 Danai Valladares-Garrido1,2Pedro P. Quiroga-Castañeda3Iván Berrios-Villegas3
Danai Valladares-Garrido1,2Pedro P. Quiroga-Castañeda3Iván Berrios-Villegas3 J. Pierre Zila-Velasque4,5Claudia Anchay-Zuloeta3,6Marisella Chumán-Sánchez3,6Víctor J. Vera-Ponce7,8
J. Pierre Zila-Velasque4,5Claudia Anchay-Zuloeta3,6Marisella Chumán-Sánchez3,6Víctor J. Vera-Ponce7,8 César J. Pereira-Victorio9*
César J. Pereira-Victorio9* Virgilio E. Failoc-Rojas10
Virgilio E. Failoc-Rojas10 Cristian Díaz-Vélez11,12
Cristian Díaz-Vélez11,12 Mario J. Valladares-Garrido3,13,14
Mario J. Valladares-Garrido3,13,14- 1Escuela de Medicina, Universidad Cesar Vallejo, Trujillo, Peru
- 2Oficina de Salud Ocupacional, Hospital de Apoyo II Santa Rosa, Piura, Peru
- 3Facultad de Medicina, Universidad de San Martín de Porres, Chiclayo, Peru
- 4Universidad Nacional Daniel Alcides Carrión, Facultad de Medicina Humana, Pasco, Peru
- 5Red Latinoamericana de Medicina en La Altitud e Investigación (REDLAMAI), Pasco, Peru
- 6Sociedad Científica de Estudiantes de Medicina Veritas (SCIEMVE), Chiclayo, Peru
- 7Instituto de Investigación en Ciencias Biomédicas, Universidad Ricardo Palma, Lima, Peru
- 8Universidad Tecnológica del Perú, Lima, Peru
- 9School of Medicine, Universidad Continental, Lima, Peru
- 10Unidad de Investigación para Generación y Síntesis de Evidencia en Salud, Universidad San Ignacio de Loyola, Lima, Peru
- 11Escuela de Medicina, Universidad Privada Antenor Orrego, Trujillo, Peru
- 12Red Peruana de Salud Colectiva, Lima, Peru
- 13South American Center for Education and Research in Public Health, Universidad Norbert Wiener, Lima, Peru
- 14Oficina de Epidemiología, Hospital Regional Lambayeque, Chiclayo, Peru
Objective: To determine the prevalence and factors associated with depressive, anxious, and stress symptoms in medical students in Peru, during the second pandemic wave of COVID-19.
Methods: We conducted an analytical cross-sectional study in 405 medical students from a university in northern Peru. The DASS-21 instrument was used to evaluate mental health outcomes (depression, anxiety, and stress), and to investigate their association with socio-educational characteristics.
Results: We found a prevalence of depressive, anxious, and stress symptoms of 71.6% (95% CI: 66.94–75.95), 71.9% (95% CI: 67.2–76.2), and 62.7% (95% CI: 57.8–67.4); respectively. Students with eating behavior disorders had a higher prevalence of depressive symptoms (PR: 1.35), anxious symptoms (PR: 1.27), and stress symptoms (PR: 1.31). The prevalence of depressive symptoms (PR: 1.57), anxious symptoms (PR: 1.27), and stress symptoms (PR: 1.24) increased in students who did not report regular physical activity. In addition, having almost always academic exhaustion increased the prevalence of depressive symptoms (PR: 1.46), stress symptoms (PR: 1.72). On the contrary, the prevalence of depressive symptoms (PR: 0.79), anxious symptoms (PR: 0.73) and stress symptoms (PR: 0.82) decreased in male students. Students who reported sleeping 8 or more hours daily had a lower prevalence of stress symptoms (PR: 0.82).
Conclusion: Symptoms of depression and anxiety occurred in 7 out of 10 students, and stress in 6 out of 10. Among the factors associated with the presence of anxiety, depression, and stress were eating behavior disorder and not regularly exercising. Periodic evaluations of mental symptomatology are required and counseling should be promoted in medical schools.
Introduction
The pandemic caused by COVID-19 has had physical and mental repercussions in all regions of the world and every professions since students, health personnel, general population and military personnel (1–4). In Latin America and the Caribbean, a prevalence of 35 and 32% of depressive and anxious symptoms was reported (5); and in Peru, 30 and 40% of young people between 19 and 26 years of age showed symptoms of depression and anxiety in the context of COVID-19, respectively (6). In relation to medical students, in an Asian country it was found that 31.9% of students showed symptoms of depression, 32.9% of anxiety and 14.6% of stress (7). In Latin America, a prevalence of 49.8% of severe anxiety, 30.4% moderate depression and 17.8% severe stress was identified (8) and in Peru, prevalence of anxiety (28.5%), depression (24.3%) and stress (13.0%) was found during the first wave of the pandemic (9). And among the factors that increased these psychological disorders were the female gender; family, social and economic changes, high educational level and fear of going through a new pandemic, having comorbidities, low social support and low physical activity (2, 10–13).
However, there is not enough conclusive evidence about the persistence of mental health symptoms due to the pandemic and the factors associated with their presentation in medical students after the first year of the COVID-19 pandemic, characterized mainly by periods of confinement and restrictions globally. Additionally, studies that have described our research question present some methodological limitations, such as the small sample size (14), measurement bias since there are little explored variables and that are potentially associated with mental health outcomes (eating behavior disorder, insomnia, having burnout syndrome, physical activity) (15–19), they have a descriptive epidemiological design (20–24) and have not been carried out under rigorous biostatistical methods (20, 25, 26). Also, the Peruvian population it is different to other countries because the Peru it was one of the most affected by the pandemic with high numbers of deaths, more than 200,000, with more of two millions of contagions (27), being the country most affected in Latin America, fact that gave the students more time in their houses by a period almost 3 years, situations that increases the mental health problems (28).
While there is extensive documented evidence about the impact of COVID-19 on the mental health of medical students (29–32), little or nothing has been explored about the persistence of the impact of the pandemic when they have already returned to face-to-face classes at their universities worldwide (33–36) even more so in Latin American countries like Peru, severely hit by the pandemic. Medical students have constantly been exposed to stressful and anxious factors, particularly due to exposure to SARS-CoV-2 during clinical rotations upon returning to their face-to-face classes. Therefore, this research is favorable to reinforce the implementation of long-term preventive and mental support interventions in future doctors. The evaluation of mental health during this transition period from virtual education to face-to-face education through this research helps to solidly understand the challenges and changes caused by the pandemic in medical education.
Therefore, the main objective of this study was to identify the factors associated with depression, anxiety, and stress in a medical school in northern Peru.
Materials and methods
Study design
An analytical cross-sectional study was conducted during the 2021-II academic semester among medical students at the San Martin de Porres University (USMP), Chiclayo, Peru, in the context of the second pandemic wave of COVID-19.
Population and sample
The study population consisted of 1,325 medical students who were studying between the first and seventh academic year of the 2021-II academic semester of the Human Medicine career at the USMP. Students who were enrolled in the 2021-II academic semester and who answered the questions of the dependent variables of the research (depression, anxiety, and stress) were included. Students who did not voluntarily agree to participate in the research were excluded. The sampling was non-probabilistic for convenience. A representative sample of medical students was estimated, using the Epi Info 7.0 program. An estimated proportion of 37.3% (26), a precision of 5%, a confidence level of 95, and 20% for incomplete surveys were used, with a formula for known population (N = 1,325). This gave us a sample size of 340 participants. However, we were able to capture a larger number of participants (n = 405).
Instrument
Depression Anxiety and Stress Scales (DASS-21): an instrument that has 21 items, with four response options in Likert format (It has not happened to me = 0, It has happened a little = 1, It has happened quite a bit = 2 and It has happened a lot = 3). It contains questions about depressive, anxious, and stress symptoms presented in the last 2 weeks. It is considered a brief scale, easy to administer and answer, with its interpretation being straightforward. The total score ranges from 0 to 63 points (37). The DASS-21 questionnaire comprises three distinct dimensions that assess different aspects of mental health. Each subscale is assessed through a point sum ranging from 0 to 21. These dimensions are Depression, including items 3, 5, 10, 13, 16, 17, and 21; Anxiety, encompassing items 2, 4, 7, 9, 15, 19, and 20; and stress, covering items 1, 6, 8, 11, 12, 14, and 18. The cutoff points used were as follows: normal (0–4 points), mild (5–6 points), moderate (7–10 points), severe (11–13 points), and extremely severe (14 points or more). Subsequently, responses were dichotomized into: absence of symptoms (<5 points) and presence of symptoms (5 points or more). Regarding the reliability analyses, for the Depression scale, a sensitivity of 88.5% and specificity of 86.7% were identified. For the Anxiety scale, with a sensitivity of 87.5% and specificity of 83.4% and for the Stress scale, a sensitivity of 81.5% and specificity of 71.4% (38). With internal consistency for the depression scale (0.85), anxiety (0.72), and stress (0.79) (39), validated in the Latin American population.
