 Adam Gędek
Adam Gędek Szymon Modrzejewski
Szymon Modrzejewski Marta Gędek4,5
Marta Gędek4,5 Anna Z. Antosik
Anna Z. Antosik Monika Dominiak
Monika Dominiak
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 14 November 2023
Sec. ADHD
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1258868
Introduction: Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder with an unclear etiology. Systemic inflammation and immune dysregulation may play a role in the pathogenesis of ADHD. Morphology-derived parameters such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and monocyte to lymphocyte ratio (MLR), have been proposed as peripheral biomarkers of the immune-inflammatory process in various diseases. However, studies examining their role in ADHD remain inconclusive.
Methods: A systematic review and a meta-analysis were conducted to evaluate the association between NLR, MLR, PLR and ADHD. Relevant articles were identified, screened, and assessed for quality according to PRISMA guidelines. Moreover, a qualitative and quantitative analyses were performed.
Results: The review contained eight eligible studies, five of which were included in the meta-analysis. The meta-analysis showed that ADHD patients had higher NLR and PLR values compared to health controls. No significant difference in MLR value was observed between the two groups. Analysis in relation to ADHD subtypes showed no significant differences in inflammatory markers in any of the included studies as well. The influence of medical treatment on these ratios could not be adequately assessed due to limited data.
Conclusion: ADHD patients exhibit higher NLR and PLR than healthy controls, which may indicate the potential immune-inflammatory involvement in this disorder. Further studies on inflammatory markers and ADHD, especially those considering the impact of treatment and clinical symptoms, are essential to comprehensively understand this association.
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity (1). The disorder affects individuals across different age groups, carrying significant implications for daily functioning and the overall quality of life for them and their families (2). Despite its prevalence and impact, the exact underlying pathophysiological mechanisms remain undiscovered (3).
In recent years, there has been a growing interest in exploring the role of systemic inflammation and immune dysregulation in the pathogenesis of ADHD (4, 5). Inflammatory and autoimmune diseases, such as eczema, asthma, rheumatoid arthritis, type 1 diabetes, or hypothyroidism, co-occur significantly more frequently with ADHD (6, 7). Studies to date have suggested that patients with ADHD have higher levels of inflammatory cytokines, such as Il-6 or Il-10, than healthy individuals (8, 9). Furthermore, some of the studies have also demonstrated an association of inflammatory markers with disease severity (10). In addition, it has been observed that the patients who take psychostimulants display lower levels of inflammatory markers (11). Moreover, several lines of evidence from genetic studies have indicated links between ADHD and polymorphisms in genes associated with inflammatory pathways (5).
Alterations in various peripheral blood cell ratios, such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and monocyte to lymphocyte ratio (MLR), have been shown to serve as potential biomarkers of immune-inflammatory processes or poor prognoses in various diseases, such as cancers, cerebrovascular, cardiovascular, or autoimmune diseases (12–16). In recent years, the assessment of NLR, MLR, and PLR in patients with mental illnesses has also been investigated. These inflammatory markers were elevated in depressed, bipolar, or non-affective psychosis patients (17–20).
To date, several studies have investigated the link between NLR, PLR, MLR, and ADHD, but the findings have been inconsistent. Some studies have reported elevated ratios among individuals with ADHD, suggesting a potential role of inflammation in the pathophysiology of the disorder (21, 22). However, other studies have found no significant differences in these parameters among ADHD patients, pointing to the complexity of the immune-inflammatory mechanisms involved (23, 24).
Therefore, the aim of this study was to conduct a systematic review and meta-analysis to evaluate the association between immune-inflammatory markers such as NLR, PLR, MLR, and ADHD. Specifically, we planned to: (1) compare NLR, MLR, PLR levels between ADHD patients and healthy controls; (2) assess the effects of psychostimulant treatment on NLR, MLR, PLR in ADHD patients; (3) evaluate the association of NLR, MLR, PLR levels with ADHD subtypes; (4) evaluate the association of NLR, MLR, PLR levels with ADHD symptoms and their severity. To our best knowledge, no systematic review on this topic has been conducted to date.
We hypothesized that NLR, MLR and PLR levels differ significantly between ADHD patients and healthy controls, and that psychostimulant treatment affects these markers in ADHD subjects. We also hypothesized that NLR, MLR and PLR level differ in various subtypes of ADHD and are related to symptoms and severity of the disease. This systematic review and meta-analysis provide a comprehensive insight into the relationship between NLR, MLR, PLR and ADHD.
This systematic review was conducted according to the PRISMA statement (Preferred reporting items for systematic review and meta-analysis) (25).
A literature search in April 2023 included the contents of Pubmed, Scopus, and Web of Science electronic databases without any filters. Additionally, clinicaltrialregistry.gov was searched. The following search strategy was used: (“neutrophil-to-lymphocyte ratio” OR “NLR” OR “neutrophil to lymphocyte ratio” OR “neutrophil/lymphocyte ratio” OR “neutrophil-lymphocyte ratio” OR “neutrophil lymphocyte ratio” OR “platelet-to-lymphocyte ratio” OR “PLR” OR “platelet to lymphocyte ratio” OR “platelet/lymphocyte ratio” OR “platelet-lymphocyte ratio” OR “platelet lymphocyte ratio” OR “monocyte-to-lymphocyte ratio” OR “MLR” OR “monocyte to lymphocyte ratio” OR “monocyte/lymphocyte ratio” OR “monocyte-lymphocyte ratio” OR “monocyte lymphocyte ratio”) AND (“ADHD” OR “Attention Deficit Hyperactivity Disorder”). In addition, references from selected articles were screened to confirm potentially related studies.
