
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 31 October 2023
Sec. Mood Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1250987
 Albino J. Oliveira-Maia1,2
Albino J. Oliveira-Maia1,2 Benoit Rive3*
Benoit Rive3* Joachim Morrens4
Joachim Morrens4 Yordan Godinov5Jedelyn Cabrieto4Nolen Perualila4Siobhán Mulhern-Haughey6
Yordan Godinov5Jedelyn Cabrieto4Nolen Perualila4Siobhán Mulhern-Haughey6Background: The efficacy of esketamine nasal spray (NS) as a rapid-acting agent for treatment resistant depression (TRD) was demonstrated in comparisons with placebo, when both were given in addition to a newly initiated selective serotonin reuptake inhibitor (SSRI)/serotonin norepinephrine reuptake inhibitor (SNRI). How esketamine NS compares with commonly used real-world (RW) polypharmacy treatment strategies is not known.
Method: ICEBERG was an adjusted indirect treatment comparison that analysed data from SUSTAIN-2 (NCT02497287; clinicaltrials.gov), a long-term, open-label study of esketamine NS plus SSRI/SNRI, and the European Observational TRD Cohort (EOTC; NCT03373253; clinicaltrials.gov), an observational study of routine clinical practice. Data were compared between patients receiving esketamine NS (SUSTAIN-2) and those from the EOTC treated with polypharmacy treatment strategies, either combination or augmentation. Analyses were adjusted for potential confounders, using rescaled average treatment effect among treated estimates. Threshold analyses were conducted to assess potential impact of unmeasured confounders on the robustness of analyses where esketamine NS was found to be significantly superior. Sensitivity analyses were used to understand the impact of analysis method selection and data handling.
Results: Esketamine NS treatment resulted in a higher probability of 6-month response (49.7% [95% confidence interval (CI) 45.6–53.9]) and remission (33.6% [95% CI 29.7–37.6]) versus RW polypharmacy (26.8% [95% CI 21.0–32.5] and 19.4%, [95% CI 14.2–24.6], respectively). Relative risk calculations showed esketamine NS was 1.859 (95% CI 1.474–2.345; p < 0.0001) times as likely to result in response and 1.735 (1.297–2.322; p = 0.0002) times as likely to result in remission versus RW polypharmacy at 6 months. Threshold and extensive sensitivity analyses supported that analyses of esketamine NS superiority were robust.
Conclusion: ICEBERG supports esketamine NS being superior to current RW individualized polypharmacy strategies, including augmentation, with benefits extending beyond acute use, to improved chance of 6-month response and remission. While unobserved confounding factors may certainly impact results of an indirect comparison, threshold analysis supported a low likelihood of this affecting the conclusions.
To view an animated summary of this publication, please click on the Supplementary video.
Treatment resistant depression (TRD) is most often defined as a major depressive episode (MDE) that fails to respond to two or more different antidepressants given at adequate dose and duration (1, 2), and affects 10–30% of patients with major depressive disorder (MDD) (3–6). In the real-world (RW) setting, as many as 74% of patients with TRD do not achieve a response (i.e., 50% or greater reduction in symptom severity, as measured, for example, by the Montgomery-Åsberg Depression Rating Scale score [MADRS]) to new treatment after 6 months, and as few as 17% achieve symptom remission (defined according to minimal symptom severity, such as total MADRS score ≤ 10) (7). Importantly, the likelihood of achieving response or remission decreases as treatment failures increase (5, 8). Furthermore, relapse is common, especially in patients who achieve response but not remission (5, 7). TRD has a greater patient and societal burden than non-treatment resistant MDD, including lower health-related quality of life (HRQoL) and increased work and activity impairment (4, 9, 10). It is therefore crucial to identify which treatments are most likely to result in, and maintain, remission for patients with TRD.
A lack of evidence to support one treatment over others has resulted in a heterogenous treatment landscape for TRD. Currently, real-world treatment (RWT) involves the use of any treatment or combination of treatments approved for use in MDD (7, 11), including pharmacological monotherapy or polypharmacy (6, 11). Pharmacological monotherapy can be of any substance approved for use in MDD, prescribed on its own. Polypharmacy can be either the prescription of combinations of antidepressant medications or the augmentation of at least one antidepressant with a substance without primary antidepressant properties for MDD, such as second generation antipsychotics (e.g., aripiprazole, quetiapine and risperidone) or mood stabilizers (e.g., lithium and lamotrigine) (6, 11–14). A recent study of patients in Europe reported use of more than 50 different pharmacological medications among a cohort of 411 patients with TRD across seven European countries, with polypharmacy as the most common treatment strategy (7).
To date, almost all pharmacological antidepressant treatments target the monoamine pathway (15). In the last decade, however, newer treatments targeting glutamatergic neurotransmission have emerged as promising alternatives (16–18), including esketamine nasal spray (NS), an N-methyl-D-aspartate (NMDA) receptor antagonist (19). In randomised controlled trials (RCTs), esketamine NS in addition to either a selective serotonin reuptake inhibitor (SSRI) or a serotonin norepinephrine reuptake inhibitor (SNRI) was more effective for patients with TRD than antidepressant plus placebo (20–23). Based on these results, esketamine NS, in combination with a SSRI or SNRI, obtained American and European-wide market approval specifically for TRD (19, 24). However, only newly-initiated SSRI/SNRI monotherapy was used as the active comparator in these RCTs. Furthermore, the existing phase 3 RCTs did not combine acute and maintenance treatment phases in a single, long-term comparative study to assess esketamine NS during both treatment phases (20–23). The Indirect adjusted Comparison Estimating the Benefit of Esketamine compared with Routine treatment of TRD in General psychiatry (ICEBERG) analyses were designed to address this evidence gap. The objective was to compare long-term (6-month) data, from two distinct studies, on the efficacy of esketamine NS with that of RWT, extending both the range of comparators and period of treatment relative to currently available data.
Focusing on clinical response and remission, a parallel publication from the ICEBERG study showed patients receiving esketamine NS were almost twice as likely to achieve response or remission compared with patients receiving their physician’s best choice (RWT) (25). However, as RWT is very heterogenous (7), these findings do not guarantee superiority of esketamine NS over each different treatment type included in the mixed comparator group. Here, we focus on a more homogenous treatment strategy type, presenting adjusted comparison of response and remission rates at 6 months for patients receiving esketamine NS plus SSRI/SNRI relative to patients receiving RW polypharmacy treatment strategies. Given that there is no robust evidence to suggest higher efficacy for either combination or augmentation strategies and guidelines do not specify a preferred approach (26–28) they have been pooled in a single RW polypharmacy treatment group for the purposes of these analyses.
