing to graduate (10, 11). Moreover, SAD is linked to severe functional disability and noticeably diminished quality of life (9), raising the likelihood of developing another major comorbid disorder such as anxiety and mood disorders and substance or alcohol use disorders throughout the course of the lifespan (12–15).
Furthermore, while SAD can progress and worsen with the development of paranoic delusion, on the other social anxiety has also been reported as a major component in patients with schizophrenia, influencing its treatment, progression and prognosis (16, 17). In particular, the risk of developing depression, is significantly increased by SAD and, in this case, linked to a worse prognosis and a higher chance of suicide attempts (18, 19). In this context, one of the most common co-occurrent disorder reported with SAD is autism spectrum disorder (ASD) (20).
One of the primary concerns in the field of SAD since its conceptualization, has been the establishment of a diagnostic threshold (21). Many researchers indicated that SAD should be categorized as spectrum of severity rather than a discrete condition based on subjectively selected thresholds (22), and that the borders of SAD should be established by severity rather than qualitative traits (23, 24). In this framework, the most recent editions of the DSM introduced some adjustments to the chapter on SAD, reflecting a new and improved knowledge of the disorder in various social contexts (3, 24). Following this idea, some research postulated that SAD should be better classified as a dimensional continuum (22). According to such researches, a spectrum model of psychopathology can help identify the wide range of sub-threshold manifestations that may coexist with the primary mental condition (25). The term “spectrum” is used in this context to characterize mental health illnesses that include a variety of symptoms and behavioral patterns linked to a recognized DSM or ICD construct (25). While the spectrum of symptoms and traits includes the primary symptoms of the current DSM diagnostic categories, it also includes sub-clinical and atypical manifestations, as well as temperamental and/or personality traits and isolated signs and symptoms, symptom clusters, and behavioral patterns (26–32). According to this viewpoint, spectrum symptomatology is similar to the hidden section of an iceberg beneath the water’s surface, whereas full-blown diagnostic criterion symptoms represent only the visible portion (25). Following this model, the “Social Phobia Spectrum Self-report” (SHY-SR) instrument was developed and validated in the early 2000s as part of the “spectrum project,” an international collaboration aimed at shedding light on the validity of a dimensional approach to psychopathology (25–32). The SHY-SR was designed to measure not only the prototypic symptoms of SAD, but also atypical presentations, temperamental features, and other notable clinical and sub-clinical aspects associated with the primary symptoms (33, 34). The questionnaire had a high internal consistency, strong inter-rater reliability, and discriminant validity and throughout the years it has been employed in a variety of clinical contexts throughout the last few decades (7, 33, 35, 36). However, due to the excessively long time for its compilation and some outmoded and superfluous items, recently its application in routine clinical practice has been difficult; for this reason, the same authors recently proposed a shortened and renewed version, the Social Anxiety Spectrum – Short Version (SHY-SV) (37).
ASD is a frequent neurodevelopmental disorder that affect at least 1% of the population (38). The core characteristics of ASD are impaired social communication skills, repetitive and restricted interests and behaviors, and hypo-and hyper-reactivity to sensory stimuli (3). The more recent conceptualization of ASD depicts it as a heterogeneous disorder whose symptoms lie across a continuum that ranges from the milder presentations to most severe ones. In the recent years, research on ASD has emphasized the need to examine milder, sub-clinical manifestations of the autism spectrum as well as the full-blown clinical forms, which appear to be distributed along a continuum from the general to the clinical population (31, 39–42). First-degree relatives of people with ASD were firstly studied for sub-threshold autistic features, which are referred to as “broad autism phenotype” (43, 44); however, additional research has discovered other groups of people that are more likely to exhibit autistic features, from students of scientific courses to psychiatric patients with different types of disorders (44–53). In particular, subthreshold autistic traits are of interest because they exert a negative impact on quality of life and to represent a major risk factor for the emergence of various psychiatric disorders, as well as suicidal thoughts and behaviors (54–57). However, considering that autism spectrum is still a condition mainly associated to child healthcare due to its early onset, subthreshold autistic traits, or even milder clinical forms of ASD may easily remain under-recognized and undertreated during adulthood, silently worsening the trajectory of other comorbid disorders (58).
Due to their similar behavioral presentation, it can sometimes be challenging to distinguish between SAD and the social avoidance that is frequently described in ASD (59, 60). To this date, many researches have demonstrated that the symptoms of SAD and ASD significantly overlap in many fields. The key areas where most of the symptomatologic overlap happens are those of social interaction and social skills (61); for example, the two disorders share the difficulties in talking in front of others (62) and the avoidance of eye contact as well as paying little attention to the area around an interlocutor’s eyes (63). In particular, atypicalities in social attention have been linked to both SAD and ASD. In the first the avoidance of social clues like faces with direct gaze can make it harder for the subject to reappraise or get used to the perceived threat, thus contributing to the maintenance of SAD symptoms (64). In the latter, atypical social attentiveness has been observed to precede clinical signs in ASD (65, 66). A growing body of evidences highlighted that a significant proportion of subjects with ASD also meet the requirements for SAD (67–69), while, in a similar way, subjects with SAD tend to exhibit a higher prevalence of autistic traits (67, 70). In this context, in light due to the relevance of autistic traits even in non-ASD clinical samples, some authors proposed the idea that various psychiatric illnesses might arise as a result of a neurodevelopmental alteration comparable to the one connected to ASD (38, 58, 71, 72), where the vast range of ASD presentations ought to be viewed as the tip of a larger iceberg that contains a number of clinical and non-clinical phenotypes (31, 73).
Accordingly, the recent literature has stressed the necessity to consider disorders like SAD and ASD as extremes along natural continuums phenotypes of traits that are typically distributed throughout the general population, implying the absence of clear-cut borderlines between having no symptoms, increased sub-clinical traits and a formal diagnosis, while even in the latter there are significant individual variances in symptom strength (74–78). Moreover, given the heterogeneity of social competence among the general population, it is plausible that difficulties in social competence functions may link autism spectrum symptoms to increased social anxiety even in non-clinical individuals (79, 80).
In this framework, the aim of the present study was to evaluate prevalence and symptomatologic correlates of autistic traits in a sample of adult subjects diagnosed with SAD and healthy controls (HC), by using two self-report questionnaires, the SHY-SV and the AdAS Spetrum, validated to assess not only the typical symptoms of the two disorders as described by DSM-5-TR criteria, but also the full spectrum of signs and symptoms (so-called atypical as long as they are not included in the diagnostic criteria of the DSM), temperamental traits, and behavioral manifestations of SAD and ASD. Possible autism spectrum dimensions statistically predictive of higher SAD symptoms were also evaluated.
2 Methods
Data have been collected between September 2022 and March 2023 at the Psychiatric clinic of the University of Pisa.
2.1 Study sample and procedure
The total sample was made of 112 subjects belonging to two diagnostic groups, the SAD group and the HC group, which both counted 56 subjects each. The subjects in the SAD group were recruited from out-patients afferent at the Psychiatric Clinic of the University of Pisa, while subjects in the HC group belonged to health care and paramedical personnel; the recruitment of the latter was carried following a sex-and gender-matched criteria. All subjects had to be between the ages of 18 and 70 and be prepared to sign an informed consent in order to be recruited. The diagnoses of SAD, as well as the lack of mental disorders among HC individuals, were confirmed using the Structured Clinical Interview for DSM-5, Research Version (SCID-5-RV) (81). Exclusion criteria included an age under 18 or over 70, language or intellectual impairment that made the examinations difficult to complete mental disabilities, lack of collaboration skills, and persistent psychotic symptoms.