The following criteria were a condition for the inclusion of the studies in this systematic review: (1) observational study design (case-control, cohort, or cross-sectional); (2) concerning ADHD patients over 6 years of age and under 18 years of age and controls without mental disorders; (3) at least one of the NLR, MLR, or PLR levels were measured; (4) published in English. The exclusion criteria were as follows: (1) reviews, letters, and conference abstracts; (2) non-human studies; (3) duplicate data; (4) full text was not available; (5) not in English. Two investigators worked independently to complete the preliminary screening through browsing titles and abstracts. The final decisions were made after reviewing the full texts. Disagreements between the researchers were resolved by consultation with the third author.
The original data was extracted from the included studies by two of the researchers. The following information was collected: the surname of the first author, publication year, country, matching information for sex and age, diagnostic criteria, sample size, mean age, percentage of men, information about comorbidities, medical treatment and subtypes of ADHD, peripheral blood cell ratios (NLR, MLR, PLR). Any divergences were resolved through discussion between the two investigators and consultation by a third researcher.
The quality of the selected studies was independently evaluated by two authors with the Newcastle-Ottawa scale (NOS) (26). The study was assessed with respect to three aspects: Selection, Comparability, and Exposure. A maximum of one star was awarded in each category for Selection and Exposure, while a maximum of two stars could be awarded for Comparability. Studies were rated from 0 to 9, with those scoring from 0 to 2 being ranked as poor quality, 3 to 5 as fair quality and 6 to 9 as high quality. Any disagreements were managed by group discussion. Only high and fair quality studies were included in meta-analysis.
The meta-analysis was conducted using RevMan5 (version 5.4; Cochrane Collaboration) software. Continuous outcomes were pooled as standardized mean difference (SMD). Heterogeneity was evaluated visually on the Forest plot and statistically using the Chi2, I2, and Tau2. Thresholds from Cochrane Collaboration were consistent with interpretation of heterogeneity: 0–40% might be not important; 30–60% may represent moderate heterogeneity; 50–90% may represent substantial heterogeneity, and 75–100% high level of heterogeneity. A fixed-effect model was used to analyze and p < 0.05 was set as a statistical significance. The subgroup analysis with regard to the psychostimulant treatment used was planned.
A total of 110 articles were identified through the search strategy. After removing 57 duplicates, 53 remained for titles and abstracts screening. Initially, eleven full-text articles were carefully assessed for eligibility. However, this number was later reduced to eight eligible articles, which were used for data extraction and summarization of the results (21–24, 27–30). Five of the articles were included in quantitative analysis (21–24, 30). The search process flow and results are detailed in Figure 1.
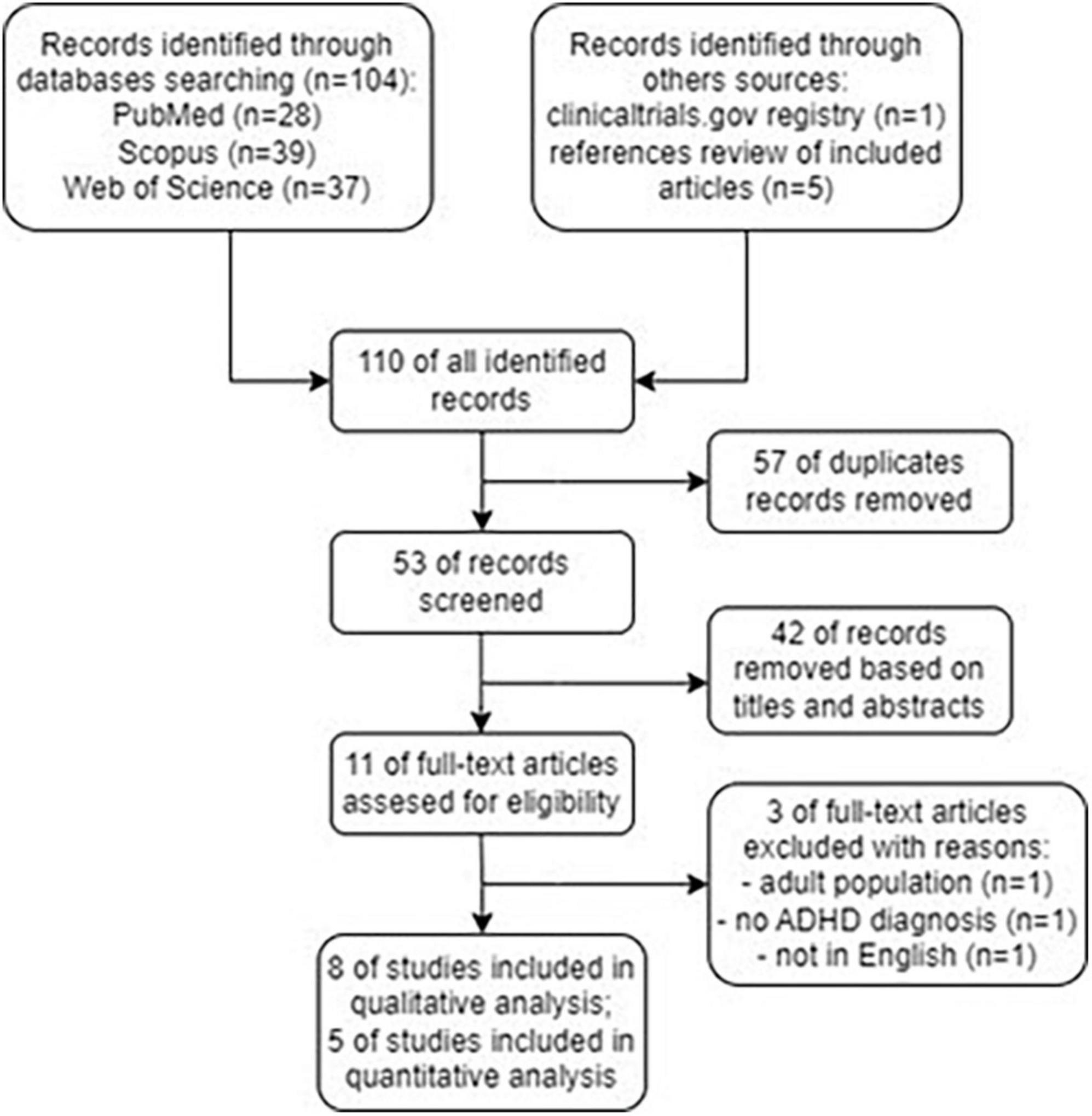
Figure 1. Flowchart showing an overview of the study selection process.