An indirect adjusted treatment comparison (ITC) of esketamine NS with RW polypharmacy was performed using individual patient 6-month response and remission data from two studies of patients with TRD. SUSTAIN-2 (NCT02497287) was a global, long-term, single-arm, open-label study of the safety and efficacy of esketamine NS given in combination with a new oral antidepressant (SSRI or SNRI, as per the label), which included patients from Europe (29). The European Observational TRD Cohort (EOTC; NCT03373253) study was a prospective, non-interventional, multicenter study of patients initiating a new, routine treatment for TRD in RW clinical practice (7). In this RW study, all patients were receiving medication and/or other treatments according to usual care in their treatment setting, with treatment, dose and administration at the discretion of the prescribing clinician (7, 30). These studies were selected for comparison as they were designed with similar inclusion and exclusion criteria, including the same operational definition of TRD, and both provided long-term follow-up of patients. EOTC and SUSTAIN-2 study designs, along with key inclusion and exclusion criteria, are provided in Supplementary Figure S1 and the Supplementary methods, with a summary table found in Supplementary Table S1. All participants in both studies provided written informed consent.
Data included in the adjusted ITC from the EOTC study were restricted to those from patients starting an antidepressant treatment involving at least one oral antidepressant medication. Patients that did not receive at least one antidepressant medication (e.g., receiving an antipsychotic as monotherapy, or receiving only neurostimulation treatments and/or psychosocial interventions without an accompanying antidepressant) were excluded. No patients in the EOTC received esketamine NS as it was not available to prescribe until after the study ended. The analyses reported here focused on patients from the EOTC who were on a polypharmacy treatment strategy. This included any patient taking at least one oral antidepressant (a) combined with one or more additional oral antidepressant (combination therapy) and/or (b) augmented with one or more antipsychotic or mood stabilizing substances (augmentation therapy). Handling of dropouts and treatment changes is described in Supplementary methods and Supplementary Table S2.
Some level of imbalance was expected between the two treatment groups, as patients were not randomly assigned to one or the other of the studies. It is possible that the cohorts may have had different baseline prognostic factors leading to confounding effects on the outcomes and bias in favor of one treatment. Patient covariates, reported in both SUSTAIN-2 and the EOTC studies, covering sociodemographics as well as clinical, psychometric, disease and treatment history (Supplementary Table S3), were used in analyses comparing data from the two studies.
Esketamine NS was compared to polypharmacy using two different approaches to adjust for imbalances between both study populations, based on potential prognostic factors. Both approaches used 17 baseline patient covariates that both SUSTAIN-2 and the EOTC data had in common. For the main analysis, propensity score (PS) based inverse probability weighting (IPW) comparisons were used. Data from patients in the RW polypharmacy arm (EOTC) were reweighted using a rescaled average treatment effect among treated (ATT) IPW method. This approach, based on propensity scores estimated using the 17 patient covariates, aimed to remodel the EOTC data to act as a matched RW polypharmacy pseudo-control arm for the data from SUSTAIN-2. Data from patients on RW monotherapy were also reweighted using ATT IPW for comparison purposes with the main analyses. The covariates and IPW are described in more detail in the Supplementary methods.
Response to treatment (≥50% improvement in total MADRS score, relative to baseline) and remission (total MADRS score ≤10) at 6 months were compared between the two studies. Analysis was based on observed cases and treatment effect was calculated as an odds ratio (OR). For illustrative and interpretation purposes, values for relative risk (RR), risk difference (RD) and number needed to treat (NNT), as well as the estimated probability of achieving response or remission, were also produced. Threshold analyses were carried out when esketamine NS was significantly superior, to assess how much lower the rates of response and remission for esketamine NS could be without losing statistically significant superiority over RW polypharmacy (Supplementary methods).
The second approach used multivariable logistic regression models to compare esketamine NS with RW polypharmacy while accounting for potential between-study imbalances in the distribution of the 17 covariates. Using the adjusted OR, the models were also used to identify the variables that were the strongest predictors of response and remission.
Sensitivity analyses (SA), examining the effect of using either different IPW methods (SA1, SA2 and SA3) or different data handling approaches (SA4 and SA5) are described in Supplementary methods.
Study flow diagrams detailing inclusion of patients from the SUSTAIN-2 and EOTC studies are shown in Supplementary Figure S2. Before reweighting, baseline characteristics of patients in the esketamine NS group (n = 559) were largely comparable to those in the RW polypharmacy group (n = 225) including the percentage of women, mean age, mean number of treatment failures in the current MDE and mean duration of each treatment received during the current MDE (Table 1).