The presence of BD or Major Depressive Disorder was excluded through the use of the SCID-5-RV and clinical and anamnestic evaluation at the time of recruitment. However, a small number of participants were contemplated to be experiencing a depressive episode as long as the depression symptoms were not as severe as those of the category disorder. Similarly, the existence of other anxiety disorders was acknowledged as long as their symptoms were noticeably less severe than the ones of the SAD.
The study was conducted in accordance with the Declaration of Helsinki. The study was fully explained to the eligible individuals, who then gave their written informed permission after having a chance to ask any questions. The subjects received no compensation for taking part.
2.2 Measures
Assessment procedures included the SCID-5-RV (81), the Social Anxiety Spectrum – Short Version questionnaire (SHY-SV) and the Adult Autism Subthreshold Spectrum (AdAS Spectrum). Questionnaire evaluations were carried by psychiatrists, who were trained and certified in the use of the study instruments.
2.2.1 Social anxiety spectrum – short version questionnaire
The SHY-SV consists in 139 items organized in 5 domains (Interpersonal sensitivity, Behavioral inhibition, Performance, Social situations and Substance Abuse) and an appendix (Childhood and adolescence). The answers to the various items are coded in a dichotomous way (yes/no) and the scores relating to the single domains and appendices are obtained by counting the number of positive answers. The SHY-SV was developed by Dell’Osso et al. (37); the validation study reported strong internal consistency, great test–retest reliability and convergent validity with other dimensional measures of SAD.
2.2.2 Adult autism subthreshold spectrum
AdAS Spectrum is a self-report questionnaire designed to assess the wide range of autism spectrum manifestations in adults who do not have language or intellectual disabilities. The questionnaire consists of 160 organized into seven domains: Childhood and adolescence, Verbal communication, Nonverbal communication, Empathy, Inflexibility and Adherence to Routine, Restricted interests and rumination and Hyper-and Hyporeactivity to Sensory Input. The answers to the various items are coded in a dichotomous way (yes/no) and the scores relating to the single domains and appendices are obtained by counting the number of positive answers. The AdAS Spectrum was developed by Dell’Osso et al. (32); the validation study reported a high internal consistency, excellent test–retest reliability (Kunder-Richiardson coeffi-cient = 0.964, ICC = 0.976) and convergent validity with other dimensional measures of autism spectrum (31). The validity and reliability of the questionnaire was confirmed by further studies (39, 40) and a diagnostic threshold was defined at the score of 70.
2.3 Statistical analysis
Student’ t-test and Chi-square tests were used for comparing socio-demographic variables among group. Student’ t-test was used to compare the scores obtained by the two diagnostic groups on the SHY-SV and AdAS questionnaires as well as to compare the scores obtained in the two questionnaires in the SAD group divided by gender. Pearson’s correlation coefficient was used for evaluating the pattern of correlations among the scores reported on the two psychometric instruments within the SAD, and HC subjects. Subsequently, in order to evaluate which AdAS Spectrum domains were statistically predictive of SHY-SV score in the sample, linear regression analyses were performed with SHY-SV scores as the dependent variable and AdAS Spectrum total (first regression) and domain scores (second regression) as independent variables. All statistical analyses were performed with SPSS version 26.0 (82).
3 Results
The SAD sample reported a mean age of 39.57 years (±12.56) and consisted of 29 (51.8%) males and 27 (48.2%) females. The HC group reported a mean age of 38.52 years (±13.05) and consisted of 25 (44.6%) males and 31 (55.4%) females (see Table 1). Regarding the educational level, 14 (12.5%) subjects reported to have a master degree, 39 (38.4%) subjects reported to have a degree, 47 (42%) subjects referred to have graduated, 10 (8.9%) subjects had a middle school certificate, 1 (0.9) subject did not finish the elementary school and 1 subject preferred not to disclose. Regarding the occupational role, 23 (20.5%) subjects were students, 19 (17%) subjects were unoccupied, 19 (17%) subjects were housewives, 35 (31.3%) subjects were employed, 1 (0.9%) subject was retired and 15 (13.4%) subjects preferred not to disclose. Regarding the marital status 13 (11.6) subjects referred to live with their parents, 19 (17%) subjects were married, 29 (25.9%) subjects were unmarried, 6 (5.4%) subjects were divorced, 1 (0.9%) subject was a widower and 44 (39.2%) subjects preferred not to disclose.
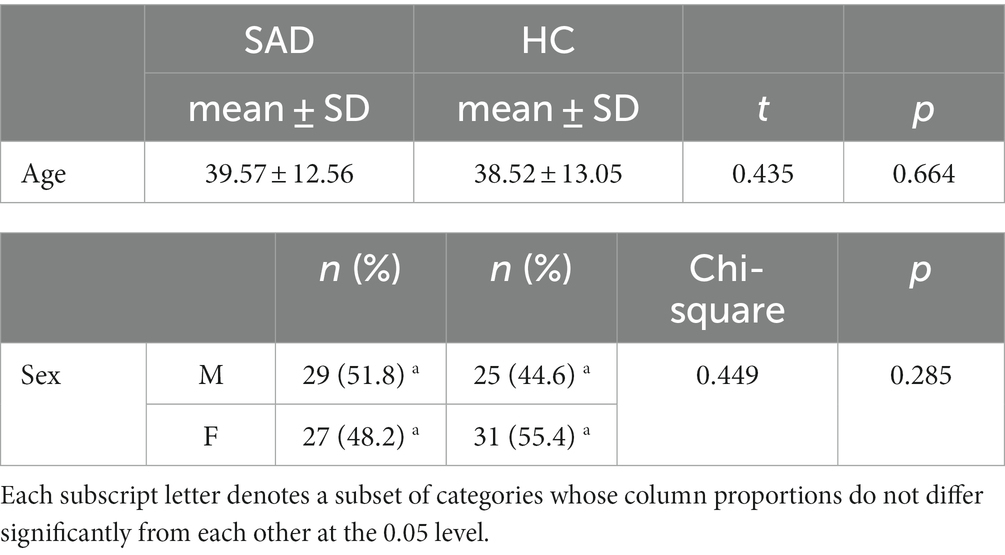
Table 1. Age and sex in the overall sample and comparison between diagnostic groups.
Student t-test results showed that SAD group scored significantly higher in all AdAS Spectrum and SHY-SV domains as well as in their total compared to the HC group (see Tables 2, 3).
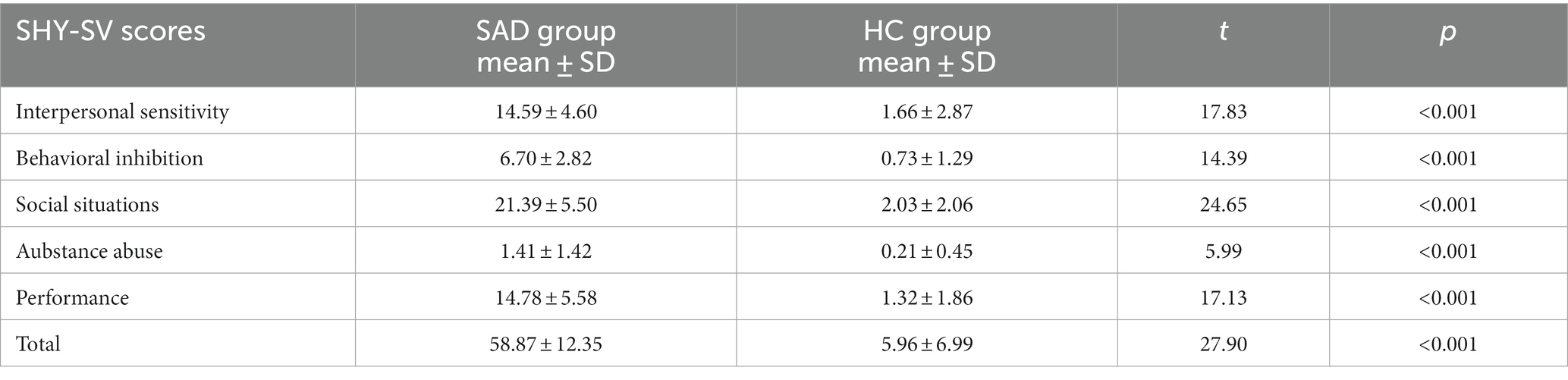
Table 2. Comparison of SHY-SV scores among the diagnostic groups.