Among included studies 8, 7, and 6 of them investigated the NLR, PLR, and MLR, respectively. The papers were published between 2018 and 2022. All studies included both male and female subjects. The age of patients ranged from 8.3 ± 1.7 to 10.33 ± 3.15 years old. Seven of these studies were conducted in Turkey, one in Egypt. In all papers ADHD diagnoses were identified based on DSM-V criteria, while in one study additionally with the Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL) (23). Patients with other mental disorder were excluded in all cases. All ADHD children were diagnosed with delayed language development (DLD) in one of the studies (27) and in another with specific learning disorder (SLDs) (30). One study excluded patients with other psychiatric disorders, with the exception of oppositional defiant disorder (ODD) (24). In all but one study, participants received no treatment, in one study the majority of patients (85%) were treated. One study did not provide information about diagnosis criteria, numbers and sex of participants, comorbidities and medical treatment (29). The detailed information about included studies are presented in Table 1.
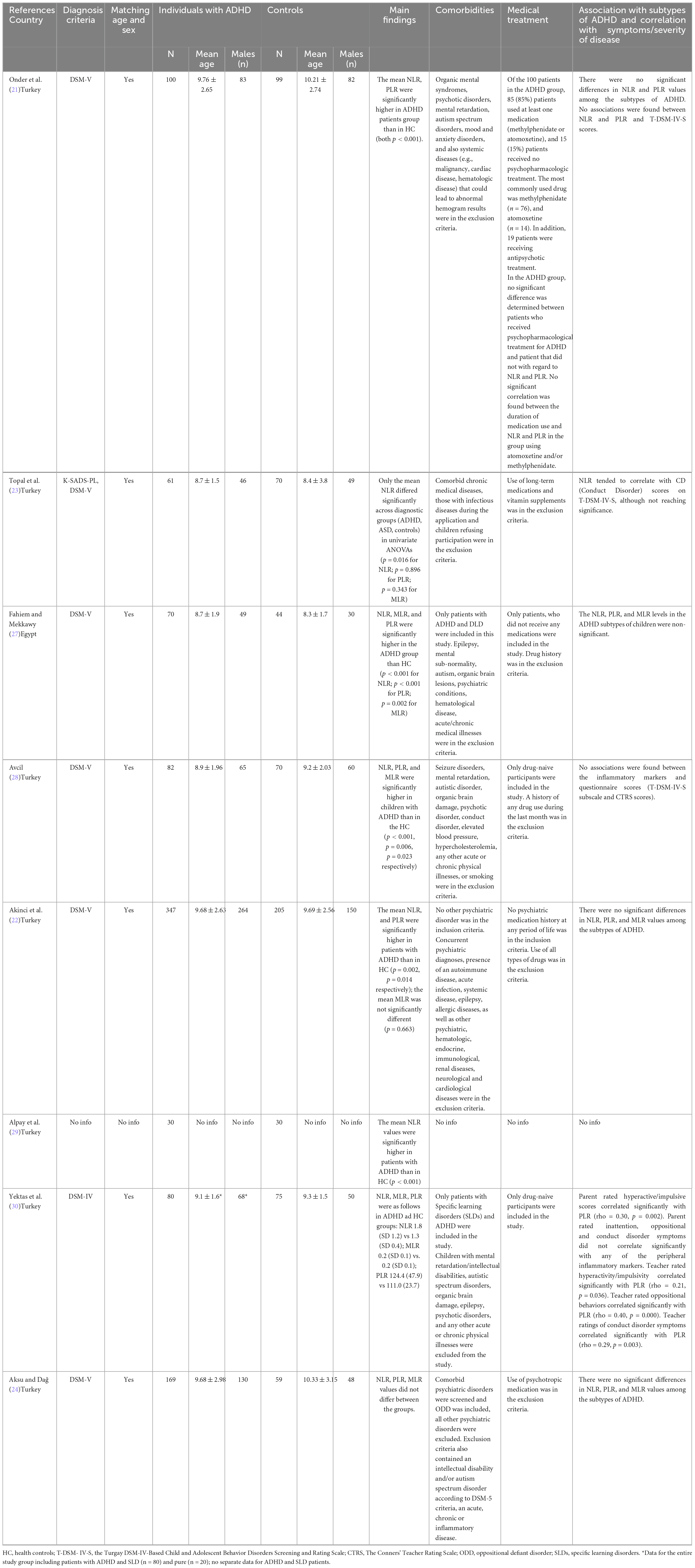
Table 1. Characteristics of included studies.
Table 2 provides quality scores for the papers, assessing risk of bias. Six of the studies were of high quality, one was of fair quality (30), and one was of poor quality (29). Only the high and fair quality studies were included in meta-analysis.