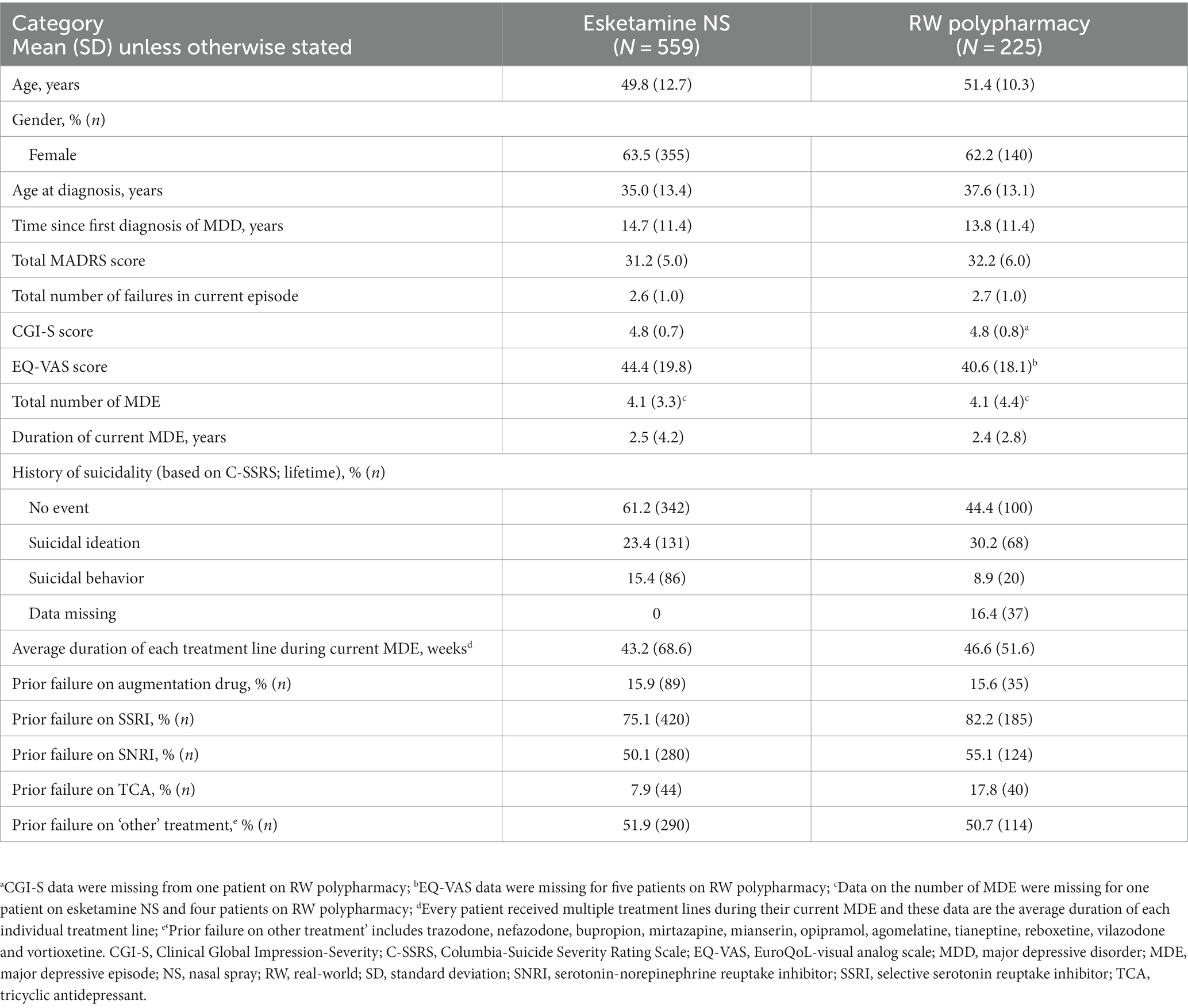
Table 1. Baseline characteristics.
PS reweighting of the baseline covariates showed a larger overlap in distributions after reweighting. Following reweighting, standardised mean difference (SMD) between polypharmacy and esketamine NS treatment was reduced across almost all baseline variables (Supplementary Figure S3). Indeed, all SMDs were between −0.2 and + 0.2, indicating that none were clinically detectable. In exploratory analyses, PS reweighting was also applied to data from 82 patients treated with monotherapy at baseline, for potential comparison with the main analyses. However, in this subgroup, reweighting did not reduce the SMD between treatments for any of the variables in the full, 17 covariate model (Supplementary Figure S4). Including fewer covariates also did not lead to reductions in the SMDs (data not shown), so no further analysis was feasible in the monotherapy subgroup.
In unadjusted analyses of data observed at Month 6, response was reached in 278/559 (49.7%) of patients taking esketamine NS. In patients receiving RW polypharmacy, 57/225 (25.3%) reached response and following ATT reweighting, the estimated probability of response was 26.8% (95% confidence interval [CI] 21.0–32.5%; Figure 1). The OR (95% CI) of achieving response with esketamine NS versus RW polypharmacy was 2.709 (1.930–3.802; p < 0.0001; Table 2). Significant superiority of esketamine NS in achieving response was also found when other treatment effect measures were estimated. In terms of RR, patients taking esketamine NS were 1.859 (1.474–2.345; p < 0.0001) times as likely to achieve response than patients on RW polypharmacy. RD (95% CI) values represented an additional 23.0% (15.9–30.1%) of patients achieving response with esketamine NS compared with RW polypharmacy. When NNT values were considered, five patients would need to be treated with esketamine NS and five with RW polypharmacy to obtain one additional patient experiencing response in the esketamine group relative to the RW polypharmacy group.
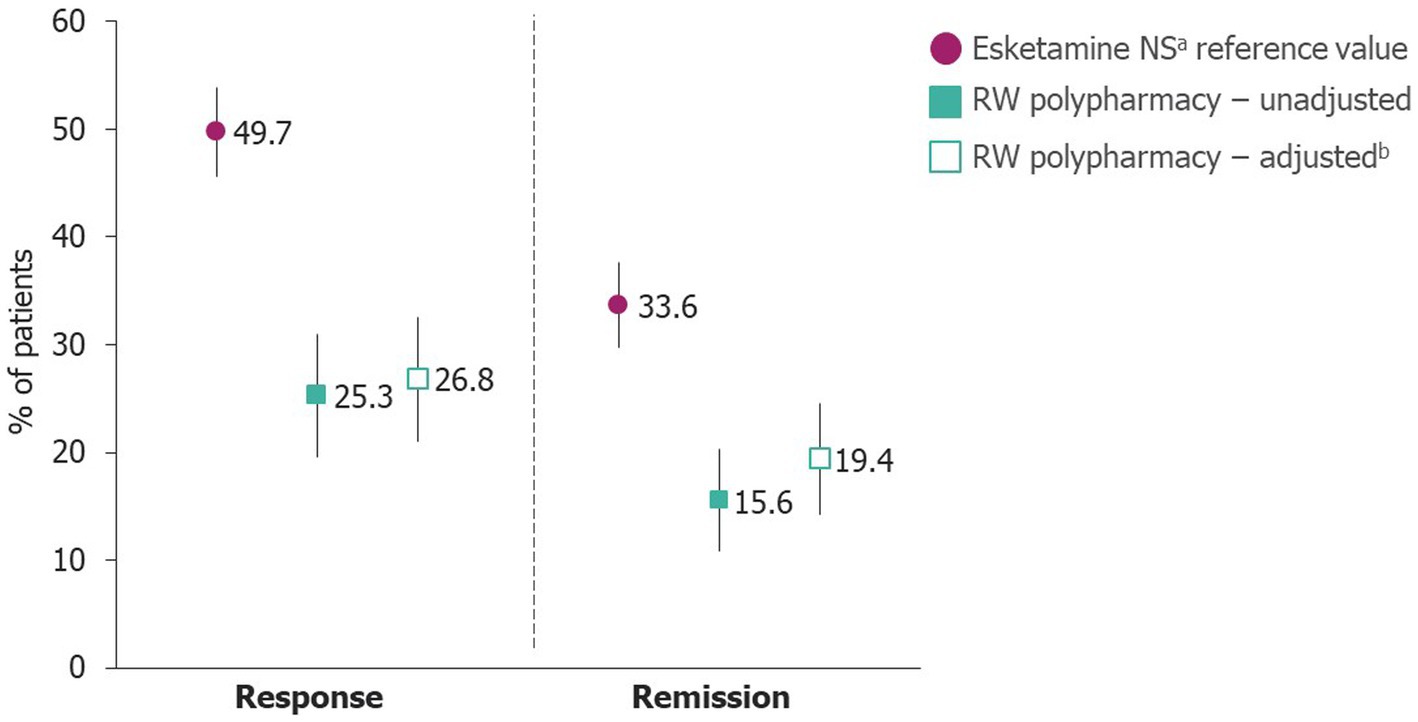
Figure 1. Probability of response and remission at Month 6. aGiven in combination with an SSRI or SNRI; bRW polypharmacy data were adjusted using the ATT-cumulative covariate adjustment method. Error bars represent upper and lower CIs. ATT, rescaled average treatment effect among treated; CI, confidence interval; NS, nasal spray; RW, real-world; SNRI, serotonin norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
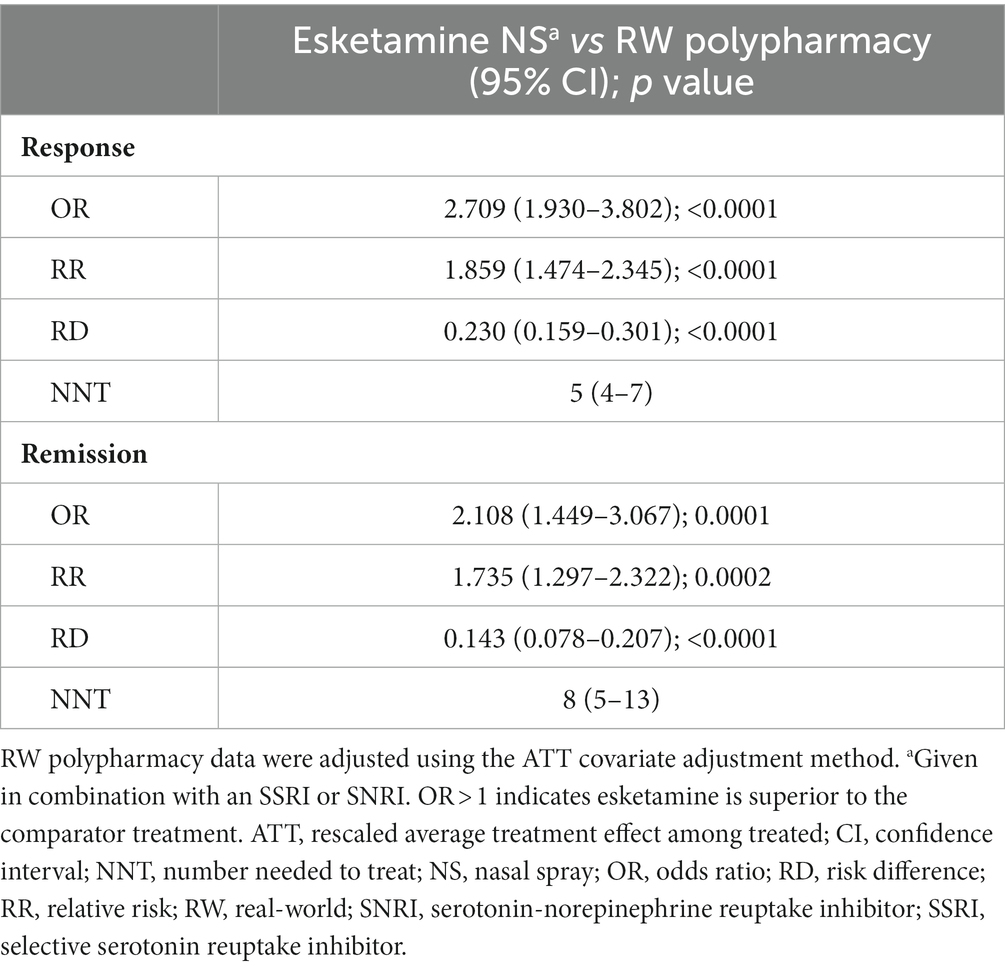