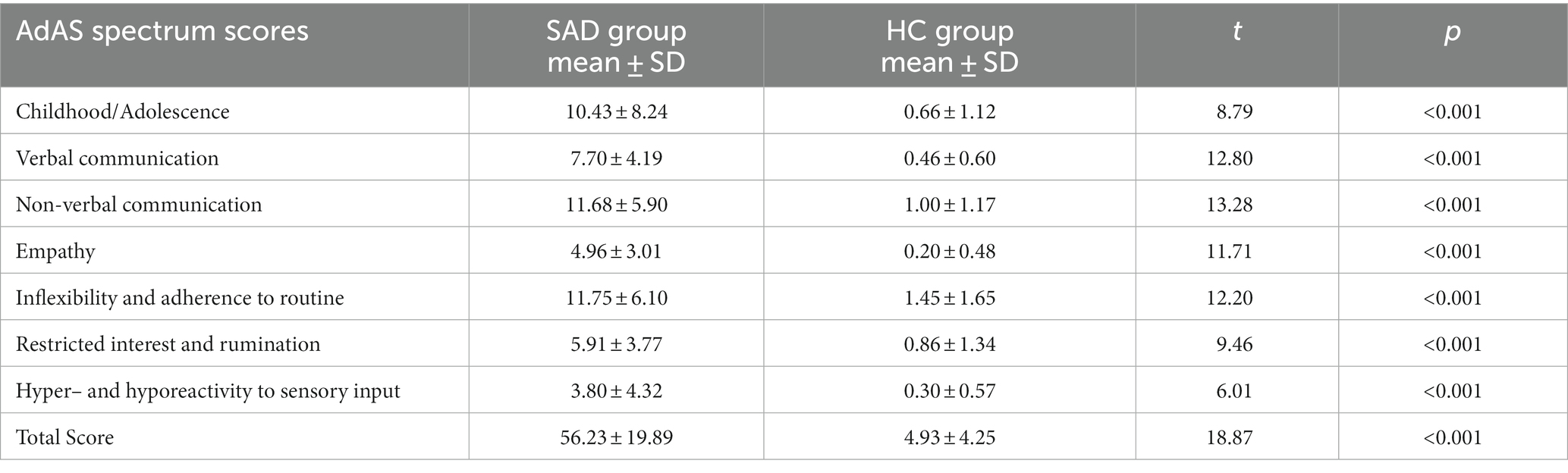
Table 3. Comparison of SHY-SV scores among the diagnostic groups.
Moreover, results from the comparison between gender in the SAD group highlighted no significative difference in the scores obtained on the AdAS Spectrum (see Table 4).
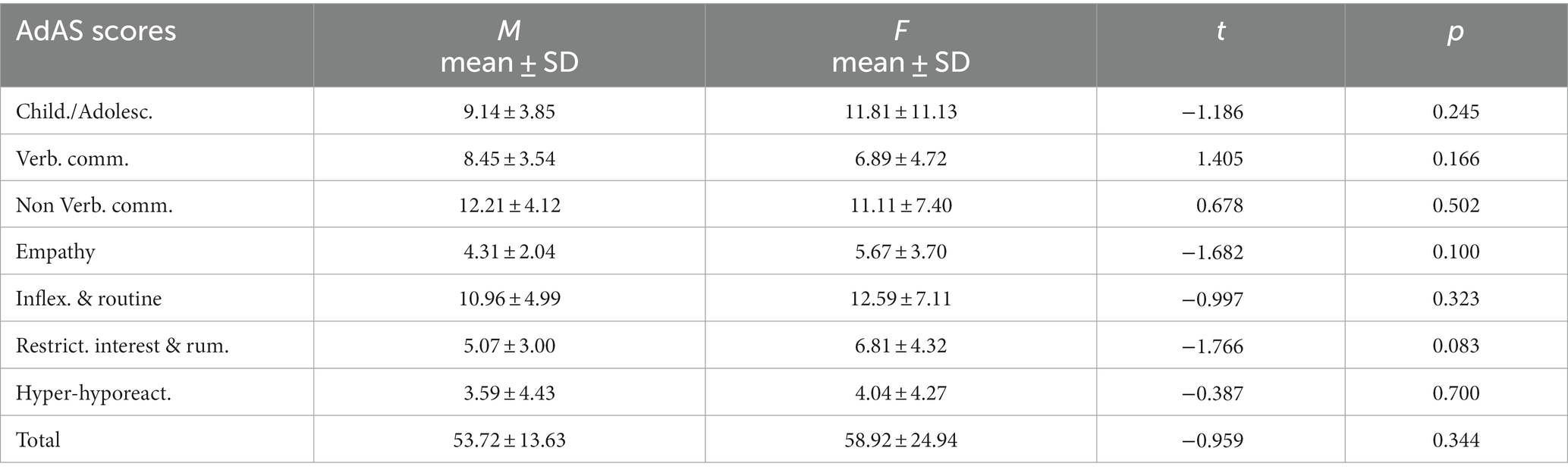
Table 4. Comparison of AdAS spectrum scores between males and females in the SAD group.
According to the correlation analysis, in the total sample, the total SHY-SV scores, as well as all SHY-SV domains scores, were significantly and positively correlated with all AdAS Spectrum domain and AdAS total score. All correlation coefficients were strong, with the exception of those reported for the SHY-SV domain Substance abuse, which were medium or weak (see Table 5).
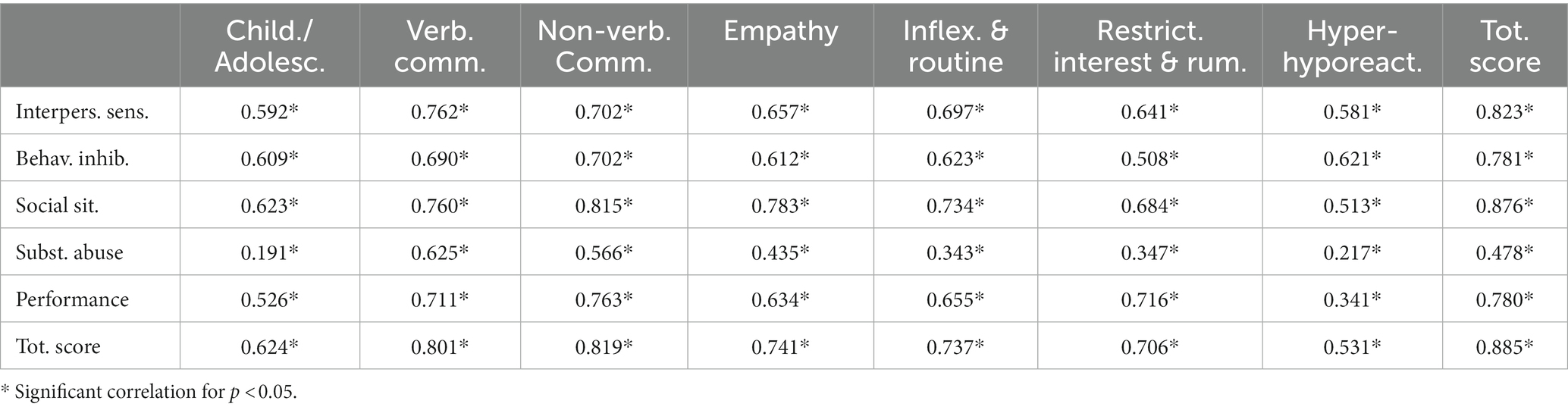
Table 5. Pearson’s correlations coefficients (r) among SHY-SV domains score and AdAS spectrum scores in the total sample.