SCOFF Questionnaire: an instrument that has been designed to identify symptoms related to eating disorders (such as anorexia nervosa and bulimia nervosa) in the last 3 months. It presents five questions in total, each of which is answered with a “yes” or “no” (40). Each affirmative answer is worth one point, while negative answers are worth zero points. Therefore, the answers are valued on a five-point Likert scale, with a total score ranging from 0 to 5. A score of 2 or more indicates an eating behavior disorder. It presents adequate a sensitivity of 81.9% and specificity of 93.5% (41, 42).
General data
This section was made up of socio-educational questions: academic year, age, sex, weight and height report, to then estimate body mass index, frequent alcohol and tobacco consumption report, academic burnout report to the question “do your career’s academic activities have you emotionally exhausted?,” regular physical activity report to the question “do you exercise regularly?,” sleep quality measured with the question “how many hours do you sleep?,” with response option of less than 8 h daily and 8 h or more, and report of currently living at parents’ house, own house or apartment rental.
Variables
The dependent variables were depression, anxiety, and stress, which were operationally defined, according to the explanation made about the use of the DASS-21 scale.
The independent variables were age in years, sex (female, male), year of studies (first to seventh), report of frequent alcohol consumption (no, yes), report of frequent tobacco consumption (no, yes), report of regular physical activity (no, yes), body mass index (normal, overweight, obesity), hours of sleep (<8 h daily, ≥8 h daily) and eating behavior disorder (no, yes).
Study procedure
After obtaining the necessary authorizations at the university and the approval of the ethics committee, we created a survey in the REDCap data entry system. This questionnaire was shared through the official social network groups (Facebook, WhatsApp) of all the years of study of the participating university. The survey was self-administered and students took an average of 12 min to complete the required information. Subsequently, the data obtained were exported to a spreadsheet in Microsoft Excel for quality control and analysis.
Statistical analysis
The statistical analysis was performed in the Stata v.17.0 program.
In the descriptive analysis, absolute and relative frequencies of categorical variables were shown. In numerical variables (age), the best measure of central tendency and dispersion was reported, after evaluating the assumption of normal distribution.
In the bivariate analysis, the factors associated with the dependent variables, that is, the mental health outcomes (depression, anxiety, and stress) were investigated. For the categorical independent variables, the chi-square test was useful, after evaluating the assumption of expected frequencies. In the numerical variable age, the Mann–Whitney U test was considered suitable, after evaluating the assumption of normal distribution. A significance level of 5% was used.
In the simple regression analysis, the factors associated with mental health outcomes (depression, anxiety, and stress) were identified through the construction of generalized linear models, Poisson family, log link function, and robust variance. The variables that were associated in the simple regression were included in the multiple regression model using a parsimonic model with forward selection (p < 0.05) to estimate prevalence ratios (PR) and 95% confidence intervals (IC95%). Collinearity between the variables of interest was evaluated.
Ethical aspects
The confidentiality of the participating medical students was maintained, since the questionnaires were anonymous. Their desire to participate in the research was consulted through the filling out of informed consent, before accessing the questionnaires of interest. The research was approved by the Ethics Committee of the San Martin de Porres University.
Results
General characteristics of medical students
Of 405 medical students, we found that the majority were women (66.7%), were in their third year of study (22.5%), slept less than 8 h daily (78.0%), always or almost always feel emotionally drained from their academic activities (42.4%) and did not regularly perform physical activity (51.0%). 7.9 and 4.0% reported frequent consumption of alcohol and tobacco, respectively. The prevalence of depressive, anxious, and stress symptoms was 71.6% (95% CI: 66.94–75.95), 71.9% (95% CI: 67.2–76.2), and 62.7% (95% CI: 57.8–67.4; Table 1).

Table 1. Características de participantes (n = 405).
Factors associated with mental health symptoms (depression, anxiety, and stress), in bivariate analysis
In the bivariate analysis, we found that female students had a higher frequency of depressive symptoms (62.6% vs. 39.3%; p < 0.001), anxious symptoms (73.7% vs. 47.4%), and stress symptoms (50.4% vs. 37.8%; p = 0.017); compared to male. Students who reported having emotional exhaustion almost always/always had a higher frequency of depressive symptoms (69.8% vs. 44.2%; p < 0.001), anxious symptoms (77.5% vs. 55.8%; p < 0.001), and stress symptoms (63.9% vs. 33.3%); compared to those who never/almost never had such exhaustion. Students who reported not exercising regularly had a higher frequency of depressive symptoms (67.2% vs. 42.3%; p < 0.001), anxious symptoms (77.5% vs. 52.0%; p < 0.001), and stress symptoms (54.9% vs. 37.2%; p < 0.001); compared to those who reported exercising regularly. Additionally, students with eating behavior disorders had a higher frequency of depressive symptoms (70.5% vs. 44.4%; p < 0.001), anxious symptoms (78.5% vs. 55.6%; p < 0.001), and stress symptoms (56.4% vs. 39.4%; p = 0.001; Table 2).
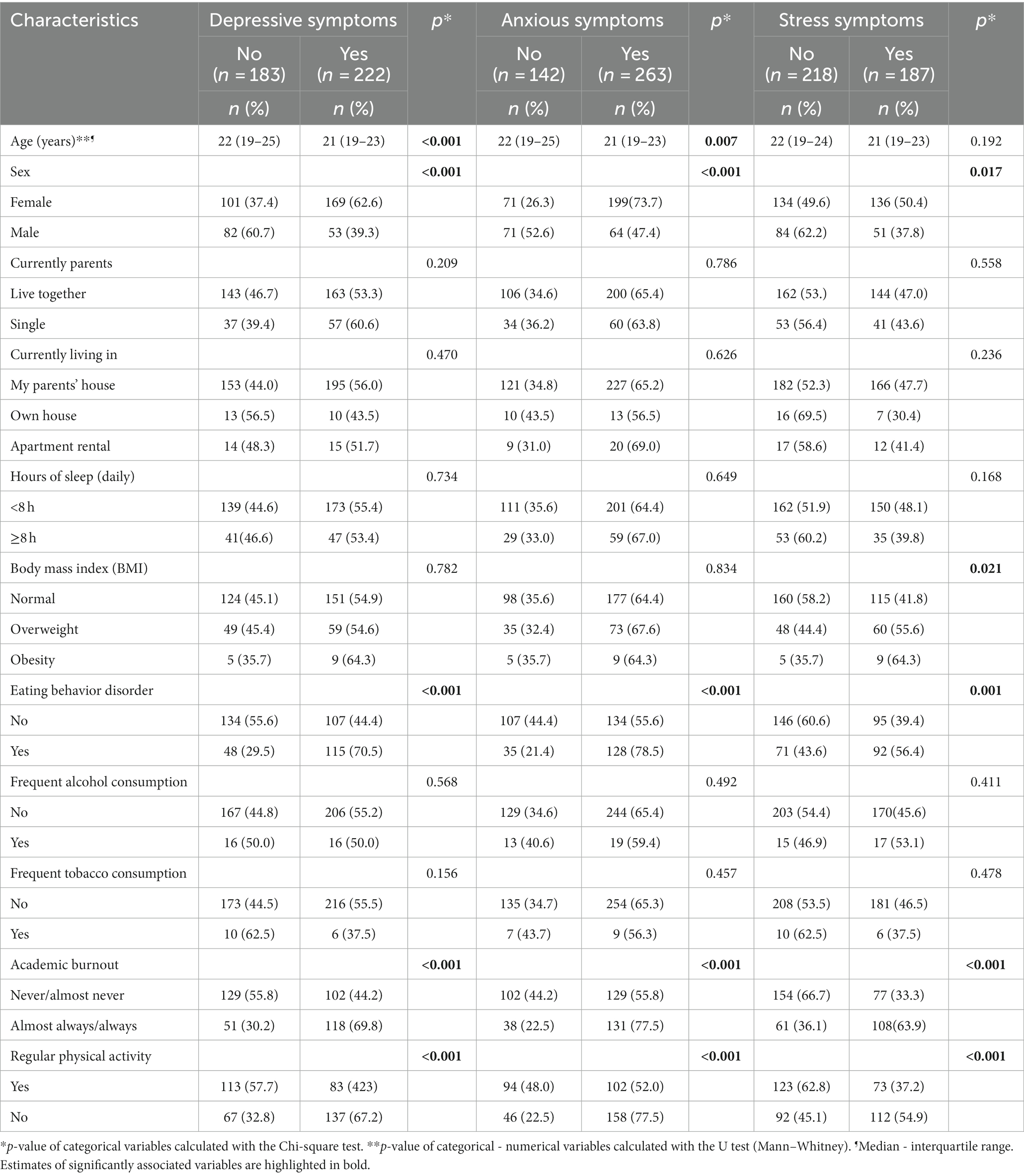
Table 2. Characteristics associated with mental health symptoms (depression, anxiety, and stress), in bivariate analysis.