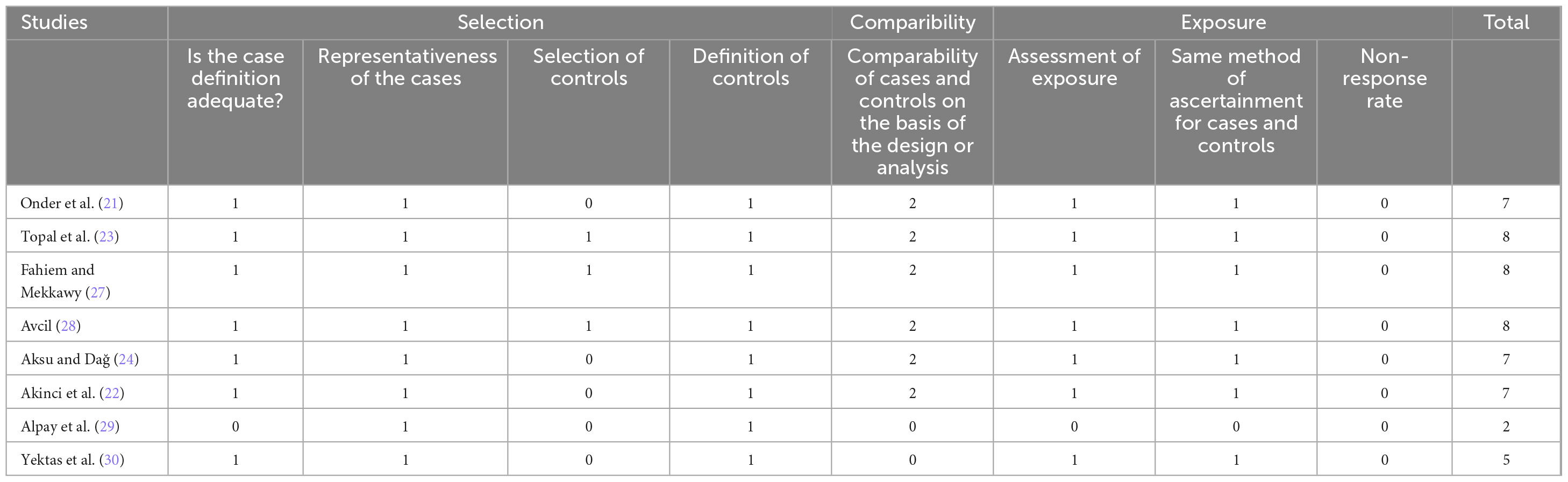
Table 2. Quality assessment of included studies with Newcastle-Ottawa Scale (NOS).
Table 3 provides information about inflammatory markers (NLR, MLR, PLR) in studies included in the meta-analysis.

Table 3. Studies included in meta-analysis and inflammatory markers ratio.
NLR in ADHD patients was evaluated in eight studies. The mean NLR were significantly higher in ADHD patients group than in healthy controls in six of them (6/8, 75%). the difference between groups was not significant in one of the studies (24), in another one the statistical significance was not reported (30).
Three of the eight studies were excluded from the meta-analysis: two due lack of raw data (27, 28) and one due to poor quality (29). The pooled analyses showed that the ADHD subjects had higher levels of NLR than the healthy controls. The heterogeneity of the studies was substantial (I2 = 86%, Chi2 = 28.75, df = 4, Tau2 = 0.12, p < 0.00001). The standardized mean difference (SMD) was 0.49 [0.15, 0.82]. Test for overall effect: Z = 2.87 (p = 0.004). The analysis found discrepancies reflected in the considerable heterogeneity of analyzed studies. Specifically, we identified one significant outlier (21). This study was the only one in which the majority of the patients (85%) received medical treatment. Thus, we performed a sensitive analysis excluding this study. It resulted in a substantial decrease in heterogeneity (I2 = 78%, Chi2 = 13.71, df = 3, Tau2 = 0.07, p = 0.003). The result of meta-analysis did not change substantially. SMD was 0.37 [0.07, 0.66], test for overall effect: Z = 2.43, p = 0.02 (Figure 2).

Figure 2. Meta-analysis forest plot for NLR.
PLR in ADHD patients was evaluated in seven studies. The mean PLR were significantly higher in ADHD patients group than in healthy controls in four of them (4/7, 57%). The difference between groups was not significant in two of the studies (23, 24), in another one the statistical significance was not reported (30).
Two of seven studies were excluded from the meta-analysis due to lack of raw data (27, 28). The heterogeneity of included studies was substantial (I2 = 81%, Chi2 = 21.36, df = 4, Tau2 = 0.08, p = 0.0003). The standardized mean difference (SMD) was 0.31 [0.03, 0.59]. Test for overall effect: Z = 2.14 (p = 0.03). The sensitivity analysis was performed and one significant outlier was identified (21). This study was the only one in which the majority of patients (85%) received medical treatment. Excluding this one outlier resulted in a substantial decrease in heterogeneity (I2 = 33%, Chi2 = 4.49, df = 3, Tau2 = 0.01, p = 0.21). SMD was 0.17 [0.00, 0.33], test for overall effect: Z = 1.97, p = 0.05 (Figure 3).

Figure 3. Meta-analysis forest plot for PLR.
MLR in ADHD patients was evaluated in six studies. The mean MLR were significantly higher in ADHD patients group than in healthy controls in two of the studies (2/6, 33%) (27, 28). The difference between groups was not significant in three of the studies (22–24), in another one the statistical significance was not reported (30).
Two of six studies were excluded from the meta-analysis due to lack of raw data (27, 28). The heterogeneity was substantial (I2 = 72%, Chi2 = 10.56, df = 3, Tau2 = 0.05, p = 0.01). The standardized mean difference (SMD) was 0.22 [−0.04, 0.47]. Test for overall effect: Z = 1.63 (p = 0.10) (Figure 4).

Figure 4. Meta-analysis forest plot for MLR.
Four of the studies evaluated these inflammatory markers in ADHD subtypes (21, 22, 24, 27). Two of the studies did not provide any raw data on inflammatory parameter values (21, 27) and one did not report the exact number of patients for each disease subtype (24). Therefore, a meta-analysis was not feasible. However, the narrative synthesis appears to provide consistent results.
The mean NLR and PLR values with regard to the subtypes of ADHD were assessed in four of the studies. There were no statistically significant differences in these values among the subtypes of ADHD in all of them (4/4, 100%) (21, 22, 24, 27).