Table 2. Relative chances of response and remission at Month 6.
In unadjusted analyses, remission was reached by 188/559 (33.6%) patients receiving esketamine NS and 35/225 (15.6%) patients receiving RW polypharmacy at Month 6. Following ATT IPW adjustments, the estimated probability (95% CI) of remission for esketamine NS was 33.6% (29.7–37.6%) and 19.4% (14.2–24.6%) in the RW polypharmacy group (Figure 1). The OR (95% CI) of achieving remission with esketamine NS versus RW polypharmacy was 2.108 (1.449–3.067; p = 0.0001; Table 2). Regarding RR, patients taking esketamine NS were 1.735 (1.297–2.322, p = 0.0002) times as likely to achieve remission than patients on RW polypharmacy. RD (95% CI) values represented an additional 14.3% (7.8–20.7%) of patients achieving remission on esketamine NS compared with RW polypharmacy. NNT values showed that eight patients need to be treated with esketamine NS so that one more patient would achieve remission relative to the numbers obtained with RW polypharmacy.
The main analysis used the ATT IPW adjustment approach to reweighting. Three sensitivity analyses using alternative IPW approaches (average treatment effect among control [ATC; SA1], stabilized average treatment effect [sATE; SA2] and average treatment effect among the overlap population [ATO; SA3]) also demonstrated superiority of esketamine NS over RW polypharmacy (Supplementary Tables S4, S5). To assess the impact of alternate approaches to the handling of dropouts and other sources of missing data, two further SAs were conducted, designed to be less conservative regarding inclusion in the esketamine NS group (SA4), or more conservative regarding treatment changes in the RW polypharmacy group (SA5). Baseline characteristics of the resulting SA treatment groups are shown in Supplementary Table S6. Neither SA altered the conclusion that esketamine NS was superior to RW polypharmacy, with SA5 actually suggesting a greater benefit from esketamine NS (Supplementary Tables S4, S5). Thus, the results for response and remission at Month 6 were significantly in favor of esketamine NS, across all reweighting adjustments in the RW polypharmacy group data and sensitivity analyses conducted.
Threshold analysis showed the maximum loss of absolute response rate that could occur in patients receiving esketamine NS before loss of significance (p > 0.05) in comparison with RW polypharmacy ranged from 15.4–15.9%, depending on efficacy measure. The equivalent threshold value for remission was 7.3–7.8% (Supplementary Table S7).