Lastly, results from linear regression analysis showed that AdAS Spectrum total score was a significant predictor of a higher SHY-SV score (beta = 0.88; t = 19.92; p < 0.001) (see Table 6). A further linear regression highlighted the AdAS Spectrum Childhood/Adolescence (beta = 0.12; t = 2.19; p = 0.031), Non Verbal Communication (beta = 0.35; t = 4.28; p < 0.001), Empathy (beta = 0.26; t = 4.54; p < 0.001), Restricted interests and Rumination (beta = 0.21; t = 3.10; p = 0.002) domain scores as significant positive predictors of high SHY-SV total scores (see Table 7).

Table 6. Linear regression analysis with SHY-SV total score as a dependent variable and AdAS Spectrum total score as independent variables in the total sample.
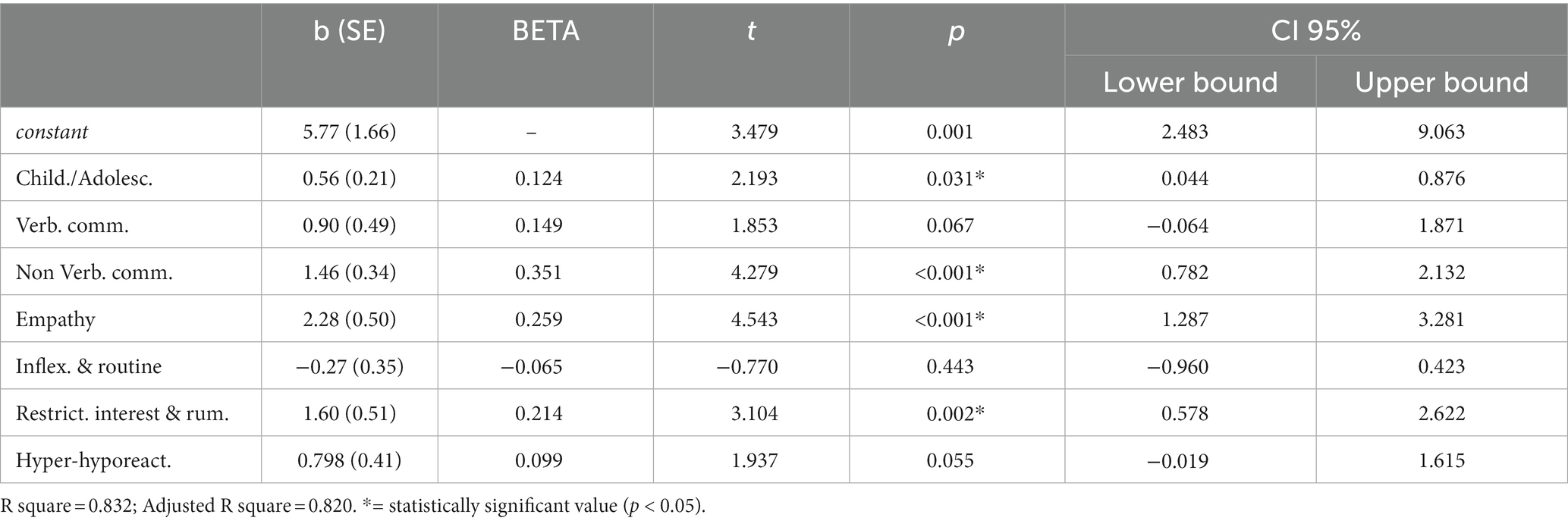
Table 7. Linear regression analysis with SHY-SV total score as a dependent variable and AdAS spectrum domains as independent variables in the total sample.
4 Discussion
According to our results, the group of subjects diagnosed with SAD not only scored, as expected, significantly higher in the SHY-SV questionnaire than the HC group, but also reported a higher prevalence of positive answers in all AdAS Spectrum domains as well as in the questionnaire’s total score with no significant difference when compared by gender. Moreover, we globally found significant and strong positive correlations between SHY-SV and AdAS Spectrum domain scores.
Our results are in line with previous studies, confirming the significant presence of autistic traits in adults with SAD. Previous researches, mainly conducted in children, adolescents or young adults, while exploring the relationship between ASD and SAD in clinical and non-clinical samples (83–85) reported that the symptoms of SAD and ASD significantly overlap in many fields, to the point that it can sometimes be challenging to distinguish between SAD and the social avoidance that is frequently described in ASD (58, 60). The recent literature reported how the symptomatologic overlap between the two conditions has been mainly identified, in children and adolescents, in the areas of social interaction and social skills (61), including difficulties in talking in front of others (62) and the avoidance of eye contact (63). Moreover, many studies highlighted not only that traits of both disorders can co-occur and are highly correlated, but also that the correlation is not exclusively due to the symptomatologic overlap between the disorders, nor to artefacts of measurement errors. Additionally, alongside the evidences of a high prevalence of SAD in ASD subjects (67–70) and similarly of autistic traits in SAD patients (67, 70), some studies reported how autistic traits and SAD symptoms are correlated even in subjects that do not meet the full diagnostic criteria while, in neurotypical children, higher autistic traits have been associated with a greater risk of developing SAD later in life (86).
According to our results, the AdAS Spectrum total score and AdAS Spectrum Childhood/Adolescence, Non Verbal Communication, the Empathy and the Restricted interests and Rumination domains were significant positive predictors of higher scores in the SHY-SV. While previous studies in children and adolescents also reported how greater autistic traits significantly predict higher SAD symptoms (60, 68), the finding of Non Verbal communication and Empathy domain scores being positive predictors of SAD is consistent with a large body of research that identified in deficits of social competence the main common background for the relationship between SAD and autistic traits (80). Indeed, subjects with elevated autistic traits are more likely to have lower social skills, which can be shown as difficulties in social interactions with their peers as well as a higher vulnerability to bullying and victimization (87). Similarly, reduced social competence may predict, also in neurotypical subjects, negative changes in peer interactions and stressful social experiences, playing a crucial role in the development of SAD (88–90). According to other authors, the combination of increased physiological arousal and decreased social competence, significantly predicted social anxiety symptoms in children with and without ASD (89, 90). Furthermore, somewhat in line with our finding of a predictive role of impaired empathy skills for SAD symptoms, studies that focused on evaluating the Theory of Mind (ToM) in SAD samples reported how higher levels of SAD were related to reduced ToM ability (91–96) and empathic accuracy, especially for positive stimuli (91). As a matter of fact, the use of strategies of social camouflaging have been reported among autistic people in order to cope with social difficulties: while the use of these strategies may actually improve social functioning, it was associated with higher anxiety and depressive symptoms (47). Subjects with high functioning ASD or autistic traits may be more aware of their social incompetence than subjects with more severe forms of ASD, thus more frequently developing SAD symptoms. At the same time, the increased tendency towards ruminative thinking may further increase the risk of brooding about social difficulties and fear of judgment (58, 97). In this context, in light of recent findings that highlighted how the presence of higher autistic traits predicts worse treatment results, it is crucial to understand the mechanisms and processes through which ASD symptoms increase the risk of co-occurring social anxiety symptoms (98, 99). Social competence is a skill that both typically developing children (100) and children with ASD (101) can learn with proper support; therefore, it is critical to investigate how emphasizing social competence development in all children, and particularly in those with neuroatypical traits, may reduce the risk for future distress and impairment, such as increased social anxiety. Social competence has been previously identified as a suitable intervention target to reduce overall social anxiety symptoms both in the clinical and non-clinical population (102, 103). Additionally, it could be a crucial target for the prevention of SAD also among subjects with elevated autistic traits, in line with most first-line psychosocial treatments for ASD (103), but also in neurotypical subjects and even those with psychiatric disorders other than ASD (74). Due to the continuous distribution of autistic and social anxiety traits in the general population, disorders like SAD and ASD could be better conceptualized as extremes along continuum phenotypes of traits, implying the absence of clear-cut borderlines between having no symptoms, increased sub-clinical traits and a formal diagnosis (74–78, 104, 105).