The mean MLR value in context of ADHD subtypes was assessed in three of the studies. There was no statistically significant difference in MLR value among the subtypes of ADHD in three of them (3/3, 100%) (22, 24, 27).
Only one study assessed patients with ADHD on medical treatment (85% participants) (21). This study was also a cause of heterogeneity in the meta-analysis. However, in the ADHD group, no significant difference was observed between patients who received psychopharmacological treatment for ADHD and patients who did not, with regard to NLR and PLR. Moreover, no significant correlation was found between the duration of medication use and the values of NLR or PLR in the group using atomoxetine and/or methylphenidate (21).
The correlation between inflammatory markers and scores on clinical scales was assessed in three studies. One of the studies showed no associations between NLR and PLR and T-DSM-IV-S scores (Turgay DSM-IV-Based Child and Adolescent Behavior Disorders Screening and Rating Scale) (21). Another one found no associations between the inflammatory markers (NLR, MLR, PLR) and questionnaire scores (T-DSM-IV-S subscale and CTRS scores - The Conners’ Teacher Rating Scale) (28). In third one NLR tended to correlate with CD (Conduct Disorder) scores on T-DSM-IV-S, although not reaching significance (23).
One study assessed correlation between inflammatory markers and parent/teacher-rated symptoms on T-DSM-IV-S (30). Parent-rated hyperactive/impulsive scores correlated significantly with PLR (rho = 0.30, p = 0.002). Nevertheless, parent-rated inattention, oppositional and conduct disorder symptoms did not correlate significantly with any of the peripheral inflammatory markers. Teacher-rated hyperactivity/impulsivity, oppositional behaviors and conduct disorder symptoms correlated significantly with PLR (rho = 0.21, p = 0.036; rho = 0.40, p = 0.000; rho = 0.29, p = 0.003, respectively) (30).
The present study aimed to systematically review and meta-analyze data on the association between - morphology-derived parameters - NLR, PLR, and MLR values and ADHD. To the best of our knowledge, this is the first systematic review and meta-analysis examining the above-mentioned associations in ADHD.
This study demonstrated that NLR and PLR values are higher in ADHD patients as compared to healthy controls. Undoubtedly, prospective clinical studies would be needed to confirm the role of these parameters as markers in ADHD; however, retrospective studies to date indicate the possibility of such potential use. These findings, however, may point to the involvement of inflammation in the pathogenesis of ADHD. NLR is a marker of systemic inflammation that links two different immune pathways. Neutrophils are front-line cells of innate immune defense and engage in a variety of physiological and pathological processes, such as inflammation, autoimmunity, and others (31). While migrating to the site of infection, they engage in phagocytosis and subsequently execute the elimination of pathogens (32). On the other hand, lymphocytes play a central role in adaptive immunity by actively contributing to the recognition of pathogen-specific immune responses, the generation of immune memory, and the maintenance of host immune homeostasis (33). The result of our meta-analysis may indicate that innate immunity is probably more responsible than adaptive immunity in the pathogenesis of ADHD. However, these pathways are connected as indicated by the neutrophil’s interaction with adaptive immunity. Furthermore, both neutrophils and lymphocytes can migrate into the brain, taking part in the development and exacerbation of neuroinflammation (20). Several studies have shown that platelets are important components of both innate and adaptive immunity (34). They are a major source of cytokines and pro-inflammatory molecules and have some similarities with neurons, such as the transport, metabolism, and release of several neurotransmitters. Although this effect was not as strong as that of NLR, our study demonstrated that PLR can suggest neuroinflammation in patients with ADHD. In contrast, the combined MLR score of the four studies showed no significant difference between ADHD patients and health control. Monocytes are involved in innate and adaptive immunity, primarily responsible for phagocytosis, antigen presentation, and cytokine production (35). They can also migrate to the brain, where cooperating with microglia, they contribute to neuroinflammation (36). More research is needed in this field to draw more reliable conclusions.
Only one study included patients treated with psychostimulants. No significant difference was determined between patients who received psychopharmacological treatment for ADHD and patients that did not with regard to NLR and PLR. However, this study was an outlier contributing significantly to the heterogeneity in the meta-analysis comparing ADHD patients with healthy controls, suggesting that psychostimulant treatment may affect peripheral inflammatory markers (21). Some previous studies reported proinflammatory properties of psychostimulants. Preclinical study found that chronic treatment with methylphenidate can cause oxidative stress, neuroinflammation and neurodegeneration in hippocampus of adult rats (37). Moreover, young animals appear to be more susceptible to damage induced by methylphenidate (38). Another animal study found that amphetamine-like agents induced neuroinflammation in the hippocampus of mice, which could be prevented by anti-inflammatory treatment (39). However, in human study lower levels of IFN-γ and IL-13 in treated patients with ADHD compared to untreated patients were reported, indicating an effect of medication on levels of these cytokines (11). Further prospective studies are needed to assess the correlation of NLR, MLR, PLR, and others inflammatory markers with drug treatment in ADHD.
Our study did not find any significant association between NLR, PLR, and MLR, and specific subtypes of ADHD diagnosis. These result suggest that increased inflammation may be a feature of overall ADHD diagnosis rather than specific subtypes. Our finding are consistent with those of other studies on inflammatory markers in ADHD. No difference in Il-6, TNF-α and morning cortisol measurement was observed between combined and inattentive ADHD subtypes (40, 41). Additionally, inflammation may indicate a ADHD diagnosis, but not reflect the severity of the disease. None of the studies included in the review confirmed a correlation between scores on the clinical assessment scale and inflammatory markers.