Associated factors with mental health symptoms (depression, anxiety, and stress), in simple and multiple regression analysis
We found that the factors associated with a higher prevalence of depressive symptoms were reporting infrequent physical activity (PR: 1.37; 95% CI: 1.23–1.52) and presenting an eating disorder (PR: 1.35; 95% CI: 1.21–1.50). On the contrary, male students presented a 21% lower prevalence of depressive symptoms (PR: 0.79; 95% CI: 0.63–0.99).
Regarding anxious symptoms, we found that these increase in students who reported physical inactivity (PR: 1.27; 95% CI: 1.20–1.45) and presenting an eating disorder (PR: 1.27; 95% CI: 1.16–1.39). On the other hand, the prevalence of anxious symptoms reduced by 27% in male students (PR: 0.73; 95% CI: 0.55–0.98).
Finally, the factors positively associated with stress symptoms were having academic burnout always and almost always (PR: 1.72; 95% CI: 1.14–2.59), reporting physical inactivity (PR: 1.24; 95% CI: 1.07–1.44), and having an eating disorder (PR: 1.31; 95% CI: 1.14–1.49). On the contrary, students who reported sleeping 8 or more hours daily had a 16% lower prevalence of stress symptoms (PR: 0.84; 95% CI: 0.74–0.97), likewise, the prevalence of stress symptoms reduced by 18% in male students (PR: 0.82; 95% CI: 0.74–0.90; Table 3).
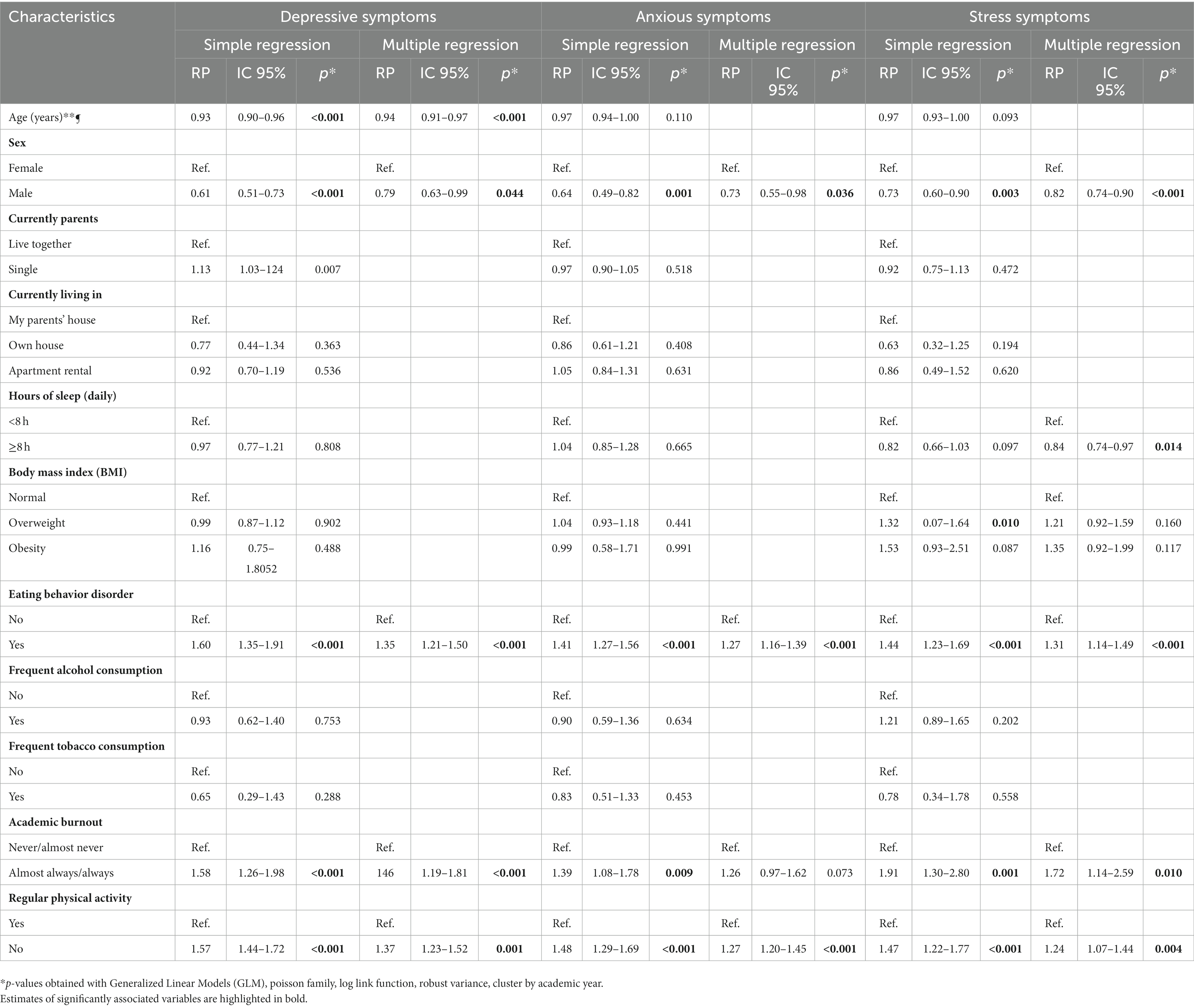
Table 3. Factors associated with mental health symptoms (depression, anxiety, and stress), in simple and multiple regression analysis.
Discussion
Prevalence of mental health symptoms
We found that 7 out of 10 students showed symptoms of depression (71.7%), where 27.3, 12.3, and 15.3% presented moderate, severe, and extreme-severe depression, respectively. This is lower than reported in an American study conducted in university students during the COVID-19 pandemic, in which the prevalence of depression was 80.6% (26). However, it is higher than studies conducted in Chinese and Ethiopian university students during the pandemic context, where the prevalence was 23.3% (43) and 46.3% (29), respectively. Also, before the COVID-19 pandemic, prevalences of 29.7% (44) and 27.2% (45) were found in regions of Nepal among medical students.
This high frequency of depressive symptoms could be explained by a substantial burden of depressive symptoms in this student population, and its explanation is multifaceted, involving both factors related to the COVID-19 pandemic and factors inherent to the nature of medical education. Firstly, it is important to consider the context of the COVID-19 pandemic. Adapting to mandatory social distancing measures imposed to contain the virus’s spread has profoundly disrupted people’s lives worldwide. Medical students are no exception to this, and the restriction on social interaction, isolation from friends and loved ones, and the decrease in normal social activities may have significantly contributed to the increased depressive symptoms. Furthermore, the uncertainty and fear associated with the pandemic, as well as constant exposure to information about the health crisis, may have had a negative psychological impact on students. Another relevant aspect is the abrupt transition to virtual education, which has become the norm during the pandemic. Medical students faced unique challenges, as much of their learning relies on clinical experience and in-person interactions with patients and classmates. The shift to a virtual environment may have resulted in a sense of disconnection, loss of practical learning opportunities, and an increase in the feeling of isolation. In addition to pandemic-related factors, medical education itself can be stressful and demanding. Medical students often face an intense workload, tight schedules, high academic expectations, and constant pressure to excel. This academic and professional pressure can contribute to the onset and exacerbation of depressive symptoms. Lastly, while the COVID-19 pandemic has played a role in the increased depressive symptoms among medical students, it is essential to recognize that several additional factors are at play. The combination of academic pressure, emotional demands, financial difficulties, and other challenges inherent to medical education can contribute to the high prevalence of depression in this student population (46, 47).
We found that 7 out of 10 students showed anxious symptoms; where 16.2 and 26.5% suffered from moderate and extreme-severe anxiety, respectively. This is similar to what was reported during the first months of the pandemic in the United States by Lee et al. where 16.1% of medical students presented symptoms of moderate anxiety (48). It also coincides with a study conducted in Peru, where 28.5% of medical students had moderate levels of anxiety in the context of the first pandemic wave (9). However, it differs from the medical student population in China, of which only 15.8% suffered from anxiety disorder according to the study conducted by Xiao et al. in the context of the first wave (49).
Several factors may contribute to this elevated prevalence of anxious symptoms. Firstly, it is important to acknowledge the impact of the COVID-19 pandemic, which disrupted the traditional medical education system (48). The absence of face-to-face clinical practices and the abrupt shift to virtual learning likely had negative effects on the mental health of students (48). Clinical exposure and hands-on experience are integral components of medical education, allowing students to develop practical skills, interact with patients, and gain confidence in their abilities (48). The sudden interruption of these crucial learning experiences may have generated anxiety and uncertainty among students, especially given the essential nature of clinical training in medical education. Moreover, the extended duration of remote learning in Peru, with a return to face-to-face classes after 2 years, as indicated by the Ministry of Education (MINEDU) (50), adds another layer of complexity to the situation (48). Prolonged periods of virtual education can intensify feelings of isolation, hinder peer interactions, and contribute to a sense of detachment from the medical community. The anticipation of transitioning back to in-person classes may have also caused anxiety, as students may worry about readjusting to clinical settings and the potential challenges associated with this transition. Additionally, it is crucial to consider individual differences in coping mechanisms and resilience. Not all students respond to stressors and changes in the same way, and some may be more susceptible to anxiety symptoms than others. The competitive and demanding nature of medical education, coupled with the stressors brought about by the pandemic, may have pushed some students to the threshold of anxiety.