This study should be considered in light of important limitations. First of all, the cross-sectional design prevented us to make inferences about temporal or causal relationship between the investigated variables. In addition, Moreover, the relatively small sample size limits the extensibility of our results. Globally, more studies, possibly with a longitudinal design are needed to clarify the role of underlying autistic traits in the development and militainment of SAD symptoms.
5 Conclusion
In conclusion, our results confirm the link between SAD and autistic traits also in adult population, describing not only high levels of autistic traits in SAD adults, but also significant correlation between many core features of the two disorders and a predictive role of autistic traits on higher SAD symptoms. This data may support the hypothesis of a possible neurodevelopmental basis for different psychiatric conditions: in particular, several psychiatric illnesses may arise as a result of a neurodevelopmental alteration similar to the one associated with ASD (33, 52, 65) where the wide range of ASD manifestations can be seen as the tip of a wider iceberg featuring clinical and non-clinical phenotypes. In this framework, as hypothesized for eating disorders, SAD could also be conceptualized as a specific phenotype of the autism spectrum (93). On this basis and in light of the now recognized existence of an ASD presentation unique to females that differ from the typical male conceptualization, future researches should also delve deeper into the possibility of considering some disorders as gender influenced autistic phenotypes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethical Committee of Azienda Ospedaliera Universitaria Pisana. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BC: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. BN: Investigation, Writing – original draft, Writing – review & editing. CB: Investigation, Writing – review & editing. EM: Formal analysis, Writing – review & editing. GA: Investigation, Writing – review & editing. IC: Conceptualization, Supervision, Writing – review & editing. SP: Conceptualization, Supervision, Writing – review & editing. LD: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kessler, RC, Petukhova, M, Sampson, NA, Zaslavsky, AM, and Wittchen, HU. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. (2012) 21:169–84. doi: 10.1002/mpr.1359
2. Fehm, L, Pelissolo, A, Furmark, T, and Wittchen, H-U. Size and burden of social phobia in Europe. Eur Neuropsychopharmacol. (2005) 15:453–62. doi: 10.1016/j.euroneuro.2005.04.002
3. American Psychiatric Association. Diagnostic and statistical manual for mental disorders, 5th edition – Text revision (DSM-V-TR). Arlington, VA: American Psychiatric Publishing (2023).
4. National Institute for Health and Care Excellence (NICE). Social anxiety disorder: recognition, assessment and treatment, NICE guidelines [CG159] Department of Health (2013).
5. Keller, MB. The lifelong course of social anxiety disorder: a clinical perspective. Acta Psychiatr Scand Suppl. (2003) 108:85–94. doi: 10.1034/j.1600-0447.108.s417.6.x
6. Marazziti, D, Abelli, M, Baroni, S, Carpita, B, Piccinni, A, and Dell'Osso, L. Recent findings on the pathophysiology of social anxiety disorder. Clin Neuropsychiatry. (2014) 20:100–11. doi: 10.1017/S109285291400008X
7. Dell'Osso, L, Abelli, M, Pini, S, Carpita, B, Carlini, M, Mengali, F, et al. The influence of gender on social anxiety spectrum symptoms in a sample of university students. Riv Psichiatr. (2015) 50:295–301. doi: 10.1708/2098.22688
8. Pini, S, Berardi, D, Rucci, P, Piccinelli, M, Neri, C, Tansella, M, et al. Identification of psychiatric distress by primary care physicians. Gen Hosp Psychiatry. (1997) 19:411–8. doi: 10.1016/s0163-8343(97)00053-4
9. Stein, MB, and Kean, YM. Disability and quality of life in social phobia: epidemiologic findings. Am J Psychiatry. (2000) 157:1606–13. doi: 10.1176/appi.ajp.157.10.1606
10. Wittchen, HU, and Fehm, L. Epidemiology and natural course of social fears and social phobia. Acta Psychiatr Scand Suppl. (2003) 108:4–18. doi: 10.1034/j.1600-0447.108.s417.1.x
11. Russell, G, and Topham, P. The impact of social anxiety on student learning and well-being in higher education. J Ment Health. (2012) 21:375–85. doi: 10.3109/09638237.2012.694505
12. Schneier, FR, Johnson, J, Hornig, CD, Liebowitz, MR, and Weissman, MM. Social phobia. Comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. (1992) 49:282–8. doi: 10.1001/archpsyc.1992.01820040034004
13. Wong, N, Sarver, DE, and Beidel, DC. Quality of life impairments among adults with social phobia: the impact of subtype. J Anxiety Disord. (2012) 26:50–7. doi: 10.1016/j.janxdis.2011.08.012
14. Pini, S, Maser, JD, Dell'Osso, L, Abelli, M, Muti, M, Gesi, C, et al. Social anxiety disorder comorbidity in patients with bipolar disorder: a clinical replication. J Anxiety Disord. (2006) 20:1148–57. doi: 10.1016/j.janxdis.2006.03.006
15. Dell'Osso, L, Pini, S, Tundo, A, Sarno, N, Musetti, L, and Cassano, GB. Clinical characteristics of mania, mixed mania, and bipolar depression with psychotic features. Compr Psychiatry. (2000) 41:242–7. doi: 10.1053/comp.2000.7432
16. Dagani, J, Sisti, D, Abelli, M, Di Paolo, L, Pini, S, Raimondi, S, et al. Do we need oxytocin to treat schizophrenia? A randomized clinical trial. Schizophr Res. (2016) 172:158–64. doi: 10.1016/j.schres.2016.02.011
17. Galderisi, S, Maj, M, Kirkpatrick, B, Piccardi, P, Mucci, A, Invernizzi, G, et al. COMT Val(158)met and BDNF C(270)T polymorphisms in schizophrenia: a case-control study. Schizophr Res. (2005) 73:27–30. doi: 10.1016/j.schres.2004.06.017
18. Beesdo, K, Bittner, A, Pine, DS, Stein, MB, Höfler, M, Lieb, R, et al. Incidence of social anxiety disorder and the consistent risk for secondary depression in the first three decades of life. Arch Gen Psychiatry. (2007) 64:903–12. doi: 10.1001/archpsyc.64.8.903
19. Stein, MB, Fuetsch, M, Müller, N, Höfler, M, Lieb, R, and Wittchen, HU. Social anxiety disorder and the risk of depression: a prospective community study of adolescents and young adults. Arch Gen Psychiatry. (2001) 58:251–6. doi: 10.1001/archpsyc.58.3.251
20. Spain, D, Sin, J, Linder, KB, McMahon, J, and Happé, F. Social anxiety in autism spectrum disorder: a systematic review. Res Autism Spectr Disord. (2018) 52:51–68. doi: 10.1016/j.rasd.2018.04.007
21. Dell'Osso, L, Rucci, P, Ducci, F, Ciapparelli, A, Vivarelli, L, Carlini, M, et al. Social anxiety spectrum. Eur Arch Psychiatry Clin Neurosci. (2003) 253:286–91. doi: 10.1007/s00406-003-0442-5
22. Davidson, JR, Hughes, DC, George, LK, and Blazer, DG. The boundary of social phobia. Exploring the threshold. Arch Gen Psychiatry. (1994) 51:975–83. doi: 10.1001/archpsyc.1994.03950120047008
23. Furmark, T. Social phobia. From epidemiology to brain function (Doctoral dissertation, Acta Universitatis Upsaliensis) Acta Universitatis Upsaliensis (2000).
24. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Publishing (2013).
25. Frank, E, Cassano, GB, Shear, M, Rotondo, A, Dell'Osso, L, Mauri, M, et al. The Spectrum model: a more coherent approach to the complexity of psychiatric symptomatology. CNS Spectr. (1998) 3:23–34. doi: 10.1017/S1092852900005836
26. Cassano, GB, Michelini, S, Shear, MK, Coli, E, Maser, JD, and Frank, E. The panic-agoraphobic spectrum: a descriptive approach to the assessment and treatment of subtle symptoms. Am J Psychiatry. (1997) 154:27–38. doi: 10.1176/ajp.154.6.27
27. Cassano, GB, Dell'Osso, L, Frank, E, Miniati, M, Fagiolini, A, Shear, K, et al. The bipolar spectrum: a clinical reality in search of diagnostic criteria and an assessment methodology. J Affect Disord. (1999) 54:319–28. doi: 10.1016/s0165-0327(98)00158-x
28. Dell'Osso, L, Amatori, G, Nardi, B, Bonelli, C, Gravina, D, Benedetti, F, et al. Validation of the short version of the panic agoraphobic Spectrum (PAS-SV) questionnaire. Clin Neuropsychiatry. (2023) 20:151–6. doi: 10.36131/cnfioritieditore20230207
29. Dell'Osso, L, Luche, RD, Gesi, C, Moroni, I, Carmassi, C, and Maj, M. From Asperger's Autistischen Psychopathen to DSM-5 autism Spectrum disorder and beyond: a subthreshold autism Spectrum model. Clin Pract Epidemiol Ment Health. (2016) 12:120–31. doi: 10.2174/1745017901612010120
30. Dell'Osso, L, Amatori, G, Cappelli, A, Cremone, IM, Massimetti, G, Gravina, D, et al. Catatonia Spectrum: validation of a questionnaire investigating catatonia Spectrum. Front Psych. (2022) 13:913286. doi: 10.3389/fpsyt.2022.913286
31. Dell'Osso, L, Gesi, C, Massimetti, E, Cremone, IM, Barbuti, M, Maccariello, G, et al. Adult autism subthreshold Spectrum (AdAS Spectrum): validation of a questionnaire investigating subthreshold autism spectrum. Compr Psychiatry. (2017) 73:61–83. doi: 10.1016/j.comppsych.2016.11.001
32. Dell’Osso, L, Abelli, M, Pini, S, Carlini, M, Carpita, B, Macchi, E, et al. Dimensional assessment of DSM-5 social anxiety symptoms among university students and its relationship with functional impairment. Neuropsychiatr Dis Treat. (2014) 10:1325–32. doi: 10.2147/NDT.S59348
33. Dell'Osso, L, Rucci, P, Cassano, GB, Maser, JD, Endicott, J, Shear, MK, et al. Measuring social anxiety and obsessive-compulsive spectra: comparison of interviews and self-report instruments. Compr Psychiatry. (2002) 43:81–7. doi: 10.1053/comp.2002.30795
34. Dell'Osso, L, Cassano, GB, Sarno, N, Millanfranchi, A, Pfanner, C, Gemignani, A, et al. Validity and reliability of the structured clinical interview for obsessive-compulsive Spectrum (SCI-OBS) and the structured clinical interview for Social-phobia (SCI-SHY). Int J Methods Psychiatr Res. (2000) 9:11–24.
35. Dell'Osso, L, Saettoni, M, Papasogli, A, Rucci, P, Ciapparelli, A, Di Poggio, AB, et al. Social anxiety spectrum: gender differences in Italian high school students. J Nerv Ment Dis. (2002) 190:225–32. doi: 10.1097/00005053-200204000-00003
36. Carpita, B, Muti, D, Petrucci, A, Romeo, F, Gesi, C, Marazziti, D, et al. Overlapping features between social anxiety and obsessive-compulsive spectrum in a clinical sample and in healthy controls: toward an integrative model. CNS Spectr. (2020) 25:527–34. doi: 10.1017/S109285291900138X
37. Dell'Osso, L, Cremone, IM, Nardi, B, Amatori, G, Bonelli, C, Gravina, D, et al. Measuring the neglected anxiety disorder: validation of the social anxiety spectrum-short version (SHY-SV) questionnaire. BMC Psychiatry. (2023) 23:708. doi: 10.1186/s12888-023-05137-5
38. Brugha, TS, McManus, S, Bankart, J, Scott, F, Purdon, S, Smith, J, et al. Epidemiology of autism spectrum disorders in adults in the community in England. Arch Gen Psychiatry. (2011) 68:459–65. doi: 10.1001/archgenpsychiatry.2011.38
39. Dell'Osso, L, Dalle Luche, R, and Maj, M. Adult autism spectrum as a transnosographic dimension. CNS Spectr. (2016) 21:131–3. doi: 10.1017/S1092852915000450
40. Dell'Osso, L, Carmassi, C, Cremone, IM, Muti, D, Salerni, A, Barberi, FM, et al. Defining the optimal threshold scores for adult autism subthreshold Spectrum (AdAS Spectrum) in clinical and general population. Clin Pract Epidemiol Ment Health. (2020) 16:204–11. doi: 10.2174/1745017902016010204
41. Donati, MA, Berrocal, C, Primi, C, Petracchi, G, Carpita, B, Cosci, F, et al. Measuring subthreshold autistic traits in the general population: psychometric properties of the adult autism subthreshold Spectrum (AdAS Spectrum) scale. Psychiatry Res. (2019) 281:112576. doi: 10.1016/j.psychres.2019.112576
42. Rosen, NE, Lord, C, and Volkmar, FR. The diagnosis of autism: from Kanner to DSM-III to DSM-5 and beyond. J Autism Dev Disord. (2021) 51:4253–70. doi: 10.1007/s10803-021-04904-1
43. Carpita, B, Carmassi, C, Calderoni, S, Muti, D, Muscarella, A, Massimetti, G, et al. The broad autism phenotype in real-life: clinical and functional correlates of autism spectrum symptoms and rumination among parents of patients with autism spectrum disorder. CNS Spectr. (2020) 25:765–73. doi: 10.1017/S1092852919001615
44. Carpita, B, Muti, D, Cremone, IM, Fagiolini, A, and Dell’Osso, L. Eating disorders and autism spectrum: links and risks. CNS Spectr. (2022) 27:272–80. doi: 10.1017/S1092852920002011
45. Billeci, L, Calderoni, S, Conti, E, Gesi, C, Carmassi, C, Dell'Osso, L, et al. The broad autism (Endo)phenotype: Neurostructural and Neurofunctional correlates in parents of individuals with autism Spectrum disorders. Front Neurosci. (2016) 10:346. doi: 10.3389/fnins.2016.00346
46. Dell'Osso, L, Abelli, M, Carpita, B, Pini, S, Castellini, G, Carmassi, C, et al. Historical evolution of the concept of anorexia nervosa and relationships with orthorexia nervosa, autism, and obsessive-compulsive spectrum. Neuropsychiatr Dis Treat. (2016) 12:1651–60. doi: 10.2147/NDT.S108912
47. Dell'Osso, L, Cremone, IM, Chiarantini, I, Arone, A, Massimetti, G, Carmassi, C, et al. Autistic traits and camouflaging behaviors: a cross-sectional investigation in a university student population. CNS Spectr. (2022) 27:740–6. doi: 10.1017/S1092852921000808