As regards the relationship between inflammatory markers and ADHD symptoms, this issue remains unclear. In study conducted by Oates et al., elevated levels of IL-13 were associated with inattention, while elevated levels of IL-16 were associated with hyperactivity. Oppositional symptoms were found to be associated with a decrease in IL-2. Furthermore, an increase in IL-16 and a decrease in TNF-α and IL-6 were positively correlated with commissions errors (10). In our review, two studies found no correlation with scores on the T-DSM-IV-S scale (21, 28), while one observed a tendency to correlate with conduct disorder symptoms (23). Interestingly, PLR was correlated with hyperactive/impulsive scores assessed by parents and hyperactive/impulsive scores, oppositional behaviors and conduct disorder symptoms assessed by teachers (30). Although the results obtained so far do not appear to support a correlation between symptoms and NLR, MLR, and PLR, more research is needed to evaluate this issue.
Current treatment of ADHD involves symptom reduction and is purely symptomatic. Investigating the role of inflammation in the pathogenesis of ADHD may contribute to the development of new therapies. To date, no study has been conducted to assess the efficacy of anti-inflammatory treatment in ADHD, with used e.g., non-steroidal anti-inflammatory drugs (NSAIDs). Clinical trials have confirmed the efficacy and safety of NSAIDs in other mental disorders in which inflammation plays a role in the pathogenesis, such as mood disorders (42, 43). However, there are studies evaluating additional treatment of nutraceuticals with postulated anti-inflammatory properties in ADHD. A randomized controlled trial conducted over 8 weeks with 103 children showed that supplementation with omega-3 fatty acids, which are involved in arachidonic acid pathways, led to a significant reduction in inflammatory markers such as CRP and IL-6. In addition, this supplementation resulted in a noticeable clinical improvement (44). A recent meta-analysis showed that polyunsaturated fatty acids (PUFA) may have a limited effect on treatment outcomes in ADHD (45). Nevertheless, a better understanding of the inflammatory background in ADHD may help to identify patients with higher levels of inflammation. For these patients, the probability of response to add-on anti-inflammatory treatment could be much greater and result in an improved quality of life.
In recent years, the number of adults diagnosed with ADHD has been increasing (46). To date, there has been only one study evaluating NLR, MLR, and PLR values in adult patients (47). There were no differences in these parameters compared to the control group, as well as no associations with treatment or clinical symptoms were observed. However, further studies with a prospective, longitudinal model including a larger study group are required for conclusive results.
Our study has certain limitations, that should be acknowledged. Firstly, the correlations presented may not demonstrate a causal relationship. Elevations in inflammatory markers may indicate the role of inflammation in the pathogenesis of ADHD; however, it is also possible that ADHD develops independently and that its particular features, such as hyperactivity, lower social functioning status, or hygiene, contribute to the increase of these markers. Therefore, careful interpretation of the results is required to understand the complex association between ADHD and inflammatory markers. Secondly, with the exception of one study, all the included studies were conducted within the same country. A recent meta-analysis demonstrated that individuals with depression in Turkey and China displayed significantly higher NLR values compared to other countries. Conversely, PLR was higher among individuals from China rather than Turkey (17). This indicates that these parameters may vary depending on ethnicity. Thirdly, only one study included pharmacologically treated patients. Additional investigations are needed to evaluate whether these markers can serve as indicators of treatment efficacy. Fourthly, we did not conduct a subgroup analysis based on gender differences, as the majority of the studies did not include gender-specific groups. Gender disparities may play a crucial role and potentially explain the diverse range of outcomes observed. Fifth, inflammatory markers may be affected by many other variables, such as medical disease, nutrition, or smoking, which many studies have not reported. Future studies should consider these variables in the evaluation of NLR, MLR, and PLR.
The original contributions presented in this study are included in this article/supplementary material, further inquiries can be directed to the corresponding author.
AG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review and editing. SM: Data curation, Investigation, Writing – original draft. MG: Data curation, Investigation, Writing – original draft. AA: Funding acquisition, Supervision, Writing – review and editing. PM: Project administration, Supervision, Writing – review and editing. MD: Funding acquisition, Project administration, Supervision, Writing – review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to acknowledge Oliwia Bielecka for her help in the evaluation and linguistic corrections of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Posner J, Polanczyk GV, Sonuga-Barke E. Attention-deficit hyperactivity disorder. Lancet. (2020) 395:450–62. doi: 10.1016/S0140-6736(19)33004-1
2. Harpin V. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child. (2005) 90, (Suppl. 1):i2–7. doi: 10.1136/adc.2004.059006
3. Sharma A, Couture J. A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Ann Pharmacother. (2014) 48:209–25. doi: 10.1177/1060028013510699
4. Saccaro L, Schilliger Z, Perroud N, Piguet C. Inflammation, anxiety, and stress in attention-deficit/hyperactivity disorder. Biomedicines. (2021) 9:1313. doi: 10.3390/biomedicines9101313
5. Dunn G, Nigg J, Sullivan E. Neuroinflammation as a risk factor for attention deficit hyperactivity disorder. Pharmacol Biochem Behav. (2019) 182:22–34.