We found that 6 out of 10 students showed symptoms of stress (62.8%), where 21.9 and 19% presented moderate and severe stress, respectively. Similar to what was reported in university students (66.1%) from Ecuador during the first wave of the pandemic (51). This is consistent with what was described in Brazil, where 57.5% of university students presented stress during the COVID-19 pandemic (12). Also, in Chile during the pandemic, a prevalence of stress of 52.9% has been evidenced in university students (52).
This high frequency of stress symptoms can be attributed to a constellation of interconnected elements, both intrinsic and extrinsic to medical education. First and foremost, the demanding nature of medical training itself plays a significant role. Medical students are exposed to an intensive workload characterized by rigorous coursework, complex subject matter, and the expectation of exceptional academic performance. Additionally, they contend with tight schedules, the need to juggle multiple responsibilities, and the pressure to excel in a highly competitive environment. The pursuit of medical knowledge and the acquisition of clinical skills often demand long hours of study and practice, which can lead to exhaustion and heightened stress levels. The disruption caused by the COVID-19 pandemic further exacerbated the stress experienced by medical students. The abrupt transition to virtual education posed challenges such as reduced social interaction, limited hands-on learning opportunities, and the potential for technical issues during online classes. This shift in the educational paradigm forced students to adapt quickly, and the uncertainty surrounding the pandemic’s trajectory and impact contributed to heightened stress and anxiety. Furthermore, the fear of contracting COVID-19 added an extra layer of stress for medical students. As individuals aspiring to work in healthcare settings, they were acutely aware of the risks associated with the virus and may have experienced anxiety about their own health and safety, as well as the health of their loved ones. Financial concerns stemming from the pandemic also weighed heavily on students. Many faced economic hardships due to family job losses or reduced income, which could have increased their financial stress. The combination of academic pressures, virtual learning challenges, health-related anxieties, and financial burdens likely synergistically contributed to the observed high prevalence of stress symptoms (19, 26).
Factors associated with depression symptoms
Male students had a lower prevalence of depression. This is consistent with what was described in a study conducted in Peru during the first wave of the pandemic, which revealed that being a woman was associated with depressive symptoms (OR = 1.34) (53). However, it contrasts with what was reported by a study conducted in medical students in China where no association was evidenced between depression and gender (54). This association could be explained because women, due to certain factors to which they are exposed, such as domestic violence and sexual abuse, are often more prone to develop mental health disorders (55, 56). This added to the fact that the female population often takes on more responsibilities at an early age and it has been shown that they present cognitive disorders and hyperactivity more frequently (55, 57). Unlike males, who, having behaviors of impulsivity and irritability, often camouflage depressive symptoms (58).
University students who reported not exercising had a 37% higher prevalence of depression. Our result is similar to reported in a study conducted in the university population, exercising is usually associated with less prevalence of depression (59), a result supported by different systematic reviews (60, 61). This association could be explained because having mental health symptomatology generates an imbalance in the monoaminergic systems, so its management focuses on correcting this imbalance, before this physical activity has shown that it increases the levels of noradrenaline, the levels of “free tryptophan fatty acids” which conditions the increase of serotonin (involved in depression) and finally decreases the stress response of the hypothalamus-pituitary–adrenal axis (involved because its hyperactivity with the consequent secretion of cortisol has been seen altered in depression) (62).
Having an eating disorder increased the prevalence of depression by 35%. This result is supported by what was found in the general population of Australia, which identified that having an EAD increased the risk of having a moderate and extreme level of depression in the pandemic context by 50% (63). Also, in Bolivian students it was evidenced that having an EAD increased the risk of depression by 66%, it should be noted that the study was conducted in a pre-pandemic context (64). Different from what was described by another study (65) that concludes a bidirectionality between the variables because depression predisposes the development of some eating disorder. This association could be explained because both pathologies share common biological mechanisms such as alterations in the mesocorticolimbic circuits, generating a decrease in the sensation of hunger; the dysfunction of the brain-microbiome relationship, through early fullness and the development of nausea and vomiting; and an endocrine-entero deregulation leading to starvation (66). Situations that lead to a multidisciplinary approach due to the different facets involved in the association.
Factors associated with anxiety symptoms
Being male reduced the prevalence of anxious symptoms in medical students by 27%. This is consistent with what was described by Sheshtawy et al. in Egyptian medical students during the COVID-19 pandemic, who evidenced that belonging to the male sex presents a lower risk of developing symptoms of anxiety (67). However, it contrasts with what was reported by Yuan et al. in Chinese medical students (OR: 0.783) (30) in the context of the pandemic and by Simegn et al. in Ethiopian medical students (29). This association could be explained because each gender in particular has notable differences within their types of personalities. In the case of males, they tend to be more objective and usually seek immediate solutions to problems, this could make them less prone to suffer anxiety (68). Also, it has been reported that women tend to suffer from appetite disorders, hypochondria, and anxiety more frequently in contrast to males (56).
Having an eating disorder increased the prevalence of anxiety by 27%. This is consistent with what was described in a study conducted by Attouche et al. in Moroccan medical students during pre-pandemic, where having an eating disorder was associated with an increase in anxiety. Also, it has been identified that having an EAD increased the risk of anxiety by 54%, it should be noted that the study was conducted in a pre-pandemic context (64). However, a bidirectional relationship has been identified between the variables due to shared reward circuits (69). This association is explained by the influence of anxiety on the domains of eating behavior, such as cognitive restriction, referred to decision-making according to each food to consume due to its calorie-based composition, where anxiety in these people is elevated; also, it has been seen that anxiety predominates in the other domain such as Disinhibition because it generates impulsive consumption of food as in binges; and finally in hunger due to its neurobiological connections (70).
Factors associated with stress symptoms
Being male reduced the prevalence of stress symptoms in medical students by 18%. This is consistent with what was described by Awadalla et al. in Saudi Arabian medical students during the COVID-19 pandemic, who evidenced that belonging to the female sex presents a higher risk of developing symptoms of stress (71). However, it contrasts with what was reported by Atta et al. in Egyptian medical students, who reported that prevalence of stress was higher in male (>85.0%) (72). This can be explained by the fact that male students are more self-confident and have more resilience strategies than female students, in addition to having more social support, which leads to developing less stress (73).
Reporting burnout syndrome increased the prevalence of stress. This is consistent with what was described by Yusoff et al. in second-year medical students during pre-pandemic context (74), also, it has been evidenced that burnout syndrome presented a variance for the development of stress in 19% (75). However, it contrasts with what was reported by a study that evidenced a negative correlation between personal fulfillment (3rd dimension of burnout syndrome) and the level of stress, concluding that the higher the stress, the lower the burnout syndrome (76). This association could be explained because medical students represent a special group because they often face many academic demands throughout their medical training (77), which in the context of the pandemic the high level of stress was evidenced in 1 out of every 10 students (11), in addition to dealing with the constant pressure to be successful in their career, the long hours of study, and the reduced amount of time for their social activities (78).
Not exercising was associated with a higher prevalence of stress symptoms. This is consistent with what was described by Leuchter et al. in American medical students in a pre-pandemic context, who reveals that the greater the intensity of exercise performed, the lower the levels of stress (79). Similarly, in Mexican medical students, a positive association was found between physical activity and a lower level of stress in a pre-pandemic context (80). We did not find studies that contradict this association. This association could be explained because there are potential mechanisms through which exercise could act on the body’s stress response, especially through the hypothalamus-pituitary–adrenal axis or the circulation of glucocorticoids (81, 82). In addition, physical exercise helps in the stimulation of processes relevant for the proper functioning of the brain, among them the stimulation of neurogenesis and angiogenesis, and the positive regulation of growth factors such as brain-derived neurotrophic factor (83). Therefore, thanks to the promotion of the functioning of those brain regions that play an important role in stress-related conditions, exercise could be a protective factor for developing stress symptoms.
Students who reported sleeping 8 h or more had a lower prevalence of stress. This is consistent with what was described in a study conducted in medical students in Saudi Arabia in a non-pandemic context, who found that the greater the amount of rest, the lower the prevalence of stress (84). Also, in American medical students in the context of the pandemic, an association was identified between the number of hours slept (7 h) and the lower level of stress (85). However, we found a study that evidenced bidirectionality between the variables (quality of sleep and stress) explaining that dealing with the COVID-19 infection, uncertainty about the pandemic, social confinement, and decreased physical activity make up a multifactorial origin that each of the variables share (86), variables that affect structures involved in the mechanisms of sleep regulation such as the hypothalamus-pituitary–adrenal axis and the immune system (87).