48. Carpita, B, Cremone, IM, Amatori, G, Cappelli, A, Salerni, A, Massimetti, G, et al. Investigating the relationship between orthorexia nervosa and autistic traits in a university population. CNS Spectr. (2022) 27:613–20. doi: 10.1017/S1092852921000420
49. Dell'Osso, L, Nardi, B, Benedetti, F, Cremone, IM, Casagrande, D, Massimetti, G, et al. Orthorexia and autism spectrum in university workers: relationship with gender, body mass index and dietary habits. Eat Weight Disord. (2022) 27:3713–23. doi: 10.1007/s40519-022-01514-3
50. Dell'Osso, L, Carpita, B, Bertelloni, CA, Diadema, E, Barberi, FM, Gesi, C, et al. Subthreshold autism spectrum in bipolar disorder: prevalence and clinical correlates. Psychiatry Res. (2019) 281:112605. doi: 10.1016/j.psychres.2019.112605
51. Dell'Osso, L, Cremone, IM, Carpita, B, Fagiolini, A, Massimetti, G, Bossini, L, et al. Correlates of autistic traits among patients with borderline personality disorder. Compr Psychiatry. (2018) 83:7–11. doi: 10.1016/j.comppsych.2018.01.002
52. Baron-Cohen, S, Wheelwright, S, Skinner, R, Martin, J, and Clubley, E. The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord. (2001) 31:5–17. doi: 10.1023/a:1005653411471
53. Dell'Osso, L, Amatori, G, Massimetti, G, Nardi, B, Gravina, D, Benedetti, F, et al. Investigating the relationship between autistic traits and symptoms and catatonia Spectrum. Eur Psychiatry. (2022) 65:e81. doi: 10.1192/j.eurpsy.2022.2334
54. Dell'Osso, L, Buselli, R, Corsi, M, Baldanzi, S, Bertelloni, CA, Marino, R, et al. Do autistic traits correlate with post-traumatic stress and mood Spectrum symptoms among workers complaining of occupational stress? Int J Environ Res Public Health. (2022) 19:3809. doi: 10.3390/ijerph19073809
55. Dell'Osso, L, Cremone, IM, Amatori, G, Cappelli, A, Cuomo, A, Barlati, S, et al. Investigating the relationship between autistic traits, ruminative thinking, and suicidality in a clinical sample of subjects with bipolar disorder and borderline personality disorder. Brain Sci. (2021) 11:621. doi: 10.3390/brainsci11050621
56. Dell'Osso, L, Bertelloni, CA, Di Paolo, M, Avella, MT, Carpita, B, Gori, F, et al. Problematic internet use in university students attending three superior graduate schools in Italy: is autism Spectrum related to suicide risk? Int J Environ Res Public Health. (2019) 16:1098. doi: 10.3390/ijerph16071098
57. Dell'Osso, L, Nardi, B, Bonelli, C, Gravina, D, Benedetti, F, Amatori, G, et al. Investigating suicidality across the autistic-catatonic continuum in a clinical sample of subjects with major depressive disorder and borderline personality disorder. Front Psych. (2023) 14:1124241. doi: 10.3389/fpsyt.2023.1124241
58. Dell'Osso, L, Lorenzi, P, and Carpita, B. Autistic traits and illness trajectories. Clin Pract Epidemiol Ment Health. (2019) 15:94–8. doi: 10.2174/1745017901915010094
59. Farrugia, S, and Hudson, J. Anxiety in adolescents with Asperger syndrome: negative thoughts, behavioral problems, and life interference. Focus Autism Other Dev Disabil. (2006) 21:25–35. doi: 10.1177/10883576060210010401
60. Kuusikko-Gauffin, S, Pollock-Wurman, R, Mattila, ML, Jussila, K, Ebeling, H, Pauls, D, et al. Social anxiety in parents of high-functioning children with autism and Asperger syndrome. J Autism Dev Disord. (2013) 43:521–9. doi: 10.1007/s10803-012-1581-1
61. White, SW, Ollendick, T, and Bray, BC. College students on the autism spectrum: prevalence and associated problems. Autism. (2011) 15:683–701. doi: 10.1177/1362361310393363
62. Muris, P, and Ollendick, TH. Selective mutism and its relations to social anxiety disorder and autism spectrum disorder. Clin Child Fam Psychol Rev. (2021) 24:294–325. doi: 10.1007/s10567-020-00342-0
63. Noris, B, Barker, M, Nadel, J, Hentsch, F, Ansermet, F, and Billard, A. Measuring gaze of children with autism spectrum disorders in naturalistic interactions. Annu Int Conf IEEE Eng Med Biol Soc. (2011) 2011:5356–9. doi: 10.1109/IEMBS.2011.6091325
64. Bögels, SM, and Mansell, W. Attention processes in the maintenance and treatment of social phobia: hypervigilance, avoidance and self-focused attention. Clin Psychol Rev. (2004) 24:827–56. doi: 10.1016/j.cpr.2004.06.005
65. Chawarska, K, Macari, S, and Shic, F. Decreased spontaneous attention to social scenes in 6-month-old infants later diagnosed with autism spectrum disorders. Biol Psychiatry. (2013) 74:195–203. doi: 10.1016/j.biopsych.2012.11.022
66. Shic, F, Macari, S, and Chawarska, K. Speech disturbs face scanning in 6-month-old infants who develop autism spectrum disorder. Biol Psychiatry. (2014) 75:231–7. doi: 10.1016/j.biopsych.2013.07.009
67. Cath, DC, Ran, N, Smit, JH, Van Balkom, AJ, and Comijs, HC. Symptom overlap between autism spectrum disorder, generalized social anxiety disorder and obsessive-compulsive disorder in adults: a preliminary case-controlled study. Psychopathology. (2007) 41:101–10. doi: 10.1159/000111555
68. White, SW, Oswald, D, Ollendick, T, and Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin Psychol Rev. (2009) 29:216–29. doi: 10.1016/j.cpr.2009.01.003
69. Simonoff, E, Pickles, A, Charman, T, Chandler, T, and Baird, G. Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am Acad Child Adolesc Psychiatry. (2008) 47:921–9. doi: 10.1097/CHI.0b013e318179964f
70. Puleo, CM, and Kendall, PC. Anxiety disorders in typically developing youth: autism spectrum symptoms as a predictor of cognitive-behavioral treatment. J Autism Dev Disord. (2011) 41:275–86. doi: 10.1007/s10803-010-1047-2
71. White, PD, Rickards, H, and Zeman, AZ. Time to end the distinction between mental and neurological illnesses. BMJ. (2012) 344:e3454. doi: 10.1136/bmj.e3454
72. Carpita, B, Marazziti, D, Palego, L, Giannaccini, G, Betti, L, and Dell'Osso, L. Microbiota, immune system and autism spectrum disorders: an integrative model towards novel treatment options. Curr Med Chem. (2020) 27:5119–36. doi: 10.2174/0929867326666190328151539
73. Dell’Osso, L, Lorenzi, P, and Carpita, B. The neurodevelopmental continuum towards a neurodevelopmental gradient hypothesis. J Psychopathol. (2019) 25:179–82.