Multivariable analysis is presented in Supplementary Figure S5. Treatment with esketamine NS was the largest predictor of response and remission. Age at MDD diagnosis of ≥55 years was strongly associated with a reduced chance of response. Baseline MADRS >34, as well as prior failure on augmentation, SNRI, tricyclic antidepressant (TCA) or ‘other’ treatment (trazodone, nefazodone, bupropion, mirtazapine, mianserin, opipramol, agomelatine, tianeptine, reboxetine, vilazodone and vortioxetine) were also associated with a reduced chance of response. Baseline MADRS ≥31, prior failure on augmentation and prior failure on ‘other’ treatment were all associated with a reduced chance of remission.
It is widely acknowledged that TRD is a difficult condition to treat (6, 11, 13, 31). Despite the large number of treatments available for MDD and an even greater number of combinations that can be devised and tailored to each patient, response or remission is not achieved in most patients with TRD (7). With no clear evidence to date for any one pharmacological treatment being better than others, patients with TRD may remain unwell for long periods of time while multiple different medications and combinations of medications are prescribed and failed (7, 30). The indirect comparison presented here provides support for the superiority of esketamine NS over RW polypharmacy strategies used in Europe, including combinations of several antidepressants and augmentation of an oral antidepressant with medications such as antipsychotics and mood stabilizers. In fact, when compared with those receiving RW polypharmacy treatment, the chance of response to treatment in patients with TRD treated with esketamine NS relatively increased by 86%, while the likelihood of remission was relatively increased by 74%. Such an increase in remission rate may be of even greater value in the long-term, since relapse is less likely in patients with TRD who achieve remission rather than just response (32, 33).
The methods described here are widely accepted and recommended in the absence of a direct comparison (34–38). A more detailed discussion of the methods employed in this study was provided in the first analysis of these data (25), a key strength being the use of individual patient level data. Congruent conclusions across all methods and sensitivity analyses support the robustness of the main analysis.
Although the population characteristics of the two studies used in this comparison were broadly similar, it was fundamental to rule out potential bias in favor of one of the two populations due to differences in baseline characteristics. Thus, PS reweighting, using covariates corresponding to baseline patient characteristics, was used to create a well-matched pseudo control arm for the ITC analyses. These same covariates were added to the ITC models, resulting in outputs that were adjusted for potential confounding factors. Importantly, results from adjusted versus unadjusted comparisons were largely similar, confirming that treatment effect differences were not substantially biased by differences in the characteristics of the two study populations.
Threshold analyses were conducted to measure the margin by which the remission or response rate might theoretically be lost in the esketamine NS group, while retaining significant superiority over RW polypharmacy. A 15.4% loss of absolute response rate and a 7.3% loss of remission rate in patients receiving esketamine NS would be possible without losing significance in the superiority over RW polypharmacy. This analysis can also be used to measure how much a hypothetical, unobserved confounder might be contributing to artificially overestimate response or remission rates in the esketamine NS arm in the absence of significant differences relative to RW polypharmacy. Indeed, if there was a hypothetical unobserved confounder that had increased response rates by 50% and was 30% more prevalent in the SUSTAIN-2 population than the EOTC population, this could have artificially overestimated the esketamine response rate by 15% (50% x 30%) in SUSTAIN-2. However, even if such an overestimate was adjusted for, superiority of esketamine NS versus RW polypharmacy would still be statistically significant, as 15% is below the estimated margin (15.5%) calculated in the threshold analysis. Similarly, for remission, a hypothetical unobserved confounder that had increased remission rates by 35% and was 20% more prevalent in the SUSTAIN-2 population than the EOTC population, could result in an artificial overestimation of the esketamine remission rate by 7% (35% x 20%) in SUSTAIN-2. However, even after adjusting for such an overestimate, the superiority of esketamine NS versus RW polypharmacy would still be statistically significant, as 7% is below the estimated margin (7.5%) calculated in the threshold analysis. In any case, it is unlikely that unobserved confounders with such high levels of prevalence and impact exist.
This study is the first to generate data on the long-term efficacy of esketamine NS compared with routinely used polypharmacy treatment strategies and, as such, adds substantially to currently available evidence (39). Short-term (3 months) RWE data are available in country-specific studies, such as the REAL-ESK study, and show a significant reduction in depressive symptoms (40). In the ICEBERG analysis, after 6 months of treatment, esketamine NS showed significant benefit over other polypharmacy strategies. Although the efficacy of esketamine NS has been demonstrated in the context of a rapid-acting acute phase TRD treatment (20–23, 29, 41), longer-term use of esketamine NS may be of further benefit to patients to avoid relapse. The SUSTAIN-1 clinical trial examined the effect of withdrawing esketamine NS treatment (20). After 16 weeks on esketamine NS, stable remitters and responders were randomised to either continue or switch from esketamine NS to placebo NS. The risk of relapse was both substantially and significantly greater in patients who stopped esketamine NS treatment compared with those who continued. Furthermore, the relapse risk was greater in patients who had only achieved response, rather than remission, highlighting the importance of achieving remission for patients with TRD.
The results from the ICEBERG polypharmacy analyses confirmed previously published results that found numerically larger treatment effects with esketamine NS versus placebo compared with second-generation antipsychotics versus placebo (14). The polypharmacy methodology reported here allowed for further testing of the differences between esketamine NS and polypharmacy treatment. The large sample size of both the EOTC and SUSTAIN-2 studies was an important strength of these analyses. Despite creating a smaller, strategy-specific treatment dataset (polypharmacy) from the RWT group, the resulting sample size was still adequate to include all the key medically relevant variables (covering sociodemographics, treatment and disease history, and baseline clinical and patient-reported scales) in the adjustments.
The rationale for pooling combination and augmentation to create a polypharmacy subgroup population was based on several considerations. First, current treatment guidelines consistently recommend that escalation strategies after failure of second-line treatment include combination or augmentation strategies as evidence-based therapeutic approaches in TRD (28, 42, 43). However, guidelines do not specify the treatment line deemed most appropriate for initiation of either strategy (26). Second, selection of treatment options for patients with TRD beyond second-line treatment is highly individualized, taking into account previous treatment history, comorbidities and current concomitant medications, as well as each patient’s circumstances and treatment preferences (28, 43). Thus, there is no guidance for choosing either combination or augmentation strategy in any specific patient population. Third, both augmentation and combination treatment strategies are significantly associated with severe depression symptoms, high psychiatric burden, treatment resistance and high levels of comorbidities (44). Patients in these treatment groups are likely to be more complex than patients on monotherapy, having reached these types of treatments via stepwise treatment escalation, but are not necessarily more complex than each other. In summary, there is no robust evidence to suggest that either combination or augmentation therapy is more effective than the other, and this is reflected in the treatment-agnostic approach set out in the current guidelines to select between one or the other (28, 42, 43).