Having an eating disorder, evaluated with the SCOFF questionnaire, increased the prevalence of stress symptoms by 31%. This is consistent with what was described in a study conducted by Iyer S et al. (88, 89) in Indian medical students in a pre-pandemic context, who found that the eating disorder increased stress. Also, in the context of the pandemic in French students, a positive association was found between the variables of eating disorder and stress in French medical students (90). However, it contrasts with what was reported by a study in medical students conducted in Malaysia in a pre-pandemic context that did not evidence an association between the variables of eating disorder and stress (91), it should be noted that a different evaluation instrument was used (EAT-26). In our country, a prevalence of EAD has been evidenced in 2 out of every 10 medical students in the context of the COVID-19 pandemic (3). Eating disorders have a multifactorial origin, so this association could be explained because most medical students usually face the career during their youth years, where in addition to (92) being exposed to the academic load and the probable lack of time management (93), they must also face their transition to adult life and sociocultural factors such as social pressure to have a certain physical appearance (94–96). All of this makes them more prone to suffer from eating disorders.
Correlates between anxiety, depression and stress
The strongest correlates found in our population were that more than half of the population between 1 and 7 medical students presented at least one of the negative mental health symptoms. There was a direct correlation between being female, not exercising, presenting an eating disorder, presenting burnout syndrome with the development of these negative symptoms, as opposed to presenting an optimal sleep quality with a rest of more than 8 h, demonstrating a negative association with these negative symptoms. Although the pandemic as an unforeseen event developed the ideal context to develop these negative factors, discarding the biological sex and unlike the students who did not present these symptoms. It is well known that the natural relationship between these pathologies (anxiety, depression and stress) represent “normal” symptoms that are acquired in the course of medical school (97). We are convinced that reversing these negative factors and strengthening protective factors in students is not only aimed at preventing the development of these negative mental health symptoms associated with implementing a healthy lifestyle and an adequate social life that become distant upon entering medical school, but also to prevent the development of these negative mental health symptoms associated with implementing a healthy lifestyle and an adequate social life that become distant upon entering medical school (98).
Relevance of findings in public health
This study provides information on mental health in a phase of the COVID-19 pandemic little evidenced (third wave of pandemic). The role of mental health assessment in a particular population like medical students is vital to be able to observe their evolution and the measures of associated factors. This study provides information that helps to understand the evolution of mental health symptoms in a country that was very affected by the pandemic, compared to other countries in the region. We evidenced variables that have been little evaluated [being male, not doing any exercise, and rest time (8 h)], variables that have not shown association in other studies in the context of the pandemic and results that to our understanding would be the first reported in our region (Latin America). We highlight that despite the decrease in the number of infections, negative mental health symptoms still persist. Therefore, we believe that periodic evaluations of these symptoms, the implementation and execution of mental health programs, and continuous accompaniment in those who present these negative symptoms, would correspond to the public health measures to be introduced in every institution to avoid their increase and complications of their non-management.
Limitations and strengths
In relation to the limitations of the study, first, the cross-sectional design of the study did not allow us to identify causal relationships between the study variables, but as a strength, in our study we used validated instruments on anxiety (99), depression (100) and stress (101). Also, another limitation found in the study we formulated structured questions for the evaluation of sleep quality, physical activity, substance use, and burnout syndrome. As a second limitation, we identified selection biases stemming from the lack of representativeness because we focused on a single university. Additionally, the use of snowball sampling limits the generalizability of the results and could potentially introduce biases such as misclassification bias and response bias, as students with better internet connectivity or higher motivation to participate might be overrepresented or underrepresented in the findings. However, it’s important to emphasize that these limitations do not invalidate the research results. But as a strength, we covered a broad sample of students from various academic years and from a region where research is flourishing and has been significantly impacted by the COVID-19 pandemic. Furthermore, we were able to engage a student population that faced accessibility challenges due to the virtual classes prompted by the COVID-19 pandemic (102). This proved beneficial for capturing diverse and partially representative information while maintaining flexibility and adaptability in data collection for the research. As a third limitation is the potential measurement bias because the questionnaires were self-administered and being an instrument that does not represent the Gold Standard of diagnosis of these mental health symptoms (103), in addition to not covering variables the post-traumatic stress disorder (PTSD) that gives us information about the chronicity of the symptoms, but as a strength we covered various variables that evidence important information in the context of the pandemic (EAD, amount of rest hours, physical activity, and gender). This research has measured variables that have been widely in the first year of the pandemic, however, it generates evidence in this new period of normality (3rd wave of the pandemic).
Conclusion
We identified that symptoms of depression and anxiety were present in 7 out of 10 students, and stress in 6 out of 10. Among the factors associated with the presence of anxiety, depression, and stress were the eating disorder and not regularly exercising. Given this, we recommend periodic evaluations of these symptoms and the corresponding counseling in each institution.
Data availability statement
The dataset generated and analyzed during the current study is not publicly available because the ethics committee has not provided permission/authorization to publicly share the data, but it is available from the corresponding author upon reasonable request.
Ethics statement
The studies involving humans were approved by San Martin de Porres University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DV-G: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. PQ-C: Investigation, Methodology, Validation, Visualization, Writing – original draft. IB-V: Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. JZ-V: Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. CA-Z: Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. MC-S: Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. VV-P: Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. CP-V: Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VF-R: Funding acquisition, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CD-V: Investigation, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. MJV-G was supported by the Fogarty International Center of the National Institutes of Mental Health (NIMH) under Award Number D43TW009343 and the University of California Global Health Institute (UCGHI).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. León-Jiménez, F, Vives-Kufoy, C, Failoc-Rojas, VE, and Valladares-Garrido, MJ. Mortalidad en pacientes hospitalizados por COVID-19. Estudio prospectivo en el norte del Perú, 2020. Rev Med Chile. (2021) 149:1459–66. doi: 10.4067/s0034-98872021001001459
2. Zila-Velasque, JP, Grados-Espinoza, P, Coba-Villan, N, Quispe-Chamorro, J, Taipe-Guillén, YF, Pacheco, E, et al. Mental disorders and level of resilience in eight high-altitude cities of Peru during the second pandemic wave: a multicenter population-based study. Int J Environ Res Public Health. (2022) 20:519. doi: 10.3390/ijerph20010519
3. Pierre Zila-Velasque, J, Grados-Espinoza, P, Regalado-Rodríguez, KM, Luna-Córdova, CJ, Calderón, GSS, Diaz-Vargas, M, et al. Prevalence and factors associated with eating disorders in Peruvian human medicine students in the context of the COVID-19 pandemic: a multicentre study. Rev Colomb Psiquiatr. (2022) 1:10 doi: 10.1016/j.rcp.2022.07.005
4. Valladares-Garrido, MJ, Picón-Reátegui, CK, Zila-Velasque, JP, Grados-Espinoza, P, Hinostroza-Zarate, CM, Failoc-Rojas, VE, et al. Suicide risk in military personnel during the COVID-19 health emergency in a Peruvian region: a cross-sectional study. Int J Environ Res Public Health. (2022) 19:13502. doi: 10.3390/ijerph192013502
5. La, OPS. Lanza Nueva Campaña Para Frenar el Estigma Hacia las Personas con Problemas de Salud Mental - OPS/OMS | Organización Panamericana de la Salud; (2023). Available at: https://www.paho.org/es/noticias/7-10-2022-ops-lanza-nueva-campana-para-frenar-estigma-hacia-personas-con-problemas-salud (Accessed September 06, 2023).
6. Instituto Nacional de Salud Entre 40 y 30% de Jóvenes de 19 y 26 años en el Perú Presentaron Síntomas de Ansiedad y Depresión tras la Llegada de la Pandemia de la COVID-19; (2023). Available at: https://web.ins.gob.pe/es/prensa/noticia/entre-40-y-30-de-jovenes-de-19-y-26-anos-en-el-peru-presentaron-sintomas-de-ansiedad. (Accessed September 06, 2023).