6. Instanes J, Halmøy A, Engeland A, Haavik J, Furu K, Klungsøyr K. Attention-deficit/hyperactivity disorder in offspring of mothers with inflammatory and immune system diseases. Biol Psychiatry. (2017) 81:452–9. doi: 10.1016/j.biopsych.2015.11.024
7. Lin Y, Chen Y, Gau S, Yeh T, Fan H, Hwang Y, et al. Associations between allergic diseases and attention deficit hyperactivity/oppositional defiant disorders in children. Pediatr Res. (2016) 80:480–5. doi: 10.1038/pr.2016.111
8. Darwish A, Elgohary T, Nosair N. Serum Interleukin-6 level in children with Attention-Deficit Hyperactivity Disorder (ADHD). J Child Neurol. (2019) 34:61–7. doi: 10.1177/0883073818809831
9. Donfrancesco R, Nativio P, Borrelli E, Giua E, Andriola E, Villa MP, et al. Serum cytokines in pediatric neuropsychiatric syndromes: focus on Attention deficit hyperactivity disorder. Minerva Pediatr. (2021) 73:398–404. doi: 10.23736/S2724-5276.16.04642-9
10. Oades RD, Myint A-M, Dauvermann MR, Schimmelmann BG, Schwarz MJ. Attention-deficit hyperactivity disorder (ADHD) and glial integrity: an exploration of associations of cytokines and kynurenine metabolites with symptoms and attention. Behav Brain Funct. (2010) 6:32. doi: 10.1186/1744-9081-6-32
11. Oades RD, Dauvermann MR, Schimmelmann BG, Schwarz MJ, Myint A-M. Attention-deficit hyperactivity disorder (ADHD) and glial integrity: S100B, cytokines and kynurenine metabolism–effects of medication. Behav Brain Funct. (2010) 6:29. doi: 10.1186/1744-9081-6-29
12. Urbanowicz T, Olasińska-Wiśniewska A, Michalak M, Rodzki M, Witkowska A, Straburzyńska-Migaj E, et al. The prognostic significance of neutrophil to Lymphocyte Ratio (NLR), Monocyte to Lymphocyte Ratio (MLR) and Platelet to Lymphocyte Ratio (PLR) on Long-Term Survival in Off-Pump Coronary Artery Bypass Grafting (OPCAB) procedures. Biology. (2021) 11:34. doi: 10.3390/biology11010034
13. Mihai A, Caruntu A, Opris-Belinski D, Jurcut C, Dima A, Caruntu C, et al. The predictive role of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), Monocytes-to-Lymphocyte Ratio (MLR) and gammaglobulins for the development of cutaneous vasculitis lesions in Primary Sjögren’s syndrome. J Clin Med. (2022) 11:5525. doi: 10.3390/jcm11195525
14. Qun S, Tang Y, Sun J, Liu Z, Wu J, Zhang J, et al. Neutrophil-to-lymphocyte ratio predicts 3-month outcome of acute ischemic stroke. Neurotox Res. (2017) 31:444–52. doi: 10.1007/s12640-017-9707-z
15. Erre GL, Paliogiannis P, Castagna F, Mangoni AA, Carru C, Passiu G, et al. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur J Clin Invest. (2019) 49:e13037. doi: 10.1111/eci.13037
16. Zhao W-M, Tao S-M, Liu G-L. Neutrophil-to-lymphocyte ratio in relation to the risk of all-cause mortality and cardiovascular events in patients with chronic kidney disease: a systematic review and meta-analysis. Ren Fail. (2020) 42:1059–66. doi: 10.1080/0886022X.2020.1832521
17. Su M, Ouyang X, Song Y. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and monocyte to lymphocyte ratio in depression: {A} meta-analysis. J Affect Disord. (2022) 308:375–83. doi: 10.1016/j.jad.2022.04.038
18. Mazza MG, Lucchi S, Tringali AGM, Rossetti A, Botti ER, Clerici M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: a meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 84:229–36. doi: 10.1016/j.pnpbp.2018.03.012
19. Mazza MG, Lucchi S, Rossetti A, Clerici M. Neutrophil-lymphocyte ratio, monocyte-lymphocyte ratio and platelet-lymphocyte ratio in non-affective psychosis: a meta-analysis and systematic review. World J Biol Psychiatry. (2020) 21:326–38. doi: 10.1080/15622975.2019.1583371
20. Cheng Y, Wang Y, Wang X, Jiang Z, Zhu L, Fang S. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and monocyte-to-lymphocyte ratio in depression: an updated systematic review and meta-analysis. Front Psychiatry. (2022) 13:893097. doi: 10.3389/fpsyt.2022.893097
21. Onder A, Coban OG, Adanir AS, Önder A, Gizli Çoban Ö, Sürer Adanır A. Elevated neutrophil-to-lymphocyte ratio in children and adolescents with attention-deficit/hyperactivity disorder. Int J Psychiatry Clin Pract. (2021) 25:43–8. doi: 10.1080/13651501.2020.1804940
22. Akinci MA, Uzun N, Akıncı MA, Uzun N. Evaluation of hematological inflammatory markers in children and adolescents with attention deficit/hyperactivity disorder. Bratislava Med J. (2021) 122:256–62. doi: 10.4149/BLL_2021_042
23. Topal Z, Tufan AE, Karadag M, Gokcen C, Akkaya C, Sarp AS, et al. Evaluation of peripheral inflammatory markers, serum B12, folate, ferritin levels and clinical correlations in children with autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD). Nord J Psychiatry. (2022) 76:150–7. doi: 10.1080/08039488.2021.1946712
24. Aksu GG, Dağ P. Evaluation of the indicators of inflammation in children and adolescents with attention deficit and hyperactivity disorder: effect of sex and subtype. Duzce Med J. (2020) 22:84–90. doi: 10.18678/dtfd.690128
25. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. (2021) 372:n160. doi: 10.1136/bmj.n160
26. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. (2000). Available online at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed June 1, 2023).