Ideally, a direct and randomised comparison of esketamine NS with all other treatments and combinations used in routine clinical practice would be conducted. However, such is the heterogeneity of treatments prescribed to patients with TRD (7), that it would be prohibitively complicated to design such an interventional study with the numbers of patients needed to statistically power each individual comparison. An indirect treatment comparison using data from two well-aligned studies was therefore considered as a best-in-class alternative approach, albeit still restricted by the heterogeneity of the RW polypharmacy data. The EOTC patients, together, reported over 50 different pharmacological treatments at baseline (7), with the top five treatments representing only 40% of the medications reported by patients, and thus not representing the majority. To analyse individual treatments and combinations in the EOTC would result in too small sample sizes; this would hinder the inclusion of relevant adjustment variables into the statistical regression model (PSs) and leave the results vulnerable to potential confounders.
When data from patients on monotherapy were analysed, PS reweighting failed to reduce the mean difference between the treatments across any of the variables, even when fewer variables were included in the model. The size of the monotherapy population was thus insufficient to provide a reliable adjusted comparison for a robust ITC analysis and polypharmacy treatment is the smallest comparator subgroup for which ITC analysis is presented. This polypharmacy grouping may have masked differences in efficacy between esketamine NS and individual pharmacological treatments that may otherwise have been apparent. However, the high degree of additional benefit of esketamine NS over polypharmacy adds confidence to the conclusions drawn. Furthermore, such a stratification by treatment strategy type (i.e., separating out the polypharmacy subgroup) resulted in a more homogenous pool of treatments than when analysing the mixed RWT group as a whole (i.e., patients receiving any pharmacological treatment). Stratification therefore provided a good trade-off between the homogeneity of the comparator and the ability to adjust for potential confounders, optimizing the unbiased estimation of treatment effect.
As in any non-randomised comparison, residual confounding due to unobserved prognostic factors cannot be ruled out. However, most clinically important variables were taken into account in these analyses. It is possible that study-related factors aside from the specific medications received may have differentially influenced response and remission rates in the esketamine NS group compared with the RW polypharmacy group. For example, motivation and compliance of patients in the SUSTAIN-2 trial may have been higher due to the nature of clinical trial management. Furthermore, patients in SUSTAIN-2 had more frequent clinic visits than those in the EOTC, since healthcare professionals were required to directly supervise administration of esketamine NS, and the impact of increased contact with healthcare professionals in this context is unknown. However, threshold analyses suggest that, to change the conclusion regarding the significant benefit of esketamine NS over RW polypharmacy, the impact of such study-related factors would need to be substantial.
An open-label randomised study to compare esketamine NS with extended-release quetiapine (ESCAPE-TRD; NCT04338321) will provide additional comparative evidence (45). Quetiapine is an augmentation agent that is recommended as an add-on treatment in patients with MDD who have had a suboptimal response to treatment with other antidepressants (46). In the interim, this ITC provides data supporting the benefit of esketamine NS over a very diverse set of polypharmacy treatment strategy types.
This indirect treatment comparison suggests esketamine NS is beneficial over the RW polypharmacy strategies currently used in general psychiatry for treatment of TRD. This evidence is robust, and indicates that the benefit extends beyond acute use, with substantial improvements in the chances of achieving remission over other treatment strategies after 6 months. Esketamine NS, as a more effective alternative to existing RW polypharmacy strategy types, may provide a clearer treatment path for patients in an otherwise heterogenous treatment landscape, and thus increase their chances of achieving remission quickly.
To view an animated summary of this publication, please click on the Supplementary video, or visit the manuscript online at: https://doi.org/10.3389/fpsyt.2023.1250987.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not required for the studies involving humans because as this publication reports findings from an indirect treatment comparison, ethical approval was independently obtained from the primary studies. Further information regarding ethical approval can be found in the respective primary publications. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because as this publication reports findings from an indirect treatment comparison, written informed consent from patients was not required for this analysis.
AJOM, BR, JM, YG, JC, NP, and SMH contributed to study conception, design, analysis, interpretation of the data, and drafting the article or revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
The authors thank the patients, the investigators and their teams who took part in this study. The authors also acknowledge Julia Stevens, and Emma Phillips, from Costello Medical, UK, for medical writing and editorial assistance based on the authors’ input and direction.
AJOM received grants from Schuhfried GmBH, Janssen and Compass Pathways, Ltd, payment or honoraria from MSD, Neurolite AG, Janssen, and the European Monitoring Centre for Drugs and Drug Addiction, participated in advisory boards for Janssen and Angelini, investigator-driven research funded by Fundação para Ciência e Tecnologia (PTDC/MED-NEU/31331/2017; PTDC/SAU-NUT/3507/2021; PTDC/MED-NEU/1552/2021), Fundação para Ciência e Tecnologia and FEDER (PTDC/MEC-PSQ/30302/2017_LISBOA-01-0145-FEDER-030845; PTDC/MEC-PSQ/30302/2017_LISBOA-01-0145-FEDER-30302), the European Commission Horizon 2020 program (H2020-SC1-2017-CNECT-2-777167-ΒΟUNCE; H2020-SC1-DTH-2019-875358-FAITH), the European Joint Programme in Rare Diseases (Joint Translational Call 2019) through Fundação para Ciência e Tecnologia (EJPRD/0001/2020) and the European Research Council (grant agreement 950357). JM is a former employee of Janssen EMEA and current employee of AbbVie. BR, YG, JC, NP, and SMH are employees of Janssen EMEA.
The authors declare that this study was sponsored by Janssen EMEA. The funder had the following involvement in the study: this article was based on the original studies 54135419DEP4001 and ESKETINTRD3004, both sponsored by Janssen EMEA. Support for third-party writing assistance for this article, provided by Julia Stevens, and Emma Phillips, Costello Medical, UK, was funded by Janssen EMEA in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1250987/full#supplementary-material
1. European Medicines Agency. Guideline on clinical investigation of medicinal products in the treatment of depression. EMA/CHMP/185423/2010 rev 2. (2013). Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-depression_en.pdf (Accessed June 16, 2023).