7. Chang, WW, Shi, LX, Zhang, L, Jin, YL, and Yu, JG. The mental health status and associated factors among medical students engaged in online learning at home during the pandemic: a cross-sectional study from China. Front Psych. (2021) 12:755503. doi: 10.3389/fpsyt.2021.755503
8. Aveiro-Róbalo, TR, Garlisi-Torales, LD, Chumán-Sánchez, M, Pereira-Victorio, CJ, Huaman-Garcia, M, Failoc-Rojas, VE, et al. Prevalence and associated factors of depression, anxiety, and stress in university students in Paraguay during the COVID-19 pandemic. Int J Environ Res Public Health. (2022) 19:12930. doi: 10.3390/ijerph191912930
9. Sandoval, KD, Morote-Jayacc, PV, Moreno-Molina, M, and Taype-Rondan, A. Depresión, estrés y ansiedad en estudiantes de Medicina humana de Ayacucho (Perú) en el contexto de la pandemia por COVID-19. Rev Colomb Psiquiatr. (2021) 9:8 doi: 10.1016/j.rcp.2021.10.005
10. Wang, X, Zhang, N, Pu, C, Li, Y, Chen, H, and Li, M. Anxiety, depression, and PTSD among college students in the post-COVID-19 era: a cross-sectional study. Brain Sci. (2022) 12:1553. doi: 10.3390/brainsci12111553
11. Grados-Espinoza, P, Zila-Velasque, JP, Soriano-Moreno, DR, Regalado-Rodríguez, KM, Sosa-Nuñez, F, Barzola-Farfán, W, et al. A cross-sectional study to assess the level of satisfaction with virtual education in Peruvian medical students. Front Public Health. (2022):10:1004902. doi: 10.3389/fpubh.2022.1004902
12. Lopes, AR, and Nihei, OK. Depression, anxiety and stress symptoms in Brazilian university students during the COVID-19 pandemic: predictors and association with life satisfaction, psychological well-being and coping strategies. PLoS One. (2021) 16:e0258493. doi: 10.1371/journal.pone.0258493
13. Peng, P, Hao, Y, Liu, Y, Chen, S, Wang, Y, Yang, Q, et al. The prevalence and risk factors of mental problems in medical students during COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. (2023) 321:167–81. doi: 10.1016/j.jad.2022.10.040
14. Saraswathi, I, Saikarthik, J, Senthil Kumar, K, Madhan Srinivasan, K, Ardhanaari, M, and Gunapriya, R. Impact of COVID-19 outbreak on the mental health status of undergraduate medical students in a COVID-19 treating medical college: a prospective longitudinal study. PeerJ. (2020) 8:e10164. doi: 10.7717/peerj.10164
15. Liu, H, Liu, X, and Xu, W. Prevalence and influencing factors of anxiety in medical students during the COVID-19 pandemic. Heliyon. (2022) 8:e10487. doi: 10.1016/j.heliyon.2022.e10487
16. Nakhostin-Ansari, A, Sherafati, A, Aghajani, F, Khonji, MS, Aghajani, R, and Shahmansouri, N. Depression and anxiety among Iranian medical students during COVID-19 pandemic. Iran J Psychiatry. (2020) 15:228–35. doi: 10.18502/ijps.v15i3.3815
17. Campos, R, Pinto, V, Alves, D, Rosa, CP, and Pereira, H. Impact of COVID-19 on the mental health of medical students in Portugal. J Pers Med. (2021) 11:986. doi: 10.3390/jpm11100986
18. Ferreira, LC, Amorim, RS, Melo Campos, FM, and Cipolotti, R. Mental health and illness of medical students and newly graduated doctors during the pandemic of SARS-Cov-2/COVID-19. PLoS One. (2021) 16:e0251525. doi: 10.1371/journal.pone.0251525
19. Chootong, R, Sono, S, Choomalee, K, Wiwattanaworaset, P, Phusawat, N, Wanghirankul, N, et al. The association between physical activity and prevalence of anxiety and depression in medical students during COVID-19 pandemic: a cross-sectional study. Ann Med Surg. (2012) 2022:103408. doi: 10.1016/j.amsu.2022.103408
20. Lu, L, Wang, X, Wang, X, Guo, X, and Pan, B. Association of Covid-19 pandemic-related stress and depressive symptoms among international medical students. BMC Psychiatry. (2022) 22:20. doi: 10.1186/s12888-021-03671-8
21. Cao, W, Fang, Z, Hou, G, Han, M, Xu, X, Dong, J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. (2020) 287:112934. doi: 10.1016/j.psychres.2020.112934
22. Essangri, H, Sabir, M, Benkabbou, A, Majbar, MA, Amrani, L, Ghannam, A, et al. Predictive factors for impaired mental health among medical students during the early stage of the COVID-19 pandemic in Morocco. Am J Trop Med Hyg. (2021) 104:95–102. doi: 10.4269/ajtmh.20-1302
23. Gupta, P, Anupama, BK, and Ramakrishna, K. Prevalence of depression and anxiety among medical students and house staff during the COVID-19 health-care crisis. Acad Psychiatry. (2021) 45:575–80. doi: 10.1007/s40596-021-01454-7
24. Kuman Tunçel, Ö, Taşbakan, SE, Gökengin, D, Erdem, HA, Yamazhan, T, Sipahi, OR, et al. The deep impact of the COVID-19 pandemic on medical students: an online cross-sectional study evaluating Turkish students’ anxiety. Int J Clin Pract. (2021) 75:e14139. doi: 10.1111/ijcp.14139
25. Pereira, MB, Casagrande, AV, Almeida, BC, Neves, BA, da Silva, TC, Miskulin, FP, et al. Mental health of medical students before and during COVID-19 pandemic: a 3-year prospective study. Med Sci Educ. (2022) 32:873–81. doi: 10.1007/s40670-022-01580-3
26. Wang, X, Hegde, S, Son, C, Keller, B, Smith, A, and Sasangohar, F. Investigating mental health of US College students during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. (2020) 22:e22817. doi: 10.2196/22817
27. Malca, CG, Gideon, J, and Romero, MJ. How Peru became the Country with the Highest COVID Death Rate in the World. The Conversation; (2021). Available at: http://theconversation.com/how-peru-became-the-country-with-the-highest-covid-death-rate-in-the-world-169779 (Accessed September 06, 2023).
28. Ruiz-Frutos, C, Palomino-Baldeón, JC, Ortega-Moreno, M, Villavicencio-Guardia, MD, Dias, A, Bernardes, JM, et al. Effects of the COVID-19 pandemic on mental health in Peru: psychological distress. Healthcare. (2021) 9:691. doi: 10.3390/healthcare9060691
29. Simegn, W, Dagnew, B, Yeshaw, Y, Yitayih, S, Woldegerima, B, and Dagne, H. Depression, anxiety, stress and their associated factors among Ethiopian university students during an early stage of COVID-19 pandemic: an online-based cross-sectional survey. PLoS One. (2021) 16:e0251670. doi: 10.1371/journal.pone.0251670
30. Yuan, LL, Lu, L, Wang, XH, Guo, XX, Ren, H, Gao, YQ, et al. Prevalence and predictors of anxiety and depressive symptoms among international medical students in China during COVID-19 pandemic. Front Psych. (2021) 12:761964. doi: 10.3389/fpsyt.2021.761964
31. Risal, A, Shikhrakar, S, Mishra, S, Kunwar, D, Karki, E, Shrestha, B, et al. Anxiety and depression during COVID-19 pandemic among medical students in Nepal. Kathmandu Univ Med J. (2020) 18:333–9. doi: 10.21203/rs.3.rs-91574/v1
32. Çimen, İD, Alvur, TM, Coşkun, B, and Şükür, NEÖ. Mental health of Turkish medical students during the COVID-19 pandemic. Int J Soc Psychiatry. (2022) 68:1253–62. doi: 10.1177/00207640211066734
33. Liao, X, Zhang, S, Wang, Y, Jiang, J, Li, Y, and Zhang, W. Mental burden among Chinese undergraduate medical students: a prospective longitudinal study before, during, and after the COVID-19 outbreak. Front Psych. (2022) 13:982469. doi: 10.3389/fpsyt.2022.982469
34. Zheng, C, Yi, P, Shen, G, and Chen, W. Effects of school resumption on college students’ mental health during the COVID-19 pandemic. J Psychosoc Nurs Ment Health Serv. (2022) 60:19–27. doi: 10.3928/02793695-20211118-02
35. Duan, H, Gong, M, Zhang, Q, Huang, X, and Wan, B. Research on sleep status, body mass index, anxiety and depression of college students during the post-pandemic era in Wuhan, China. J Affect Disord. (2022) 301:189–92. doi: 10.1016/j.jad.2022.01.015
36. Conteh, I, Yan, J, Dovi, KS, Bajinka, O, Massey, IY, and Turay, B. Prevalence and associated influential factors of mental health problems among Chinese college students during different stages of COVID-19 pandemic: a systematic review. Psychiatry Res Commun. (2022) 2:100082. doi: 10.1016/j.psycom.2022.100082
37. Antúnez, Z, and Vinet, EV. Escalas de Depresión, Ansiedad y Estrés (DASS - 21): Validación de la Versión abreviada en Estudiantes Universitarios Chilenos. Ter Psicológica. (2012) 30:49–55. doi: 10.4067/S0718-48082012000300005
38. Román, F, Santibáñez, P, and Vinet, EV. Uso de las Escalas de Depresión Ansiedad Estrés (DASS-21) como Instrumento de Tamizaje en Jóvenes con Problemas Clínicos1. Acta Investig Psicológica Psychol Res Rec. (2016) 6:2325–36. doi: 10.1016/S2007-4719(16)30053-9
39. Mella, FR, Vinet, EV, and Alarcón Muñoz, AM. Escalas de Depresión, Ansiedad y Estrés (DASS-21): Adaptación y propiedades psicométricas en estudiantes secundarios de temuco. Rev Argent Clín Psicol. (2014) 23:179–90.
40. Campo-Arias, A, Cogollo, Z, and Díaz, CE. Cuestionario SCOFF para tamizaje de trastornos de la conducta alimentaria: Consistencia interna en estudiantes de un colegio de Cartagena, Colombia. Revista de la Facultad de Ciencias de la Salud. (2007) 4:6.