27. Fahiem RA, Mekkawy LH. A new perspective of attention deficit hyperactivity disorder associated with delayed language development: an Egyptian sample. Psychiatry Investig. (2022) 19:164–70. doi: 10.30773/pi.2021.0232
28. Avcil S. Evaluation of the neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and mean platelet volume as inflammatory markers in children with attention-deficit hyperactivity disorder. Psychiatry Clin Neurosci. (2018) 72:522–30. doi: 10.1111/pcn.12659
29. Alpay M, Yektas C, Karacor K. The systemic cell apoptotic-based neutrophil-lymphocyte ratio: experience in children diagnosed with ADHD and Autism Spectrum Disorder. Konuralp Tip Derg. (2021) 13:74–81. doi: 10.18521/ktd.737628
30. Yektas C, Tufan AE, Kilicaslan O, Yazici M, Karakaya SEK, Sarigedik E. Elevated monocyte levels maybe a common peripheral inflammatory marker in specific learning disorders and attention deficit/hyperactivity disorder. Psychiatry Behav Sci. (2022) 12:125–33. doi: 10.5455/PBS.20210518080022
31. Liew PX, Kubes P. The neutrophil’s role during health and disease. Physiol Rev. (2019) 99:1223–48. doi: 10.1152/physrev.00012.2018
32. Mayadas TN, Cullere X, Lowell CA. The multifaceted functions of neutrophils. Annu Rev Pathol. (2014) 9:181–218. doi: 10.1146/annurev-pathol-020712-164023
33. Bonilla FC, Oettgen HC. Adaptive immunity. J Allergy Clin Immunol. (2010) 125:S33–40. doi: 10.1016/j.jaci.2009.09.017
34. Koupenova M, Clancy L, Corkrey HA, Freedman JE. Circulating platelets as mediators of immunity, inflammation, and thrombosis. Circ Res. (2018) 122:337–51. doi: 10.1161/CIRCRESAHA.117.310795
35. Germic N, Frangez Z, Yousefi S, Simon H-U. Regulation of the innate immune system by autophagy: monocytes, macrophages, dendritic cells and antigen presentation. Cell Death Differ. (2019) 26:715–27. doi: 10.1038/s41418-019-0297-6
36. Wohleb ES, Fenn AM, Pacenta AM, Powell ND, Sheridan JF, Godbout JP. Peripheral innate immune challenge exaggerated microglia activation, increased the number of inflammatory CNS macrophages, and prolonged social withdrawal in socially defeated mice. Psychoneuroendocrinology. (2012) 37:1491–505. doi: 10.1016/j.psyneuen.2012.02.003
37. Motaghinejad M, Motevalian M, Shabab B. Effects of chronic treatment with methylphenidate on oxidative stress and inflammation in hippocampus of adult rats. Neurosci Lett. (2016) 619:106–13. doi: 10.1016/j.neulet.2015.12.015
38. Foschiera LN, Schmitz F, Wyse ATS. Evidence of methylphenidate effect on mitochondria, redox homeostasis, and inflammatory aspects: insights from animal studies. Prog Neuropsychopharmacol Biol Psychiatry. (2022) 116:110518. doi: 10.1016/j.pnpbp.2022.110518
39. Gonçalves J, Baptista S, Martins T, Milhazes N, Borges F, Ribeiro CF, et al. Methamphetamine-induced neuroinflammation and neuronal dysfunction in the mice hippocampus: preventive effect of indomethacin. Eur J Neurosci. (2010) 31:315–26. doi: 10.1111/j.1460-9568.2009.07059.x
40. Corominas-Roso M, Armario A, Palomar G, Corrales M, Carrasco J, Richarte V, et al. IL-6 and TNF-α in unmedicated adults with ADHD: relationship to cortisol awakening response. Psychoneuroendocrinology. (2017) 79:67–73. doi: 10.1016/j.psyneuen.2017.02.017
41. Ramos-Quiroga JA, Corominas-Roso M, Palomar G, Ferrer R, Valero S, Corrales M, et al. Cortisol awakening response in adults with attention deficit hyperactivity disorder: subtype differences and association with the emotional lability. Eur Neuropsychopharmacol. (2016) 26:1140–9. doi: 10.1016/j.euroneuro.2016.03.014
42. Gędek A, Szular Z, Antosik AZ, Mierzejewski P, Dominiak M. Celecoxib for mood disorders: a systematic review and meta-analysis of randomized controlled trials. J Clin Med. (2023) 12:3497. doi: 10.3390/jcm12103497
43. Dominiak M, Gędek A, Sikorska M, Mierzejewski P, Wojnar M, Antosik-Wójcińska A. Acetylsalicylic acid and mood disorders: a systematic review. Pharmaceuticals. (2022) 16:67. doi: 10.3390/ph16010067
44. Hariri M, Djazayery A, Djalali M, Saedisomeolia A, Rahimi A, Abdolahian E. Effect of n-3 supplementation on hyperactivity, oxidative stress and inflammatory mediators in children with attention-deficit-hyperactivity disorder. Malays J Nutr. (2012) 18:329–35.
45. Gillies D, Leach MJ, Perez Algorta G. Polyunsaturated fatty acids (PUFA) for attention deficit hyperactivity disorder (ADHD) in children and adolescents. Cochr Datab Syst Rev. (2023) 4:CD007986. doi: 10.1002/14651858.CD007986.pub3
46. Adamis D, Flynn C, Wrigley M, Gavin B, McNicholas F. ADHD in adults: a systematic review and meta-analysis of prevalence studies in outpatient psychiatric clinics. J Atten Disord. (2022) 26:1523–34. doi: 10.1177/10870547221085503
47. Ceyhun HA, Gürbüzer N. New hematological parameters as inflammatory biomarkers: systemic immune inflammation index, platerethritis, and platelet distribution width in patients with adult attention deficit hyperactivity disorder. Adv Neurodev Disord. (2022) 6:211–23. doi: 10.1007/s41252-022-00258-6
Keywords: attention-deficit hyperactivity disorder, neutrophil-to-lymphocyte ratio, platelet-to lymphocyte ratio, monocyte-to lymphocyte ratio, inflammation, blood parameters
Citation: Gędek A, Modrzejewski S, Gędek M, Antosik AZ, Mierzejewski P and Dominiak M (2023) Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and monocyte to lymphocyte ratio in ADHD: a systematic review and meta-analysis. Front. Psychiatry 14:1258868. doi: 10.3389/fpsyt.2023.1258868
Received: 14 July 2023; Accepted: 26 October 2023;
Published: 14 November 2023.
Edited by:
İlhan Bahşi, University of Gaziantep, TürkiyeReviewed by:
Elijah W. Hale, University of Colorado Anschutz Medical Campus, United StatesCopyright © 2023 Gędek, Modrzejewski, Gędek, Antosik, Mierzejewski and Dominiak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adam Gędek, YWRhbWdlZGVrQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.