2. Souery, D, Amsterdam, J, de Montigny, C, Lecrubier, Y, Montgomery, S, Lipp, O, et al. Treatment resistant depression: methodological overview and operational criteria. Eur Neuropsychopharmacol. (1999) 9:83–91. doi: 10.1016/S0924-977X(98)00004-2
3. Al-Harbi, KS. Treatment-resistant depression: therapeutic trends, challenges, and future directions. Patient Prefer Adherence. (2012) 6:369–88. doi: 10.2147/PPA.S29716
4. Jaffe, DH, Rive, B, and Denee, TR. The humanistic and economic burden of treatment-resistant depression in Europe: a cross-sectional study. BMC Psychiatry. (2019) 19:247. doi: 10.1186/s12888-019-2222-4
5. Rush, AJ, Trivedi, MH, Wisniewski, SR, Nierenberg, AA, Stewart, JW, Warden, D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. (2006) 163:1905–17. doi: 10.1176/ajp.2006.163.11.1905
6. Voineskos, D, Daskalakis, ZJ, and Blumberger, DM. Management of Treatment-Resistant Depression: challenges and strategies. Neuropsychiatr Dis Treat. (2020) 16:221–34. doi: 10.2147/NDT.S198774
7. Heerlein, K, Perugi, G, Otte, C, Frodl, T, Degraeve, G, Hagedoorn, W, et al. Real-world evidence from a European cohort study of patients with treatment resistant depression: treatment patterns and clinical outcomes. J Affect Dis. (2021) 290:334–44. doi: 10.1016/j.jad.2021.03.073
8. Gaynes, BN, Warden, D, Trivedi, MH, Wisniewski, SR, Fava, M, and Rush, JA. What did STAR*D teach us? Results from a large-scale, practical, clinical trial for patients with depression. Psychiatr Serv. (2009) 60:1439–45. doi: 10.1176/ps.2009.60.11.1439
9. Amos, TB, Tandon, N, Lefebvre, P, Pilon, D, Kamstra, RL, Pivneva, I, et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression: a matched-cohort study using a US commercial claims database. J Clin Psychiatry. (2018) 79:11725. doi: 10.4088/JCP.17m11725
10. Mrazek, DA, Hornberger, JC, Altar, CA, and Degtiar, I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996-2013. Psychiatr Serv. (2014) 65:977–87. doi: 10.1176/appi.ps.201300059
11. Ionescu, DF, Rosenbaum, JF, and Alpert, JE. Pharmacological approaches to the challenge of treatment-resistant depression. Dialogues Clin Neurosci. (2015) 17:111–26. doi: 10.31887/DCNS.2015.17.2/dionescu
12. Cantù, F, Ciappolino, V, Enrico, P, Moltrasio, C, Delvecchio, G, and Brambilla, P. Augmentation with atypical antipsychotics for treatment-resistant depression. J Affect Disord. (2021) 280:45–53. doi: 10.1016/j.jad.2020.11.006
13. Dunner, DL, Rush, AJ, Russell, JM, Burke, M, Woodard, S, Wingard, P, et al. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J Clin Psychiatry. (2006) 67:688–95. doi: 10.4088/JCP.v67n0501
14. Dold, M, Bartova, L, and Kasper, S. Treatment response of add-on Esketamine nasal spray in resistant major depression in relation to add-on second-generation antipsychotic treatment. Int J Neuropsychopharmacol. (2020) 23:440–5. doi: 10.1093/ijnp/pyaa034
15. Hillhouse, TM, and Porter, JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. (2015) 23:1–21. doi: 10.1037/a0038550
16. Artigas, F. Glutamatergic antidepressants? The intriguing antidepressant properties of ketamine. Revista de Psiquiatría y Salud Mental. (2011) 4:183–6. doi: 10.1016/j.rpsm.2011.07.002
17. Gonda, X, Dome, P, Neill, JC, and Tarazi, FI. Novel antidepressant drugs: Beyond monoamine targets. CNS Spectr. (2021):1–10. doi: 10.1017/S1092852921000791
18. Murrough, JW, Abdallah, CG, and Mathew, SJ. Targeting glutamate signalling in depression: progress and prospects. Nat Rev Drug Discov. (2017) 16:472–86. doi: 10.1038/nrd.2017.16
19. European Medicines Agency. Esketamine nasal spray summary of product characteristics. (2021). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/spravato (Accessed June 16, 2023).
20. Daly, EJ, Trivedi, MH, Janik, A, Li, H, Zhang, Y, Li, X, et al. Efficacy of Esketamine nasal spray plus Oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. (2019) 76:893–903. doi: 10.1001/jamapsychiatry.2019.1189
21. Fedgchin, M, Trivedi, M, Daly, EJ, Melkote, R, Lane, R, Lim, P, et al. Efficacy and safety of fixed-dose Esketamine nasal spray combined with a new Oral antidepressant in treatment-resistant depression: results of a randomized, double-blind, active-controlled study (TRANSFORM-1). Int J Neuropsychopharmacol. (2019) 22:616–30. doi: 10.1093/ijnp/pyz039
22. Ochs-Ross, R, Daly, EJ, Zhang, Y, Lane, R, Lim, P, Morrison, RL, et al. Efficacy and safety of Esketamine nasal spray plus an Oral antidepressant in elderly patients with treatment-resistant depression-TRANSFORM-3. Am J Geriatr Psychiatry. (2020) 28:121–41. doi: 10.1016/j.jagp.2019.10.008
23. Popova, V, Daly, EJ, Trivedi, M, Cooper, K, Lane, R, Lim, P, et al. Efficacy and safety of flexibly dosed Esketamine nasal spray combined with a newly initiated Oral antidepressant in treatment-resistant depression: a randomized double-blind active-controlled study. Am J Psychiatry. (2019) 176:428–38. doi: 10.1176/appi.ajp.2019.19020172
24. U.S. Food and Drug Administration. Esketamine US prescribing information. (2019). Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211243lbl.pdf (Accessed June 16, 2023).
25. Oliveira-Maia, AJ, Morrens, J, Rive, B, Godinov, Y, Cabrieto, J, Perualila, N, et al. ICEBERG study: an indirect adjusted comparison estimating the long-term benefit of esketamine nasal spray when compared with routine treatment of treatment resistant depression in general psychiatry. Front. Psychiatry (2023) 14:1250980. doi: 10.3389/fpsyt.2023.1250980
26. Bayes, AJ, and Parker, GB. Comparison of guidelines for the treatment of unipolar depression: a focus on pharmacotherapy and neurostimulation. Acta Psychiatr Scand. (2018) 137:459–71. doi: 10.1111/acps.12878
27. DGPPN. S3 guidelines for unipolar depression, 2nd Ed. (2017). Available at: https://www.dgppn.de/_Resources/Persistent/d53e5967ade4134e444e71973752e10bcaebda79/S3-NVL_depression-2aufl-vers1-kurz.pdf
28. National Institute for Health and Care Excellence. Clinical guideline [CG90]: the NICE guideline on the treatment and Management of Depression in adults. (2020). Available at: https://www.nice.org.uk/guidance/cg90/evidence/full-guidline-pdf-4840934509 (Accessed June 16, 2023).