41. Rueda Jaimes, GE, Díaz Martínez, LA, Ortiz Barajas, DP, Pinzón Plata, C, Rodríguez Martínez, J, and Cadena Afanador, LP. Validación del cuestionario SCOFF Para el cribado de los trastornos del comportamiento alimentario en adolescentes escolarizadas. Aten Primaria. (2005) 35:89–94. doi: 10.1157/13071915
42. Solmi, F, Hatch, SL, Hotopf, M, Treasure, J, and Micali, N. Validation of the SCOFF questionnaire for eating disorders in a multiethnic general population sample. Int J Eat Disord. (2015) 48:312–6. doi: 10.1002/eat.22373
43. Chi, X, Becker, B, Yu, Q, Willeit, P, Jiao, C, Huang, L, et al. Prevalence and psychosocial correlates of mental health outcomes among Chinese college students during the coronavirus disease (COVID-19) pandemic. Front Psych. (2020) 11:803. doi: 10.3389/fpsyt.2020.00803
44. Basnet, B, Jaiswal, M, Adhikari, B, and Shyangwa, PM. Depression among undergraduate medical students. Kathmandu Univ Med J. (2012) 10:56–9. doi: 10.3126/kumj.v10i3.8021
45. Shrestha, N, Shrestha, N, Khanal, S, Dahal, S, Lama, R, Simkhada, P, et al. Prevalence of depression among medical students of a tertiary care teaching hospital. JNMA J Nepal Med Assoc. (2019) 57:403–7. doi: 10.31729/jnma.4738
46. Galindo-Vázquez, O, Ramírez-Orozco, M, Costas-Muñiz, R, Mendoza-Contreras, LA, Calderillo-Ruíz, G, and Meneses-García, A. Symptoms of anxiety, depression and self-care behaviors during the COVID-19 pandemic in the general population. Gac Med Mex. (2020) 156:298–305. doi: 10.24875/GMM.20000266
47. García, SA. A propósito del COVID-19: ¿sería recomendable para Chile la mediación familiar en línea? Rev Chil Derecho Tecnol. (2020) 9:93–119. doi: 10.5354/0719-2584.2020.57339
48. Lee, CM, Juarez, M, Rae, G, Jones, L, Rodriguez, RM, Davis, JA, et al. Anxiety, PTSD, and stressors in medical students during the initial peak of the COVID-19 pandemic. PLoS One. (2021) 16:e0255013. doi: 10.1371/journal.pone.0255013
49. Xiao, H, Shu, W, Li, M, Li, Z, Tao, F, Wu, X, et al. Social distancing among medical students during the 2019 coronavirus disease pandemic in China: disease awareness, anxiety disorder, depression, and behavioral activities. Int J Environ Res Public Health. (2020) 17:5047. doi: 10.3390/ijerph17145047
50. El Peruano, T. Universidades Públicas y Privadas Deben Volver a Clases Presenciales el Segundo Semestre; (2023). Available at: https://elperuano.pe/noticia/161795-universidades-publicas-y-privadas-deben-volver-a-clases-presenciales-el-segundo-semestre (Accessed January 19, 2023).
51. Moreno-Montero, EM, Naranjo-Hidalgo, T, Poveda-Ríos, S, and Izurieta-Brito, D. Estrés académico en universitarios durante la pandemia de COVID-19. Rev Médica Electrónica. (2022) 44:468–82.
52. Solari-Montenegro, G, Rivera-Iratchet, M, Álvarez-Andrade, M, Velasco-Mur, A, Yaitul-Barrientos, P, Gómez-Inostroza, P, et al. Prevalencia del estrés académico en estudiantes de Kinesiología durante el período de pandemia de COVID-19, 2021. FEM Rev Fund Educ Médica. (2022) 25:197–203. doi: 10.33588/fem.255.1227
53. Huarcaya-Victoria, J, Elera-Fitzcarrald, C, Crisol-Deza, D, Villanueva-Zúñiga, L, Pacherres, A, Torres, A, et al. Factors associated with mental health in Peruvian medical students during the COVID-19 pandemic: a multicentre quantitative study. Rev Colomb Psiquiatr. (2021) 52:236–244. doi: 10.1016/j.rcp.2021.06.002
54. Liu, J, Zhu, Q, Fan, W, Makamure, J, Zheng, C, and Wang, J. Online mental health survey in a medical College in China during the COVID-19 outbreak. Front Psych. (2020) 11:459. doi: 10.3389/fpsyt.2020.00459
55. Arenas, MC, and Puigcerver, A. Diferencias entre hombres y mujeres en los trastornos de ansiedad: una aproximación psicobiológica. Escr Psicol Internet. (2009) 3:20–9.
56. Gaviria Arbeláez, SL. ¿Por qué las mujeres se deprimen más que los hombres? Rev Colomb Psiquiatr. (2009) 38:316–24.
57. Liu, N, Zhang, F, Wei, C, Jia, Y, Shang, Z, Sun, L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. (2020) 287:112921. doi: 10.1016/j.psychres.2020.112921
58. Dumais, A, Lesage, AD, Alda, M, Rouleau, G, Dumont, M, Chawky, N, et al. Risk factors for suicide completion in major depression: a case-control study of impulsive and aggressive behaviors in men. Am J Psychiatry. (2005) 162:2116–24. doi: 10.1176/appi.ajp.162.11.2116
59. Grasdalsmoen, M, Eriksen, HR, Lønning, KJ, and Sivertsen, B. Physical exercise, mental health problems, and suicide attempts in university students. BMC Psychiatry. (2020) 20:175. doi: 10.1186/s12888-020-02583-3
60. Pearce, M, Garcia, L, Abbas, A, Strain, T, Schuch, FB, Golubic, R, et al. Association between physical activity and risk of depression: a systematic review and Meta-analysis. JAMA Psychiatry. (2022) 79:550–9. doi: 10.1001/jamapsychiatry.2022.0609
61. Wolf, S, Seiffer, B, Zeibig, JM, Welkerling, J, Brokmeier, L, Atrott, B, et al. Is physical activity associated with less depression and anxiety during the COVID-19 pandemic? A rapid systematic review. Sports Med. (2021) 51:1771–83. doi: 10.1007/s40279-021-01468-z
63. Phillipou, A, Meyer, D, Neill, E, Tan, EJ, Toh, WL, Van Rheenen, TE, et al. Eating and exercise behaviors in eating disorders and the general population during the COVID-19 pandemic in Australia: initial results from the COLLATE project. Int J Eat Disord. (2020) 53:1158–65. doi: 10.1002/eat.23317
64. Mérida Pérez, C, and López, HR. Prevalencia de los trastornos de la conducta alimentaria y su relación con la ansiedad y depresión en adolescentes de secundaria de la ciudad de La Paz. Rev Investig Psicol. (2013) 10:69–85.
65. Fragkos, KC, and Frangos, CC. Assessing eating disorder risk: the pivotal role of achievement anxiety, depression and female gender in non-clinical samples. Nutrients. (2013) 5:811–28. doi: 10.3390/nu5030811
66. Skowron, K, Kurnik-Łucka, M, Dadański, E, Bętkowska-Korpała, B, and Gil, K. Backstage of eating disorder—about the biological mechanisms behind the symptoms of anorexia nervosa. Nutrients. (2020) 12:2604. doi: 10.3390/nu12092604
67. Sheshtawy, HA, Hemead, S, Shaheen, A, Shaheen, N, Elrewany, E, and Hemead, HM. Prevalence of depression, anxiety and stress disorders among medical students in Alexandria Faculty of Medicine during COVID-19 pandemic. BJPsych Open. (2021) 7:S2. doi: 10.1192/bjo.2021.68
68. Loving, RD, Aragón, SR, and Matus, PWV. Masculinidad-feminidad y salud mental. Persona. (2012) 15:137–57.
69. Frank, GKW, Shott, ME, Pryor, T, Swindle, S, Nguyen, T, and Stoddard, J. Trait anxiety is associated with amygdala expectation and caloric taste receipt response across eating disorders. Neuropsychopharmacology. (2023) 48:380–90. doi: 10.1038/s41386-022-01440-z
70. Hussenoeder, FS, Conrad, I, Engel, C, Zachariae, S, Zeynalova, S, Glaesmer, H, et al. Analyzing the link between anxiety and eating behavior as a potential pathway to eating-related health outcomes. Sci Rep. (2021) 11:14717. doi: 10.1038/s41598-021-94279-1
71. Awadalla, NJ, Alsabaani, AA, Alsaleem, MA, Alsaleem, SA, Alshaikh, AA, Al-Fifi, SH, et al. Increased mental stress among undergraduate medical students in South-Western Saudi Arabia during the COVID-19 pandemic. PeerJ. (2022) 10:e13900. doi: 10.7717/peerj.13900
72. Atta, IS, and Almilaibary, A. The prevalence of stress among medical students studying an integrative curriculum during the COVID-19 pandemic. Adv Med Educ Pract. (2022) 13:35–45. doi: 10.2147/AMEP.S345330
73. Freire, C, Del, FM, Regueiro, B, Rodríguez, S, Valle, A, and Núñez, JC. Coping strategies and self-efficacy in university students: a person-centered approach. Front Psychol. (2020):11. doi: 10.3389/fpsyg.2020.00841
74. Yusoff, MSB, Hadie, SNH, and Yasin, MAM. The roles of emotional intelligence, neuroticism, and academic stress on the relationship between psychological distress and burnout in medical students. BMC Med Educ. (2021) 21:293. doi: 10.1186/s12909-021-02733-5
75. Spányik, A, Simon, D, Rigó, A, Griffiths, MD, and Demetrovics, Z. Subjective COVID-19-related work factors predict stress, burnout, and depression among healthcare workers during the COVID-19 pandemic but not objective factors. PLoS One. (2022) 17:e0270156. doi: 10.1371/journal.pone.0270156
76. Amro, TM, Arcos González, P, Montero Viñuales, E, and Castro, DR. Impact of COVID-19 pandemic on stress and burnout levels amongst emergency medical technicians: a cross-sectional study in Spain. Ann Med. (2022) 54:3007–16. doi: 10.1080/07853890.2022.2137735
77. Yousuf, T. Relationship between academic stress and personal wellness in medical university students. Liaquat Med Res J. (2021).