74. Constantino, JN, and Todd, RD. Autistic traits in the general population: a twin study. Arch Gen Psychiatry. (2003) 60:524–30. doi: 10.1001/archpsyc.60.5.524
75. Robinson, EB, Koenen, KC, McCormick, MC, Munir, K, Hallett, V, Happé, F, et al. Evidence that autistic traits show the same etiology in the general population and at the quantitative extremes (5, 2.5, and 1%). Arch Gen Psychiatry. (2011) 68:1113–21. doi: 10.1001/archgenpsychiatry.2011.119
76. Fehm, L, Beesdo, K, Jacobi, F, and Fiedler, A. Social anxiety disorder above and below the diagnostic threshold: prevalence, comorbidity and impairment in the general population. Soc Psychiatry Psychiatr Epidemiol. (2008) 43:257–65. doi: 10.1007/s00127-007-0299-4
77. Schneier, F, and Socha, J. Is there a spectrum of social anxiety disorder? In: H Simpson, Y Neria, R Lewis-Fernándex, and F Schneier, editors. Anxiety disorders-theory, research, and clinical perspectives. Cambridge: Cambridge University Press (2010)
78. Kleberg, JL, Högström, J, Nord, M, Bölte, S, Serlachius, E, and Falck-Ytter, T. Autistic traits and symptoms of social anxiety are differentially related to attention to others' eyes in social anxiety disorder. J Autism Dev Disord. (2017) 47:3814–21. doi: 10.1007/s10803-016-2978-z
79. Rose-, KL. The nature of social competence: a theoretical review. Soc Dev. (1997) 6:111–35. doi: 10.1111/j.1467-9507.1997.tb00097.x
80. Stark, C, Groves, NB, and Kofler, MJ. Is reduced social competence a mechanism linking elevated autism spectrum symptoms with increased risk for social anxiety? Br J Clin Psychol. (2023) 62:129–45. doi: 10.1111/bjc.12398
81. First, MB, Williams, JBW, Karg, RS, and Spitzer, RL. Structured clinical interview for DSM-5— Research version (SCID-5 for DSM-5, research version; SCID-5-RV). VA, American Psychiatric Association: Arlington (2015).
83. Dickter, CL, Burk, JA, Fleckenstein, K, and Kozikowski, CT. Autistic traits and social anxiety predict differential performance on social cognitive tasks in typically developing young adults. PLoS One. (2018) 13:e0195239. doi: 10.1371/journal.pone.0195239
84. White, SW, Bray, BC, and Ollendick, TH. Examining shared and unique aspects of Social anxiety disorder and autism Spectrum disorder using factor analysis. J Autism Dev Disord. (2012) 42:874–84. doi: 10.1007/s10803-011-1325-7
85. White, SW, Kreiser, NL, Pugliese, C, and Scarpa, A. Social anxiety mediates the effect of autism spectrum disorder characteristics on hostility in young adults. Autism. (2012) 16:453–64. doi: 10.1177/1362361311431951
86. Pickard, H, Hirsch, C, Simonoff, E, and Happé, F. Exploring the cognitive, emotional and sensory correlates of social anxiety in autistic and neurotypical adolescents. J Child Psychol Psychiatry. (2020) 61:1317–27. doi: 10.1111/jcpp.13214
87. van Roekel, E, Scholte, RH, and Didden, R. Bullying among adolescents with autism spectrum disorders: prevalence and perception. J Autism Dev Disord. (2010) 40:63–73. doi: 10.1007/s10803-009-0832-2
88. Motoca, LM, Williams, S, and Silverman, WK. Social skills as a mediator between anxiety symptoms and peer interactions among children and adolescents. J Clin Child Adolesc Psychol. (2012) 41:329–36. doi: 10.1080/15374416.2012.668843
89. Bellini, S. The development of social anxiety in adolescents with autism spectrum disorders. Focus Autism Other Dev Disabil. (2006) 21:138–45. doi: 10.1177/10883576060210030201
90. Rapee, RM, and Spence, SH. The etiology of social phobia: empirical evidence and an initial model. Clin Psychol Rev. (2004) 24:737–67. doi: 10.1016/j.cpr.2004.06.004
91. Alvi, T, Kouros, CD, Lee, J, Fulford, D, and Tabak, BA. Social anxiety is negatively associated with theory of mind and empathic accuracy. J Abnorm Psychol. (2020) 129:108–13. doi: 10.1037/abn0000493
92. Buhlmann, U, Wacker, R, and Dziobek, I. Inferring other people’s states of mind: comparison across social anxiety, body dysmorphic, and obsessive-compulsive disorders. J Anxiety Disord. (2015) 34:107–13. doi: 10.1016/j.janxdis.2015.06.003
93. Hezel, DM, and McNally, RJ. Theory of mind impairments in social anxiety disorder. Behav Ther. (2014) 45:530–40. doi: 10.1016/j.beth.2014.02.010
94. Lyvers, M, Scott, K, and Thorberg, FA. Social anxiety and alexithymia in relation to problematic drinking and theory of mind. Am J Psychol. (2019) 132:325–42. doi: 10.5406/amerjpsyc.132.3.0325
95. Maleki, G, Zabihzadeh, A, Richman, MJ, Demetrovics, Z, and Mohammadnejad, F. Decoding and reasoning mental states in major depression and social anxiety disorder. BMC Psychiatry. (2020) 20:463. doi: 10.1186/s12888-020-02873-w
96. Washburn, D, Wilson, G, Roes, M, Rnic, K, and Harkness, KL. Theory of mind in social anxiety disorder, depression, and comorbid conditions. J Anxiety Disord. (2016) 37:71–7. doi: 10.1016/j.janxdis.2015.11.004
97. Dell’Osso, L, and Carpita, B. What misdiagnoses do women with autism spectrum disorder receive in the DSM-5? CNS Spectr. (2023) 28:269–70. doi: 10.1017/S1092852922000037
98. Pellecchia, M, Connell, JE, Kerns, CM, Xie, M, Marcus, SC, and Mandell, DS. Child characteristics associated with outcome for children with autism in a school-based behavioral intervention. Autism. (2016) 20:321–9. doi: 10.1177/1362361315577518
99. Maddox, BB, Miyazaki, Y, and White, SW. Long-term effects of CBT on social impairment in adolescents with ASD. J Autism Dev Disord. (2017) 47:3872–82. doi: 10.1007/s10803-016-2779-4
100. Denham, SA, and Brown, C. “Plays nice with others”: social–emotional learning and academic success. Early Educ Dev. (2010) 21:652–80. doi: 10.1080/10409289.2010.497450
101. Williams White, S, Keonig, K, and Scahill, L. Social skills development in children with autism spectrum disorders: a review of the intervention research. J Autism Dev Disord. (2007) 37:1858–68. doi: 10.1007/s10803-006-0320-x
102. Cassano, GB, Baldini Rossi, N, and Pini, S. Psychopharmacology of anxiety disorders. Dialogues Clin Neurosci. (2002) 4:271–85. doi: 10.31887/DCNS.2002.4.3/gcassano
103. Gates, JA, Kang, E, and Lerner, MD. Efficacy of group social skills interventions for youth with autism spectrum disorder: a systematic review and meta-analysis. Clin Psychol Rev. (2017) 52:164–81. doi: 10.1016/j.cpr.2017.01.006
104. Amore, M, Murri, MB, Calcagno, P, Rocca, P, Rossi, A, Aguglia, E, et al. Italian network for research on psychoses; members of the Italian network for research on psychoses involved in this study. The association between insight and depressive symptoms in schizophrenia: undirected and Bayesian network analyses. Eur Psychiatry. (2020) 63:1–21. doi: 10.1192/j.eurpsy.2020.45
Keywords: social anxiety disorder, social anxiety spectrum, autism spectrum disorder, subthreshold autism spectrum, autistic traits
Citation: Carpita B, Nardi B, Bonelli C, Massimetti E, Amatori G, Cremone IM, Pini S and Dell’Osso L (2024) Presence and correlates of autistic traits among patients with social anxiety disorder. Front. Psychiatry. 14:1320558. doi: 10.3389/fpsyt.2023.1320558
Edited by:
Rita Barone, University of Catania, ItalyReviewed by:
Stefano Marini, Independent Researcher, Termoli, ItalyFrancisco Alcantud-Marín, University of Valencia, Spain
Copyright © 2024 Carpita, Nardi, Bonelli, Massimetti, Amatori, Cremone, Pini and Dell’Osso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Carpita, YmFyYmFyYS5jYXJwaXRhQHVuaXBpLml0