29. Wajs, E, Aluisio, L, Holder, R, Daly, EJ, Lane, R, Lim, P, et al. Esketamine nasal spray plus Oral antidepressant in patients with treatment-resistant depression: assessment of long-term safety in a phase 3, open-label study (SUSTAIN-2). J Clin Psychiatry. (2020) 81:19m12891. doi: 10.4088/JCP.19m12891
30. Heerlein, K, Young, A, Otte, C, Frodl, T, Degraeve, G, Hagedoorn, W, et al. Real-world evidence from a European cohort study of patients with treatment resistant depression: baseline patient characteristics. J Affect Disord. (2021) 283:115–22. doi: 10.1016/j.jad.2020.11.124
31. Kverno, KS, and Mangano, E. Treatment-resistant depression: approaches to treatment. J Psychosoc Nurs Ment Health Serv. (2021) 59:7–11. doi: 10.3928/02793695-20210816-01
32. Mendlewicz, J. Towards achieving remission in the treatment of depression. Dialogues Clin Neurosci. (2008) 10:371–5. doi: 10.31887/DCNS.2008.10.4/jmendlewicz
33. Rush, AJ, Kraemer, HC, Sackeim, HA, Fava, M, Trivedi, MH, Frank, E, et al. Report by the ACNP task force on response and remission in major depressive disorder. Neuropsychopharmacology. (2006) 31:1841–53. doi: 10.1038/sj.npp.1301131
34. Faria, R., Hernandez Alava, M., Manca, A., and Wailoo, A.J. NICE DSU technical support document 17: The use of observational data to inform estimates of treatment effectiveness for technology appraisal: Methods for comparative individual patient data. (2015).
35. Haute Autorité de santé. (2020). Choices in methods for economic evaluation 2020. Available at: https://www.has-sante.fr/jcms/r_1499251/en/choices-in-methods-for-economic-evaluation (Accessed June 16, 2023).
36. Hoaglin, DC, Hawkins, N, Jansen, JP, Scott, DA, Itzler, R, Cappelleri, JC, et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR task force on indirect treatment comparisons good research practices: part 2. Value Health. (2011) 14:429–37. doi: 10.1016/j.jval.2011.01.011
37. Klinkhammer-Schalke, M, Kaiser, T, Apfelbacher, C, Benz, S, Dreinhöfer, KE, Geraedts, M, et al. Manual for methods and use of routine practice data for knowledge generation. Gesundheitswesen. (2020) 82:716–22. doi: 10.1055/a-1237-4011
38. Latimer, NR. Survival analysis for economic evaluations alongside clinical trials-extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Mak. (2013) 33:743–54. doi: 10.1177/0272989X12472398
39. Capuzzi, E, Caldiroli, A, Capellazzi, M, Tagliabue, I, Marcatili, M, Colmegna, F, et al. Long-term efficacy of intranasal Esketamine in treatment-resistant major depression: a systematic review. Int J Mol Sci. (2021) 22:9338. doi: 10.3390/ijms22179338
40. Martinotti, G, Vita, A, Fagiolini, A, Maina, G, Bertolino, A, Dell'Osso, B, et al. Real-world experience of esketamine use to manage treatment-resistant depression: a multicentric study on safety and effectiveness (REAL-ESK study). J Affect Disord. (2022) 319:646–54. doi: 10.1016/j.jad.2022.09.043
41. Daly, EJ, Singh, JB, Fedgchin, M, Cooper, K, Lim, P, Shelton, RC, et al. Efficacy and safety of intranasal Esketamine adjunctive to Oral antidepressant therapy in treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. (2018) 75:139–48. doi: 10.1001/jamapsychiatry.2017.3739
42. Bennabi, D, Charpeaud, T, Yrondi, A, Genty, JB, Destouches, S, Lancrenon, S, et al. Clinical guidelines for the management of treatment-resistant depression: French recommendations from experts, the French Association for Biological Psychiatry and Neuropsychopharmacology and the fondation FondaMental. BMC Psychiatry. (2019) 19:262. doi: 10.1186/s12888-019-2237-x
43. Cleare, A, Pariante, CM, Young, AH, Anderson, IM, Christmas, D, Cowen, PJ, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J Psychopharmacol. (2015) 29:459–525. doi: 10.1177/0269881115581093
44. Dold, M, Bartova, L, Mendlewicz, J, Souery, D, Serretti, A, Porcelli, S, et al. Clinical correlates of augmentation/combination treatment strategies in major depressive disorder. Acta Psychiatr Scand. (2018) 137:401–12. doi: 10.1111/acps.12870
45. ClinicalTrials.Gov. NCT04338321. (2020). Available at: https://clinicaltrials.gov/ct2/show/NCT04338321 (Accessed June 16, 2023).
46. European Medicines Agency. (2014). Questions and answers on Seroquel, Seroquel XR and associated names (quetiapine). Available at: https://www.ema.europa.eu/en/documents/referral/questions-answers-seroquel-seroquel-xr-associated-names-quetiapine_en.pdf (Accessed June 16, 2023).
Keywords: treatment resistant depression, real-world evidence, indirect comparison, augmentation, polypharmacy, esketamine nasal spray
Citation: Oliveira-Maia AJ, Rive B, Morrens J, Godinov Y, Cabrieto J, Perualila N and Mulhern-Haughey S (2023) Indirect adjusted comparison of 6-month clinical outcomes between esketamine nasal spray and other real-world polypharmacy treatment strategies for treatment resistant depression: results from the ICEBERG study. Front. Psychiatry. 14:1250987. doi: 10.3389/fpsyt.2023.1250987
Edited by:
Marcin Siwek, Jagiellonian University, Medical College, PolandReviewed by:
Mariusz Stanisław Wiglusz, Medical University of Gdansk, PolandCopyright © 2023 Oliveira-Maia, Rive, Morrens, Godinov, Cabrieto, Perualila and Mulhern-Haughey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benoit Rive, YnJpdmVAaXRzLmpuai5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.