78. Bergmann, C, Muth, T, and Loerbroks, A. Medical students’ perceptions of stress due to academic studies and its interrelationships with other domains of life: a qualitative study. Med Educ Online. (2019) 24:1603526. doi: 10.1080/10872981.2019.1603526
79. Leuchter, RK, Stuber, ML, McDonald, AL, and Croymans, DM. Relationship between exercise intensity and stress levels among U.S. medical students. Med Educ Online. (2022) 27:2027651. doi: 10.1080/10872981.2022.2027651
80. Fouilloux, C, Fouilloux-Morales, M, Tafoya, SA, and Petra-Micu, I. Asociación entre actividad física y salud mental positiva en estudiantes de medicina en México: un estudio transversal. Cuad Psicol Deporte. (2021) 21:1–15.
81. Anderson, E, and Shivakumar, G. Effects of exercise and physical activity on anxiety. Front Psych. (2013) 4:27. doi: 10.3389/fpsyt.2013.00027
82. Wegner, M, Helmich, I, Machado, S, Nardi, AE, Arias-Carrion, O, and Budde, H. Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets. (2014) 13:1002–14. doi: 10.2174/1871527313666140612102841
83. Kandola, A, Hendrikse, J, Lucassen, PJ, and Yücel, M. Aerobic exercise as a tool to improve hippocampal plasticity and function in humans: practical implications for mental health treatment. Front Hum Neurosci. (2016) 10:373. doi: 10.3389/fnhum.2016.00373
84. Alsaggaf, MA, Wali, SO, Merdad, RA, and Merdad, LA. Sleep quantity, quality, and insomnia symptoms of medical students during clinical years. Saudi Med J. (2016) 37:173–82. doi: 10.15537/smj.2016.2.14288
85. McKinley, B, Daines, B, Allen, M, Pulsipher, K, Zapata, I, and Wilde, B. Mental health and sleep habits during preclinical years of medical school. Sleep Med. (2022) 100:291–7. doi: 10.1016/j.sleep.2022.09.001
86. Neculicioiu, VS, Colosi, IA, Costache, C, Sevastre-Berghian, A, and Clichici, S. Time to sleep?—a review of the impact of the COVID-19 pandemic on sleep and mental health. Int J Environ Res Public Health. (2022) 19:3497. doi: 10.3390/ijerph19063497
87. Han, KS, Kim, L, and Shim, I. Stress and Sleep Disorder. Exp Neurobiol. (2012) 21:141–50. doi: 10.5607/en.2012.21.4.141
88. Rotenstein, LS, Ramos, MA, Torre, M, Segal, JB, Peluso, MJ, Guille, C, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and Meta-analysis. JAMA. (2016) 316:2214–36. doi: 10.1001/jama.2016.17324
89. Iyer, S, and Shriraam, V. Prevalence of eating disorders and its associated risk factors in students of a medical College Hospital in South India. Cureus. (2021) 13:e12926. doi: 10.7759/cureus.12926
90. Tavolacci, MP, Ladner, J, and Dechelotte, P. COVID-19 pandemic and eating disorders among university students. Nutrients. (2021) 13:4294. doi: 10.3390/nu13124294
91. Ngan, SW, Chern, BCK, Rajarathnam, DD, Balan, J, Hong, TS, and Tiang, KP. The relationship between eating disorders and stress among medical undergraduate: a cross-sectional study. Open J Epidemiol. (2017) 7:85–95. doi: 10.4236/ojepi.2017.72008
92. Attouche, N, Hafdi, S, Somali, R, Battas, O, and Agoub, M. Facteurs associés au risque de troubles du comportement alimentaire chez les étudiants en médecine de Casablanca. Maroc Pan Afr Med J. (2021) 39:270. doi: 10.11604/pamj.2021.39.270.19976
93. Britz, J, and Pappas, E. Sources and outlets of stress among university students: correlations between stress and unhealthy habits. Undergrad Res J Hum Sci. (2010) 9:15
94. Boujut, E, and Bruchon-Schweitzer, M. Les troubles des comportements alimentaires chez des étudiants de première année: une étude prospective multigroupes. Psychol Fr. (2010) 55:295–307. doi: 10.1016/j.psfr.2010.08.001
95. Ansari, WE, Clausen, SV, Mabhala, A, and Stock, C. How do I look? Body image perceptions among university students from England and Denmark. Int J Environ Res Public Health. (2010) 7:583–95. doi: 10.3390/ijerph7020583
96. Eisenberg, D, Nicklett, EJ, Roeder, K, and Kirz, NE. Eating disorder symptoms among college students: prevalence, persistence, correlates, and treatment-seeking. J Am Coll Health. (2011) 59:700–7. doi: 10.1080/07448481.2010.546461
97. Karpinski, RI, Kinase Kolb, AM, Tetreault, NA, and Borowski, TB. High intelligence: a risk factor for psychological and physiological overexcitabilities. Intelligence. (2018) 66:8–23. doi: 10.1016/j.intell.2017.09.001
98. Brenneisen Mayer, F, Souza Santos, I, Silveira, PSP, Itaqui Lopes, MH, de Souza, AR, Campos, EP, et al. Factors associated to depression and anxiety in medical students: a multicenter study. BMC Med Educ. (2016) 16:282. doi: 10.1186/s12909-016-0791-1
99. Franco-Jimenez, RA, Nuñez-Magallanes, A, Franco-Jimenez, RA, and Nuñez-Magallanes, A. Propiedades psicométricas del GAD-7, GAD-2 y GAD-Mini en universitarios peruanos. Propósitos Represent. (2022) 10:9. doi: 10.20511/pyr2022.v10n1.1437
100. Huarcaya-Victoria, J, De-Lama-Morán, R, Quiros, M, Bazán, J, López, K, Lora, D, et al. Propiedades psicométricas del Patient Health Questionnaire (PHQ-9) en estudiantes de medicina en Lima, Perú. Rev Neuro-Psiquiatr. (2020) 83:72–8. doi: 10.20453/rnp.v83i2.3749
101. Guzmán-Yacaman, JE, and Reyes-Bossio, M. Adaptación de la Escala de Percepción Global de Estrés en estudiantes universitarios peruanos. Rev Psicol PUCP. (2018) 36:719–50. doi: 10.18800/psico.201802.012
102. Díaz-Vélez, C, Failoc-Rojas, VE, Valladares-Garrido, MJ, Colchado, J, Carrera-Acosta, L, Becerra, M, et al. SARS-CoV-2 seroprevalence study in Lambayeque, Peru. June-July 2020. PeerJ. (2021) 9:e11210. doi: 10.7717/peerj.11210
103. Asociación Americana de Psiquiatría. Publica el Manual Diagnóstico y Estadístico de Trastornos Mental. (2023). Available at: https://www.psychiatry.org:443/news-room/news-releases/asociacion-americana-de-psiquiatria-publica-el-man (Accessed January 29, 2023).
Keywords: depression, anxiety, stress, COVID-19, medical students, Peru
Citation: Valladares-Garrido D, Quiroga-Castañeda PP, Berrios-Villegas I, Zila-Velasque JP, Anchay-Zuloeta C, Chumán-Sánchez M, Vera-Ponce VJ, Pereira-Victorio CJ, Failoc-Rojas VE, Díaz-Vélez C and Valladares-Garrido MJ (2023) Depression, anxiety, and stress in medical students in Peru: a cross-sectional study. Front. Psychiatry. 14:1268872. doi: 10.3389/fpsyt.2023.1268872
Edited by:
Marco Grados, Johns Hopkins University, United StatesReviewed by:
Pu Peng, Central South University, ChinaMahmood Moosazadeh, Mazandaran University of Medical Sciences, Iran
Copyright © 2023 Valladares-Garrido, Quiroga-Castañeda, Berrios-Villegas, Zila-Velasque, Anchay-Zuloeta, Chumán-Sánchez, Vera-Ponce, Pereira-Victorio, Failoc-Rojas, Díaz-Vélez and Valladares Garrido. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: César J. Pereira-Victorio, Y3BlcmVpcmF2QGNvbnRpbmVudGFsLmVkdS5wZQ==;